Characteristics of referred muscle pain to the head from ... · trigger points in women with...
13
ORIGINAL Characteristics of referred muscle pain to the head from active trigger points in women with myofascial temporomandibular pain and fibromyalgia syndrome Cristina Alonso-Blanco • Ce ´sar Ferna ´ndez-de-las-Pen ˜as • Ana Isabel de-la-Llave-Rinco ´n • Pedro Zarco-Moreno • Fernando Gala ´n-del-Rı ´o • Peter Svensson Received: 21 July 2012 / Accepted: 18 August 2012 / Published online: 31 August 2012 Ó The Author(s) 2012. This article is published with open access at Springerlink.com Abstract Our aim was to compare the differences in the prevalence and the anatomical localization of referred pain areas of active trigger points (TrPs) between women with myofascial temporomandibular disorder (TMD) or fibro- myalgia (FMS). Twenty women (age 46 ± 8 years) with TMD and 20 (age 48 ± 6 years) with FMS were recruited from specialized clinic. Bilateral temporalis, masseter, ster- nocleidomastoid, upper trapezius, and suboccipital muscles were examined for TrPs. TrPs were identified by palpation and considered active when the pain reproduced familiar pain symptom experienced by the patient. The referred pain areas were drawn on anatomical maps, digitalized and also measured. A new analysis technique based on a center of gravity (COG) method was used to quantitative estimate of the localization of the TrP referred pain areas. Women with FMS exhibited larger areas of usual pain symptoms than women with myofascial TMD (P \ 0.001). The COG coordinates of the usual pain on the frontal and posterior pain maps were located more superior in TMD than in FMS. The number of active TrPs was significantly higher in TMD (mean ± SD 6 ± 1) than in FMS (4 ± 1) (P = 0.002). Women with TMD exhibited more active TrPs in the tem- poralis and masseter muscles than FMS (P \ 0.01). Women with FMS had larger referred pain areas than those with TMD for sternocleidomastoid and suboccipital muscles (P \ 0.001). Significant differences within COG coordinates of TrP referred pain areas were found in TMD, the referred pain was more pronounced in the orofacial region, whereas the referred pain in FMS was more pronounced in the cer- vical spine. This study showed that the referred pain elicited from active TrPs shared similar patterns as usual pain symptoms in women with TMD or FMS, but that distinct differences in TrP prevalence and location of the referred pain areas could be observed. Differences in location of referred pain areas may help clinicians to determine the most relevant TrPs for each pain syndrome in spite of overlaps in pain areas. Keywords Temporomandibular disorders Fibromyalgia Trigger points Referred pain Pain assessment C. Alonso-Blanco Department of Nursing, Universidad Rey Juan Carlos, Alcorco ´n, Madrid, Spain C. Ferna ´ndez-de-las-Pen ˜as A. I. de-la-Llave-Rinco ´n F. Gala ´n-del-Rı ´o Department of Physical Therapy, Occupational Therapy, Rehabilitation and Physical Medicine, Universidad Rey Juan Carlos, Alcorco ´n, Madrid, Spain C. Ferna ´ndez-de-las-Pen ˜as A. I. de-la-Llave-Rinco ´n F. Gala ´n-del-Rı ´o Esthesiology Laboratory of Universidad Rey Juan Carlos, Alcorco ´n, Spain C. Ferna ´ndez-de-las-Pen ˜as (&) Facultad de Ciencias de la Salud, Universidad Rey Juan Carlos, Avenida de Atenas s/n, 28922 Alcorco ´n, Madrid, Spain e-mail: [email protected]; [email protected] P. Zarco-Moreno Department of Rheumatology, Fundacio ´n Hospital Alcorco ´n, Alcorco ´n, Spain P. Svensson Department of Clinical Oral Physiology, School of Dentistry, University of Aarhus, Aarhus, Denmark P. Svensson Department of Oral and Maxillofacial Surgery, Aarhus University Hospital, Aarhus, Denmark P. Svensson Orofacial Pain Laboratory, Center for Sensory-Motor Interaction, Aalborg University, Aalborg, Denmark 123 J Headache Pain (2012) 13:625–637 DOI 10.1007/s10194-012-0477-y
Transcript of Characteristics of referred muscle pain to the head from ... · trigger points in women with...

ORIGINAL
Characteristics of referred muscle pain to the head from activetrigger points in women with myofascial temporomandibularpain and fibromyalgia syndrome
Cristina Alonso-Blanco • Cesar Fernandez-de-las-Penas •
Ana Isabel de-la-Llave-Rincon • Pedro Zarco-Moreno •
Fernando Galan-del-Rıo • Peter Svensson
Received: 21 July 2012 / Accepted: 18 August 2012 / Published online: 31 August 2012
� The Author(s) 2012. This article is published with open access at Springerlink.com
Abstract Our aim was to compare the differences in the
prevalence and the anatomical localization of referred pain
areas of active trigger points (TrPs) between women with
myofascial temporomandibular disorder (TMD) or fibro-
myalgia (FMS). Twenty women (age 46 ± 8 years) with
TMD and 20 (age 48 ± 6 years) with FMS were recruited
from specialized clinic. Bilateral temporalis, masseter, ster-
nocleidomastoid, upper trapezius, and suboccipital muscles
were examined for TrPs. TrPs were identified by palpation
and considered active when the pain reproduced familiar
pain symptom experienced by the patient. The referred pain
areas were drawn on anatomical maps, digitalized and also
measured. A new analysis technique based on a center of
gravity (COG) method was used to quantitative estimate of
the localization of the TrP referred pain areas. Women with
FMS exhibited larger areas of usual pain symptoms than
women with myofascial TMD (P \ 0.001). The COG
coordinates of the usual pain on the frontal and posterior
pain maps were located more superior in TMD than in FMS.
The number of active TrPs was significantly higher in TMD
(mean ± SD 6 ± 1) than in FMS (4 ± 1) (P = 0.002).
Women with TMD exhibited more active TrPs in the tem-
poralis and masseter muscles than FMS (P \ 0.01). Women
with FMS had larger referred pain areas than those with
TMD for sternocleidomastoid and suboccipital muscles
(P \ 0.001). Significant differences within COG coordinates
of TrP referred pain areas were found in TMD, the referred
pain was more pronounced in the orofacial region, whereas
the referred pain in FMS was more pronounced in the cer-
vical spine. This study showed that the referred pain elicited
from active TrPs shared similar patterns as usual pain
symptoms in women with TMD or FMS, but that distinct
differences in TrP prevalence and location of the referred
pain areas could be observed. Differences in location of
referred pain areas may help clinicians to determine the most
relevant TrPs for each pain syndrome in spite of overlaps in
pain areas.
Keywords Temporomandibular disorders � Fibromyalgia �Trigger points � Referred pain � Pain assessment
C. Alonso-Blanco
Department of Nursing, Universidad Rey Juan Carlos,
Alcorcon, Madrid, Spain
C. Fernandez-de-las-Penas � A. I. de-la-Llave-Rincon �F. Galan-del-Rıo
Department of Physical Therapy, Occupational Therapy,
Rehabilitation and Physical Medicine, Universidad Rey
Juan Carlos, Alcorcon, Madrid, Spain
C. Fernandez-de-las-Penas � A. I. de-la-Llave-Rincon �F. Galan-del-Rıo
Esthesiology Laboratory of Universidad
Rey Juan Carlos, Alcorcon, Spain
C. Fernandez-de-las-Penas (&)
Facultad de Ciencias de la Salud, Universidad Rey Juan Carlos,
Avenida de Atenas s/n, 28922 Alcorcon, Madrid, Spain
e-mail: [email protected]; [email protected]
P. Zarco-Moreno
Department of Rheumatology,
Fundacion Hospital Alcorcon, Alcorcon, Spain
P. Svensson
Department of Clinical Oral Physiology, School of Dentistry,
University of Aarhus, Aarhus, Denmark
P. Svensson
Department of Oral and Maxillofacial Surgery,
Aarhus University Hospital, Aarhus, Denmark
P. Svensson
Orofacial Pain Laboratory, Center for Sensory-Motor
Interaction, Aalborg University, Aalborg, Denmark
123
J Headache Pain (2012) 13:625–637
DOI 10.1007/s10194-012-0477-y

Introduction
Temporomandibular (TMD) pain is a musculoskeletal local
pain condition with a prevalence rate between 3 and 15 %,
an incidence rate between 2 and 4 % [1] and a women–men
ratio 2:1 [2]. Similar, fibromyalgia (FMS) is a widespread
diffuse musculoskeletal pain condition with a prevalence
ranging from 0.5 % to 5.0 and a higher proportion of
women [3, 4]. Although the etiology and pathology
of TMD and FMS are under debate, there is evidence of
facilitated nociceptive processes in both conditions. In fact,
TMD pain has been frequently diagnosed on fibromyalgia
subjects [5, 6] whereas the presence of widespread pain has
been shown to be a significant risk factor for myofascial
TMD [7]. A recent study has found an increased risk for the
onset of clinically significant TMD pain when subjects also
had FMS [8]. Therefore, it seems that TMD and FMS may
share some patho-physiological mechanisms.
