Chickenpox Causative agent –Varicella-Zoster virus –Herpes virus One of the most common rashes...
31
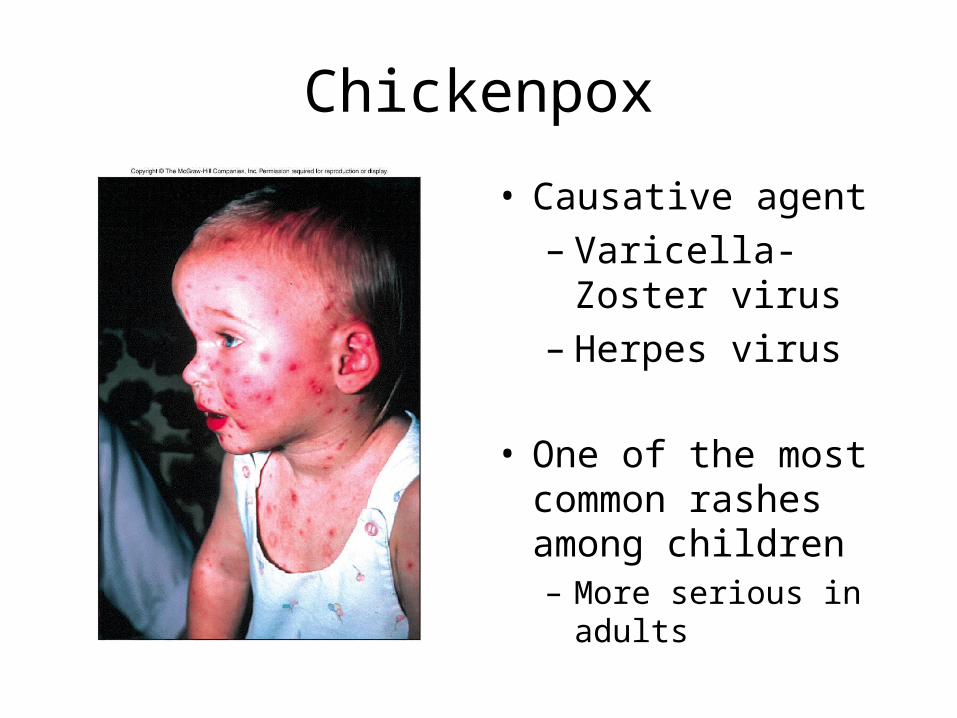
Chickenpox • Causative agent – Varicella- Zoster virus – Herpes virus • One of the most common rashes among children – More serious in adults
-
Upload
rose-jemimah-anderson -
Category
Documents
-
view
236 -
download
0
Transcript of Chickenpox Causative agent –Varicella-Zoster virus –Herpes virus One of the most common rashes...
Chickenpox
• Causative agent– Varicella-Zoster
virus– Herpes virus
• One of the most common rashes among children– More serious in adults
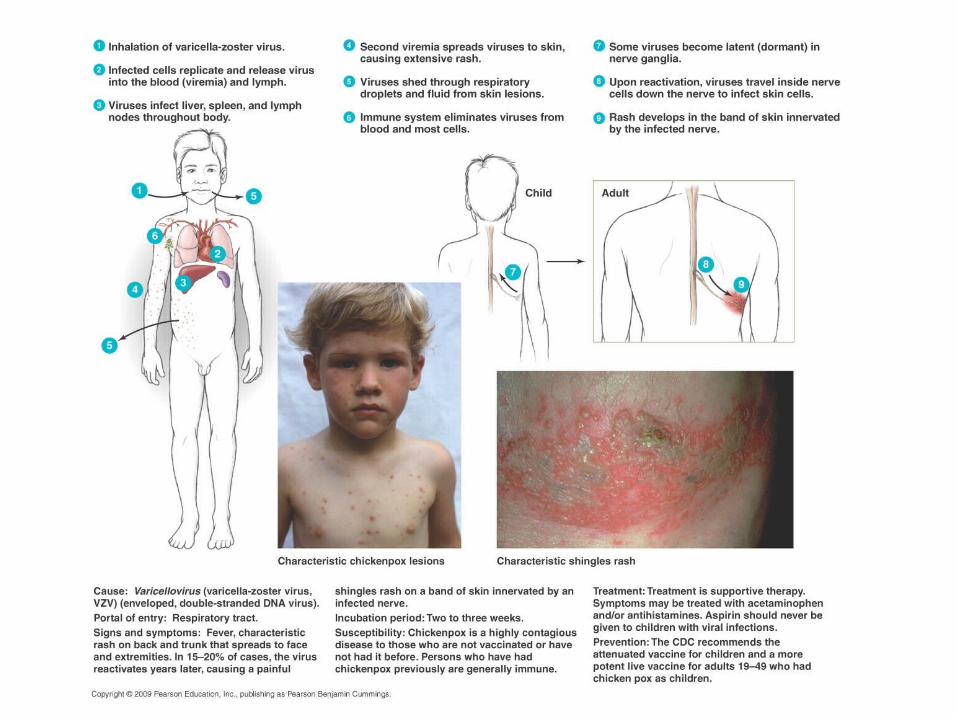
• Signs& Symptoms– Skin rash appears on body trunk then spreads to
face, neck and limbs• Rash is diagnostic• Itchy rash progresses from red spots to pus filled
blisters that break and crust over
