EPIDEMIC HEMORRHAGIC FEVER ( Hemorrhagic fever with renal syndrome )

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 95
Chemotherapy-induced hemorrhagic cystitis:
pathogenesis, pharmacological approaches and new insights
Ronaldo A. Ribeiro1,2
, Roberto C.P. Lima-Junior1, Caio Abner V.G. Leite
1,
Jose Mauricio S.C. Mota1, Francisco Y.B. Macedo
1, Marcos V.A. Lima
3, Gerly A.C. Brito
4
1Department of Physiology and Pharmacology, Faculty of Medicine, Federal University of Ceara;
2Department of Clinical Oncology, Haroldo Juacaba Hospital, Cancer Institute of Ceara;
3Department of Surgery, Haroldo Juacaba Hospital, Cancer Institute of Ceara;
4Department of Morphology, Faculty of Medicine, Federal University of Ceara; Fortaleza, Ceara, Brazil.
Abstract
Chemotherapy-induced hemorrhagic cystitis (HC) remains a common and life-
threatening clinical complication, mainly due to the increasing usage of alkylating agents during conditioning regimen for hematopoietic cell transplantation.
Currently, mesna and hyperhydration are the two more employed preventive measures.
However, these prophylactic approaches have been proven not to be completely effective, since cystoscopic and histopathologic bladder damage are evidenced. Therefore,
understanding the pathogenesis of HC must be the cornerstone for the development of
novel therapeutic strategies.
The purpose of this review is to examine the current knowledge regarding the
pathogenesis of HC, describing the importance of transcription factors (nuclear factor
kappaB), cytokines (tumor necrosis factor-α, interleukin-1β, -4, -6, and -8), enzymes (inducible nitric oxide synthase and cyclooxygenase-2), among other mediators, for the
bladder injury. We also discuss the currently available animal models and future
perspectives on the management of HC.
Key words:
Cancer; Chemotherapy;
Hemorrhagic cystitis; Pathogenesis
Correspondence:
R.A. Ribeiro / R.C.P. Lima-Junior Departamento de Fisiologia e
Farmacologia,
Faculdade de Medicina, Universidade Federal do Ceara,
Rua Cel Nunes de Melo, 1127,
Rodolfo Teofilo, 60430-270, Fortaleza, Ceara, Brazil.
[email protected] / [email protected]
Received: December 28, 2011
Accepted: January 11, 2012 Published online: March 8, 2012
J Exp Integr Med 2012; 2:95-112
DOI:10.5455/jeim.080312.ir.010
©2012 GESDAV. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License which
permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided that the work is properly cited.
Introduction Cystitis is a common clinical occurrence in
cancer patients. It can be separated into three broad
categories: cystitis consequent to bladder cancer or
adjacent cancers that encroach upon the bladder
from the prostate, uterus, cervix, or rectum;
infectious cystitis that occurs in immune-
compromised cancer patients; and chemotherapy-
or radiotherapy-induced cystitis [1].
Whatever the cause, patients often have
complaints typical of cystitis, which can be grouped
into a cluster of symptoms called “LUTS” (lower
urinary tract symptoms): dysuria, frequency,
urgency, nocturia, suprapubic pain, and
microscopic or gross hematuria [1].
In this context, hemorrhagic cystitis (HC) is
considered to be the most severe form in the
spectrum of the chemotherapy-induced bladder
injuries and is defined as the inflammation of the
urinary bladder leading to irritative LUTS up to
severe hemorrhage [1-3]. In patients with mild HC,
hematuria can cause iron deficiency anemia, but in
severe cases, it may lead to hemodynamic
instability due to hypovolemic shock. In addition to
the somatic symptoms, we hypothesize that HC
may also lead to a burden of suffering, depression,
limitations and a worse quality of life, although
there has been a complete absence of studies in this
area.
Although busulfan, adenovirus, BK virus,
cytomegalovirus, graft-versus-host disease and
radiation are causative factors of HC, it most often
occurs following chemotherapy, mainly after
regimens with oxazaphosphorines (cyclophos-
phamide or ifosfamide) [4]. Cyclophosphamide and
ifosfamide are alkylating agents with therapeutic
efficacies in multiple malignancies, including
testicular cancer, small-cell and non small-cell lung
cancer, soft tissue sarcoma, gynecological cancer,
bladder cancer, non-Hodgkin’s lymphoma, ad-
vanced breast cancer, and high-dose cyclophos-
phamide is often used as part of a conditioning
regimen for hematopoietic cell transplantation [5].
The incidence of HC is variable and appears to be
dependent on the type of treatment given. Before
the use of prophylactic regimens, HC occurred in
Invited
Review

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 96
10-40% of the patients exposed to high-dose
cyclophosphamide chemotherapy for solid tumors
[6] and up to 70% of patients following bone
marrow transplantation [7]. The incidence has been
reduced to 6-50% using prophylactic measures,
such as hyperhydration, bladder irrigation and
2-mercapto-ethane-sodium sulphonate (mesna)
[7-9]. Recently, Hadjibabaie et al performed a non-
randomized controlled clinical study and showed
that continuous bladder irrigation with mesna
treatment and hyperhydration can additionally
decrease the incidence of cyclophosphamide-
induced HC (by 32 to 50%) and its relative
complications in a conditioning regimen for allo-
geneic hematopoietic cell transplantation [10].
Despite the prophylactic approaches, HC remains
a common and life-threatening complication of
high-dose chemotherapy during bone marrow
transplantation, leading to prolonged hospitalization
[10, 11] and sometimes death [12]. It seems that the
standard preventive protocol does not completely
protect from the chemotherapy-induced bladder
injury, even when clinical signs and symptoms are
not reported. In a randomized controlled clinical
study of ifosfamide-based chemotherapy recipients,
we demonstrated that even with classical
prophylaxis with three doses of mesna, 66.7% of
patients presented with gross cystoscopic injuries,
and 100% had urothelial damage, such as edema,
exocytosis, and hemorrhage [13], possibly
revealing a novel concept of “subclinical
hemorrhagic cystitis.” It remains unknown if this
clinical occurrence may have any negative
consequences.
Thus, HC remains a clinical problem, and both
therapeutic and preventive measures have been
tested. Various therapeutic interventions are utilized
to produce hemostasis, such as continuous bladder
irrigation with isotonic saline, clot evacuation by
cystoscopy, electrocoagulation of bleeding vessels,
intravesical therapy with chemicals (formalin,
aluminum, phenol, silver nitrate, and prosta-
glandin), and hyperbaric oxygen therapy. In more
severe cases, the embolization or ligation of the
vesical [14] or internal iliac arteries, urinary
diversion, and cystectomy are used, although they
are usually reserved for refractory hemorrhage [15].
Therefore, understanding the pathogenesis of
oxazaphosphorine-induced HC must be the
cornerstone for the development of novel effective
preventive and therapeutic strategies. For that
reason, animal models of HC have been created
recently to aid in the studies of HC pathogenesis.
The most recent hypothesis implicates a number of
transcription factors, cytokines, and inducible
enzymes. This review will describe in detail the
ultimate mediators and pathways involved in the
generation of HC and will also discuss the currently
available animal models and future perspectives on
the management of HC.
Animal models for understanding HC
pathogenesis
Animal models have been developed to focus on
the morphological changes in the bladder and on
the pathogenic processes involved. The choice of an
animal model depends on various factors, such as
the accessibility to the animal, cost, administration
route, and the question under investigation. In
summary, there are two major models of
oxazaphosphorine-induced HC in rats or mice: the
systemic injections of cyclophosphamide or
ifosfamide and the intravesical injections of
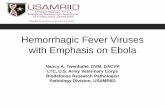
acrolein (Fig.1).
Figure 1. Experimental hemorrhagic cystitis.
Routes of administration commonly used for the induction of experimental hemorrhagic cystitis.
(a) intravesical injection of acrolein;
(b) intraperitoneal injection of cyclophosphamide or ifosfamide;
(c) normal bladder;
(d) bladder presenting hemorrhagic cystitis;
(e) histopathologic aspect of
(e) normal
and (f) injured bladder.

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 97
Cyclophosphamide-induced HC
Experimental cyclophosphamide-induced bladder
damage has previously been shown in rats, dogs
[16] and mice [17]. However, the first rat model
was generated by Tolley and Castro in 1975 [18].
The animals received cyclophosphamide by
intraperitoneal or intravenous injections (50, 100,
150, 200 and 250 mg/kg). At different times
thereafter (from 2 h to 16 days), the animals were
killed, and their bladders were removed and
analyzed by histopathology. In this system, HC
occurred in a dose-dependent manner and was
measured by bladder wall edema, polymorpho-
nuclear infiltration and submucosal hemorrhage,
mainly identified 8 h following a single intravenous
injection of 100 mg/kg [18]. Furthermore, Gray et
al defined a system for the score evaluation of
macroscopic edema and bleeding and for histo-
logical changes [19]. Souza-Filho et al assessed
bladder edema by measuring the bladder wet
weight and vascular permeability by Evans blue
extravasation, with greater damage occurring 24 h
after the cyclophosphamide injection [20].
Ifosfamide-induced HC
Based on the evidence that HC is observed more
often in patients receiving ifosfamide than in those
receiving cyclophosphamide [21], our group
developed a model to study the ifosfamide-induced
HC in Swiss mice [22]. HC was induced by the
intraperitoneal injection of 100, 200 and 400 mg/kg
ifosfamide. At various times thereafter (6, 12, 24,
36 and 48 h), the animals were euthanized, and
their bladders were removed, emptied of urine and
evaluated for vesical edema (bladder wet weight),
macroscopic and microscopic Gray’s criteria [19].
Ifosfamide-induced vesical edema was greatest at
12 h after ifosfamide administration. The
microscopic analysis revealed vascular congestion,
edema, hemorrhage, fibrin deposition, neutrophil
infiltration, and epithelial denudation [22]. In a
similar study with rats, our group induced HC with
an intraperitoneal injection of 400 mg/kg
ifosfamide, and the bladders were removed 24 h
later [23].
Acrolein-induced HC
In 1985, Chaviano et al administered acrolein
into rat bladders and observed HC similar to that
found with cyclophosphamide injected
intraperitoneally [24]. Conversely, our group
showed for the first time a mouse model of
acrolein-induced HC using a pharmacological dose-
response curve (25, 75 and 225 μg/bladder) [25].
This work showed that the intravesical
administration of acrolein induced a dose- and
time-dependent (3, 6, 12, 24 h) increase in the
vascular permeability and bladder wet weight as
confirmed by histopathological Gray’s criteria, and
pretreatment with mesna inhibited all the changes
induced by acrolein [25]. The injury was greatest at
12 h. This model has a potential advantage over the
systemic administration of cyclophosphamide or
ifosfamide because it does not require the hepatic
metabolism to acrolein and could be a simple and
useful model for the evaluation of HC pathogenesis
and new uroprotective drugs.
Hemorrhagic cystitis pathogenesis
For a long time, the mechanisms involved in the
pathogenesis of HC were largely unknown and
were a matter of considerable interest for
researchers. Over the last two decades, several
studies have tried to elucidate these pathways. Most
of the published articles concentrated on the
cyclophosphamide-induced injury, and only a few
are related to ifosfamide; however, the underlying
mechanisms seem to be equivalent.
The first description of symptomatic bladder
damage with macro- and microscopic hematuria
after cyclophosphamide administration was
described shortly after its introduction as an
antineoplastic agent in 1958 [26, 27]. In addition,
cyclophosphamide was shown to induce bladder
lesions in rats and dogs [16].
Early studies focused on implicating the
alkylating agent itself. However, Philips et al
demonstrated that the effects were caused by the
metabolic products excreted into the urine [16].
They also found that the urine from the dogs treated
with cyclophosphamide could reproduce cystitis
when transplanted into the bladder of control dogs
[16]. Ten years later, acrolein was characterized as
a component present in the urine after cyclophos-
phamide metabolism [28]. In 1979, subsequent
work by Cox definitively identified acrolein as the
causative agent of HC lesions [29].
Another important hallmark was the first clinical
description of the preventive use of mesna in the
late 1970s [30]. Despite this knowledge, the first
demonstration of the involvement of pro-
inflammatory mediators, such as cytokines and
nitric oxide (NO), in the pathogenesis of
oxazaphosphorine-induced HC was described more
than fifteen years later by our group [20, 31]. Since
then, remarkable progress has been made.
Based on the current information on the
pathophysiology of HC and taking into account the
four-stage model proposed by Sonis for alimentary

