Chest Pain and Risk Stratification - bryanhealth.com file8/29/2018 3 Patient Style/Behavior • A...
26
8/29/2018 1 Chest Pain and Risk Stratification Joseph L. Kummer, MD, FACC Bryan Heart Fall Conference September 1 st , 2018 Chest Pain Demographics • Chest Pain is the second most common complaint in the ER and among the most common complaints in the general medical practice clinical setting • 6 million ER visits annually in the US Etiologies • Usually benign, but need to exclude potentially emergent causes • Life-threatening causes: – Acute Myocardial Infarction – Pulmonary Embolus – Aortic Dissection – Tension Pneumothorax – Esophageal, Gastric Perforation – Cardiac Tamponade
Transcript of Chest Pain and Risk Stratification - bryanhealth.com file8/29/2018 3 Patient Style/Behavior • A...

8/29/2018
1
Chest Pain and Risk Stratification
Joseph L. Kummer, MD, FACC
Bryan Heart
Fall Conference
September 1st, 2018
Chest Pain Demographics
• Chest Pain is the second most common complaint in the ER and among the most common complaints in the general medical practice clinical setting
• 6 million ER visits annually in the US
Etiologies
• Usually benign, but need to exclude potentially emergent causes
• Life-threatening causes:– Acute Myocardial Infarction– Pulmonary Embolus– Aortic Dissection– Tension Pneumothorax– Esophageal, Gastric Perforation– Cardiac Tamponade

8/29/2018
2
ER Chest Pain Etiology
CAUSE PREVALENCE
Musculoskeletal 36
Gastrointestinal 19
Cardiac 16
+ Stable Angina 10.5
+ USA/MI 1.5
+ Other Cardiac 4
Psychiatric 8
Pulmonary 5
Unknown 16
ER Chest Pain EtiologyNon-Ischemic Cardiac Pulmonary Gastrointestinal
Aortic Dissection Pleurisy Biliary
Myocarditis Pneumonia + Cholangitis
Pericarditis Pulmonary Embolus + Choledocholithiasis
Tension Pneumothorax + Cholecystitis
Chest Wall + Colic
Cervical Disc Disease Psychiatric Esophageal
Costochondritis Depression + GERD
Herpes Zoster Anxiety Disorders + Esophagitis
Neuropathic + Primary Anxiety + Spasm
Rib Fracture + Hyperventilation + Rupture
Arthritis + Panic Disorder Pancreatitis
Somatiform Disorders Peptic Ulcer Disease
Trauma Secondary Gain + Non-perforating
+ Perforating
Missed Diagnosis
• An estimated 2.2% of patients with an Acute Coronary Syndrome are mistakenly discharged from the ED
• Typical characteristics:– Women less than 55 years of age
– Nonwhite
– Shortness of breath as the major symptom
– Normal or non-diagnostic ECG

8/29/2018
3
Patient Style/Behavior
• A study had physicians watch videos of an actress complaining to a doctor of chest pain using a scripted interview
• One setting, the actress was “businesslike,” in the other, she was “histrionic”
Patient Style/Behavior
• Coronary disease was suspected in 50% of the “businesslike” patient but only 13% of the “histrionic” patient
• Evaluation recommend in 93% of the “businesslike” group but only 53% in the “histrionic” group
Diagnostic Testing
• Laboratory– CBC, BMP, LFT’s, U/A– Cardiac Enzymes– Rheumatoid Factor, ESR
• Radiography– Chest X-Ray– Rib, Shoulder Films– CT Chest, Abdomen
• EKG
8/29/2018
4
Physical Examination
• General Appearance
• Vitals (pulse discrepancy)
• Palpation (reproducibility)
• Auscultation– Murmur (AS, MR, AI), Rub
– Breath Sounds (Present, Crackles, Wheezes)
– Abdominal Exam (Bowel Sounds, RUQ Tenderness, Abdominal Aorta)
CXR
• Aortic Dissection
• Pneumothorax
• Pulmonary Edema
• Pneumonia
• Neoplasm, PE, Pericardial Effusion
EKG
• A normal EKG at the time of chest pain markedly reduces the likelihood of cardiac ischemia
• A truly “normal” EKG is seen in less than 4% of patients in the ER with an acute MI

