CLINICAL PHARMACOLOGY OF ANTIBACTERIAL AGENTS. Actions of antibacterial drugs on bacterial cells.
Upload
mohamed-bahrCategory
view
259download
2
CHEMOTHERAPYHIGHLIGHTS
MOHAMED BAHR; MD, PHD
Antibacterial Drugs

Mohamed Bahr; MD, PhD
CELL WALL INHIBITORS

Mohamed Bahr; MD, PhD
I. BETA-LACTAM ANTIBIOTICS

Mohamed Bahr; MD, PhD
A. PENICILLINS1928
Alexander Fleming

Mohamed Bahr; MD, PhD
Beta Lactam Ring

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Cell wall of gram +ve bacteria

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
PREPARATIONS

Mohamed Bahr; MD, PhD
1. NATURAL PENICILLINS (PENICILLIN G [BENZYLPENICILLIN], PENICILLIN V)
Narrow spectrum (gram +ve cocci and bacilli and gram -ve
cocci).
Penicillin V is acid-stable (PO); penicillin G is less stable (IM).
Inactivated by β-lactamase.

Mohamed Bahr; MD, PhD
2. ANTI-STAPH PENICILLINS (OXACILLIN, CLOXACILLIN, FLUCLOXACILLIN, NAFCILLIN)
Narrow spectrum as natural penicillins.
Stable to gastric acidity.
Stable to β-lactamase.

Mohamed Bahr; MD, PhD
3. BROAD-SPECTRUM PENICILLINS (AMPICILLIN AND AMOXICILLIN)
Broad-spectrum (as natural penicillins plus some gram -ve
bacilli).
Stable to gastric acidity.
Inactivated by β-lactamase.

Mohamed Bahr; MD, PhD
4. ANTIPSEUDOMONAL (OR EXTENDED-SPECTRUM) PENICILLINS (CARBENICILLIN INDANYL, TICARCILLIN, PIPERACILLIN)
Broad-spectrum including Pseudomonas and many gram -ve
bacilli. Piperacillin is also active against Klebseilla
pneumonia.
Unstable to gastric acidity (given parenterally).
Inactivated by β-lactamase.

Mohamed Bahr; MD, PhD
5. LONG-ACTING PENICILLINS (BENZATHINE PENICILLIN, PROCAINE PENICILLIN)
Insoluble salts of penicillin G →
allow slow drug absorption with
long duration of action (penicillin
G is short-acting; 6 hours).
Procaine penicillin: given /12
hours.
Benzathine penicillin: given
once/month.

Mohamed Bahr; MD, PhD
MRSA
VRvancomycin, rifampin

Mohamed Bahr; MD, PhD
ROUTE DETERMINED BY
Stability of the penicillin
Severity of infection

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
PENICILLINS CAN:Cross placenta
Cross inflamed meninges

Mohamed Bahr; MD, PhD
Essential features of BBB

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Elimination

Mohamed Bahr; MD, PhD
COMMON USESStreptococcal infections:
• Acute throat infections, wound sepsis, puerperal fever.
• Bacterial endocarditis: penicillin is given plus an aminoglycoside
(facilitate penetration of aminoglycosides by interfering with
bacterial cell wall synthesis → synergistic bactericidal effect).
Staphylococcal infections.
Pneumococcal infections.
Diphtheria, tetanus and gas gangrene (penicillin plus specific
antitoxins).

Mohamed Bahr; MD, PhD
COMMON USESMeningococcal meningitis: penicillin G or ampicillin IV plus
chloramphenicol.
Gonorrhea (alternative: fluorinated quinolones).
Typhoid and paratyphoid fever: amoxicillin and ampicillin.
Syphilis
Prophylaxis against:
• Recurrence of rheumatic fever: benzathine penicillin (1.2 million
units/month).
• Bacterial endocarditis (plus an aminoglycoside).

