Characteristics of early onset esotropia
7
Original Articles ~~ ~ ~ ~ Characteristics of early onset esotropia Gary Page, DOBA Hugh Ryan, FRACO Chris Prior, DOBA Justin O’Day, FRACO” Abstract Some 115 patients with a reported onset of esotropia within the first six months of life were studied retrospectively to assess ocular findings and the evolution of any changes with time. All patients had been treated by one ophthalmologist and one orthoptist since 1972. Of the 115 patients, 27% had an accommodative element associated with the esotropia. Patients with an accommodative esotropia had higher levels of hypermetropia when compared to the non- accommodative group, but there were no other distinguishing characteristics. The groups exhibited a large variation in angle size, ranging from four to 45 degrees at the initial visit. The presence of fusion, amblyopia and the degree of hypermetropia had no significant effect on the course of the squint. Amblyopia was noted in 67% of cases and appeared to stabilise at a later- than-expected age, with 66% of patients with ambylopia stabilising between eight and 11 years. Surgical intervention had no effect on the incidence of amblyopia at the initial or final visits. Key words: Amblyopia, esotropia, fusion, hyper- rnetropia. Esotropia with an onset before six months of age if commonly referred to as congenital. The charac- teristics of congenital esotropia have been described as follow^:^-^ onset before six months of age; a large, constant and stable angle ( > 15 degrees); non-accommodative esotropia; limited potential for binocular function; presence of amblyopia (35% to 72% incidence reported); and associated ocular motility defects such as dissociated vertical divergence (DVD),* inferior oblique overactions, latent nystagmus, abnormal head posture and limitations of abduction. This longitudinal study was undertaken to deter- mine if there was any variation from the above characteristics in a group of patients with a reported onset of esotropia in the first six months of life. An analysis was made to determine if there were any predictors (e.g. presence of fusion, absence of amblyopia and degree of hypermetropia) as to which patients had a better prognosis with respect to either a cosmetically satisfactory squint or the develop- ment of fusion. The patients within this study were unique in that all were examined by one ophthalmologist (HR) and one orthoptist over a long follow-up period. In addition each patient’s history had been meticu- lously recorded in exactly the same manner at each visit ensuring comparable results throughout each history. The patients were first examined between the years 1959 and 1977 at a time when the synop- tophore was in common use. Patients and methods The records of all patients were reviewed and cases were included if the following criteria were met: From St Vincent’s Hospital, Melbourne, Victoria. *Senior Ophthalmologist. Reprints: Dr J O’Day, Suite 3, 2nd Floor, 55 Victoria Parade, Fitzroy, Victoria 3065, Australia. Characteristics of early onset esotropia 15
Transcript of Characteristics of early onset esotropia

Original Articles ~~ ~ ~ ~
Characteristics of early onset esotropia Gary Page, DOBA Hugh Ryan, FRACO Chris Prior, DOBA Justin O’Day, FRACO”
Abstract Some 115 patients with a reported onset of esotropia within the first six months of life were studied retrospectively to assess ocular findings and the evolution of any changes with time. All patients had been treated by one ophthalmologist and one orthoptist since 1972.
Of the 115 patients, 27% had an accommodative element associated with the esotropia. Patients with an accommodative esotropia had higher levels of hypermetropia when compared to the non- accommodative group, but there were no other distinguishing characteristics.
The groups exhibited a large variation in angle size, ranging from four to 45 degrees at the initial visit. The presence of fusion, amblyopia and the degree of hypermetropia had no significant effect on the course of the squint. Amblyopia was noted in 67% of cases and appeared to stabilise at a later- than-expected age, with 66% of patients with ambylopia stabilising between eight and 11 years. Surgical intervention had no effect on the incidence of amblyopia at the initial or final visits.
Key words: Amblyopia, esotropia, fusion, hyper- rnetropia.