– Viral incubation period approximately 2 weeks• Infective 1 to 2 days before rash until all blisters crust
• Epidemiology– Disease transmitted by respiratory secretions
and skin lesions– Virus typically enters through respiratory
route, replicates and moves to the skin via blood stream
– Infected cells swell and lyse• Release viruses which enter sensory nerves
– Usually self limiting
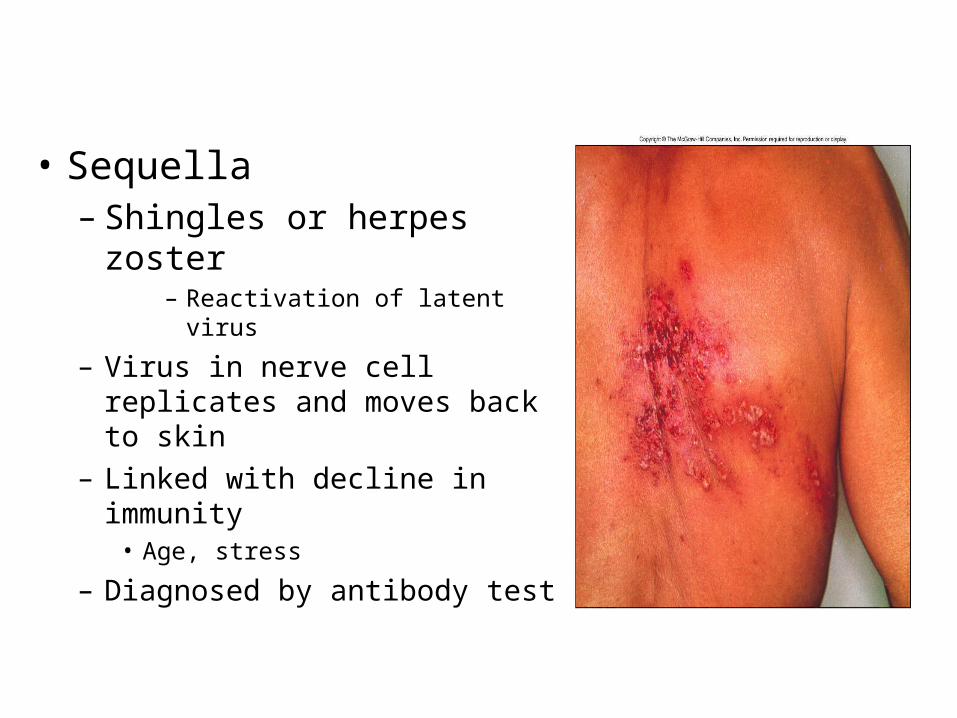
• Sequella– Shingles or herpes zoster
– Reactivation of latent virus
– Virus in nerve cell replicates and moves back to skin
– Linked with decline in immunity• Age, stress
– Diagnosed by antibody test

• Prevention and treatment– Prevention directed at vaccination
• Attenuated vaccine licensed in 1995• Recommended for healthy individuals 12 months
and older
– Treatment is directed at alleviating symptoms• Acyclovir given in high risk cases