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 98
tract mucositis [32], we suggest a four-stage model
to describe the phases involved in HC (Fig.2). The
first stage (initiation phase) occurs after acrolein
accumulates in the bladder, leading to urothelial
damage. The following stage (inflammatory phase)
is marked by the up-regulation of transcription
factors, such as nuclear factor kappaB (NF-κB)
[33, 34], and the local release of inflammatory
cytokines by the epithelial and conjunctive resident
cells, such as macrophages [22, 31]. The amplified
response is marked by large amounts of cytokines,
reactive oxygen species and the expression of
inflammatory enzymes, such as the inducible nitric
oxide synthase (iNOS) isoform and
cyclooxygenase-2 (COX-2) [20, 22, 31, 35-37]. The
combination of NO and superoxide radicals can
lead to the production of the over-reactive free
radical peroxynitrite [38]. The third stage
(symptomatic phase) involves the urothelial
denudation and ulcer formation, also leading to
visceral pain and bladder dysfunction [39]. The
fourth stage (healing phase) involves the tissue
repair with possible signaling from the fibroblasts
and the local release of growth factors, such as
keratinocyte growth factor [40]. In the following
sections, we attempt to describe the main
pathological aspects of chemotherapy-induced HC.
Figure 2. Proposed sequential phases of the development of
hemorrhagic cystitis.
The role of transcription factors and
inflammatory mediators in the pathogenesis of
hemorrhagic cystitis
Along with other groups, our laboratory has
investigated the role of inflammatory mediators in
the pathogenesis of alkylating agent-induced HC.
Beginning with the demonstration of the
participation of tumor necrosis factor-α (TNF-α)
and interleukin-1β (IL-1β) [31] and through the
latest studies, the involvement of several cytokines
and other inflammatory mediators has been
suggested [20, 22, 35-39, 41-43]. Each of these
mediators can be up-regulated by the activation of
the NF-κB pathway in response to inflammatory
damage, which makes this transcription factor a
possible target for the prevention of chemotherapy-
induced HC [44].
Nuclear factor kappaB
The transcription factor NF-κB is one of the key
regulators of the genes involved in the immune and
inflammatory response [45]. Under most
circumstances, NF-κB homodimers or heterodimers
are bound to IκB inhibitory proteins in the
cytoplasm of unstimulated cells. Many cytokines
promote the classical NF-κB pathway, in which the
serine phosphorylation and degradation of the IκB
proteins leads to the dissociation of the inactive
cytosolic NF-κB/IκB complexes and the subsequent
NF-κB translocation to the nucleus for DNA
binding. Upon translocation to the nucleus, the
NF-κB dimer binds to the promoters of the NF-κB-
dependent genes and facilitates their transcription
[46]. NF-κB induces the expression of the cytokines
TNF-α and IL-1β, the acute phase proteins iNOS
and COX-2, and adhesion molecules [34]. The
inappropriate activation of NF-κB can lead to
diseases, such as HC.
The first experimental evidence for the role of
NF-κB in the pathogenesis of HC was assessed by
Kiuchi and co-workers [34] through the use of a
potent NF-κB inhibitor, parthenolide [47]. These
authors clearly showed by western blotting that
parthenolide prevents the phosphorylation of
NF-κB p65 and also blocks IκBα
phosphorylation/degradation and NF-κB nuclear
translocation [34]. They also demonstrated that
parthenolide causes the marked inhibition of
COX-2 expression in the bladders of cyclophos-
phamide-treated animals and inflammatory
urothelial cells. These in vitro and in vivo anti-
inflammatory effects of parthenolide were
suggested to be dependent on the inhibition of
NF-κB activity. NF-κB activity in the cyclophos-

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 99
phamide-treated animals contributes to the
activation of downstream inflammatory genes,
leading to bladder hyperactivity and HC [34].
Tumor necrosis factor-α
TNF-α regulates a number of cell functions,
including cell proliferation, survival, differen-
tiation, and apoptosis. TNF-α has been shown to
play a pivotal role in orchestrating the cytokine
cascade in many inflammatory diseases. Because of
this role as a key regulator of inflammatory
cytokine production, it has been proposed as a
therapeutic target for a number of diseases [48].
Aberrant TNF-α production and TNF receptor
signaling have been associated with the
pathogenesis of several diseases, including
rheumatoid arthritis, psoriasis [49], Crohn’s disease
[50], sepsis [51] and diabetes [52]. The receptors
for TNF-α are either constitutively expressed in
most mammalian tissues (TNF-R1) or are highly
regulated and expressed in the cells of the immune
system [53]. TNF, through its interaction with
TNF-R1, causes various cellular events, including
the activation of the caspase cascade that leads to
apoptosis. The interaction between TNF and
TNF-R1 also leads to the activation of NF-κB.
TNF-R2 is known not to possess a death domain
and therefore cannot directly cause apoptosis [53].
Depending on the cell type, TNF-R1 and TNF-R2
may have both distinct and overlapping roles in
signal transduction and gene expression [48].
The role of TNF-α in the inflammatory cascade
of HC was previously investigated by Gomes et al
[31]. These authors clearly demonstrated that anti-
TNF-α serum inhibits the histopathologic
parameters of cyclophosphamide-induced tissue
damage, such as mucosal erosion, hemorrhage,
edema, leukocyte migration, fibrin deposition and
ulcerations. The gains in both the bladder wet
weight and vascular permeability were prevented in
the anti-TNF-α serum-treated mice. These results
are supported by the fact that thalidomide, which
has been reported to inhibit the production of
TNF-α by increasing its mRNA degradation [54],
also prevented the ifosfamide-induced bladder
injury [22]. Therefore, considering that anti-TNF-α
therapy has been shown to effectively manage
several malignances [55-58], clinical trials are
needed to investigate the efficacy of specific TNF-
modulating agents to treat HC.
Interleukin-1β
IL-1β is a highly inflammatory cytokine that
affects nearly every cell type and often works in
concert with other cytokines or small mediator
molecules. The IL-1 receptor family (IL-1R)
includes coreceptors, decoy receptors, binding
proteins, and inhibitory receptors [59]. IL-1β
interacts with two IL-1 receptors, type I (IL-1RI),
which transduces cell signaling, and type II
(IL-1RII), which lacks the signaling-competent
cytosolic domain and is a decoy receptor [60, 61].
The extracellular IL-1 receptor chains, also known
as soluble IL-1RI (sIL-1RI), sIL-1RII, and
sIL-1RAcP, are inducible negative regulators of
IL-1β signaling in the extracellular space [61].
IL-1β first binds to the ligand-binding chain,
IL-1RI, and then the coreceptor chain, termed the
accessory protein (IL-1RAcP), is recruited. The
signal is initiated with the recruitment of the
adaptor protein MyD88 to the Toll-IL-1 receptor
(TIR) domain [62]. Subsequently, several kinases
are phosphorylated, NF-κB translocates to the
nucleus, and several inflammatory genes are
expressed [62].
IL-1β is a pivotal pro-inflammatory cytokine
implicated in the pathogenesis of stroke, diabetes
and rheumatoid arthritis [62, 63]. Agents that
reduce the production and/or activity of IL-1 are
likely to impact the clinical management of
pathologies such as HC.
Gomes et al evaluated the effect of anti-IL-1β
serum on the animal model of hemorrhagic cystitis
[31]. This modulating approach was beneficial
against the cyclophosphamide-induced bladder
damage and vesical wet weight gain but to a milder
degree than the anti-TNF serum. In addition,
pentoxifylline exerts multiple beneficial immune-
modulatory effects by down-regulating IL-1β and
TNF-α synthesis, decreasing interferon-γ (IFN-γ),
granulocyte-macrophage colony-stimulating factor
and IL-6 secretion, and attenuating the cell surface
expression of the IL-2 receptor [64] and was also
shown to inhibit the vesical edema and microscopic
alterations induced by ifosfamide administration
[22]. In fact, IL-1β is highly expressed in the
epithelial and subepithelial bladder cells of the
ifosfamide-injected mice as demonstrated by
immunohistochemistry [43].
Considering the ability of IL-1β to orchestrate the
inflammatory process and the protective effect
achieved by its inhibition, the selective inhibition of
IL-1 function could also present interesting clinical
outcomes.
Interleukin-4
IL-4 is a cytokine that acts as an anti-
inflammatory compound under certain conditions
and is therefore responsible for the homeostasis of

