Chapter 8 The Respiratory System. 2 Objectives State the major developmental events of the...
29
Chapter 8 The Respiratory System
-
Upload
randolph-logan -
Category
Documents
-
view
219 -
download
4
Transcript of Chapter 8 The Respiratory System. 2 Objectives State the major developmental events of the...

Chapter 8
The Respiratory System

2
Objectives
• State the major developmental events of the respiratory system in the womb.
• Describe the key elements of normal fetal circulation.
• State what happens to the respiratory system at birth.• Describe the developmental events in the respiratory system that
continue after birth.


4
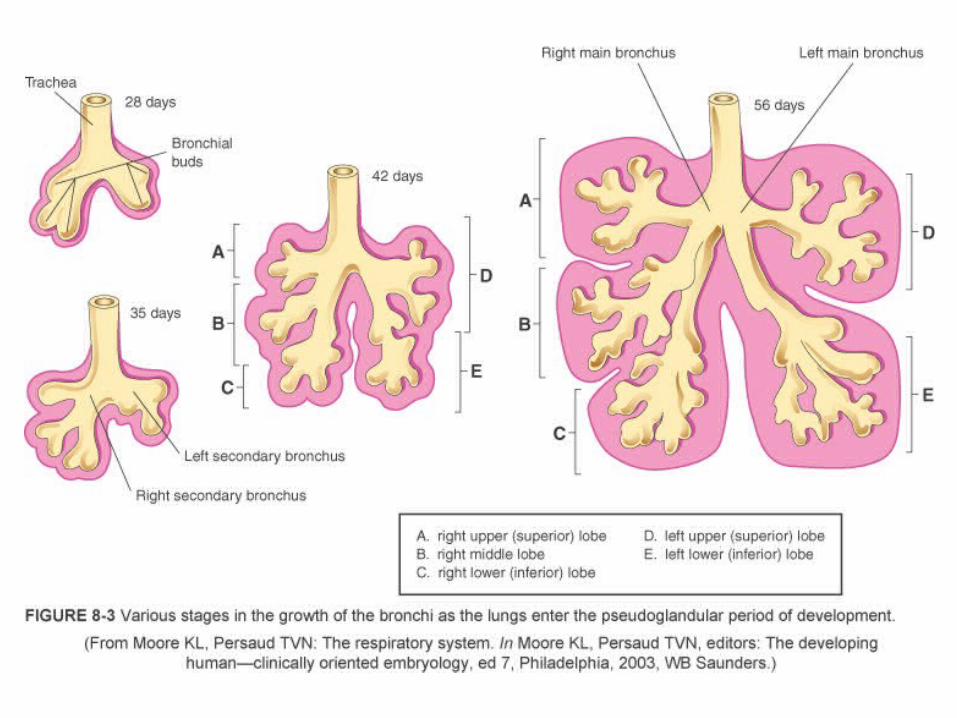
Development of the Respiratory System
• Extends from almost conception into childhood.
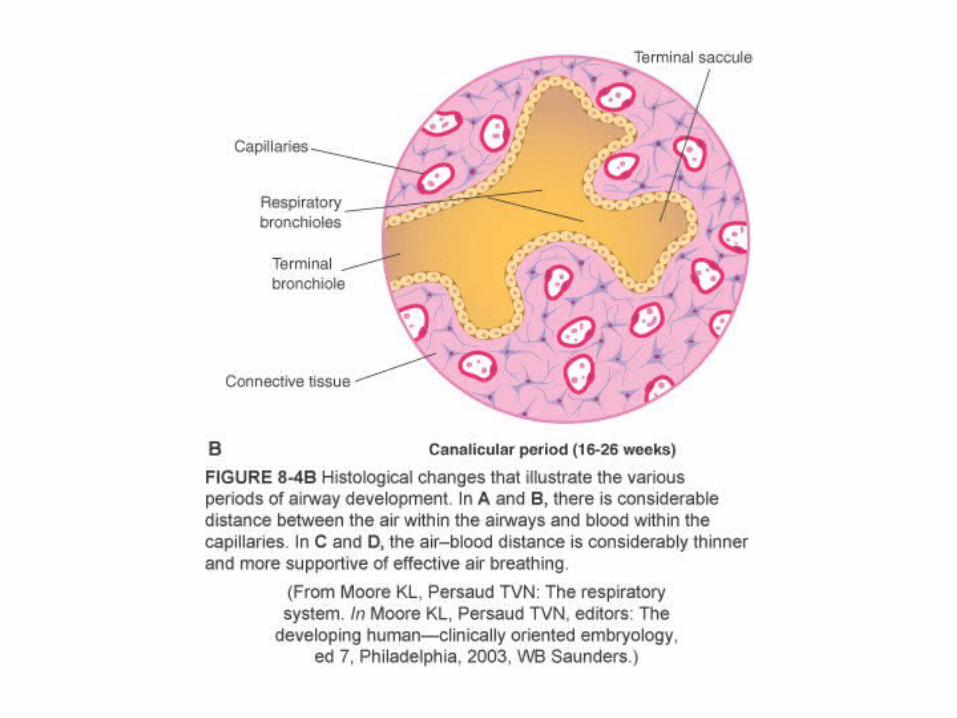
• During canalicular phase, life becomes possible.