Mohamed Bahr; MD, PhD
Skin and Soft Tissue Infections Folliculitis
Furuncle, carbuncle
Cellulitis
Impetigo
Mastitis
Surgical wound infections
Hidradenitis suppurativa
Musculoskeletal InfectionsSeptic ar thritis
Osteomy elitis
Py omy os itis
Ps oas abs c es s
Respiratory Tract InfectionsVentila tor -as sociated or nos oc omia l pneumonia
Septic pu lmonary emboli
Pos tvir al pneumonia ( e.g., in fluenza)
Empyema
Bacteremia and Its ComplicationsSepsis, septic shock
Metastatic foci of infection (kidney, joints, bone, lung)
Infective endocarditis

Mohamed Bahr; MD, PhD
Infective EndocarditisInjection drug use–associated
Native-valve
Prosthetic-valve
Nosocomial
Device-Related Infections (e.g., intravascular catheters, prosthetic joints)
Toxin-Mediated Illnesses
Toxic shock syndrome
Food poisoning
Staphylococcal scalded-skin syndrome
Invasive Infections Associated with Community-Acquired MRSA
Necrotizing fasciitis
Waterhouse-Friderichsen syndrome
Necrotizing pneumonia
Purpura fulminans

Mohamed Bahr; MD, PhD
Penicillin G

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSHypersensitivity (most important). Maybe either direct effect, rashes
and phlebitis; or immunological (due to antigenic metabolites),
angioedema (marked swelling of lips, tongue, periorbital area) and
anaphylaxis. This is more with penicillin G, so its use is restricted.
Cross-allergy may occur between β-lactam antibiotics.
Diarrhea: disruption of normal balance of intestinal flora; more with
incompletely absorbed and broad-spectrum agents.
Seizures: IT - RF.
Cation disturbance: hyperkalemia with penicillin G.

Mohamed Bahr; MD, PhD
B. CEPHALOSPORINS

Mohamed Bahr; MD, PhD
1st Generation Cephalexin (PO)Cefazolin (IV)
G +ve cocci (Strept - Staph), some G -ve organisms (E coli - Klebsiella)
Cephalexin: Broad spectrum in URTI, UTI
Cefazolin: 1st choice in surgical prophylaxisIn orthopedic surgery: penetrates bone well, penicillinase resistant (Staph)
2nd GenerationCefaclor (PO)Cefuroxime (IV)Cephamycins (cefoxitin, cefotetan, cefmetazole) (IV)
Less active on G +ve, extended spectrum on G -ve organismsCephamycins: aerobic and anerobic G –ve bacilli
Oral agents are used in sinusititis, otitis
Cefuroxime: also in community acquired pneumonia (H influenza).
Cephamycins are structurally related to cephalosporins, used in mixed anaerobic infections (including B fragillis), e.g., peritonitis

Mohamed Bahr; MD, PhD
3rd Generation Cefoperazone, Cefotaxime, Ceftriaxone (IV)
↑ activity against resistant G -ve organisms (e.g. Pseudomonas)
Used in serious infections
Most agents cross BBB (used in meningitis)
Ceftriaxone (Longest t½): used in gonorrhea (single injection), typhoid (resistant cases)Bone: good penetration. BBB: crosses BBB, so can be used in meningitis. Bile: excreted in bile (40%), used in biliary infection and in renal dysfunction.
4th Generation Cefepime (IV)
Similar spectrum to 3rd generation on G –ve, effective on penicillin-resistant Strept and Staph
Crosses BBB well

Mohamed Bahr; MD, PhD
5th Generation: Ceftarolene fosamil (IV)
Broad spectrum prodrug, effective against MRSA,
VRSA, H influenza, G -ve organisms (plus
aminoglycosides).
Used in skin infections and community-acquired
pneumonia.
Adjust dose in renal impairment.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Reverse type, PO

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSHypersensitivity: cross-allergy with penicillins → avoided in patients
with serious (immediate) hypersensitivity to penicillin.
Hypoprothrombinemia and bleeding.
Nephrotoxicity especially if used with aminoglycosides.
Local irritation → severe pain after IMI and thrombophlebitis after IVI.
Intolerance to alcohol → disulfiram-like reaction.
Cross-resistance with penicillins: avoided in penicillin-resistant
infections.

Mohamed Bahr; MD, PhD
C. CARBAPENEMS: IMIPENEM (IV) BROADEST
Effective against gram +ve, -ve organisms and anaerobes.
Resistant to β-lactamase.
High cross-allergy with penicillin.
High risk of toxicity:
• Metabolized in the kidney to an inactive nephrotoxic metabolite, thus
it is given with cilastatin to inhibit renal metabolism.
• High risk of convulsion → avoided in meningitis.
Meropenem and ertapenem are similar to imipenem with less renal
degradation (cilastatin is not required) and less risk of convulsions.

