
Chapter 81_Chapter+8... · ... negative N balance and pregnant women CRE (creatinine) (0.6-1.3...
35
CLINICAL: BIOCHEMICAL ASSESSMENT Chapter 8 1
Transcript of Chapter 81_Chapter+8... · ... negative N balance and pregnant women CRE (creatinine) (0.6-1.3...
CLINICAL: BIOCHEMICAL ASSESSMENT
Chapter 81

Objectives2
Describe why lab tests are used in the nutrition care of a patient Describe: Whole blood, serum and plasma Describe specimen types Explain static vs functional assay Define what makes up the Basic Metabolic Panel (BMP) and the Comprehensive
Metabolic Panel (CMP) Explain what each test of the BMP and CMP can tell the provider Explain what makes up a CBC Describe a CBC differential- list the leukocytes and what too high or low
percentages may indicate Summarize stool and urine assessments Describe what happens to the body during acute stress and the role of nutrition
support at this time. Explain the role of albumin Describe nutritional anemias and how to treat
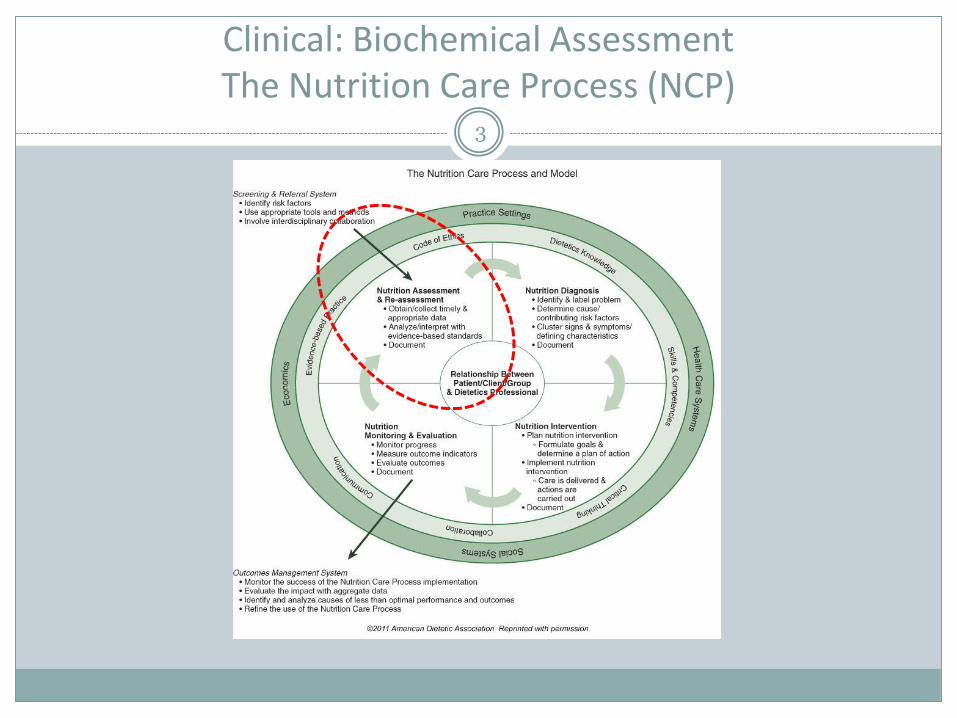
Clinical: Biochemical AssessmentThe Nutrition Care Process (NCP)
3
Clinical: Biochemical Assessment
4
Lab tests are ordered to diagnose, support a diagnosis and monitor treatment
Illness or injury can compromise nutrition status very quickly in an inpatient setting
Objective data
Laboratory assessment is highly controlled process
Compares a control (analyte) to patient specimen