In the last years, there has been an increasing interest for
the role of myofascial trigger points (TrPs) in both TMD [9]
and FMS [10]. TrPs are defined as hypersensitive spots
within a taut band of a skeletal muscle that are painful on
stimulation and give rise to a referred distant pain [11].
Active TrPs are spots with local and referred pain that
reproduce the clinical pain symptom experienced by the
patient and associated with the usual pain reported by the
patient. Latent TrPs have similar clinical findings as active
TrPs, but, in contrast, they do not mimic the painful symp-
toms [11]. Clinical distinction between active and latent TrPs
is substantiated by histo-chemical findings because higher
levels of neuroactive mediators (i.e., bradykinin, substance
P, or serotonin) have been found in active TrPs compared
with latent TrPs and non-TrP [12, 13].
Two recent studies have demonstrated that referred pain
from TrPs in the head and neck muscles reproduced
symptoms in women with myofascial TMD [14] or FMS
[15]. Nevertheless, these previous studies did not provide a
quantitative estimation of the localization of referred pain
areas. Two previous studies have used a new analysis
technique based on a centre of gravity (COG) method to
estimate the localization of the referred pain areas elicited
by injection of hypertonic saline into head and neck mus-
cles in healthy subjects [16, 17]. With this technique it
would be possible to estimate the anatomical localization
of the referred pain elicited by active TrPs in pain popu-
lations. Previous studies demonstrated that FMS is highly
co-morbid with primary headaches such as tension-type
and migraine headaches [18, 19] and TMD [5–7]. The
identification and quantification of differences in TrP dis-
tribution and location of the referred pain between patients
with TMD or FMS could be helpful for better clinical
identification of pain patterns in these populations in spite
of overlaps in symptomatology and clinical presentation of
pain. In addition, identification of those muscles most
affected by TrP in each group of patients could possibly
also be helpful for better management of TrP in these
populations. Application of the COG technique with
quantification of overlapping pain patterns in the head
could therefore be an important novel feature in a more
standardized description of patients with TMD and FMS.
To the best of the authors’ knowledge, no previous study
has investigated the differences in the prevalence of active
muscle TrPs and the anatomical localization of the referred
pain areas between patients with TMD and FMS. There-
fore, the aims of the current study were to compare the
differences in the prevalence and the anatomical localization
of referred pain areas of active TrPs in head and neck–
shoulder musculature between women with strict myofascial
TMD and FMS.
Methods
Participants
In the current study, women with a main diagnosis of FMS
or myofascial TMD were included. Participants were
recruited among patients referred from a tertiary special-
ized clinic on chronic pain in Madrid, Spain. They were
carefully screened and explored to further determine the
inclusion and exclusion criteria by an experienced dentist
(TMD group) or rheumatologist (FMS group). All patients
had prior to the referral received treatment but without
adequate pain relief, i.e., they represented, at least in part, a
treatment resistant proportion of myofascial TMD and
FMS patients.
To be included in the TMD group, women should fulfill
a primary and exclusive diagnosis of myofascial TMD
according to the Research Diagnostic Criteria for TMD
(RDC/TMD) [20]. Pain location, range of jaw motion,
temporomandibular joint (TMJ) pain, clicking sounds,
crepitation, and pain upon palpation of muscles and TMJ
were assessed with the use of the RDC/TMD criteria. Pain
should be presented with duration of at least 3 months and
an intensity of at least 3 on an 11-point numerical pain
rating scale (NPRS; 0: no pain; 10: maximum pain). Sub-
jects were excluded if they exhibited any of the following:
1, signs or symptoms according to categories II-III of the
RDC-TMD criteria (disc displacement, arthralgia, osteo-
arthrosis or osteoarthritis); 2, TMJ surgery or steroid
injections; 3, comorbid fibromyalgia; 4, diagnosis of any
systemic disease (rheumatoid arthritis, systemic lupus
erythematosis, psoriatic arthritis); 5, previous cervical or
head trauma; 6, presence of a score[8 points in the BDI-II;
7, diagnosis of primary headache (tension-type headache or
migraine); or, 8, cognitive impairment.
626 J Headache Pain (2012) 13:625–637
123

To be included within the FMS group, women should
fulfil the criteria from the American College of Rheuma-
tology (ACR) [21]. Tender points were tested by digital
palpation at the nine paired sites according to the ACR by
an experienced rheumatologist. The presence of wide-
spread pain, fatigue and altered sleep was also recorded. In
this group, the presence of TMD symptoms was not con-
sidered as exclusion criteria. Subjects were excluded if
presented any of the following: 1, severe physical dis-
ability; 2, comorbid conditions (inflammatory disease,
irritable bowel syndrome, interstitial cystitis); 3, uncon-
trolled endocrine disorders (hypo-thyroidism, diabetes); 4,
diagnosis of primary headaches (tension-type headache or
migraine); 5, malignancy; 6, psychiatric illnesses (schizo-
phrenia or substance abuse); 7, medication usage other than
as-needed analgesics (excluding long-term narcotics); 8,
history of surgery; 9, previous history of whiplash injury;
10, presence of a score [8 points in the BDI-II; or, 11,
cognitive impairment.
The study protocol was approved by local Ethics
Committee (URJC 08-30) and conducted following the
Helsinki Declaration. All participants signed informed
consent prior to their inclusion.
Self-reported measures
A numerical pain rate scale (NPRS) was used to assess the
usual level of pain, worst and lowest level of pain expe-
rienced in the preceding week at rest in the orofacial area
[22]. In the present study, the usual level of pain was
related to pain experienced normally by the patient, and not
the pain level on the day of examination. Women with
FMS were asked to focus the pain assessment on the oro-
facial region. They were also asked to draw the distribution
of their usual pain pattern within an anatomical map
including lateral, frontal, and occipital projections of the
face (dimensions 65 9 80 mm, Fig. 1).
The Beck Depression Inventory (BDI-II) a 21-item self-
report measure assessing affective, cognitive and somatic
symptoms of depression, was used to exclude patients with
depressive symptoms (BDI-II [8 points) [23]. The BDI-II
has shown good internal consistency (a = 0.86) with higher
scores indicating higher levels of depression [24, 25].
Muscle trigger point (TrP) examination
Trigger points were bilaterally explored within the tem-
poralis, masseter, upper trapezius, sternocleidomastoid and
suboccipital muscles by an examiner with more than
10 years’ experience in muscle TrP examination. TrP
diagnosis was done following the criteria as described by
Simons et al. [11]: 1, presence of a palpable taut band in a
skeletal muscle; 2, presence of a sensitive spot within the
taut band; 3, local twitch response elicited by the snapping
palpation of the taut band; and 4, presence of referred pain
in response to TrP compression (approximately 20 N force
for 5 s). Gerwin et al. [26] found that these criteria, when
applied by an experienced examiner, have good inter-
examiner reliability (kappa) ranging from 0.84 to 0.88.
Trigger point diagnosis within the suboccipital muscles
was made when there was local tenderness in the suboc-
cipital region, referred pain with maintained pressure for
10 s and increased referred pain with active extension of
the upper cervical spine [27].
Trigger points were considered active when both the
local and the referred pain evoked by the compression
reproduced the usual pain symptoms, and the elicited pain
was familiar for the participant [11]. For that purpose, after
TrP assessment on each muscle, subjects were asked:
‘‘When I pressed this muscle, did you feel pain or dis-
comfort locally, and in another area (referred pain). If yes,
please tell me whether the pain that you felt in the other
area reproduced the pain that you normally experience.’’
The order of muscle TrP evaluation was randomized
Fig. 1 Schematic presentation of the center-of-gravity (COG) technique. The X and Y coordinates of the COG were calculated in a 13 9 16 grid
system (see ‘‘Methods’’)
J Headache Pain (2012) 13:625–637 627
123

between participants. As both groups have pain symptoms,
TrP assessment was conducted in a blinded fashion in
relation to specific diagnosis.
Assessment of referred pain area and center of gravity
(COG)
Local pain was defined as pain located around the com-
pression site, and referred pain was defined as the pain
located at least 1 cm outside the local pain area evoked by
TrP palpation. Participants were asked to draw the distri-
bution of the referred pain after palpation of each muscle
TrP on the same anatomical map including lateral, frontal,
and occipital projections of the face/neck (dimensions:
65 9 80 mm). Specific information on possible referral
patterns was avoided in order not to induce bias [28]. The
usual pain area and the TrPs referred pain areas were
measured with a digitizer (ACECAD, model D9000 ?
digitizer, Taiwan) to calculate the area of perceived pain
expressed in arbitrary units (au).
