
CHAPTER IV KAP STUDY ON AEDES BORNE...
79
166 Ph.D Thesis Mosquito fauna CHAPTER IV KAP STUDY ON AEDES BORNE DISEASES
Transcript of CHAPTER IV KAP STUDY ON AEDES BORNE...
166
Ph.D Thesis Mosquito fauna
CHAPTER IV
KAP STUDY ON AEDES BORNE
DISEASES
Chapter IV KAP study on Aedes borne diseases
167
Ph.D Thesis Mosquito fauna
CONTENT
Chapter IV. KAP STUDY ON AEDES BORNE DISEASES
4.1 INTRODUCTION 169-183
4.1.1 Chikungunya 170
4.1.2 Dengue Fever 176
4.1.3 Vector mosquito 182
4.2 REVIEW OF LITERATURE 184-185
4.3 MATERIALS AND METHODS 186-197
4.4 OBSERVATIONS 198-231
4.4.1 Socio-economic-demographic profile of the respondents 198
4.4.2 Over-all level of Knowledge 204
4.4.3 Over-all level of Attitude and practice 214
4.4.4 Incidence of diseases 220
4.4.5 Association between socio-economic-demographic
profile and Over-all level of Knowledge 221
4.4.6 Association between socio-economic-demographic
profile and Over-all level of Attitude and Practice 225
4.4.7 Association between level of Knowledge and
over-all level of Attitude and Practice 228
4.4.8 Association between incidence of disease and
over-all level of Knowledge 230
4.4.9 Association between incidence of disease and
over-all level of Attitude and Practice 231
Chapter IV KAP study on Aedes borne diseases
168
Ph.D Thesis Mosquito fauna
4.5 DISCUSSION AND CONCLUSION 232-240
4.5.1 Socio-economic-demographic profile of the respondents 232
4.5.2 Over-all level of Knowledge 233
4.5.3 Over-all level of Attitude and practice 235
4.5.4 Incidence of vector-borne disease in the
study area (CG&DF) 236
4.5.5 Association between socio-economic-demographic
profile and Over-all level of Knowledge 236
4.5.6 Association between socio-economic-demographic
profile and Over-all level of Attitude and Practice 237
4.5.7 Association between level of Knowledge and
over-all level of Attitude and Practice 237
4.5.8 Association between incidence of disease and
over-all level of Knowledge 239
4.5.9 Association between incidence of disease and
over-all level of Attitude and Practice 240
4.5.9 Conclusions 240
GENERAL SUMMARY AND CONCLUSION OF THE STUDY 241-244
Chapter IV KAP study on Aedes borne diseases
169
Ph.D Thesis Mosquito fauna
4.1. INTRODUCTION
For the success of prevention and control of any vector-borne disease, the
most important prerequisite is community participation. Prevention of disease through
better education, knowledge, socio-economic condition and practice is the appropriate
way to keep disease away and remain healthy (Tyagi et al., 2005). Ignorance and
impoverished conditions of people contribute to creating vector breeding source and
spread of diseases and hinder disease control strategy (Wessen, 1972; Yaav et al.,
1999; Collins et al., 1997). Programme implementations need to understand the
disease related knowledge, attitude and practices of the population (Jane et al., 2002).
So the knowledge, attitude and practices of the community should be measured before
the implementation of a control programme. Deficiency, if any, should be
compensated for through proper awareness campaign. Prevention and control become
more effective when community has proper knowledge, attitude and practice
regarding disease and vector.
Knowledge, Attitude and Practice (KAP) study measures the Knowledge,
Attitude and Practices of a community. KAP Study tells us what people know about
certain things, how they feel and also how they behave. The knowledge possessed by a
community refers to their understanding of a given topic. The attitude refers to their
feelings towards this subject as well as any preconceived ideas that they may have had
towards it. The practice refers to the ways in which they demonstrate their knowledge

Chapter IV KAP study on Aedes borne diseases
170
Ph.D Thesis Mosquito fauna
and attitude through their actions. Thus KAP study is an educational diagnosis of the
community. Understanding the levels of Knowledge, Attitude and Practice will
expedite a more efficient process of awareness creation, as it will allow the program to
be tailored more appropriately to the needs of the community.
The purpose of KAP study is to assess the community level aspects of
epidemic or vector-borne diseases. Aedes-borne diseases such as DF and CG have
caused serious public health problem in Kerala, especially in rubber plantation belt. In
Kerala Ae.albopictus has been incriminated as the primary vector of DF and CG. In
the present study a sincere attempt has been made to understand the knowledge,
attitude and practice regarding Ae. albopictus mosquito and arboviral diseases such as
DF and CG among adult population of study area.
4.1.1. Chikungunya
CG is a mosquito-borne viral disease. The disease was observed for the first
time in 1952 in Tanzania. (Robinson, 1955; Lumsden, 1955). The name comes from
‘Makonde’ word which means “that which bend up” for walking with a stoop,
reflecting the posture of the person suffering from the disease. This virus has affected
millions of people in Africa, Southeast Asia since it was first reported. Sporadic cases
are regularly reported from different countries in the world. The outbreaks of CG virus
in many countries since 2005 are the most recent example to be cited. The recent
outbreaks appear to be the most severe and the biggest one caused by this virus within
the last 40 years (WHO, 2006 ; Schuffenecker et al., 2006).
Chapter IV KAP study on Aedes borne diseases
171
Ph.D Thesis Mosquito fauna
a. Origin
CG is believed to have originated in Africa (Brooks et al., 2004;
Schuffenecker et al., 2006) where it has maintained in sylvatic cycle involving
wild primates and forest dwelling Aedes mosquitoes. It was subsequently
introduced in Asia where it is transmitted from human to human by Aedes aegypti
and Aedes albopictus through an urban transmission cycle (Jupp and McIntosh,
1988).
b. Epidemiology
Since the Tanzanian outbreak in 1952, CG virus has caused outbreak in
different areas of Africa, Asia, and elsewhere. The most recent epidemic re-
emerged in Africa was documented in 1999-2000 in Kinshasa (Pastorino et al.,
2004). In Asia, epidemics have been documented in India, Srilanka, Myanmar,
Thailand, Indonesia, Philippines, Cambodia, Vietnam, Hong Kong and Malaysia.
(Sam and AbuBakar, 2006; Kamath et al., 2006). Since the beginning of 2005, CG
virus has emerged in the islands of the southwestern Indian Ocean. The outbreak
was first reported in Comoros in the beginning of the 2005 (Schuffenecker et al.,
2006; Paquet et al., 2006) . Later in the same year, the virus circulated to the other
islands and countries—Mayotte, Seychelles, Reunion and Mauritius, Madagaskar
and India.

Chapter IV KAP study on Aedes borne diseases
172
Ph.D Thesis Mosquito fauna
Fig. 4.1 Chikungunya affected states of India (Source NVBDCP)
India has a long history of CG. There was an outbreak of CG during 1963-
64 in Kolkata (Shah et al.,1964). Since its first isolation in Calcutta in 1963, there
have been several reports of CG virus infection in different parts of India, such as
Vellore, Chennai and Pondicherry in Tamil Nadu (Jadhav et al., 1965; Dandavate
et al.,1965; Thiruvengadam et al.,1965), Visakhapatanam, Rajahmundry and

Chapter IV KAP study on Aedes borne diseases
173
Ph.D Thesis Mosquito fauna
Kakinada in Andra Pradesh (Jupp and McIntosh,1988; Ravi, 2006; Yergolkar et
al., 2006). The last epidemic in India was reported from Barsi, Maharashtra in
1973 (Padbidri and Gnaneswar, 1979) when a morbidity of 37.5% was reported
from the whole town. CG virus had almost disappeared from India after 1973
and since then, no case had been reported till end of 2005 (Neogi et al., 1995;
Mourya et al., 2001). Recent reports of large scale outbreaks of fever caused by
CG virus infection in several parts of Southern India have confirmed the re-
emergence of this virus. (Enserink, 2006 ; Ravi,2006) The recent outbreak in
India started at the end of 2005 when cases of suspected fever were reported
from Andhra Pradesh and Karnataka (NICD, 2006; WHO, 2006). The initial
foci of the disease were reported from Hyderabad, Secundrabad and Anantput
district of Andra Pradesh. Several districts of Karnataka state such as Gulbarga,
Tumkur, Bidar, Raichur, Bellary, Chitradurga, Davanagere, Kolar and Bijapur
have also recorded large number of CG virus related fever cases. About 762026
suspected CG cases were reported from Karnataka during 2006. More similar
cases were reported from other states like Tamil Nadu, Kerala, Rajasthan,
Madhya Pradesh and Gujarat.
Since May-June 2006, Kerala has reported outbreaks of CG in some
localities of Kozhikode, Trivandrum, Ernakulam and Alappuzha districts. Soon
it spread to other districts, especially of central Kerala. Kottayam,
Pathanamthitta and Idukki districts showed a high incidence of CG in 2006. By
the end of 2006, all the 14 districts were affected. According to Directorate of

Chapter IV KAP study on Aedes borne diseases
174
Ph.D Thesis Mosquito fauna
Health Services Kerala, 70731 suspected cases were reported from Kerala in
2006 and 23052 in 2007. When the epidemic acquired a gigantic proportion, the
army’s medical wing was called in to assist the Kerala government mainly in its
cleanliness drives to tackle the mosquito borne viral disease. The number of
suspected cases reported from 2008 to 2011 was 24683, 11765, 11311 and 183
respectively. No death due to CG was officially reported (DHS Kerala, 2012).
c. Chikungunya Virus
Chikungunya is caused by an arbovirus, belonging to the genus
Alphavirus under the Togoviridae family. The virus is an RNA virus (Brooks et
al., 2004 ; Barrett and Weaver, 2002). The virus alternately affects vertebrates
and Arthropods. The transmission cycle of CG virus is characterized by a
periodicity of 3-4 years (Diallo et al., 1999). This silence is associated with the
development of immunity in animals. Vertical transmission has also been
reported in recent studies.( Schuffenecker et al., 2006; Weaver and Barrett,
2004)
d. Clinical features
Incubation period of disease lies between 1-12 days. Symptoms
generally develop after an incubation period of 4-7 days. The infected person
develop sudden onset of fever, severe headache, vomiting and severe arthalgia.
The symptom is less severe in children than in adults. Patients also have rashes
on the body. The rash is most intense on the trunk and the limbs. Migratory
polyarthritis usually affects the small joints. The joints of the extremities, in