– Reye’s Syndrome– Associated with a number of viral infections – Linked to aspirin usage in children – Characterized by vomiting and coma
» Liver and brain damage– Mortality around 30%
[INSERT DISEASE AT A GLANCE 19.7]

Measles
• Causative agent– Rubeola virus– paramyxovirus
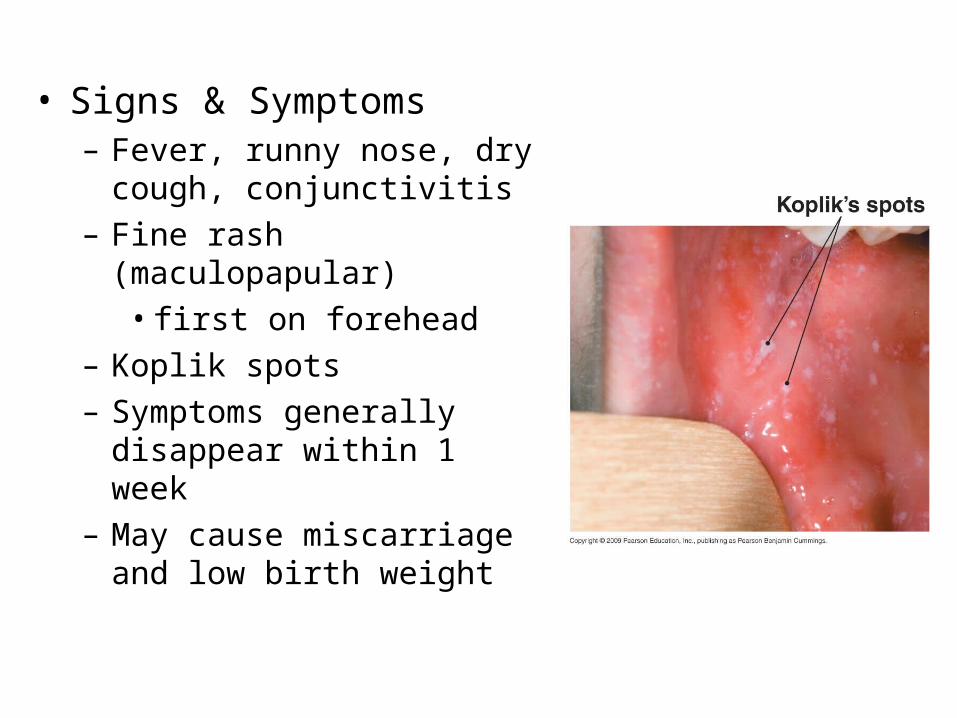
• Signs & Symptoms– Fever, runny nose, dry
cough, conjunctivitis – Fine rash (maculopapular)
• first on forehead– Koplik spots– Symptoms generally
disappear within 1 week– May cause miscarriage and
low birth weight
• Epidemiology– Humans are only natural host– Virus spread by respiratory droplets– Replicates in epithelium of upper respiratory
tract • 8-10 day incubation
– Spreads to lymph becoming systemic– Typically self-limiting
– Many cases complicated by secondary infections
• Pneumonia and earaches