8/29/2018
5
Validity of Chest Pain Characteristics
Characteristic Likelihood Ratio
Radiation to Right Arm or Shoulder 4.7
Radiation to Bilateral Arms/Shoulders 4.1
Exertional 2.4
Radiation to Left Arm 2.3
Diaphoresis 2.0
Nausea/Vomiting 1.9
Worse than or similar to previous MI 1.8
Pressure 1.3
Validity of Chest Pain Characteristics
Characteristic Likelihood Ratio
Pleuritic 0.2
Positional 0.3
Sharp 0.3
Reproducible 0.3
Inframammary Location 0.8
Nonexertional 0.8
Other Pain Characteristics
• Chest pain lasting only seconds and present for months is almost never angina
• Relief with eating is likely GI in origin
• Relief (or lack thereof) with NTG or GI Cocktail does not change likelihood of a cardiac etiology
8/29/2018
6
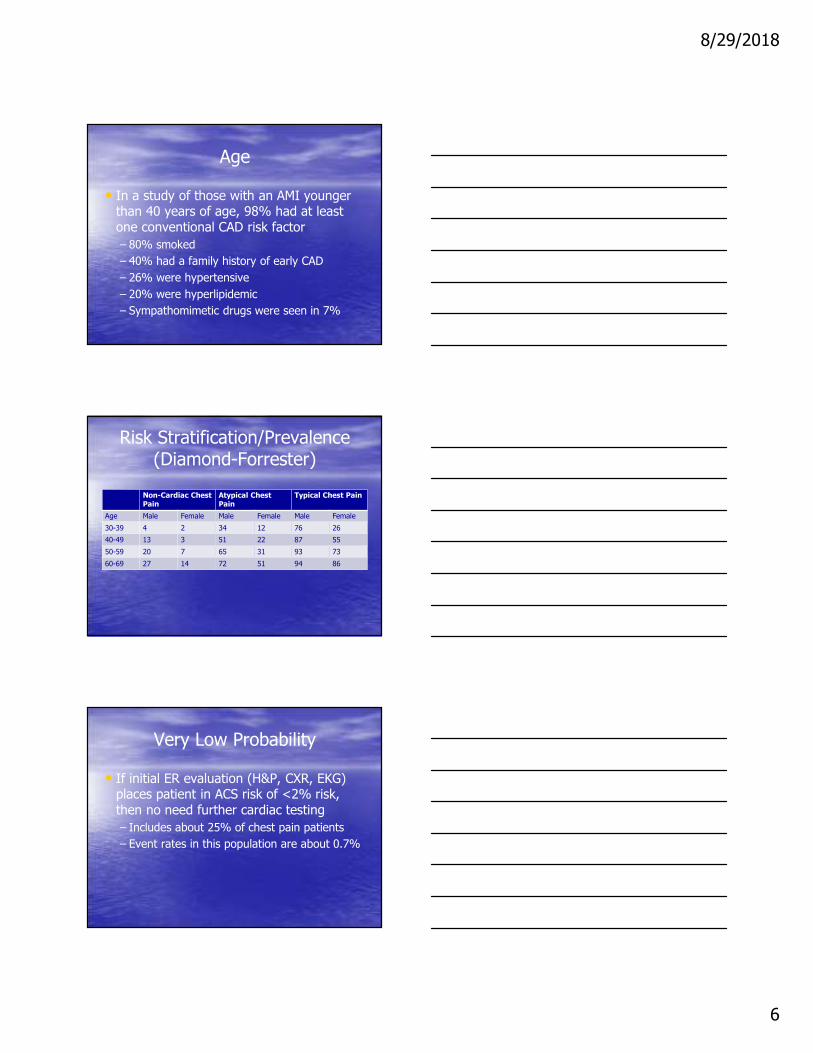
Age
• In a study of those with an AMI younger than 40 years of age, 98% had at least one conventional CAD risk factor
– 80% smoked
– 40% had a family history of early CAD
– 26% were hypertensive
– 20% were hyperlipidemic
– Sympathomimetic drugs were seen in 7%
Risk Stratification/Prevalence(Diamond-Forrester)
Non-Cardiac Chest Pain
Atypical Chest Pain
Typical Chest Pain
Age Male Female Male Female Male Female
30-39 4 2 34 12 76 26
40-49 13 3 51 22 87 55
50-59 20 7 65 31 93 73
60-69 27 14 72 51 94 86
Very Low Probability
• If initial ER evaluation (H&P, CXR, EKG) places patient in ACS risk of <2% risk, then no need further cardiac testing
– Includes about 25% of chest pain patients
– Event rates in this population are about 0.7%
8/29/2018
7
Risk Models
• Multiple models have been used for risk stratification
– TIMI
– GRACE
– PURSUIT
– FRISC
– HEART SCORE
HEART SCORE
• www.heartscore.nl
• http://annals.org/aim/article/2622872/effect-using-heart-score-patients-chest-pain-emergency-department-stepped
• Effect of Using the HEART Score in Patients With Chest Pain in the Emergency Department: A Stepped-Wedge, Cluster Randomized Trial. Poldervaart JM, et al. Ann Intern Med. 2017;166(10):689-697.
HEART SCORE
• Heart Score is now widely used for risk stratification and hence, disposition planning for ER patients
• Superior to TIMI and GRACE for risk stratification