Chapter IV KAP study on Aedes borne diseases
175
Ph.D Thesis Mosquito fauna
particular, become swollen and painful to the touch. In most cases the disease is
self-limiting and most symptoms disappear within 5-7 days. Occasionally other
complications may arise (Schuffenecker et al., 2006; Robinson, 1995; Paquet et
al., 2006). Although rare, the infection can result in Meningoencephalitis,
especially in newborns and those with pre-existing medical conditions.
Pregnant women can pass the virus to their fetus. Residual arthritis, with
morning stiffness, swelling and pain on movement may persist for weeks or
months after recovery. A full-fledged disease is most common among adults, in
whom the clinical picture may be dramatic. Severe cases of CG can occur in the
elderly, in the very young (newborns) and in those who are
immunocompromised. (NICD, 2006). Older patients usually continue to suffer
recurrent joint pain for several years. Deaths are very rare but have been
reported due to CG virus (Sarkar, et al., 1964)
e. Diagnosis
Chikungunya should be suspected when epidemic disease occurs with
the characteristic triad of fever, rash and rheumatic manifestations. The
definitive diagnosis can be made by laboratory means. The virus produces
neutralizing and Haemagglutination Inhibition (HI) antibodies and that helps in
making serological diagnosis. HI test is a simple diagnostic test, but it identifies
the group rather than the specific virus. IgM capture ELISA is the most
sensitive serological assay as it is vitally necessary to distinguish the disease
from DF. Virus-specific IgM antibodies may persist even for more than 6
Chapter IV KAP study on Aedes borne diseases
176
Ph.D Thesis Mosquito fauna
months. All patients will be positive by 5 to 7 day of illness. Reverse
Transcriptase Polymerase Chain Reaction is confirmatory for the identification
of virus (Brooks et al., 2004; Barrett and Weaver, 2002)
f. Treatment
The disease is self-limiting. There is no specific treatment or vaccine for
CG. Treatment is mostly supportive (bed rest, fluids) and symptoms may be
treated with analgesics and some antipyretics. Movement and mild exercise
tend to reduce stiffness and morning arthralgia, but heavy exercise may
exacerbate symptoms. Some cases may require hospitalization and appropriate
management is done for the complications. (Schuffenecker et al., 2006;
Vanlandingham et al., 2005). People affected by virus should be protected from
further mosquito bites to avoid further transmission.
4.1.2 Dengue Fever
Dengue Fever is a human disease caused by a virus and transmitted
amog human by infected mosquitoes. Dengue Fever (DF) and its severe
forms—Dengue Haemorrhagic Fever (DHF) and Dengue Shock Syndrome
(DSS)—have become major international public health concerns. Over the past
three decades, there has been a dramatic global increase in the frequency of DF,
DHF and DSS and their epidemics, with a concomitant increase in disease
incidence. It occurs commonly in tropical and subtropical regions of the world,
predominantly in urban-suburban areas. It is the most important arboviral
disease of humans, affecting 50-100 million persons annually (Gubler, 2000).
Chapter IV KAP study on Aedes borne diseases
177
Ph.D Thesis Mosquito fauna
a. Origin
The first epidemic of dengue was recorded in 1635 in the French West
Indies, although a disease outbreak compatible with dengue had been reported
in China as early as 992 AD (Howe, 1997; Gubler, 1997). During the 18th, 19th
and early 20th centuries, epidemics of dengue-like diseases were reported and
recorded globally, both in tropical as well and temperate regions.
b. Epidemiology
Dengue fever has a wide distribution in the tropical and subtropical
areas of the world, with over 2.5 billion people living in dengue endemic areas
(Halstead, 1980, Rosen, 1982). The currently known geographical distribution
of the various dengue virus serotypes reflects the development of
hyperendemicity in most tropical areas of the world in the past 15-20 years. In
1997, DF/DHF has been the most important arboviral disease of humans, with
an estimated 50 to 100 million cases of DF and several hundred thousand cases
of DHF occurring each year, depending on epidemic activity (Monath, 1994).
Currently, DHF is a leading cause of hospitalization and death among children
in many south-east Asian countries where epidemics first occurred in the 1950s
(WHO, 1986). Epidemic DHF spread to the South Pacific islands in the 1970s,
and reached the Caribbean Basin in the 1980s (Gubler, 1987). The pattern of
severe haemorrhagic disease has evolved in the American region in the 1980s
and 1990s in a manner similar to the way it did in south-east Asia in the 1960s
and 1970s (Gubler, 1987,1993).
Chapter IV KAP study on Aedes borne diseases
178
Ph.D Thesis Mosquito fauna
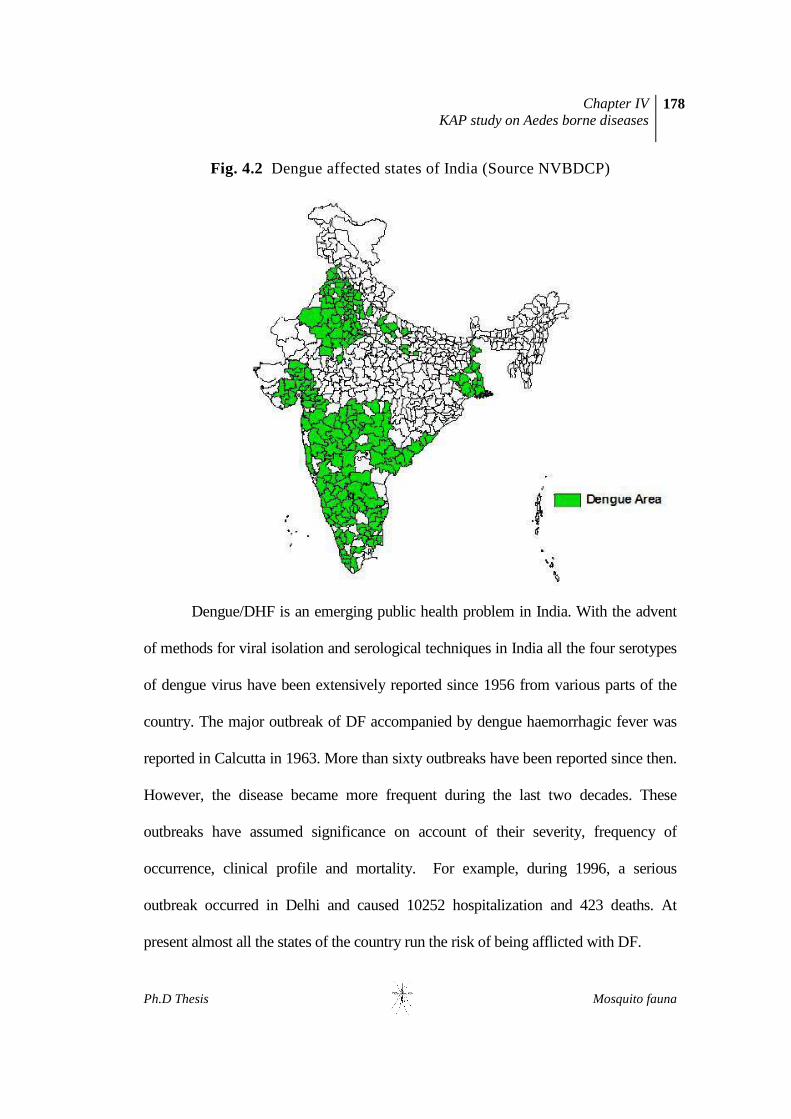
Fig. 4.2 Dengue affected states of India (Source NVBDCP)
Dengue/DHF is an emerging public health problem in India. With the advent
of methods for viral isolation and serological techniques in India all the four serotypes
of dengue virus have been extensively reported since 1956 from various parts of the
country. The major outbreak of DF accompanied by dengue haemorrhagic fever was
reported in Calcutta in 1963. More than sixty outbreaks have been reported since then.
However, the disease became more frequent during the last two decades. These
outbreaks have assumed significance on account of their severity, frequency of
occurrence, clinical profile and mortality. For example, during 1996, a serious
outbreak occurred in Delhi and caused 10252 hospitalization and 423 deaths. At
present almost all the states of the country run the risk of being afflicted with DF.
Chapter IV KAP study on Aedes borne diseases
179
Ph.D Thesis Mosquito fauna
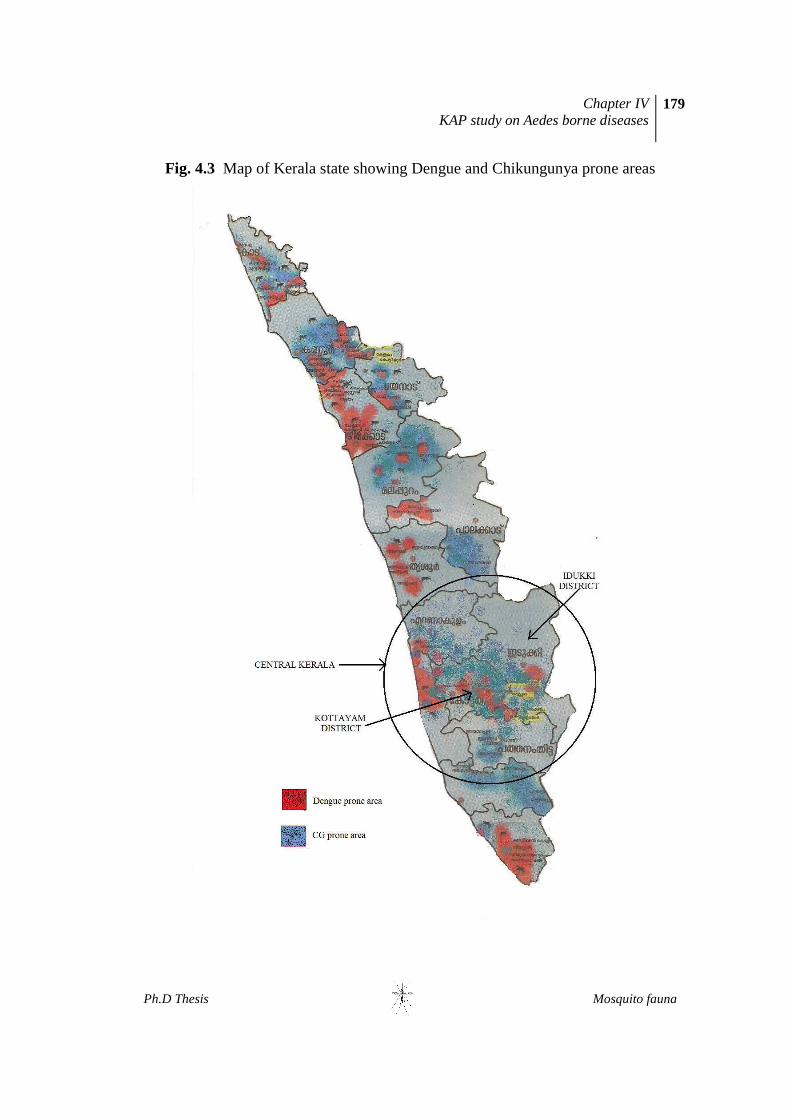
Fig. 4.3 Map of Kerala state showing Dengue and Chikungunya prone areas
Chapter IV KAP study on Aedes borne diseases
180
Ph.D Thesis Mosquito fauna
In Kerala, DF was first appeared in 1997 when 14 suspected cases with
4 deaths were reported from Kottayam district. This was followed by an
outbreak with 67 cases with 13 deaths in the same district in 1998. By 2001, DF
which was confined to Kottayam district, spread to neighbouring districts like
Ernakulum and Idukki. Sixteen cases were reported from these districts (DHS
Kerala, 2005), followed by 219 cases in 2002 with some death in the state. The
year 2003 experienced a severe epidemic yielding 3546 confirmed cases and a
toll of 68 lives, spread for the first time all over the Kerala’s fourteen districts.
(ICMR, 2006). Since then, DF cases reports became a routine affair in all the
fourteen districts in Kerala.
c. Dengue Virus
Dengue is caused by Dengue virus (DENV). It is a single stranded RNA
positive-strand virus of the family Flaviviridae, genus Flavivirus. Human
dengue can be caused by four distinct serotypes- DEN-1, DEN-2, DEN-3, and
DEN-4. The four dengue serotypes are sufficiently different that infection with
one type does not provide immunity for infection with the others.
d. Clinical features
Dengue virus infection causes a spectrum of illness ranging from
inapparent or mild febrile illness to severe and fatal haemorrhagic disease.
Clinical presentation in both children and adults may vary in severity,
depending on the strain and serotypes of the infecting virus, and the immune
status, age and the genetic background of the patient. However classical DF is
Chapter IV KAP study on Aedes borne diseases
181
Ph.D Thesis Mosquito fauna
characterized by a sudden onset of fever and one or more of a number of non-
specific signs and symptoms such as severe headache, backache, joint pains,
nausea and vomiting, eye pain, and rash. (WHO, 1986; Gubler, 1988; Siler et
al., 1926). Generally, younger children are more affected than older children
and adults. Anorexia, queer taste sensation and mild sore throat are not
uncommon. Clinical laboratory findings associated with DF include leukopenia,
and in some patients thrombocytopenia and elevated liver enzymes.
Dengue hemorrhagic fever is characterized by a fever that lasts from 2
to 7 days, with general signs and symptoms that could occur with many other
illnesses (e.g., nausea, vomiting, abdominal pain, and headache). The critical
stage in DHF occurs when the patient develops a capillary-leak syndrome, with
signs of circulatory failure and haemorrhagic manifestations such as skin
haemorrhages, bleeding nose or gums, and possibly internal bleeding.
Thrombocytopenia (<100 000/mm3) and elevated haematocrit are prominent
features. DHF can be a very dramatic disease with the patient’s condition
deteriorating very rapidly with the onset of shock and resulting in death if the
plasma leakage is not detected and corrected with fluid replacement therapy.
Leukopenia, thrombocytopenia and haemoconcentration are constant findings;
hepatomegaly and elevated liver enzymes are common.
e. Diagnosis
The diagnosis of DF is usually made when a patient exhibits the typical
clinical symptoms of headache, fever, eye pain, severe muscle-aches and rash.

Chapter IV KAP study on Aedes borne diseases
182
Ph.D Thesis Mosquito fauna
f. Treatment
Because dengue is caused by a virus, there is no specific medicine or
antibiotic to treat it, the only treatment is to treat the symptoms. For typical
dengue, the treatment is purely concerned with relief of the symptoms
(symptomatic). Rest and fluid intake for adequate hydration is important.
4.1.3 Vector Mosquito
a. Characteristics and behaviour
Ae.albopictus acts as the primary vector of DF and CG in Kerala.
Epidemics are sustained by human-mosquito-human transmission.
Characteristics of the vector are detailed in the chapter 3. The species is a peri-
domesticated one and all its biological activities like breeding, resting, feeding,
mating and oviposition are confined around human dwelling, within a radius of
100 meters. These mosquitoes usually breed in clean water collections in
containers, tanks, disposables, tree holes, junk materials in peri-domestic
situations. Rainfall influences the seasonal pattern of the species. Asian tiger
mosquitoes occur in urban, suburban and rural regions. They can also exist in
woodlands, particularly on the outer fringes close to human settlements. The
Asian tiger mosquito bites during the day time, mostly during the morning and
early evening. Depending upon region and biotype there are differing active
peaks (WHO,1999).

Chapter IV KAP study on Aedes borne diseases
183
Ph.D Thesis Mosquito fauna
b. Vector Control
Both larval and adult control measures are recommended for reducing
the vector population density. However, breeding source reduction is the best
method for Aedes control. Specific measures for controlling larvae of Aedes
mosquito are detailed in chapter 3. Adult mosquitoes can be controlled by
outdoor chemical spray around the houses; however, larval control is more
economical and provides sustainable control.
Chapter IV KAP study on Aedes borne diseases
184
Ph.D Thesis Mosquito fauna
4.2. REVIEW OF LITERATURE
4.2.1. KAP studies
Participation and co-operation of population is essential to the
implementation of control activities. Studies pertaining to knowledge, attitude and
practices showed that direct interaction with community played an important role
in controlling many mosquito borne diseases (Collin et al., 1997; Singh et al.,
1998). Van Benthem et al., (2002) observed that people with knowledge of dengue
had a significantly higher use of preventive practices than people without
knowledge of Dengue.
Abedi et al., (2011) conducted a cross sectional study in Aligarh, India, to
asses knowledge, attitude and preventive practices on dengue. A significant
positive correlation was found between knowledge and practice, but no significant
correlation was found between attitude and knowledge and attitude and practice.
The results have suggested that good attitude does not translates into good
practices, therefore, health promotion activities should be strengthened for
improving knowledge, so as to ensure that people are receptive to the messages
and make it easier for them to adopt desired change of behaviour.
A study from Cameroon showed that poor knowledge of disease
transmission led to incorrect methods of preventive measures. A good percentage
of respondents practised incorrect malaria preventive measures. Prevention of

Chapter IV KAP study on Aedes borne diseases
185
Ph.D Thesis Mosquito fauna
disease was consistent with the educational status of the participants (Dickson et
al., 2011)
Itrat et al., (2008) conducted a hospital based study to assess the level of
knowledge, attitudes and practices regarding DF in adult population Karachi,
Pakistan. This study showed that literate individuals were relatively more well-
informed about DF as compared with the illiterate people. However knowledge
based upon preventive measures was found to be predominantly focussed towards
prevention of mosquito bites rather than eradication of mosquito population.
Koenraadt et al., (2006) observed a positive correlation between knowledge
of Dengue prevention and source elimination practice. The study also reported that
no relationship existed between knowledge of DF and adult mosquito reduction
practices.
Matta et al., (2006) conducted a hospital based KAP on DF in Delhi.
Though knowledge regarding dengue transmission, breeding ground, etc was good
among the respondents, practices for the elimination of breeding sites were not
commendable.
Kumar and Gururaj (2005) conducted a KAP study on mosquito borne
diseases in Karnataka and showed that many people were unaware of the breeding
sites of mosquito. Similarly one third of the respondents did not know any
preventive measures against mosquitoes at community level.

Chapter IV KAP study on Aedes borne diseases
186
Ph.D Thesis Mosquito fauna
Because of the small number of KAP studies and conflicting results,
relationships among demographic factors, knowledge, practices, and mosquito
infestation are not well understood in countries like India. A better understanding
of how these factors interact to create patterns of behaviour, mosquito infestation,
and disease exposure risk would be valuable in creating more effective awareness
campaigns and source eradication programme. Despite the magnitude of vector-
borne diseases, no documented evidence exists on the KAP of people of Kerala,
especially in respect to Aedes mosquitoes. In the present study an attempt has been
made to understand the knowledge, attitude and practice regarding Aedes mosquito
among the adult population of Kerala.
4.2.2. Objectives
The broad objective of the study was to understand Knowledge, Attitude and
Practice (KAP) of people regarding Ae.albopictus and Ae. albopictus-borne
diseases such as DF and CG. The specific objectives were:-
1. To analyse the socio-economic-demographic profile of the respondents.
2. To study the Over-all Level of Knowledge of respondents about Ae.
albopictus and Ae. albopictus –borne diseases (CG&DF).
3. To study the Over-all Level of Attitude and Practice of respondents
about disease prevention and control
4. To record the extent of incidence of Ae. albopictus –borne diseases in the
study area.

Chapter IV KAP study on Aedes borne diseases
187
Ph.D Thesis Mosquito fauna
5. To study the association of socio-economic-demographic status with the
over-all level of knowledge about Ae. albopictus and Ae. albopictus -
borne diseases (CG&DF)..
6. To study the association of socio-ecnomic-demographic status with the
over-all level of attitude and practice about disease prevention and control
7. To study the association between over-all level of knowledge and over-all
level of attitude and practice regarding disease prevention and control.
8. To correlate the association of incidence of disease with the over-all level
of knowledge about Ae. albopictus and Ae. albopictus - borne diseases
(CG&DF)..
9. To correlate the association of incidence of vector-borne disease with the
over-all level of attitude and practice regarding disease prevention and
control.
Chapter IV KAP study on Aedes borne diseases
188
Ph.D Thesis Mosquito fauna
4.3. MATERIALS AND METHODS
4.3.1 Study area and population
Mundakayam Panchayat, belonging to Kanjirappally taluk of Kottayam
district was selected for the present Study (Fig 3.1). Selection of study area was
purposive, based on the previous history of vector borne diseases and the
panchayat being a rubber plantation area. Kanjirappally is popularly known as the
capital of rubber production in India. In Kerala Dengue Fever was first reported
from this Panchayat. Heavy incidence of CG was experienced in 2006 and 2007.
Mundakayam panchayat belonging to Kanjirappally taluk of Kottayam
district was selected for the KAP Study. Mundakayam is located 55 kms east of
Kottayam district headquarters and situated on latitude 9°33’ N a longitude 76 °53’
E. Panchayat has an area of 82 sq.km. and divided into 20 wards (at the time of
study). (In 2005 Panchayat was divided and formed Koruthoodu Panchayat). It is
bordered by Kanjirappally, Parathode, Koruthoode and Erumely panchayats. As of
2001 India census, Panchayat has a population of 47987 and has an average
literacy rate of 94 %. There are 12260 households within the panchayat limitan
and population density is 580. Mundakayam is a highland area and is a gateway to
the highrange. Rubber plantation is the main source of income. Besides some
estates (above 20 hectare), rubber plantation in this area is mainly owed by small
scale farmers (mostly below 2 hectare per owner) (Mundakayam Panchayat,2008).
Chapter IV KAP study on Aedes borne diseases
189
Ph.D Thesis Mosquito fauna
4.3.2. Study design and Sampling technique
A cross sectional study was conducted between May 2010 and July 2010 in
the selected site. A house was considered as a unit for the survey and every 10th
house was selected for the study. The nearby house was considered in case of any
inconvenience. Thirty houses each were sampled from 7 randomly selected wards.
Thus a total of 210 houses were surveyed during the present study. People above
the age 18 (adults) were considered for the survey. Before the survey a verbal
consent for a face to face interview was sought from the eldest available member
of the family. The purpose of the study was also intimated. The medium of
communication was Malayalam. At the end of the interview each respondent was
given sufficient clarification and other information regarding vector characteristics,
preventive measures, breeding source eradication, etc. The information given by
each respondent was kept confidential.
4.3.3. Research Tool
The survey was based on a self-prepared pre-tested structured questionnaire
consisting of 30 questions, which was intended to collect data regarding basic
demography, knowledge regarding CG and DF, vector characteristics, personal
preventive and source reduction practices (Appendix-III). As no suitable
readymade questionnaire was available, it was prepared based on the literature and
under the supervision of entomologists and epidemiologists of various institutions.
Self prepared questionnaire was pretested among 40 people and made necessary
changes before the administration of the questionnaire.
Chapter IV KAP study on Aedes borne diseases
190
Ph.D Thesis Mosquito fauna
Questions in the questionnaire were grouped into 7 categories as follows:
Category 1 – Socioeconomic- demographic profile
This category contained 6 questions (Question 1 to 6), which were intended
to collect data regarding basic demographic profile of the study population, such as
age, sex, education, occupation and financial background. A single question on
source of information was also included in this category.
Category 2 – Knowledge regarding CG
There were 6 questions (Question 7 to 12) in this category and were asked
to assess the knowledge of the respondent regarding various aspects of CG such as
awareness of CG, causative parasite, symptoms, mode of transmission, vector and
possibility of causality due to CG.
Category 3 – Knowledge regarding DF
This category contained 6 questions (Question 13 to 18) and was intended
to gauge the knowledge of respondent regarding awareness of DF, causative
parasite, symptoms, mode of transmission, vector and possibility of causality due
to DF.
Category 4 – Knowledge regarding vector mosquito
This section contained 4 questions (Question 19 to 22). These questions
were framed to collect information regarding vector characteristics such as biting
time, feeding preference, breeding sites and their ability to identify the Aedes.
Chapter IV KAP study on Aedes borne diseases
191
Ph.D Thesis Mosquito fauna
Category 5 – Personal preventive practices against vector biting
There were only two questions in this part (Question 23 and 24) and were
designed to know the personal preventive practices of respondents against Aedes
biting.
Category 6 – Attitude and practice towards vector control and treatment
This category included questions related to the attitude and practice of
respondents towards source reduction and diseases treatment. There were 5
questions in this section (Question 25 to 29). The first one asked the respondents to
select the best mosquito control measure. The second and third questions were
included to measure the attitude and participation of respondent towards mosquito
control measures. The fourth question was peculiar and not put to the respondent.
Instead the interviewer observed the premises for positive larval containers. The
fifth question was pertaining to the source of treatment in the case diseases
Category 7 – Incidence of vector borne disease (CG&DF)
The single question of this category (Question 30) asked the respondent
whether there was any incidence of DF/CG in the past or present.
4.3.4. Analysis of Data
Collected data was entered in a computer and analysed by using Statistical
Package for Social Science (SPSS) software version 17. The analysis was done at
3 stages. The objective of the first stage was to summarise the response of