– Rare complications• encephalitis and subacute sclerosing
panencephalitis (SSPE)• persistent viral infection
• Prevention and treatment
– Prevention directed to vaccination• Vaccine is usually given in conjunction with mumps
and rubella vaccine– MMR
• Before routine immunization, over 99% of population infected
• Measles are no longer endemic in US
– No antiviral drug exists for rubeola infection• May treat with passive immunotherapy

German Measles
• Causative agent– Rubella virus– togavirus
• Typically mild
• Difficult to diagnose
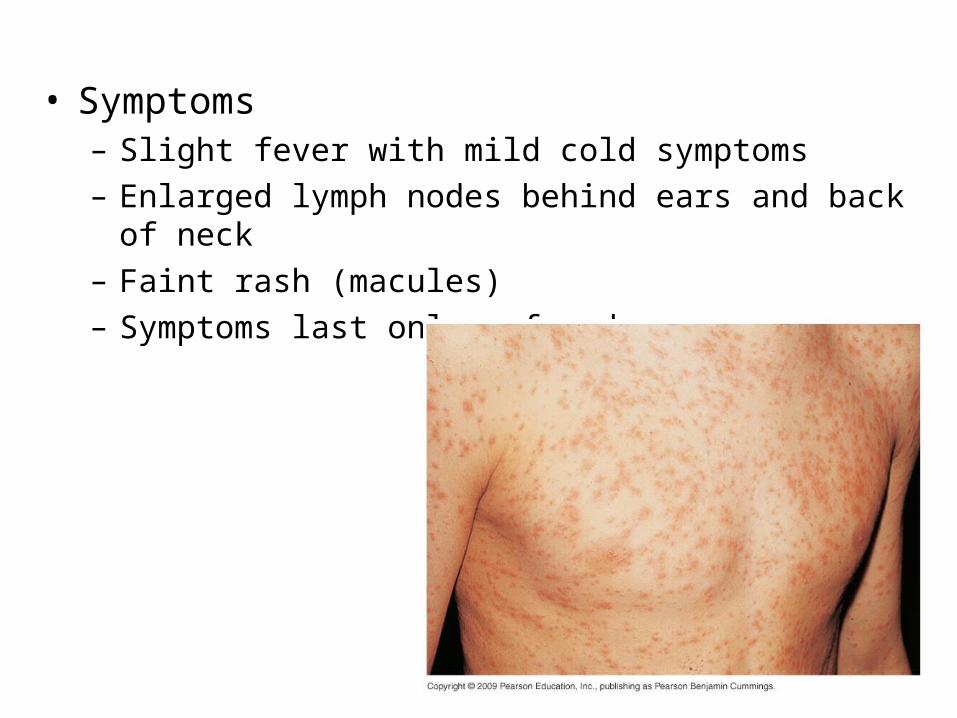
• Symptoms– Slight fever with mild cold symptoms– Enlarged lymph nodes behind ears and back of neck– Faint rash (macules)– Symptoms last only a few days
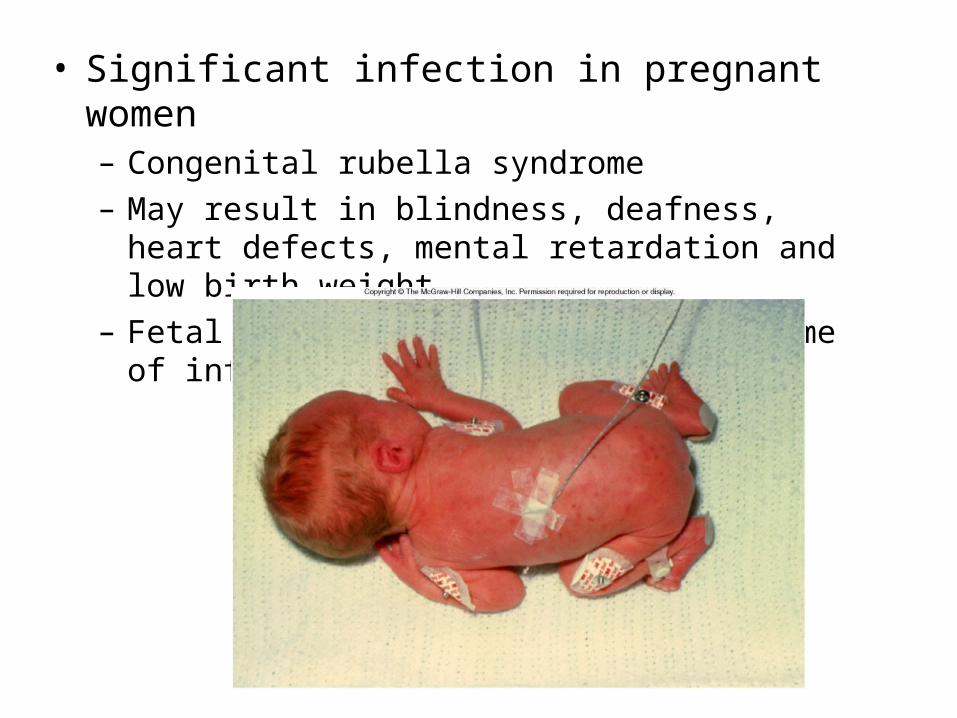
• Significant infection in pregnant women– Congenital rubella syndrome – May result in blindness, deafness, heart defects,
