Chest Pain Intern Report Curriculum. Five point approach 1: ECG 2:History Most diagnoses are clear...
32
Chest Pain Intern Report Curriculum
-
Upload
meaghan-wilkerson -
Category
Documents
-
view
217 -
download
0
Transcript of Chest Pain Intern Report Curriculum. Five point approach 1: ECG 2:History Most diagnoses are clear...
Chest PainIntern Report Curriculum
Five point approach
1: ECG 2:History
• Most diagnoses are clear from a good history 3: Physical exam 4: CXR 5: Labs

Sick vs. Not Sick
Evaluate need for emergent care and associated emergent management• Guided by Focused History and Physical, along with
ECG and chest radiograph
• Awaiting labs may not be appropriate in emergent situations
• If patients are sick and may need emergent intervention, always get your resident, fellow, etc. involved early!
History: listen to the patient! Let the patient describe
symptoms – few will say “I’m having chest pain” • Discomfort
• Heaviness
• Squeezing
• Pressure
• Tightness
• Burning
• Indigestion
Quickly find out what chronic conditions the patient has:• CAD
– CABG, PCI
• DM2
• HTN
• PAD
• COPD
• GERD
• CKD
History: Questions to ask
#1: Are you having chest pain right now? (acuity) Have you ever had pain like this before? (history) When did the pain start? (timing) What were you doing when the pain started?
(association with activity) How would you describe the pain? (quality)

History: Questions to ask How would you rate the pain (1-10)? (quantity) Can you point to the pain? (location) Does the pain go to your back, neck, or arm?
(radiation) Were there other symptoms that accompanied the
pain? (SOB, diaphoresis, nausea, lightheadedness, palpitations)
Is there anything that makes the pain better or worse? (deep breaths, sitting up/lying down, SLNTG)
Physical exam
Obtain vital signs and look at the patient• Respiratory distress, diaphoresis, alertness
Pulmonary exam• Crackles, wheezes, decreased breath sounds
Cardiac exam• Assess JVP!
• Palpate carotids – note rate and rhythm
• Palpate the precordium
• Listen for murmurs and S3/S4
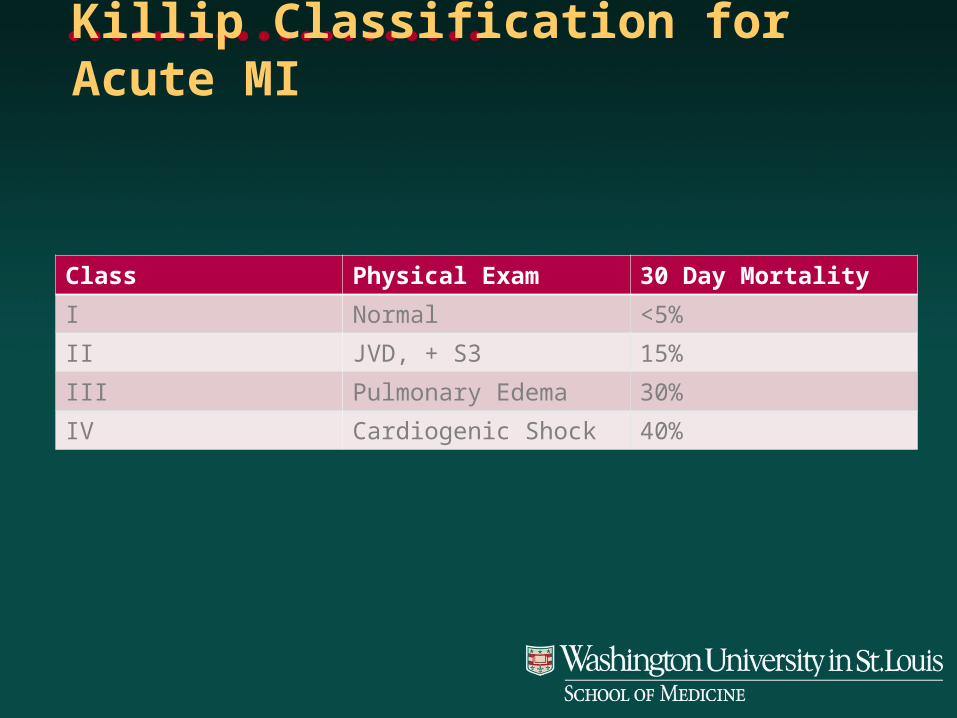
Killip Classification for Acute MI
Class Physical Exam 30 Day Mortality
I Normal <5%
II JVD, + S3 15%
III Pulmonary Edema 30%
IV Cardiogenic Shock 40%