8/29/2018
8
HEART SCORE
• Primary objective is disposition
A) URGENT REVASCULARIZATION
B) ADMIT TO OBSERVATION
C) DISCHARGE WITH OUTPATIENT FOLLOW-UP
HEART SCORE
• Primary objective is disposition
– Not the final word on whether or not the patient has CAD/Ischemia
– Some patients with symptomatic CAD will be discharged from ER and eventually undergo revascularization as outpatients
HEART SCORE
• Points are assigned based upon 5 categories
– 0, 1, or 2 points are assigned per category
– Sum of all components guides disposition

8/29/2018
9
HEART SCORE
• Categories:
–History
–EKG
–Age
–Risk Factors
–Troponin
H - HISTORY
• 0: Not Suspicious for Angina
• 1: Moderately Suspicious for Angina
• 2: Highly Suspicious for Angina
E - EKG
• 0: Normal EKG
• 1: Non-Specific Repolarization Abnormalities; LBBB; Paced Rhythm
• 2: Significant ST Deviation

8/29/2018
10
A - AGE
• 0: ≤ 45 Years Old
• 1: 45 – 65 Years Old
• 2: ≥ 65 Years Old
R – Risk Factors
• 0: No Risk Factors
• 1: One or Two Risk Factors
• 2: ≥ Three Risk Factors OR Known CAD
R – Risk Factors
Dyslipidemia Cigarette Smoking
Hypertension Family History of Early CAD
Diabetes Mellitus Obesity (BMI ≥ 30 kg/m2)

8/29/2018
11
T - Troponin
• 0: < Normal Limit
• 1: One to Three Times Normal Limit
• 2: ≥ Three Times Normal Limit
HEART SCORE
• Evaluates the six week risk of MACE following ER evaluation
• MACE includes:
– Myocardial Infarction
– PTCA
– CABG
– Death

8/29/2018
12
HEART SCORE - Prognosis
HEART SCORE - Disposition
SCORE Prevalence MACE/n MACE % Death Policy
0-3 32% 38/1993 1.9% 0.05% Discharge
4-6 51% 413/3136 13% 1.3% Observation. Risk Mgmt
7-10 17% 518/1045 50% 2.8% Early aggressive Mgmt
HEART SCORE
• US studies with over 2000 patients1,2
– > 99% sensitivity for 30-day events
– 30-40% of patients can be discharged safely without stress testing
.
1. Mahler, et al. Identifying patients…chest pain. Int J Cardiol. 2013 Sep;168(2):795-8022. Mahler, et al. The HEART...early discharge. Circ Cardiovasc Qual Outcomes. 2015 Mar;8(2):195-203
8/29/2018
13
HEART SCORE
• US studies with over 2000 patients1,2
– Decreased cardiac testing by 12%
– Time to discharge was decreased by 12 hours
– 21% increase in early discharge with no adverse events in this group
.
1. Mahler, et al. Identifying patients…chest pain. Int J Cardiol. 2013 Sep;168(2):795-8022. Mahler, et al. The HEART...early discharge. Circ Cardiovasc Qual Outcomes. 2015 Mar;8(2):195-203
Cardiac Biomarkers
• Multiple biomarkers used in past, these continue to evolve
• Sensitivity is most important, balance vs specificity
• Troponin is gold standard – multiple assays exist
Cardiac Biomarkers –Creatine Kinase
• Creatine Kinase (CK)
– Formerly Creatine Phosphokinase (CPK)
– Found in skeletal muscle
– Very non-specific for cardiac muscle injury
– Affected by total body muscle mass