mental retardation and low birth weight – Fetal injury varies based on the time of infection
• Epidemiology– Humans are only natural host– Virus spread by respiratory droplets – Multiplies in nasopharynx then enters blood– Disease is highly contagious
• Infectious 7 days before appearance of rash and up to 7 days after it disappears
• Prevention and treatment– Vaccination with attenuated rubella virus
vaccine• Administered at 12 months and boostered at 4 to 6
years of age• Produces long-lasting immunity
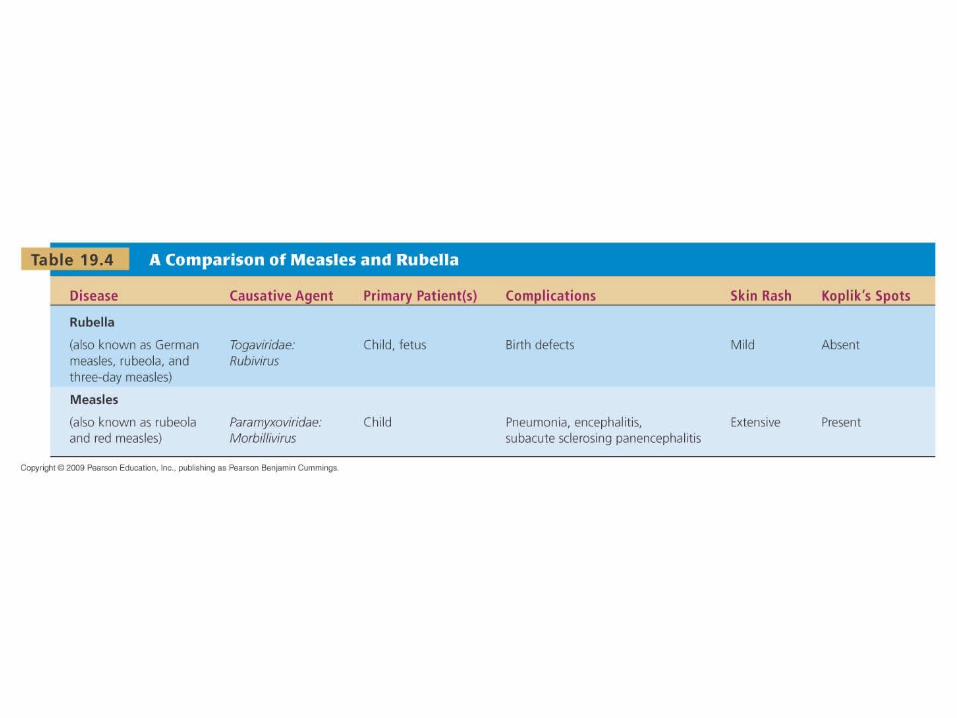
[INSERT TABLE 19.4]
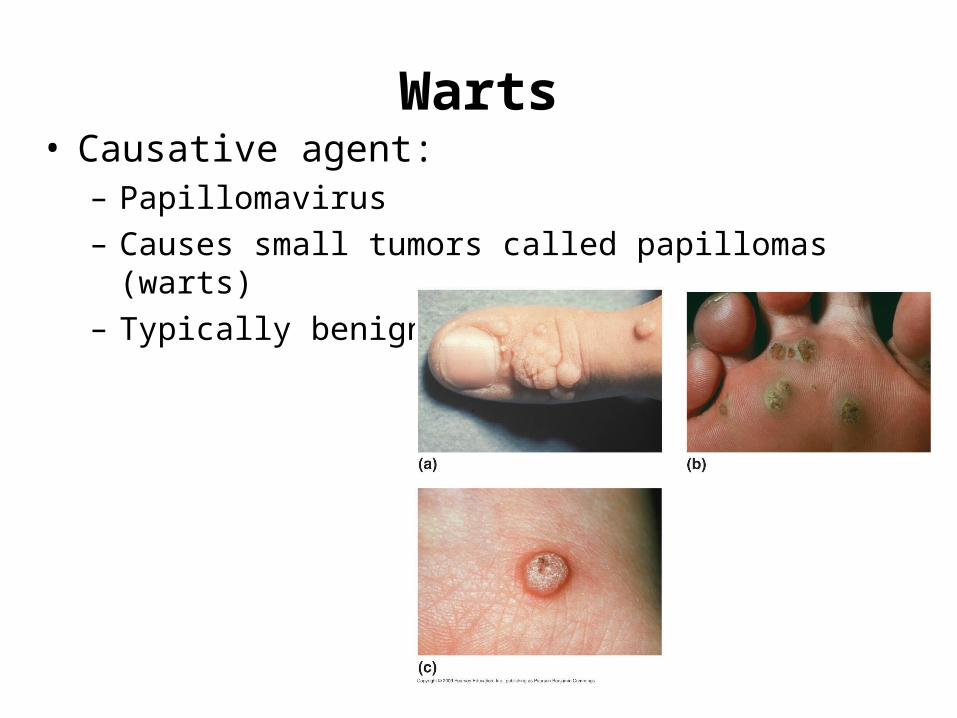
Warts• Causative agent:
– Papillomavirus – Causes small tumors called papillomas (warts)– Typically benign
• 50 different papillomaviruses known to infect humans– infect skin through minor abrasions– Direct, indirect or auto- inoculation – Viruses can survive on a number of fomites