To obtain a quantitative estimate of the localization of
the perceived pain areas, usual pain symptoms or referred
pain areas elicited by active TrPs, the centre-of-gravity
(COG) was calculated according to previous studies [16,
17]: a grid outline with 5-mm resolutions (i.e., a total of
13 9 16 = 208 grids) was superimposed on lateral, frontal
and occipital pain maps (Fig. 1). Each grid in the coordi-
nate system was assigned a value on a dichotomous basis
(0: no pain, 1: pain). The COG coordinates (X anterior–
posterior, Y inferior–superior) in arbitrary units (au) were
calculated according to the following formula:
x ¼X13
i¼0
X16
j¼0
xi � grid valuei;j
� �=X13
i¼0
X16
j¼0
grid valuei;j
y ¼X13
i¼0
X16
j¼0
yi � grid valuei;j
� �=X13
i¼0
X16
j¼0
grid valuei;j
Statistical analysis
Results are expressed as means, standard deviations (SD)
and 95 % confidence intervals (95 % CI). The Kolmogorov–
Smirnov test revealed a normal distribution of all quanti-
tative variables (P [ 0.05). Differences in pain parameters
between groups were assessed with the unpaired Student’s
t test. The Chi square (v2) test was used to assess the dif-
ferences in the distribution of TrPs for each muscle on
either side within both groups. A two-way analysis of
variance (ANOVA) with area (frontal, non-dominant
dominant, posterior) as within-subjects variable and group
(TMD, FMS) as the between-subjects variable was used to
assess differences in usual symptomatic pain areas between
groups. Differences in X and Y coordinates of usual pain
areas between groups were assessed with the unpaired
Student’s t test. Differences in the number of active TrPs
between groups were assessed with the non-parametric
Mann–Whitney U test. A three-way analysis of variance
(ANOVA) was used to compare referred pain areas (au)
between sides (dominant/non dominant) and muscles (i.e.,
temporalis, masseter, upper trapezius, and sternocleido-
mastoid) as within-subjects factors and group (TMD, FMS)
as between-subjects factor. A similar 2-way ANOVA was
used for the referred pain area from suboccipital muscles
without side as factor. The Bonferroni test was used for
post hoc analyses. Differences in X and Y coordinates of
TrPs referred pain areas between groups were assessed
with the unpaired Student’s t test. Finally, the Spearman’s
rho (rs) test was used to analyze the association between
the number of TrPs, the referred pain areas and pain
parameters. A P value \ 0.05 was considered statistically
significant.
Results
Demographic and clinical data of the sample
Table 1 summarizes clinical and demographic data of both
groups. Sixty-two (n = 62) consecutive patients with a
diagnosis of TMD (n = 30) or FMS (n = 32) were
screened for eligibility criteria. Ten (33 %) patients with
TMD [migraine (n = 4), fibromyalgia syndrome (n = 4),
previous whiplash (n = 2)] and 12 (37 %) with FMS [high
levels of depression (n = 7), previous whiplash (n = 5)]
were excluded. Finally, a total of 20 women with strict
myofascial TMD (mean age 46 ± 8 years) and 20 women
with FMS (age 48 ± 6 years) satisfied all the inclusion
criteria and agreed to participate.. Women with FMS exhib-
ited a longer duration of the pain condition (P \ 0.001), and
higher usual level of pain, worst and lowest level of pain
experienced in the preceding week at rest in the orofacial area
(P \ 0.001).
Usual pain areas in the orofacial region
Table 2 shows the mean values of X and Y coordinates of
the COG for women with myofascial TMD or FMS. The
mean usual pain area in women with myofascial TMD was
12.5 au (95 % CI 8.1–17.0) in the frontal region (n = 17,
85 %), 43.7 au (95 % CI 28.4–59.0) in the occipital region
and posterior part of the neck (n = 12, 60 %), 24.5 au
(95 % CI 17.3–31.7) on the dominant side of the head
(n = 14, 70 %), and 17.8 au (95 %CI 12.1–23.6) in the
non-dominant side of the face (n = 20, 100 %). Women
with FMS reported a usual pain area of 36.1 au (95 % CI
22.0–49.8) in the frontal area (n = 19, 95 %), 71.1 au
628 J Headache Pain (2012) 13:625–637
123
(95 % CI 46.3–95.9) in the occipital region and posterior
part of the neck (n = 20, 100 %), 34.3 au (95 % CI
25.1–43.6) on the dominant side of the head (n = 16,
80 %), and 27.2 au (95 % CI 18.5–36.4) on the non-
dominant side of the face (n = 15, 75 %).
The ANOVA indicated significant differences between
groups (F = 15.207; P \ 0.001) and regions (F = 12.005;
P \ 0.001) for usual pain symptoms. No significant group 9
region interaction was found (F = 1.005, P = 0.370). The
post hoc analysis revealed that women with FMS exhibited
larger pain areas of usual pain symptoms in the face than
women with myofascial TMD (P \ 0.01), and that the pain
area within the posterior region of the head was signifi-
cantly larger than the remaining pain areas (P \ 0.001). No
significant associations between the intensity or duration of
pain and usual pain areas in either group were found
(P [ 0.145).
In addition, significant differences between the location
of the Y coordinate on the frontal side (t = -2.190;
P = 0.045) and posterior region (t = -2.981; P = 0.006):
the pain areas in women with TMD were located more
superior (higher Y value) than in women with FMS. No
significant differences for the remaining coordinates of the
COG were found between groups (P [ 0.147, Fig. 2).
Prevalence of Muscle TrPs
Table 3 details the distribution of TrPs in both women with
myofascial TMD or FMS. The mean ± SD number of
active TrPs in women with myofascial TMD was 6 ± 1
and 4 ± 1 in women with FMS (z = -3.105; P = 0.002).
A significant association between the number of active
TrPs and usual pain (rs = 0.492; P = 0.027) was found in
TMD, but not in FMS (rs = 0.027; P = 0.909). No other
association between the number of active TrPs and the
other pain parameters was found.
The distribution of active muscle TrPs between women
with myofascial TMD or FMS was significantly different for
both temporalis (right: v2 = 18.649, P \ 0.001; left: v2 =
26.471, P \ 0.001), left masseter (v2 = 6.154, P = 0.046),
left upper trapezius (v2 = 10.326, P = 0.006), and both
sternocleidomastoid (right: v2 = 21.073, P \ 0.001; left:
v2 = 12.939, P = 0.002) muscles: women with myofascial
TMD exhibited a greater number of active TrPs in these
muscles as compared to women with FMS.
No significant differences in the distribution of right
masseter (v2 = 4.732, P = 0.984), right upper trapezius
(v2 = 5.700, P = 0.058), and suboccipital (v2 = 4.637,
P = 0.098) muscles were found between groups.