6
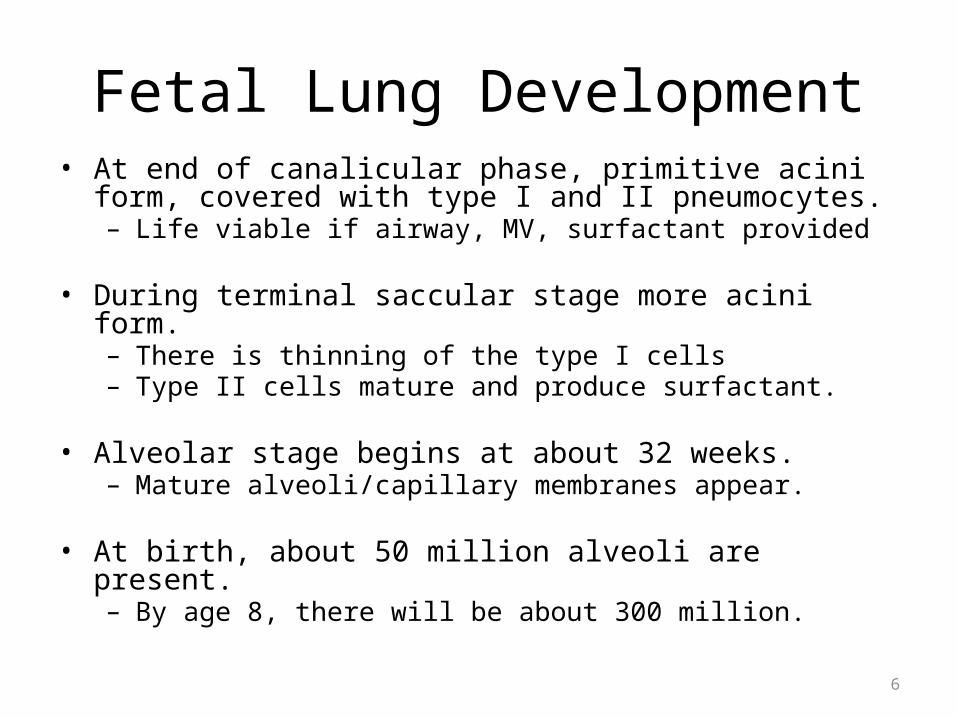
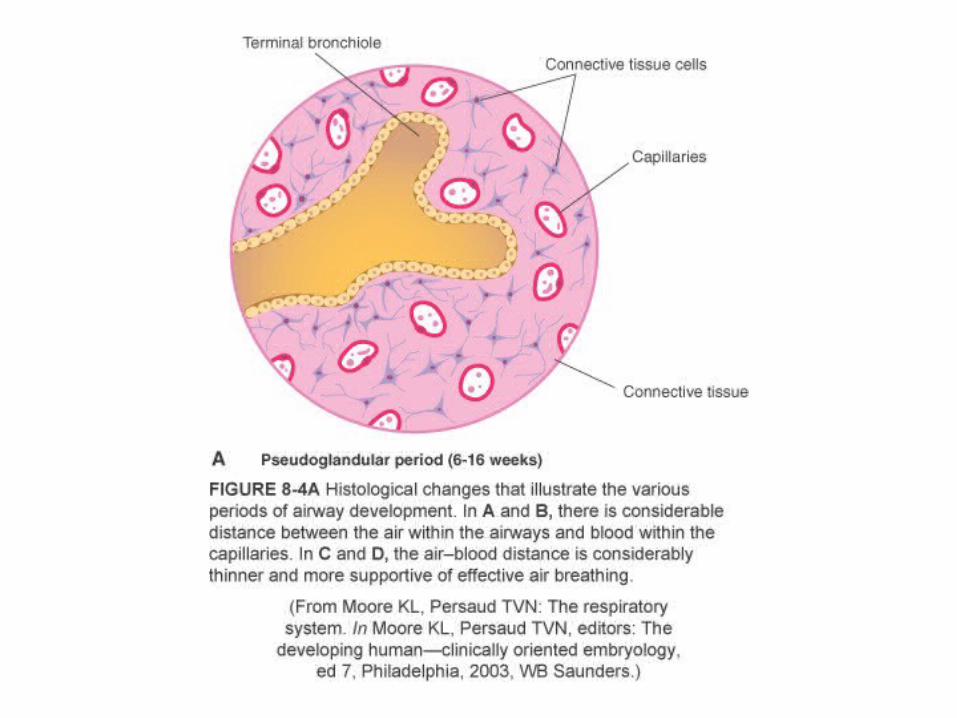
Fetal Lung Development• At end of canalicular phase, primitive acini form, covered with type I
and II pneumocytes.– Life viable if airway, MV, surfactant provided
• During terminal saccular stage more acini form.– There is thinning of the type I cells – Type II cells mature and produce surfactant.
• Alveolar stage begins at about 32 weeks.– Mature alveoli/capillary membranes appear.
• At birth, about 50 million alveoli are present.– By age 8, there will be about 300 million.