Clinical: Biochemical Assessment- Specimen Types
5
Whole blood: None of the elements are removed; the sample contains RBC, WBC, platelets and plasma
Serum: Liquid fraction of whole blood that is collected after the blood is allowed to clot (15-30 min @ room temp) and is centrifuged–no anti-coagulant used.
Plasma: The semi-clear (light straw color) liquid component of blood is produced when whole blood is collected in tubes that are treated with an anticoagulant (e.g. EDTA). The supernatant (plasma) is made up of water, blood proteins, inorganic electrolytes
Clinical: Biochemical Assessment- Specimen Types
6
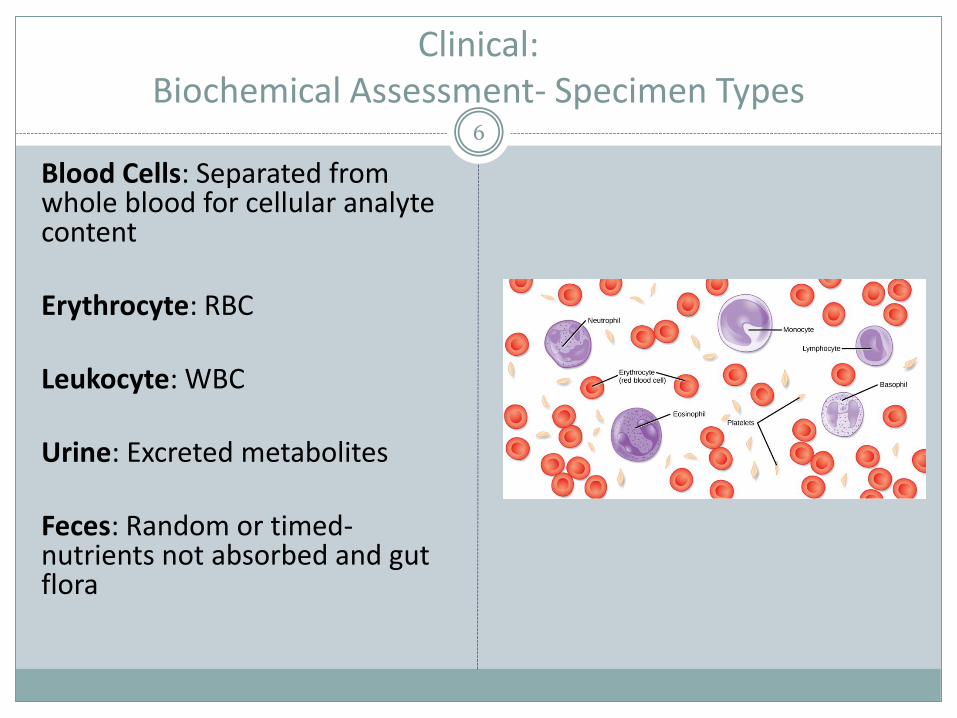
Blood Cells: Separated from whole blood for cellular analytecontent
Erythrocyte: RBC
Leukocyte: WBC
Urine: Excreted metabolites
Feces: Random or timed-nutrients not absorbed and gut flora
Clinical: Biochemical Assessment- Specimen Types
7
Less common tests
Breath: Evaluate nutrient metabolism (CHO)
Hair and nails: Exposure to toxic metals- not good for nutrient levels
Saliva: Adrenal stress and hormone levels
Sweat: Cystic Fibrosis (electrolytes)

Clinical: Biochemical Assessment- Assays
8
Static assays
Measure the actual level of nutrient in the specimen Serum iron
WBC ascorbic acid
[NUTRIENT] DO NOT REFLECT THE AMOUNT OF NUTRIENT STORED IN OTHER TISSUES THAT HAVE NOT BEEN SAMPLED
Functional assays
Quantitatively measure a biochemical or physiologic activity that depends on the nutrient of interest Serum ferritin- good indicator of iron storage pool
Clinical: Biochemical Assessment- Routine Medical Lab Tests
9
Clinical Chemistry PanelsPanel: group of tests
Basic Metabolic Panel (BMP) 8 tests1.GLU2.Ca3.Na+4.K+5.CO2 (HCO3-)6.Cl-7.BUN8.Cre
Comprehensive Metabolic Panel (CMP) BMP + 6 additional1. GLU2. Ca3. Na+4. K=5. CO2 (HCO3-)6. Cl-7. BUN8. Cre
9. Albumin10.Total PRO11.ALP12.ALT13.AST14.Bilirubin

Clinical: Biochemical Assessment- Routine Medical Lab Tests
10
Labs are often grouped as defined by the Centers for Medicare and Medicaid Services
Reimbursement

Clinical: Biochemical Assessment- Routine Medical Lab Tests
11
Basic Metabolic Panel (BMP)
GLU (fasting): 70-100 mg/dL
A fasting GLU of >100mg/dL is an indicator of insulin resistance
A fasting GLU of >125 mg/dL in indicates DM