TrP referred pain areas
Table 4 summarizes size of the referred pain areas in all
muscles in women with myofascial TMD or FMS. A three-
way ANOVA revealed significant differences in referred
pain areas between muscles (F = 24.002, P \ 0.001), but
not between groups (F = 3.023, P = 0.083) or sides
(F = 0.084, P = 0.772). A significant interaction between
Table 1 Clinical pain parameters between women with myofascial TMD (n = 20) or FMS (n = 20)
Myofascial TMD FMS Significance
Pain history (years) 2.3 ± 1.3 (1.7–2.9) 6.7 ± 2.3 (5.6 –7.8) z = -5.003; P \ 0.001
Usual level of pain (0–10) 4.1 ± 1.3 (3.5–4.8) 6.0 ± 1.0 (5.5–6.4) z = -3.812; P \ 0.001
Worst level of pain (0–10) 6.5 ± 0.9 (6.0–6.9) 8.4 ± 0.8 (8.0–8.8) z = -4.787; P \ 0.001
Lowest levels of pain (0–10) 1.9 ± 0.8 (1.6–2.4) 3.8 ± 1.0 (3.3–4.3) z = -4.538; P \ 0.001
Data are expressed as mean ± SD (95 % confidence interval)
TMD temporomandibular disorder, FMS fibromyalgia syndrome, NPRS numerical pain rate scale
Table 2 Center-of-gravity (COG) measurements of usual pain drawing in the orofacial region in women with myofascial TMD or with FMS
[mean ± SD (95 % CI)]
Frontal projection Posterior projection Dominant (right) side Non-dominant (left) side
X Y* X Y* X Y X Y
TMD 7.4 ± 1.2
(6.7–7.2)
10.4 ± 2.3
(12.5–13.5)
6.9 ± 0.4
(6.8–7.0)
7.1 ± 2.3
(5.7–7.6)
7.3 ± 1.2
(7.4–8.9)
9.5 ± 2.0
(12.0–14.0)
7.3 ± 1.6
(7.5–8.2)
8.7 ± 1.8
(11.8–13.4)
FMS 6.8 ± 0.7
(6.4–7.0)
12.1 ± 2.9
(13.5–14.0)
7.1 ± 0.2
(7.0–7.1)
5.3 ± 1.2
(6.2–10.5)
7.4 ± 1.1
(6.0–8.0)
11.3 ± 3.4
(11.5–14.6)
7.4 ± 2.1
(6.9–8.5)
8.9 ± 4.4
(12.4–14.0)
TMD temporomandibular disorder, FMS fibromyalgia syndrome
* Significant differences between TMD and FMS (Student’s t test, P \ 0.05)
J Headache Pain (2012) 13:625–637 629
123
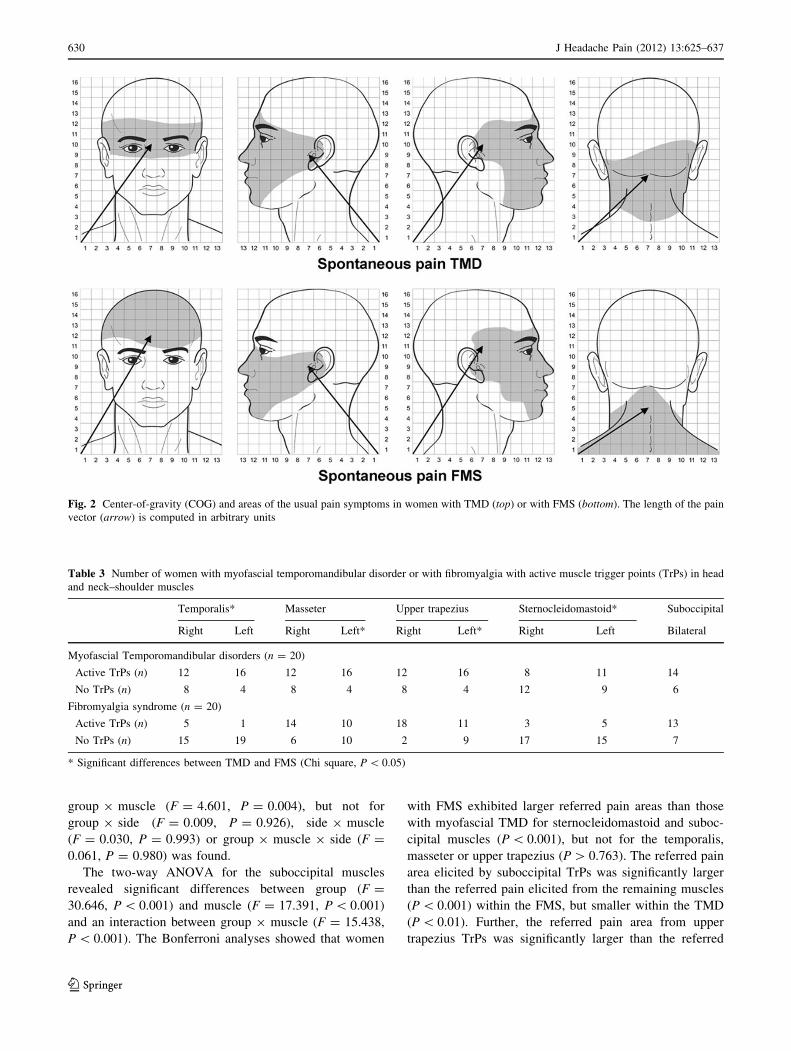
group 9 muscle (F = 4.601, P = 0.004), but not for
group 9 side (F = 0.009, P = 0.926), side 9 muscle
(F = 0.030, P = 0.993) or group 9 muscle 9 side (F =
0.061, P = 0.980) was found.
The two-way ANOVA for the suboccipital muscles
revealed significant differences between group (F =
30.646, P \ 0.001) and muscle (F = 17.391, P \ 0.001)
and an interaction between group 9 muscle (F = 15.438,
P \ 0.001). The Bonferroni analyses showed that women
with FMS exhibited larger referred pain areas than those
with myofascial TMD for sternocleidomastoid and suboc-
cipital muscles (P \ 0.001), but not for the temporalis,
masseter or upper trapezius (P [ 0.763). The referred pain
area elicited by suboccipital TrPs was significantly larger
than the referred pain elicited from the remaining muscles
(P \ 0.001) within the FMS, but smaller within the TMD
(P \ 0.01). Further, the referred pain area from upper
trapezius TrPs was significantly larger than the referred
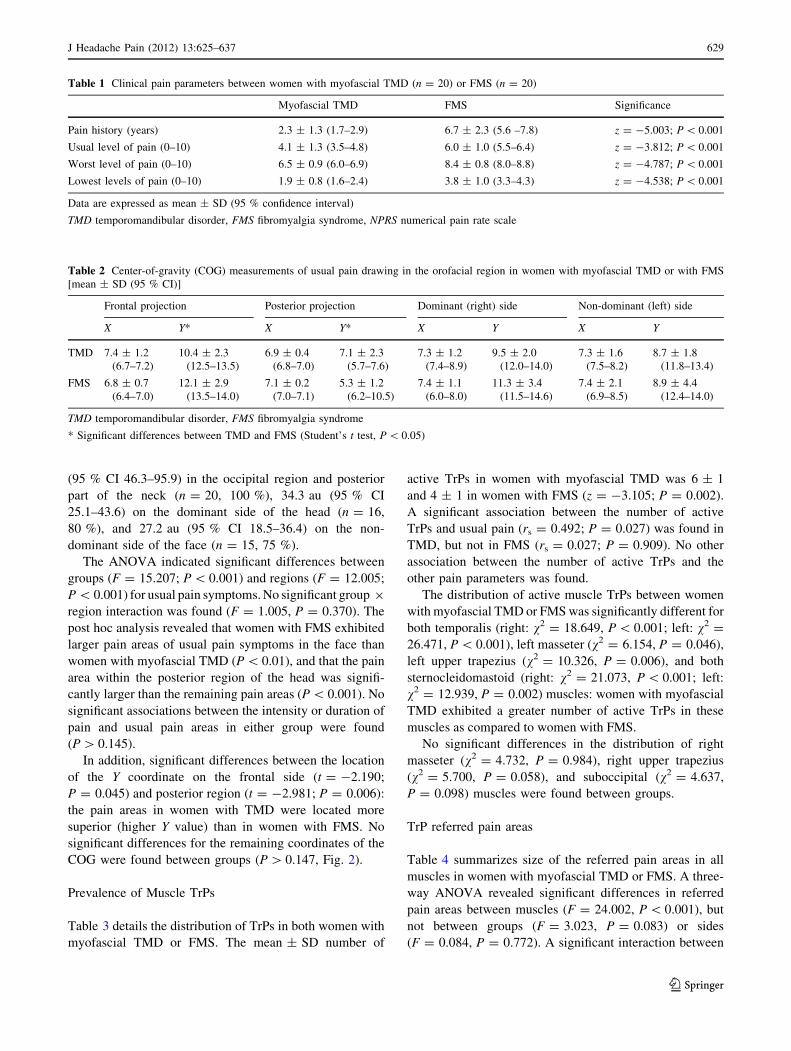
Fig. 2 Center-of-gravity (COG) and areas of the usual pain symptoms in women with TMD (top) or with FMS (bottom). The length of the pain
vector (arrow) is computed in arbitrary units
Table 3 Number of women with myofascial temporomandibular disorder or with fibromyalgia with active muscle trigger points (TrPs) in head
and neck–shoulder muscles
Temporalis* Masseter Upper trapezius Sternocleidomastoid* Suboccipital
Right Left Right Left* Right Left* Right Left Bilateral
Myofascial Temporomandibular disorders (n = 20)
Active TrPs (n) 12 16 12 16 12 16 8 11 14
No TrPs (n) 8 4 8 4 8 4 12 9 6
Fibromyalgia syndrome (n = 20)
Active TrPs (n) 5 1 14 10 18 11 3 5 13
No TrPs (n) 15 19 6 10 2 9 17 15 7
* Significant differences between TMD and FMS (Chi square, P \ 0.05)
630 J Headache Pain (2012) 13:625–637
123
pain areas elicited by temporalis, masseter and sternoclei-
domastoid muscle TrPs in both groups (P \ 0.001).