8/29/2018
14
Cardiac Biomarkers –CK-MB
• CK-MB
– Significantly more specific for cardiac muscle injury, but also present in skeletal muscle
– Increase mildly delayed compared to Troponin and resolution within 48 hours
• Troponin detectable for up to 2 weeks
– Troponin has better prognostic significance
Cardiac Biomarkers –Myoglobin
• Myoglobin
– Also found in skeletal muscle
– Rises slightly before earlier Troponin assays
– With more sensitive contemporary Troponin testing, this is no longer the case
Cardiac Biomarkers –Copeptin
• Copeptin
– AVP precursor secreted by pituitary with AMI
– Very sensitive early in ACS
– Combined with Troponin in patients within 6 hours of CP onset, Negative Predictive Value of 99.2% for ACS1
– However, 1h hs-cTnT is superior to Copeptin with NPV up to 99.6%2
1. Maisel A., et al. Copeptin helps…CHOPIN Trial. J Am Coll Cardiol. 2013;62(2):150.2. Hillinger P, et al. Optimizing early…Copeptin. Clin Chem. 2015;61(12):1466

8/29/2018
15
Cardiac Biomarkers –Heart-Type Fatty Acid Binding Protein
• Heart-Type Fatty Acid Binding Protein
– Released very early in ACS
– Similar to myoglobin but more cardiospecific
– Strong association with prognosis1
– May be more sensitive at 2 hours than older but likely not newer Troponin assays
– Not well studied, not available in US
1. O’Donoghue M, et al. Prognostic utility…syndromes. Circulation. 2006;114(6):550.
Cardiac Biomarkers –Glycogen Phosphorylase BB
• Glycogen Phosphorylase BB
– Very sensitive early on in ACS
– Combined with hs-cTn, can achieve extremely high sensitivity but only 30-40% specific
– Likely not superior to current Troponin
1. Shortt C, et al. Comparison of cTnI…onset. Clinica Chimica Acta 419 (2013) 39-41.
Cardiac Biomarkers
• Lactate Dehydrogenase
– Sensitive but much less specific that Troponin
– Rises later (10 hours) after ACS
– No current clinical utility

8/29/2018
16
Compared to Troponin
SENSITIVITY SPECIFICITY
Creatine Kinase Worse Worse
CK-MB Worse Worse
Myoglobin Worse Worse
Copeptin Worse/?Similar Worse
HT-FABP Worse/?Similar Worse
Glycogen Phosphorylase BB Worse/?Similar Worse
LDH Worse Worse
Clinical Decision Making
Twin Patient A Twin Patient B
EKG Normal Normal
CP History Atypical Atypical
CK 1000 U/L (0-165 U/L) 50 U/L (0-165 U/L)
CK-MB 100 ng/mL (0.5-3.6 ng/mL) 1 ng/mL (0.5-3.6 ng/mL)
CK-MB Index 10 (0-4) 2 (0-4)
Myoglobin 250 (12-76 ng/mL) 25 (12-76 ng/mL)
Troponin I 0.02 (0.00-0.04 ng/mL) 0.02 (0.00-0.04 ng/mL)
Clinical Decision Making
• What to do with Twin A vs Twin B?
• With both having a normal Troponin, the elevated CK, CK-MB, and Myoglobin are basically irrelevant from an ischemic standpoint