Chapter IV KAP study on Aedes borne diseases
192
Ph.D Thesis Mosquito fauna
participants. Descriptive statistics (frequency, percentage) were used to summarize
the responses to each question. Summarised data is presented in suitable tables .
In the second stage the over-all level of knowledge of respondents about
the Ae.albopictus and Ae.albopictus -borne disease and over-all level of attitude
and practice regarding the disease prevention and control was calculated. One
score was assigned to each correct response while zero for inappropriate response
to a question. For multiple response questions the score (one) was equality divided
among the correct choices, wherever appropriate.
A. Calculation of over-all level of knowledge of respondents about the
Ae.albopictus and Ae.albopictus-borne disease
Before calculating the over-all level of knowledge about the Ae.albopictus
and Ae.albopictus-borne disease, knowledge level of respondent regarding CG
(category 2), DF (category 3) and Aedes vector (category 4) was measured
separately. Total score of a respondent in each category was calculated by adding
the score of individual question falling in that category. The minimum possible
score for any respondent was zero while maximum possible score varied with
number of question in each category. Based on the points scored respondents were
divided into three levels- low, moderate and high. Cut off score was determined
arbitrarily by dividing the maximum score by three. Score less than 1/3(upto 33.33
% of the total) of the total score forms the low level, those higher than 2/3 (above
66.66% of the total) of the total score forms the high level and score in between
these two scores (above 33.33 &below 66.66 of the total) forms the moderate level.

Chapter IV KAP study on Aedes borne diseases
193
Ph.D Thesis Mosquito fauna
i. Calculation of level of knowledge regarding CG (Category 2 )
The maximum possible score under this category is 6 (sum of the scores of
all the 6 questions). So the score secured by any respondent varied from 0 (possible
minimum) to 6 (possible maximum) points and were grouped into 3 levels as
follows:
Level of knowledge Score range
Low level (upto33.33%) - 0 to 2 score
Moderate level (between l33.33% & 66.66%) - 2.1 to 4 score
High level (above 66.66%) - 4.1 to 6
ii. Calculation of level of knowledge regarding DF (Category 3)
The maximum possible score under this category is 6 (sum of the scores of
all the 6 questions). So the score secured by any respondent varied from 0
(Possible minimum) to 6 (possible maximum) points and were grouped into 3
levels as follows:
Level of knowledge Score range
Low level(upto33.33%) - 0 to 2 score
Moderate level(between l33.33% & 66.66%)- 2.1 to 4 score
High level(above 66.66%) - 4.1 to 6
Chapter IV KAP study on Aedes borne diseases
194
Ph.D Thesis Mosquito fauna
iii. Calculation of level of knowledge regarding vector mosquito (Category 4)
For multiple response questions the score was equally divided among the
correct choices. The score varied from 0 to 4 points and were grouped into 3 levels
as follows:
Level of knowledge Score range
Low level(upto33.33%) - 0 to 1.3 score
Moderate level(between l33.33% & 66.66%)- 1.4 to 2.6 score
High level (above 66.66%) - 2.7 to 4 score
Knowledge level of respondents regarding CG and DF was compared.
For the calculation of over-all level of knowledge of respondents about the
Ae.albopictus and Ae.albopictus-borne disease, responses to category 2
(knowledge regarding CC), category 3 (knowledge regarding DF) and category 4
(knowledge regarding vector mosquito) was considered together. The minimum
possible score for any respondent was zero while maximum possible score was 16
(as there were 16 questions under the above 3 categories). Based on the points
scored respondents were divided into three levels- low, moderate and high. Cut off
score was determined arbitrarily by dividing the maximum score (16) by three.
Score less than 1/3 (upto 33.33 % of the total 16) of the total forms the low level,
those higher than 2/3 (above 66.66% of the total 16) of the total score forms the
high level and score in between these two scores (above 33.33 & below 66.66 of
the total 16) forms the moderate level, as follows:
Chapter IV KAP study on Aedes borne diseases
195
Ph.D Thesis Mosquito fauna
Over-all level of knowledge Score range
Low level (upto33.33%) - 0 to 5.30 score
Moderate level (between l33.33% & 66.66%) - 5.31 to 10.6 score
High level (above 66.66%) - 10.7 to 16 score
B. Calculation of over-all level of attitude and practice about disease
prevention and control
Over-all level of attitude and practice about disease prevention and control was
calcualated from the responses aginst category five and six.
i. Level of personal preventive practices against vector biting (Category 5 )
First question of this category is multiple response type with two correct
answers. Any one of these responses was sufficient to take protection against
mosquito bite. So score of one was assigned for either or both responses. The total
scores of this category varied from 0 to 2 and were divided into 3 levels as follows:
Level of attitude and practice Score range
Low level (upto33.33%) - 0 to 0.66 score
Moderate level (between l33.33% & 66.66%) - 0.67 to 1.32 score
High level (above 66.66%) - 1.34 to 2 score

Chapter IV KAP study on Aedes borne diseases
196
Ph.D Thesis Mosquito fauna
ii. Level of attitude and practice towards vector control and treatment
(Category 6 )
There were 5 questions in this section. For assessing knowledge level one
score was assigned to each suitable response and zero for inappropriate response to
a question.
Level of attitude and practice Score range
Low level (upto33.33%) - 0 to 1.66 score
Moderate level (between l33.33% & 66.66%) - 1.67 to 3.33 score
High level (above 66.66%) - 3.34 to 5 score
For the calculation of over-all level of attitude and practice of respondents
about the disease prevention and control, responses to category 5 (personal
preventive practices against vector biting), and category 6 (vector control and
treatment) was considered together. The score varied from 0 to 7 points and were
grouped into 3 levels of practice as follows:
Over-all Level of Attitude and Practice Score range .
Poor (upto33.33%) - 0 to 2.3 score
Fair (between l33.33% & 66.66%) - 3.4 to 4.6 score
Healthy (above 66.66%) - 4.7 to 7 score
Mean, Standard Deviation, Minimum and Maximum scores were also
determined for each category.

Chapter IV KAP study on Aedes borne diseases
197
Ph.D Thesis Mosquito fauna
Finally, association between socio-economic-demographic profile and
over-all level of knowledge; association between socio-economic-demographic
profile and over-all level of attitude and practice regarding disease preventive
practices were analysed and presented in a graspable and comprehensible manner.
Similarly association between over-all level of knowledge and over-all level of
preventive practices were analysed. Association between incidences of disease and
over-all level of knowledge; association between incidences of disease and over-all
level of preventive practices were also measure. Chi-squire was used to find out
the significance of association.
Chapter IV KAP study on Aedes borne diseases
198
Ph.D Thesis Mosquito fauna
4.4. OBSERVATIONS
The collected data was processed using suitable statistical tools and
presented in the form of tables and graphs. The data regarding Socio-economic-
demographic profile of the respondents, knowledge on CG, DF and Ae.albopictus,
attitude and practice regarding personal protection and vector control, association
of socio-demographic status with overall level of knowledge and overall
preventive practices, association between overall knowledge and overall preventive
practices and finally association of incidence of diseases with overall level of
knowledge and with overall prevention are provided in the following part of the
chapter.
4.4.1 Socio-economic-demographic profile of the respondents
The present study was conducted among 210 households of Mundakayam
panchayt of Kottayam district. Socio-economic-demographic profile of the
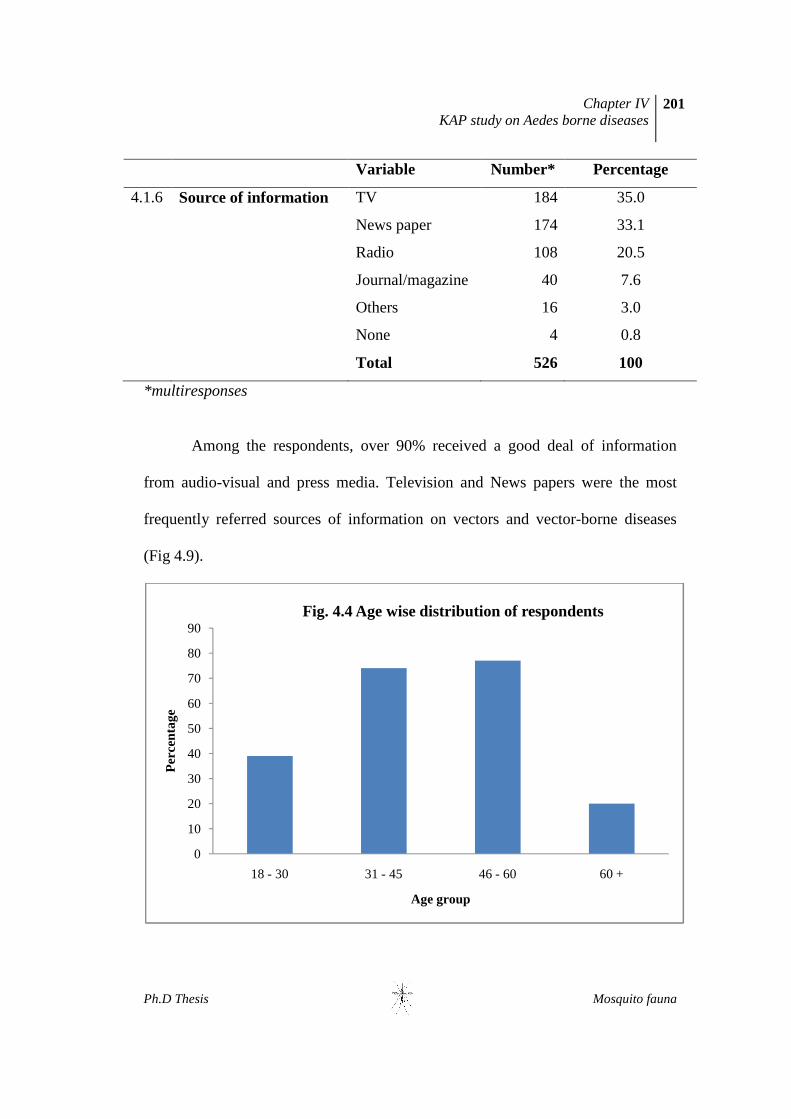
participants is given in the table 4.1. The age of the respondents varied from 18 to
75. The majority of respondents belong to the age group 46-60 (36.7%) and 31-45
(35.2%) (Fig 4.4). Males constituted the major respondents and formed about 66%
of the total (Fig 4.5). Respondents were well-educated - 31% had secondary
education while 23.3 % had higher secondary education (Fig 4.6). The people of
study area were engaged in various occupations. Agriculture/rubber plantation was
the major occupation of the people (23.5%). 20% of the respondents were busy
with house hold activities, especially female. Business men, government
Chapter IV KAP study on Aedes borne diseases
199
Ph.D Thesis Mosquito fauna
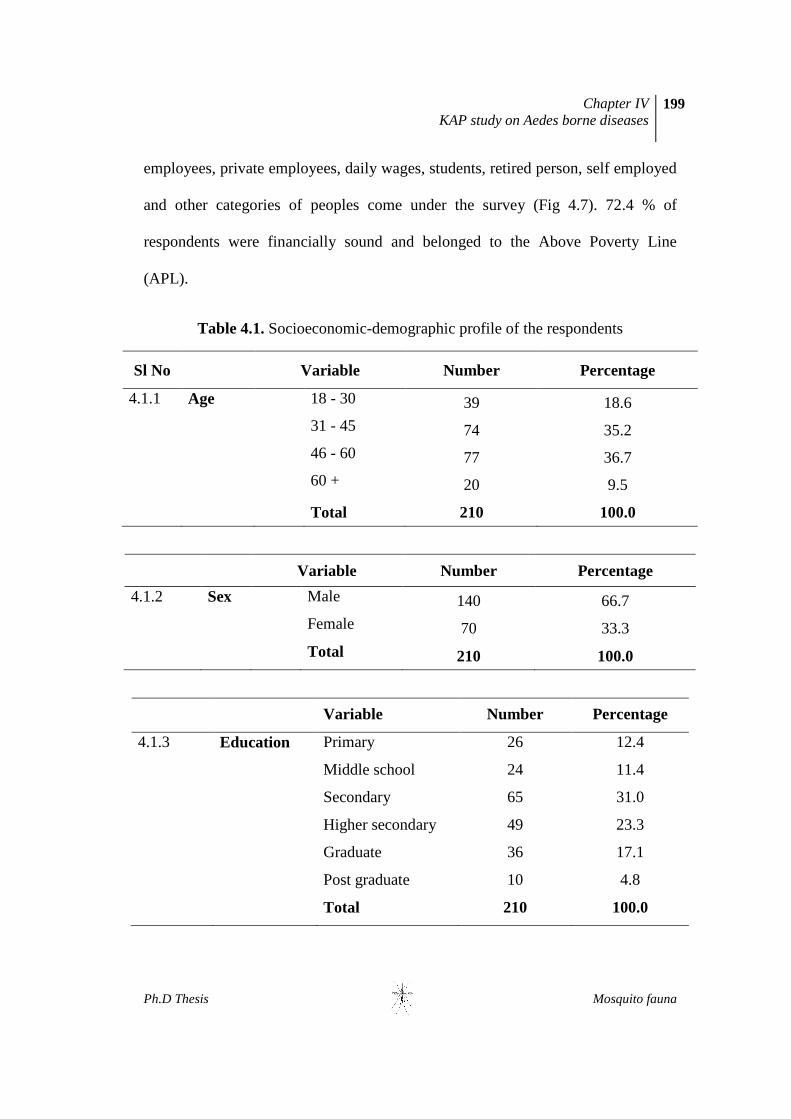
employees, private employees, daily wages, students, retired person, self employed
and other categories of peoples come under the survey (Fig 4.7). 72.4 % of
respondents were financially sound and belonged to the Above Poverty Line
(APL).
Table 4.1. Socioeconomic-demographic profile of the respondents
Sl No Variable Number Percentage
4.1.1 Age 18 - 30 39 18.6
31 - 45 74 35.2
46 - 60 77 36.7
60 + 20 9.5
Total 210 100.0
Variable Number Percentage
4.1.2 Sex Male 140 66.7
Female 70 33.3
Total 210 100.0
Variable Number Percentage
4.1.3 Education Primary 26 12.4
Middle school 24 11.4
Secondary 65 31.0
Higher secondary 49 23.3
Graduate 36 17.1
Post graduate 10 4.8
Total 210 100.0