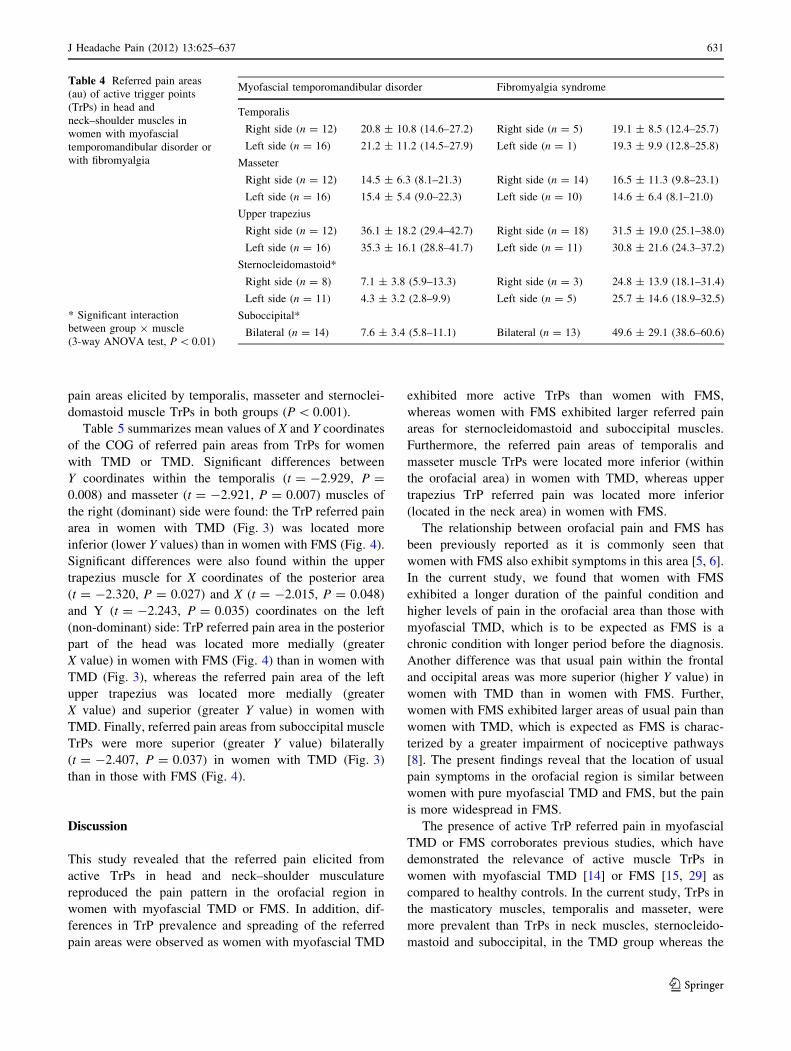
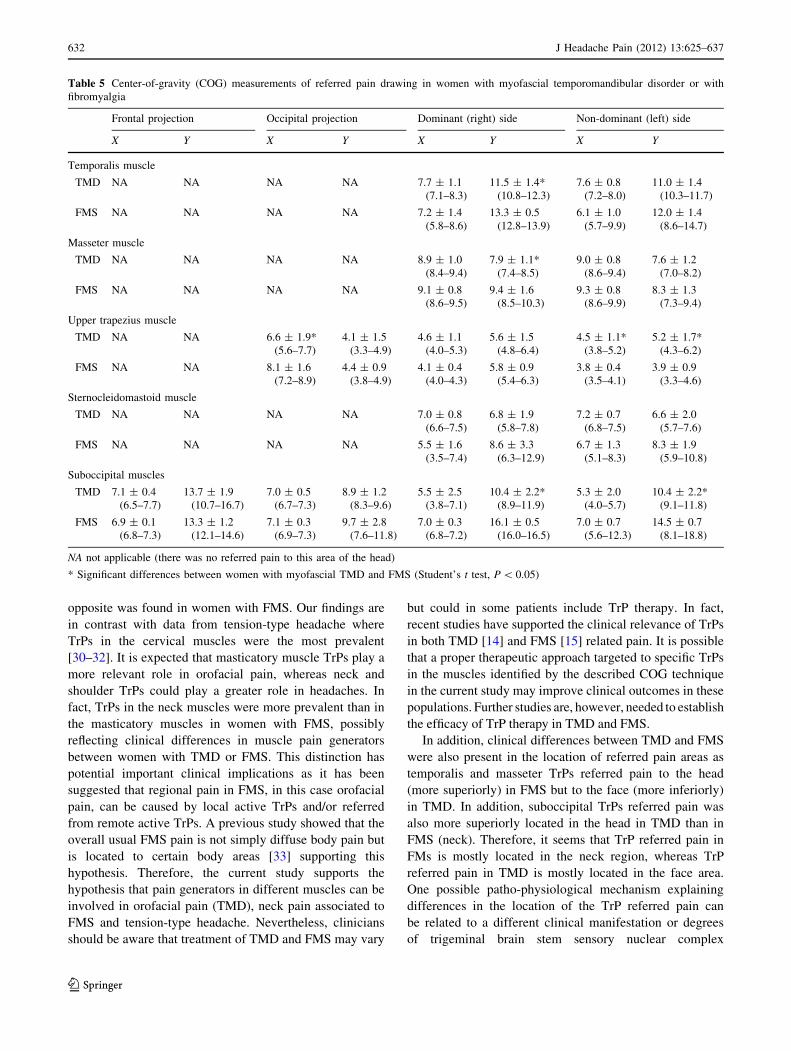
Table 5 summarizes mean values of X and Y coordinates
of the COG of referred pain areas from TrPs for women
with TMD or TMD. Significant differences between
Y coordinates within the temporalis (t = -2.929, P =
0.008) and masseter (t = -2.921, P = 0.007) muscles of
the right (dominant) side were found: the TrP referred pain
area in women with TMD (Fig. 3) was located more
inferior (lower Y values) than in women with FMS (Fig. 4).
Significant differences were also found within the upper
trapezius muscle for X coordinates of the posterior area
(t = -2.320, P = 0.027) and X (t = -2.015, P = 0.048)
and Y (t = -2.243, P = 0.035) coordinates on the left
(non-dominant) side: TrP referred pain area in the posterior
part of the head was located more medially (greater
X value) in women with FMS (Fig. 4) than in women with
TMD (Fig. 3), whereas the referred pain area of the left
upper trapezius was located more medially (greater
X value) and superior (greater Y value) in women with
TMD. Finally, referred pain areas from suboccipital muscle
TrPs were more superior (greater Y value) bilaterally
(t = -2.407, P = 0.037) in women with TMD (Fig. 3)
than in those with FMS (Fig. 4).
Discussion
This study revealed that the referred pain elicited from
active TrPs in head and neck–shoulder musculature
reproduced the pain pattern in the orofacial region in
women with myofascial TMD or FMS. In addition, dif-
ferences in TrP prevalence and spreading of the referred
pain areas were observed as women with myofascial TMD
exhibited more active TrPs than women with FMS,
whereas women with FMS exhibited larger referred pain
areas for sternocleidomastoid and suboccipital muscles.
Furthermore, the referred pain areas of temporalis and
masseter muscle TrPs were located more inferior (within
the orofacial area) in women with TMD, whereas upper
trapezius TrP referred pain was located more inferior
(located in the neck area) in women with FMS.
The relationship between orofacial pain and FMS has
been previously reported as it is commonly seen that
women with FMS also exhibit symptoms in this area [5, 6].
In the current study, we found that women with FMS
exhibited a longer duration of the painful condition and
higher levels of pain in the orofacial area than those with
myofascial TMD, which is to be expected as FMS is a
chronic condition with longer period before the diagnosis.
Another difference was that usual pain within the frontal
and occipital areas was more superior (higher Y value) in
women with TMD than in women with FMS. Further,
women with FMS exhibited larger areas of usual pain than
women with TMD, which is expected as FMS is charac-
terized by a greater impairment of nociceptive pathways
[8]. The present findings reveal that the location of usual
pain symptoms in the orofacial region is similar between
women with pure myofascial TMD and FMS, but the pain
is more widespread in FMS.