8/29/2018
17
Why check biomarkers other than Troponin?
• “It is difficult to find any situation in which CK-MB adds anything other than cost to the clinical utility of cardiac troponin”
• “When cTn is available, CK-MB should not be used for the initial diagnosis of acute MI. If it is the only assay available, it can be used but is far less sensitive and specific”
� Alan Jaffe, et al. Up To Date
Cardiac Biomarkers
• Jim McCord, MD Challenge
• $100 to diagnose an MI with normal Troponin
Non-ACS Causes of Elevated Troponin (Type 2 NSTEMI)
Tachycardia Hypertensive Conditions
Critical Illness (Shock, Sepsis) Heart Failure
Myocarditis/Pericarditis Takotsubo Cardiomyopathy
Structural Heart Disease (AS) Aortic Dissection
Pulmonary Embolus/Pulm HTN Renal Dysfunction
Coronary Spasm CVA/SAH
Cardiac Contusion or Surgery/PCI Hyper- or Hypo-Thyroidism
Infiltrative Cardiomyopathy Myocardial Drug Toxicity
Extreme Endurance Activity Rhabdomyolysis
8/29/2018
18
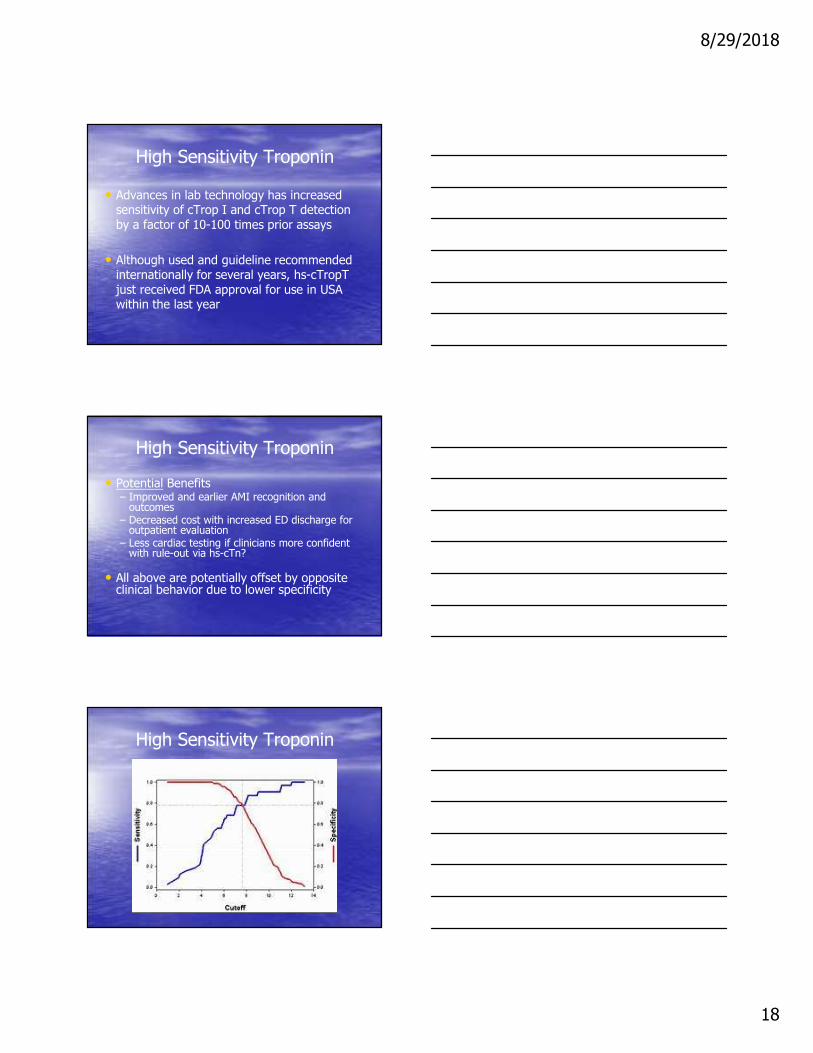
High Sensitivity Troponin
• Advances in lab technology has increased sensitivity of cTrop I and cTrop T detection by a factor of 10-100 times prior assays
• Although used and guideline recommended internationally for several years, hs-cTropTjust received FDA approval for use in USA within the last year
High Sensitivity Troponin
• Potential Benefits– Improved and earlier AMI recognition and
outcomes– Decreased cost with increased ED discharge for
outpatient evaluation– Less cardiac testing if clinicians more confident
with rule-out via hs-cTn?
• All above are potentially offset by opposite clinical behavior due to lower specificity
High Sensitivity Troponin

8/29/2018
19
High Sensitivity Troponin
High Sensitivity Troponin
• Compared with Standard Troponin Assays
– Higher NPV for Acute MI
– Reduce “Troponin-Blind” Period
• Abnormal earlier after ACS onset
– 4% absolute (and 20% relative) increase in detection of Type I MI
– 2-Fold increase in diagnosis of Type 2 MI
High Sensitivity Troponin
• A hs-cTnT value < 5 ng/L and a non-ischemic EKG have a 30-Day negative predictive value for MI and death of 99.8% and 100%1
1. Bandstein, et al. Undetectable…myocardial infarction. J Am Coll Cardiol. 2014;63(23):2569