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 100
the immune system. It has a marked inhibitory
effect on the expression and release of pro-
inflammatory mediators, such as the monocyte-
derived cytokines TNF-α and IL-1β [65] and a
modulating effect on the expression of IL-1
receptor antagonist (IL-1ra) [66]. In addition to the
inhibition of the production of inflammatory
cytokines, IL-4 has been reported to inhibit the
induction of COX-2, with a consequent reduction in
the production of prostaglandins [67].
Macedo et al explored the anti-inflammatory
potential of IL-4 in the model of ifosfamide-
induced HC [43]. Interestingly, IL-4 production is
enhanced after ifosfamide administration. However,
the administration of exogenous IL-4 inhibits
inflammatory parameters, such as the expression of
pro-inflammatory cytokines (TNF-α and IL-1β) and
enzymes (iNOS and COX-2) [43]. In addition, it
was demonstrated that both IL-4 antiserum-treated
and genetically deficient mice have exacerbated
HC.
Interleukin-6 and interleukin-8
IL-6 is a member of a cytokine family sharing a
common signal transducer (gp130), which also
includes IL-11, IL-27, IL-31, leukemia inhibitory
factor, ciliary neurotrophic factor and
cardiotrophin-1 [68]. Some studies have reported an
increased local expression of IL-6 in the bladder or
in the serum after cyclophosphamide challenge
[69-71]. Nishii et al [69] showed that IL-6 gene
expression is significantly up-regulated in the
submucosal layer of the bladder after
cyclophosphamide administration in mice, peaking
at 6 h and declining thereafter. In addition, Girard
et al also showed that IL-6, IL-6 receptor α subunit
(IL-6Rα) and gp130 (β subunit) are highly
expressed in the urothelium and detrusor following
cyclophosphamide treatment [71]. In contrast, IL-8
expression and its role in HC have never been
investigated. IL-8 is a critical chemo-attractant
responsible for leukocyte recruitment, cancer
proliferation, and angiogenesis [72]. IL-8 has been
implicated in the pathogenesis of diseases,
including acute lung injury and acute respiratory
distress syndrome [73], osteoarthritis [74] and
cystic fibrosis [75].
We showed that IL-6 and IL-8 are involved in the
pathogenesis of HC. Mice intraperitoneally injected
with 200 mg/kg cyclophosphamide had significant
increases in bladder wet weight and vascular
permeability when compared to the saline-treated
group. Furthermore, treatment with anti-IL-6 and
anti-IL-8 sera (25 or 50 uL/animal) before the
cyclophosphamide injection markedly prevented
the development of edema (unpublished data).
As far as we know, this is the first report of an
experimental modulation of IL-6 and IL-8 and the
pathological contribution of these cytokines to the
cyclophosphamide-induced edema in HC. Further
studies are needed to precisely define the role of
these mediators in the inflammatory cascade
involved in this pathology.
Bradykinin
Bradykinin and its homologues, known
collectively as kinins, are produced by the action of
kallikrein enzymes [76]. The kinins are blood-
derived, local-acting peptides that have broad
effects mediated by two related G-protein-coupled
receptors, the B1 and B2 bradykinin receptors. The
endogenous kallikrein-kinin system controls blood
circulation and kidney function and promotes
inflammation and pain in pathological conditions
[77], including sepsis and cancer [78].
Maggi and co-workers demonstrated the
participation of bradykinin via B2 receptors in the
genesis of detrusor hyperreflexia during cyclophos-
phamide-induced cystitis [79]. In addition, a study
published by Chopra and colleagues showed that
the B2 receptor, but not the B1 receptor, is
expressed in the urothelium and detrusor smooth
muscle of bladders from control animals [80].
However, the expression of B1 receptors is highly
increased during cyclophosphamide-induced HC.
Convincingly, these authors demonstrated that the
urothelial expression of bradykinin receptors is
plastic and altered by pathology, indicating a role of
both bradykinin receptors in the cyclophosphamide-
induced bladder hyperactivity via the extracellular
release of urothelial-derived factors, such as ATP,
which act on the pelvic nerve afferents [80].
The participation of the B2 receptors in
cyclophosphamide-induced bladder edema
formation was also investigated. Rats had a
significant increase in their bladder wet weight and
vascular permeability 48 h after the administration
of cyclophosphamide (100 mg/kg) when compared
to the saline-treated group. Animals pre-treated
with Hoe-140 (2 mg/kg), a B2 receptor antagonist,
plus cyclophosphamide markedly ameliorated both
the vesical wet weight and vascular permeability in
comparison with the cyclophosphamide-injected
rats (unpublished data).
Despite the knowledge concerning the
inflammatory importance of bradykinin, only one
bradykinin receptor antagonist, icatibant (Hoe-140),

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 101
has reached the market for the treatment of
hereditary angioedema [81].
Cyclooxygenases
COX is a group of bifunctional enzymes that
have both cyclooxygenase and peroxidase
activities. COXs catalyze the complex conversion
of arachidonic acid to prostaglandins and
thromboxanes, which act as autacoids with
autocrine and paracrine biological effects to trigger
many physiological and pathophysiological
responses [82, 83]. Three isoforms of COX have
been described to date: COX-1, -2, and -3. COX-2
is an isoform whose expression is commonly up-
regulated during inflammatory processes. It plays
an important role in pain [84], tumor activation
[83], inflammation and neurodegenerative diseases
[85]. The expression of COX-2 was already
demonstrated during cyclophosphamide- [86],
ifosfamide-[36] and acrolein- [37] induced HC.
Our group assessed the role of COX-2 on the
pathogenesis of ifosfamide-related HC with a
selective inhibitor of COX-2, etoricoxib, and a non-
selective inhibitor, indomethacin. We observed that
COX-2 is highly expressed 24 h after a single
injection of ifosfamide to induce HC mainly in
myofibroblasts and, to a lesser extent, in mast cells
[36].
Hu et al also provided evidence for COX-2
mRNA expression due to cyclophosphamide
injection [86]. The demonstration that COX-2 is
observed a few hours after the induction of HC
suggests the participation of other mediators in the
first hours following ifosfamide administration
[20, 22]. We verified this hypothesis by the use of
non-selective cytokine inhibitors, thalidomide and
pentoxifylline [36]. It was shown that these agents
prevent some of the inflammatory parameters when
compared to the groups treated only with
ifosfamide, which is in accordance with the data
published by Ribeiro et al [22]. In addition, a lower
expression of COX-2 was observed when the
animals were given thalidomide and pentoxifylline
before ifosfamide administration, which supports a
role for cytokines on COX-2 expression in this
animal model of HC [26].
It is known that HC can arise as a complication of
both cyclophosphamide and ifosfamide treatment
and that it is caused by the urinary metabolite
acrolein. Our group showed in mice that acrolein
can cause severe edema and hemorrhage, similar to
cyclophosphamide and ifosfamide [25].
In another study published by our group, acrolein
injected into the rat bladder induced a dose- and
time-dependent HC, and the resulting lesion is
partially mediated by the increased expression of
COX-2 [37]. However, this study also showed that
even 3 and 6 h after the acrolein instillation into the
bladder, COX-2 expression is almost absent,
despite the presence of severe edema and
hemorrhage.
Macedo et al reported that these observations
suggest the participation of other inflammatory
mediators in the changes observed within the first
hours of acrolein-induced HC [37], as demonstrated
previously for ifosfamide- and cyclophosphamide-
induced HC [22, 31]. Macedo et al showed that
between 3 and 6 h, there is not sufficient expression
of the COX-2 enzyme to affect the increase of
bladder wet weight in animals injected with
acrolein [37]. The anti-inflammatory effect of
etoricoxib was only detected 12 h post-acrolein
injection.
Hu et al demonstrated that conscious cystometry
in rats injected with cyclophosphamide and the
COX-2 inhibitor 5,5-dimethyl-3-(3-fluorophenyl)-
4-(4-methylsulfonyl)phenyl2(5H)-furanone (DFU)
showed increased micturition intervals 4 and 48 h
after cyclophosphamide treatment and decreased
intravesical pressures during filling and micturition
compared with rats administered cyclophosphamide
[86]. This finding clearly suggested an involvement
of the urinary bladder COX-2 and its metabolites in
the altered micturition reflexes during cyclophos-
phamide-induced cystitis.
Additionally, a very recent article published by
our group showed that the HC experimentally
induced by ifosfamide promotes detrimental
changes in the motor functions of the rat lower
urinary tract, interferes with the urinary bladder
emptying process in anesthetized rats, and alters the
contractile behavior as assessed by in vitro methods
[39]. We also suggested that this phenomenon
involves the inflammatory events mediated by the
COX-2 expression within the urinary bladder with a
consequent rise in the plasma levels of PGE2 [39].
In addition, the selective pharmacological inhibition
of COX-2 activity partially ameliorated these
functional changes. We concluded that the
prevention of the inflammatory process ameliorates
the consequences of the ifosfamide-induced cystitis.
Maggi [87] reviewed the role of prostanoids, such
as PGE2, as activators of bladder afferents, which
changes the micturition reflex threshold. The
mechanism of PGE2-induced normal bladder
hyperactivity was investigated by Ishizuka and
colleagues [88], who showed that intravesical
PGE2 might stimulate micturition by releasing

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 102
tachykinins from the nerves in and/or immediately
below the urothelium. These tachykinins, in turn,
initiate a micturition reflex by stimulating the NK1
and NK2 receptors, contributing to both urge and
the bladder hyperactivity observed in the
inflammatory conditions of the lower urinary tract.
However, the precise mechanisms involved in the
detrimental effects of ifosfamide in HC deserve
further investigation. Possible explanations involve
the modification of the synaptic mechanisms in the
urinary bladder, e.g., those related to the muscarinic
receptor response to agonists, which still needs to
be proven.
Nitric oxide
NO is synthesized by a family of enzymes known
as nitric oxide synthases (NOSs). Three distinct
isoforms of NOS, namely endothelial nitric oxide
synthase (eNOS), neuronal nitric oxide synthase
(nNOS) and inducible nitric oxide synthase (iNOS),
have been described based on the cells in which
they were first identified, isolated, purified, and
cloned [89]. Over the past two decades, NO has
gained increasing recognition as an important
neurotransmitter and cell mediator with a broad
range of functions in the lower urinary tract.
A convincing first report on the participation of
NO in the pathogenesis of chemotherapy-induced
HC was published by our group [20]. This study
showed that the injection of cyclophosphamide
increases iNOS activity. Additionally, two NOS
inhibitors, L-NAME and L-NOARG, dose-
dependently inhibited the cyclophosphamide-
induced plasma protein extravasation and bladder
wet weight, which was reversed by L-arginine, a
NO precursor. Such inhibitory actions on NOS
activation critically prevented bladder damage, as
shown both macroscopically and microscopically
by the reduced mucosal damage. Another study
performed by Oter and colleagues evaluated the
role of iNOS-derived NO on bladder injury due to
cyclophosphamide injection [35]. In that study, the
administration of S-methylisothiourea, a selective
iNOS inhibitor, led to similar results as those
previously reported.
We also investigated the role of constitutive NOS
enzymes and found that NOS activity in the normal
bladder was mainly due to the cNOS (calcium-
dependent) isoform (>95%). Cyclophosphamide
administration significantly increased the calcium-
independent activity of iNOS, which was evident
6 h after the injection and remained elevated for up
to 48 h. In contrast, cNOS decreased over a similar
time course in the presence of cyclophosphamide
[20]. Consistent with these findings, nicotinamide
adenine dinucleotide phosphate diaphorase
(NADPH-d), a marker for NOS-containing cells,
was expressed in the urothelium and in the lamina
propria of control rats. This expression decreased
dramatically 12 h following cyclophosphamide
administration and coincided with an intense
sloughing of the urothelium. Alfieri et al also
explored the effect of the selective inhibition of
nNOS, which did not result in a protective effect
[41]. These observations indicate that inducible, but
not constitutive, NOS-derived NO exerts a
fundamental role in the pathogenesis of HC.
TNF-α and IL-1β were shown to mediate the
production of NO through iNOS induction in the
pathogenesis of ifosfamide- and cyclophosphamide-
induced HC [22, 31]. The induction of iNOS in the
urothelium appeared to depend on the production of
the cytokines IL-1β and TNF-α because antisera
against these cytokines also reduced the expression
of iNOS in the urothelium [31].
Peroxynitrite
The cellular damage that commonly occurs
during conditions of oxidative stress has been
observed following the formation of peroxynitrite
(ONOO-), which originates from the reaction of NO
with superoxide free radicals (O2-) [90]. An
excessive formation of peroxynitrite represents an
important mechanism contributing to DNA damage,
the inactivation of metabolic enzymes, ionic pumps,
and structural proteins, and the disruption of cell
membranes. Peroxynitrite reacts with the tyrosine
in proteins to create nitrotyrosines [91]. Because of
its ability to oxidize biomolecules, peroxynitrite is
implicated in an increasing number of diseases,
including neurodegenerative and cardiovascular
disorders, inflammation, pain, autoimmunity,
cancer, and aging [92].
A first report published by Korkmaz et al showed
that peroxynitrite might contribute to the
pathogenesis of cyclophosphamide-induced HC
[38]; Korkmaz et al reported that ebselen, which
has potent scavenging properties and was shown to
react with peroxynitrite [93], markedly protects
against the development of HC. The results of this
study suggest that the scavenging of peroxynitrite
and the inhibition of iNOS have similar protective
effects.
Platelet activating factor
Platelet-activating factor (PAF; 1-O-alkyl-2-
acetyl-sn-glycero-3-phosphocholine) is a phospho-
lipid mediator that acts largely by binding to its
receptor (PAFR), a G-protein-coupled receptor