12
The Fetal Lung• Lung maturation is determined by surfactant.
– Phosphatidylcholine levels predictive• Lecithin/sphingomyelin ratio (L/S ratio)• Phosphatidylglycerol (PG) concentration
• Fetal lung fluid is constantly produced– Slight positive pressure keeps lungs inflated.
• Promotes normal lung development• At birth, lungs hold about 40 ml of fluid.• If deficient, can result in hypoplastic lung

13
Uterine Life• In utero life depends on placental structure, which provides, among
many things:– Gas exchange– Nutrients and waste removal– Defense against disease
• Fetal circulation incorporates the placenta by the umbilicus and use of three special shunts:– Ductus venosus, ductus arteriosus, and foramen ovale


15
Uterine Life (cont.)

16
Fetal Circulation• Placenta large volume, low resistance system, so fetal SVR is low
• Umbilical vein returns oxygenated blood from the placenta to fetus via the ductus venosus.
• Flows into the IVC and on to the RA
• Oxygenated blood is preferentially shunted through the foramen ovale from the right to the left atrium.– Provides oxygenated blood to systemic circulation

17
Fetal Circulation (cont.)
• In utero fetal lungs have high PVR due to low PAO2.– Ductus arteriosus shunts blood from high-resistance pulmonary artery
to low-resistance aorta.
18
Cardiopulmonary Events at Birth• Fetal lung fluid
– Prior to birth, production stops and absorption starts.– One third of fluid is expelled by vaginal squeeze.– Pulmonary lymphatics absorb remaining fluid.
• Tactile and thermal stimuli initiate first breath.– Initial breath requires transpulmonary pressures >40 cm H2O.– Subsequent breaths require progressively less pressure as lung volume
increases.
19
Cardiopulmonary Events at Birth (cont.)
• Air in lung increases PO2 and pH, while PCO2 decreases, which results in:– Pulmonary vasodilation and decreased PVR– Ductus arteriosus constriction/closure– Increased pulmonary blood flow
• At the same time, placenta removal results in:– Sudden increase in SVR
• Net results:– LAP > RAP, so foramen ovale closes– Transition to extrauterine circulation complete


22
Postnatal Upper Airway• Head flexion can cause airway obstruction.
• Factors contributing to airway obstruction– Tongue is relatively larger compared with adults.– Nasal passages are relatively smaller.
• Most infants nose breathe exclusively.• At 4 to 5 months, most infants can breathe orally.
– Infections or Intubations can cause obstruction at the cricoid cartilage (narrowest point) or the epiglottis, which is relatively longer and less flexible than that of an adult.


24
Vascular Development• Basic structure is in place at birth.
• Subsequent vascular growth involves increased smooth muscle growth and increased density of arterioles and capillaries in distal regions.
• Lungs are unique as blood from RV and LV provide flow to alveoli microcirculation.– Pulmonary circulation from RV– Bronchial circulation from LV– Provides greater stability and resistance against the impact of disease
processes

25
Lymphatic and Nervous Development
• Lymph nodes and vessels are located in connective tissues beside pulmonary structures – Provide fluid control and defense
• Absorbed fluid travels to hilar lymph nodes
• Nervous tissue development– Brainstem centers for automatic control– Phrenic and intercostal nerves form to carry motor signals to diaphragm
and intercostal muscles– Autonomic fibers form for smooth muscle control

26
Chest Wall Development, Diaphragm and Lung Volume
• Infant thorax is more compliant than that of an adult.
• FRC is established by the equal and opposing forces of chest wall to expand against the lungs tendency to collapse.
• The infant’s more compliant thorax results in lower FRC and TLC. – Predisposes infant to early airway closure, atelectasis, V/Q mismatch,
and hypoxemia– Combated by ending expiration early, results in gas trapping,
narrowing the glottis, back pressure • Patient will make a grunting sound
. .