Chapter IV KAP study on Aedes borne diseases
200
Ph.D Thesis Mosquito fauna
Variable Number Percentage
4.1.5 Financial
background
APL 152 72.4
BPL 58 27.6
Total 210 100.0
Variable Number Percentage
4.1.4 Occupation Business 13 6.1
Govt employee 15 7.1
Pvt employee 10 4.8
Plantation/agriculture 49 23.3
Daily wager 24 11.4
House hold 42 20.0
Student 10 4.8
Retired 1 0.5
Self employed 14 6.7
Others 32 15.2
Total 210 100.0
Chapter IV KAP study on Aedes borne diseases
201
Ph.D Thesis Mosquito fauna
Variable Number* Percentage
4.1.6 Source of information TV 184 35.0
News paper 174 33.1
Radio 108 20.5
Journal/magazine 40 7.6
Others 16 3.0
None 4 0.8
Total 526 100
*multiresponses
Among the respondents, over 90% received a good deal of information
from audio-visual and press media. Television and News papers were the most
frequently referred sources of information on vectors and vector-borne diseases
(Fig 4.9).
0
10
20
30
40
50
60
70
80
90
18 - 30 31 - 45 46 - 60 60 +
Per
cent
age
Age group
Fig. 4.4 Age wise distribution of respondents

Chapter IV KAP study on Aedes borne diseases
202
Ph.D Thesis Mosquito fauna
66.7
33.3
Fig. 4.5 Sex wise distribution of respondents
Male
Female
0
5
10
15
20
25
30
35
Primary Middle school
Secondary Higher secondary
Graduate Post graduate
Per
cent
age
Fig 4.6 Education level of respondents
Education

Chapter IV KAP study on Aedes borne diseases
203
Ph.D Thesis Mosquito fauna
0
5
10
15
20
25
Per
cent
age
Fig 4.7 Occupation of respondents
Occupation
72%
28%
Fig 4.8 Financial back ground of respondents
APL
BPL

Chapter IV KAP study on Aedes borne diseases
204
Ph.D Thesis Mosquito fauna
4.4.2. Over-all Level of Knowledge of respondents
Before assessing the over-all level of knowledge about the Ae.albopictus
and Ae.albopictus-borne diseases (CG&DF), knowledge level of respondent
regarding CG (category 2), DF (category 3) and Aedes vector (category 4) was
measured separately.
a. Knowledge of respondents about Chikungunya (CG)
This category comprised 6 questions which were intended to collect
information concerning CG. The details of responses are given in the table 4.2. All
the respondents had heard of a disease called CG. A good proportion of
respondents (38%) knew that virus is the causative agent of CG. The majority were
0
5
10
15
20
25
30
35
40
Per
cent
age
Fig. 4.9 Sources of information
Chapter IV KAP study on Aedes borne diseases
205
Ph.D Thesis Mosquito fauna
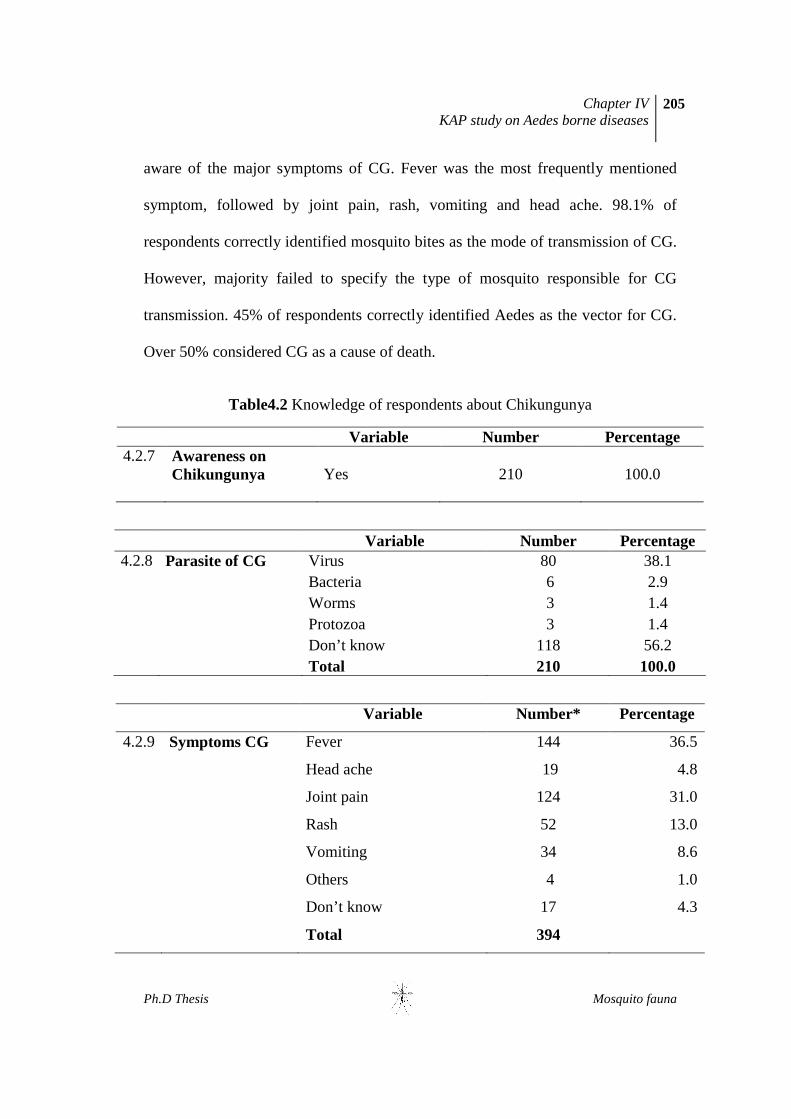
aware of the major symptoms of CG. Fever was the most frequently mentioned
symptom, followed by joint pain, rash, vomiting and head ache. 98.1% of
respondents correctly identified mosquito bites as the mode of transmission of CG.
However, majority failed to specify the type of mosquito responsible for CG
transmission. 45% of respondents correctly identified Aedes as the vector for CG.
Over 50% considered CG as a cause of death.
Table4.2 Knowledge of respondents about Chikungunya
Variable Number Percentage 4.2.7 Awareness on
Chikungunya
Yes 210 100.0
Variable Number Percentage 4.2.8 Parasite of CG Virus 80 38.1 Bacteria 6 2.9 Worms 3 1.4 Protozoa 3 1.4 Don’t know 118 56.2 Total 210 100.0
Variable Number* Percentage
4.2.9 Symptoms CG Fever 144 36.5
Head ache 19 4.8
Joint pain 124 31.0
Rash 52 13.0
Vomiting 34 8.6
Others 4 1.0
Don’t know 17 4.3
Total 394

Chapter IV KAP study on Aedes borne diseases
206
Ph.D Thesis Mosquito fauna
Variable Number Percentage
4.2.10 Mode of
transmission of CG
Mosquito bite 206 98.1
Personal contact 1 .5
Air borne 2 1.0
Don’t know 1 .5
Total 210 100.0
Variable Number Percentage
4.2.11 Name of the
CG vector
Aedes 95 45.2
Anopheles 4 1.9
Culex 3 1.4
Don’t know 108 51.4
Total 210 100.0
Variable Number Percentage
4.2.12 Death by CG Yes 106 50.5
No 92 43.8
Don’t know 12 5.7
Total 210 100.0
Table 4.3 Knowledge Level of respondent regarding CG
Level Number Percentage
Low level (0-2) 4 1.9
Moderate level (2.1-4) 137 65.2
High level (4.1-6) 69 32.9
Total 210 100.0
Mean=3.6 S. D =0.87 Min. 1.4 Max.5.8

Chapter IV KAP study on Aedes borne diseases
207
Ph.D Thesis Mosquito fauna
Level of knowledge of study population was calculated based on the
response of the participants (Table 4.3). About 65% of respondents had moderate
level of knowledge while 32.9% had a high level of knowledge. The mean score of
respondents regarding CG was 3.6 with a standard deviation of 0.87. Minimum
score secured by any respondent was 1.4 and maximum was 5.8.
b. Knowledge of respondents about Dengue Fever (DF)
This section contains 6 questions pertaining to DF. Details of the
knowledge of the participants regarding dengue Fever are given in the table 4.4.
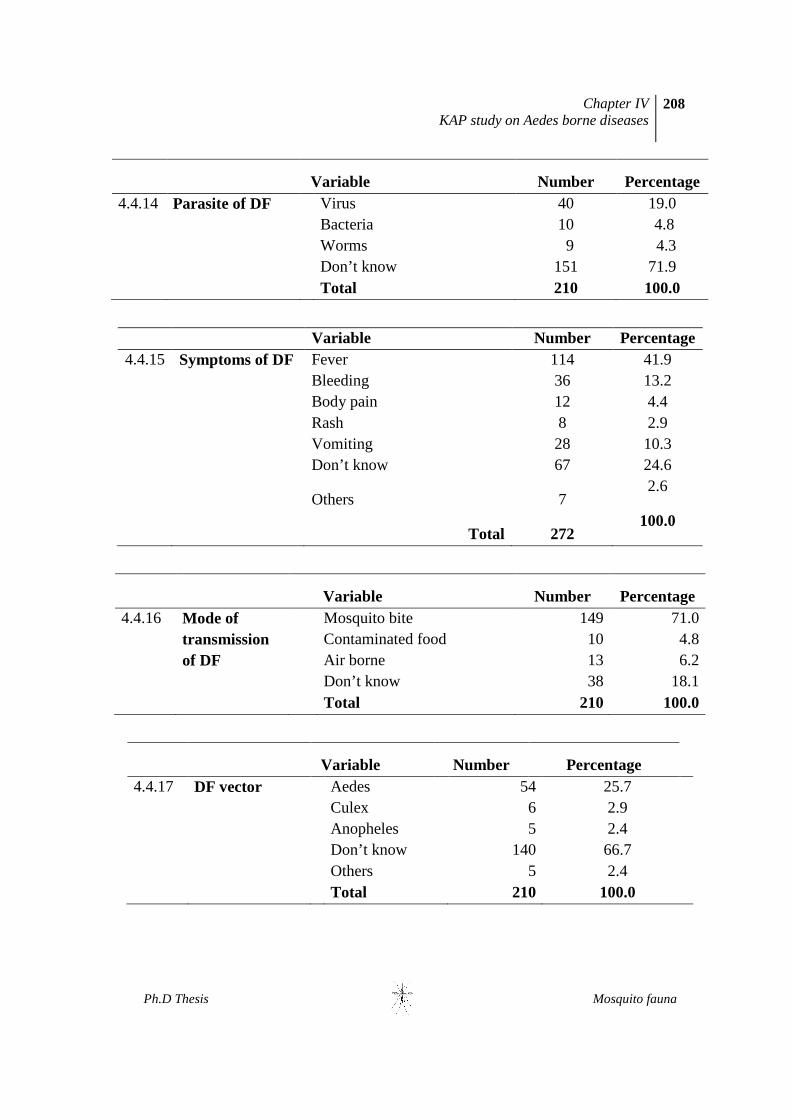
Over 10 % of respondents were unaware of a disease called DF. Similarly the
majority (71%) were unaware of the causative agent of the disease. Fever was
reported as the major symptom. Bleeding, vomiting, body pain, rash etc were the
other symptoms reported in the order. The majority (81%) considered mosquito as
the vector. However, only 25.7% knew that Aedes was the mosquito that spread
the disease. The majority of respondents considered dengue as the prime cause of
death.
Table 4.4 Knowledge of respondents about Dengue Fever
Variable Number Percentage 4.4.13 Awareness of
DF Yes
188 89.5
No 22 10.5 Total 210 100.0
Chapter IV KAP study on Aedes borne diseases
208
Ph.D Thesis Mosquito fauna
Variable Number Percentage
4.4.14 Parasite of DF Virus 40 19.0 Bacteria 10 4.8 Worms 9 4.3 Don’t know 151 71.9 Total 210 100.0
Variable Number Percentage 4.4.15 Symptoms of DF
Fever 114 41.9
Bleeding 36 13.2 Body pain 12 4.4 Rash 8 2.9 Vomiting 28 10.3 Don’t know 67 24.6
Others 7 2.6
Total 272
100.0
Variable Number Percentage
4.4.16 Mode of transmission of DF
Mosquito bite 149 71.0 Contaminated food 10 4.8 Air borne 13 6.2 Don’t know 38 18.1 Total 210 100.0
Variable Number Percentage
4.4.17 DF vector Aedes 54 25.7 Culex 6 2.9 Anopheles 5 2.4 Don’t know 140 66.7 Others 5 2.4 Total 210 100.0
Chapter IV KAP study on Aedes borne diseases
209
Ph.D Thesis Mosquito fauna
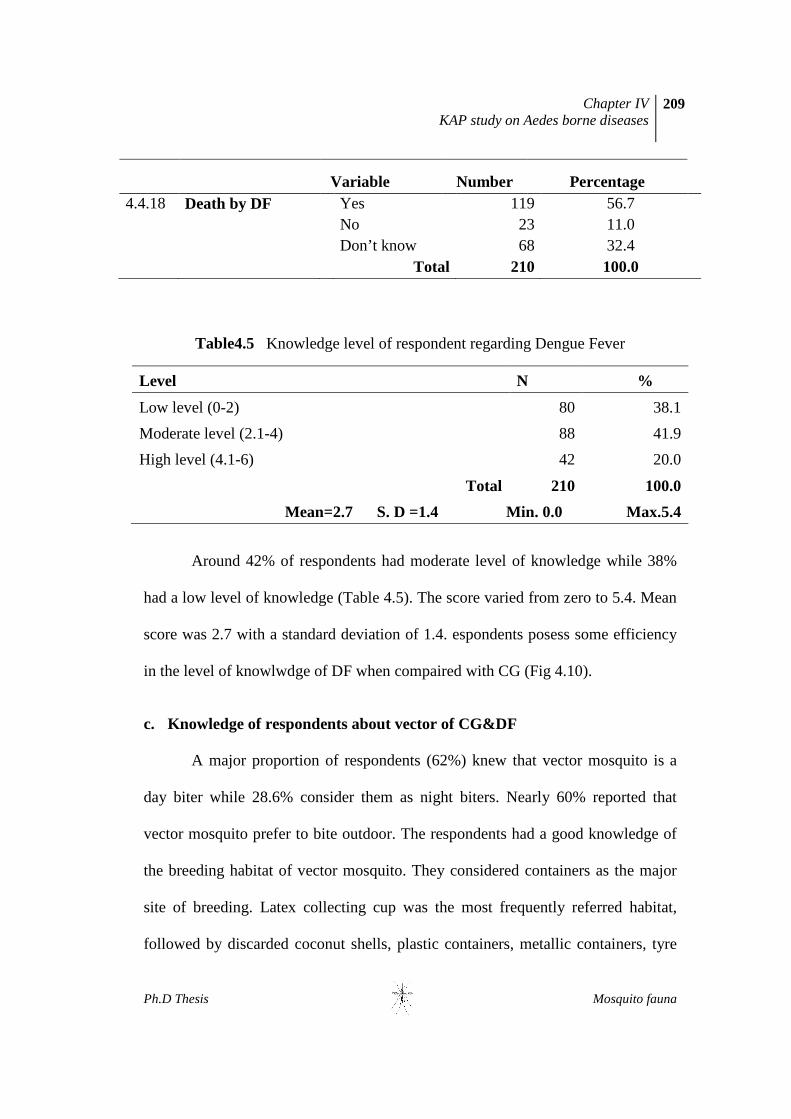
Variable Number Percentage
4.4.18 Death by DF Yes 119 56.7 No 23 11.0 Don’t know 68 32.4 Total 210 100.0
Table4.5 Knowledge level of respondent regarding Dengue Fever
Level N %
Low level (0-2) 80 38.1
Moderate level (2.1-4) 88 41.9
High level (4.1-6) 42 20.0
Total 210 100.0
Mean=2.7 S. D =1.4 Min. 0.0 Max.5.4
Around 42% of respondents had moderate level of knowledge while 38%
had a low level of knowledge (Table 4.5). The score varied from zero to 5.4. Mean
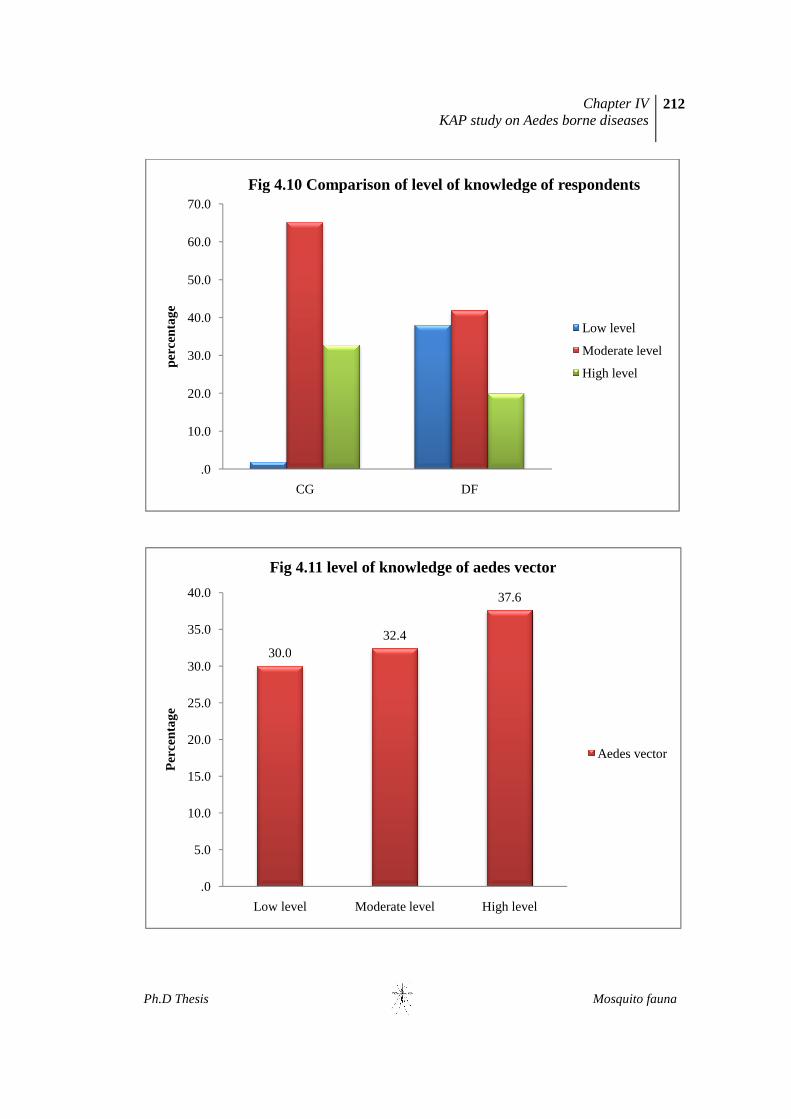
score was 2.7 with a standard deviation of 1.4. espondents posess some efficiency
in the level of knowlwdge of DF when compaired with CG (Fig 4.10).
c. Knowledge of respondents about vector of CG&DF
A major proportion of respondents (62%) knew that vector mosquito is a
day biter while 28.6% consider them as night biters. Nearly 60% reported that
vector mosquito prefer to bite outdoor. The respondents had a good knowledge of
the breeding habitat of vector mosquito. They considered containers as the major
site of breeding. Latex collecting cup was the most frequently referred habitat,
followed by discarded coconut shells, plastic containers, metallic containers, tyre