ECG
Take at least 1 minute to read the entire ECG Look for ST segment changes or new LBBB Other clues:
• T-wave inversion or peaking
• Q waves (old MI)
• Conduction abnormality (new BBB or AVB)
• Axis deviation

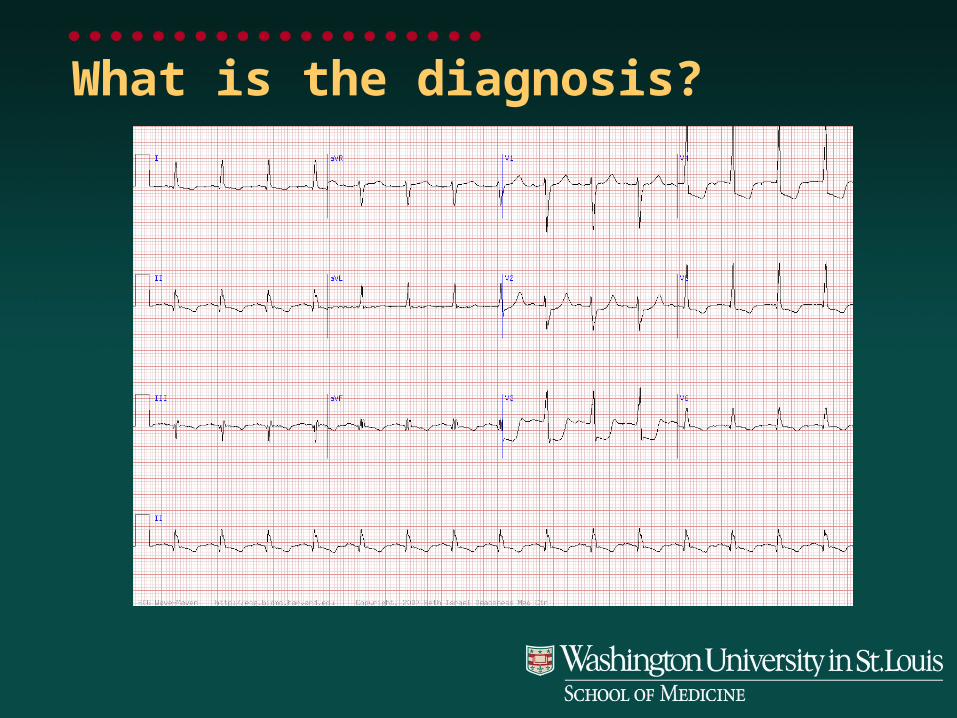
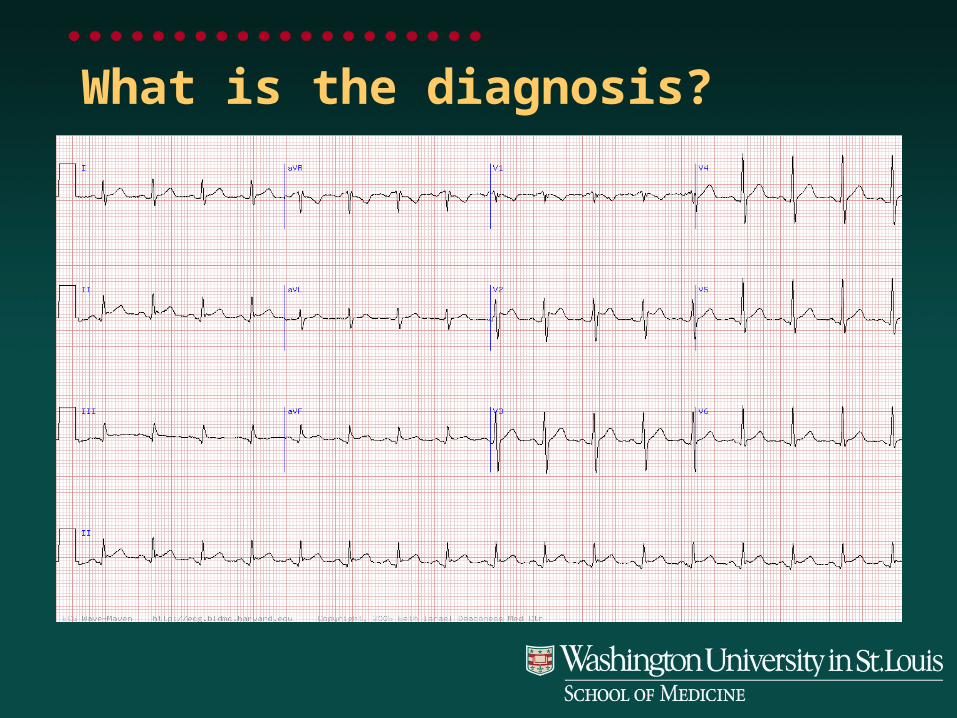
What is the diagnosis?