The presence of active TrP referred pain in myofascial
TMD or FMS corroborates previous studies, which have
demonstrated the relevance of active muscle TrPs in
women with myofascial TMD [14] or FMS [15, 29] as
compared to healthy controls. In the current study, TrPs in
the masticatory muscles, temporalis and masseter, were
more prevalent than TrPs in neck muscles, sternocleido-
mastoid and suboccipital, in the TMD group whereas the
Table 4 Referred pain areas
(au) of active trigger points
(TrPs) in head and
neck–shoulder muscles in
women with myofascial
temporomandibular disorder or
with fibromyalgia
* Significant interaction
between group 9 muscle
(3-way ANOVA test, P \ 0.01)
Myofascial temporomandibular disorder Fibromyalgia syndrome
Temporalis
Right side (n = 12) 20.8 ± 10.8 (14.6–27.2) Right side (n = 5) 19.1 ± 8.5 (12.4–25.7)
Left side (n = 16) 21.2 ± 11.2 (14.5–27.9) Left side (n = 1) 19.3 ± 9.9 (12.8–25.8)
Masseter
Right side (n = 12) 14.5 ± 6.3 (8.1–21.3) Right side (n = 14) 16.5 ± 11.3 (9.8–23.1)
Left side (n = 16) 15.4 ± 5.4 (9.0–22.3) Left side (n = 10) 14.6 ± 6.4 (8.1–21.0)
Upper trapezius
Right side (n = 12) 36.1 ± 18.2 (29.4–42.7) Right side (n = 18) 31.5 ± 19.0 (25.1–38.0)
Left side (n = 16) 35.3 ± 16.1 (28.8–41.7) Left side (n = 11) 30.8 ± 21.6 (24.3–37.2)
Sternocleidomastoid*
Right side (n = 8) 7.1 ± 3.8 (5.9–13.3) Right side (n = 3) 24.8 ± 13.9 (18.1–31.4)
Left side (n = 11) 4.3 ± 3.2 (2.8–9.9) Left side (n = 5) 25.7 ± 14.6 (18.9–32.5)
Suboccipital*
Bilateral (n = 14) 7.6 ± 3.4 (5.8–11.1) Bilateral (n = 13) 49.6 ± 29.1 (38.6–60.6)
J Headache Pain (2012) 13:625–637 631
123
opposite was found in women with FMS. Our findings are
in contrast with data from tension-type headache where
TrPs in the cervical muscles were the most prevalent
[30–32]. It is expected that masticatory muscle TrPs play a
more relevant role in orofacial pain, whereas neck and
shoulder TrPs could play a greater role in headaches. In
fact, TrPs in the neck muscles were more prevalent than in
the masticatory muscles in women with FMS, possibly
reflecting clinical differences in muscle pain generators
between women with TMD or FMS. This distinction has
potential important clinical implications as it has been
suggested that regional pain in FMS, in this case orofacial
pain, can be caused by local active TrPs and/or referred
from remote active TrPs. A previous study showed that the
overall usual FMS pain is not simply diffuse body pain but
is located to certain body areas [33] supporting this
hypothesis. Therefore, the current study supports the
hypothesis that pain generators in different muscles can be
involved in orofacial pain (TMD), neck pain associated to
FMS and tension-type headache. Nevertheless, clinicians
should be aware that treatment of TMD and FMS may vary
but could in some patients include TrP therapy. In fact,
recent studies have supported the clinical relevance of TrPs
in both TMD [14] and FMS [15] related pain. It is possible
that a proper therapeutic approach targeted to specific TrPs
in the muscles identified by the described COG technique
in the current study may improve clinical outcomes in these
populations. Further studies are, however, needed to establish
the efficacy of TrP therapy in TMD and FMS.
In addition, clinical differences between TMD and FMS
were also present in the location of referred pain areas as
temporalis and masseter TrPs referred pain to the head
(more superiorly) in FMS but to the face (more inferiorly)
in TMD. In addition, suboccipital TrPs referred pain was
also more superiorly located in the head in TMD than in
FMS (neck). Therefore, it seems that TrP referred pain in
FMs is mostly located in the neck region, whereas TrP
referred pain in TMD is mostly located in the face area.
One possible patho-physiological mechanism explaining
differences in the location of the TrP referred pain can
be related to a different clinical manifestation or degrees
of trigeminal brain stem sensory nuclear complex
Table 5 Center-of-gravity (COG) measurements of referred pain drawing in women with myofascial temporomandibular disorder or with
fibromyalgia
Frontal projection Occipital projection Dominant (right) side Non-dominant (left) side
X Y X Y X Y X Y
Temporalis muscle
TMD NA NA NA NA 7.7 ± 1.1
(7.1–8.3)
11.5 ± 1.4*
(10.8–12.3)
7.6 ± 0.8
(7.2–8.0)
11.0 ± 1.4
(10.3–11.7)
FMS NA NA NA NA 7.2 ± 1.4
(5.8–8.6)
13.3 ± 0.5
(12.8–13.9)
6.1 ± 1.0
(5.7–9.9)
12.0 ± 1.4
(8.6–14.7)
Masseter muscle
TMD NA NA NA NA 8.9 ± 1.0
(8.4–9.4)
7.9 ± 1.1*
(7.4–8.5)
9.0 ± 0.8
(8.6–9.4)
7.6 ± 1.2
(7.0–8.2)
FMS NA NA NA NA 9.1 ± 0.8
(8.6–9.5)
9.4 ± 1.6
(8.5–10.3)
9.3 ± 0.8
(8.6–9.9)
8.3 ± 1.3
(7.3–9.4)
Upper trapezius muscle
TMD NA NA 6.6 ± 1.9*
(5.6–7.7)
4.1 ± 1.5
(3.3–4.9)
4.6 ± 1.1
(4.0–5.3)
5.6 ± 1.5
(4.8–6.4)
4.5 ± 1.1*
(3.8–5.2)
5.2 ± 1.7*
(4.3–6.2)
FMS NA NA 8.1 ± 1.6
(7.2–8.9)
4.4 ± 0.9
(3.8–4.9)
4.1 ± 0.4
(4.0–4.3)
5.8 ± 0.9
(5.4–6.3)
3.8 ± 0.4
(3.5–4.1)
3.9 ± 0.9
(3.3–4.6)
Sternocleidomastoid muscle
TMD NA NA NA NA 7.0 ± 0.8
(6.6–7.5)
6.8 ± 1.9
(5.8–7.8)
7.2 ± 0.7
(6.8–7.5)
6.6 ± 2.0
(5.7–7.6)
FMS NA NA NA NA 5.5 ± 1.6
(3.5–7.4)
8.6 ± 3.3
(6.3–12.9)
6.7 ± 1.3
(5.1–8.3)
8.3 ± 1.9
(5.9–10.8)
Suboccipital muscles
TMD 7.1 ± 0.4
(6.5–7.7)
13.7 ± 1.9
(10.7–16.7)
7.0 ± 0.5
(6.7–7.3)
8.9 ± 1.2
(8.3–9.6)
5.5 ± 2.5
(3.8–7.1)
10.4 ± 2.2*
(8.9–11.9)
5.3 ± 2.0
(4.0–5.7)
10.4 ± 2.2*
(9.1–11.8)
FMS 6.9 ± 0.1
(6.8–7.3)
13.3 ± 1.2
(12.1–14.6)
7.1 ± 0.3
(6.9–7.3)
9.7 ± 2.8
(7.6–11.8)
7.0 ± 0.3
(6.8–7.2)
16.1 ± 0.5
(16.0–16.5)
7.0 ± 0.7
(5.6–12.3)
14.5 ± 0.7
(8.1–18.8)
NA not applicable (there was no referred pain to this area of the head)
* Significant differences between women with myofascial TMD and FMS (Student’s t test, P \ 0.05)
632 J Headache Pain (2012) 13:625–637
123
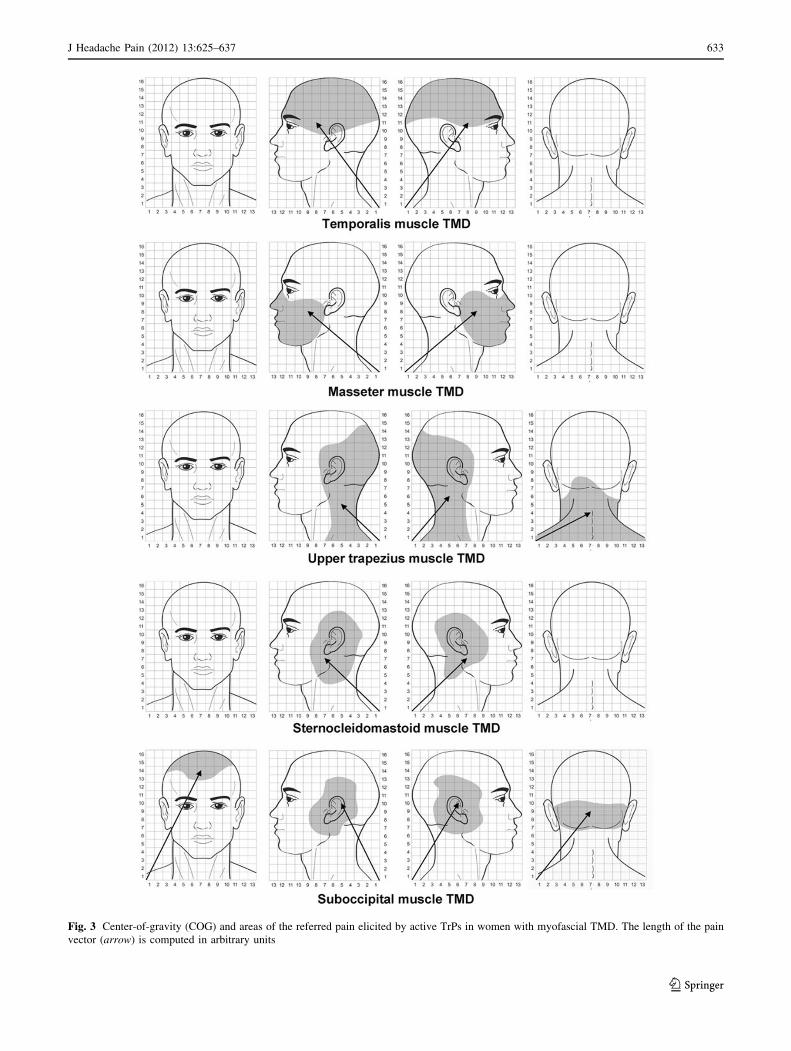
Fig. 3 Center-of-gravity (COG) and areas of the referred pain elicited by active TrPs in women with myofascial TMD. The length of the pain
vector (arrow) is computed in arbitrary units
J Headache Pain (2012) 13:625–637 633
123
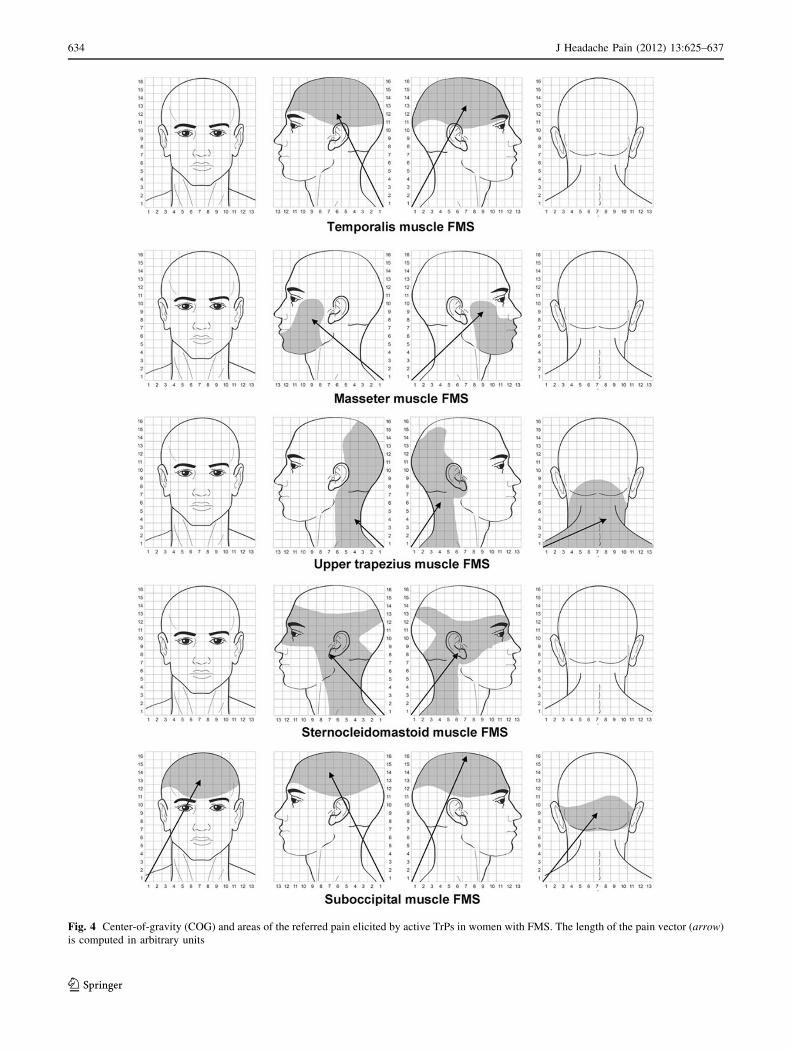
Fig. 4 Center-of-gravity (COG) and areas of the referred pain elicited by active TrPs in women with FMS. The length of the pain vector (arrow)
is computed in arbitrary units
634 J Headache Pain (2012) 13:625–637
123

sensitization relative to cervical/spinal sensitization. It is
plausible that women with TMD would exhibit a greater
sensitization of the trigeminal neurons than women with
FMS which would explain the TrP referred pain location in