Mohamed Bahr; MD, PhD
D. MONOBACTAMS: AZTREONAM (IV & IM) NARROW
Effective against aerobic gram -ve organisms (as
aminoglycosides).
Resistant to β-lactamase.
No cross-allergy with β-lactams.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
COMBINATION

Mohamed Bahr; MD, PhD
II. VANCOMYCIN G+, IVI• Staph resistant to penicillin (MRSA): drug of choice. It is used
in serious infections as Staph pneumonia, endocarditis and
osteomyelitis.
• Severe Staph infections in patients allergic to penicillins or
cephalosporins.
• Pseudomembranous colitis following antibiotic use.

Mohamed Bahr; MD, PhD
Vancomycin

Mohamed Bahr; MD, PhD Daptomycin

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS• Fever, chills, rigors and phlebitis.
• Shock with rapid infusion → red man syndrome (due to
histamine release). Avoided by slow infusion and
pretreatment with antihistamines.
• Ototoxic.
• Nephrotoxic.

Mohamed Bahr; MD, PhD
DRUG-INDUCED PSEUDOMEMBRANOUS COLITIS
Clindamycin.
Broad-spectrum antimicrobials: tetracyclines, co-trimoxazole, chloramphenicol → kill intestinal flora → flourishing of Clostridium difficile (G +ve anaerobe) and its toxins → colitis
Treatment
Vancomycin
Metronidazole
Cholestyramine (Why?)

Mohamed Bahr; MD, PhD
Broad-spectrum antimicrobials can induce pseudomembranous colitis

Mohamed Bahr; MD, PhD
CELL MEMBRANEINHIBITORS

Mohamed Bahr; MD, PhD
DAPTOMYCIN G+, IV/ IMMore rapidly bactericidal. Vancomycin-resistant organisms.
Skin and soft tissue infections.
Bacteremia and endocarditis.
Adverse effects
1. GIT upset and elevated liver enzymes.
2. Myopathy → avoid with statins.

Mohamed Bahr; MD, PhD
PROTEIN SYNTHESISINHIBITORS

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
I. TETRACYCLINES

Mohamed Bahr; MD, PhD
USES

Mohamed Bahr; MD, PhD
PHARMACOKINETICSPO
Bile
Bone
BBB
Urine
Pregnancy

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS AND CONTRAINDICATIONS• Epigastric pain due to gastric irritation (noncompliance).
• Teeth discoloration and bone hypoplasia.
• Hepatotoxicity (in renal failure or pregnancy).
• Phototoxicity (sensitivity of skin to sun light).
• Superinfection with Candida, C difficile or resistant Staph in intestine.
• Fanconi-like syndrome: renal tubular dysfunction with outdated
tetracyclines.
• Contraindicated in renal dysfunction.

Mohamed Bahr; MD, PhD
TIGECYCLINE (SLOW IVI)• Similar to tetracycline in structure, mechanism, and adverse
effects; with less resistance.
• Effective against gram +ve, gram -ve, and anaerobes; a wide
variety of multidrug-resistant nosocomial infections.
• Causes nausea.
• Adjust in liver impairment.

Mohamed Bahr; MD, PhD
II. AMINOGLYCOSIDES

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
SPECTRUM AND ACTIVITY• Effective against aerobic organisms.
• Ineffective against anaerobes (requires O2 for transport into
cells).
• Act mainly against gram -ve organisms, e.g., E coli,
Pseudomonas, cholera.
• Gentamycin is also effective against Staph infections.
• Amikacin resists bacterial enzymatic inactivation, thus it is the
most effective aminoglycoside against gram -ve bacilli.

Mohamed Bahr; MD, PhD
PHARMACOKINETICS• Absorption: not absorbed orally thus have to be given
parenterally.
• Distribution: do not cross BBB even when meninges are
inflamed. They are concentrated in renal cortex, perilymph and
endolymph of inner ear → nephrotoxicity and ototoxicity.
• Excretion: unchanged through the kidney (care in renal
dysfunction).

