Cholestérol: Quelle normalité? chol.pdf · HPS-S 4S-S HPS-P CARE-P LIPID-P 4S-P 0 5 10 15 20 25...
61
Cholestérol: Quelle normalité? C. Abdelkhirane, MD, PhD Cardiologue Cardiologie Maarif ∞ Clinique Maarif AMBM/AMCAR 19 février 2015
Transcript of Cholestérol: Quelle normalité? chol.pdf · HPS-S 4S-S HPS-P CARE-P LIPID-P 4S-P 0 5 10 15 20 25...

Cholestérol: Quelle normalité?
C. Abdelkhirane, MD, PhD
Cardiologue
Cardiologie Maarif ∞ Clinique Maarif
AMBM/AMCAR 19 février 2015

C=control; T=treatment; A=aggressive; M=moderate.
Yusuf S, Anand S. Circulation. 1996;93:1774-1776.
5
10
15
20
25
Post-treatment TC (mg/dL)
5-yr CV events (%)
CARE-T
Post-CABG-A 4S-T
CARE-C
Post-CABG-M 4S-C
155 174 193 212 232 251 271
Risk of CHD Events and Level of
Cholesterol

PI=placebo; Rx=treatment Shepherd J et al. N Engl J Med. 1995;333:1301-1307. 4S Study Group. Lancet. 1995;345:1274-1275. Sacks FM et al. N Engl J Med. 1996;335:1001-1009. Downs JR et al. JAMA. 1998;279:1615-1622. Tonkin A. Presented at AHA Scientific Sessions, 1997.
Mean LDL-C level at follow-up (mg/dL)
Relation Between CHD Events and
LDL-C in Recent Statin Trials
0
5
10
15
20
25
30
90 110 130 150 170 190 210
% with CHD event CARE-Rx
LIPID-Rx
4S-Rx
CARE-PI LIPID-PI
4S-PI
2° Prevention
1° Prevention
WOSCOPS-PI
WOSCOPS-Rx AFCAPS/TexCAPS-Rx
AFCAPS/TexCAPS-PI

CHD Event Rates in Secondary Prevention and ACS Trials
Updated from - O’Keefe, J. et al., J Am Coll Cardiol 2004;43:2142-6.
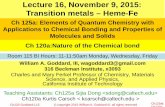
y = 0.1629x · 4.6776 R² = 0.9029 p < 0.0001
LDL Cholesterol (mg/dl)
CH
D E
ven
ts (
%)
PROVE-IT-PR
PROVE-IT-AT CARE-S
LIPID-S
HPS-S 4S-S
HPS-P
CARE-P
LIPID-P
4S-P
0
5
10
15
20
25
30
30 50 70 90 110 130 150 170 190 210
TNT 80
TNT 10 A2Z 80
A2Z 20
IDEAL S20/40
IDEAL A80

Cholesterol Trialist Collaboration Meta-Analysis of Dyslipidemia Trials
50%
40%
30%
20%
10%
0%
-10%
Adapted from CTT Collaborators. Lancet. 2005; 366:1267-78
0.5 1.0 1.5 2.0
Reduction in LDL Cholesterol (mmol/L)
Major Vascular Events P
rop
ort
ion
al R
edu
ctio
n in
Eve
nt
Rat
e (S
E)
TNT
IDEAL

The Statin Decade For LDL: “Lower is Better”
0
5
10
15
20
25
30R² = 0.9029 p < 0.0001
LDL Cholesterol (mg/dl)
CH
D E
ven
ts (
%)
Adapted and Updated from O’Keefe, J. et al., J Am Coll Cardiol 2004;43:2142-6.
30 50 70 90 110 130 150 170 190 210
4S
CARE LIPID
HPS
PROVE IT –TIMI 22
66 52
TNT
IMPROVE IT

