
CHF guidelines 2013seminar
139
2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and International Society for Heart and Lung Transplantation Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation © American College of Cardiology Foundation and American Heart Association, Inc. Dr Manish Ruhela
-
Upload
manishdmcardio -
Category
Health & Medicine
-
view
284 -
download
0
Transcript of CHF guidelines 2013seminar

2013 ACCF/AHA Guideline for the
Management of Heart Failure
Developed in Collaboration With the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and International Society for Heart and Lung Transplantation
Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation
© American College of Cardiology Foundation and American Heart Association, Inc.
Dr Manish Ruhela
Clyde W. Yancy and Mariell Jessup
ACCF/AHA Heart Failure Guideline Writing Committee MembersClyde W. Yancy, MD, MSc, FACC, FAHA, Chair†‡
Mariell Jessup, MD, FACC, FAHA, Vice Chair*†
*Writing committee members are required to recuse themselves from voting on sections to which their specific relationships with industry and other entities may apply; see Appendix 1 for recusal
information.
†ACCF/AHA Representative. ‡ACCF/AHA Task Force on Practice Guidelines Liaison. §American College of Physicians Representative. ║American College of Chest Physicians
Representative. ¶International Society for Heart and Lung Transplantation Representative. #ACCF/AHA Task Force on Performance Measures Liaison. **American Academy of Family
Physicians Representative. ††Heart Rhythm Society Representative.

Practice Guidelines• ACC/AHA: 1995, 2001, 2005, 2009
my.americanheart.org
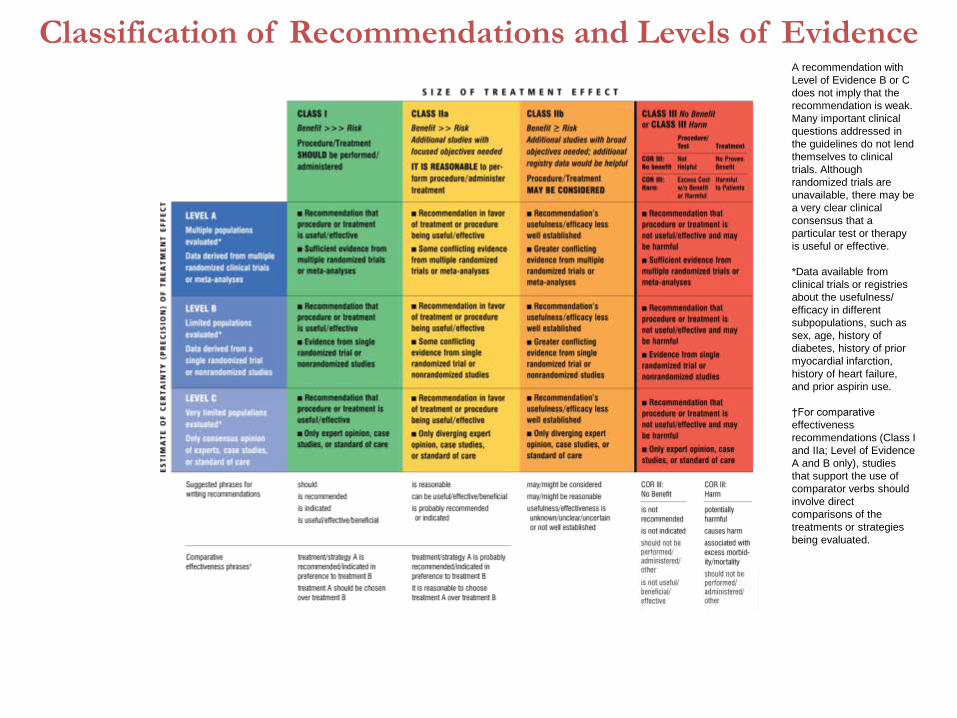
Classification of Recommendations and Levels of EvidenceA recommendation with
Level of Evidence B or C
does not imply that the
recommendation is weak.
Many important clinical
questions addressed in
the guidelines do not lend
themselves to clinical
trials. Although
randomized trials are
unavailable, there may be
a very clear clinical
consensus that a
particular test or therapy
is useful or effective.
*Data available from
clinical trials or registries
about the usefulness/
efficacy in different
subpopulations, such as
sex, age, history of
diabetes, history of prior
myocardial infarction,
history of heart failure,
and prior aspirin use.
†For comparative
effectiveness
recommendations (Class I
and IIa; Level of Evidence
A and B only), studies
that support the use of
comparator verbs should
involve direct
comparisons of the
treatments or strategies
being evaluated.

Definition HF is a complex clinical syndrome that results from any structural or functional
impairment of ventricular filling or ejection of blood.
The cardinal manifestations of HF are dyspnea and fatigue, which may limitexercise tolerance, and fluid retention, which may lead to pulmonary and/or
splanchnic congestion and/or peripheral edema.
Some patients have exercise intolerance but little evidence of fluid retention,
whereas others complain primarily of edema, dyspnea, or fatigue. Because somepatients present without signs or symptoms of volume overload, the term “heartfailure” is preferred over “congestive heart failure.”
There is no single diagnostic test for HF because it is largely a clinical diagnosisbased on a careful history and physical examination.
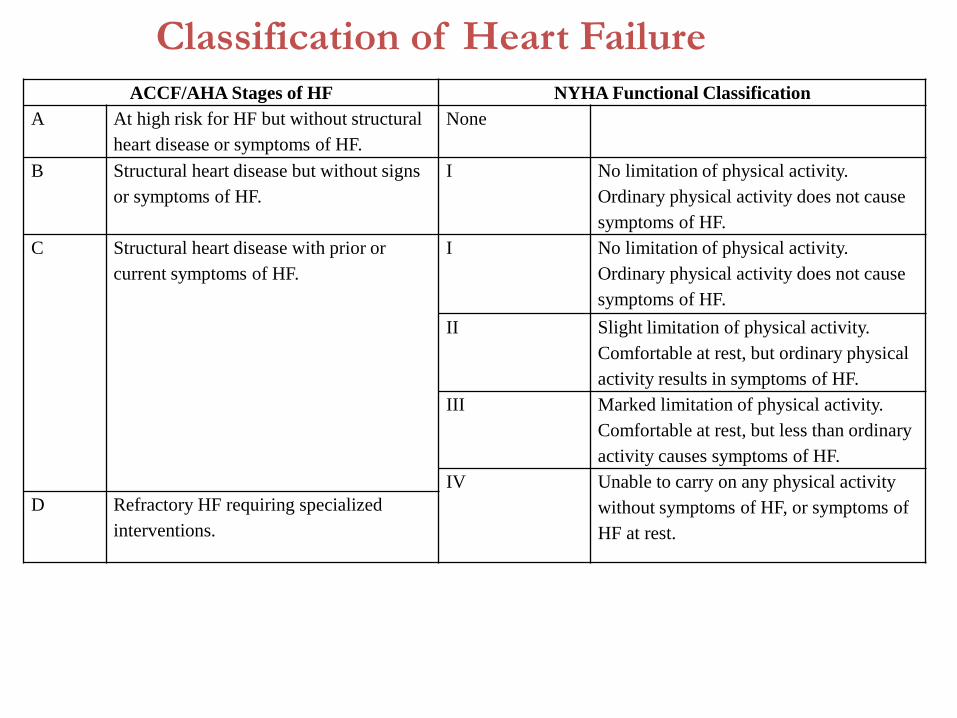
Classification of Heart Failure
ACCF/AHA Stages of HF NYHA Functional Classification
A At high risk for HF but without structural
heart disease or symptoms of HF.
None
B Structural heart disease but without signs
or symptoms of HF.
I No limitation of physical activity.
Ordinary physical activity does not cause
symptoms of HF.
C Structural heart disease with prior or
current symptoms of HF.
I No limitation of physical activity.
Ordinary physical activity does not cause
symptoms of HF.
II Slight limitation of physical activity.
Comfortable at rest, but ordinary physical
activity results in symptoms of HF.
III Marked limitation of physical activity.
Comfortable at rest, but less than ordinary
activity causes symptoms of HF.
IV Unable to carry on any physical activity
without symptoms of HF, or symptoms of
HF at rest.
D Refractory HF requiring specialized
interventions.

Definition of Heart FailureClassification Ejection
Fraction
Description
I. Heart Failure with
Reduced Ejection Fraction
(HFrEF)
≤40% Also referred to as systolic HF. Randomized clinical trials have
mainly enrolled patients with HFrEF and it is only in these patients
that efficacious therapies have been demonstrated to date.
II. Heart Failure with
Preserved Ejection
Fraction (HFpEF)
≥50% Also referred to as diastolic HF. The diagnosis of HFpEF is
challenging because it is largely one of excluding other potential
noncardiac causes of symptoms suggestive of HF. To date,
efficacious therapies have not been identified.
a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their
characteristics, treatment patterns, and outcomes appear similar to
those of patient with HFpEF.
b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF
previously had HFrEF. These patients with improvement or recovery
in EF may be clinically distinct from those with persistently
preserved or reduced EF. Further research is needed to better
characterize these patients.