8/29/2018
20
High Sensitivity Troponin
High Sensitivity Troponin
• The higher the level, the more likely an MI
• Expect typical rise & fall pattern with an MI
– Flat/stable elevation less likely due to ischemia
• Abnormal levels frequently present in healthy individuals (physiologic)
High Sensitivity Troponin
• Levels up to 3 X Upper Limit have only 50-60% PPV for Type I MI; often due to other causes
• Over 5 X Upper Limit has PPV > 90% for Type I MI
8/29/2018
21
High Sensitivity Troponin
• Australian study randomized standard Troponin with/without hs-TropT reporting
• No significant change in discharge, MI diagnosis, diagnostic testing, outcomes
• Normal standard Troponin subset had lower MACE at 1 year with hs-TropT reporting1
1. Chew DP, Zeitz C, Worthley M, et al. Randomized comparison of high-sensitivity troponin reporting in undifferentiated chest pain
assessment. Circ Cardiovasc Qual Outcomes. 2016
High Sensitivity Troponin
• Prior study highlights importance of proper utilization of this test data
– Protocols necessary to guide physician behavior to affect process and outcomes
– Concern that higher sensitivity could drive more unnecessary ischemic testing
High Sensitivity Troponin
• Debate remains whether or not to adjust reference values– Gender
– Age
– BMI
• Protocols being developed to evaluate “Delta” = percentage of change with serial tests to increase specificity

8/29/2018
22
ER Protocols
• The HEART Score by itself is very good at triaging patients for early discharge
• Protocols are underway looking at the additional benefit if high sensitivity Troponin
ER Protocols
• 0 hour/1hour protocol with hs-cTnT1
– Initial value and amount of change in 1 hour
• 1282 patients in ER with chest pain– 17% with MI
– 64% Ruled out
– 22% Triaged to Observation
– Negative Predictive Value 99.1%
– Sensitivity 96.7%
– PPV 77.2%, Specificity 96.1%1. Mueller C, et al. Multicenter Evaluation..Troponin T. Ann Emer Med. 2016 Jul;68(1):76-87.e4. doi: 10.1016/j.annemergmed.2015.11.013. Epub 2016 Jan 12.
ER Protocols
• In above study, 1 year mortality in the “Rule Out” group was <1%
• Compared well vs 2 hour or longer time for second Troponin
• Likely more effective than single absolute cut-off value if CP onset within the prior three hours

8/29/2018
23
ER Protocols
• Mueller’s protocol has been further refined by Twerendbold1 and a 0h/1h algorithm is now recommended in Europe
• This algorithm has recently been prospectively validated (for Trop T and I)
1. Twerendbold R, et al. Prospective Validation…Infarction. J Am Coll Cardiol. 2018;72:620-632.
ER Protocols
• 4368 Patients with suspected ACS
– High Sensitivity Troponin T at 0h/1h
• 57% Ruled Out vs 18% Ruled-In
ER Protocols
• For Rule Out with hs-cTnT:
– 0h Troponin < 12 ng/L
– 1h Troponin Change of < 3 mg/L
OR
– If Chest Pain > 3h, then 0h Troponin < 5 ng/L
8/29/2018
24
ER Protocols
• For Rule In with hs-cTnT:
– 0h Troponin ≥ 52 ng/L
– 1h Troponin Change of ≥ 5 mg/L
ER Protocols
• 5 NSTEMI’s found in the Rule Out group for Negative PV of 99.8%
• 30 Day Mortality in Rule Out group was only 0.1%, 1-Year Mortality 0.8%
ER Protocols
• Positive PV in the Rule In group was 74.5%
• 30-Day mortality in the Rule In group was 29X higher than in the Rule Out Group
• 16% were ruled out with a single test at 0h, NPV was 100% in this group

8/29/2018
25
ER Protocols
• Both Trop T and Trop I were very effective, with Trop T slightly better
• Protocol very effective in early presenters and across multiple co-morbidities, including ESRD
European Society of Cardiology Guidelines (2015)
• I-A: Measure Troponin with sensitive or high sensitive assay
• I-B: A rapid rule-out with hs-cTn at 0h and 3h is recommended
• I-B: A rapid rule-in and rule-out protocol at 0h and 1h is recommended if hs-cTntest with a validated 0h/1h algorithm is available
ER Protocols

8/29/2018
26
Summary
• Chest Pain is the second most common compliant in the ER, and it has a wide differential diagnosis
• It is usually benign, but exclusion of life-threatening possibilities needs to be performed in an effective, cost-efficient, and safe manner
• HEART Score and High Sensitivity Troponin are promptly becoming the standard of care for risk assessment and disposition planning