the face rather than in the neck for TrPs in the masticatory
muscles.
The presence of active TrPs indicates sensitization of
muscle nociceptors in both TMD and FMS since high
levels of neuroactive mediators [12, 13] and lower pressure
pain thresholds [34–37] have been found in active TrPs. In
fact, Hong [38–40] suggested the concept of multiple
sensitized nociceptors in the TrP region as the sensory units
responsible for the local twitch response when the TrP is
mechanically stimulated. Further, there is evidence dem-
onstrating that active TrPs may serve as potent peripheral
noxious input sensitizing central nervous system in FMS
and TMD. This hypothesis is supported by human experi-
mental studies showing that a single intramuscular anes-
thetic injection into the midpoint of the upper trapezius
muscle, a typical site of active TrPs in FMS patients, sig-
nificantly increased pain thresholds and decreases second-
ary heat hyperalgesia in FMS [41]. Therefore, studies
investigating the clinical relevance of TrPs inactivation in
the course of pain in the orofacial area in women with
myofascial TMD or FMS are clearly needed.
Finally, we should recognize some strengths and limi-
tations of the study. First, we included patients recruited
from tertiary clinics which may not represent the general
population. It is possible that patients seeking treatment in
specialized clinics exhibit different features and charac-
teristics than those recruited from a general population and
it is a common clinical observation that these patients
have inadequate pain relief from a variety of therapeutic
approaches (e.g., oral appliances, medication, etc.) [42]; so
direct extrapolations of the current results to the general
population should be avoided at this stage. In addition, our
sample size was relatively small. Therefore, future studies
with greater sample sizes and including patients recruited
from the general population are now needed to further
confirm the current results. Furthermore, FMS diagnosis is
a challenge for clinicians and researchers and new diag-
nostic criteria have been proposed [43]. Women with FMS
included in our study were diagnosed according to first
diagnostic criteria [21]. We do not know if the same results
would be found in women with FMS presenting the new
proposed criteria, but we speculate that there is a signifi-
cant concordance between the two sets of criteria. Second,
the TrP examination was conducted by a blinded examiner
ruling of the chance of bias. Nevertheless, it is possible that
a potential bias of patients’ recognition of the referred pain
may be present in TrP examination although this seems
unlikely. In addition, reproducibility of TrP diagnosis has
been questioned in recent reviews since studies of high
quality are needed [44, 45]. Factors that may have con-
tributed to the varying reliability of the results from pre-
vious studies are lack of identification of taut bands,
inexperience of the examiners in assessing TrPs or incor-
rect palpation techniques. Nevertheless, Gerwin et al. [26]
reported that TrP diagnosis has good inter-examiner reli-
ability when applied by an experienced examiner, as this
was conducted in this study. It should also be acknowl-
edged that the understanding of TrP remains incomplete
and further studies will be needed to clarify underlying
mechanisms as well as clinical manifestations. Third, we
included a specific group of women with strictly myofas-
cial TMD or with FMS. We excluded patients with other
concomitant RCD/TMD diagnosis and other co-morbid
conditions, i.e., primary headaches, with may be also
related to the presence of TrPs. Therefore, our results
should be considered with caution when extrapolate to
different groups of patient with FMS or TMD. Fourth, it is
suggested that psychological factors, e.g., anxiety and
depression, may enhance central nervous system responses
[46]. In the current study, we excluded a state of depression
in our patients with TMD or FMS ([8 points BDI-II).
Therefore, data are representative for women with myo-
fascial TMD pain or FMS without depression. Neverthe-
less, we do not know if anxiety, sleep disturbances, pain
catastrophizing etc. could also influence our results.
Finally, since we only included women, future studies
should investigate gender differences and determine if
similar results are present in men with TMD or FMS.
Conclusion
This study showed that the referred pain elicited from
active TrPs in head and neck–shoulder musculature
reproduced the pain pattern in the orofacial region in
women with myofascial TMD or FMS. Women with
myofascial TMD exhibited more active TrPs than women
with FMS, whereas women with FMS exhibited larger
referred pain areas for neck muscle TrPs. The referred pain
areas of temporalis and masseter muscle TrPs were located
more inferior (in the orofacial area) in TMD, whereas
upper trapezius TrP referred pain was located more inferior
(in the neck area) in FMS. The current study supports that
generators in different muscles can be involved in orofacial
pain (TMD) and neck–face pain associated to FMS.
Conflict of interest No conflict of interest has been declared by the
author(s).
Open Access This article is distributed under the terms of the
Creative Commons Attribution License which permits any use, dis-
tribution, and reproduction in any medium, provided the original
author(s) and the source are credited.
J Headache Pain (2012) 13:625–637 635
123
References
1. LeResche L (1997) Epidemiology of temporomandibular disor-
ders: implications for the investigation of etiologic factors. Crit
Rev Oral Biol Med 8:291–305
2. Isong U, Gansky SA, Plesh O (2008) Temporomandibular joint
and muscle disorder-type pain in US adults: the National Health
Interview Survey. J Orofac Pain 22:317–322
3. Branco JC, Bannwarth B, Failde I, Abello Carbonell J, Blotman
F, Spaeth M, Saraiva F, Nacci F, Thomas E, Caubere JP, Le Lay
K, Taieb C, Matucci-Cerinic M (2010) Prevalence of fibromy-
algia: a survey in five European countries. Semin Arthr Rheum
39:448–453
4. Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H,
Deyo RA, Gabriel S, Hirsch R, Hochberg MC, Hunder GG,
Jordan GM, Katz JN, Kremers HM, Wolfe F, National Arthritis
Work Group (2008) Estimates of the prevalence of arthritis and
other rheumatic conditions in the United States: part II. Arthr
Rheum 58:26–35
5. Pennacchio EA, Borg-Stein J, Keith DA (1998) The incidence of
pain in the muscles of mastication in patients with fibromyalgia.