I. Initial and Serial Evaluation of the HF Patient
(including HFpEF)
II. Treatment of Stage A thru D Heart Failure
(including HFpEF)
III. The Hospitalized Patient
IV. Surgical/Percutaneous/Transcatheter Interventional Treatments
V. Coordinating Care for Patients With Chronic HF
VI. Quality Metrics/Performance Measures
Outline

Clinical Evaluation
Initial and Serial Evaluation of the HF Patient

Initial and Serial Evaluation of
the HF Patient
Guideline for HF
History and Physical
Examination
Initial and Serial Evaluation of the HF Patient

A thorough history and physical examination should beobtained/performed in patients presenting with HF toidentify cardiac and noncardiac disorders or behaviors that might cause or accelerate the development or progression of HF.
In patients with idiopathic DCM, a 3-generational family history should be obtained to aid in establishing the diagnosis of familial DCM.
Volume status and vital signs should be assessed at each patient encounter. This includes serial assessment of weight, as well as estimates of jugular venous pressure and the presence of peripheral edema or orthopnea.
History and Physical ExaminationI IIa IIb III
I IIa IIb III
I IIa IIb III

Risk Scoring
Initial and Serial Evaluation of the HF Patient

Risk Scoring
Validated multivariable risk scores can be useful to estimate subsequent risk of mortality in ambulatory or hospitalized patients with HF.
I IIa IIb III

Risk Scores to Predict Outcomes in HF
Risk Score Reference (from full-text guideline)/Link
Chronic HF
All patients with chronic HF
Seattle Heart Failure Model (204) / http://SeattleHeartFailureModel.org
Heart Failure Survival Score (200) / http://handheld.softpedia.com/get/Health/Calculator/HFSS-Calc-
37354.shtml
CHARM Risk Score (207)
CORONA Risk Score (208)
Specific to chronic HFpEF
I-PRESERVE Score (202)
Acutely Decompensated HF
ADHERE Classification and Regression
Tree (CART) Model
(201)
American Heart Association Get With the
Guidelines Score
(206) /
http://www.heart.org/HEARTORG/HealthcareProfessional/GetWithTheGuidel
inesHFStroke/GetWithTheGuidelinesHeartFailureHomePage/Get-With-The-
Guidelines-Heart-Failure-Home- %20Page_UCM_306087_SubHomePage.jsp
EFFECT Risk Score (203) / http://www.ccort.ca/Research/CHFRiskModel.aspx
ESCAPE Risk Model and Discharge Score (215)
OPTIMIZE HF Risk-Prediction Nomogram (216)

Seattle Heart Failure Model
www.SeattleHeartFailureModel.org Levy WC et al. Circulation 2006;113:1424-1433

Diagnostic Tests
Initial and Serial Evaluation of the HF Patient

Diagnostic Tests
Initial lab. evaluation of patients presenting with HF should include CBC, urinalysis, electrolytes (including calcium and magnesium), BUN, serum creatinine, glucose, fasting lipid profile, LFTs, and thyroid-stimulating hormone.
Serial monitoring, when indicated, should include serum electrolytes and renal function.
I IIa IIb III
I IIa IIb III

Diagnostic Tests (cont.)
A 12-lead ECG should be performed initially on all patients presenting with HF.
Screening for hemochromatosis or HIV is reasonable in selected patients who present with HF.
Diagnostic tests for rheumatologic diseases, amyloidosis, or pheochromocytoma are reasonable in patients presenting with HF in whom there is a clinical suspicion of these diseases.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Biomarkers
Ambulatory/Outpatient
Initial and Serial Evaluation of the HF Patient

Ambulatory/Outpatient
In ambulatory patients with dyspnea, measurement of BNP or NT-proBNP is useful to support clinical decision making regarding the diagnosis of HF, especially in the setting of clinical uncertainty.
Measurement of BNP or NT-proBNP is useful for establishing prognosis or disease severity in chronic HF.
I IIa IIb III
I IIa IIb III

Ambulatory/Outpatient (cont.)
BNP- or NT-proBNP guided HF therapy can be useful to achieve optimal dosing of GDMT in selected clinically euvolemic patients followed in a well-structured HF disease management program.
The usefulness of serial measurement of BNP or NT-proBNP to reduce hospitalization or mortality in patients with HF is not well established.
Measurement of other clinically available tests such as biomarkers of myocardial injury may be considered for additive risk stratification in patients with chronic HF.
I IIa IIb III
I IIa IIb III
I IIa IIb III
Biomarkers
Hospitalized/Acute
Initial and Serial Evaluation of the HF Patient

Hospitalized/Acute
Measurement of BNP or NT-proBNP is useful to support clinical judgment for the diagnosis of acutely decompensated HF, especially in the setting of uncertainty for the diagnosis.
Measurement of BNP or NT-proBNP and/or cardiac troponin is useful for establishing prognosis or disease severity in acutely decompensated HF.
I IIa IIb III
I IIa IIb III

Hospitalized/Acute (cont.)
The usefulness of BNP- or NT-proBNP guided therapy for acutely decompensated HF is not well-established.
Measurement of other clinically available tests such as biomarkers of myocardial injury or fibrosis may be considered for additive risk stratification in patients with acutely decompensated HF.
I IIa IIb III
I IIa IIb III

Recommendations for Biomarkers in HFBiomarker, Application Setting COR LOE
Natriuretic peptides
Diagnosis or exclusion of HFAmbulatory,
AcuteI A
Prognosis of HFAmbulatory,
AcuteI A
Achieve GDMT Ambulatory IIa B
Guidance of acutely decompensated
HF therapyAcute IIb C
Biomarkers of myocardial injury
Additive risk stratificationAcute,
Ambulatory I A
Biomarkers of myocardial fibrosis
Additive risk stratification
Ambulatory IIb B
AcuteIIb A

Causes for Elevated Natriuretic Peptide
Levels
Cardiac Noncardiac
Heart failure
Acute coronary syndrome
Heart muscle disease, including
LVH
Valvular heart disease
Pericardial disease
Atrial fibrillation
Myocarditis
Cardiac surgery
Cardioversion
Advancing age
Anemia
Renal failure
Pulmonary causes: obstructive
sleep apnea, severe pneumonia,
pulmonary hypertension
Critical illness
Bacterial sepsis
Severe burns
Toxic-metabolic insults, including
cancer chemotherapy

Noninvasive Cardiac Imaging
Initial and Serial Evaluation of the HF Patient

Noninvasive Cardiac ImagingPatients with suspected or new-onset HF, or presenting with acute decompensated HF, should undergo a C x-ray to assess heart size and pulmonary congestion, and to detect alternative cardiac, pulmonary, and other diseases that may cause or contribute to the patients’ symptoms.
A 2-D echo with Doppler should be performed during initial evaluation of patients presenting with HF to assess ventricular function, size, wall thickness, wall motion, and valve function.
Repeat measurement of EF and severity of structural remodeling are useful to provide information in patients with HF who have had a significant change in clinical status.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Noninvasive Cardiac Imaging (cont.)
Noninvasive imaging to detect myocardial ischemia and viability is reasonable in patients presenting with de novo HF who have known CAD and no angina unless the patient is not eligible for revascularization of any kind.
Viability assessment is reasonable in select situations when planning revascularization in HF patients with CAD.
Radionuclide ventriculography or MRI can be useful to assess LVEF and volume when echocardiography is inadequate.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Noninvasive Cardiac Imaging (cont.)
MRI is reasonable when assessing myocardial infiltrative processes or scar burden.
Routine repeat measurement of LV function assessment in the absence of clinical status change or treatment interventions should not be performed.
I IIa IIb III
No Benefit
I IIa IIb III

Recommendations for Noninvasive Imaging
Recommendation COR LOE
Patients with suspected, acute, or new-onset HF should undergo a chest x-
rayI C
A 2-D echo with Doppler should be performed for initial evaluation of HF I C
Repeat measurement of EF is useful in patients with HF who have had a
significant change in clinical status or received treatment that might affect
cardiac function, or for consideration of device therapy
I C
Noninvasive imaging to detect myocardial ischemia and viability is
reasonable in HF and CADIIa C
Viability assessment is reasonable before revascularization in HF patients
with CADIIa B
Radionuclide ventriculography or MRI can be useful to assess LVEF and
volume IIa C
MRI is reasonable when assessing myocardial infiltration or scar IIa B
Routine repeat measurement of LV function assessment should not be
performed
III: No
BenefitB

Invasive Evaluation
Initial and Serial Evaluation of the HF Patient

Invasive EvaluationInvasive hemodynamic monitoring with a pulmonary artery catheter should beperformed to guide therapy in patients who have respiratory distress or clinicalevidence of impaired perfusion in whom the adequacy or excess of intracardiac fillingpressures cannot be determined from clinical assessment.
Invasive hemodynamic monitoring can be useful for carefully selected patients withacute HF who have persistent symptoms despite empiric adjustment of standardtherapies and
a. whose fluid status, perfusion, or systemic or pulmonary vascular resistance isuncertain;
b. whose systolic pressure remains low, or is associated with symptoms, despiteinitial therapy;
c. whose renal function is worsening with therapy;
d. who require parenteral vasoactive agents; or
e. who may need consideration for MCS or transplantation.
I IIa IIb III
I IIa IIb III