Esotropia with an onset before six months of age if commonly referred to as congenital. The charac- teristics of congenital esotropia have been described as follow^:^-^
onset before six months of age; a large, constant and stable angle ( > 15 degrees); non-accommodative esotropia; limited potential for binocular function; presence of amblyopia (35% to 72% incidence reported); and associated ocular motility defects such as dissociated vertical divergence (DVD),* inferior oblique overactions, latent nystagmus, abnormal head posture and limitations of abduction. This longitudinal study was undertaken to deter-
mine if there was any variation from the above characteristics in a group of patients with a reported onset of esotropia in the first six months of life. An analysis was made to determine if there were any predictors (e.g. presence of fusion, absence of amblyopia and degree of hypermetropia) as to which patients had a better prognosis with respect to either a cosmetically satisfactory squint or the develop- ment of fusion.
The patients within this study were unique in that all were examined by one ophthalmologist (HR) and one orthoptist over a long follow-up period. In addition each patient’s history had been meticu- lously recorded in exactly the same manner at each visit ensuring comparable results throughout each history. The patients were first examined between the years 1959 and 1977 at a time when the synop- tophore was in common use.
Patients and methods The records of all patients were reviewed and cases were included if the following criteria were met:
From St Vincent’s Hospital, Melbourne, Victoria. *Senior Ophthalmologist. Reprints: Dr J O’Day, Suite 3, 2nd Floor, 55 Victoria Parade, Fitzroy, Victoria 3065, Australia.
Characteristics of early onset esotropia 15

Table 1. Summary of patients in the non-accommodative and partially accommodative groups
Number of operations
None One Two Three Total Group
Non-accommodative 25 36 18 3 82 Partially-accommodative 16 8 4 3 31 Total 41 44 22 6 113
reported onset before six months of age; more than three years’ follow-up; no prior surgical intervention by another ophthalmologist; first examined at less than seven years of age; absence of any congenital or acquired medical condition affecting the central nervous system, thought to be a contributing factor; and absence of any impairment of the ocular media. Data from the following consultations were
selected from each patient’s history and entered into a personal computer using a relational database. Non-surgical cases: initial visit; every six months until age four years; annually until age 10 years; every two years until age 18 years; and final visit. Surgical cases were recorded as above with the addi- tion of the preoperative and postoperative visits.
The information recorded at each visit for all cases included the following:
age in years of the patient; date of assessment;
visual acuity; cover test, near and far with and without glasses; synoptophore angle measurement, fixing right and left, with and without glasses where appropriate; synoptophore fusion; ocular motility assessment; refractive state, including cycloplegic (Atropine) refraction and spectacle correction where appropriate (the full plus correction was not given for the majority of patients); and surgical details where appropriate. Details of any previous ocular history, family
history and date of birth were also recorded at the initial visit. Partially accommodative esotropia was defined as an esotropia which decreased in size when the hypermetropia was corrected, but remained manifest for both near and distance fixa- tion.8 The non-accommodative patients had no decrease in angle size with correction of their hyper- metropia. Patients defined as non-surgical did not undergo surgical correction of their esotropia. Surgical patients were those who underwent one or more operations to correct their esotropia. Statistical analysis was carried out using a statistical analysis program in consultation with an indepen- dent consultant statistician. Statistical test used were, chi-square, t-test and one-way analysis of variance.
Results Of the 11 5 patients found to meet the criteria of the study only two were found to have features of
Table 2. Mean angle measurement in degrees (f SD) for patients at the initial, final, preoperative and postoperative visits’
Group Initial Preoperativet Postoperative1 Finals
All surgical (n = 72)
Partially accommodative
Non-accommodative
Non-surgical (n = 41)
Partially accommodative
Non-accommodative
29.5 (9.8) 29.1 (9.9) 31.5 (8.9) 28.6 (10.0) 29.0 (10.0) 29.6 (9.2) 14.9 (9.5) 12.6 (8.9) 21.8 (9.0) 16.6 (10.4) 10.6 (7.0) 10.1 (6.7)
31.9 (9.0) 29.5 (9.0) 32.4 (9.7) 28.6 (9.0) 30.4 (9.0) 29.8 (9.0)
-
-
-
16.0 (8.2) 15.2 (8.4) 17.2 (7.4)
15.3 (8.8) 15.1 (8.7)
15.5 (7.5)
-
-
-
7.5 (9.0) 5.9 (8.1)
13.4 (6.2) 7.0 (3.0) 5.9 (9.1) 4.4 (8.1)
10.7 (7.4) 8.2 (6.8)
14.2 (7.7) 13.9 (7.6) 8.5 (6.5) 6.5 (4.7)
*Top figure =angle size without spectacle correction, bottom figure =angle size with spectacle correction. ?Preoperative visit refers to the visit immediately before the first or only operation. $Postoperative visit refers to the visit immediately after rhe first or-only operation. §The final visit refers to the last recorded visit in the patient’s history. The period between the postoperative and final visit may have included subsequent additional surgery.