Mohamed Bahr; MD, PhD
THERAPEUTIC USES• Peritonitis, septicemia, pneumonia.
• Complicated UTI.
• Bacterial endocarditis.
• Streptomycin is used in TB.
• Amikacin and netilmicin are reserved for resistant cases.
• Neomycin (too nephrotoxic for systemic use): used orally in
hepatic coma and intestinal antiseptic before surgery (not
absorbed) and topically in infected wounds.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS Nephrotoxicity: acute tubular necrosis (may be irreversible).
Risk ↑ by dehydration, old age, ↑ dose, ↑ duration or concurrent
use of nephrotoxic drugs.
Ototoxicity: may be irreversible. Coadministration of loop
diuretics or quinidine → ↑ risk.
Neuromuscular paralysis (inhibit ACh release), especially after
intraperitoneal or intrapleural infusion of large doses.
Allergy: contact dermatitis with topically applied neomycin.

Mohamed Bahr; MD, PhD
SPECTINOMYCIN
Gonorrhea in patients allergic to
penicillin or patients with penicillin-
resistant gonococcal infection
(single deep IMI).

Mohamed Bahr; MD, PhD
III. MACROLIDES

Mohamed Bahr; MD, PhD
Macrolides

Mohamed Bahr; MD, PhD
Erythromycin
Clarithromycin Azithromycin Roxithromycin

Mohamed Bahr; MD, PhD
SPECTRUM AND USESChlamydia, Mycoplasma, Spirochetes, gram +ve cocci
and bacilli as an alternative to penicillins and
tetracyclines. They are of choice in:
Patients with allergy to β lactam antibiotics.
Urogenital Chlamydia infection in pregnancy.
Mycoplasma pneumonia in children (tetracyclines are
contraindicated).

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSEpigastric pain and GIT distress (increases bowel
motility).
Cholestatic jaundice (erythromycin estolate). CI in
liver disease.
Ototoxicity and may lead to transient deafness.
Thrombophlebitis if injected IV.
Prolonged QT interval.

Mohamed Bahr; MD, PhD
Enzyme inhibitor: ↑ level of theophylline,
warfarin, carbamazepine and terfenadine (→
arrhythmias).
↑ Digoxin level (inhibits intestinal flora that
inactivate digoxin).

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
IV. CLINDAMYCIN
Bone
Anaerobic
Pseudomembranous
colitis

Mohamed Bahr; MD, PhD
V. CHLORAMPHENICOLRarely used
Typhoid fever (not carrier), but replaced by fluoroquinolones.
Bacterial meningitis (e.g., H influenza) plus penicillin.
Anaerobic infection, e.g., anaerobic brain abscess.
Topically in eye infections.

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSGIT upsets and superinfection.
Bone marrow depression: may be dose-independent or
idiosyncratic.
Gray baby syndrome in neonates (↓ drug clearance due to
undeveloped liver and kidney functions).
Optic neuritis.
Enzyme inhibitor: ↑ warfarin, phenytoin and oral hypoglycemics
level.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
VI. STREPTOGRAMINS: QUINUPRISTIN/DAFLOPRISTIN (IVI)
Complex with bacterial 50S ribosomal subunits to
inhibit protein synthesis.
Serious infections with resistant gram +ve organisms,
e.g., MRSA and Streptococcus pneumoniae (when?)

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS
Arthralgia and myalgia.
Thrombophlebitis.
Enzyme inhibitor (similar to erythromycin).

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
VII. OXAZOLIDINONES: LINEZOLID
Binds to a unique site on the 50S subunit →
inhibits initiation complex → inhibits protein
synthesis.

Mohamed Bahr; MD, PhD
Linezolid

Mohamed Bahr; MD, PhD
SPECTRUM AND USES (PO, IV; 100% F)
Restricted to serious infections with gram +ve
organisms resistant to vancomycin or MRSA in
patients intolerant to vancomycin or if IV
access is unavailable.

Mohamed Bahr; MD, PhD
Linezolid

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS
GIT: Nausea, vomiting and diarrhea.
Thrombocytopenia.