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 103
found on most cells, such as monocytes,
neutrophils, B lymphocytes, and keratinocytes
[94-96]. PAF is involved in many biological
processes, including cellular activation, cytoskeletal
reorganization and intracellular signaling, and is a
potent mediator in many inflammatory processes,
including inflammatory bowel disease [97],
multiple sclerosis [98], and asthma [99].
In a study by Rickard et al, the combination of
increased prostacyclin and PAF in the bladder
circulation resulted in vasodilation and increased
polymorphonuclear leukocyte adherence to the
endothelium and facilitated the recruitment of
polymorphonuclear leukocytes to the bladder wall
of patients with interstitial cystitis [100]. In
addition, we found that PAF is one of the
inflammatory mediators contributing to the
activation of the L-arginine–NO pathway in HC
[20]. This conclusion was reached by the use of the
PAF antagonist BN52021, which markedly
protected rats from the cyclophosphamide-induced
plasma protein extravasation and bladder wet
weight gain as well as further prevented the
increase in bladder iNOS activity without
modifying cNOS activity. The maintenance of
cNOS activity during the PAFR blockade implies
that the integrity of the epithelial surface was also
maintained, corroborating the deleterious effect of
PAF in HC.
Substance P
Neurogenic inflammation, components of which
include arteriolar vasodilation (flare) and edema
caused by the extravasation of plasma from post-
capillary venules, is triggered by the release of
substances, such as the proinflammatory
neuropeptides substance P (SP) and calcitonin
gene-related peptide (CGRP), from sensory nerve
terminals [101]. In the urinary tract, such responses
include hyperemia, plasma protein leakage,
contraction of the ureter and bladder and
hyperactivity of the bladder.
Acting through the tachykinin NK1 receptors, SP
may induce tissue inflammation [102] due to the
increased production of NO [103]. Structurally
unrelated antagonist of the NK1 receptors has been
shown to ameliorate the increase in the plasma
permeability extravasation and the histological
damage of the bladder induced by
cyclophosphamide both in rats and ferrets [104]. It
is possible that SP released from the primary
afferent capsaicin-sensitive fibers stimulated by
cyclophosphamide or its metabolite acrolein may
increase NO levels, thereby inducing inflammatory
changes [41].
Alpha1-adrenoceptor
Sympathetic efferents are known to modulate the
neurogenic inflammatory responses by interacting
with primary afferent terminals. α1-Adrenoceptor
antagonists have been successfully used for the
treatment of the symptoms in patients with
indwelling double-J urethral stents [105], ureteral
colic [106], prostatitis and benign prostatic
hyperplasia [107].
Trevisani et al investigated whether α1-adreno-
ceptors are expressed in primary sensory neurons
and whether they contribute to the neurogenic
inflammatory responses that originated in the
urinary tract following cyclophosphamide treatment
[108]. These authors suggested that the α1-adreno-
ceptors contribute to neurogenic inflammation in
the bladder based on the finding that locally applied
phenylephrine increases plasma extravasation in a
manner abolished by alfuzosin, an α1-adrenoceptor
antagonist, and by NK1 receptor blockade. In
addition, these agents were equally effective at
inhibiting the bladder plasma extravasation due to
cyclophosphamide injection. However, alfuzosin
failed to affect the plasma extravasation evoked by
the direct stimulation of the endothelial NK1
receptor by [Sar9,Met(O2)
11]-SP, indicating
selectivity. These results suggest that α1-adreno-
ceptor activation at the terminals of primary
sensory neurons releases SP, which in turn
stimulates the vascular NK1 receptors, promoting
plasma protein leakage in the bladder tissue [108].
Pharmacological approaches to hemorrhagic
cystitis
Table 1 shows a broad review of the experimental
tools, natural products, and clinically available
drugs that have already been tested in
acrolein/chemotherapy-induced HC models.
Among them, mesna and hyperhydration are
currently the only measures used clinically to
prevent HC. From our point of view, the literature
lacks studies that test the effectiveness of anti-
cytokine therapy of HC. However, some anti-
inflammatory cytokines, such as IL-4, IL-11 and
keratinocyte growth factor, have been
experimentally evaluated with important
contributions.
Interleukin-4
As discussed above, exogenous IL-4
administration was able to prevent the development
of HC. Additionally, IL-4 seems to play an
important role in HC pathogenesis, possibly in
counteracting the inflammatory pathways, because

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 104
HC was exacerbated in IL-4-deficient mice and in
anti-IL-4 serum-treated mice [43].
Interleukin-11
IL-11 is a pleiotropic 178-amino acid polypeptide
with a molecular weight of 18 kDa and is secreted
by osteoblasts, synoviocytes, fibroblasts,
chondrocytes, trophoblasts, and many other cell
types in culture [109].
Recombinant human IL-11 (rhIL-11, oprevelkin)
has a number of biological activities, including the
inhibition of pro-inflammatory cytokines (TNF-α
and IL-1β), IL-12, NO synthesis and apoptosis
[110, 111] as well as the stimulation of cell
proliferation, differentiation and connective tissue
protection [111]. Several studies have shown a
protective role for IL-11 in a variety of models of
inflammatory diseases, such as inflammatory bowel
disease, psoriasis, and autoimmune joint disease
[112, 113].
IL-11 affects various stages of megakaryo-
cytopoiesis and thrombopoiesis, and its clinical use
has been shown to shorten the duration of
chemotherapy-induced thrombocytopenia [114].
Additionally, the potential anti-inflammatory
modulating effect of IL-11 was further investigated
in a study published by our group [115] using an
animal model of ifosfamide-induced HC. This
study showed that rhIL-11 inhibits ifosfamide-
induced vascular permeability and edema formation
in a dose-dependent manner, which was confirmed
by macroscopic and microscopic analysis. These
results indicate that the therapeutic manipulation of
IL-11 signaling may provide clinical benefits for
HC.
Keratinocyte growth factor
Keratinocyte growth factor (KGF), a heparin-
binding fibroblast growth factor also known as
FGF-7, has been suggested to play an important
role in the mesenchymal stimulation of normal
epithelial cell proliferation [116]. The
administration of KGF has been shown to protect
animals from various insults, such as radiation- and
bleomycin-induced lung injury [117] and mucositis
[118, 119]. Furthermore, Ulich et al showed that
KGF protects against cyclophosphamide-induced
HC with a marked trophic action on urothelial cells
and minor histological changes, such as edema and
acute inflammation of the urothelium and
submucosa [40].
Figure 3.
Proposed pathways
for the pathogenesis of hemorrhagic cystitis.

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 105
Table 1. Pharmacological approaches in acrolein- or cyclophosphamide(CYP)/ifosfamide(IFO)-induced hemorrhagic cystitis
Experimental
model Compounds Mechanisms of action Improved outcomes References
CYP-induced HC N-acetylcysteine Antioxidant activity Microscopic [18]
CYP-induced HC Mesna Chemical antagonist of
Acrolein Macro and microscopic [122]
CYP-induced HC Penicillamine Anti-inflammatory activity Macro and microscopic [123]
CYP-induced HC Misoprostol Prostaglandin E1 analog Macro and microscopic [19]
CYP-induced HC Prostaglandin F2 alpha Prostaglandin F2 alpha Macro and microscopic [124]
CYP-induced HC Carboprost
tromethamine
Prostaglandin F2 alpha
analog Macro and microscopic [125]
CYP-induced HC L-NAME/L-NOARG NOS inhibitor Macro and microscopic [20]
CYP-induced HC BN-52021 Platelet activating factor
antagonist Macro and microscopic [20]
CYP-induced HC Keratinocyte growth
factor epithelial growth factor Macro and microscopic [40]
CYP-induced HC L-2-oxothiazolidine-4-
carboxylate Antioxidant activity Macro and microscopic [126]
CYP-induced HC Dexamethasone Anti-inflammatory activity Macro and microscopic [121]
CYP-induced HC Glucose-mannose
binding lectins Anti-inflammatory activity Macro and microscopic [127]
CYP-induced HC Berberine Anti-inflammatory activity Macroscopic [128]
IFO-induced HC Thalidomide Inhibitor of TNF
production
Macro and microscopic and
permeability, and iNOS
inhibition
[22]
IFO-induced HC Pentoxifylline
Inhibitor of pro-
inflammatory cytokine
synthesis
Macro and microscopic and
permeability, and iNOS
inhibition
[22]
CYP-induced HC Eviprostat Anti-inflammatory activity Macro and microscopic and
function [129]
IFO-induced HC Ternatin Anti-inflammatory activity Macro and microscopic [130]
IFO-induced HC Latex from Calotropis
procera Antioxidant activity Macro and microscopic [131]
CYP-induced HC Taurine Antioxidant activity
Macro and
microscopic and oxidative
stress
[132]
CYP-induced HC Melatonin Antioxidant, iNOS inhibitor
and peroxynitrite scavenger
Macro and microscopic and
iNOS inhibitor [133]
CYP-induced HC REN1820 Nerve growth factor
recombinant Function [134]
CYP-induced HC Cyclopentenone
prostaglandin (PG) J2
Ligand for the peroxisome
proliferator-activated
receptor-gamma (PPAR-γ)
Macro and microscopic, pro-
inflammatory cytokines and
iNOS inhibition
[135]
CYP-induced HC Alpha-tocopherol Antioxidant activity Macro and microscopic [136]
Acrolein-induced
HC/ IFO-induced
HC
Amifostine Antioxidant activity Macro and microscopic [137]
Acrolein-induced
HC/ IFO-induced
HC
Glutathione Antioxidant activity Macro and microscopic [137]
IFO-induced HC Oprevelkin (rIL-11) Anti-inflammatory activity Macro, microscopic and
permeability [115]
CYP-induced HC Hemin Chemical inducer of HO Macro and microscopic and
iNOS inhibitor [138]
CYP-induced HC Epinephrine Alpha- and beta-adrenergic
receptor agonist Macro and microscopic
[139]
CYP-induced HC Ebselen Seleno compound
Peroxynitrite scavenger Macro and microscopic [140]
CYP-induced HC 1400W Selective iNOS inhibitor Macro and microscopic [140]
CYP-induced HC 3-aminobenzamide Poly(ADP-ribose)
polymerase inhibition Macro and microscopic [140]
CYP-induced HC S-allylcysteine Antioxidant activity Macro and microscopic [141]