J Mass Dent Soc 47:8–12
6. Rhodus NL, Fricton J, Carlson P, Messner R (2003) Oral
symptoms associated with fibromyalgia syndrome. J Rheumatol
30:1841–1845
7. Torsten J, Miglioretti DL, Leresche L, Von Korff M, Critchlow
CW (2003) Widespread pain as a risk factor for dysfunctional
temporomandibular disorder pain. Pain 102:257–263
8. Velly AM, Look JO, Schiffman E, Lenton PA, Kang W, Messner
RP, Holcroft CA, Fricton JR (2010) The effect of fibromyalgia
and widespread pain on the clinically significant temporoman-
dibular muscle and joint pain disorders: a prospective 18-month
cohort study. J Pain 11:1155–1164
9. Svenson P (2007) Muscle pain in the head: overlap between
temporomandibular disorders and tension-type headaches. Curr
Opin Neurol 20:320–325
10. Ge HY (2010) Prevalence of myofascial trigger points in fibro-
myalgia: the overlap of two common problems. Curr Pain
Headache Rep 14:339–345
11. Simons DG, Travell J, Simons LS (1999) Travell and Simons’
Myofascial pain and dysfunction: the trigger point manual, vol 1,
2nd edn. Williams & Wilkins, Baltimore
12. Shah JP, Phillips TM, Danoff JV, Gerber LH (2005) An in
vitro microanalytical technique for measuring the local bio-
chemical milieu of human skeletal muscle. J Appl Physiol
99:1977–1984
13. Shah JP, Danoff JV, Desai MJ, Parikh S, Nakamura LY, Phillips
TM, Gerber LH (2008) Biochemical associated with pain and
inflammations are elevated in sites near to and remote from active
myofascial trigger points. Arch Phys Med Rehabil 89:16–23
14. Fernandez-de-Las-Penas C, Galan-Del-Rıo F, Alonso-Blanco C,
Jimenez-Garcıa R, Arendt-Nielsen L, Svensson P (2010) Referred
pain from muscle trigger points in the masticatory and neck–
shoulder musculature in women with temporomandibular disor-
ders. J Pain 11:1295–1304
15. Alonso-Blanco C, Fernandez-de-Las-Penas C, Morales-Cabezas
M, Zarco-Moreno P, Ge H, Florez-Garcıa M (2011) Multiple
active myofascial trigger points reproduce the overall spontane-
ous pain pattern in women with fibromyalgia and are related to
widespread mechanical hypersensitivity. Clin J Pain 27:405–413
16. Schmidt-Hansen PT, Svensson P, Jensen TS, Graven-Nielsen T,
Bach F (2006) Patterns of experimentally induced pain in peri-
cranial muscles. Cephalalgia 26:568–577
17. Svensson P, Bak J, Troest T (2003) Spread and referral of
experimental pain in different jaw muscles. J Orofac Pain
17:214–223
18. de Tommaso M, Sardaro M, Serpino C, Costantini F, Vecchio E,
Prudenzano MP, Lamberti P, Livrea P (2009) Fibromyalgia
comorbidity in primary headaches. Cephalalgia 29:453–464
19. de Tommaso M, Federici A, Serpino C, Vecchio E, Franco G, Sardaro
M, Delussi M, Livrea P (2011) Clinical features of headache patients
with fibromyalgia comorbidity. J Headache Pain 12:629–638
20. Dworkin SF, LeResche L (1992) Research diagnostic criteria for
temporomandibular disorders: review, criteria, examinations and
specifications, critique. Cranio 6:301–355
21. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,
Goldenberg DL, Tugwell P, Campbell SM, Abeles M, Clark P
(1990) The American College of Rheumatology 1990 criteria for
classification of fibromyalgia: report of the multicenter criteria
committee. Arthr Rheum 33:160–170
22. Jensen MP, Turbner JA, Romano JM, Fisher L (1999) Compar-
ative reliability and validity of chronic pain intensity measures.
Pain 83:157–162
23. Beck AT, Steer RA, Brown GK (1996) Beck depression inven-
tory, 2nd edn. The Psychological Corporation, San Antonio
24. Beck AT, Steer RA, Garbin MG (1988) Psychometric properties
of the Beck Depression Inventory: twenty-five years of evalua-
tion. Clin Psychol Rev 8:77–100
25. VanVoorhis WCR, Blumentritt TL (2007) Psychometric proper-
ties of the Beck Depression inventory-II in a clinically-identified
sample of Mexican American adolescents. J Child Family Studies
16:789–798
26. Gerwin RD, Shanon S, Hong CZ, Hubbard D, Gevirtz R (1997)
Interrater reliability in myofascial trigger point examination. Pain
69:65–67
27. Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Gerwin
RD, Pareja JA (2006) Trigger points in the suboccipital muscles and
forward headposture in tension type headache. Headache 46:454–460
28. Branch MA, Carlson CR, Okeson J (2000) Influence of biased
clinician statements on patient reports of referred pain. J Orofac
Pain 14:120–127
29. Ge HY, Nie H, Madeleine P, Danneskiold-Samsøe B, Graven-
Nielsen T, Arendt-Nielsen L (2009) Contribution of the local and
referred pain from active myofascial trigger points in fibromy-
algia syndrome. Pain 147:233–240
30. Fernandez-de-las-Penas C, Ge H, Arendt-Nielsen L, Cuadrado
ML, Pareja JA (2007) The local and referred pain from myo-
fascial trigger points in the temporalis muscle contributes to pain
profile in chronic tension-type headache. Clin J Pain 23:786–792
31. Fernandez-de-las-Penas C, Ge H, Arendt-Nielsen L, Cuadrado
ML, Pareja JA (2007) Referred pain from trapezius muscle
trigger point shares similar characteristics with chronic tension
type headache. Eur J Pain 11:475–482
32. Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML,
Gerwin RD, Pareja JA (2006) Myofascial trigger points and their
relationship with headache clinical parameters in chronic tension
type headache. Headache 46:1264–1272
33. Staud R, Vierck CJ, Robinson ME, Price DD (2006) Overall
fibromyalgia pain is predicted by ratings of local pain and pain-
related negative affect—possible role of peripheral tissues.
Rheumatology 45:1409–1415
34. Hong CZ, Chen YN, Twehous D, Hong DH (1996) Pressure
threshold for referred pain by compression on the trigger point
and adjacent areas. J Musculoskelet Pain 4(3):61–79
35. Hong CZ (1998) Algometry in evaluation of trigger points and
referred pain. J Musculoskelet Pain 6(1):47–59
36. Ge HY, Fernandez-de-las-Penas C, Madeleine P, Arendt-Nielsen L
(2008) Topographical mapping and mechanical pain sensitivity of
myofascial trigger points in the infraspinatus muscle. Eur J Pain
12:859–865
37. Fernandez-de-las-Penas C, Caminero AB, Madeleine P, Guillem-
Mesado A, Ge HY, Arendt-Nielsen L, Pareja JA (2009) Multiple
636 J Headache Pain (2012) 13:625–637
123

active myofascial trigger points and pressure pain sensitivity
maps in the temporalis muscle are related in chronic tension type
headache. Clin J Pain 25:506–512
38. Hong CZ (1993) Myofascial trigger point injection. Crit Rev
Phys Rehabil Med 5:203–217
39. Hong CZ (1994) Consideration and recommendation of myo-
fascial trigger point injection. J Musculoskelet Pain 2(1):29–59
40. Hong CZ (1996) Pathophysiology of myofascial trigger point.
J Formos Med Assoc 95:93–104
41. Staud R, Nagel S, Robinson ME, Price DD (2009) Enhanced
central pain processing of fibromyalgia patients is maintained by
muscle afferent input: a randomized, double-blind, placebo-con-
trolled study. Pain 145:96–104
42. List T, Axelsson S (2010) Management of TMD: evidence from
systematic reviews and meta-analyses. J Oral Rehabil 37:430–451
43. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS,
Mease P, Russell AS, Russell IJ, Winfield JB, Yunus MB (2010)
The American College of Rheumatology preliminary diagnostic
criteria for fibromyalgia and measurement of symptom severity.
Arthr Care Res 62:600–610
44. Myburgh C, Larsen AH, Hartvigsen J (2008) A systematic, crit-
ical review of manual palpation for identifying myofascial trig-
gers points: evidence and clinical significance. Arch Phys Med
Rehabil 89:1169–1176
45. Lucas N, Macaskill P, Irwig L, Moran R, Bogduk N (2009)
Reliability of physical examination for diagnosis of myofascial
trigger points: a systematic review of the literature. Clin J Pain
25:80–89
46. Rhudy JL, Meagher M (2000) Fear and anxiety: divergent effects
on human pain thresholds. Pain 84:65–75
J Headache Pain (2012) 13:625–637 637
123