Invasive Evaluation (cont.)
When ischemia may be contributing to HF, coronary arteriographyis reasonable for patients eligible for revascularization.
Endomyocardial biopsy can be useful in patients presenting withHF when a specific diagnosis is suspected that would influencetherapy.
I IIa IIb III
I IIa IIb III

Invasive Evaluation (cont.)
Routine use of invasive hemodynamic monitoring is notrecommended in normotensive patients with acutedecompensated HF and congestion with symptomatic responseto diuretics and vasodilators.
Endomyocardial biopsy should not be performed in the routineevaluation of patients with HF.
I IIa IIb III
No Benefit
I IIa IIb III
Harm

Recommendations for Invasive Evaluation
Recommendation COR LOE
Monitoring with a pulmonary artery catheter should be performed in patients
with respiratory distress or impaired systemic perfusion when clinical
assessment is inadequate
I C
Invasive hemodynamic monitoring can be useful for carefully selected
patients with acute HF with persistent symptoms and/or when hemodynamics
are uncertain
IIa C
When coronary ischemia may be contributing to HF, coronary arteriography
is reasonable IIa C
Endomyocardial biopsy can be useful in patients with HF when a specific
diagnosis is suspected that would influence therapyIIa C
Routine use of invasive hemodynamic monitoring is not recommended in
normotensive patients with acute HF
III: No
Benefit
B
Endomyocardial biopsy should not be performed in the routine evaluation of
HFIII: Harm C

Treatment of Stages A to D
Guideline for HF

Stages, Phenotypes and Treatment of HF
STAGE AAt high risk for HF but
without structural heart
disease or symptoms of HF
STAGE BStructural heart disease
but without signs or
symptoms of HF
THERAPY
Goals
Control symptoms
Improve HRQOL
Prevent hospitalization
Prevent mortality
Strategies
Identification of comorbidities
Treatment
Diuresis to relieve symptoms
of congestion
Follow guideline driven
indications for comorbidities,
e.g., HTN, AF, CAD, DM
Revascularization or valvular
surgery as appropriate
STAGE CStructural heart disease
with prior or current
symptoms of HF
THERAPYGoals Control symptoms Patient education Prevent hospitalization Prevent mortality
Drugs for routine use Diuretics for fluid retention ACEI or ARB Beta blockers Aldosterone antagonists
Drugs for use in selected patients Hydralazine/isosorbide dinitrate ACEI and ARB Digoxin
In selected patients CRT ICD Revascularization or valvular
surgery as appropriate
STAGE DRefractory HF
THERAPY
Goals
Prevent HF symptoms
Prevent further cardiac
remodeling
Drugs
ACEI or ARB as
appropriate
Beta blockers as
appropriate
In selected patients
ICD
Revascularization or
valvular surgery as
appropriate
e.g., Patients with:
Known structural heart disease and
HF signs and symptoms
HFpEF HFrEF
THERAPY
Goals
Heart healthy lifestyle
Prevent vascular,
coronary disease
Prevent LV structural
abnormalities
Drugs
ACEI or ARB in
appropriate patients for
vascular disease or DM
Statins as appropriate
THERAPYGoals Control symptoms Improve HRQOL Reduce hospital
readmissions Establish patient’s end-
of-life goals
Options Advanced care
measures Heart transplant Chronic inotropes Temporary or permanent
MCS Experimental surgery or
drugs Palliative care and
hospice ICD deactivation
Refractory symptoms of HF at rest, despite GDMT
At Risk for Heart Failure Heart Failure
e.g., Patients with:
Marked HF symptoms at
rest
Recurrent hospitalizations
despite GDMT
e.g., Patients with:
Previous MI
LV remodeling including
LVH and low EF
Asymptomatic valvular
disease
e.g., Patients with:
HTN
Atherosclerotic disease
DM
Obesity
Metabolic syndrome
or
Patients
Using cardiotoxins
With family history of
cardiomyopathy
Development of
symptoms of HFStructural heart
disease

Stage A
Treatment of Stages A to D

Stage A
Hypertension and lipid disorders should be controlled in accordance with contemporary guidelines to lower the risk of HF.
Other conditions that may lead to or contribute to HF, such as obesity, diabetes mellitus, tobacco use, and known cardiotoxic agents, should be controlled or avoided.
I IIa IIb III
I IIa IIb III

Stage B
Treatment of Stages A to D
Stage B
In all patients with a recent or remote history of MI or ACS and reduced EF, ACE inhibitors should be used to prevent symptomatic HF and reduce mortality. In patients intolerant of ACE inhibitors, ARBs are appropriate unless contraindicated.
In all patients with a recent or remote history of MI or ACS and reduced EF, evidence-based beta blockers should be used to reduce mortality.
In all patients with a recent or remote history of MI or ACS, statins should be used to prevent symptomatic HF and cardiovascular events.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Stage B (cont.)
In patients with structural cardiac abnormalities, including LV hypertrophy, in the absence of a history of MI or ACS, blood pressure should be controlled in accordance with clinical practice guidelines for hypertension to prevent symptomatic HF.
ACE inhibitors should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do not have a history of MI.
Beta blockers should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do not have a history of MI.
I IIa IIb III
I IIa IIb III
I IIa IIb III
Stage B (cont.)
To prevent SCD, placement of an ICD is reasonable in patients withasymptomatic ischemic cardiomyopathy who are at least 40 dayspost-MI, have an LVEF of 30% or less, are on appropriate medicaltherapy and have reasonable expectation of survival with a goodfunctional status for more than 1 year.
Nondihydropyridine calcium channel blockers with negativeinotropic effects may be harmful in asymptomatic patients withlow LVEF and no symptoms of HF after MI.
I IIa IIb III
I IIa IIb III
Harm

Recommendations for Treatment of Stage B HF
Recommendations COR LOE
In patients with a history of MI and reduced EF, ACE inhibitors or
ARBs should be used to prevent HFI A
In patients with MI and reduced EF, evidence-based beta blockers
should be used to prevent HFI B
In patients with MI, statins should be used to prevent HF I A
Blood pressure should be controlled to prevent symptomatic HF I A
ACE inhibitors should be used in all patients with a reduced EF to
prevent HFI A
Beta blockers should be used in all patients with a reduced EF to
prevent HFI C
An ICD is reasonable in patients with asymptomatic ischemic
cardiomyopathy who are at least 40 d post-MI, have an LVEF
≤30%, and on GDMT
IIa B
Nondihydropyridine calcium channel blockers may be harmful in
patients with low LVEF III: Harm C

Stage C
Treatment of Stages A to D
Nonpharmacological
Interventions
Treatment of Stages A to D
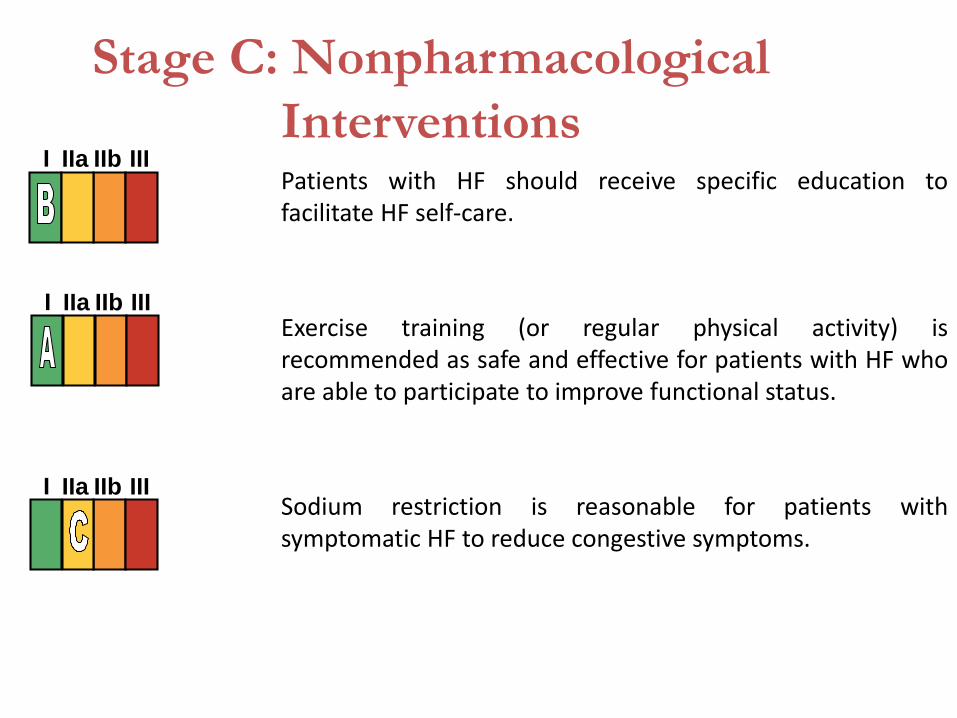
Stage C: Nonpharmacological
InterventionsPatients with HF should receive specific education tofacilitate HF self-care.
Exercise training (or regular physical activity) isrecommended as safe and effective for patients with HF whoare able to participate to improve functional status.
Sodium restriction is reasonable for patients withsymptomatic HF to reduce congestive symptoms.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Stage C: Nonpharmacological
Interventions (cont.)
Continuous positive airway pressure (CPAP) can be beneficial to increase LVEF and improve functional status in patients with HF and sleep apnea.
Cardiac rehabilitation can be useful in clinically stable patients with HF to improve functional capacity, exercise duration, and mortality.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF
Treatment of Stages A to D