16 Australian and New Zealand Journal of Ophthalmology 1993; 21(1)
-- I I
2 3 4 5 6 7 8 9 10 Age Wears)
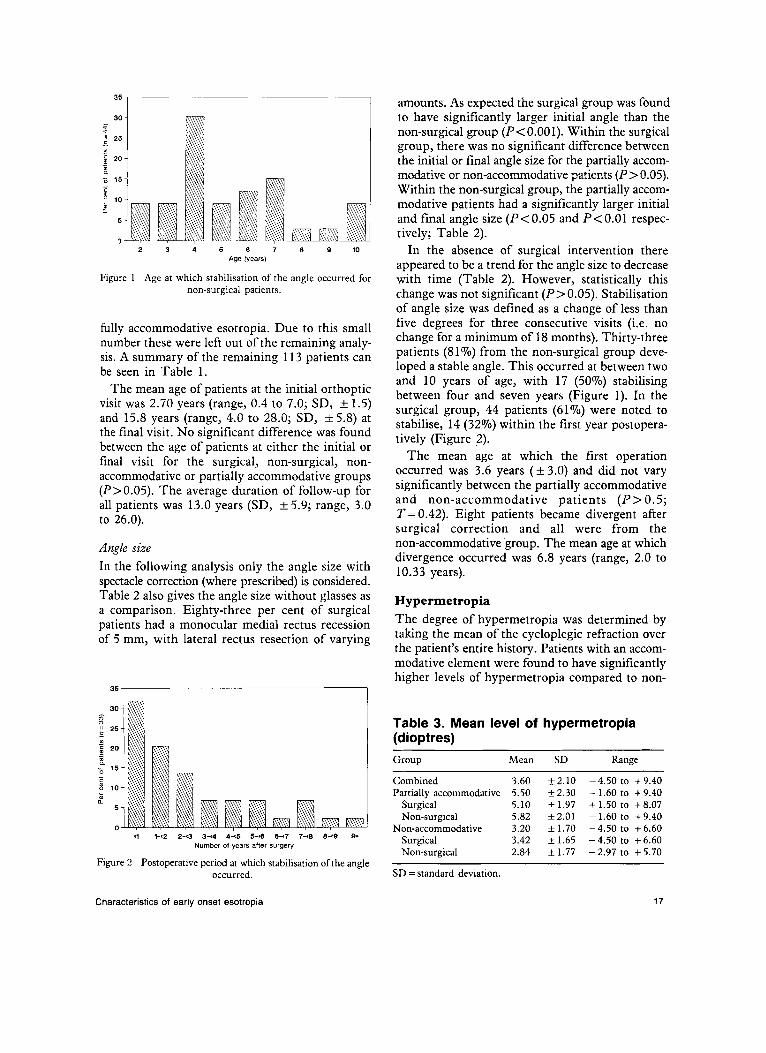
Figure 1 Age at which stabilisation of the angle occurred for non-surgical patients.
fully accommodative esotropia. Due to this small number these were left out of the remaining analy- sis. A summary of the remaining 113 patients can be seen in Table 1.
The mean age of patients at the initial orthoptic visit was 2.70 years (range, 0.4 to 7.0; SD, f 1.5) and 15.8 years (range, 4.0 to 28.0; SD, f 5.8) at the final visit. No significant difference was found between the age of patients at either the initial or final visit for the surgical, non-surgical, non- accommodative or partially accommodative groups (P>0.05). The average duration of follow-up for all patients was 13.0 years (SD, f 5.9; range, 3.0 to 26.0).
