Chemotherapy-Induced Nausea and Vomiting. Update on Chemotherapy-Induced... · Update on...
39
Update on Chemotherapy- Induced Nausea and Vomiting (CINV): An Interprofessional Approach Stephanie Sutphin, PharmD, BCOP Hematology/Oncology Clinical Specialist University of Kentucky HealthCare Assistant Professor, Adjunct University of Kentucky College of Pharmacy
Transcript of Chemotherapy-Induced Nausea and Vomiting. Update on Chemotherapy-Induced... · Update on...

Update on Chemotherapy-Induced Nausea and Vomiting (CINV): An Interprofessional
Approach
Stephanie Sutphin, PharmD, BCOP
Hematology/Oncology Clinical Specialist
University of Kentucky HealthCare
Assistant Professor, Adjunct
University of Kentucky College of Pharmacy

Learning Objectives
Evaluate a patient’s chemotherapy regimen to determine the NCCN risk category for chemotherapy-induced nausea and vomiting (CINV) Develop a treatment plan for a patient receiving moderately emetogenic chemotherapy Discuss how multiple health care professionals can contribute to the care of a patient receiving chemotherapy in order to prevent and/or treat CINV


CINV Rates N = 322
Pts assessed
245 (76%) Nausea (N)
139 (43%) Acute N
126 (39%) Acute & Delayed N
234 (73%) Delayed N
96 (30%) Vomiting (V)
36 (11%) Acute V
21 (7%) Acute & Delayed V
81 (25%) Delayed V
Hickok, J.T., et al. Cancer 2003;97:2880-6
Cycle 1

Palonosetron Trial HEC
Time (h)
10
20
0
30
40
50
60
70
80
90
100
0 24 48 72 96 120
Palonosetron 0.25 mg (n=223) Palonosetron 0.75 mg (n=223) Ondansetron 32 mg (n=221)
P=NS for palonosetron 0.25 mg or 0.75 mg vs ondansetron.
Time to Treatment Failure = time to 1st emetic episode or use of rescue medication.
PALO-99-05 HEC
Time (h)
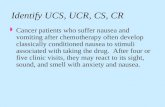
Palonosetron Trial MEC
10
20
0
30
40
50
60
70
80
90
100
0 24 48 72 96 120
Palonosetron 0.25 mg (n=189) Palonosetron 0.75 mg (n=189) Dolasetron 100 mg (n=191)
*P=0.017 for palonosetron 0.25 mg vs dolasetron. †P=0.025 for palonosetron 0.75 mg vs dolasetron.
†
*
Time to Treatment Failure = time to 1st emetic episode or use of rescue medication.
PALO-99-04 MEC

Is CINV still a problem?

Nausea
Unpleasant sensation, inclination to vomit (subjective) loss of gastric (stomach) tone & motility duodenal contractions reflux of intestinal contents into stomach cold sweat, salivation, tachycardia patient-scored (0-10) or visual analogue scale
(VAS)

Vomiting (Emesis)
Rapid, forceful evacuation of stomach contents out of mouth (involuntary) Abdominal/chest wall muscle contraction Objective quantification: how many episodes in 24 hours Often responds to medication emesis=retching + vomiting

Incidence of CINV
One of most common toxicities of chemotherapy >75 % of patients receiving combination therapy ↑ frequency & severity w/repetition Significant impact on quality of life (QOL) 15% will still have severe acute CINV despite optimal treatment Delayed CINV still poorly controlled
Abeloff 2004

Implications of CINV Quality of life – Fatigue, depression, anxiety – Degeneration of functional ability and self care – Decline in performance status and mental status
Compliance Nutritional status Dehydration Electrolyte imbalances Anorexia, weight loss Esophageal tears, fractures

Other Causes of Emesis in Cancer Patients
Bowel obstruction Vestibular dysfunction Brain mets Electrolytes: ↑Ca, ↑Glu, ↓Na Uremia Drugs Gastroparesis (drug or tumor) or other causes (diabetes) Psychophysiologic (anxiety or anticipatory) Radiation Treatment
Emetic Syndromes
Anticipatory Acute Delayed Breakthrough Refractory