Clinical: Biochemical Assessment- Routine Medical Lab Tests
12
Basic Metabolic Panel (BMP) Con’tCa (8.5-10.5mg /dL)
99 % of body’s Ca is in bone- the other 1% is intracelluar and extracellular and is needed for many functions e.g. muscle contraction, blot clotting, nerve conduction, some hormone regulation
Hypercalcemia associated with endocrine disorders, malignancy and hypervitaminosis D, hyperparathyroidism
Hypocalcemia associated with vitamin D deficiency. Inadequate hepatic or renal vit D activation, hypoparathyroidism, renal failure. Serum calcium <7mg/dL can be associated with tetany
HOWEVER –About half of blood calcium is serum-bound so serum calcium levels need to be adjusted for patients with low serum albumin.
[normal alb-observed alb) x 0.8] + serum calcium= corrected calcium

Clinical: Biochemical Assessment- Routine Medical Lab Tests
13
Basic Metabolic Panel (BMP) ContNa+ (135-145 mEq/L)- most abundant cation in the body; serum electrolyteNa <120 mEq/L= danger! Hyponatremia due to excessive water intake or syndrome of inappropriate antidiuretic hormone secretion(SIADH): Inability to secrete diluted urine CNS disorder or CA.Symptoms:
confusion hypotension irritability lethargy seizures
Hypernatremia- usually caused by dehydration (not excessive Na intake)Symptoms:
irritability thirst decreased skin turgor
Correct hypernatremia slowly- rapid correction can lead to cerebral edema
Clinical: Biochemical Assessment- Routine Medical Lab Tests
14
Basic Metabolic Panel (BMP) Cont
K+ (3.6-5 mEq/L)- Major intracellular cation- needed for contraction of smooth, cardiac and skeletal muscle and maintaining electrolyte balance
Levels <2.5 mEq/L or > 6.5 mEq/L can lead to arrhythmias and death
Hypokalemia- Often a result of K losses due to mediations – often prescribed supplements to counteract
Hyperkalemia- Often seen with renal dysfunction or medications- diet or tube feed change often needed to decrease K intake.

Clinical: Biochemical Assessment- Routine Medical Lab Tests
15
Basic Metabolic Panel (BMP) Cont
HCO3- or total CO2 (21-31 mEq/L): Detecting an acid-base imbalance: Test can help determine if acidity or alkalinity is:
Respiratory (due to an imbalance between the amount of oxygen coming in and CO2 being released)
OR
Metabolic (due to increased or decreased amounts of bicarbonate in the blood)
Cl- (101-111 mEq/L)
These electrolyte labs (Na, K, CO2/HCO3, Cl) are important for patient monitoring such as those on: TPN, renal, COPD, poorly managed DM, endocrine
disorders, ascites or edema, decreases K+ s/p v/d
Clinical: Biochemical Assessment- Routine Medical Lab Tests
16
Basic Metabolic Panel (BMP) Con’t
BUN (blood urea nitrogen) (5-20mg urea nitrogen/dL):Urea is the major nonprotein, nitrogenous end-product of protein catabolism and is excreted by the kidneys. Indicator of glomular insufficiency or failure but can be eleveted d/t dehydration, GI bleed, or catabolic state. 100mg /dL- may need to reduce/stop protein delivery
Increased in those with renal dx, excessive protein catabolism Decreased in those with liver failure, negative N balance and pregnant women
CRE (creatinine) (0.6-1.3 mg/dL): A byproduct of breakdown of muscle creatinephosphate- excreted by kidneys. Those with renal disease have a decreased ability to excrete creatinine resulting in elevated levels- better indicator of renal ds than BUN
Clinical: Biochemical Assessment- Routine Medical Lab Tests
17Comprehensive Metabolic Panel (CMP)
Alb (3.5 to 5.0 g/dL) Albumin is a protein made by the liver and is a marker of visceral protein status. Albumin has a half-life of 21 days so is not a real-time indicator of nutritional health.
Low albumin can be caused by: Poor diet (PEM) Liver ds Malabsorption Diarrhea Severe burns Sepsis Edema Acute inflammation
High: Dehydration
NOT PART OF THE CMP
Prealbumin (pAlb or PAB) (18.5-35mg/dL)Prealbumin is a better indicator of visceral protein status,. It has a shorter half life of about 2 days so it’s a better marker for monitoring response to nutrition therapy.
Sensitive to metabolic stress so low levels can be seen in catabolic states (eg sepsis, burns, postop). In these cases must also look a CRP. If patient has low PAB and CRP the low PAB is not due to malnutrition)
Total PRO (6.3 to 7.9 g/dL) The total protein test measures the total amount of two classes of proteins found in the fluid portion of your blood. These are albumin and globulin. Tests for done to diagnose nutritional problems, kidney disease or liver disease.
Clinical: Biochemical Assessment- Routine Medical Lab Tests
18
Comprehensive Metabolic Panel (CMP) con’tSerum Enzymes
ALP (Alkaline phosphatase aka ALK PHOS) (30 to 120 IU/L): An enzyme found in all body tissues. Tissues with higher amounts of ALP include the liver, bile ducts, and bone used to dx liver or bone disease, check liver functioning
ALT(alanine aminotransferase) (4 to 36 IU/L) An enzyme found in the highest amounts in the liver. Injury to the liver results in release of the substance into the blood. Higher due to hepatitis, hepatic CA, MI, burns, mononucleosis, pancreatitis, obesity
AST(aspartate aminotransferase) (10 to 35 IU/L) An enzyme found in high amounts in liver, heart, and muscle cells. It is also found in lesser amounts in other tissues. Increased in: acute cirrhosis, hepatitis, pancreatitis, renal ds, trauma, crushing injury, gangrene