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 106
Experimental
model Compounds Mechanisms of action Improved outcomes References
Acrolein-induced
HC and IFO-
induced HC
Etoricoxib COX2 inhibitor Macro and microscopic, COX2
inhibition and function
[36, 37, 39]
Acrolein-induced
HC and IFO-
induced HC
Indomethacin COX inhibitor Macro and microscopic, COX2
inhibition and function
[26, 37, 39]
CYP-induced HC A-317491 P2X3/P2X2/3 antagonist Function [142]
CYP-induced HC Curcumin Antioxidant and anti-
inflammatory activity Macro and microscopic [143]
CYP-induced HC Acacia Senegal gum
exudate
Antioxidant and anti-
inflammatory activity Macro and microscopic [144]
CYP-induced HC Aminoguanidine, Selective iNOS inhibitor Macro and microscopic [145]
CYP-induced HC Parthenolide Nuclear factor-kappaB
inhibitor
Macro, microscopic and
function, COX2 and TNF
inhibition
[34]
CYP-induced HC Rolipram Specific type-4
phosphodiesterase inhibitor
Macro and microscopic and
iNOS inhibition [146]
CYP-induced HC Simvastatin Anti-inflammatory activity
Macro and microscopic, and
pro-inflammatory cytokines
inhibition
[70]
CYP-induced HC Ipomoea obscura (L.) Antioxidant activity
Macro and microscopic, and
pro-inflammatory cytokines
inhibition
[147]
CYP-induced HC Glutamine Antioxidant activity Oxidative stress and neutrophil
infiltration inhibition [148]
CYP-induced HC Seleno-L-methionine Antioxidant activity Macro and microscopic,
oxidative stress inhibition [149]
CYP-induced HC MV8608 and MV8612 Anti-inflammatory and
antinociceptive activity
Macro, microscopic,
hypernociception, and
neutrophil infiltration inhibition
[150]
CYP-induced HC Tacrolimus Inhibitor of interleukin-2
production by T-cells
Microscopic and function, and
PGE2 and EP4 inhibition [151]
CYP-induced HC ISO-1 Macrophage migration
inhibitory factor
Macro, microscopic, function
and hypernociception, nerve
growth factor and pro-
inflammatory cytokines
inhibition
[152]
CYP-induced HC HC-067047 Selective TRPV4
antagonist Function [18]
CYP-induced HC ONO-8130 Selective prostanoid EP1
antagonist
Permeability and
hypernociception [153]
CYP-induced HC Hydroalcoholic extract
of Phyllanthus niruri Unknown
Macro, microscopic,
hypernociception and oxidative
stress
[154]
CYP-induced HC A-438079 P2X7 receptor antagonist
Macro, microscopic, neutrophil
and macrophage infiltration,
and inflammatory cytokines
inhibition
[155]
Chemotherapy-induced HC was considered to be
an unsolved problem in the oncology patient
population. Currently, clinical studies with
palifermin (recombinant KGF) have indicated that
hematopoietic stem cell transplant patients treated
with high-dose cytotoxic regimens present with a
reduced severity of lesions in the oral mucosa
[120]. Considering that mucosal ulceration seems to
be a key event in the most symptomatic phase of
HC, further studies are needed to better investigate
the potential protective effect of KGF on this
disease.
Corticosteroid therapy
Taking into consideration the unquestionable
participation of various inflammatory mediators in
the pathogenesis of HC, there is a question of
whether corticosteroids would be effective at
preventing HC-associated bladder damage. This

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 107
hypothesis was experimentally tested by our group
[23, 121]. In these studies, we verified that
dexamethasone in combination with mesna was
efficient in attenuating cyclophosphamide- or
ifosfamide-induced HC. However, the replacement
of the last two doses of mesna with saline or all of
the mesna doses with dexamethasone did not
prevent HC. This is a clear demonstration that
mesna is still needed to prevent the initial epithelial
bladder damage, which is not achieved by
dexamethasone alone. However, the corticosteroid
inhibition of cytokine activation prevents the
underlying inflammatory aspect of HC. Therefore,
clinical trials are needed to prove the experimental
findings using corticosteroids.
Conclusions
Hemorrhagic cystitis is an important clinical
issue that has been recently brought to attention due
to an augmented incidence mainly following the
increase in treatment regimens of high-dose
alkylating agents in the context of hematopoietic
stem cell transplantation and cancer chemotherapy.
Several inflammatory mediators have been
implicated in the development of hemorrhagic
cystitis due to chemotherapy agents (Fig.3). Despite
the recent advances in the knowledge of the
pathogenesis of this clinical condition, further
investigation is needed to determine the precise
inflammatory cascade involved. The enhanced
understanding of the role played by these
inflammatory pathways may allow the
identification of novel pharmacologic targets for
this pathology.
Acknowledgements.
R.A.R. is a researcher from Conselho Nacional de
Desenvolvimento Cientifico e Tecnologico (CNPq),
Brazil. This work was supported by research grants from
the CNPq and Fundacao Cearense de Apoio ao
Desenvolvimento Cientifico (FUNCAP) –Nucleo de
Estudos da Toxicidade do Tratamento Oncologico
(NETTO) - Processo 21.01.00/08.
References
1. Moy B. Cystitis in patients with cancer. In: UpToDate
version 20.3 via http://www.uptodate.com/contents/cystitis-in-patients-with-cancer (Accessed 15 February 2012).
2. Coggins PR, Ravdin RG, Eisman SH. Clinical evaluation
of a new alkylating agent: cytoxan (cyclophosphamide). Cancer 1960; 13:1254-60.
3. Stillwell TJ, Benson RC Jr. Cyclophosphamide-induced
hemorrhagic cystitis: a review of 100 patients. Cancer 1988; 61:451-7.
4. Seber A, Shu XO, Defor T, Sencer S, Ramsay N. Risk
factors for severe hemorrhagic cystitis following BMT. Bone Marrow Transplant 1999; 23:35-40.
5. Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R,
Miller LG, Moran GJ, Nicolle LE, Raz R, Schaeffer AJ,
Soper DE. International clinical practice guidelines for the
treatment of acute uncomplicated cystitis and
pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for
Microbiology and Infectious Diseases. Clin Infect Dis
2011; 52:e103-20. 6. Watson NA, Notley RG. Urological complications of
cyclophosphamide. Br J Urol 1973; 45:606-9. 7. Shepherd JD, Pringle LE, Barnett MJ, Klingemann HG,
Reece DE, Phillips GL. Mesna versus hyperhydration for
the prevention of cyclophosphamide-induced hemorrhagic cystitis in bone marrow transplantation. J Clin Oncol 1991;
9:2016-20.
8. Vose JM, Reed EC, Pippert GC, Anderson JR, Bierman PJ, Kessinger A, Spinolo J, Armitage JO. Mesna compared
with continuous bladder irrigation as uroprotection during
high-dose chemotherapy and transplantation: a randomized trial. J Clin Oncol 1993; 11:1306-10.
9. Meisenberg B, Lassiter M, Hussein A, Ross M,
Vredenburgh JJ, Peters WP. Prevention of hemorrhagic cystitis after high-dose alkylating agent chemotherapy and
autologous bone marrow support. Bone Marrow Transplant
1994; 14:287-91.
10. Hadjibabaie M, Alimoghaddam K, Shamshiri AR, Iravani
M, Bahar B, Mousavi A, Jahani M, Khodabandeh A, Anvari Y, Gholami K, Ghavamzadeh A. Continuous
bladder irrigation prevents hemorrhagic cystitis after
allogeneic hematopoietic cell transplantation. Urol Oncol. 2008; 26:43-6.
11. Koc S, Hagglund H, Ireton RC, Perez-Simon JA, Collins
SJ, Appelbaum FR. Successful treatment of severe hemorrhagic cystitis with cystectomy following matched
donor allogeneic hematopoietic cell transplantation. Bone
Marrow Transplant 2000; 26:899-901. 12. El-Zimaity M, Saliba R, Chan K, Shahjahan M, Carrasco
A, Khorshid O, Caldera H, Couriel D, Giralt S, Khouri I,
Ippoliti C, Champlin R, de Lima M. Hemorrhagic cystitis
after allogeneic hematopoietic stem cell transplantation:
donor type matters. Blood 2004; 103:4674-80.
13. Lima MV, Ferreira FV, Macedo FY, de Castro Brito GA, Ribeiro RA. Histological changes in bladders of patients
submitted to ifosfamide chemotherapy even with mesna
prophylaxis. Cancer Chemother Pharmacol 2007; 59:643-50.
14. Gine E, Rovira M, Real I, Burrel M, Montana J, Carreras E, Montserrat E. Successful treatment of severe hemorrhagic
cystitis after hemopoietic cell transplantation by selective
embolization of the vesical arteries. Bone Marrow Transplant 2003; 31:923-5.
15. Manikandan R, Kumar S, Dorairajan LN. Hemorrhagic
cystitis: A challenge to the urologist. Indian J Urol 2010; 26:159-66.
16. Philips FS, Sternberg SS, Cronin AP, Vidal PM.
Cyclophosphamide and urinary bladder toxicity. Cancer Res 1961; 21:1577-89.
17. Campobasso O, Berrino F. Early effects of
cyclophosphamide on mouse bladder epithelium. Pathol Microbiol (Basel) 1972; 38:144-57.

