China and India Medical Issues for Expatriate and Local National Employees PAUL GRUNDY, MD -...
21
China and India Medical Issues for Expatriate and Local National Employees PAUL GRUNDY, MD - Director, Healthcare, Technology and Strategic Initiatives IBM Global Wellbeing Services and Health Benefits LYNDON E. LAMINACK, MD - Medical Director, CIGNA International LORNA FRIEDMAN, MD, MBA - Senior Medical Executive, CIGNA International
-
Upload
alma-secker -
Category
Documents
-
view
214 -
download
0
Transcript of China and India Medical Issues for Expatriate and Local National Employees PAUL GRUNDY, MD -...
China and India Medical Issues for
Expatriate and Local National Employees
PAUL GRUNDY, MD - Director, Healthcare, Technology and Strategic Initiatives IBM Global Wellbeing Services and Health Benefits
LYNDON E. LAMINACK, MD - Medical Director, CIGNA International
LORNA FRIEDMAN, MD, MBA - Senior Medical Executive, CIGNA International
CIGNA International Expatriate Benefits• CIGNA International Expatriate Benefits is the
world’s largest provider of employer-sponsored health care benefits and services for expatriate employees
• The expatriate benefits solution for more than 40% of the Fortune 100 and 25% of the Fortune 500
• Truly International Perspective– Operational Presence in More than 20 Countries– Understanding of Daily Challenges of Living/Working
Abroad– Knowledge of Local, Customs, Health Care Practices,
Laws and Compliance Issues– World-wide Compliance- Fully Compliant with all
ERISA, COBRA and HIPAA rules; Country Specific Compliance

IBM
• IBM is the fourth largest employer and is the largest information technology employer in the world. IBM remains the most profitable IT company and holds more patents than any other U.S. based technology company
• IBM has engineers and consultants in over 170 countries and IBM Research has eight laboratories worldwide.
• IBM employees have earned three Nobel Prizes, four Turing Awards, five National Medals of Technology, and five National Medals of Science.
China: Specific Health Threats
1.Infectious Diseases
Tuberculosis, Hepatitis B
Hepatitis A
Japanese Encephalitis
Cholera
Emerging Diseases
• SARS
• Avian Influenza
2.Respiratory Illness (pollution)
3.Gastro-intestinal
4.Motor Vehicle Accidents
5.Heart Attacks

China: Notes on Health Care
• Rapid improvement in medical infrastructure in major cities
• No concept of primary care
• High cost and no care without payment
– Cash (not credit cards)
– Poor cooperation with insurance
• Long hospitalizations
• International accreditation (JCI) of a few private hospitals
• Inefficient local ambulance system
China: Issues for “Western” Expats
• Quality of Care• Access to care (Language, payment, aesthetics)• Air Quality
– Implications for employees with respiratory problems
– lead levels a concern in children• Pharmaceuticals
– “Imitation” more common than counterfeiting– Tamiflu purchased outside reputable
pharmacies is probably fake – China will allow up to one year’s supply of
prescription meds to be brought in (a practice CIEB encourages)
– Source: CIEB Medical Advisory Council
Best Practices: Western Expats
• Carve out health insurance
• Strong Assistance Provider
• Experienced EAP
• Pre-departure Preparation/Screening
• Pre-departure Medical Screening/Prep

China: Issues for Asian Expats
• Chinese-speaking expats are better able to access the system, but are accustomed to high levels of hygiene and quality
• There is a very strong distrust of Chinese hospitals for emergency and serious care (TCNs are happy to get acupuncture and try traditional medicine for routine treatment, but don’t trust the hospitals for emergencies.)
• Some Asians, such as Japanese, will have as much or more difficulty with Chinese healthcare as do Western expats.
• Culture-specific IEAP-most Asian plans exclude mental health, so there may be a heavier reliance upon EAP services if it is available
• Source: CIEB Medical Advisory Council

Best Practices: Asian Expats
• Similar to expats, but recognizing that many coming from Asia have some familiarity with China (which is both good and bad)
• Adjust insurance plan design to better fit their expectations (100% coinsurance, lower deductible, limited access to US care)
• Assistance plan is very important – Most will want to be evacuated for serious problems
• EAP important for this group, too
China: Issues for Chinese Nationals
• Quality of care/Distrust of public hospitals
• Hepatitis B, HIV testing/workplace discrimination
• Mobility issues (highly mobile society with people migrating to major cities)
• Health Promotion• Source: MAC

Best Practices: Local Nationals
• Health insurance / access to Private system
• Occupational health focus for factories – keeping the workforce healthy
• EAPs • there is a real culture clash between the
traditional way of life (slow) and the new corporate life (fast)
• New found wealth leads to concerns about responsible financial habits

India: Medical Concerns
• Drug-resistant TBc
• HIV
• Chickungunya fever
• Malaria
• MVA’s/public transport
• Diseases of affluence: obesity, diabetes, CAD, tobacco

India: Notes on Healthcare
• Many excellent doctors available. Also many charlatans. Little regulation.
• Vast improvement in private hospitals in past decade: can handle both emergencies and routine.
• Government hospitals crowded, inefficient, dirty.
• Ambulances not reliable or well-equipped.