• Towels• Shower floors
• Treatment involves killing abnormal cells – Freezing– Cauterization– Corrosive chemicals – Surgical removal– Laser
Mycoses of the Integument
• Most fungi are opportunistic pathogens
• Mycoses classified by location
– Superficial – hair, nails, and outer skin layers
• most common
– Cutaneous – in the skin
– Subcutaneous – in the hypodermis and muscles
– Systemic – affect numerous systems
• Superficial Mycoses
– Pityriasis versicolor• Caused by Malassezia furfur• Endogenous
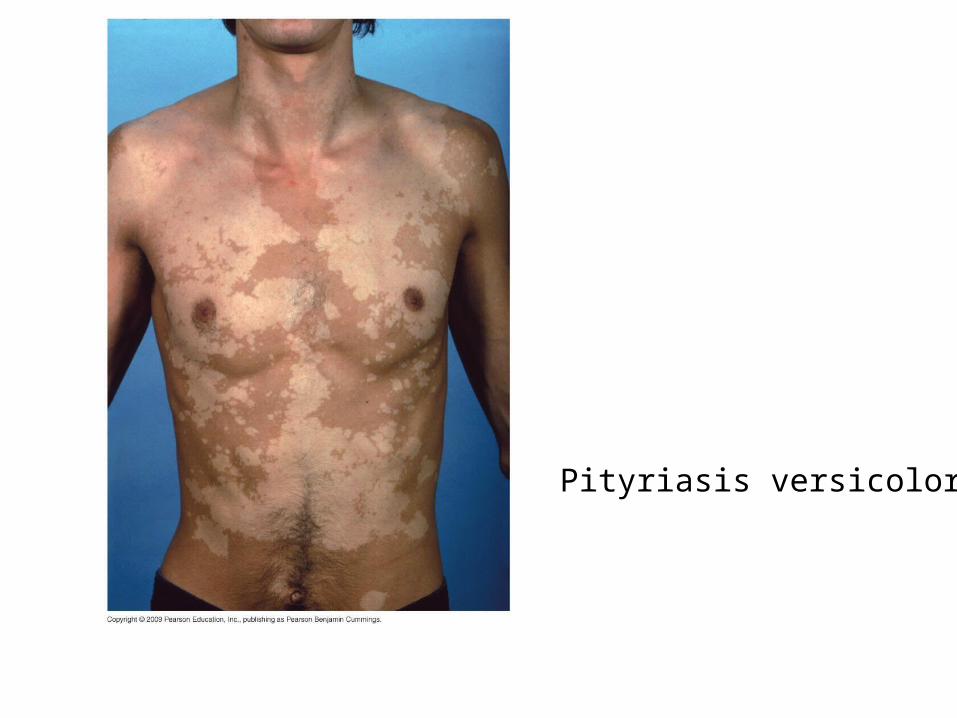
Pityriasis versicolor

– Pathogenesis• Superficial fungi produce keratinase, which dissolves
keratin
– Diagnosis, treatment, and prevention
• Identified by green color under ultraviolet light and
treated with topical or oral drugs