Pharmacological Treatment for Stage
C HFrEF
Measures listed as Class I recommendations for patients in stages A and B are recommended where appropriate for patients in stage C. (Levels of Evidence: A, B, and C as appropriate)
GDMT as depicted in Figure 1 should be the mainstay of pharmacological therapy for HFrEF.
I IIa IIb III
I IIa IIb III
See
recommendations
for stages A, B,
and C LOE for
LOE

Pharmacologic Treatment for Stage C HFrEFHFrEF Stage C
NYHA Class I – IV
Treatment:
For NYHA class II-IV patients.
Provided estimated creatinine
>30 mL/min and K+ <5.0 mEq/dL
For persistently symptomatic
African Americans,
NYHA class III-IV
Class I, LOE A
ACEI or ARB AND
Beta Blocker
Class I, LOE C
Loop Diuretics
Class I, LOE A
Hydral-Nitrates
Class I, LOE A
Aldosterone
Antagonist
AddAdd Add
For all volume overload,
NYHA class II-IV patients

Pharmacological Treatment for
Stage C HFrEF (cont.)
Diuretics are recommended in patients with HFrEF who haveevidence of fluid retention, unless contraindicated, to improvesymptoms.
ACE inhibitors are recommended in patients with HFrEF and currentor prior symptoms, unless contraindicated, to reduce morbidity andmortality.
ARBs are recommended in patients with HFrEF with current or priorsymptoms who are ACE inhibitor-intolerant, unless contraindicated,to reduce morbidity and mortality.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Drugs Commonly Used for HFrEF
(Stage C HF)
Drug Initial Daily Dose(s) Maximum Doses(s)Mean Doses Achieved in
Clinical Trials
ACE Inhibitors
Captopril 6.25 mg 3 times 50 mg 3 times 122.7 mg/d (421)
Enalapril 2.5 mg twice 10 to 20 mg twice 16.6 mg/d (412)
Fosinopril 5 to 10 mg once 40 mg once ---------
Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35.0 mg/d (444)
Perindopril 2 mg once 8 to 16 mg once ---------
Quinapril 5 mg twice 20 mg twice ---------
Ramipril 1.25 to 2.5 mg once 10 mg once ---------
Trandolapril 1 mg once 4 mg once ---------
ARBs
Candesartan 4 to 8 mg once 32 mg once 24 mg/d (419)
Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d (420)
Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d (109)
Aldosterone Antagonists
Spironolactone 12.5 to 25 mg once 25 mg once or twice 26 mg/d (424)
Eplerenone 25 mg once 50 mg once 42.6 mg/d (445)

Drugs Commonly Used for HFrEF
(Stage C HF) (cont.)
Drug Initial Daily Dose(s) Maximum Doses(s)Mean Doses Achieved in
Clinical Trials
Beta Blockers
Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d (118)
Carvedilol 3.125 mg twice 50 mg twice 37 mg/d (446)
Carvedilol CR 10 mg once 80 mg once ---------
Metoprolol succinate
extended release
(metoprolol CR/XL)
12.5 to 25 mg once 200 mg once 159 mg/d (447)
Hydralazine & Isosorbide Dinitrate
Fixed dose combination
(423)
37.5 mg hydralazine/
20 mg isosorbide
dinitrate 3 times daily
75 mg hydralazine/
40 mg isosorbide
dinitrate 3 times daily
~175 mg hydralazine/90 mg
isosorbide dinitrate daily
Hydralazine and
isosorbide dinitrate (448)
Hydralazine: 25 to 50
mg, 3 or 4 times daily
and isorsorbide
dinitrate:
20 to 30 mg
3 or 4 times daily
Hydralazine: 300 mg
daily in divided doses
and isosorbide dinitrate
120 mg daily in
divided doses
---------


Pharmacological Treatment for
Stage C HFrEF (cont.)
ARBs are reasonable to reduce morbidity and mortality asalternatives to ACE inhibitors as first-line therapy for patients withHFrEF, especially for patients already taking ARBs for otherindications, unless contraindicated.
Addition of an ARB may be considered in persistently symptomaticpatients with HFrEF who are already being treated with an ACEinhibitor and a beta blocker in whom an aldosterone antagonist isnot indicated or tolerated.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
Routine combined use of an ACE inhibitor, ARB, and aldosteroneantagonist is potentially harmful for patients with HFrEF.
Use of 1 of the 3 beta blockers proven to reduce mortality (i.e.,bisoprolol, carvedilol, and sustained-release metoprolol succinate)is recommended for all patients with current or prior symptoms ofHFrEF, unless contraindicated, to reduce morbidity and mortality.
I IIa IIb III
I IIa IIb III
Harm

Pharmacological Treatment for
Stage C HFrEF (cont.)
Aldosterone receptor antagonists are recommended inpatients with NYHA class II-IV and who have LVEF of 35% orless, unless contraindicated, to reduce morbidity and mortality.
Patients with NYHA class II should have a history of priorcardiovascular hospitalization or elevated plasma natriureticpeptide levels to be considered for aldosterone receptorantagonists.
Creatinine should be 2.5 mg/dL or less in men or 2.0 mg/dLor less in women (or estimated glomerular filtration rate >30mL/min/1.73m2) and potassium should be less than 5.0 mEq/L.
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
Aldosterone receptor antagonists are recommended to reducemorbidity and mortality following an acute MI in patients whohave LVEF of 40% or less who develop symptoms of HF or whohave a history of diabetes mellitus, unless contraindicated.
Inappropriate use of aldosterone receptor antagonists ispotentially harmful because of life-threatening hyperkalemia orrenal insufficiency when serum creatinine greater than 2.5mg/dL in men or greater than 2.0 mg/dL in women (orestimated glomerular filtration rate <30 mL/min/1.73m2),and/or potassium above 5.0 mEq/L.
I IIa IIb III
I IIa IIb III
Harm

Pharmacological Treatment for
Stage C HFrEF (cont.)
The combination of hydralazine and isosorbide dinitrate isrecommended to reduce morbidity and mortality for AfricanAmericans patients with NYHA class III–IV HFrEF receivingoptimal therapy with ACE inhibitors and beta blockers, unlesscontraindicated.
A combination of hydralazine and isosorbide dinitrate can beuseful to reduce morbidity or mortality in patients with currentor prior symptomatic HFrEF who cannot be given an ACEinhibitor or ARB because of drug intolerance, hypotension, orrenal insufficiency, unless contraindicated.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
Digoxin can be beneficial in patients with HFrEF, unlesscontraindicated, to decrease hospitalizations for HF.
Patients with chronic HF with AF and an additional risk factorfor cardioembolic stroke (history of hypertension, diabetesmellitus, previous stroke or transient ischemic attack, or ≥75years of age) should receive chronic anticoagulant therapy (inthe absence of contraindications to anticoagulation).
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
The selection of an anticoagulant agent for AF should beindividualized on the basis of risk factors, cost, tolerability,patient preference, potential for drug interactions, and otherclinical characteristics, including time in the internationalnormalized rate therapeutic ration if the patient has beentaking warfarin.
Chronic anticoagulation is reasonable for patients with chronicHF who have AF but are without an additional risk factor forcardioembolic stroke (in the absence of contraindications toanticoagulation).
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
Anticoagulation is not recommended in patients with chronicHFrEF without AF, a prior thromboembolic event, or acardioembolic source.
Statins are not beneficial as adjunctive therapy whenprescribed solely for the diagnosis of HF in the absence of otherindications for their use.
Omega-3 PUFA supplementation is reasonable to use asadjunctive therapy in patients with NYHA class II-IV symptomsand HFrEF or HFpEF, unless contraindicated, to reducemortality and cardiovascular hospitalizations.
I IIa IIb III
No Benefit
I IIa IIb III
No Benefit
I IIa IIb III

Pharmacological Treatment for
Stage C HFrEF (cont.)
Nutritional supplements as treatment for HF are notrecommended in patients with current or prior symptoms ofHFrEF.
Hormonal therapies other than to correct deficiencies are notrecommended for patients with current or prior symptoms ofHFrEF.
Drugs known to adversely affect the clinical status of patientswith current or prior symptoms of HFrEF are potentially harmfuland should be avoided or withdrawn whenever possible (e.g.,most antiarrhythmic drugs, most calcium channel blockingdrugs (except amlodipine), NSAIDs, or TZDs).
No Benefit
I IIa IIb III
I IIa IIb III
I IIa IIb III
No Benefit
Harm

Pharmacological Treatment for
Stage C HFrEF (cont.)
Long-term use of infused positive inotropic drugs is potentiallyharmful for patients with HFrEF, except as palliation for patientswith end-stage disease who cannot be stabilized with standardmedical treatment (see recommendations for stage D).
Calcium channel blocking drugs are not recommended asroutine treatment for patients with HFrEF.
Harm
I IIa IIb III
I IIa IIb III
No Benefit