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 108
18. Tolley DA, Castro JE. Cyclophosphamide-induced cystitis of the urinary bladder of rats and its treatment. Proc R Soc
Med 1975; 68:169-70.
19. Gray KJ, Engelmann UH, Johnson EH, Fishman IJ. Evaluation of misoprostol cytoprotection of the bladder
with cyclophosphamide (Cytoxan) therapy. J Urol 1986;
136: 497-500. 20. Souza-Fiho MV, Lima MV, Pompeu MM, Ballejo G,
Cunha FQ, Ribeiro Rde A. Involvement of nitric oxide in
the pathogenesis of cyclophosphamide-induced hemorrhagic cystitis. Am J Pathol 1997; 150:247-56.
21. Zhang J, Quan T, Zhou SF. Clinical pharmacology of
cyclophosphamide and ifosfamide. Current Drug Therapy 2006; 1:55-84.
22. Ribeiro RA, Freitas HC, Campos MC, Santos CC,
Figueiredo FC, Brito GA, Cunha FQ. Tumor necrosis factor-alpha and interleukin-1beta mediate the production
of nitric oxide involved in the pathogenesis of ifosfamide
induced hemorrhagic cystitis in mice. J Urol 2002; 167:2229-34.
23. Vieira MM, Brito GA, Belarmino-Filho JN, Macedo FY,
Nery EA, Cunha FQ, Ribeiro RA. Use of dexamethasone with mesna for the prevention of ifosfamide-induced
hemorrhagic cystitis. Int J Urol 2003; 10:595-602.
24. Chaviano AH, Gill WB, Ruggiero KJ, Vermeulen CW. Experimental cytoxan cystitis and prevention by
acetylcysteine. J Urol 1985; 134:598-600.
25. Batista CK, Brito GA, Souza ML, Leitao BT, Cunha FQ, Ribeiro RA. A model of hemorrhagic cystitis induced with
acrolein in mice. Braz J Med Biol Res 2006; 39:1475-81.
26. Arnold H, Bourseaux F, Brock N. Neuartige Krebs-Chemotherapeutika aus der Gruppe der zyklischen N-Lost-
Phosphamidester. Naturwissenschaften 1958; 45:64-6.
27. deVries CR, Freiha FS. Hemorrhagic cystitis: a review. J Urol 1990; 143:1-9.
28. Alarcon RA, Meienhofer J. Formation of the cytotoxic
aldehyde acrolein during in vitro degradation of cyclophosphamide. Nat New Biol 1971; 233:250-2.
29. Cox PJ. Cyclophosphamide cystitis--identification of
acrolein as the causative agent. Biochem Pharmacol 1979; 28:2045-9.
30. Scheef W, Klein HO, Brock N, Burkert H, Gunther U,
Hoefer-Janker H, Mitrenga D, Schnitker J, Voigtmann R. Controlled clinical studies with an antidote against the
urotoxicity of oxazaphosphorines: preliminary results.
Cancer Treat Rep 1979; 63:501-5. 31. Gomes TN, Santos CC, Souza-Filho MV, Cunha FQ,
Ribeiro RA. Participation of TNF-alpha and IL-1 in the
pathogenesis of cyclophosphamide-induced hemorrhagic cystitis. Braz J Med Biol Res 1995; 28:1103-8.
32. Sonis ST. Mucositis as a biological process: a new
hypothesis for the development of chemotherapy-induced stomatotoxicity. Oral Oncol 1998; 34:39-43.
33. Korkmaz A, Topal T, Oter S. Pathophysiological aspects of cyclophosphamide and ifosfamide induced hemorrhagic
cystitis; implication of reactive oxygen and nitrogen
species as well as PARP activation. Cell Biol Toxicol 2007; 23:303-12.
34. Kiuchi H, Takao T, Yamamoto K, Nakayama J, Miyagawa
Y, Tsujimura A, Nonomura N, Okuyama A. Sesquiterpene
lactone parthenolide ameliorates bladder inflammation and
bladder overactivity in cyclophosphamide induced rat
cystitis model by inhibiting nuclear factor-kappaB phosphorylation. J Urol 2009; 181:2339-48.
35. Oter S, Korkmaz A, Oztas E, Yildirim I, Topal T, Bilgic H.
Inducible nitric oxide synthase inhibition in
cyclophosphamide induced hemorrhagic cystitis in rats. Urol Res 2004; 32:185-9.
36. Macedo FY, Baltazar F, Almeida PR, Tavora F, Ferreira
FV, Schmitt FC, Brito GA, Ribeiro RA. Cyclooxygenase-2 expression on ifosfamide-induced hemorrhagic cystitis in
rats. J Cancer Res Clin Oncol 2008; 134:19-27.
37. Macedo FY, Baltazar F, Mourao LC, Almeida PR, Mota JM, Schmitt FC, Ribeiro RA. Induction of COX-2
expression by acrolein in the rat model of hemorrhagic
cystitis. Exp Toxicol Pathol 2008; 59:425-30. 38. Korkmaz A, Oter S, Sadir S, Coskun O, Topal T, Ozler M,
Bilgic H. Peroxynitrite may be involved in bladder damage
caused by cyclophosphamide in rats. J Urol 2005; 173:1793-6.
39. Macedo FY, Mourao LT, Palheta RC Jr, Juca DM, Lima
RC Jr, Neto Jde S, Magalhaes PJ, Santos AA, Souza MH, Brito GA, Ribeiro RA. Cyclooxygenase-2 contributes to
functional changes seen on experimental hemorrhagic
cystitis induced by ifosfamide in rat urinary bladder. Cancer Chemother Pharmacol 2011; 67:935-43.
40. Ulich TR, Whitcomb L, Tang W, O'Conner Tressel P,
Tarpley J, Yi ES, Lacey D. Keratinocyte growth factor ameliorates cyclophosphamide-induced ulcerative
hemorrhagic cystitis. Cancer Res 1997; 57:472-5.
41. Alfieri AB, Malave A, Cubeddu LX. Nitric oxide synthases and cyclophosphamide-induced cystitis in rats. Naunyn
Schmiedebergs Arch Pharmacol 2001; 363:353-7.
42. Malley SE, Vizzard MA. Changes in urinary bladder cytokine mRNA and protein after cyclophosphamide-
induced cystitis. Physiol Genomics 2002; 9:5-13.
43. Macedo FY, Mourao LT, Freitas HC, Lima-Junior RC, Wong DV, Oria RB, Vale ML, Brito GA, Cunha FQ,
Ribeiro RA. Interleukin-4 modulates the inflammatory
response in ifosfamide-induced hemorrhagic cystitis. Inflammation 2011; doi:10.1007/s10753-011-9319-3.
44. Hahn NM. Learning to control cyclophosphamide induced
cystitis. J Urol 2009; 181:1987-8. 45. Baldwin AS Jr. The NF-kappa B and I kappa B proteins:
new discoveries and insights. Annu Rev Immunol 1996;
14:649-83. 46. Pfeffer LM. The role of nuclear factor κB in the interferon
response. J Interferon Cytokine Res 2011; 31:553-9.
47. Hehner SP, Heinrich M, Bork PM, Vogt M, Ratter F, Lehmann V, Schulze-Osthoff K, Droge W, Schmitz ML.
Sesquiterpene lactones specifically inhibit activation of
NF-kappa B by preventing the degradation of I kappa B-alpha and I kappa B-beta. J Biol Chem 1998; 273:1288-97
48. Parameswaran N, Patial S. Tumor necrosis factor-α
signaling in macrophages. Crit Rev Eukaryot Gene Expr 2010; 20:87-103.
49. Schett G, Coates LC, Ash ZR, Finzel S, Conaghan PG.
Structural damage in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: traditional views,
novel insights gained from TNF blockade, and concepts for the future. Arthritis Res Ther 2011; 13(Suppl 1):S4.
50. Reinisch W, Dejaco C, Feichtenschlager T, Haas T, Kaser
A, Miehsler W, Novacek G, Petritsch W, Platzer R, Tilg H, Vogelsang H, Knoflach P. Infliximab therapy for Crohn's
disease - a practical guideline: actualised consensus of the
working group for chronic inflammatory bowel diseases of
the Austrian Society for Gastroenterology and Hepatology.
Z Gastroenterol. 2011; 49:534-42.
51. Exley AR, Cohen J, Buurman W, Owen R, Hanson G, Lumley J, Aulakh JM, Bodmer M, Riddell A, Stephens S,
Riddell A, Perry M. Monoclonal antibody to TNF in severe
septic shock. Lancet 1990; 335:1275-7.