Odds ratio
0.5 1 3.0
Study (n)
Treatment Achieved LDL (mg/dl)
Odds ratio (95% CI)
0.74 (0.58,0.94) TNT (10,001) Atorvastatin 80 77
0.72 (0.52,0.98) A to Z (4497) Simvastatin 80 63
0.54 (0.34,0.85) PROVE-IT (4162) Atorvastatin 80 62
0.80 (0.61,1.05) IDEAL (8888) Atorvastatin 80 81
0.73 (0.63,0.84), p<0.001 Overall (95% CI)
Intensive statin therapy better
Moderate statin therapy better
Atorvastatin 10 101
Simvastatin 20 77
Pravastatin 40 95
Simvastatin 20 104
Intensive Moderate
Scirica BM, et al. AHA 2005
Meta-Analysis of Intensive Statin Therapy CHF

Quelques exemples de rendus d’analyses biologiques






Définitions
Norme : Règle, principe, critère auquel se réfère tout jugement Normalité : 1-État, caractère de ce qui est conforme à la norme, à ce qui est considéré comme l'état normal. 2-Rapport de la concentration d'une solution titrée à celle de la solution normale du même corps dissous. (La normalité d'une solution normale est égale à l'unité.) 3-En psychiatrie, caractère heureux des relations aux autres et à soi-même, quelle que puisse être la nature des conflits sous-jacents.
LAROUSSE, 2014

La loi Normale (Laplace-Gauss)

La densité de la courbe modale

La répartition modale

La symétrie (normale)

Distribution non normale

Densité de probabilité (Fonction de masse)
La courbe rouge représente la fonction Phi, densité de probabilité de la loi normale centrée réduite.

Fonction de répartition
La courbe rouge représente la fonction Théta , fonction de répartition de la loi normale centrée réduite.

Courbes en biologie humaine!!!


Modèle du cholestérol cutané et le pourcentage des sténoses artérielles


Etablissement d’une normalité

The area under a density estimate curve: Parametric estimates - The DO Loop on September 5, 2011

The area under a density estimate curve: Parametric estimates - The DO Loop on September 5, 2011
a
a

Peterbuck, Primary and early secondary prevention of cardiovascular disease, 2010

Influence de l’âge sur la distribution
Circulation.1998; 97: 1087-1094 doi: 10.1161/01.CIR.97.11.1087

Distribution vs conséquences
Martin et al. , Curr Control Trials Cardiovasc Med (2001)

The Princeton Longevity Center Medical News, 2010

Quel niveau de cholestérol pour quel pays?

Maroc



Implication du changement de normes
H. Gilbert Welch et al, Dartmouth Medicine Mag, 2010
+13.000.000

Que disent les recommandations?


SCORE Scale
• A particular problem relates to young people with high levels of risk factors.
• Although the absolute SCORE risk can be low in young patients, if several risk factors are present, the relative risk will be high. ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011 Jul;32(14):1769-818.

SCORE Scale
• The preference for the SCORE system over other risk scales is based on the fact that it was designed and evaluated using representative European cohorts.
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011 Jul;32(14):1769-818.

SCORE Scale
• The SCORE scale allows for estimating the 10-year risk of the first fatal atherosclerotic complication based on the following risk factors:
– Age
– Gender
– Smoking
– Systolic blood pressure
– Total cholesterol
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011 Jul;32(14):1769-818.

Score Européen selon régions
Région risque bas :Belgium, Germany, Finland, France, Greece, Italy, Spain, Denmark, The Netherlands, United Kingdom, Sweden, Norway, Iceland, Ireland, Austria, Malta, Portugal, Slovenia, Monaco, San Marino.
Région risque haut:Bulgaria, Macedonia, Russia, Moldova, Ukraine, Belarus, Latvia.

SCORE Scale
• SCORE database has shown that HDL-C modifies risk at all levels of risk as estimated from the SCORE cholesterol charts.
• Risk will be higher than indicated in the charts in individuals with low HDL-C.
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011 Jul;32(14):1769-818.

Stratégies d’intervention
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2011 Jul;32(14):1769-818.


