The Relationship of Psychologic Stress With Childhood Asthma
Upload
olulode-olufemi-sCategory
view
220download
0description
Dr. Olulode Olufemi S.
**
Chronic disease of the airways that may causeWheezingBreathlessnessChest tightnessNighttime or early morning coughing
Episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.
**
AllergensInfectionsExerciseAbrupt changes in the weatherExposure to airway irritants, such as tobacco smoke**
Recurrent asthma episodes, involving Shortness of breath Coughing Wheezing Chest pain or tightnessRange in severity from Mild intermittentSevere persistent**
Increases risk for early deathCompromises childs quality of lifeAffects familys quality of lifeIncreased costs associated with Increased utilization of health care
**
Most common cause of school absenceAn average of 9.7 days per year for asthmaMost prevalent cause of childhood disability (long-term reduction in ability to do normal activities)In 1994-95, 1.4% of U.S. children experienced some disability due to asthmaThis is 21% of all children with asthmaSES disadvantage doubles rate of disabilityChildren with asthma have higher rates of social and emotional problems
**
Asthma is the most common chronic disease among childrenIt has increased at epidemic rates since the early 1980sMost common cause of ED visits, hospitalization and missed school daysIn past 2 decades, African American children had 2-4 times more ED visits than other racesStudies show a rise in worldwide prevalenceSeems to be more prevalent in affluent nations
**
Etiology of asthma is due to the interaction of environmental and genetic factorsAtopy, the genetically inherited susceptibility to asthma, cannot account for epidemic.Probably NOT due to outdoor air qualityIndoor air contaminants may be a factorTighter construction trapping contaminants.Children spending more time indoors.
**
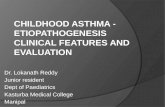
10.1% Overall**
Chart1
14.210.1
9.110.1
1010.1
7.110.1
10.210.1
Sheet1
Non-Hispanic BlackNon-HispanicWhiteHispanicAsianAmerican Indian / Alaska Native
14.29.1107.110.2
10.110.110.110.110.1
Low-income populations, minorities, and children living in inner cities experience more ED visits, hospitalizations, and deaths due to asthma than the general population.
The burden of asthma falls disproportionately on non-Hispanic black, American Indian/Alaskan Native and some Hispanic populations.**
By genderMales 0 17 years are more likely than girls to have asthma or experience an asthma attackBy race/ethnicityHigher for Black non-Hispanic childrenHigher for Hispanic children
**
Current asthma prevalence is higher amongchildren than adultsboys than girlswomen than menAsthma morbidity and mortality is higher amongAfrican Americans than Caucasians.
**
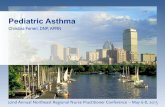
Groups 6 - 7 Yrs 13-14 Yrs
Wheeze 5.6 % 6.0% (0.8 - 14.6)(1.6 - 17.8)
> 4 attacks 1.5%1.6% (0.1 - 4.7)(0.5 - 3.5)
Night Cough 12.3%14.1% (3.3 - 27) (3.8 - 32.2)
Ever had Asthma 3.7%4.5% (1.0 - 14.4)(1.12.4)
Shah, Amdekar, Mathur, IJMS,6,2000,213-22**
**
**
**
Parental AsthmaAllergyAtopic dermatitisAllergic rhinitisFood allergy Inhalant allergen sensitization Food allergen sensitization
**
Severe lower respiratory tract infectionsWheezing apart from coldsMale genderLow birth weightTobacco smoke exposureExposure to chlorinated swimming poolsPossible use of Acetaminophen**
Common Viral infectionsAeroallergensAnimal dander Dust mite Cockroaches Molds Pollen **
Air pollutantsOzone Sulfur dioxide Particulate matter Dust Tobacco smokeStrong/ noxious fumesCold, dry airExercise
**
Occupational exposuresFarm and barn exposure Formaldehyde, paint fumesCrying, laughter, hyperventilationCo morbid conditions: Rhinitis, Sinusitis**
Symptoms:Intermittent dry coughExpiratory wheezingShortness of breathChest tightnessChest painFatigueDifficulty keeping up with peers in physical activities**
Signs:Expiratory wheezingProlonged expiratory phaseDecreased breath soundsCrackles/ ralesAccessory muscle useNasal flaringAbsence of wheezing in severe casesPulses paradoxus**
Spirometry:
Feasible in children >6 years of ageMonitoring Asthma and efficacy of treatmentMeasures FVC, FEV 1 and FEV1/FVC RatioNormal values for children available on the basis of height, gender and ethnicity.**