Types of Nausea and Vomiting
Anticipatory Acute Delayed
Time
Chemo 24 hours

Goals of Therapy
Achieve complete control in all settings Maximum convenience to patient and staff Eliminate side effects Minimize the cost of treatment
DeVita 2005

Risk Factors
Chemotherapy drugs used – Emetogenic potential, dose, schedule
Patient Characteristics – Age (<50 years), gender (female), alcohol use
(chronic alcoholism decreases risk), prior control, motion sickness, pregnancy-induced nausea
Antiemetics – Dose, schedule, combination

Anticipatory Emesis
Triggers: sights, smells, sounds, memory, fear, anticipation Cause: inadequate control in past (cortex) Conditioned behavior Incidence: 18-57% Risks: treatment>6month
and/or history anxiety/depression Variable response to therapy

Anticipatory Treatment – Best therapy is prevention of emesis during
chemotherapy – Relaxation techniques shown to be effective – Acupunture/Acupressure – Benzodiazepines
Lorazepam or alprazolam usually beginning prior to chemotherapy or triggering event.

Emetogenic Risk of Chemotherapy
Based on % of patients that will get sick if given placebo
Minimal Risk < 10% Low Risk 10 - 30% Moderate Risk 30 - 90% High Risk > 90%

High Emetic Risk (>90%) AC (doxorubicin or epirubicin + cyclophosphamide) Carmustine > 250 mg/m2
Cisplatin Cyclophosphamide > 1,500 mg/m2 Dacarbazine Doxorubicin > 60mg/m2
Epirubicin > 90mg/m2
Ifosfamide > 2gm/m2
Mechlorethamine Streptozocin
NCCN @www.nccn.org v.1.2013
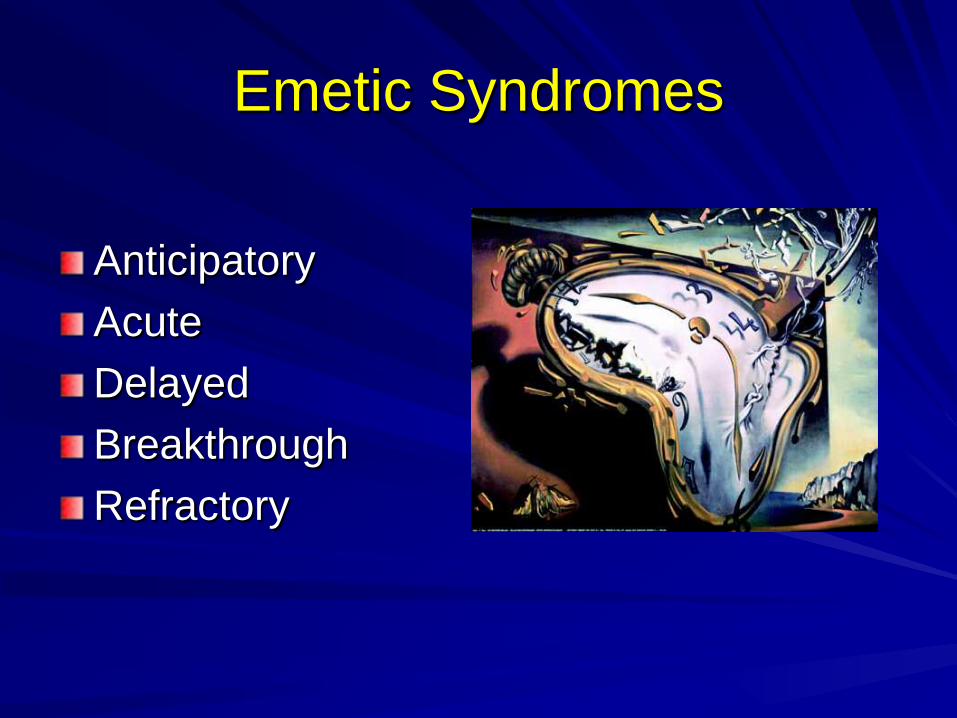
Moderate Emetic Risk (30-90%) Aldesleukin >12-15 mu/m2
Amifostine > 500 mg/m2
Arsenic trioxide Azacitadine Bendamustine Busulfan Carboplatin Carmustine ≤ 250 mg/m2 Clofarabine Cyclophosphamide <1500 mg/m2
Cytarabine > 200mg/m2
Dactinomycin Daunorubicin Doxorubicin < 60mg/m2
Epirubicin < 90mg/m2
Idarubicin Ifosfamide < 2gm/m2 Interferon alfa >10,000/m2
Irinotecan Melphalan Methotrexate > 250mg/m2
Oxaliplatin Temozolomide
NCCN @www.nccn.org v.1.2013
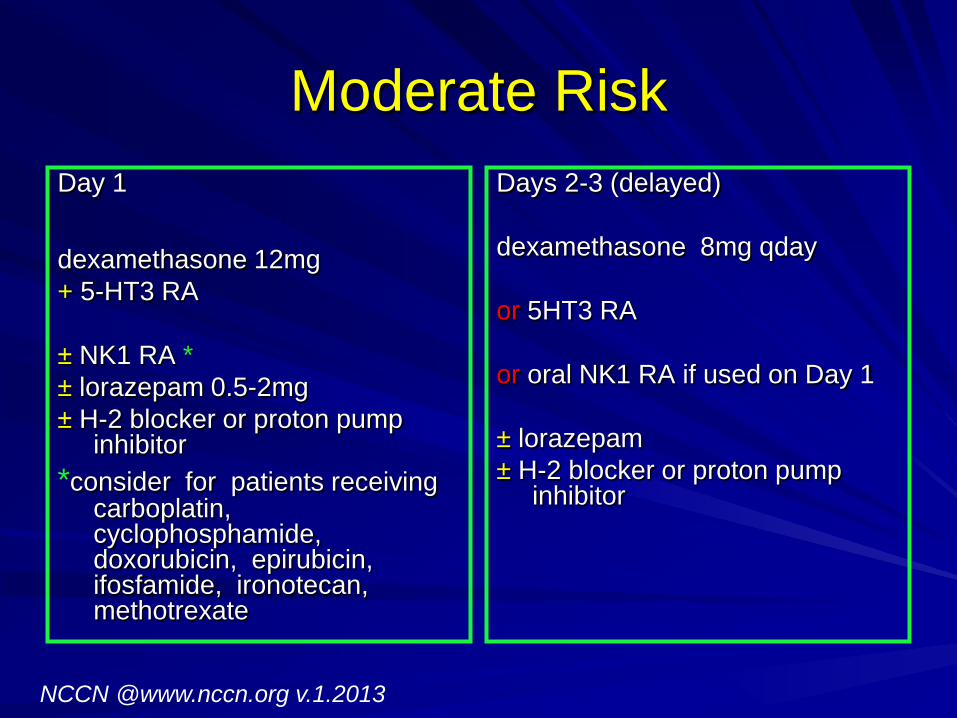
Moderate Risk Day 1 dexamethasone 12mg + 5-HT3 RA ± NK1 RA * ± lorazepam 0.5-2mg ± H-2 blocker or proton pump
inhibitor *consider for patients receiving
carboplatin, cyclophosphamide, doxorubicin, epirubicin, ifosfamide, ironotecan, methotrexate