Pharmacological Treatment for
Stage C HFpEF Systolic and diastolic blood pressure should be controlled inpatients with HFpEF in accordance with published clinicalpractice guidelines to prevent morbidity.
Diuretics should be used for relief of symptoms due to volumeoverload in patients with HFpEF.
Coronary revascularization is reasonable in patients with CAD inwhom symptoms (angina) or demonstrable myocardialischemia is judged to be having an adverse effect onsymptomatic HFpEF despite GDMT.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFpEF (cont.)
Management of AF according to published clinical practiceguidelines in patients with HFpEF is reasonable to improvesymptomatic HF.
The use of beta-blocking agents, ACE inhibitors, and ARBs inpatients with hypertension is reasonable to control bloodpressure in patients with HFpEF.
I IIa IIb III
I IIa IIb III

Pharmacological Treatment for
Stage C HFpEF (cont.)
The use of ARBs might be considered to decreasehospitalizations for patients with HFpEF.
Routine use of nutritional supplements is not recommended forpatients with HFpEF.
I IIa IIb III
No Benefit
I IIa IIb III

Pharmacological Therapy for
Management of Stage C HFrEFRecommendations COR LOE
Diuretics
Diuretics are recommended in patients with HFrEF with fluid
retention I C
ACE Inhibitors
ACE inhibitors are recommended for all patients with HFrEF I A
ARBs
ARBs are recommended in patients with HFrEF who are ACE
inhibitor intolerant I A
ARBs are reasonable as alternatives to ACE inhibitor as first
line therapy in HFrEFIIa A
The addition of an ARB may be considered in persistently
symptomatic patients with HFrEF on GDMTIIb A
Routine combined use of an ACE inhibitor, ARB, and
aldosterone antagonist is potentially harmful III: Harm C
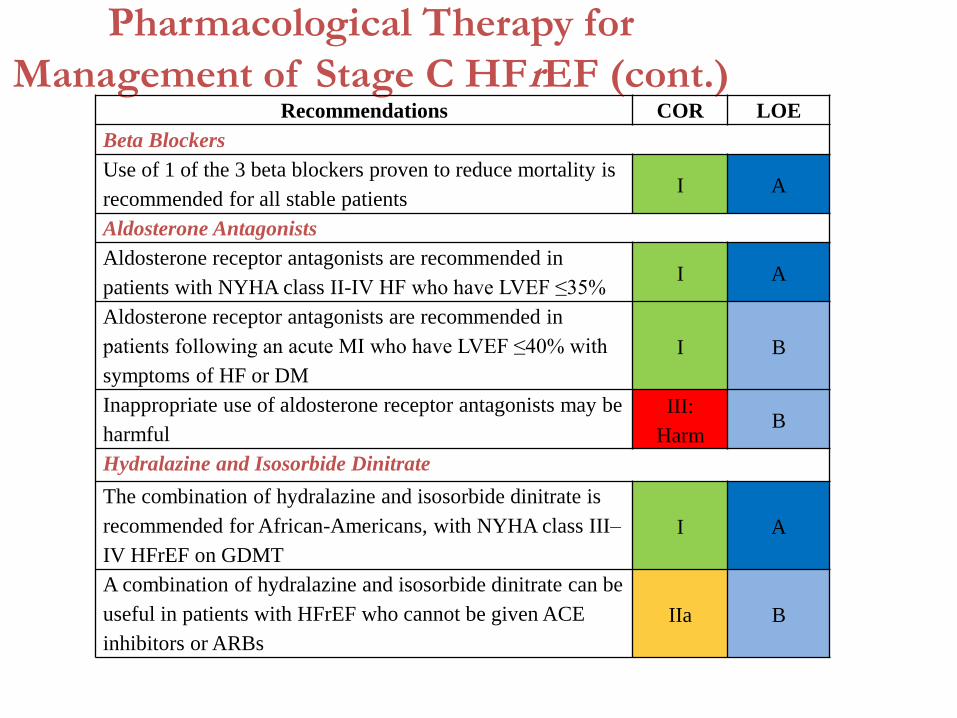
Pharmacological Therapy for
Management of Stage C HFrEF (cont.)Recommendations COR LOE
Beta Blockers
Use of 1 of the 3 beta blockers proven to reduce mortality is
recommended for all stable patientsI A
Aldosterone Antagonists
Aldosterone receptor antagonists are recommended in
patients with NYHA class II-IV HF who have LVEF ≤35% I A
Aldosterone receptor antagonists are recommended in
patients following an acute MI who have LVEF ≤40% with
symptoms of HF or DM
I B
Inappropriate use of aldosterone receptor antagonists may be
harmful
III:
HarmB
Hydralazine and Isosorbide Dinitrate
The combination of hydralazine and isosorbide dinitrate is
recommended for African-Americans, with NYHA class III–
IV HFrEF on GDMT
I A
A combination of hydralazine and isosorbide dinitrate can be
useful in patients with HFrEF who cannot be given ACE
inhibitors or ARBs
IIa B

Pharmacologic Therapy for
Management of Stage C HFrEF (cont.)Recommendations COR LOE
Digoxin
Digoxin can be beneficial in patients with HFrEF IIa B
Anticoagulation
Patients with chronic HF with permanent/persistent/paroxysmal AF and an
additional risk factor for cardioembolic stroke should receive chronic
anticoagulant therapy*
I A
The selection of an anticoagulant agent should be individualized I C
Chronic anticoagulation is reasonable for patients with chronic HF who have
permanent/persistent/paroxysmal AF but without an additional risk factor for
cardioembolic stroke*
IIa B
Anticoagulation is not recommended in patients with chronic HFrEF without
AF, prior thromboembolic event, or a cardioembolic source
III: No
BenefitB
Statins
Statins are not beneficial as adjunctive therapy when prescribed solely for HF III: No
BenefitA
Omega-3 Fatty Acids
Omega-3 PUFA supplementation is reasonable to use as adjunctive therapy in
HFrEF or HFpEF patients IIa B

Pharmacological Therapy for
Management of Stage C HFrEF (cont.)
Recommendations COR LOE
Other Drugs
Nutritional supplements as treatment for HF are not recommended
in HFrEF
III: No
BenefitB
Hormonal therapies other than to replete deficiencies are not
recommended in HFrEF
III: No
BenefitC
Drugs known to adversely affect the clinical status of patients with
HFrEF are potentially harmful and should be avoided or
withdrawn
III: Harm B
Long-term use of an infusion of a positive inotropic drug is not
recommended and may be harmful except as palliationIII: Harm C
Calcium Channel Blockers
Calcium channel blocking drugs are not recommended as routine
in HFrEF
III: No
BenefitA

Treatment for Stage C HFpEF
Treatment of Stages A to D

Treatment of HFpEFRecommendations COR LOE
Systolic and diastolic blood pressure should be controlled
according to published clinical practice guidelines I B
Diuretics should be used for relief of symptoms due to
volume overloadI C
Coronary revascularization for patients with CAD in
whom angina or demonstrable myocardial ischemia is
present despite GDMT
IIaC
Management of AF according to published clinical
practice guidelines for HFpEF to improve symptomatic
HF
IIa C
Use of beta-blocking agents, ACE inhibitors, and ARBs
for hypertension in HFpEF IIa C
ARBs might be considered to decrease hospitalizations in
HFpEFIIb B
Nutritional supplementation is not recommended in
HFpEF
III: No
BenefitC

Device Treatment for Stage C
HFrEF
Treatment of Stages A to D

Device Therapy for Stage C HFrEF
ICD therapy is recommended for primary prevention of SCD to reducetotal mortality in selected patients with nonischemic DCM or ischemicheart disease at least 40 days post-MI with LVEF of 35% or less, andNYHA class II or III symptoms on chronic GDMT, who have reasonableexpectation of meaningful survival for more than 1 year.
CRT is indicated for patients who have LVEF of 35% or less, sinusrhythm, left bundle-branch block (LBBB) with a QRS duration of 150 msor greater, and NYHA class II, III, or ambulatory IV symptoms on GDMT.
I IIa IIb III
I IIa IIb III
NYHA Class III/IV
I IIa IIb III
NYHA Class II

Device Therapy for Stage C HFrEF
(cont.)
ICD therapy is recommended for primary prevention of SCD toreduce total mortality in selected patients at least 40 days post-MI with LVEF less than or equal to 30%, and NYHA class Isymptoms while receiving GDMT, who have reasonableexpectation of meaningful survival for more than 1 year.
CRT can be useful for patients who have LVEF of 35% or less,sinus rhythm, a non-LBBB pattern with a QRS duration of 150ms or greater, and NYHA class III/ambulatory class IV symptomson GDMT.
I IIa IIb III
I IIa IIb III

Device Therapy for Stage C HFrEF
(cont.)
CRT can be useful for patients who have LVEF of 35% or less,sinus rhythm, LBBB with a QRS duration of 120 to 149 ms, andNYHA class II, III, or ambulatory IV symptoms on GDMT.
CRT can be useful in patients with AF and LVEF of 35% or less onGDMT if a) the patient requires ventricular pacing or otherwisemeets CRT criteria and b) atrioventricular nodal ablation orpharmacological rate control will allow near 100% ventricularpacing with CRT.
I IIa IIb III
I IIa IIb III