Chapter IV KAP study on Aedes borne diseases
210
Ph.D Thesis Mosquito fauna
etc. Nearly 10% responses favoured plant axils as the potential breeding site.
More than half of the respondents could identify the vector mosquito from the
mosquito sample shown to them. Details of the response of the people regarding
vector mosquito are given in the table 4.6
Table 4.6 Knowledge of respondents about vector of CG&DF
Variable Number Percentage
4.6.19 Mosquito biting time Day time 131 62.4 Night time 60 28.6 Any time 19 9.0 Total 210 100.0
Variable Number Percentage
4.6.20 Preference for feeding
Out door 124 59.0 Indoor 66 31.4 Indoor and out door 20 9.5 Total 210 100.0
Variable Number* Percentage 4.6.21 Aedes breeding site Latex collecting cups 186 35.5 Coconut shell 102 19.5
Drains/canals 42 8.0
Plastic/metallic container 56 10.7
Safety tank 44 8.4
Plant axils/tree hole 20 3.8
Tyre 32 6.1
Cattle shed 41 7.8
Others 1 0.2
Total 524 100.0

Chapter IV KAP study on Aedes borne diseases
211
Ph.D Thesis Mosquito fauna
Variable Number Percentage
4.6.22 Ability to identify
the Aedes mosquito
Identified 119 56.7
Not identified 91 43.3
Total 210 100.0
Table 4.7 Knowledge Level of respondents regarding Vector mosquito
Level Number %
Low level (0-1.3) 63 30.0
Moderate level (1.4-2.6) 68 32.4
High level (2.7-4) 79 37.6
Total 210 100.0
Mean=2.15 S. D =1.2 Min. 0.0 Max.3.8
As per the table above (4.7), 37.6 % had a high level of knowledge while
32.4 had a moderate level. The mean score of respondents regarding vector was
2.15 with a standard deviation of 1.2. the minimum score found to be zero and the
maximum was 3.8 (Fig 4.11).
Ph.D Thesis
.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
perc
enta
ge
Fig 4.10 Comparison of level of knowledge of respondents
30.0
.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Low level
Per
cent
age
Fig 4.11 level of knowledge of aedes vector
KAP study on Aedes borne diseases
CG DF
Fig 4.10 Comparison of level of knowledge of respondents
30.032.4
37.6
Low level Moderate level High level
Fig 4.11 level of knowledge of aedes vector
Chapter IV KAP study on Aedes borne diseases
212
Mosquito fauna
Fig 4.10 Comparison of level of knowledge of respondents
Low level
Moderate level
High level
Aedes vector
Chapter IV KAP study on Aedes borne diseases
213
Ph.D Thesis Mosquito fauna
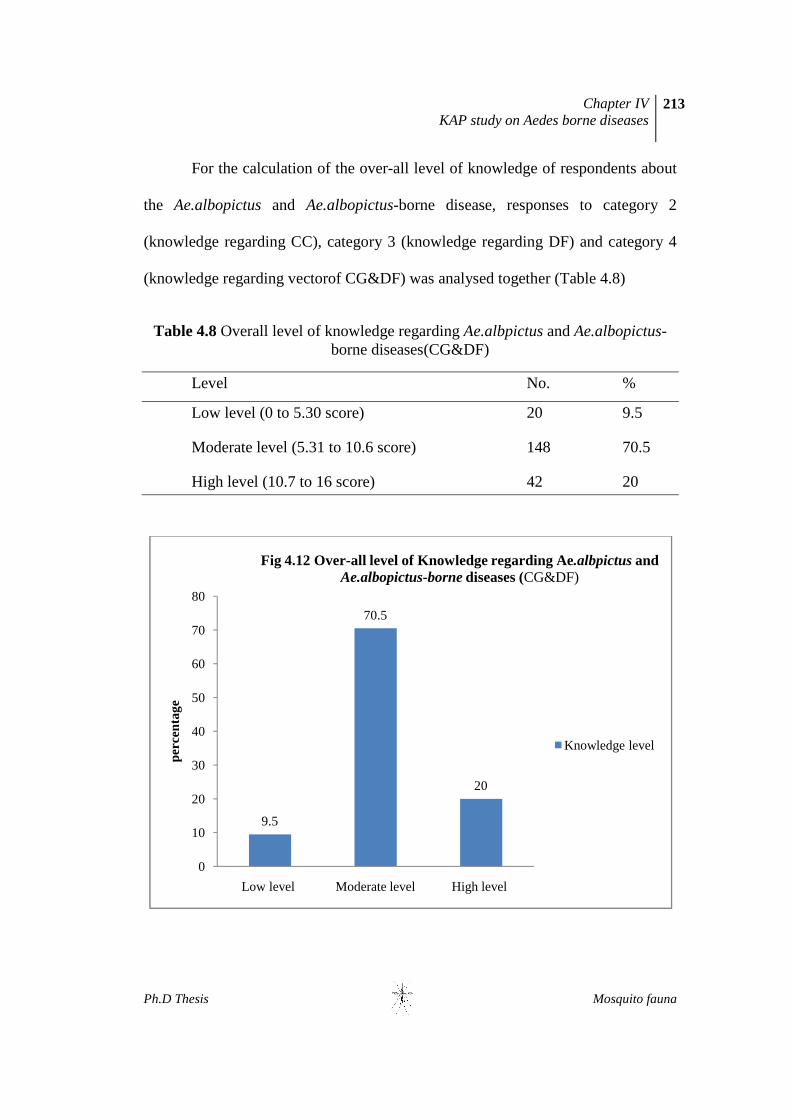
For the calculation of the over-all level of knowledge of respondents about
the Ae.albopictus and Ae.albopictus-borne disease, responses to category 2
(knowledge regarding CC), category 3 (knowledge regarding DF) and category 4
(knowledge regarding vectorof CG&DF) was analysed together (Table 4.8)
Table 4.8 Overall level of knowledge regarding Ae.albpictus and Ae.albopictus-borne diseases(CG&DF)
Level No. %
Low level (0 to 5.30 score) 20 9.5
Moderate level (5.31 to 10.6 score) 148 70.5
High level (10.7 to 16 score) 42 20
9.5
70.5
20
0
10
20
30
40
50
60
70
80
Low level Moderate level High level
perc
enta
ge
Fig 4.12 Over-all level of Knowledge regarding Ae.albpictus and Ae.albopictus-borne diseases (CG&DF)
Knowledge level

Chapter IV KAP study on Aedes borne diseases
214
Ph.D Thesis Mosquito fauna
Less than 10% of respondents had a low level of knowledge as per the
given criteria while over 70% had a moderate level and 20% had a higher level of
knowledge (Fig 4.12)
4.4.3 Over-all Level of Attitude and Practice of respondents
a. Personal protective practices
In the questionnaire, there were two questions related to personal protective
practices against mosquito bite. The table 4.9 gives a clear picture of preventive
practices adopted by the respondents of the study area. Everybody practised one or
more types of preventive measures. Many of these practices were used at night and
indoor situations so they were not suitable against Aedes. Use of fan was the most
frequently referred choice for protection from mosquito bite, followed by mosquito
repellents, closing the doors and windows of houses etc. Some considered that
proper clothing and mosquito creams applied on body would protect against
mosquito bite. The period for which preventive measures were adopted varied. The
majority (46.6%) of the respondents were cautious during outbreak season while
30.5% followed preventive practices throughout the year.
Table 4.9 Personal protective practices
Variable Number* Percentage 4.9.23 Protection from
mosquito bite Mosquito net 49 8.2
Coil/mat/liquid 118 19.8
Proper clothing 8 1.3
Mosquito proof house 5 0.8
Fan 147 24.6

Chapter IV KAP study on Aedes borne diseases
215
Ph.D Thesis Mosquito fauna
Body cream 23 3.9
Close door 117 19.6
Bat 59 9.9
Smoking 68 11.4
Others 3 0.5
Total 597 100.0
Variable Number Percentage
4.9.24 Timing of
preventive
measures
Rainy/biting season 42 20.0
Disease outbreak season 100 46.6
Throughout the year 64 30.5
Others 4 1.9
Total 210 100.0
Table 4.10 Level of personal protective practice against mosquito bite
Level No. %
Poor practice (0) 127 60.5
Fair practice (1) 71 33.8
Healthy practice (2) 12 5.7
Total 210 100.0
Mean =0.45 S.D=1.1 Min =0.0 Max 2
Around 60% of respondents followed a poor practice against Aedes bite
whereas 33.8 followed fair practices. Only 5.7 knew the correct preventive
measures against Aedes bite. The mean score for personal preventive practice was
found to be 0.45 with a standard deviation of 1.1. The minimum score was zero
and maximum score was 2.(Table 4.10)