Days 2-3 (delayed) dexamethasone 8mg qday or 5HT3 RA or oral NK1 RA if used on Day 1 ± lorazepam ± H-2 blocker or proton pump
inhibitor
NCCN @www.nccn.org v.1.2013
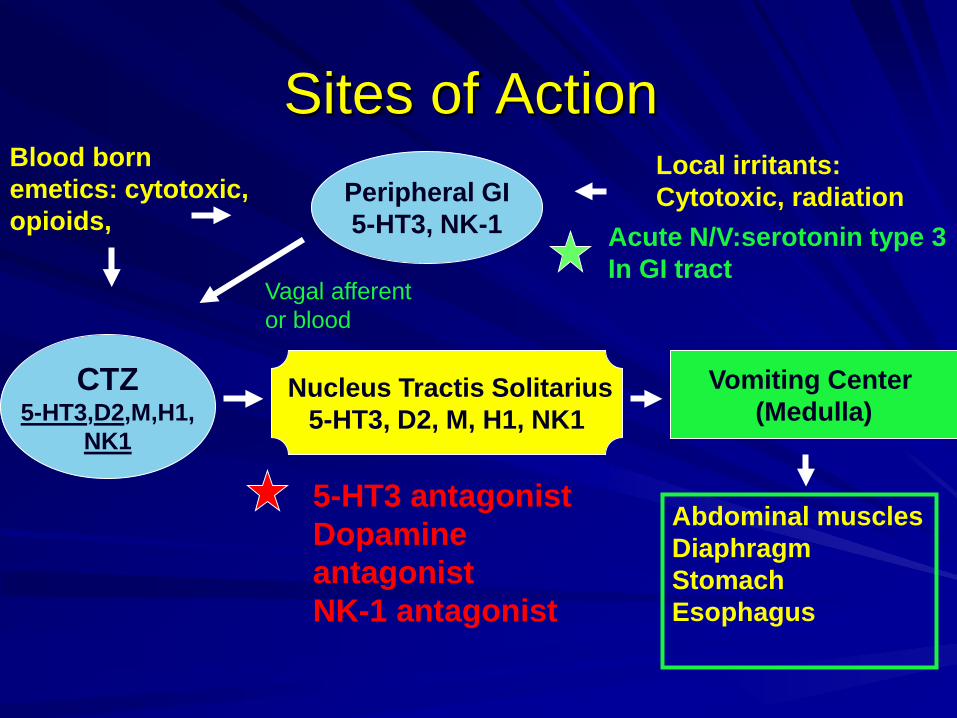
Sites of Action
CTZ 5-HT3,D2,M,H1,
NK1
5-HT3 antagonist Dopamine antagonist NK-1 antagonist
Blood born emetics: cytotoxic, opioids,
Nucleus Tractis Solitarius 5-HT3, D2, M, H1, NK1
Vomiting Center (Medulla)
Peripheral GI 5-HT3, NK-1
Local irritants: Cytotoxic, radiation
Acute N/V:serotonin type 3 In GI tract
Abdominal muscles Diaphragm Stomach Esophagus
Vagal afferent or blood
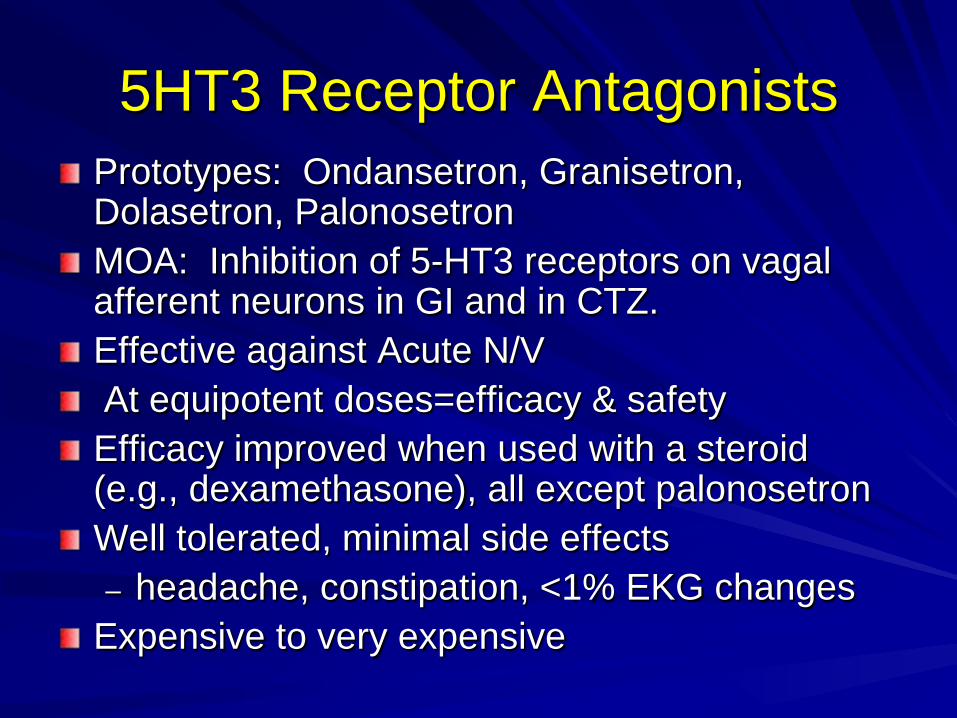
5HT3 Receptor Antagonists Prototypes: Ondansetron, Granisetron, Dolasetron, Palonosetron MOA: Inhibition of 5-HT3 receptors on vagal afferent neurons in GI and in CTZ. Effective against Acute N/V At equipotent doses=efficacy & safety Efficacy improved when used with a steroid (e.g., dexamethasone), all except palonosetron Well tolerated, minimal side effects – headache, constipation, <1% EKG changes
Expensive to very expensive