Device Therapy for Stage C HFrEF
(cont.)
CRT can be useful for patients on GDMT who have LVEF of 35%or less, and are undergoing placement of a new or replacementdevice placement with anticipated requirement for significant(>40%) ventricular pacing.
The usefulness of implantation of an ICD is of uncertain benefitto prolong meaningful survival in patients with a high risk ofnonsudden death as predicted by frequent hospitalizations,advanced frailty, or comorbidities such as systemic malignancyor severe renal dysfunction.
I IIa IIb III
I IIa IIb III

Device Therapy for Stage C HFrEF
(cont.)
CRT may be considered for patients who have LVEF of 35% orless , sinus rhythm, a non-LBBB pattern with a QRS duration of150 ms or greater, and NYHA class II symptoms on GDMT.
CRT may be considered for patients who have LVEF of 30% orless, ischemic etiology of HF, sinus rhythm, LBBB with a QRSduration of 150 ms or greater, and NYHA class I symptoms onGDMT.
I IIa IIb III
I IIa IIb III

Device Therapy for Stage C HFrEF
(cont.)
CRT is not recommended for patients with NYHA class I or IIsymptoms and non-LBBB pattern with a QRS duration of lessthan 150 ms.
CRT is not indicated for patients whose comorbidities and/orfrailty limit survival with good functional capacity to less than 1year.
I IIa IIb III
I IIa IIb III
No Benefit
No Benefit

Indications for CRT TherapyPatient with cardiomyopathy on GDMT for >3 mo or on GDMT and >40 d after MI, or
with implantation of pacing or defibrillation device for special indications
LVEF <35%
Evaluate general health status
Comorbidities and/or frailty
limit survival with good
functional capacity to <1 y
Continue GDMT without
implanted device
Acceptable noncardiac health
Evaluate NYHA clinical status
NYHA class I
LVEF ≤30%
QRS ≥150 ms
LBBB pattern
Ischemic
cardiomyopathy
QRS ≤150 ms
Non-LBBB pattern
NYHA class II
LVEF ≤35%
QRS 120-149 ms
LBBB pattern
Sinus rhythm
QRS ≤150 ms
Non-LBBB pattern
LVEF ≤35%
QRS ≥150 ms
LBBB pattern
Sinus rhythm
LVEF ≤35%
QRS ≥150 ms
Non-LBBB pattern
Sinus rhythm
Colors correspond to the class of recommendations in the ACCF/AHA Table 1.
Benefit for NYHA class I and II patients has only been shown in CRT-D trials, and while patients may not experience immediate symptomatic benefit, late remodeling may be avoided along
with long-term HF consequences. There are no trials that support CRT-pacing (without ICD) in NYHA class I and II patients. Thus, it is anticipated these patients would receive CRT-D
unless clinical reasons or personal wishes make CRT-pacing more appropriate. In patients who are NYHA class III and ambulatory class IV, CRT-D may be chosen but clinical reasons and
personal wishes may make CRT-pacing appropriate to improve symptoms and quality of life when an ICD is not expected to produce meaningful benefit in survival.
NYHA class III &
Ambulatory class IV
LVEF ≤35%
QRS 120-149 ms
LBBB pattern
Sinus rhythm
LVEF ≤35%
QRS 120-149 ms
Non-LBBB pattern
Sinus rhythm
LVEF ≤35%
QRS ≥150 ms
LBBB pattern
Sinus rhythm
LVEF≤35%
QRS ≥150 ms
Non-LBBB pattern
Sinus rhythm
Anticipated to require
frequent ventricular
pacing (>40%)
Atrial fibrillation, if
ventricular pacing is
required and rate
control will result in
near 100%
ventricular pacing
with CRT
Special CRT
Indications

Device Therapy for Stage C HFrEF (cont.)Recommendations COR LOE
ICD therapy is recommended for primary prevention of SCD in selected
patients with HFrEF at least 40 days post-MI with LVEF ≤35%, and NYHA
class II or III symptoms on chronic GDMT, who are expected to live ≥1 year*I A
CRT is indicated for patients who have LVEF ≤35%, sinus rhythm, LBBB with
a QRS ≥150 msI
A (NYHA
class III/IV)
B (NYHA
class II)
ICD therapy is recommended for primary prevention of SCD in selected
patients with HFrEF at least 40 days post-MI with LVEF ≤30%, and NYHA
class I symptoms while receiving GDMT, who are expected to live ≥1 year*I B
CRT can be useful for patients who have LVEF ≤35%, sinus rhythm, a non-
LBBB pattern with a QRS ≥150 ms, and NYHA class III/ambulatory class IV
symptoms on GDMT.
IIa A
CRT can be useful for patients who have LVEF ≤35%, sinus rhythm, LBBB
with a QRS 120 to 149 ms, and NYHA class II, III or ambulatory IV symptoms
on GDMT
IIaB
CRT can be useful in patients with AF and LVEF ≤35% on GDMT if a) the
patient requires ventricular pacing or otherwise meets CRT criteria and b) AV
nodal ablation or rate control allows near 100% ventricular pacing with CRT
IIa B

Recommendations COR LOE
CRT can be useful for patients on GDMT who have LVEF ≤35%, and are
undergoing new or replacement device with anticipated (>40%) ventricular
pacing
IIa C
An ICD is of uncertain benefit to prolong meaningful survival in patients with
high risk of nonsudden death such as frequent hospitalizations, frailty, or severe
comorbidities*
IIbB
CRT may be considered for patients who have LVEF ≤35%, sinus rhythm, a non-
LBBB pattern with QRS 120 to 149 ms, and NYHA class III/ambulatory class IV
on GDMT
IIb B
CRT may be considered for patients who have LVEF ≤35%, sinus rhythm, a non-
LBBB pattern with a QRS ≥150 ms, and NYHA class II symptoms on GDMT IIb B
CRT may be considered for patients who have LVEF ≤30%, ischemic etiology of
HF, sinus rhythm, LBBB with a QRS ≥150 ms, and NYHA class I symptoms on
GDMT
IIb C
CRT is not recommended for patients with NYHA class I or II symptoms and
non-LBBB pattern with QRS <150 ms
III: No
BenefitB
CRT is not indicated for patients whose comorbidities and/or frailty limit
survival to <1 year
III: No
BenefitC
Device Therapy for Stage C HFrEF (cont.)
Stage D
Treatment of Stages A to D

Clinical Events and Findings Useful for
Identifying Patients With Advanced HF
Repeated (≥2) hospitalizations or ED visits for HF in the past year
Progressive deterioration in renal function (e.g., rise in BUN and creatinine)
Weight loss without other cause (e.g., cardiac cachexia)
Intolerance to ACE inhibitors due to hypotension and/or worsening renal function
Intolerance to beta blockers due to worsening HF or hypotension
Frequent systolic blood pressure <90 mm Hg
Persistent dyspnea with dressing or bathing requiring rest
Inability to walk 1 block on the level ground due to dyspnea or fatigue
Recent need to escalate diuretics to maintain volume status, often reaching daily
furosemide equivalent dose >160 mg/d and/or use of supplemental metolazone therapy
Progressive decline in serum sodium, usually to <133 mEq/L
Frequent ICD shocks
Adapted from Russell et al. Congest Heart Fail. 2008;14:316-21.
Water Restriction
Treatment of Stages A to D
Water Restriction
Fluid restriction (1.5 to 2 L/d) is reasonable in stageD, especially in patients with hyponatremia, toreduce congestive symptoms.
I IIa IIb III

Inotropic Support
Treatment of Stages A to D

Inotropic Support
Until definitive therapy (e.g., coronary revascularization, MCS, heart transplantation) or resolution of the acute precipitating problem, patients with cardiogenic shock should receive temporary intravenous inotropic support to maintain systemic perfusion and preserve end-organ performance.
Continuous intravenous inotropic support is reasonable as “bridge therapy” in patients with stage D refractory to GDMT and device therapy who are eligible for and awaiting MCS or cardiac transplantation.
I IIa IIb III
I IIa IIb III

Inotropic Support (cont.)
Short-term, continuous intravenous inotropic support may be reasonable in those hospitalized patients presenting with documented severe systolic dysfunction who present with low blood pressure and significantly depressed cardiac output to maintain systemic perfusion and preserve end-organ performance.
Long-term, continuous intravenous inotropic support may be considered as palliative therapy for symptom control in select patients with stage D despite optimal GDMT and device therapy who are not eligible for either MCS or cardiac transplantation.
I IIa IIb III
I IIa IIb III
Inotropic Support (cont.)
Long-term use of either continuous or intermittent, intravenous parenteral positive inotropic agents, in the absence of specific indications or for reasons other than palliative care, is potentially harmful in the patient with HF.
Use of parenteral inotropic agents in hospitalized patients without documented severe systolic dysfunction, low blood pressure, or impaired perfusion, and evidence of significantly depressed cardiac output, with or without congestion, is potentially harmful.
I IIa IIb III
I IIa IIb III
Harm
Harm