Clinical: Biochemical Assessment- Routine Medical Lab Tests
19
Comprehensive Metabolic Panel (CMP) Con’t
Bilirubin (0.3 to 1.0 mg/dL) Bilirubin is a yellowish pigment found in bile, a fluid made by the liver. Liver disease or damage can lead to large amounts of bilirubin in the blood can lead to jaundice.

Clinical: Biochemical Assessment- Routine Medical Lab Tests
20
Complete Blood Count (CBC) includes,
RBC count
Hemoglobin
Hematocrit
Mean corpuscular volume (MCV)
Mean corpuscular hemoglobin (MCH)
Mean corpuscular hemoglobin concentration (MCHC)
WBC count
“CBC with diff” includes measurement of different types of WBC (leukocytes) to further asses type of infection

Clinical: Biochemical Assessment- Routine Medical Lab Tests
21
Complete Blood Count (CBC): A count and description of erythrocytes
Red blood cells (4.7-6.1 x10^6/uL (males); 4.2-5.4 x10^6/uL (females); If the RBC count is low (anemia), the body may not be getting the oxygen it needs. If the count is too high (polycythemia, there is a chance that the red blood cells will clump together and block capillaries)
Hemoglobin (Hgb) (14-18g/dL (males); 12-16g/dL (females) The hemoglobin molecule fills up the red blood cells. It carries oxygen and gives the blood cell its red color. The hemoglobin test measures the amount of hemoglobin in blood and is a good measure of the blood's ability to carry oxygen throughout the body.
Hematocrit (HCT) 42-52% males; 35-47% females; 33% (preg); 454-64% newborns; Measures volume RBC take up in the blood. The value is given as a percentage of red blood cells in a volume of blood. For example, a hematocrit of 38 means that 38% of the blood's volume is made of red blood cells. Hematocrit and hemoglobin values are the two major tests that show if anemia or polycythemia is present.

Clinical: Biochemical Assessment- Routine Medical Lab Tests Complete
Blood Count 22
Complete Blood Count (CBC): A count and description of erythrocytescon’t
Red blood cell indices1. Mean corpuscular volume (MCV) shows the size of the red blood cells 2. Mean corpuscular hemoglobin (MCH) amount of hemoglobin in an
average red blood cell- can be used to determine type of anemias (macro vs microcytic)
3. Mean corpuscular hemoglobin concentration (MCHC) [hemoglobin] in an average red blood cell
WBC (leukocyte) count. When a person has a bacterial infection, the number of white cells rises very quickly. The number of white blood cells is sometimes used to find an infection or to see how the body is dealing with cancer treatment.