Angle size In the following analysis only the angle size with spectacle correction (where prescribed) is considered. Table 2 also gives the angle size without glasses as a comparison. Eighty-three per cent of surgical patients had a monocular medial rectus recession of 5 mm, with lateral rectus resection of varying
amounts. As expected the surgical group was found to have significantly larger initial angle than the non-surgical group (P < 0.001). Within the surgical group, there was no significant difference between the initial or final angle size for the partially accom- modative or non-accommodative patients (P > 0.05). Within the non-surgical group, the partially accom- modative patients had a significantly larger initial and final angle size (P<O.O5 and P<O.Ol respec- tively; Table 2).
In the absence of surgical intervention there appeared to be a trend for the angle size to decrease with time (Table 2). However, statistically this change was not significant ( P > 0.05). Stabilisation of angle size was defined as a change of less than five degrees for three consecutive visits (i.e. no change for a minimum of 18 months). Thirty-three patients (8 170) from the non-surgical group deve- loped a stable angle. This occurred at between two and 10 years of age, with 17 (50%) stabilising between four and seven years (Figure 1). In the surgical group, 44 patients (61%) were noted to stabilise, 14 (32%) within the first year postopera- tively (Figure 2).
The mean age at which the first operation occurred was 3.6 years (k 3.0) and did not vary significantly between the partially accommodative and non-accommodative patients ( P > 0.5; T = 0.42). Eight patients became divergent after surgical correction and all were from the non-accommodative 'group. The mean age at which divergence occurred was 6.8 years (range, 2.0 to 10.33 years).
Hypermetropia The degree of hypermetropia was determined by taking the mean of the cycloplegic refraction over the patient's entire history. Patients with an accom- modative element were found to have significantly higher levels of hypermetropia compared to non-
Table 3. Mean level of hypermetropia (dioptres) Group Mean SD Range
<i 1-~2 2-Q 3-4 44, 540 6-7 7-<a 8-9 g, Number of years after surgery
Figure 2 Postoperative period at which stabilisation of the angle occurred.
Characteristics of early onset esotropia
Combined 3.60 k2.10 -4.50 to +9.40 Partially accommodative 5.50 52.30 - 1.60 to +9.40
Surgical 5.10 51.97 +1.50 to +8.07
Non-accommodative 3.20 f 1.70 - 4.50 to + 6.60 Non-surgical 5.82 52.01 -1.60 to +9.40
S u r g i c a 1 3.42 1.65 -4.50 to f6.60 Non-surgical 2.84 k 1.77 -2.97 to + 5.70
SD =standard deviation.
17

Table 4. Comparison of the mean initial angle for patients with low, medium and high levels of hypermetropia
Initial angle (degrees) Hypermetropia Without spectacle With spectacle
correction correction
Low ( n = 36;
Medium ( n = 62;
High ( n = 15;
< =3.0 D) 20.2 (f 12.3) 20.3 (+ 12.5)
>3.0 and 56 .0 D) 25.7 (k11.5) 25.2 (k11.8)
>6.0 D) 28.0 (*11.0) 21.2 (+11.8)
accommodative patients (P< 0.0001, T= 4.85; Table 3).
With spectacle correction, patients with medium levels of hypermetropia had a significantly larger initial angle size than either of the low or high groups (P< 0.05). Without spectacle correction, patients with low levels for hypermetropia had significantly smaller initial angles than patients with medium or high levels of hypermetropia (P< 0.05). However, over all only a weak correlation (t= 0.204) between the initial angle and the level of hypermetropia was found (Table 4).
Patients with a final angle of less than or equal to five degrees had significantly lower levels of hypermetropia compared to others (3.21 D v 4.21 D respectively; P< 0.05).
Fusion The non-surgical group was found to have a signifi- cantly higher number of patients with fusion demonstrable at both the initial and final visits as compared to the surgical group (P<O.Ol and P< 0.05 respectively; Table 5).