Chapter IV KAP study on Aedes borne diseases
216
Ph.D Thesis Mosquito fauna
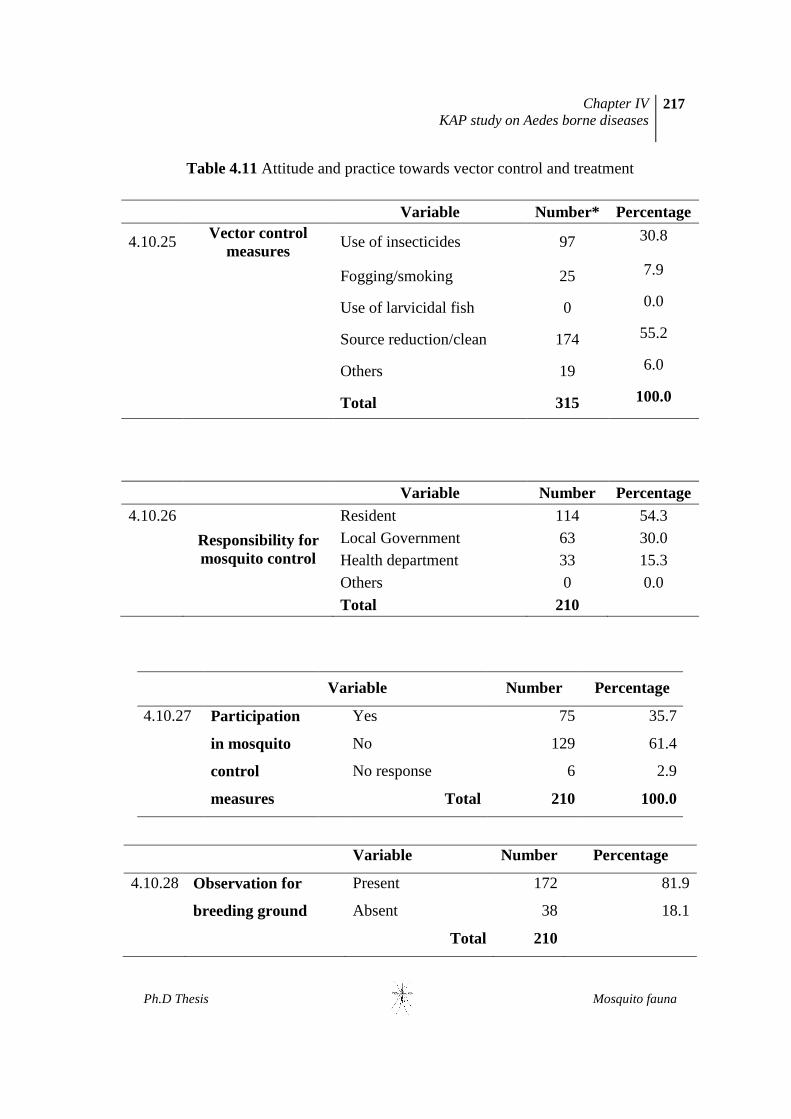
b. Vector control and treatment.
Vector control is the most important methods for preventing vector
borne diseases. Positive attitude and good practice of people are crucial in its
success. To understand the attitude and practice of respondents towards
mosquito control measures, four questions were included in this section. A fifth
question related to treatment practice was also included. The responses of
people towards various questions are summarized in the table 4.11. Over 30 %
believed in application of chemicals against adults as the best method. Over 55
% of the respondents knew that source reduction is the best method for
mosquito control. While 54% believed that mosquito control is the primary duty
of the resident himself, 45% deemed it as the duty of local governments and
health department. Though many people knew that mosquito control is the duty
of residents, their involvement is less. Only 35% of respondents gave a positive
response to a question regarding involvement/ participation in control
measures. About 82% of houses were positive for mosquito larval habitat.
Atleast one container with larvae was noted in those houses. The majority of
respondents visited hospital in the event of a disease.
Chapter IV KAP study on Aedes borne diseases
217
Ph.D Thesis Mosquito fauna
Table 4.11 Attitude and practice towards vector control and treatment
Variable Number* Percentage
4.10.25 Vector control measures
Use of insecticides 97 30.8
Fogging/smoking 25 7.9
Use of larvicidal fish 0 0.0
Source reduction/clean 174 55.2
Others 19 6.0
Total 315 100.0
Variable Number Percentage 4.10.26
Responsibility for mosquito control
Resident 114 54.3
Local Government 63 30.0 Health department 33 15.3
Others 0 0.0 Total 210
Variable Number Percentage
4.10.27 Participation
in mosquito
control
measures
Yes 75 35.7
No 129 61.4
No response 6 2.9
Total 210 100.0
Variable Number Percentage
4.10.28 Observation for
breeding ground
Present 172 81.9
Absent 38 18.1
Total 210
Chapter IV KAP study on Aedes borne diseases
218
Ph.D Thesis Mosquito fauna
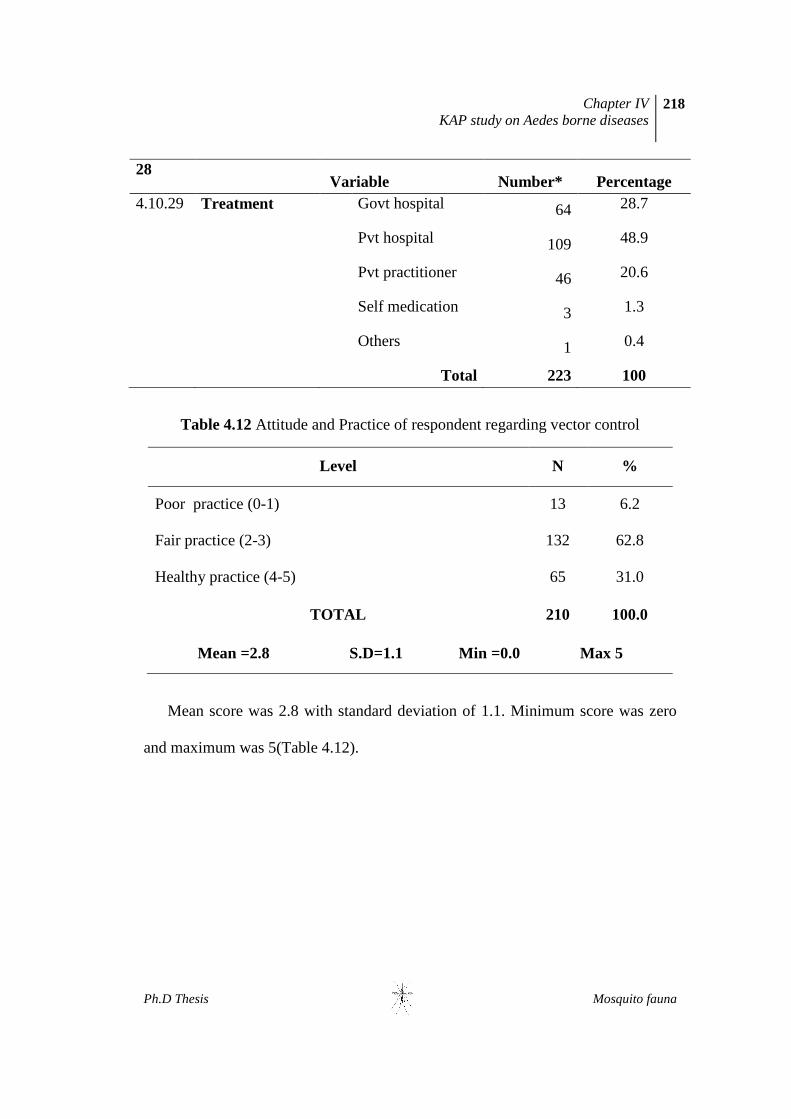
28 Variable Number* Percentage
4.10.29 Treatment Govt hospital 64 28.7
Pvt hospital 109 48.9
Pvt practitioner 46 20.6
Self medication 3 1.3
Others 1 0.4
Total 223 100
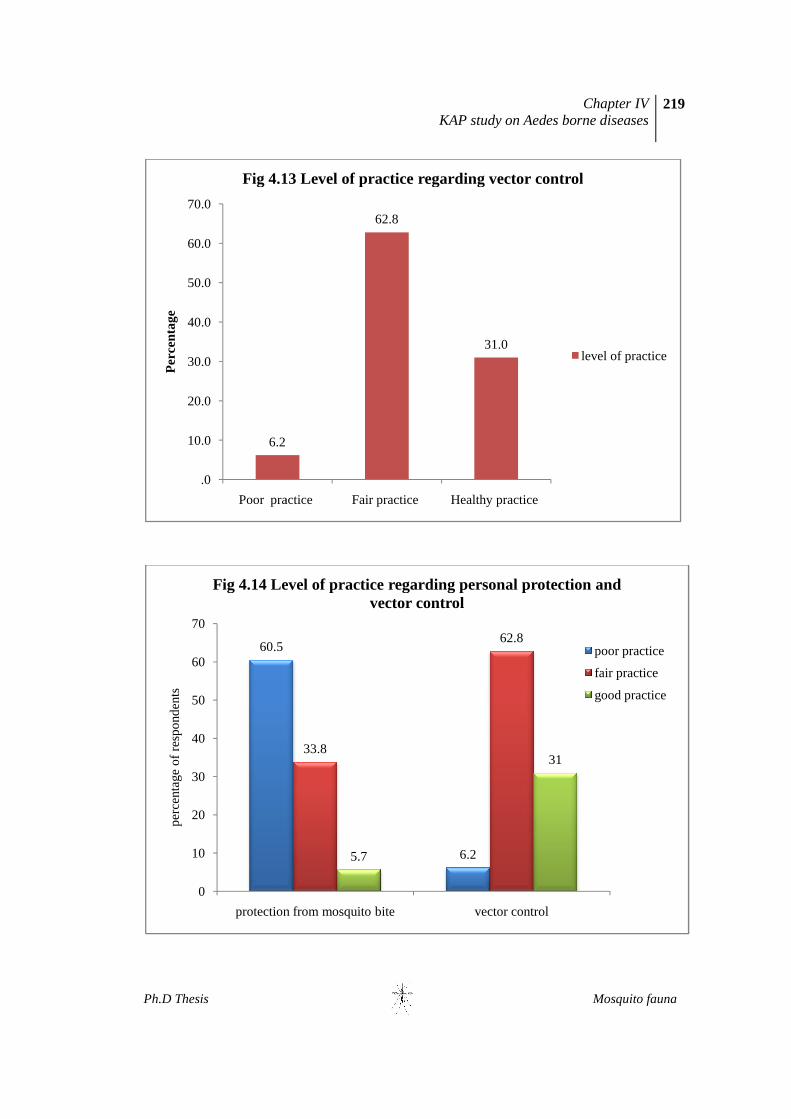
Table 4.12 Attitude and Practice of respondent regarding vector control
Level N %
Poor practice (0-1) 13 6.2
Fair practice (2-3) 132 62.8
Healthy practice (4-5) 65 31.0
TOTAL 210 100.0
Mean =2.8 S.D=1.1 Min =0.0 Max 5
Mean score was 2.8 with standard deviation of 1.1. Minimum score was zero
and maximum was 5(Table 4.12).
Ph.D Thesis
6.2
.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Poor practice
Per
cent
age
Fig 4.13 Level of practice regarding vector control
60.5
0
10
20
30
40
50
60
70
protection from mosquito bite
per
cent
age
of r
esp
ond
ents
Fig 4.14 Level of practice regarding personal protection and
KAP study on Aedes borne diseases
62.8
31.0
Poor practice Fair practice Healthy practice
Fig 4.13 Level of practice regarding vector control
6.2
33.8
62.8
5.7
31
protection from mosquito bite vector control
Fig 4.14 Level of practice regarding personal protection and vector control
Chapter IV KAP study on Aedes borne diseases
219
Mosquito fauna
Fig 4.13 Level of practice regarding vector control
level of practice
Fig 4.14 Level of practice regarding personal protection and
poor practice
fair practice
good practice

Chapter IV KAP study on Aedes borne diseases
220
Ph.D Thesis Mosquito fauna
60% of respondents adopted poor practice in taking preventive
measures aginst Aedes biting while only 5.7% adopted healthy
practice (Fig 4.14). 62.8% had a fair practice regarding vector
control while 31% showed good practice.(Fig 4.13).
Table 4.13. Over-all level of attitude and practice regarding disease prevention and
control
Over-all Level of Attitude and Practice No . %
Poor (upto33.33%) - 70 33
Fair (between l33.33% & 66.66%) - 121 57
Healthy (above 66.66%) - 19 09
Only 9% of respondents showed healthy attitude and practice towards disease
prevention and control while 33% showed poor attitude and practice (Table 4.13).
4.4.4. Incidence of disease.
Of the 210 respondent, 75 had a previous history CG and 4 had a history of DF.
Dual infection was not reported. Following table (4.14) gives more details.
Table 4.14. Incidence of disease among the respondents
Variable Number Percentage
4.12.30 Any incidence of Dengue
Fever/CG
DF 4 1.9
CG 75 35.7
Neither 131 62.4
Total 210 100.0

Chapter IV KAP study on Aedes borne diseases
221
Ph.D Thesis Mosquito fauna
Though 62% were not inflicted with any disease , 36% had a real
experience of Chikungunya and 2% were infected with Dengue virus (Fig. 4.15)
4.4.5. Association between Socio-economic-demographic profile and Over-all
Level of Knowledge
Association between various socio-economic-demographic parameters with
over-all level of knowledge regarding Ae.albopictus and Ae.albopictus-borne
diseases(CG&DF) was analysed using the SPSS software.
DF2%
CG36%
Neither62%
Fig. 4.15 Incidence of diseases in study population
Chapter IV KAP study on Aedes borne diseases
222
Ph.D Thesis Mosquito fauna
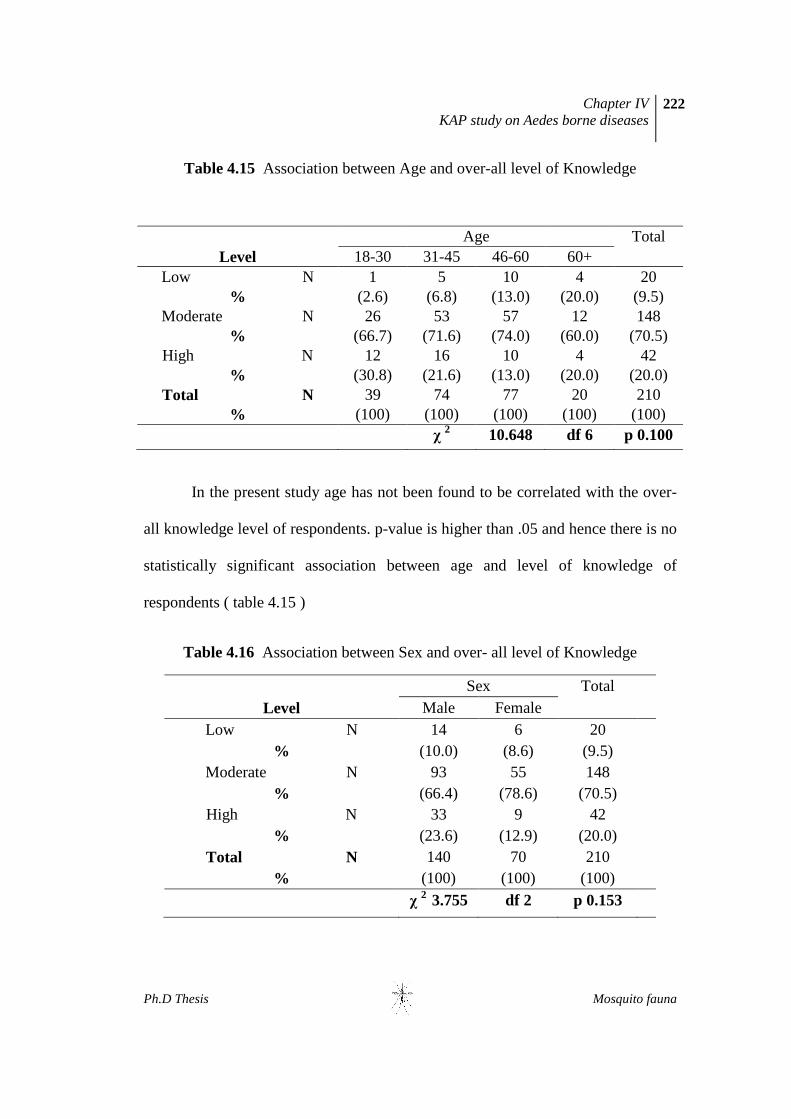
Table 4.15 Association between Age and over-all level of Knowledge
Age Total Level 18-30 31-45 46-60 60+
Low N 1 5 10 4 20
% (2.6) (6.8) (13.0) (20.0) (9.5) Moderate N 26 53 57 12 148
% (66.7) (71.6) (74.0) (60.0) (70.5) High N 12 16 10 4 42
% (30.8) (21.6) (13.0) (20.0) (20.0) Total N 39 74 77 20 210
% (100) (100) (100) (100) (100)
χ 2 10.648 df 6 p 0.100
In the present study age has not been found to be correlated with the over-
all knowledge level of respondents. p-value is higher than .05 and hence there is no
statistically significant association between age and level of knowledge of
respondents ( table 4.15 )
Table 4.16 Association between Sex and over- all level of Knowledge
Sex Total
Level Male Female
Low N 14 6 20
% (10.0) (8.6) (9.5)
Moderate N 93 55 148
% (66.4) (78.6) (70.5)
High N 33 9 42
% (23.6) (12.9) (20.0)
Total N 140 70 210
% (100) (100) (100)
χ 2 3.755 df 2 p 0.153
Chapter IV KAP study on Aedes borne diseases
223
Ph.D Thesis Mosquito fauna
Among the male respondents 66.4% had a moderate level of knowledge
while 23.6% had a high level of knowledge and 10% had a low level of
knowledge. 78.6 % of female respondents had a moderate level of knowledge
while 12.9% had a high level of knowledge (Table 4.16). There was no association
between the level of knowledge and gender of the respondents. Statistical analysis
shows that there is no significant association between sex and level of knowledge.
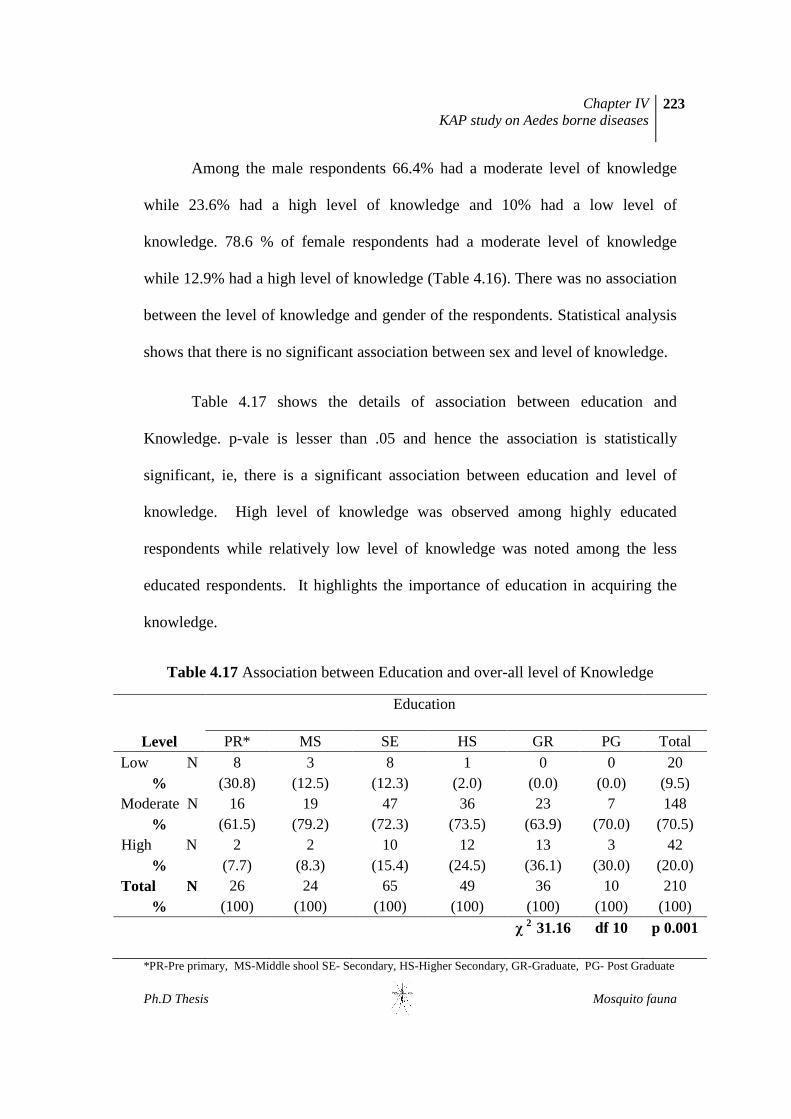
Table 4.17 shows the details of association between education and
Knowledge. p-vale is lesser than .05 and hence the association is statistically
significant, ie, there is a significant association between education and level of
knowledge. High level of knowledge was observed among highly educated
respondents while relatively low level of knowledge was noted among the less
educated respondents. It highlights the importance of education in acquiring the
knowledge.
Table 4.17 Association between Education and over-all level of Knowledge
Education
Level PR* MS SE HS GR PG Total
Low N 8 3 8 1 0 0 20 % (30.8) (12.5) (12.3) (2.0) (0.0) (0.0) (9.5)
Moderate N 16 19 47 36 23 7 148 % (61.5) (79.2) (72.3) (73.5) (63.9) (70.0) (70.5)
High N 2 2 10 12 13 3 42 % (7.7) (8.3) (15.4) (24.5) (36.1) (30.0) (20.0)
Total N 26 24 65 49 36 10 210 % (100) (100) (100) (100) (100) (100) (100)
χ 2 31.16 df 10 p 0.001
*PR-Pre primary, MS-Middle shool SE- Secondary, HS-Higher Secondary, GR-Graduate, PG- Post Graduate