Mohamed Bahr; MD, PhD
NUCLEIC ACID INHIBITORS

Mohamed Bahr; MD, PhD
I. QUINOLONES

Mohamed Bahr; MD, PhD
Inhibit bacterial:
topoisomerase II (DNA gyrase)
topoisomerase IV

Mohamed Bahr; MD, PhD
Nonfluorinated Quinolones
1st - generation•Nalidixic Acid•Not used in systemic infections, as 90% of drug is bound to plasma proteins → insufficient plasma conc.•Used only in UTI with G -ve bacilli•Rapid resistance limits its use
Fluorinated Quinolones
2nd to 4th generation•2nd → 4th Generation•Newer Fluorinated derivatives achieving systemic levels•Used in systemic Infections

Mohamed Bahr; MD, PhD
GENERATIONS OF FLUOROQUINOLONES
Originally developed because of their excellent
activity against gram -ve aerobic bacteria; they
had limited activity against gram +ve
organisms.
Several newer agents have improved activity
against … and …

Mohamed Bahr; MD, PhD
2ND GENERATIONNORFLOXACIN - CIPROFLOXACIN - OFLOXACIN - PEFLOXACIN
Norfloxacin
the least active against both gram -ve and gram +ve organisms. Only in UTI as it
does not achieve systemic levels.
Newer agents
excellent gram -ve activity
moderate to good activity against gram +ve bacteria
MRSA?
Ciprofloxacin
the most active fluoroquinolone against gram -ve organisms esp. Pseudomonas.

Mohamed Bahr; MD, PhD
3RD GENERATION LEVOFLOXACIN
Greater activity on G +ve, including
Streptococcus pneumoniae

Mohamed Bahr; MD, PhD
4TH GENERATIONMOXIFLOXACIN - CLINAFLOXACIN
Improved activity against gram +ve organisms,
particularly S pneumoniae and some Staph.
Fluoroquinolones also are active against agents of
atypical pneumonia (e.g., Mycoplasma and
Chlamydiae) and against intracellular pathogens
such as Legionella species and some Mycobacteria.
Potent against anaerobic bacteria.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
THERAPEUTIC USESUTI (gram -ve bacilli) and prostatitis.
RTI resistant to β-lactams and atypical pneumonia due to chlamydia,
mycoplasma, legionella (levofloxacin- moxifloxacin).
Typhoid and infective diarrhea (ciprofloxacin: 1st choice for empiric
therapy).
Gonorrhea (ofloxacin single dose, levofloxacin).
Bone and soft tissue infection.
Resistant TB.
Anaerobes.

Mohamed Bahr; MD, PhD
ADVERSE EFFECTS AND CONTRAINDICATIONS (CI)GIT: Nausea, vomiting and diarrhea (most common).
CNS: Headache, dizziness, insomnia, convulsions in susceptible
patients.
Phototoxicity.
Hepatotoxicity.
Reversible arthropathy (children < 18 years).
Prolonged QT.
Enzyme inhibitor.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
CI
Quinolones are contraindicated in
pregnancy and lactation.
Not routinely recommended in patients <18
years (→ arthropathy).

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Fluoroquinolones

Mohamed Bahr; MD, PhD
II. RIFAMPINBinds and inhibits DNA-dependent RNA polymerase →
inhibition of RNA synthesis.

Mohamed Bahr; MD, PhD
SPECTRUM
Effective against mycobacteria at all sites and
leprosy.
Potent broad spectrum bactericidal. Effective
against MRSA.
Antiviral effect.

Mohamed Bahr; MD, PhD
PHARMACOKINETICSWell absorbed after oral administration.
Widely distributed in body tissues and fluids and can reach TB
cavities and sputum and penetrate macrophages killing slowly
growing TB bacilli inside.
Crosses BBB.
Metabolized in the liver and it is a potent enzyme inducer.
Excreted mainly in bile (enterohepatic recycling) and slightly in
urine.

Mohamed Bahr; MD, PhD
THERAPEUTIC USES
TB (main use), leprosy.
MRSA.
Meningitis Prophylaxis.
Brucellosis; plus doxycycline (1st choice).

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSRed discoloration of urine, tears, sputum and soft contact
lenses.
Flu-like syndrome (malaise, headache and fever...).
Liver damage and jaundice.
Resistance: rapid (but no cross-resistance with other anti-TB
drugs).
Enzyme induction (serious drug interactions).

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
FOLATE INHIBITORS

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
SULFONAMIDES
SulfamethoxazoleSulfadoxineSulfadiazineSulfasalazineSulfacetamide
bacteria (TMP+SMX)malariaburnscolon (ulcerative colitis)eyes (eye infection)

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSGIT: nausea, vomiting, diarrhea.
Hypersensitivity reactions, rashes, fever, exfoliative dermatitis. Steven-
Johnson Syndrome.
Crystalluria and nephrotoxicity: metabolites formed in liver precipitate in
acidic urine. Advise fluid intake and urine alkalinization.
Hematopoietic disturbances: granulocytopenia and thrombocytopenia,
hemolytic anemia in G6PD deficiency.
Kernicterus (jaundice and CNS affection): displace bilirubin from plasma
protein. Free bilirubin crosses BBB (immature in newly-born) and
reaches CNS.