Risk Category
CHD and CHD risk equivalents Multiple (2+) risk factors Zero to one risk factor
LDL Goal (mg/dL)
<100
<130 <160
Three Categories of Risk that Modify LDL-C GOALS
ATP-3 update, Circulation, 2004

New 2013 ACC/AHA guidelines on treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in Adults
• 1-Le traitement doit être considéré dans un contexte de prévention vasculaire intégrée : usage d’un Score du risque CV Absolu
• 2-Le niveau d’action est déclenché par le taux de LDL-C: des patients à très haut, à haut et à risque intermédiaire
• 3-Les statines sont LE choix dans le traitement, mais avec une nouvelle façon : intensité du traitement
• 4-Les objectifs du traitement doivent être détaillés pour chaque situation clinique
• 5-Modifications du style de vie
Stone Nj, Robinson J, Lichtenstein Ah, Bairey Merz Cn, Lioyd-jones Dm, Blum Cb, Mcbride P, eckel Rh, Schwartz Js, Goldberg Ac, Shero St, Gordon D, Smith Sc Jr, Levy D, Watson K, Wilson Pw. 2013 ACC/AHA Guideline On The Treatment Of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk In Adults: A Report Of The American College Of Cardiology/American Heart Association Task Force On Practice Guidelines. J Am Coll Cardiol. 2013 Nov 7. Pii: S0735-1097


1,9g/L 1,10 g/L 0,39 g/L 1,7 g/L




Objectifs selon régions du monde Cholestérol total
Total Cholesterol (US et w) Total cholesterol (Can , Eu)
<200mg/dL <5.2 mmol/L Désirable
200-239 mg/dL 5.2 – 6.2 mmol/L Borderline haut
≥240 mg/dL >6.2 mmol/L haut
NHLBI. http://nhlbi.gov/guidelines/cholesterol/index.htm. May 31, 2012

Objectifs selon les régions LDL
LDL Cholesterol (US et w) LDL cholesterol (Can , Eu)
<70 mg/dL <1.8 mmol/L Idéal pour très haut risque
<100 mg/dL <2.6 mmol/L Idéal pour haur risque
100-129 mg/dL 2.6-3.3 mmol/L Presque idéal
130-159 mg/dL 3.4-4.1 mmol/L Borderline haut
160-189 mg/dL 4.2-4.9 mmol/L Haut
>190 >4.0 mmol/L Très haut
NHLBI. http://nhlbi.gov/guidelines/cholesterol/index.htm. May 31, 2012

Objectifs selon régions du monde HDL
Total Cholesterol (US et w) Total cholesterol (Can , Eu)
<40 mg/dL (H) <50 mg/dL (F)
<1 mmol/L <1.3 mmol/L
pauvre
40-49 mg/dL (H) 50-50 mg/dL (F)
1-1.3 mmol/L 1.3-1.5 mmol/L
mieux
≥60 mg/dL >1.6 mmol/L meilleur
NHLBI. http://nhlbi.gov/guidelines/cholesterol/index.htm. May 31, 2012

Objectifs selon régions du monde Triglycérides
Triglycérides (US et w) Triglycérides (Can , Eu)
<150 mg/dL <1.7 mmol/L désirable
150-199 mg/dL 1.7-2.2 mmol/L Borderline haut
200-499 mg/dL 2.3-5.6 mmol/L haut
≥500 mg/dL >5.6 mmol/L Très haut
NHLBI. http://nhlbi.gov/guidelines/cholesterol/index.htm. May 31, 2012

Conclusion

La cascade de filtres sur le niveau final
• Normalisation des techniques de dosage
• Norme sur une population (cholestérol)
• Correction par le risque encouru et sa levée (taux de décès par CAD)
• Recommandation pour réajustement selon le niveau
d’intervention pour correction donnée du risque (Bonne pratique)
• Objectif final

Retenir pour nous et pour l’heure
• CT ≤ 2 g/l
• HDL ≥ 0.6 g/l
• LDL ≤1.6 g/l
• TG < 1.5 g/l