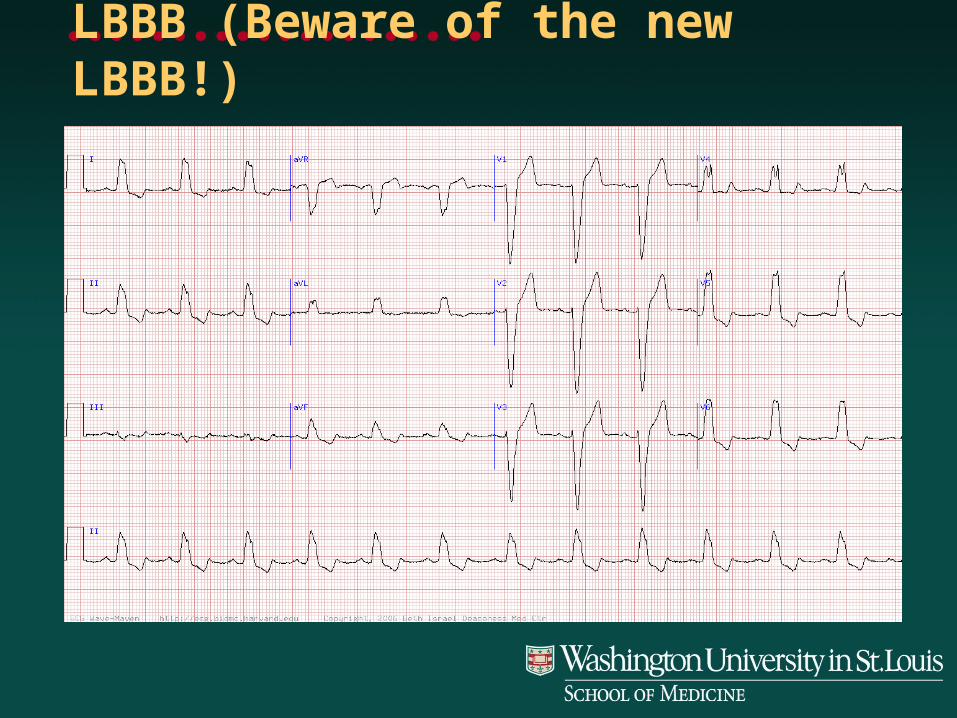
LBBB (Beware of the new LBBB!)
CXR
Systematic evaluation• Quick overview for glaring abnormalities
• Technique
• Skeleton (fractures, dislocations, lytic lesions)
• Abdomen (diaphragm, stomach)
• Airway/mediastinum
• Heart size and shape
• Lungs– Pneumothorax, infiltrates, edema, effusions