Chapter IV KAP study on Aedes borne diseases
224
Ph.D Thesis Mosquito fauna
Table 4.18 Association between Occupation and over-all-level of Knowledge
Occupation
Level BU* GO PV PL DW HH ST RT SE OT Low N
0 0 1 6 7 3 0 0 1 2
% (0.0) (0.0) (10.0) (12.2) (29.2) (7.1) (0.0) (0.0) (7.1) (6.3) Moderate
N 11 9 4 32 15 34 7 1 9 26
% (84.6) (60.0) (40.0) (65.3) (62.5) (81.0) (70.0) (100) (64.3) (81.3) High
N 2 6 5 11 2 5 3 0 4 4
% (15.4) (40.0) (50.0) (22.4) (8.3) (11.9) (30.0) (0.0) (28.6) (12.5) Total N 13 15 10 49 24 42 10 1 14 32
% (100) (100) (100) (100) (100) (100) (100) (100) (100) (100)
χ 2 31.127 df 18 p0.028
*BU-business,GO-govt employ,PV-Private employee, PL-Plantation, DW-Daily wager.HH-house wife, ST-students,RT-Retired, SE-Self employed,OT-Others.
Here the p-value is less than 0.05 and hence there is a significant relation
between occupation and level of knowledge (4.18).
Table 4.19 Association between Financial background and over-all-level of
Knowledge
Finance Total
Level APL BPL
Low N 9 11 20
% (5.9) (19.0) (9.5)
Moderate N 105 43 148
% (69.1) (74.1) (70.5)
High N 38 4 42
% (25.0) (6.9) (20.0)
Total N 152 58 210
% (100) (100) (100)
χ 2 14.532 df 2 p 0.001
Chapter IV KAP study on Aedes borne diseases
225
Ph.D Thesis Mosquito fauna
Among the respondents of BPL category only 6.95 had high level of knowledge
while 74.1 % had moderate and 19% had low level of knowledge. Among the
respondents belonging to APL category 25% had high level of knowledge while
69.1 % had moderate level and 5.9% had low level of knowledge (Table 4.19). As
shown in the table there is a significant association between the financial
background and the level of knowledge. Respondents of APL category had a better
knowledge level.
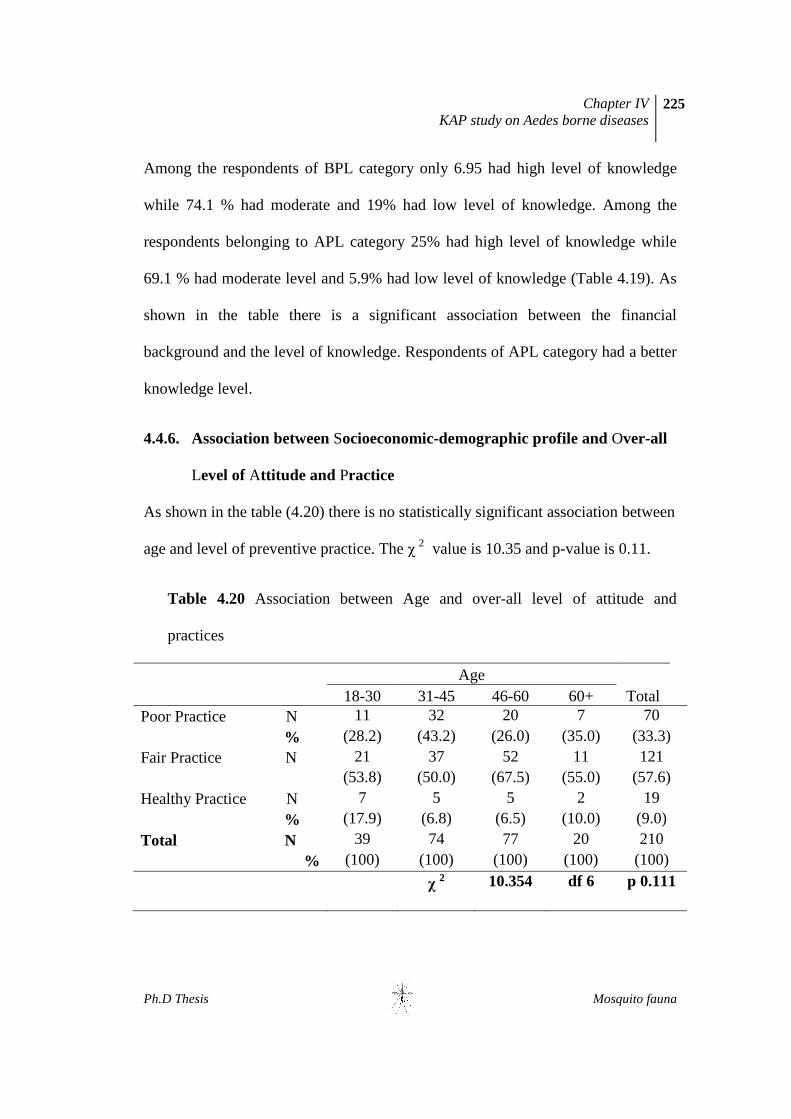
4.4.6. Association between Socioeconomic-demographic profile and Over-all
Level of Attitude and Practice
As shown in the table (4.20) there is no statistically significant association between
age and level of preventive practice. The χ 2 value is 10.35 and p-value is 0.11.
Table 4.20 Association between Age and over-all level of attitude and
practices
Age Total 18-30 31-45 46-60 60+
Poor Practice N 11 32 20 7 70 % (28.2) (43.2) (26.0) (35.0) (33.3) Fair Practice N 21 37 52 11 121
(53.8) (50.0) (67.5) (55.0) (57.6) Healthy Practice N 7 5 5 2 19 % (17.9) (6.8) (6.5) (10.0) (9.0) Total N 39 74 77 20 210
% (100) (100) (100) (100) (100)
χ 2 10.354 df 6 p 0.111

Chapter IV KAP study on Aedes borne diseases
226
Ph.D Thesis Mosquito fauna
Table 4.21 Association between Sex and over-all level of attitude and practices
Sex Male Female Total Poor Practice N 42 28 70 % (30.0) (40.0) (33.3) Fair Practice N 85 36 121 % (60.7) (51.4) (57.6) Healthy Practice N 13 6 19 % (9.3) (8.6) (9.0) Total N 140 70 210
% (100) (100) (100)
χ 2 2.125 df 2 p 0.346
As shown in the table (4.21) male respondents had a better practice than
females. However no statistically significant association between sex and level of
preventive practice was observed.
Table 4.22 Association between Education and over-all level of attitude and
practices
Education Total P M P S HS G PG Poor Practice N 11 6 27 22 4 0 70
% (42.3) (25.0) (41.5) (44.9) (11.1) (0.0) (33.3)
Fair Practice N 15 16 33 21 28 8 121 (57.7) (66.7) (50.8) (42.9) (77.8) (80.0) (57.6)
Healthy Practice 0 2 5 6 4 2 19
% (0.0) (8.3) (7.7) (12.2) (11.1) (20.0) (9.0)
Total N 26 24 65 49 36 10 210
% (100) (100) (100) (100) (100) (100) (100)
χ 2 23.752 df 10 p 0.008 *PR-Pre primary, MS-Middle shool SE- Secondary, HS-Higher Secondary, GR-Graduate, PG- Post Graduate

Chapter IV KAP study on Aedes borne diseases
227
Ph.D Thesis Mosquito fauna
As shown in the table (4.22) there is a significant association between
education and level of preventive practice. Appropriate practice was observed
among well educated (HS,G, PG) respondents.
Table 4.23 Association between Occupation and over-all level of attitude and
practice
Occupation
BU GO PV PL DW HH ST RT SE OT
Poor Practice N 6 3 1 19 10 17 4 1 0 9
% (46.2) (20.0) (10.0) (38.8) (41.7) (40.5) (40.0) (100) (0.0) (28.1)
Fair Practice N 6 10 7 27 14 23 3 0 12 19
(46.2) (66.7) (70.0) (55.1) (58.3) (54.8) (30.0) (.0) (85.7) (59.4)
Healthy Practice N 1 2 2 3 0 2 3 0 2 4
% (7.7) (13.3) (20.0) (6.1) (.0) (4.8) (30.0) (.0) (14.3) (12.5)
Total N 13 15 10 49 24 42 10 1 14 32
% (100) (100) (100) (100) (100) (100) (100) (100) (100) (100)
χ
2 26.7 df 18 p
0.085
*BU-business,GO-govt employ,PV-Private employee, PL-Plantation, DW-Daily wager.HH-house wife, ST-students,RT-Retired, SE-Self employed,OT-Others.
No significant association was observed between occupation and level of
preventive practice (Table 4.23).

Chapter IV KAP study on Aedes borne diseases
228
Ph.D Thesis Mosquito fauna
Table 4.24 Association between Financial background and over-all level of
attitude and practice
Finance Total
APL BPL Poor Practice N 49 21 70 % (32.2) (36.2) (33.3) Fair Practice N 87 34 121 % (57.2) (58.6) (57.6) Healthy Practice N 16 3 19 % (10.5) (5.2) (9.0) Total N 152 58 210
% (100) (100) (100) χ 2 1.542 df 2 p 0.462
As shown in the table (Table 4.24) there is no significant association
between financial background and level of preventive practice. Of the total APL
respondents 32.2% had poor preventive practices, 57.2% had fair practice while
10.5 % had healthy practices. Majority of BPL respondents (58.6%) had fair
preventive practices.
4.4.7. Association between over-all level of Knowledge and over-all level of
attitude and practice
As per the table (Table 4.25) there is no association between the over-all level of
Knowledge and the over-all level of attitude and practice. There is no significant
increase in practicing the preventive measures with corresponding increase in
knowledge.

Chapter IV KAP study on Aedes borne diseases
229
Ph.D Thesis Mosquito fauna
Table 4.25 Association between over-all level of Knowledge and over-all level of
attitude and practice
Level of attitude and practice
Total Level of Knowledge Poor Fair Healthy
Low N 6 13 1 20
% (8.60) (10.70) (5.30) (9.50)
Moderate N 48 85 15 148
% (68.60) (70.20) (78.90) (70.50)
High N 16 23 3 42
% (22.90) (19.00) (15.80) (20.00)
Total N 70 121 19 210
% (100) (100) (100) (100)
χ 2 1.362 df 4 p 0.851
Table 4.26 Association between participation in vector control activity and
observation of larval habitat
Observation of
Breeding Habitat
Participation Yes No Total
No
N 126 9 135
% (73.30) (24.30) (64.60)
Yes
N 46 28 74
% (26.70) (75.70) (35.40)
Total N 172 37 209
% (100) (100) (100)
χ 2 31.878 df 1 p 0.001
Chapter IV KAP study on Aedes borne diseases
230
Ph.D Thesis Mosquito fauna
Further analysis showed that participation in source reduction measures
significantly reduces the number of houses positive for larval breeding. As shown
in the table 4.26 there is a highly significant association between source reduction
practice and the occurrence of larval habitat. At the same time many breeding
habitat were observed around the houses of many respondents,where residence
reported source reduction practices.
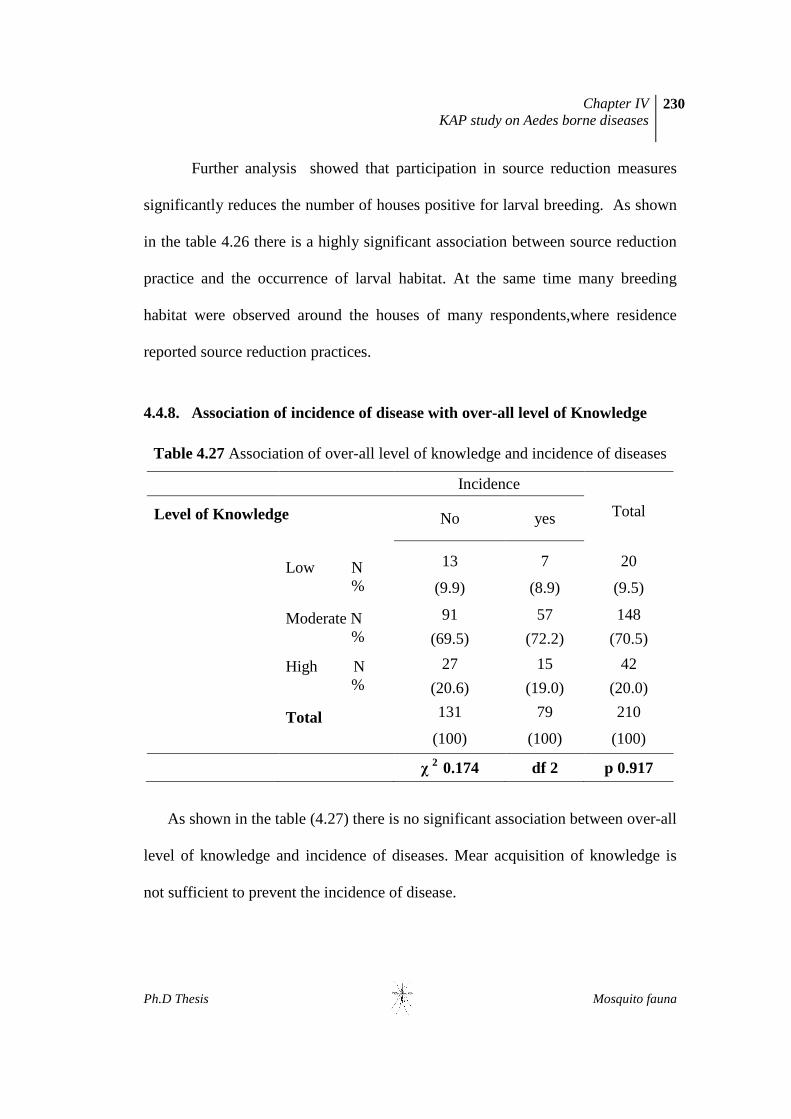
4.4.8. Association of incidence of disease with over-all level of Knowledge
Table 4.27 Association of over-all level of knowledge and incidence of diseases
Incidence
Total Level of Knowledge
No yes
Low N %
13 7 20
(9.9) (8.9) (9.5)
Moderate N %
91 57 148
(69.5) (72.2) (70.5)
High N %
27 15 42
(20.6) (19.0) (20.0)
Total
131 79 210
(100) (100) (100)
χ 2 0.174 df 2 p 0.917
As shown in the table (4.27) there is no significant association between over-all
level of knowledge and incidence of diseases. Mear acquisition of knowledge is
not sufficient to prevent the incidence of disease.

Chapter IV KAP study on Aedes borne diseases
231
Ph.D Thesis Mosquito fauna
4.4.9 Association of incidence of disease with over-all level of attitude and
practice
Table 4.28 Association of the over-all level of attitude and practices with incidence of disease
Incidence of diseases Total
No Yes
Poor Practice N 49 21 70
% (37.4) (26.6) (33.3)
Fair Practice N 74 47 121
% (56.5) (59.5) (57.6)
Healthy Practice N 8 11 19
% (6.1) (13.9) (9.0)
Total N 131 79 210
% (100) (100) (100)
χ 2 5.137 df 2 p 0.077
In the present study no significant association between the preventive
measures and incidence was observed (Table 4.28).