No difference was found in the incidence of fusion at the final visit between patients with a small
five degrees) or large final angle (chi- square = 0.019, df = 1). In contrast, a significantly larger proportion of patients had fusion demon- strable at the final visit if the initial angle was less than or equal to 10 degrees (chi-squareZ8.478, df=3; Table 6).
Amblyopia Amblyopia was defined as more than one line differ- ence in the visual acuity between each eye. Eighty-eight per cent of those patients recorded as being amblyopic at the initial visit were found to have amblyopia present based on furation behaviour noted in the cover test result. All patients had visual acuity recorded at the final visit. Amblyopia was treated using full-time and/or part-time and/or partial occlusion, depending upon its severity. Atro- pine occlusion was used where compliance to the above regime was poor. Over all, 51 patients (45%) had amblyopia at their final visit and 76 (67%) at the initial visit. This did not vary significantly between any group (chi-square = 0.341, df = 8). At the final visit no significant differences were found in the number of patients with less than 6/12 vision in the squinting eye (chi-square = 0.090, df = 3) or with two lines or more difference between the two eyes (chi-square = 0.348, df = 3), for any group shown in Table 7.
Stabilisation of ambylopia was defined as no change in the difference in visual acuity between each eye for three consecutive visits. A total of 99 patients was found to have a point at which the visual acuity stabilised, 66% of these stabilised between eight and 11 years of age. The mean age when last seen of the remaining 14 patients that did not stabilise was 8.86 years (range, four to 18). No difference was found in the incidence of amblyopia between those patients with a final angle of greater than five degrees and patients with small angle (chi-square = 2.105).
Table 5. Number of patients with fusion demonstrable at the initial and final visits
. Initial visit Final visit
With Without With Without Group N R NR
Surgical 6 61 5 25 47 0 Partially accommodative 0 15 0 4 1 1 0 Non-accommodative 6 46 5 21 36 0
Non-surgical 16 25 0 24 16 1 Partially accommodative 4 12 0 8 7 1 Non-accommodative 12 13 0 16 9 0
NR = not recorded.
18 Australian and New Zealand Journal of Ophthalmology 1993; 21(1)

Table 6. Comparison of initial angle size and presence of fusion at the final visit
Total Initial angle Number Number size with fusion without fusion
510" 10 (59%) 7 (41%) 17 11" to 20" 15 (54%) 13 (46%) 28 21" to 30" 16 (47%) 18 (53%) 34 30" + 8 (24%) 26 (76%) 34
Associated anomalies Compared with the other groups the non-surgical group had a significantly smaller number of patients with inferior oblique overactions and DVD (P<0.05). The small number of patients with nystagmus meant these were unable to be compared statistically.
Discussion The mean initial angle for patients in this study (24") is similar to those found previously, but the large range associated with each group should be noted, as 32% of patients had a smaller initial angle (5 15') than those considered typical of congenital es~tropia .*-~, '~ Previous studies have suggested that convergent squint with an accommodative element rarely occurs before one year of age.',4.11-13 Our results show that 27% of patients had an accom- modative element; unfortunately at what age an accommodative element first presented could not be confirmed as most patients did not have their initial orthoptic assessment until after one year of age.
In patients who underwent surgical correction, the angle stabilised over a short time period with more than 50% stabilising within one year, regard- less of age (Figure 2). In contrast, the non-surgical patients took longer to develop a stable angle with less than 20% stabilising by age four years (Figure 1).
Hypermetrop ia Costenbader7 and Hiles14 reported that most patients with congenital esotropia (88% and 80% respectively) had low to moderate levels of hyper- metropia and Mein et aZ.8 suggest that congenital squint is associated with predominantly low levels of hypermetropia.
Our results show that there was a broad range of refractive errors ( - 4.50 to + 9.40) with the partially accommodative esotropia being associated with higher levels of hypermetropia (mean, + 5.50 D) than non-accommodative (mean, + 3.20 D; Table 3). Parks9 and Nelson et ul.' found a similar pattern.