Medical Care In India
• Prior to 1990 there were no hospitals of international standard
• ’90’s saw boom fueled by returning (NRI) doctors
• Now on verge of regional centers of excellence, promoting medical tourism
• Accreditation
• JCI
– ISO, other
– QCI (India)

Benchmarking Quality of Care: A World Bank Study
• Adults in rural Rajastan visit a doctor once/fortnight
• In Urban India, the poor visit doctors more often than the rich
• Doctors in study completed only 26% of tasks required for pt with TB; 18% for child with diarrhea
• Doctors in private sector know less but do more vis-à-vis public sector doctors
• Private sector doctors in rich areas were far more competent than in poor areas
Das & Gertler “Variations in Practice Quality in Five Low-Income Countries” Health Affairs Mar 2007
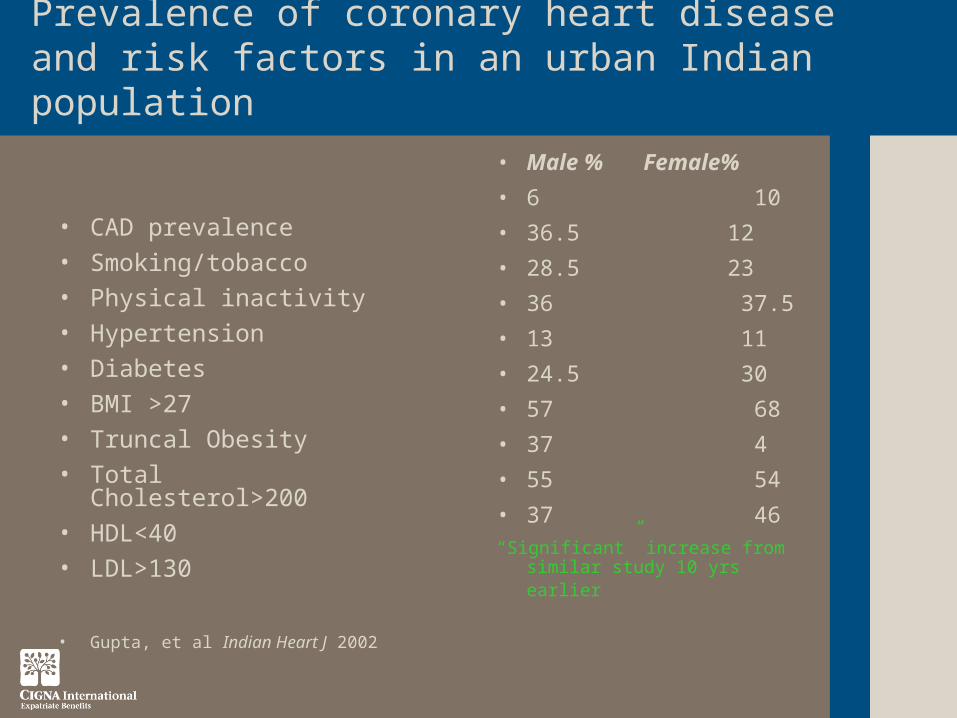
Prevalence of coronary heart disease and risk factors in an urban Indian population
• CAD prevalence• Smoking/tobacco• Physical inactivity• Hypertension• Diabetes• BMI >27• Truncal Obesity• Total Cholesterol>200• HDL<40• LDL>130
• Gupta, et al Indian Heart J 2002
• Male % Female%
• 6 10
• 36.5 12
• 28.5 23
• 36 37.5
• 13 11
• 24.5 30
• 57 68
• 37 4
• 55 54
• 37 46 “Significant” increase from
similar study 10 yrs earlier

Health Risks: Public TransportNEW DELHI (Reuters) – Jul 12 2007
“Delhi's Blue Line buses killed 59 of the 1,023 people who died on the city's roads in the first six months of this year”
Police have found a Blue Line bus in serious breach of regulations and ordered it to stop running on more than 6,000 occasions so far this year.
Many buses are halted for lacking the mechanical limiter to keep its speed below the 40 kph (25 mph) limit, for having a driver without a full license and government permit, or, like much of Delhi's traffic, for ignoring the rules of the road “
Corporate Wellness in India• Significant number of corporations are spending money on "Wellness"
• The pressure does not seem to come from any new legal requirement (Old Factory Act)
• The changes concern mostly new technologies and financial sectors involving white color workers (and no longer the blue collar workers as in the past)
• * Foreign investment/presence and an attempt to comply with headquarters International standards (ISO 9001, 14000 or more recently OSHA 18001)
• * OH/Wellness activities are particularly visible in Delhi, Mumbai, Bangalore and Chennai
• The original approach taken by these corporations is to use the OH agenda as a retention tool against high turn over in an increasing volatile and competitive labor market where white collar talents are in high demand locally. It is very common to see employers offering an Intl. standard sport/gym set up with professional trainers (outsourced) at the workplace coupled with primary care setting (on site) and OH services showing that employers do care for the wellness of their workers.
Olivier Lo, ISOS, Personal communication

• Sickness absence is not a topic capturing any interest in the corporate market in India as far as we could see (unlike in UK/Europe)
• We do not see much activity around environmental work i.e. Health Impact Assessment (unlike for our corporate clients operating in Africa or Indonesia)
Olivier Lo, ISOS, personal communication
Corporate Wellness in India

Conclusion
• Dynamic changes
• Great potential
• Challenges and caveats

Questions
Lyndon Laminack, MD
Medical Director
CIGNA International Expatriate Benefits
Phone 302.797.3167
E-Mail [email protected]
http://www.cignaexpats.com