Chapter IV KAP study on Aedes borne diseases
232
Ph.D Thesis Mosquito fauna
4.5 DISCUSSION AND CONCLUSION
Many of the previous studies measured the knowledge of vector-borne
diseases in various ways. Some studies determined the knowledge of disease from
the knowledge of the disease alone (Tram et al., 2003; Van et al., 2002), whereas
others included knowledge of the vector and control measure (Rosenbaum et al.,
1995; Lloyd et al., 1992). In the present study both these aspects were included.
Statistical analysis of collected data showed the Knowledge, Attitude and Practice
of respondents regarding various aspects of Aedes albopictus and Aedes albopictus
- borne diseases. Major findings are discussed under the following titles.
4.5.1 Socio-economic-demographic profile of the respondents
Present study showed that people of the study area live in a better
socioeconomic condition (Table 4.1). All the respondents were literate and
majority were well-educated(Fig 4.6). Majority of the respondents of the study area
were financially sound (Fig 4.8). Though agriculture/plantation was the traditional
occupation of the area educated young respondent were found to be attracted to
other occupations. The eldest male member is the head of the family in most of the
households. The household leader has a key role in vector control and disease
prevention. So household leaders be a target group for awareness campaigns.
Various media were available in each household. TV, News papers and Radio were
the major source of information (Fig 4.9).
Chapter IV KAP study on Aedes borne diseases
233
Ph.D Thesis Mosquito fauna
4.5.2 Over-all Level of Knowledge
Knowledge of a disease is very essential for its control. The present study
showed that respondents had a better level of knowledge regarding many aspects
of CG, DF and Aedes mosquito.
Several studies have shown that a higher socio-economic status correlates
with better knowledge scores (Kubik et al., 2004; McArthur et al., 2001; Potvin et
al, 2000). Our study also highlighted this conclusion. Every respondent of the
survey was aware of a disease called CG while 89.5% were aware of DF. 98% of
respondents knew that CG was transmitted by infected mosquito bite, 71% knew
the mode of transmission of DF. The respondent of the study had good knowledge
regarding symptoms of CG and DF (Table 4.2, Table 4.4). Respondents had a good
knowledge level regarding CG and DF (Fig 4.10). Knowledge level of respondents
regarding CG was found to be higher than that of Dengue Fever(Table 4.3 and
4.5). The relatively high level of knowledge regarding CG might be due to the
recent outbreak of CG and subsequent reports on various media.
The responses showed that the awareness regarding Aedes was not bad.
The analysis of data indicated that respondent had a good knowledge regarding
breeding ground of Aedes. Majority of the respondent knew that water holding
containers such as latex collecting cups, discarded coconut shells etc were the
dominant breeding sites. However breeding sites such as tree holes and tyres were
rarely referred (Table 4.6). Lack of knowledge of specific breeding habitat
appeared to be a deterrent to the elimination of that source. Respondents were

Chapter IV KAP study on Aedes borne diseases
234
Ph.D Thesis Mosquito fauna
almost equally distributed among the three knowledge levels, 37 % had a high
level of knowledge regarding the vector while 32% had moderate level and 30%
had low level of knowledge (Table 4.7).
Over-all knowledge level of respondents regarding Ae.albopictus and
Aedes-borne disease was good. More than 70% of respondents had moderate
knowledge and 20% had high level of knowledge. Only less than 10% had low
level of knowledge (Table 4.8 )
Even though many respondents were aware of many characteristics of
diseases and vector, several misconceptions were identified. One area that
respondent lacked knowledge was that CG causes death. While 50.5 % thought
that CG causes death 11 % thought that DF wouldn’t cause death (table 4.3, table
4.4). Other areas that lacked knowledge were regarding parasites and type of
mosquito responsible for CG and DF. Around 38% give wrong response to the
question on biting time. Similarly 40% were incorrectly, answered the question on
feeding place (out door/indoor) (Table 4.6). Day biting and outdoor biting are the
two important characteristics of Aedes albopictus. Awareness regarding these two
characteristics are essential to plan a specific measures against its bite. Similarly
ability to identify the vector helps to take protection, specifically. These are the
important areas which need to be emphasised more during the awareness
programme.
Chapter IV KAP study on Aedes borne diseases
235
Ph.D Thesis Mosquito fauna
4.5.3. Over-all Level of Attitude and Practice of respondents
The over-al level of attitude and practice regarding disease prevention and
control was not satisfactory. Only 30% took personal protective measures
throughout the year. This showed that majority of respondents were unaware that
dengue can occur in all seasons. 46% wait until the outbreak for taking a
preventive measure. This behaviour raises the risk of vector-borne diseases.
Similarly analysis showed that preventive measures are not species specific. A
major proportion of the respondents adopted unsuitable personal preventive
measures. Only a small proportion of the participants were conscious in using cloth
which cover major portion of the body when they go out. Preventive measures
preferred were use of mosquito coils/mat/liquid (Table 4.9). Several studies have
reported these methods to be most common means of prevention (Fradin et al,
2002; Jelinck, 2000). Use of fan was also a very popular method for prevention.
Such finding was reported in some earlier studies (Itrat et al., 2008). Other
preventive measures include the use of mosquito net, electric bat and smoke (Table
4.9). But these methods are effective against night/indoor biting mosquitoes. only
5.7% knew the correct personal preventive practice aginst Aedes biting (Tabe
4.10). It is very important to know the biting time of Aedes mosquito to protect
themselves during day time. As per the present study more than 62% knew the
biting time of Aedes but that knowledge was not put into action.
Chapter IV KAP study on Aedes borne diseases
236
Ph.D Thesis Mosquito fauna
Respondents knew that clean surrounding or source reduction is the best
method for controlling the vector density and spread of vector borne
diseases(Table 4.11). However many inappropriate attitude and practice were
observed during the survey. Over 45% of respondents felt that mosquito breeding
source reduction should be the responsibility of local government or health
department (Table 4.11).
A good health seeking behaviour was observed among the respondents.
Half of the respondents visited private hospitals. This may be due to better socio-
economic condition of respondents of the area and availability of numerous private
hospitals.
4.5.4. Incidence of vector-borne disease in the study area (CG&DF)
Ae.albopictus-borne diseases, especially CG have been a serious public health
problem in the study area. 36% of the respondents had a real experience of
Chikungunya and 2% were infected with Dengue virus (Fig. 4.15)
4.5.5. Association between socio-economic-demographic status and Over-all
Level of Knowledge
Many of the previous investigations measured either the knowledge on DF
or on CG. In the present investigation knowledge on both the DF and CG were
measured along with vector characteristics. This approach was useful for
calculating the knowledge on Aedes albopictus and arbovirus spread by it. It was
more relevant and appropriate in area where both the diseases prevalent.

Chapter IV KAP study on Aedes borne diseases
237
Ph.D Thesis Mosquito fauna
The socio-demographic characteristics investigated in the present study
were significant associated with the level of Knowledge except for age and sex. In
agreement with other studies, an association of level of knowledge with education,
occupation and financial status was found. High income respondents had better
knowledge level than low income one. Syed et al., (2011) reported a significant
associations of knowledge with education (p= 0.004) and socioeconomic status
(p=0.02). Knowledge of dengue is inadequate in the low socioeconomic class.
4.5.6. Association between Socio-economic-demographic status and Over-all
Level of Attitude and Practice
In the present study a significant association between education and
preventive practices was noted. This observation parallels with that of Dickson et
al (2011). According to Syed et al (2011) high socioeconomic group showed better
preventive practices.
4.5.7. Association between over-all level of knowledge and over-all level of
attitude and practice
The knowledge level was unrelated to preventive practice in our study.
Koenraadt et al., (2006) made similar observation in elsewhere, where knowledge
of mosquitoes was not led to source reduction practice. Knowledge alone is greatly
not sufficient to change attitude and practice. Residents may not practice source
reduction because they believe other methods (adult control measures) they use to
reduce mosquitoes are more effective or easier, or because they do not realize the

Chapter IV KAP study on Aedes borne diseases
238
Ph.D Thesis Mosquito fauna
presence of breeding ground in their premises (Tuiten et al., 2009). Many
respondents in our survey think that mosquito control is the responsibility of local
government or government departments (Table 4.11). This belief discouraged
residents from practicing source reduction as they felt residents could not
effectively reduce mosquito populations (McNaughton et al., 2010). Other factors
may include lack of motivation, time, social factors, perceived benefits, taboos etc.
On the contrary, significant association between knowledge and attitude towards
vector control were reported (Hairi et al., 2003).
Highly significant correlation was observed between self reported source
reduction practices and occurrence of breeding habitat. Present study showed that
participation in source reduction measures significantly reduces the number of
houses positive for larval breeding (Table 4.26). Similarly, during the survey, it
was also noted that relatively less number of breeding habitats was observed in
households where source reduction was practiced than households from where
source reduction was not practiced. In other words, Numbers of positive water-
holding containers were detected around many households where residents
reported source reduction practice, but these households had lower positive
containers, than those where residents did not report source reduction practice. The
efficacy of source reduction practice is often judged based on the number of water-
holding and mosquito-positive containers in residents’ premises (Koenraadt et al.,
2006; Tuiten et al., 2009). Winch et al., (2002) noted that many mosquitoes
breeding in households where residents had received source reduction education

Chapter IV KAP study on Aedes borne diseases
239
Ph.D Thesis Mosquito fauna
were found in “invisible” containers, hidden from superficial inspection. In the
present study it is assumed that residents who practiced source reduction
overlooked containers that were small or hidden from superficial observation.
Many residents were unaware of breeding sites such as tree holes, leaf axils, tyres,
plant pots and other small and uncommon breeding sites (Table 4.6). Time interval
between two successive source reductions is also important especially during rainy
season. Elimination of container is more efficient rather than empting it. In rubber
plantations method of source reduction consists mainly of keeping the latex
collecting containers upside down during rainy days/season, rather than removal of
containers. This measure is usually adopted in simultaneous with the sap
collection, on an expected rain. Farmers usually don’t practice this measure during
non rainy day/season as it causes some latex loss. Unexpected continuous rain will
store water in the container and forms a breeding site for Aedes. Education
campaigns need to emphasize practical ways to get rid of breeding sites (Koenraadt
et al., 2006), provide details on overlooked containers, give tips on how to
thoroughly search a premises of household for water-holding containers (Winch et
al., 2002), and emphasize that source reduction should be practiced at least once a
week.
4.5.8. Association of incidence of disease with over-all level of knowledge
No significant association of incidence of disease with over-all level of
knowledge was observed. This does not mean that knowledge were nothing to do with
Chapter IV KAP study on Aedes borne diseases
240
Ph.D Thesis Mosquito fauna
the incidence of diseases but there might be some other important factors that were not
considered here (Table 4.27).
4.5.9. Association of incidence of disease with Over-all Level of Attitude and
Practice
In the present study no significant association of incidence of disease and over-
all level of attitude and practices regarding disease prevention and control was
observed (Table 4.28).
4.5.10 Conclusion
The present survey showed that the participants have sufficient knowledge
regarding Aedes mosquito and Aedes-borne diseases. It may be due to the fact that CG
had been a cause of concern in Kerala recently, and since media was giving enough
awareness. However some deficiencies in their knowledge related to certain aspects
exists. High level of knowledge was not translated into a good practice. It was found
that respondents were more concerned with personal preventive measures mainly
focused towards protection from mosquito bites rather than source reduction. Where
residents practiced source reduction, mosquito sources were significantly reduced or
absent. The observed deficiency should be compensated through proper awareness
programmes and source reduction efforts could be improved by motivating residents
through community-based efforts.

Chapter IV KAP study on Aedes borne diseases
241
Ph.D Thesis Mosquito fauna
GENERAL SUMMARY AND CONCLUSION OF THE STUDY
Mosquitoes are probably the most notoriously undesirable Arthropods, with
respect to their ability to transmit various pathogens. More than a hundred species
of mosquitoes are capable of transmitting various diseases to humans and other
animals. They are also known for being irritating biting pests. Sometimes, their
nuisance bites are so severe that they make outdoor activities almost impossible.
The tourism industry is also seriously affected. Mosquitoes are undeniably more
detrimental to human health than any other group of Arthropod vectors.
Today, mosquito control is a vital public-health practice throughout the
world, especially in the tropics because of its profound negative impact on human
progress. Mosquito control in an area is effective only when it is based on the
sound of knowledge of the species- the species diversity, distribution, population
dynamics, breeding ecology, vector status and other aspects of bionomics of
vectors in that particular geographic area. Similarly Knowledge, attitude and
practice of people regarding vectors and vector control should be measured as for
the success of any vector control activity and subsequently the prevention of
vector-borne disease in that area. Ironically, the mosquito composition, diversity,
distribution, ecology and population dynamics of many species of mosquitoes are
not adequately known from Kerala. Therefore, it is highly relevant and appropriate
to investigate the mosquito fauna, especially of central Kerala which is considered
as the epicentre of various mosquito-borne diseases.
Chapter IV KAP study on Aedes borne diseases
242
Ph.D Thesis Mosquito fauna
Present study gives a clear idea on the diversity and composition of
mosquito fauna in the study area. A total of 12196 mosquitoes belonging to 10
genera and 38 species were collected during 1728 man-hours of collection.
Collected genera include Aedes, Anopheles, Armigeres, Culex, Coquillettidia,
Heizmannia, Mansonia, Mimomyia, Toxorhynchites and Uranotaenia. Genus
Culex was represented by 16 species, followed by genus Anopheles by seven
species, Aedes by six species, Mansonia by three species and one species each by
genus Armigeres, Coquilletidia, Heizmannia, Mimomyia, Toxorhynchites and
Uranotaenia Among the 10 genera, Culex was the predominant genus and was
represented by 42.5 percentages of the total mosquitoes collected, followed by
Aedes by 26.5 and Armigeres by 19.7 percentages. Armigeres sabalbatus was the
most predominant species with 2404 mosquitoes (19.7%), followed by Aedes
albopictus with 2277 mosquitoes (18.6%) and Culex tritaeniorhynchus with 1509
mosquitoes (12.3%). The remaining 35 species constituted only less than 50 per
cent of the total catches. Of the 38 species studied, 21 species were recognized as
medically important vector mosquitoes. Distribution varied with season, space and
altitude. Species diversity was not varied much with season but most of the species
showed seasonal fluctuation in population density. Spatial distribution varied from
species to species. Ar. sabalbatus showed maximum spatial distribution with 44.4
average number of localities. The average number of localities where
Ae.albopictus found was 34.7. Density and species richness declined from lower
altitude to higher altitude. Larval habitats of 31 species of mosquitoes were

Chapter IV KAP study on Aedes borne diseases
243
Ph.D Thesis Mosquito fauna
detected during the study. Ae. albopictus, Ar. sabalbatus and Cx. quinquefasciatus
were found in more than 10 habitats. Latex collecting containers, discarded
coconut shells and tank were the major breeding sites observed in the study area..
Breeding ecology and population dynamics of adult Ae.albopictus have
been explored during the study. Ae. albopictus showed a high degree of plasticity
to various breeding sites and exploited all types of available potential breeding
habitats . The main habitat exploited by Ae.albopictus for breeding was the latex
collecting cup (36.3%), followed by plastic container (10.3%). Other breeding
habitat observed during the study include coconut shells, metallic containers, mud
pot, plant pot, tyre, tank, leaf axils, tree holes and other discards. Relatively high
larval Indices were recorded during the study period. Analysis shows that all larval
indices are well above the threshold levels. Ae.albopictus was present in all
months of study and population density of adult varied from month to month and
season to season. Its monthly total density varied from 0.14 (Feb 2010) to 13.4
(May 2009). Seasonal distribution showed highest seasonal prevalence in pre-
monsoon, followed by monsoon. Monthly landing density varied from 1(Feb 10) to
28 (May2010). Larval indices and adult densities of Aedes albopictus have been
recorded above the critical levels and it implies their potential for future outbreaks.
KAP study measured the Knowledge, Attitude and Practices of residents
regarding Ae. albopictus and Ae. albopictus- borne diseases. Present survey showed
that the participants have sufficient knowledge regarding Ae.albopictus and Ae.
albopictus- borne diseases. However, the relatively higher level of knowledge was not
Chapter IV KAP study on Aedes borne diseases
244
Ph.D Thesis Mosquito fauna
translated into a corresponding level of good practice. It was found that respondents
were more concerned with personal preventive measures mainly focused towards
protection from mosquito bites rather than source reduction.
This study provides baseline information on mosquito fauna of Central
Kerala. The study has revealed the presence of many mosquito species, including
vectors of various arboviral diseases. Forest cover, high rainfall, high relative
humidity and moderate temperature along with crops such as rice, rubber, cocoa,
pineapple, coconut and arecanut make suitable conditions for mosquito breeding
and proliferation, especially for Ae.albopictus. Source reduction through
modification or eradication of habitat is essential for the control of mosquitoes and
subsequently the mosquito borne-diseases. Source reduction efforts could be
improved by motivating residents through proper education and community-based
efforts. An integrated vector control program with the participation of the public,
local Governments, various departments of government and public sectors is
advantageous because in addition to reducing the risk of mosquito-borne diseases,
it could also result in an overall reduction in densities of nuisance mosquitoes
making it more acceptable to the surrounding community.





![Aedes Mosquitoes and Aedes-Borne Arboviruses in Africa ...archive.lstmed.ac.uk/8158/1/Aedes Mosquitoes and... · Aedes aegypti almost certainly originated in Africa [12–14]. Globally](https://static.fdocuments.us/doc/165x107/5f02c52c7e708231d405ecc9/aedes-mosquitoes-and-aedes-borne-arboviruses-in-africa-mosquitoes-and-aedes.jpg)