Serotonin and Chemotherapy
0
2
4
6
8
10
12
14
16
0 5 10 15 20 25 30Urin
ary
5HIA
A (n
ote
estim
ated
va
lues
)
Hours after cisplatin administration
Cubeddu, L.X. Oncology 1996;53(suppl 1):18-25

Recommended Doses of 5-HT3 RAs
AGENT ROUTE DOSE
Ondansetron IV 8-16mg (max 16mg)
Oral 16-24mg
Granisetron IV 10 mcg/kg (max 1mg)
Oral 2 mg or 1 mg BID
Transdermal 3.1mg/24hr patch
Dolasetron Oral 100 mg
Palonosetron IV 0.25mg x1

Neurokinin-1 Receptor Antagonists
NK-1 receptor mediates effects of substance P Substance P: tachykinin (or neurokinin) – emesis – depression – pain after inflammation – inflammatory/immune response in asthma
Micromedex 2013
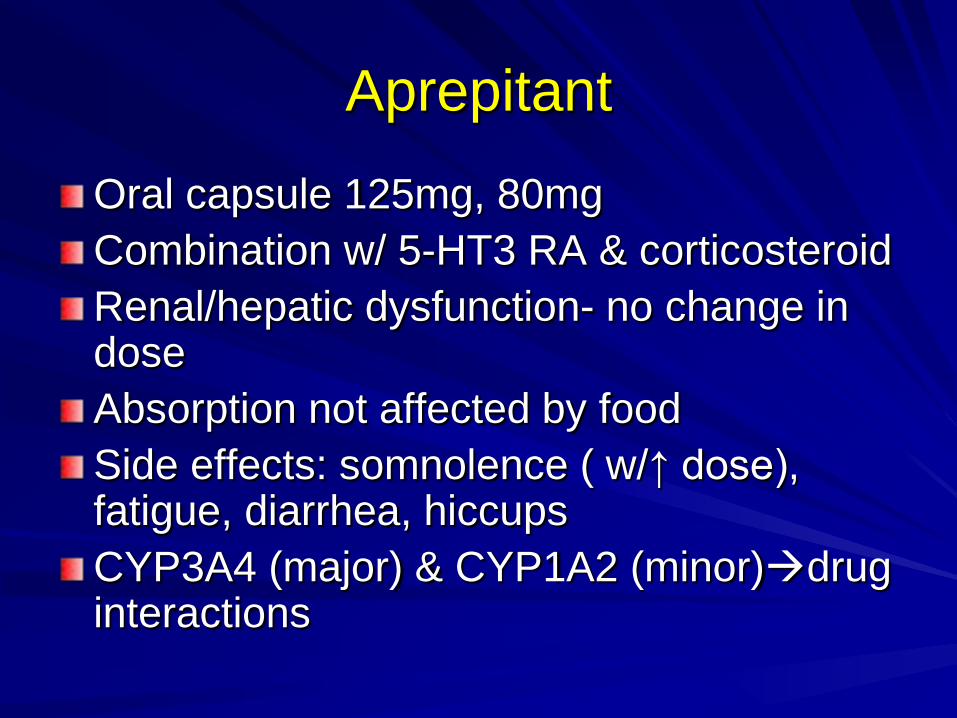
Aprepitant
Oral capsule 125mg, 80mg Combination w/ 5-HT3 RA & corticosteroid Renal/hepatic dysfunction- no change in dose Absorption not affected by food Side effects: somnolence ( w/↑ dose), fatigue, diarrhea, hiccups CYP3A4 (major) & CYP1A2 (minor)drug interactions