Costenbader7 noted that the type and amount of refractive error has little effect on the size of the deviation for congenital squint. Our results show that patients with low levels of hypermetropia had slightly smaller initial angles than other patients. However, the weak correlation ( r = 0.2) found between initial angle and hypermetropia suggests that any effect hypermetropia has on the initial angle is relatively small.
Amblyopia A number of authors suggest that congenital esotropia is commonly associated with cross fixa- tion resulting in lower levels of amblyopia than for other types of s q ~ i n t . ~ , ~ . ' ~ ~ ' ~ From Table 9 it can be seen that this group of patients is associated with a higher incidence of amblyopia than found in previous studies with the exception of Robb.6 In contrast to Baker and park^,^ the incidence of amblyopia was the same regardless of whether an accommodative element was present. Our results are supported by Fletcher et u2." who also found a similar incidence of amblyopia between partially accommodative and non-accommodative esotropia.
C a l c u P reports that in a study of 142 cases of untreated early onset esotropia, 28 patients (20'70) had two or more lines difference between the two
Table 7. Number of patients with amblyopia at the initial and final visits
Final visit Group Initial visit
L 1 line difference 2 2 lines difference <6/12 in the squinting eye
Combined 76 (67%) 52 (45%) 34 (30%) Surgical 50 (69%) 33 (46%) 23 (32%) Non-surgical 26 (63%) 18 (44%) 11 (27%) Non-accommodative 54 (66%) 35 (43%) 25 (30%) Partially accommodative 22 (71%) 16 (52%) 9 (31%)
20 (18%) 13 (18%) 7 (17%)
15 (18%) 5 (16%)
Characteristics of early onset esotropia 19

Table 8. Prevalence of associated anomalies Group Inferior oblique overaaivity DVD Nystagmus Limitation of abduction
All patients 63 (56%) 34 (30%) 17 (15%) 29 (26%) Non-accommodative 43 (52%) 25 (31%) 14 (17%) 23 (20%) Partially accommodative 20 (65%) 9 (29%) 3 (10%) 6 (19%) Surgical 48 (67%) 28 (39%) 13 (18%) 18 (25%) Non-surgical 15 (37%) 6 (15%) 4 (1 0%) 10 (24%)
eyes while only 14 (9.8%) failed to reach 6/12 in the squinting eye. In contrast to this, our study found that in the non-surgical group, 11 patients (27%) had two lines or more difference between the two eyes and seven (17%) failed to achieve 6/12 by the final visit in spite of extensive follow-up and occlusion therapy. We found no difference in the proportion of patients with amblyopia between the non-surgical and any other group of patients (Table 7). Mein and Harcourts note that the critical period may last up to approximately seven years of age. Visual acuity in this group of patients appeared to stabilise at a later age, with 66% of patients stabilising between the ages of eight and 11 years. Of the 14 patients whose angle did not stabilise, six were less than six years of age at the final visit and would not be expected to have stable vision (range, four to eight, mean, 8.9 years).
Fusion Table 6 shows that a small initial angle (I 10’) was associated with a higher incidence of demonstrable fusion at the final visit. As the non-surgical group
Table 9. Comparison of amblyopia with previous studies of esotropia with an onset before six months of age
Per cent of patients with amblyopia at the initial visit
Author
Costenbader’ Von Noordens Robb6 This study
38% 35% 72% 67%
had a significantly smaller initial angle size compared with the surgical group, this could explain why this group had a higher incidence of patients with demonstrable fusion. Bair” found that 50% of patients aligned to less than 10” after 18 months of age developed fusion. In our study no difference was found in the incidence of fusion at the final visit if the final angle was less or greater than five degrees. The results suggest that the development of fision is more likely if a small angle is present early in the course of the squint and add to the case for early surgical alignment of congen- ital esotropia.
Associated anomalies The frequent and sometimes exclusive association between congenital esotropia and the features of DVD, latent nystagmus, limited abduction of the squinting eye and inferior oblique overactions is well d o c ~ m e n t e d . ~ ~ ~ - ~ ~ ~ ~ ’ ~ ~ ~ ~ F rom Table 10 it can be seen that large variations occur in the literature with regard to the frequency of the above features. Parks9 notes that congenital squint ‘is an entity involving features other than simply esotropia’, when referring to the above characteristics. From Table 8 it can be seen that patients with an accom- modative element can also exhibit the above characteristics considered typical of congenital esotropia.