Labs
Troponin• Most sensitive for cardiac damage
• Repeat after 6-12 hours
CKMB• Helps determine timing of cardiac event
BNP?• Typically NOT useful for workup of chest pain
Others in case of urgent intervention• CBC, INR, PTT, BMP, beta-hCG

Elevation of Cardiac Biomarkers
http://www.publicsafety.net/image/graph.jpg

Differential diagnosisWhat is your DDX for
Emergent Chest pain?

JAMA 1998; 280:1256-1268
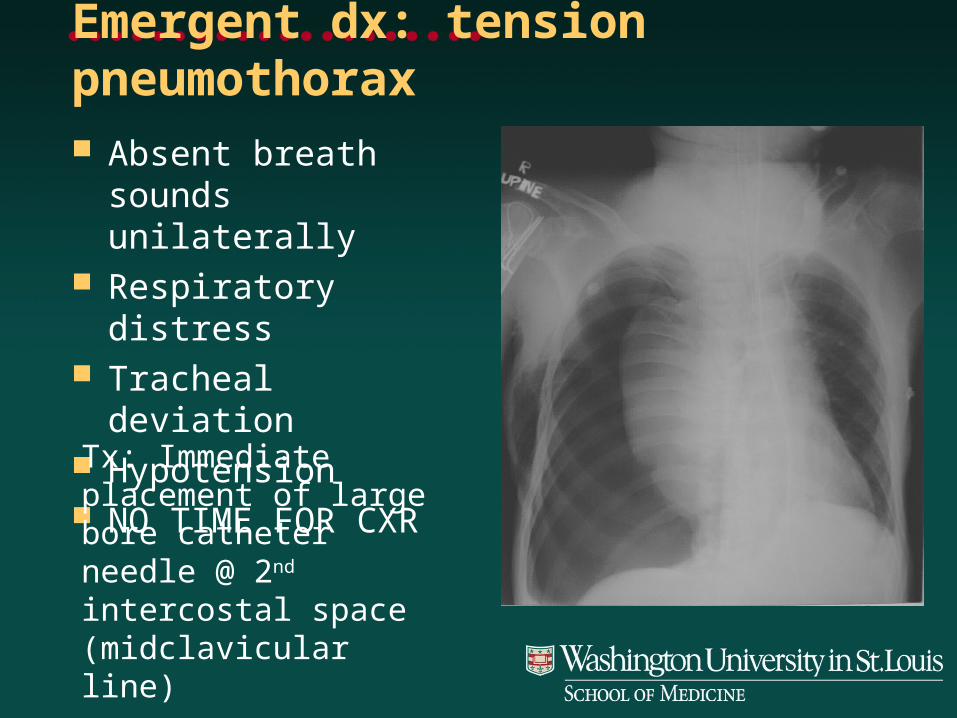
Emergent dx: tension pneumothorax Absent breath sounds