– Tolnaftate; Griseofulvin; Azoles
• Cutaneous Mycoses
– May manifest as cutaneous lesions
– Dermatophytoses
• Immune responses damage deeper tissues
• Causative Agent– Genera responsible for most dermatophytoses
• Epidermophyton• Microsporum• Trichophyton
– Collectively termed dermatophytes

Tinea capitis - scalp
Tinea corporis – body (Ringworm)
Tinea pedis - foot (Athlete’s foot)
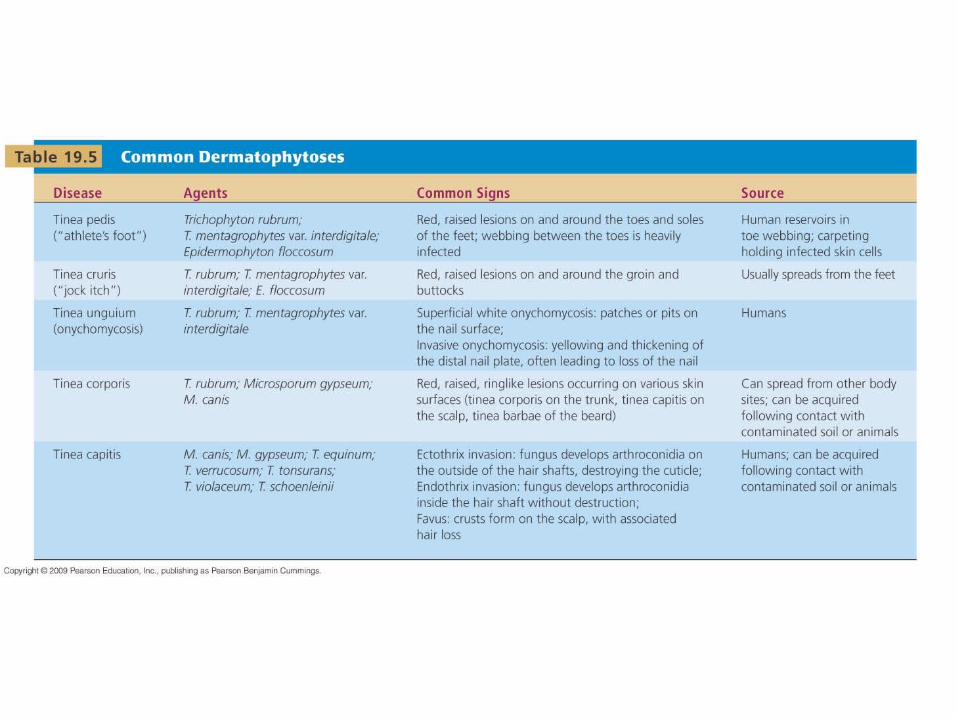
[INSERT TABLE 19.5]
– Excessive moisture allows invasion of keratinized tissue
• Most dermatophytes produce keratinase
– Scalp is invaded through hair follicle– Fungal products defuse to dermal layer and
evoke an immune response
• Treatment, and prevention– Attention to cleanliness– Maintenance of dryness– Treat limited infections with topical agents
• Tolnaftate
– Treat widespread infections with oral drugs• Griseofulvin; terbinafine