Mechanical Circulatory
Support
Treatment of Stages A to D

Mechanical Circulatory Support
MCS use is beneficial in carefully selected* patients with stage D HFrEF in whom definitive management (e.g., cardiac transplantation) or cardiac recovery is anticipated or planned.
Nondurable MCS, including the use of percutaneous and extracorporeal ventricular assist devices (VADs), is reasonable as a “bridge to recovery” or a “bridge to decision” for carefully selected patients with HFrEF with acute, profound hemodynamic compromise.
Durable MCS is reasonable to prolong survival for carefully selected patients with stage D HFrEF.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Cardiac Transplantation
Treatment of Stages A to D

Cardiac Transplantation
Evaluation for cardiac transplantation is indicated forcarefully selected patients with stage D HF despiteGDMT, device, and surgical management.
I IIa IIb III
The Hospitalized Patient
Guideline for HF

Precipitating Causes of
Decompensated HF
The Hospitalized Patient

Precipitating Causes of Decompensated
HF
ACS precipitating acute HF decompensation should be promptlyidentified by ECG and serum biomarkers including cardiactroponin testing, and treated optimally as appropriate to theoverall condition and prognosis of the patient.
Common precipitating factors for acute HF should be consideredduring initial evaluation, as recognition of these conditions iscritical to guide appropriate therapy.
I IIa IIb III
I IIa IIb III

Maintenance of GDMT During
Hospitalization
The Hospitalized Patient

Maintenance of GDMT During
Hospitalization
In patients with HFrEF experiencing a symptomatic exacerbation ofHF requiring hospitalization during chronic maintenance treatmentwith GDMT, it is recommended that GDMT be continued in theabsence of hemodynamic instability or contraindications.
Initiation of beta-blocker therapy is recommended afteroptimization of volume status and successful discontinuation ofintravenous diuretics, vasodilators, and inotropic agents. Beta-blocker therapy should be initiated at a low dose and only in stablepatients. Caution should be used when initiating beta blockers inpatients who have required inotropes during their hospital course.
I IIa IIb III
I IIa IIb III
Diuretics in Hospitalized
Patients
The Hospitalized Patient

Diuretics in Hospitalized Patients
Patients with HF admitted with evidence of significant fluid overload should be promptly treated with intravenous loop diuretics to reduce morbidity.
If patients are already receiving loop diuretic therapy, the initial intravenous dose should equal or exceed their chronic oral daily dose and should be given as either intermittent boluses or continuous infusion. Urine output and signs and symptoms of congestion should be serially assessed, and the diuretic dose should be adjusted accordingly to relieve symptoms, reduce volume excess, and avoid hypotension.
I IIa IIb III
I IIa IIb III

Diuretics in Hospitalized Patients (cont.)
The effect of HF treatment should be monitored with careful measurement of fluid intake and output, vital signs, body weight that is determined at the same time each day, and clinical signs and symptoms of systemic perfusion and congestion. Daily serum electrolytes, urea nitrogen, and creatinine concentrations should be measured during the use of intravenous diuretics or active titration of HF medications.
When diuresis is inadequate to relieve symptoms, it is reasonable to intensify the diuretic regimen using either:
a. higher doses of intravenous loop diuretics.
b. addition of a second (e.g., thiazide) diuretic.
I IIa IIb III
I IIa IIb III

Diuretics in Hospitalized Patients (cont.)
Low-dose dopamine infusion may be considered in addition to loop diuretic therapy to improve diuresis and better preserve renal function and renal blood flow.
I IIa IIb III

Parenteral Therapy in
Hospitalized HF
The Hospitalized Patient

Parenteral Therapy in Hospitalized HF
If symptomatic hypotension is absent, intravenousnitroglycerin, nitroprusside or nesiritide may beconsidered an adjuvant to diuretic therapy for reliefof dyspnea in patients admitted with acutelydecompensated HF.
I IIa IIb III
Venous Thromboembolism
Prophylaxis in Hospitalized
Patients
The Hospitalized Patient

Venous Thromboembolism Prophylaxis
in Hospitalized Patients
A patient admitted to the hospital with decompensated HF should be treated for venous thromboembolism prophylaxis with an anticoagulant medication if the risk:benefit ratio is favorable.
I IIa IIb III

Inpatient and Transitions of
Care
The Hospitalized Patient

Inpatient and Transitions of Care
The use of performance improvement systems and/or evidence-based systems of care is recommended in the hospital and early post-discharge outpatient setting to identify appropriate HF patients for GDMT, provide clinicians with useful reminders to advance GDMT, and to assess the clinical response.
I IIa IIb III

Inpatient and Transitions of Care
Throughout the hospitalization as appropriate, before hospital discharge, at the first postdischarge visit, and in subsequent follow-up visits, the following should be addressed:
a. initiation of GDMT if not previously established and not contraindicated;
b. precipitant causes of HF, barriers to optimal care transitions, and limitations in postdischarge support;
c. assessment of volume status and supine/upright hypotension with adjustment of HF therapy, as appropriate;
d. titration and optimization of chronic oral HF therapy;
e. assessment of renal function and electrolytes, where appropriate;
f. assessment and management of comorbid conditions;
g. reinforcement of HF education, self-care, emergency plans, and need for adherence; and
h. consideration for palliative care or hospice care in selected patients.
I IIa IIb III

Inpatient and Transitions of Care
Multidisciplinary HF disease-management programs are recommended for patients at high risk for hospital readmission, to facilitate the implementation of GDMT, to address different barriers to behavioral change, and to reduce the risk of subsequent rehospitalization for HF.
Scheduling an early follow-up visit (within 7 to 14 days) and early telephone follow-up (within 3 days) of hospital discharge is reasonable.
Use of clinical risk prediction tools and/or biomarkers to identify patients at higher risk for postdischarge clinical events is reasonable.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Therapies in the Hospitalized HF Patient
Recommendation COR LOE
HF patients hospitalized with fluid overload should be treated with
intravenous diureticsI B
HF patients receiving loop diuretic therapy, should receive an initial
parenteral dose greater than or equal to their chronic oral daily dose, then
should be serially adjusted
I B
HFrEF patients requiring HF hospitalization on GDMT should continue
GDMT unless hemodynamic instability or contraindicationsI B
Initiation of beta-blocker therapy at a low dose is recommended after
optimization of volume status and discontinuation of intravenous agents I B
Thrombosis/thromboembolism prophylaxis is recommended for patients
hospitalized with HFI B
Serum electrolytes, urea nitrogen, and creatinine should be measured
during the titration of HF medications, including diureticsI C

Hospital Discharge
Recommendation or Indication COR LOE
Performance improvement systems in the hospital and early postdischarge outpatient setting
to identify HF for GDMTI B
Before hospital discharge, at the first postdischarge visit, and in subsequent follow-up visits,
the following should be addressed:
a) initiation of GDMT if not done or contraindicated;
b) causes of HF, barriers to care, and limitations in support;
c) assessment of volume status and blood pressure with adjustment of HF therapy;
d) optimization of chronic oral HF therapy;
e) renal function and electrolytes;
f) management of comorbid conditions;
g) HF education, self-care, emergency plans, and adherence; and
h) palliative or hospice care.
I B
Multidisciplinary HF disease-management programs for patients at high risk for hospital
readmission are recommended I B
A follow-up visit within 7 to 14 days and/or a telephone follow-up within 3 days of hospital
discharge is reasonableIIa B
Use of clinical risk-prediction tools and/or biomarkers to identify higher-risk patients is
reasonableIIa B
Surgical/Percutaneous/
Transcatheter Interventional
Treatments of HF
Guideline for HF

Surgical/Percutaneous/Transcatheter
Interventional Treatment of HF
Recommendation COR LOE
CABG or percutaneous intervention is indicated for HF patients on GDMT with
angina and suitable coronary anatomy especially, significant left main stenosis or left
main equivalent disease
I C
CABG to improve survival is reasonable in patients with mild to moderate LV
systolic dysfunction and significant multivessel CAD or proximal LAD stenosis
when viable myocardium is present
IIa B
CABG or medical therapy is reasonable to improve morbidity and mortality for
patients with severe LV dysfunction (EF <35%), HF and significant CAD IIa B
Surgical aortic valve replacement is reasonable for patients with critical aortic
stenosis and a predicted surgical mortality of no greater than 10%IIa B
Transcatheter aortic valve replacement is reasonable for patients with critical aortic
stenosis who are deemed inoperable IIa B
CABG may be considered in patients with ischemic heart disease, severe LV systolic
dysfunction and suitable coronary anatomy whether or not viable myocardium is
present
IIb B
Transcatheter mitral valve repair or mitral valve surgery for functional mitral
insufficiency is of uncertain benefit IIb B
Surgical reverse remodeling or LV aneurysmectomy may be considered in HFrEF for
specific indications including intractable HF and ventricular arrhythmias IIb B