unilaterally Respiratory distress Tracheal deviation Hypotension NO TIME FOR CXR
Tx: Immediate placement of large bore catheter needle @ 2nd intercostal space (midclavicular line)
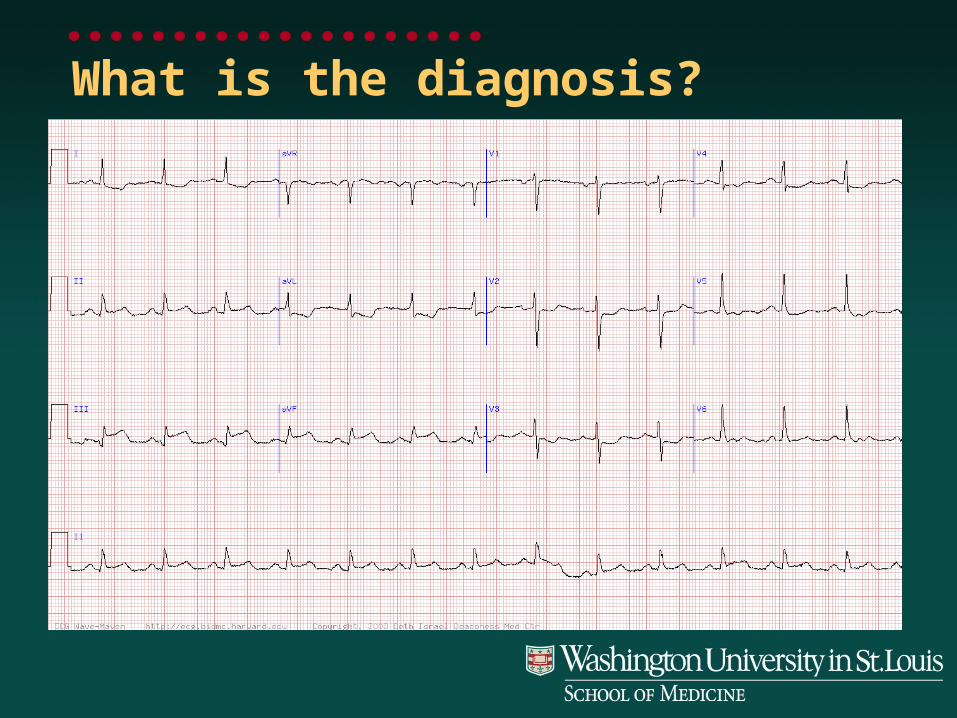
What is the diagnosis?
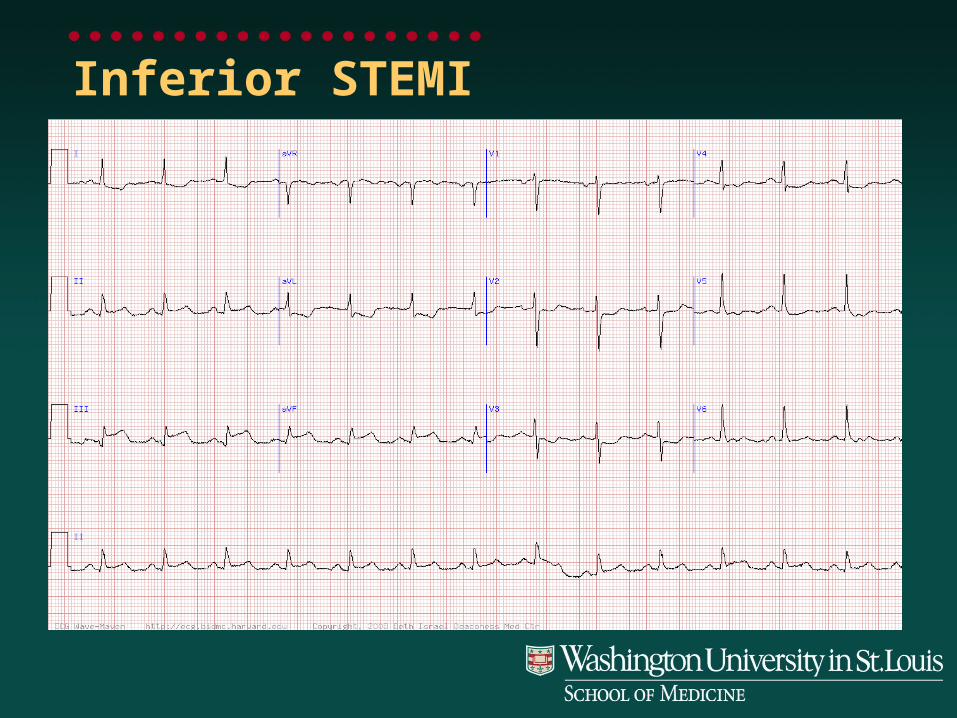
Inferior STEMI
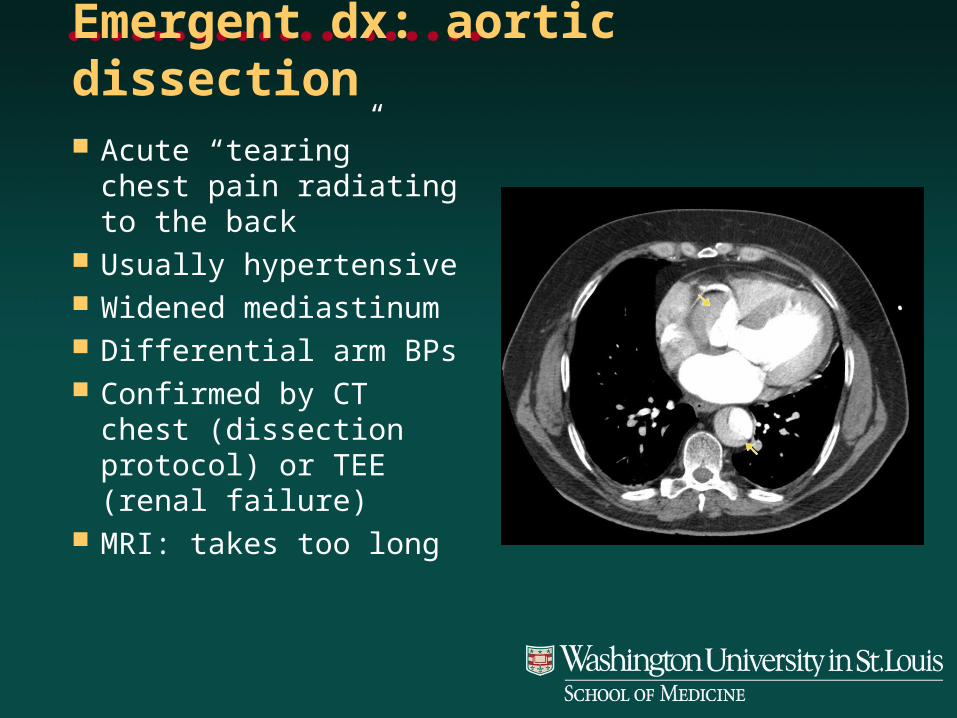
Emergent dx: aortic dissection Acute “tearing” chest
pain radiating to the back
Usually hypertensive Widened mediastinum Differential arm BPs Confirmed by CT chest
(dissection protocol) or TEE (renal failure)
MRI: takes too long