Airflow Limitation:Low FEV1FEV1/ FVC ratio < 0.80Bronchodilator response to -agonist:Improvement in FEV1 12%Exercise challenge:Worsening of FEV1 15%Daily peak flow or FEV1 AM-PM variation 20%
**
**
**
Often normalHyperinflationHelpful in identifying masqueraders
**
**
Asthma severity: Directs initial level of therapy Determined at the time of diagnosis Categories: Intermittent, Persistent Determined by the most severe level of symptomsAsthma control: Important for adjusting therapyRegular Clinic visits every 2-6 weeks until good control establishedTwo or more Asthma check ups per year for maintaining Asthma control
**
**
**
**
**
Achieve and maintain control of symptomsMaintain normal activity levels, including exerciseMaintain pulmonary function as close to normal levels as possiblePrevent asthma exacerbationsAvoid adverse effects from asthma medicationsPrevent asthma mortality **
Develop with a physician Tailor to meet individual needsEducate patients and families about all aspects of planRecognizing symptomsMedication benefits and side effectsProper use of inhalers and Peak Expiratory Flow (PEF) meters**
Breathless at restHunched forwardSpeaks in words rather than complete sentences AgitatedPeak flow rate less than 60% of normal**
Have an individual management plan containingYour medications (controller and quick-relief)Your asthma triggersWhat to do when you are having an asthma attackEducate yourself and others aboutAsthma Action Plans Environmental interventionsSeek help from asthma resources Join an asthma support group**
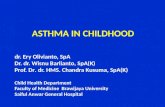
Asthma action plan for management of exacerbation
Regular follow up visitsMonitor lung functions annuallyImprove adherence to treatment
**
Eliminate/ reduce environmental exposuresTobacco smoke elimination/ reductionAllergen exposure elimination/ reductionTreat co morbid conditions: Rhinitis, Sinusitis, GER**
Initiate with higher level controller therapyStep-down, once good control is achievedIf child has had well controlled asthma for at least 3 months, consider decreasing dose or number of controller medications.Step up for poorly controlled asthma**
All persistent Asthmatics require daily controller medications**
Treatment of choice for persistent AsthmaImprove lung functionReduce use of rescue medicinesReduce ED visits, hospitalizationsMay lower the risk of death due to Asthma**
Used mainly in treatment of exacerbationsRarely in patients with severe diseaseCommon: Prednisolone, Prednisone, MethyprednisoloneWhen used in long term, cause adverse effects**
Salmeterol, FormoterolNot used as monotherapyMajor role as ad-on agents with ICSLABA use should be stopped once optimal Asthma control is achieved
**
Leukotriene synthesis inhibitor: Zileuton (Not approved for children < 12 years)Leukotriene Receptor Antagonists: Montelukast, Zafirlukast
**
Cromolyn, NedocromilInhibit exercise induced bronchospasmCan be used in combination of SABA for exercise induced bronchospasm**
Can reduce Asthma symptoms and need for SABA useNarrow therapeutic windowNot used as first line anymoreMay be used in corticostroid dependent childrenCan cause cardiac arrhythmias, seizures and death**
Anti IgE monoclonal antibodyBlocks IgE mediated allergic responseApproved for children > 12 years with moderate to severe AsthmaGiven sub cutaneously every 2-4 weeks**
Short Acting Beta Agonists: Albuterol, Levalbuterol, Terbutaline, PirbuterolDrugs of choice for acute Asthma symptomsOveruse may be associated with increased risk of deathUse of at least 1 MDI/ month or at least 3 MDI/ year indicates inadequate Asthma controlAnticholinergic Agents: Ipratropium bromide Used in combination with Albuterol
**
Dyspnea at restPeak flows < 40% of personal bestAccessory muscle useFailure to respond to initial treatment
**
Brief assessmentAdministration of SABA: Repeated doses or continuously, every 20 mins. for 1 hourInhaled anticholinergic in addition of SABAOxygen: Hypoxemia/ moderate to severe exacerbationSystemic Corticosteroids: Instituted early for moderate to severe exacerbation and failure to respond to early treatmentIntramuscular beta agonist in severe cases.
**
**
*Managing Asthma: Asthma Management GoalsManaging Asthma: Asthma Action PlanManaging Asthma: Indications of a Severe AttackManaging Asthma: Things People with Asthma Can Do