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 109
52. Wachlin G, Augstein P, Schröder D, Kuttler B, Klöting I, Heinke P, Schmidt S. IL-1beta, IFN-gamma and TNF-
alpha increase vulnerability of pancreatic beta cells to
autoimmune destruction. J Autoimmun 2003; 20:303-12. 53. Logan RM, Stringer AM, Bowen JM, Yeoh AS, Gibson RJ,
Sonis ST, Keefe DM. The role of pro-inflammatory
cytokines in cancer treatment-induced alimentary tract mucositis: pathobiology, animal models and cytotoxic
drugs. Cancer Treat Rev 2007; 33:448-60.
54. Sampaio EP, Sarno EN, Galilly R, Cohn ZA, Kaplan G. Thalidomide selectively inhibits tumor necrosis factor α
production by stimulated human monocytes. J Exp Med
1991; 173:699-703 55. Wiens A, Venson R, Correr CJ, Otuki MF, Pontarolo R.
Meta-analysis of the efficacy and safety of adalimumab,
etanercept, and infliximab for the treatment of rheumatoid arthritis. Pharmacotherapy 2010; 30:339-53.
56. Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP.
Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacol Ther 2008; 117:244-79.
57. Mossner R, Reich K. Management of severe psoriasis with
TNF antagonists. Adalimumab, etanercept and infliximab. Curr Probl Dermatol 2009; 38:107-36.
58. Inman RD, Maksymowych WP; CANDLE Study Group. A
double-blind, placebo-controlled trial of low dose infliximab in ankylosing spondylitis. J Rheumatol 2010;
37:1203-10.
59. Dinarello CA. Immunological and inflammatory functions of the interleukin-1 family. Ann Rev Immunol 2009;
27:519-50.
60. Dinarello CA. Biologic basis for interleukin-1 in disease. Blood 1996; 87:2095-147.
61. Weber A, Wasiliew P, Kracht M. Interleukin-1 (IL-1)
pathway. Sci Signal 2010; 3:cm1. 62. Dinarello CA. Interleukin-1 in the pathogenesis and
treatment of inflammatory diseases. Blood 2011; 117:3720-
32. 63. Dinarello CA. Blocking interleukin-1β in acute and chronic
autoinflammatory diseases. J Intern Med 2011; 269:16-28.
64. Kreth S, Ledderose C, Luchting B, Weis F, Thiel M. Immunomodulatory properties of pentoxifylline are
mediated via adenosine-dependent pathways. Shock 2010;
34:10-6. 65. Hart PH, Vitti GF, Burgess DR, Whitty GA, Piccoli DS,
Hamilton JA. Potential antiinflammatory effects of
interleukin 4: suppression of human monocyte tumor necrosis factor alpha, interleukin 1, and prostaglandin E2.
Proc Natl Acad Sci USA 1989; 86:3803-7.
66. Vannier E, Miller LC, Dinarello CA. Coordinated antiinflammatory effects of interleukin 4: interleukin 4
suppresses interleukin 1 production but up-regulates gene
expression and synthesis of interleukin 1 receptor antagonist. Proc Natl Acad Sci USA 1992; 89:4076-80.
67. Seitz M, Loetscher P, Dewald B, Towbin H, Ceska M, Baggiolini M. Production of interleukin-1 receptor
antagonist, inflammatory chemotactic proteins, and
prostaglandin E by rheumatoid and osteoarthritic synoviocytes--regulation by IFN-gamma and IL-4. J
Immunol 1994; 152:2060-5.
68. Heymann D, Rousselle AV. gp130 Cytokine family and
bone cells. Cytokine 2000; 12:1455-68.
69. Nishii H, Nomura M, Fujimoto N, Matsumoto T. Up-
regulation of interleukin-6 gene expression in cyclophosphamide-induced cystitis in mice: An in situ
hybridization histochemical study. Int J Urol 2006;
13:1339-43.
70. Dantas AC, Batista-Junior FF, Macedo LF, Mendes MN, Azevedo IM, Medeiros AC. Protective effect of simvastatin
in the cyclophosphamide-induced hemorrhagic cystitis in
rats. Acta Cir Bras 2010; 25:43-6. 71. Girard BM, Cheppudira BP, Malley SE, Schutz KC, May
V, Vizzard MA. Increased expression of interleukin-6
family members and receptors in urinary bladder with cyclophosphamide-induced bladder inflammation in female
rats. Front Neurosci 2011; 5:20.
72. Zhang Y, Wang L, Zhang M, Jin M, Bai C, Wang X. Potential mechanism of interleukin-8 production from lung
cancer cells: an involvement of EGF-EGFR-PI3K-Akt-Erk
pathway. J Cell Physiol 2012; 227:35-43. 73. Shen Y, Wang D, Wang X. Role of CCR2 and IL-8 in
acute lung injury: a new mechanism and therapeutic target.
Expert Rev Respir Med 2011; 5:107-14. 74. Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP,
Fahmi H. Role of proinflammatory cytokines in the
pathophysiology of osteoarthritis. Nat Rev Rheumatol 2011; 7:33-42.
75. Gambari R, Borgatti M, Bezzerri V, Nicolis E, Lampronti
I, Dechecchi MC, Mancini I, Tamanini A, Cabrini G. Decoy oligodeoxyribonucleotides and peptide nucleic
acids-DNA chimeras targeting nuclear factor kappa-B:
inhibition of IL-8 gene expression in cystic fibrosis cells infected with Pseudomonas aeruginosa. Biochem
Pharmacol 2010; 80:1887-94.
76. Bhoola KD, Figueroa CD, Worthy K. Bioregulation of kinins: kallikreins, kininogens, and kininases. Pharmacol
Rev 1992; 44:1-80.
77. Marceau F, Regoli D. Bradykinin receptor ligands: therapeutic perspectives. Nat Rev Drug Discov 2004;
3:845-52.
78. Stewart JM. Bradykinin antagonists: discovery and development. Peptides 2004; 25:527-32.
79. Maggi CA, Santicioli P, Del Bianco E, Lecci A, Guliani S.
Evidence for the involvement of bradykinin in chemically-evoked cystitis in anaesthetized rats. Naunyn
Schmiedebergs Arch Pharmacol 1993; 347:432-7.
80. Chopra B, Barrick SR, Meyers S, Beckel JM, Zeidel ML, Ford AP, de Groat WC, Birder LA. Expression and
function of bradykinin B1 and B2 receptors in normal and
inflamed rat urinary bladder urothelium. J Physiol 2005; 562:859-71.
81. Fincham CI, Bressan A, Paris M, Rossi C, Fattori D.
Bradykinin receptor antagonists--a review of the patent literature 2005-2008. Expert Opin Ther Pat 2009; 19:919-
41.
82. Jawabrah Al-Hourani B, Sharma SK, Suresh M, Wuest F. Cyclooxygenase-2 inhibitors: a literature and patent review
(2009-2010). Expert Opin Ther Pat 2011; 21:1339-432.
83. Dannenberg AJ, Altorki NK, Boyle JO, Dang C, Howe LR, Weksler BB, Subbaramaiah K. Cyclo-oxygenase 2: A
pharmacological target for the prevention of cancer. Lancet Oncol 2001; 2:544-51.
84. Kawabata A. Prostaglandin E2 and pain--an update. Biol
Pharm Bull 2011; 34:1170-3. 85. Dubois RN, Abramson SB, Crofford L, Gupta RA, Simon
LS, Van De Putte LB, Lipsky PE. Cyclooxygenase in
biology and disease. FASEB J 1998; 12:1063-73.
86. Hu VY, Malley S, Dattilio A, Folsom JB, Zvara P, Vizzard
MA. COX-2 and prostanoid expression in micturition
pathways after cyclophosphamide-induced cystitis in the rat. Am J Physiol Regul Integr Comp Physiol 2003;
284:R574-85.
87. Maggi CA. Prostanoids as local modulators of reflex micturition. Pharmacol Res 1992; 25:13-20.

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 110
88. Ishizuka O, Mattiasson A, Andersson KE. Prostaglandin E2-induced bladder hyperactivity in normal, conscious rats:
involvement of tachykinins? J Urol 1995; 153:2034-8.
89. Forstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J 2011;
doi:10.1093/eurheartj/ehr304
90. Beckman JS, Beckman TW, Chen J, Marshall PA, Freeman BA. Apparent hydroxyl radical production by peroxynitrite:
implications for endothelial injury from nitric oxide and
superoxide. Proc Natl Acad Sci USA 1990; 87:1620-4. 91. Ischiropoulos H, al-Mehdi AB. Peroxynitrite-mediated
oxidative protein modifications. FEBS Lett 1995; 364:279-
82. 92. Ascenzi P, di Masi A, Sciorati C, Clementi E.
Peroxynitrite-An ugly biofactor? Biofactors 2010; 36:264-
73. 93. Masumoto H, Sies H. The reaction of ebselen with
peroxynitrite. Chem Res Toxicol 1996; 9:262-7.
94. Muller E, Dagenais P, Alami N, Rola-Pleszczynski M. Identification and functional characterization of platelet-
activating factor receptors in human leukocyte populations
using polyclonal anti- peptide antibody. Proc Natl Acad Sci USA 1993; 90:5818-22.
95. Travers JB, Huff JC, Rola-Pleszczynski M, Gelfand EW,
Morelli JG, Murphy RC. Identification of functional platelet-activating factor receptors on human keratinocytes.
J Invest Dermatol 1995; 105:816-23.
96. Honda ZI, Ishii S, Shimizu T. Platelet-activating factor receptor. J Biochem 2002; 131:773-9.
97. Borthakur A, Bhattacharyya S, Alrefai WA, Tobacman JK,
Ramaswamy K, Dudeja PK. Platelet-activating factor-induced NF-kappaB activation and IL-8 production in
intestinal epithelial cells are Bcl10-dependent. Inflamm
Bowel Dis 2010; 16:593-603. 98. Lock C, Hermans G, Pedotti R, Brendolan A, Schadt E,
Garren H, Langer-Gould A, Strober S, Cannella B, Allard
J, Klonowski P, Austin A, Lad N, Kaminski N, Galli SJ, Oksenberg JR, Raine CS, Heller R, Steinman L. Gene-
microarray analysis of multiple sclerosis lesions yields new
targets validated in autoimmune encephalomyelitis. Nat Med 2002; 8:500-8.
99. Chakir J, Shannon J, Molet S, Fukakusa M, Elias J,
Laviolette M, Boulet LP, Hamid Q. Airway remodeling-associated mediators in moderate to severe asthma: effect
of steroids on TGF-β, IL-11, IL-17, and type I and type III
collagen expression. J Allergy Clin Immunol 2003; 111:1293-8.
100. Rickard A, Portell C, Kell PJ, Vinson SM, McHowat J.
Protease-activated receptor stimulation activates a Ca2+-independent phospholipase A2 in bladder microvascular
endothelial cells. Am J Physiol Renal Physiol 2005;
288:F714-21. 101. Geppetti P, Nassini R, Materazzi S, Benemei S. The
concept of neurogenic inflammation. BJU Int 2008; 101(Suppl 3):2-6.
102. Frode-Saleh TS, Calixto JB, Medeiros YS. Analysis of the
inflammatory response induced by substance P in the mouse pleural cavity. Peptides 1999; 20:259-65.
103. Maggi CA, Catalioto RM, Criscuoli M, Cucchi P, Giuliani
S, Lecci A, Lippi A, Meini S, Patacchini R, Renzetti AR,
Santicioli P, Tramontana M, Zagorodnyuk V, Giachetti A.
Tachykinin receptors and intestinal motility. Can J Physiol
Pharmacol 1997; 75:696-703. 104. Alfieri A, Gardner C. The NK1 antagonist GR203040
inhibits cyclophosphamide-induced damage in the rat and
ferret bladder. Gen Pharmacol 1997; 29:245-50.
105. Deliveliotis C, Chrisofos M, Gougousis E, Papatsoris A, Dellis A, Varkarakis IM. Is there a role for alpha1-blockers
in treating double-J stent-related symptoms? Urology 2006;
67:35-9. 106. Dellabella M, Milanese G, Muzzonigro G. Efficacy of
tamsulosin in the medical management of juxtavesical
ureteral stones. J Urol 2003; 170:2202-5. 107. Romics I. The role of alpha-adrenoreceptors in the
treatment of urological diseases. Neurochem Int 2007;
51:328-31. 108. Trevisani M, Campi B, Gatti R, Andre E, Materazzi S,
Nicoletti P, Gazzieri D, Geppetti P. The influence of
alpha1-adrenoreceptors on neuropeptide release from primary sensory neurons of the lower urinary tract. Eur
Urol 2007; 52:901-8.
109. Putoczki T, Ernst M. More than a sidekick: the IL-6 family cytokine IL-11 links inflammation to cancer. J Leukoc Biol
2010; 88:1109-17.
110. Orazi A, Du X, Yang Z, Kashai M, Williams DA. Interleukin-11 prevents apoptosis and accelerates recovery
of small intestinal mucosa in mice treated with combined
chemotherapy and radiation. Lab Invest 1996; 75:33-42. 111. Trepicchio WL, Bozza M, Pedneault G, Dorner AJ.
Recombinant human IL-11 attenuates the inflammatory
response through down-regulation of proinflammatory cytokine release and nitric oxide production. J Immunol
1996; 157:3627-34.
112. Schwertschlag US, Trepicchio WL, Dykstra KH, Keith JC, Turner KJ, Dorner AJ. Hematopoietic, immunomodulatory
and epithelial effects of interleukin-11. Leukemia 1999;
13:1307-15. 113. Robb L, Dimitriadis E, Li R, Salamonsen LA. Leukemia
inhibitory factor and interleukin-11: cytokines with key
roles in implantation. J Reprod Immunol 2002; 57:129-41. 114. Ciurea SO, Hoffman R. Cytokines for the treatment of
thrombocytopenia. Semin Hematol 2007; 44:166-82.
115. Mota JM, Brito GA, Loiola RT, Cunha FQ, Ribeiro Rde A. Interleukin-11 attenuates ifosfamide-induced hemorrhagic
cystitis. Int Braz J Urol 2007; 33:704-10.
116. Rubin JS, Osada H, Finch PW, Taylor WG, Rudikoff S, Aaronson SA. Purification and characterization of a newly
identified growth factor specific for epithelial cells. Proc
Natl Acad Sci USA 1989; 86:802-6. 117. Yi ES, Williams ST, Lee H, Malicki DM, Chin EM, Yin S,
Tarpley J, Ulich TR. Keratinocyte growth factor
ameliorates radiation- and bleomycin-induced lung injury and mortality. Am J Pathol 1996; 149:1963-70.
118. Farrell CL, Bready JV, Rex KL, Chen JN, DiPalma CR,
Whitcomb KL, Yin S, Hill DC, Wiemann B, Starnes CO, Havill AM, Lu ZN, Aukerman SL, Pierce GF, Thomason
A, Potten CS, Ulich TR, Lacey DL. Keratinocyte growth
factor protects mice from chemotherapy and radiation-induced gastrointestinal injury and mortality. Cancer Res
1998; 58:933-9. 119. Farrell CL, Rex KL Chen JN, Bready JV, DiPalma CR,
Kaufman SA, Rattan A, Scully S, Lacey DL. The effects of
keratinocyte growth factor inpreclinical models of mucositis. Cell Prolif 2002; 35(Suppl 1):78-85.
120. Barasch A, Epstein J, Tilashalski K. Palifermin for
management of treatment-induced oral mucositis in cancer
patients. Biologics 2009; 3:111-6.
121. Morais MM, Belarmino-Filho JN, Brito GA, Ribeiro RA.
Pharmacological and histopathological study of cyclophosphamide-induced hemorrhagic cystitis -
comparison of the effects of dexamethasone and Mesna.
Braz J Med Biol Res 1999; 32:1211-5.