Emergent dx: aortic dissection NO ENOXAPARIN NO HEPARIN NO CLOPIDOGREL Emergent cardiac surgery consultation
• Mortality is 1-2% per hour for Type A
• 50% die within 48h
Esmolol drip – FIRST!• Titrate to HR 60s
Consider nitroprusside AVOID HYDRALZINE

What is the diagnosis?

Anterior STEMI (Transmural)

Emergent dx: STEMI Immediately page CCU fellow ASA 325 mg NTG (SL then drip; remember SL more potent!) Metoprolol (IV): goal HR 60s, SBP >100 Heparin drip (anti-thrombin) Plavix load-600mg Pt needs recent CBC, PTT, INR, BMP Ask about contrast allergy Cath lab immediately (usually)
What is the diagnosis?
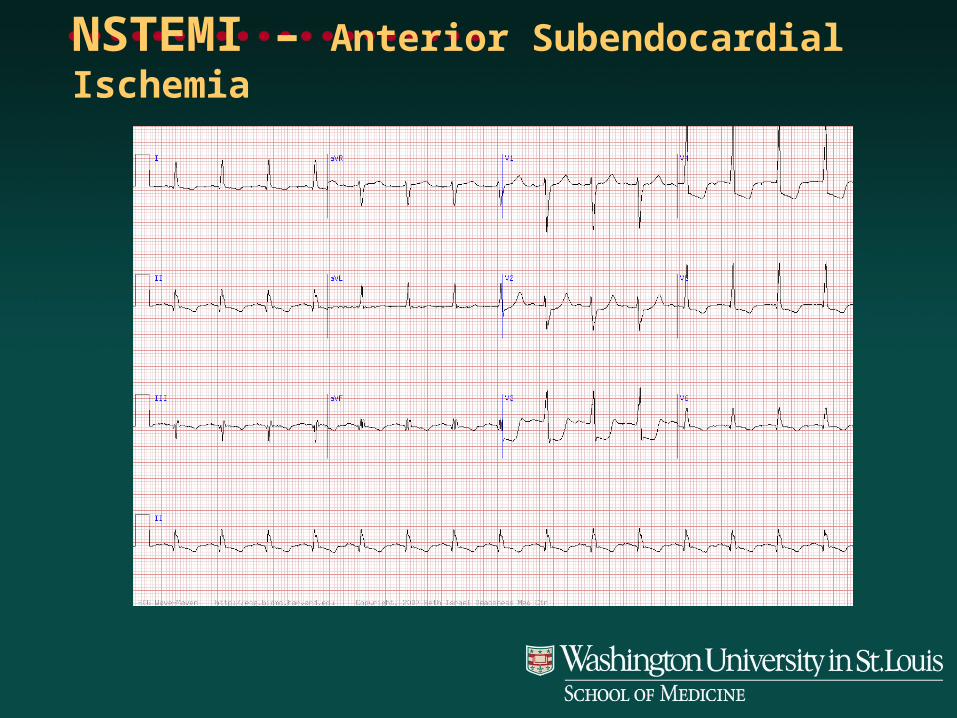
NSTEMI – Anterior Subendocardial Ischemia

What portion of heart not seen well on ECG?
Urgent dx: NSTEMI Immediate goal: relieve angina ASA 325 mg NTG: SLNTG, then IV nitro if needed
• If patient can not be made pain-free, may need cath lab Metoprolol (goal HR 60s) Heparin drip
• Consider enoxaparin GP IIb/IIIa inhibitor – usually Integrilin CAUTION Clopidogrel – load with 600 mg PO x 1

Urgent dx: pulmonary embolism Immobilized pt (ortho?) Evidence for DVT Acutely SOB Hypoxemia
High suspicion: PE protocol CT or VQ scan
Low suspicion: check D-dimer and LE Dopplers
If no contraindication and suspicion is high, begin treatment right away!
IV heparin• Consider enoxaparin
Warfarin ICU if hemodynamically
unstable Consider IVC filter if pt
cannot be anticoagulated
What is the diagnosis?

Acute Pericarditis!
Other diagnoses Acute pericarditis Hypertensive urgency Pneumonia Esophageal disease (incl. GERD, esophageal
spasm, Mallory-Weiss tear, Boerhaave’s syndrome)
Costochondritis Other GI (gastric/peptic ulcers, pancreatitis) Herpes zoster