Conclusion The results for this study suggest that not all patients who develop an esotropia before six months of age adhere to the pattern of congenital esotropia but instead encompass a wide range of features.
Table 10. Comparison of ocular motility defects with previous studies Author Inferior oblique overaction DVD Nystagmus Limitation of abduction
Hiles14 33% 76% 30% Not listed Robb6 27% 40% 26% 55% Von Noorden’ 68% 51% 25% Not listed This study 56% 30% 15% 26%
20 Australian and New Zealand Journal of Ophthalmology 1993; 21(1)

Esotropia with an accommodative element was found in a significant proportion of patients and was associated with higher levels of hypermetropia. No further differences between t k partially accom- modative and non-accommodat re groups were found with regard to the presenc of amblyopia or any associated ocular motilil defects. The frequency of inferior oblique overdctions and DVD was less in the non-surgical group.
Amblyopia stabilised at a later age than previously reported and surgical intervention did not seem to influence its incidence. Only a weak correlation was found between hypermetropia and initial angle size.
The development of fusion was more likely if a small angle (I loo) was present early in the course of the squint and was more frequent in the non- surgical patients. No other factors were found to predict which patients would be more likely to have a functional result at the final visit.
References 1. Nelson LB, et al. Congenital esotropia. Sum Ophthalmol
2. Von Noorden GK. Bowman lecture. Current concepts of
3. Von Noorden GK. Infantile esotropia. A continuing riddle.
1987;3 1 :363-83.
infantile esotropia. Eye 1988;2:343-57.
Am Orthopt J 1984;34:52-62.
4. Baker JD, Parks MM. Early onset esotropia. Am J Opthalmol
5. Von Noorden GK. A reassessment of infantile esotropia. XLIV Edward Jackson Memorial Lecture. Am J Ophthalmol
6. Robb RM, Rodier DW. The variable clinical characteristics and course of early infantile esotropia. J Paed Ophthalmol Strabismus 1987;24:276-81.
7. Costenbader FD. Infantile esotropia. Trans Am Ophthal Soc
8. Mein J, Harcourt B. Diagnosis and management of ocular motility disorders. London: Blackwell Scientific Publications,
9. Parks MM. Congenital esotropia vs infantile esotropia. Graefes Arch Clin Exp Ophthalmol 1988;226:106.
10. Von Noorden GK. Binocular vision and ocular motility. St Louis: Mosby, 1990;293-305.
11. Fletcher M, Silverman S. Strabismus: a study of 1110 consecutive cases. Part 2. Findings in 472 cases of partially accommodative and non accommodative esotropia. Am J Ophthal 1966;61:86.
12. Mazow ML, et al. Accommodative esotropia. Am Orthopt
13. Pollard ZF. Accommodative esotropia in the first year of life. Arch Ophthalmol 1976;94:1912-3.
14. Hiles DA, et al. Characteristics of infantile esotropia following early bi medial rectus recession. Arch Ophthalmol
15. Bair RV. Symposium: infantile esotropia. Am Orthopt J 1968; 18:5.
16. Calcutt C. The natural history of infantile esotropia. A study of the untreated condition in the visual adult. Transactions 7th International Orthoptic Congress, Nurnberg, 1991;3-8.
1980;90:11-8.
1988; 105: 1-10,
1961;59:397-429.
1986;22 1-34.
J 1984;34:77-82.
1980;98:697-703.
Characteristics of early onset esotropia 21






![C Infantile-Onset Esotropia - Ophthalmology...angle of the squint [5]. Faden or posterior scleral fixation This procedure was founded by Cuppers and was named as “the so called thread](https://static.fdocuments.us/doc/165x107/6067eb6aa9923c000b096038/c-infantile-onset-esotropia-ophthalmology-angle-of-the-squint-5-faden-or.jpg)