Journal of Experimental and Integrative Medicine 2012; 2(2):95-112
www.jeim.org 111
122. Brock N, Stekar J, Pohl J, Niemeyer U, Scheffler G. Acrolein, the causative factor of urotoxic side-effects of
cyclophosphamide, ifosfamide, trofosfamide and
sufosfamide. Arzneimittelforschung 1979; 29:659-61. 123. Christophidis N, Cosolo W, Louis WJ, Louis CJ. The effect
of penicillamine and related thiols on cyclophosphamide-
induced cystitis and bone marrow suppression. Int J Tissue React 1984; 6:493-8.
124. Grinberg-Funes DJ, Sheldon C, Weiss M. The use of
prostaglandin F2 alpha for the prophylaxis of cyclophosphamide induced cystitis in rats. J Urol 1990;
144:1500-4.
125. Kranc DM, Kim J, Straus F, Levine LA. Prophylactic and therapeutic carboprost tromethamine bladder irrigation in
rats with cyclophosphamide-induced hemorrhagic cystitis.
J Urol 1992; 148:1326-30. 126. Safron J, Rice D, Gordon D, Leaf C, White R. Protective
effects of L-2-oxothiazolidine-4-carboxylate treatment on
cyclophosphamide-induced cystitis in rats. J Urol 1997; 157:1946-50
127. Assreuy AM, Martins GJ, Moreira ME, Brito GA, Cavada
BS, Ribeiro RA, Flores CA. Prevention of cyclophosphamide-induced hemorrhagic cystitis by
glucose-mannose binding plant lectins. J Urol 1999;
161:1988-93. 128. Xu X, Malave A. Protective effect of berberine on
cyclophosphamide-induced haemorrhagic cystitis in rats.
Pharmacol Toxicol 2001; 88:232-7. 129. Kobayashi M, Nomura M, Nishii H, Matsumoto S,
Fujimoto N, Matsumoto T. Effect of eviprostat on bladder
overactivity in an experimental cystitis rat model. Int J Urol 2008; 15:356-60.
130. Vieira MM, Macedo FY, Filho JN, Costa AC, Cunha AN,
Silveira ER, Brito GA, Ribeiro RA. Ternatin, a flavonoid, prevents cyclophosphamide and ifosfamide-induced
hemorrhagic cystitis in rats. Phytother Res 2004; 18:135-
41. 131. Alencar NM, Figueiredo IS, Vale MR, Bitencurt FS,
Oliveira JS, Ribeiro RA, Ramos MV. Anti-inflammatory
effect of the latex from Calotropis procera in three different experimental models: peritonitis, paw edema and
hemorrhagic cystitis. Planta Med 2004; 70:1144-9.
132. Abd-Allah AR, Gado AM, Al-Majed AA, Al-Yahya AA, Al-Shabanah OA. Protective effect of taurine against
cyclophosphamide-induced urinary bladder toxicity in rats.
Clin Exp Pharmacol Physiol 2005; 32:167-72. 133. Topal T, Oztas Y, Korkmaz A, Sadir S, Oter S, Coskun O,
Bilgic H. Melatonin ameliorates bladder damage induced
by cyclophosphamide in rats. J Pineal Res 2005; 38:272-7. 134. Hu VY, Zvara P, Dattilio A, Redman TL, Allen SJ,
Dawbarn D, Stroemer RP, Vizzard MA. Decrease in
bladder overactivity with REN1820 in rats with cyclophosphamide induced cystitis. J Urol 2005; 173:1016-
21. 135. Masuda H, Chancellor MB, Kihara K, Yoshimura N. 15-
deoxy-Delta12,14-prostaglandin J2 attenuates development
of cyclophosphamide-induced cystitis in rats. Urology 2006; 67:435-9.
136. Sadir S, Deveci S, Korkmaz A, Oter S. Alpha-tocopherol,
beta-carotene and melatonin administration protects
cyclophosphamide-induced oxidative damage to bladder
tissue in rats. Cell Biochem Funct 2007; 25:521-6.
137. Batista CK, Mota JM, Souza ML, Leitao BT, Souza MH, Brito GA, Cunha FQ, Ribeiro RA. Amifostine and
glutathione prevent ifosfamide- and acrolein-induced
hemorrhagic cystitis. Cancer Chemother Pharmacol 2007; 59:71-7.
138. Matsuoka Y, Masuda H, Yokoyama M, Kihara K. Protective effects of heme oxygenase-1 against
cyclophosphamide-induced haemorrhagic cystitis in rats.
BJU Int 2007; 100:1402-8. 139. Chow YC, Yang S, Huang CJ, Tzen CY, Su YH, Wang PS.
Prophylactic intravesical instillation of epinephrine
prevents cyclophosphamide-induced hemorrhagic cystitis in rats. Exp Biol Med (Maywood) 2007; 232:565-70.
140. Korkmaz A, Kurt B, Yildirim I, Basal S, Topal T, Sadir S,
Oter S. Effects of poly(ADP-ribose) polymerase inhibition in bladder damage caused by cyclophosphamide in rats.
Exp Biol Med (Maywood) 2008; 233:338-43.
141. Bhatia K, Ahmad F, Rashid H, Raisuddin S. Protective effect of S-allylcysteine against cyclophosphamide-induced
bladder hemorrhagic cystitis in mice Food Chem Toxicol
2008; 46:3368-74. 142. Ito K, Iwami A, Katsura H, Ikeda M. Therapeutic effects of
the putative P2X3/P2X2/3 antagonist A-317491 on
cyclophosphamide-induced cystitis in rats. Naunyn Schmiedebergs Arch Pharmacol 2008; 377:483-90.
143. Arafa HM. Uroprotective effects of curcumin in
cyclophosphamide-induced haemorrhagic cystitis paradigm. Basic Clin Pharmacol Toxicol 2009; 104:393-9.
144. Al-Yahya AA, Al-Majed AA, Gado AM, Daba MH, Al-
Shabanah OA, Abd-Allah AR. Acacia Senegal gum exudate offers protection against cyclophosphamide-
induced urinary bladder cytotoxicity. Oxid Med Cell
Longev 2009; 2:207-13 145. Abraham P, Rabi S, Kulothungan P. Aminoguanidine,
selective nitric oxide synthase inhibitor, ameliorates
cyclophosphamide-induced hemorrhagic cystitis by inhibiting protein nitration and PARS activation. Urology
2009; 73:1402-6.
146. Sakura M, Masuda H, Matsuoka Y, Yokoyama M, Kawakami S, Kihara K. Rolipram, a specific type-4
phosphodiesterase inhibitor, inhibits cyclophosphamide-
induced haemorrhagic cystitis in rats. BJU Int 2009; 103:264-9.
147. Hamsa TP, Kuttan G. Protective role of Ipomoea obscura
(L.) on cyclophosphamide-induced uro- and nephrotoxi-cities by modulating antioxidant status and pro-
inflammatory cytokine levels. Inflammopharmacology
2011; 19:155-67. 148. Abraham P, Isaac B, Ramamoorthy H, Natarajan K. Oral
Glutamine Attenuates Cyclophosphamide-Induced
Oxidative Stress in the Bladder but Does Not Prevent Hemorrhagic Cystitis in Rats. J Med Toxicol 2011; 7:118-
24.
149. Ayhanci A, Yaman S, Sahinturk V, Uyar R, Bayramoglu G, Senturk H, Altuner Y, Appak S, Gunes S. Protective
effect of seleno-L-methionine on cyclophosphamide-
induced urinary bladder toxicity in rats. Biol Trace Elem Res 2010; 134:98-108.
150. Santos AA Jr, Leal PC, Edelweiss MI, Lopes TG, Calixto JB, Morrone FB, Campos MM. Effects of the compounds
MV8608 and MV8612 obtained from Mandevilla velutina
in the model of hemorrhagic cystitis induced by cyclophosphamide in rats. Naunyn Schmiedebergs Arch
Pharmacol 2010; 382:399-407.
151. Chuang YC, Tyagi P, Huang HY, Yoshimura N, Wu M,
Kaufman J, Chancellor MB. Intravesical immune
suppression by liposomal tacrolimus in cyclophosphamide-
induced inflammatory cystitis. Neurourol Urodyn 2011; 30:421-7.
152. Vera PL, Iczkowski KA, Howard DJ, Jiang L, Meyer-
Siegler KL. Antagonism of macrophage migration

Ribeiro et al: Chemotherapy-induced hemorrhagic cystitis
DOI:10.5455/jeim.080312.ir.010 112
inhibitory factor decreases cyclophosphamide cystitis in mice. Neurourol Urodyn 2010; 29:1451-7.
153. Miki T, Matsunami M, Nakamura S, Okada H, Matsuya H,
Kawabata A. ONO-8130, a selective prostanoid EP1 receptor antagonist, relieves bladder pain in mice with
cyclophosphamide-induced cystitis. Pain 2011; 152:1373-
81. 154. Boeira VT, Leite CE, Santos AA Jr, Edelweiss MI, Calixto
JB, Campos MM, Morrone FB. Effects of the
hydroalcoholic extract of Phyllanthus niruri and its isolated compounds on cyclophosphamide-induced hemorrhagic
cystitis in mouse. Naunyn Schmiedebergs Arch Pharmacol
2011; 384:265-75. 155. Martins J, Silva R, Coutinho-Silva R, Takiya C, Battastini
A, Morrone F, Campos M. The role of P2X7 purinergic
receptors in inflammatory and nociceptive changes accompanying cyclophosphamide-induced haemorrhagic
cystitis in mice. Br J Pharmacol 2012; 165:183-96.