Coordinating Care for Patients
With Chronic HF
Guideline for HF

Coordinating Care for Patients With
Chronic HFEffective systems of care coordination with special attention to care transitions should be deployed for every patient with chronic HF that facilitate and ensure effective care that is designed to achieve GDMT and prevent hospitalization.
Every patient with HF should have a clear, detailed and evidence-based plan of care that ensures the achievement of GDMT goals, effective management of comorbid conditions, timely follow-up with the healthcare team, appropriate dietary and physical activities, and compliance with Secondary Prevention Guidelines for cardiovascular disease. This plan of care should be updated regularly and made readily available to all members of each patient’s healthcare team.
Palliative and supportive care is effective for patients with symptomatic advanced HF to improve quality of life.
I IIa IIb III
I IIa IIb III
I IIa IIb III

Quality Metrics/Performance
Measures
Guideline for HF

Quality Metrics/Performance Measures
Performance measures based on professionally developed clinical practice guidelines should be used with the goal of improving quality of care for HF.
Participation in quality improvement programs and patient registries based on nationally endorsed, clinical practice guideline-based quality and performance measures may be beneficial in improving quality of HF care.
I IIa IIb III
I IIa IIb III

• Evidence-based guideline directed diagnosis, evaluation and therapy should be the mainstay for all patients with HF.
• Effective implementation of guideline-directed best quality care reduces mortality, improves QOL and preserves health care resources.
• Ongoing research is needed to answer the remaining questions including: prevention, nonpharmacological therapy of HF including dietary adjustments, treatment of HFpEF, management of hospitalized HF, effective reduction in HF readmissions, more precise use of device-based therapy.
Conclusions

Thankyou

Common Factors That Precipitate Acute Decompensated HF
Nonadherence with medication regimen,
sodium and/or
fluid restriction
Acute myocardial ischemia
Uncorrected high blood pressure
AF and other arrhythmias
Recent addition of negative inotropic drugs (e.g.,
verapamil, nifedipine, diltiazem, beta blockers)
Pulmonary embolus
Initiation of drugs that increase salt retention (e.g.,
steroids, thiazolidinediones, NSAIDs)
Excessive alcohol or illicit drug use
Endocrine abnormalities (e.g., diabetes mellitus,
hyperthyroidism, hypothyroidism)
Concurrent infections (e.g., pneumonia, viral illnesses)
Additional acute cardiovascular disorders (e.g., valve
disease endocarditis, myopericarditis, aortic dissection)

Although optimal patient selection for MCS remains an active area of
investigation, general indications for referral for MCS therapy include
patients with LVEF <25% and
NYHA class III–IV functional status despite GDMT, including,
when indicated, CRT, with either high predicted 1- to 2-year mortality
(e.g., as suggested by markedly reduced peak oxygen consumption
and clinical prognostic scores) or dependence on continuous
parenteral inotropic support.
Patient selection requires a multidisciplinary team of experienced
advanced HF and transplantation cardiologists, cardiothoracic
surgeons, nurses, and ideally, social workers and
palliative care clinicians.

ACCF/AHA/AMA-PCPI 2011 HF Performance
Measurement Set
Measure Description* Care
Setting
Level of
Measurement
1. LVEF
assessment
Percentage of patients aged ≥18 y with a diagnosis of HF for whom the
quantitative or qualitative results of a recent or prior (any time in the
past) LVEF assessment is documented within a 12 mo period
Outpatient Individual
practitioner
2. LVEF
assessment
Percentage of patients aged ≥18 y with a principal discharge diagnosis
of HF with documentation in the hospital record of the results of an
LVEF assessment that was performed either before arrival or during
hospitalization, OR documentation in the hospital record that LVEF
assessment is planned for after discharge
Inpatient Individual
practitioner
Facility
3. Symptom
and activity
assessment
Percentage of patient visits for those patients aged ≥18 y with a
diagnosis of HF with quantitative results of an evaluation of both
current level of activity and clinical symptoms documented
Outpatien
t
Individual
practitioner
*Please refer to the complete measures for comprehensive information, including measure exception.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.

ACCF/AHA/AMA-PCPI 2011 HF Performance Measurement Set (cont.)
Measure Description* Care
Setting
Level of
Measurement
4. Symptom
management†
Percentage of patient visits for those patients aged ≥18 y with a
diagnosis of HF and with quantitative results of an evaluation of both
level of activity AND clinical symptoms documented in which patient
symptoms have improved or remained consistent with treatment goals
since last assessment OR patient symptoms have demonstrated
clinically important deterioration since last assessment with a
documented plan of care
Outpatient Individual
practitioner
5. Patient self-
care education†‡
Percentage of patients aged ≥18 y with a diagnosis of HF who were
provided with self-care education on ≥3 elements of education during
≥1 visits within a 12 mo period
Outpatient Individual
practitioner
6. Beta-blocker
therapy for LVSD
(outpatient and
inpatient setting)
Percentage of patients aged ≥18 y with a diagnosis of HF with a
current or prior LVEF <40% who were prescribed beta-blocker
therapy with bisoprolol, carvedilol, or sustained release metoprolol
succinate either within a 12 mo period when seen in the outpatient
setting or at hospital discharge
Inpatient
and
Outpatient
Individual
practitioner
Facility
*Please refer to the complete measures for comprehensive information, including measure exception.
†Test measure designated for use in internal quality improvement programs only. These measures are not appropriate for any other
purpose, e.g., pay for performance, physician ranking or public reporting programs.
‡New measure.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.

ACCF/AHA/AMA-PCPI 2011 HF Performance Measurement Set (cont.)
Measure Description* Care Setting Level of
Measurement
7. ACE Inhibitor or
ARB Therapy for
LVSD (outpatient and
inpatient setting)
Percentage of patients aged ≥18 y with a diagnosis of HF with a
current or prior LVEF <40% who were prescribed ACE inhibitor or
ARB therapy either within a 12 mo period when seen in the outpatient
setting or at hospital discharge
Inpatient
and
Outpatient
Individual
practitioner
Facility
8. Counseling
regarding ICD
implantation for
patients with LVSD on
combination medical
therapy†‡
Percentage of patients aged ≥18 y with a diagnosis of HF with current
LVEF ≤35% despite ACE inhibitor/ARB and beta-blocker therapy for
at least 3 mo who were counseled regarding ICD implantation as a
treatment option for the prophylaxis of sudden death
Outpatient Individual
practitioner
9. Post-discharge
appointment for heart
failure patients
Percentage of patients, regardless of age, discharged from an inpatient
facility to ambulatory care or home health care with a principal
discharge diagnosis of HF for whom a follow-up appointment was
scheduled and documented including location, date and time for a
follow-up office visit, or home health visit (as specified)
Inpatient Facility
*Please refer to the complete measures for comprehensive information, including measure exception.
†Test measure designated for use in internal quality improvement programs only. These measures are not appropriate for any other
purpose, e.g., pay for performance, physician ranking or public reporting programs.
‡New measure.
Adapted from Bonow et al. J Am Coll Cardiol. 2012;59:1812-32.




• Volume Displacement
– Thoratec
– Novacor
– Heartmate LVAS
– Abiomed
• Axial Flow
– Heartmate II
– Jarvik
• Centrifugal
– CentriMag
– Heartware
Baughman KL, Jarcho JA. NEJM 2007;379(9):846-9.
Mechanical Circulatory Support: Ventricular Assist Devices: Bridge to Tx, Destination Therapy


Medical Therapy for Stage C HFrEF:
Magnitude of Benefit Demonstrated in RCTs
GDMTRR Reduction
in Mortality
NNT for Mortality
Reduction
(Standardized to 36 mo)
RR Reduction
in HF
Hospitalizations
ACE inhibitor or
ARB17% 26 31%
Beta blocker 34% 9 41%
Aldosterone
antagonist30% 6 35%
Hydralazine/nitrate 43% 7 33%

Therapies in the Hospitalized HF Patient (cont.)
Recommendation COR LOE
When diuresis is inadequate, it is reasonable to
a) Give higher doses of intravenous loop diuretics; or
b) add a second diuretic (e.g., thiazide)
IIa
B
B
Low-dose dopamine infusion may be considered with loop diuretics to
improve diuresis IIb B
Ultrafiltration may be considered for patients with obvious volume
overloadIIb B
Ultrafiltration may be considered for patients with refractory congestion IIb C
Intravenous nitroglycerin, nitroprusside or nesiritide may be considered an
adjuvant to diuretic therapy for stable patients with HF IIb B
In patients hospitalized with volume overload and severe hyponatremia,
vasopressin antagonists may be considered IIb B

Framingham Criteria for Congestive Heart FailureDiagnosis of CHF requires the simultaneous presence of at least 2 major criteria or 1major criterion in conjunction with 2 minor criteria.
Major criteria:· Paroxysmal nocturnal dyspnea· Neck vein distention· Rales· Radiographic cardiomegaly (increasing heart size on chest radiography)· Acute pulmonary edema· S3 gallop· Increased central venous pressure (>16 cm H2O at right atrium)· Hepatojugular reflux· Weight loss >4.5 kg in 5 days in response to treatment
Minor criteria:· Bilateral ankle edema· Nocturnal cough· Dyspnea on ordinary exertion· Hepatomegaly· Pleural effusion· Decrease in vital capacity by one third from maximum recorded· Tachycardia (heart rate>120 beats/min.)The Framingham Heart Study criteria are 100% sensitive and 78% specific foridentifying persons with definite congestive heart failure.


