NK-1 RA Summary Monotherapy not as effective as 5HT3 receptor antagonists to prevent acute CINV Additive to 5HT3 receptor antagonists and dexamethasone to prevent acute CINV Superior to dexamethasone at preventing delayed CINV Aprepitant: 125mg PO day1, 80 mg PO days 2-3 Fosaprepitant: 150mg IV on Day 1 only
Corticosteroids
Dexamethasone – High emetic risk: 12mg – Moderate emetic risk: 8-12mg – Not as a single agent for high or moderate
risk Synergistic with 5-HT RAs and metoclopramide (↑efficacy by 20%) Mechanism of action: Unknown
Steroid Side Effects Side effects from single and short course therapy are infrequent Mood changes (euphoria, anxiety) Insomnia Increased appetite Hyperglycemia Mild fluid retention Intense, transient perineal, vaginal or anal burning with rapid IV administration

Phenothiazines
MOA: blocks dopamine receptors Examples: prochlorperazine, promethazine ADRs: sedation, hypotension, akathisia (lorazepam 1-2mg) & dystonia (diphen or benztropine) Effective w/moderately & mildly emetogenic Promethazine not as potent in cancer pts

Metoclopramide 1981: high dose metoclopramide ↓ emesis by 90% Antiemetic MOA – dopamine receptor blockade (low dose) – 5-HT3 receptor blockade (high dose) – Stimulates cholinergic activity in gut ↑ motility
1-2 mg/kg prior to chemo, then q4-6h; or 3mg/kg q2h x2 doses Side effects of high dose: dystonia or trismus (34%) – Diphenhydramine 25-50mg or benztropine 1-2 mg

Miscellaneous Antiemetics Butyrophenones (haloperidol & droperidol) – Block dopamine receptors
Benzodiazepines (lorazepam) – Little to no antiemetic activity alone – Anticipatory N/V (antegrade amnesia) & ↓ anxiety
Cannabinoids (dronabinol, nabilone) – Target cannabinoid receptors in central & peripheral
CNS, synthetic form of THC, side effects Belladonna alkaloid (scopolamine patch) – Block acetylcholine receptors in vestibular apparatus – Useful when N&V positional or due to motion

Breakthrough and Refractory
Breakthrough – Occurs despite prophylactic treatment and/or – Requires rescue with antiemetics
Refractory – Occurs during subsequent treatment cycles
when prophylaxis and/or rescue have failed in previous cycles

Breakthrough Give additional agent from a different class – Prochlorperazine 10mg q6h or Promethazine 12.5-25mg q4h – Dexamethasone 12mg daily – Metoclopramide 10-40 q4-6h ± diphenhydramine – Lorazepam 0.5-2mg q4-6h – Ondansetron 16mg PO or IV – Granisetron 1-2mg PO or 0.01mg/kg IV (max 1mg) – Dolasetron 100mg daily – Haloperidol 0.5-2 mg q4-6h – Dronabinol 5-10mg q3-6h or Nabilone 1-2mg bid – Olanzapine 10 mg daily for 3 days (use with caution in elderly
dementia patients: death, DM, hyperglycemia – Scopolamine patch every 72 hours
NCCN @www.nccn.org v.1.2013

Assessing Response
Primary Endpoint: – Complete Response = no emesis and no
rescue medication Secondary Endpoints: – Frequency of vomiting episodes – Use of rescue therapy – Nausea – Quality of life

Patient Counseling Important to inform patients regarding their chemotherapy regimens Discuss options Lifestyle measures (may need dietary consult) – Small, frequent meals – Control amount consumed – Eat food at room temp
Best treatment is prevention

Last Thoughts…
>1.6 million people in US diagnosed w/cancer in 2012 – KY: >25,000
>1 million people received chemotherapy Risks for N&V are both chemotherapy & patient specific Quality of life!