Mohamed Bahr; MD, PhD
TRIMETHOPRIMMegaloblastic anemia (folate deficiency),
Granulocytopenia and leucopenia.

Mohamed Bahr; MD, PhD
CO-TRIMOXAZOLESMX-TMP 400/80UTI, gonococcal urethritis and prostatitis.
RTI due to H influenza and S pneumoniae.
Typhoid fever.

Mohamed Bahr; MD, PhD
ADVANTAGES?Synergistic combination.
Less and delayed bacterial resistance
More potent (Bactericidal) and wider-spectrum including
Proteus, Salmonella, Shigella, H. influenza and
Gonococcus.

Mohamed Bahr; MD, PhD
Growth of E coli

Mohamed Bahr; MD, PhD
ANTITUBERCULOUS DRUGS

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
1st Line Drugshigh efficacy - accepted toxicity• Rifampin: affects the organisms at all sites• Isoniazid (INH): affects intracellular and extracellular organisms
• Pyrazinamide:affects mainly intracellular organisms (resistant
strains)• Ethambutol• Streptomycin: affects only extracellular organisms 2nd Line Drugsresistance/ intolerance• Ceftriaxone• Clarithromycin• Fluoroquinolones (ciprofloxacin, levofloxacin and moxifloxacin)• Cycloserine (peripheral neuritis and CNS dysfunction)• Ethionamide (peripheral and optic neuritis)• Capreomycin (nephrotoxic and ototoxic)

Mohamed Bahr; MD, PhD
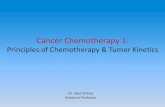
INH (CELL WALL MYCOLIC ACID)Good PO
Slow vs. Rapid

Mohamed Bahr; MD, PhD
ADVERSE EFFECTSHypersensitivity.
Neurotoxicity with slow acetylators (B6 deficiency):
peripheral neuritis, optic neuritis, memory impairment and
convulsions → vitamin B6 supplements.
Hepatitis: rare but fatal, risk is increased with age.
Enzyme inhibitor: ↑ phenytoin and carbamazepine serum
level.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
Bimodal distribution of isoniazid half-lives caused by rapid and slow acetylation of the drug

Mohamed Bahr; MD, PhD
PYRAZINAMIDE(FAS-I GENE)Good PO
TB meningitis

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
ETHAMBUTOL (RNA)Bacteriostatic. It enters active mycobacteria → inhibit RNA
synthesis.
Side Effects: optic neuritis → red/green color blindness - ↓
visual acuity.

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
LEPROSY

Mohamed Bahr; MD, PhD

Mohamed Bahr; MD, PhD
ANTILEPROTIC DRUGSDrug combinations are used to ↓resistance:
Paucibacillary leprosy: dapsone + rifampin (for 6 months).
Multibacillary leprosy: dapsone + rifampin + clofazimine (for
2 years).

Mohamed Bahr; MD, PhD
1. Rifampin: the most active agent.

Mohamed Bahr; MD, PhD
2. Dapsone
Bacteriostatic. It is related to sulfonamides and achieves ↑ skin
concentration.
Antagonist to PABA → inhibits folate synthesis.
Adverse Effects
Hemolysis (esp. in G6PD deficiency) - methemoglobuinemia.
PN.
Erythema nodosum leprosum (ENL) → suppressed by corticosteroids.

Mohamed Bahr; MD, PhD
3. Clofazimine (PO)
A dye accumulating in phagocytes and skin → bactericidal effect
through:
• Binding to DNA, preventing template formation and DNA
replication.
• Formation of cytotoxic oxygen radicals.
Anti-inflammatory: no ENL → used in patients developing ENL
with dapsone.
Adverse effects: skin discoloration (red-brown) - enteritis.

Mohamed Bahr; MD, PhD
REFERENCESLippincott’s Illustrated Reviews, 5th ed.
Color Atlas of Pharmacology, 2nd ed.
Goodman and Gilman's The Pharmacological Basis of
Therapeutics, 12th ed.