Clinical: Biochemical Assessment- Routine Medical Lab Tests WBC differential
23
Neutrophils (55-70%) ↑ Neutrophilia: ketoacidosis, trauma, stress, pyogenic (pus-forming) infx, leukemia↓ Neutropenia: PEM, aplastic anemia (not producing RBC) , chemotherapy, infx (overwhelming)
Lymphocytes (20-40%)↑ Lymphocytosis: Viral, infx, leukemia, myeloma (type of CA) , mononucleosis↓ Lymphocytopenia: Leukemia, chemo, sepsis, AIDS
Monocytes (2-8%)- increased indicates severe infxn
Eosinophils (1-4%)↑ Eosinophilia: Parasitic infx, allergy, eczema, leukemia, autoimmune ds↓ Eosinopenia: ↑ steroid production
Basophils (0.5-1%)↑Basophilia: Parasitic infx, Leukemia↓Basopenia: allergy
Clinical:
Biochemical Assessment- Routine Medical Lab Tests Stool Testing24
Fecal testing can test for blood, pathogens and gut flora
Fecal Occult Blood test:
Tests for blood in those ↑50 and those with unexplained anemia
Ordered in those with prolonged diarrhea to test for pathogens (food borne illness)
Other: Unexplained ↓wt
Clinical:
Biochemical Assessment- Routine Medical Lab Tests Urinalysis25
Check for metabolic and/or renal disorders
1. Appearance of urine
2. Result of a basic test with reagent sticks (dipstick)
3. Microscopic examination of sediment
UA’s are routine and measure glucose, ketones, blood, protein or albumin, bilirubin and leukocytes
Clinical:
Biochemical Assessment- Routine Medical Lab Tests- Urinalysis
26
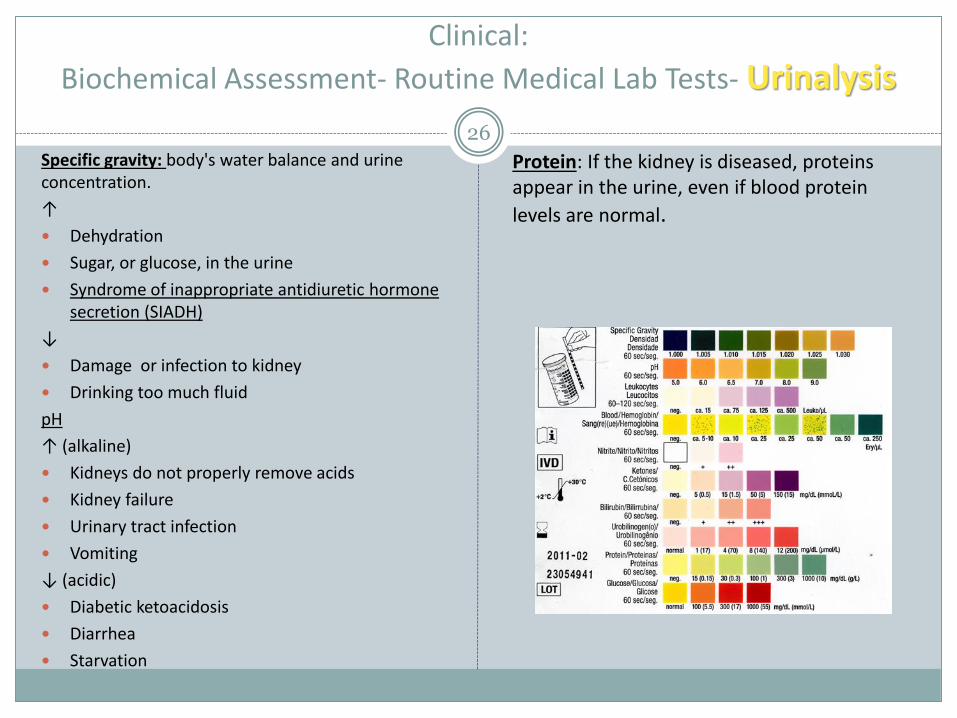
Specific gravity: body's water balance and urine concentration.
↑
Dehydration
Sugar, or glucose, in the urine
Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
↓
Damage or infection to kidney
Drinking too much fluid
pH
↑ (alkaline)
Kidneys do not properly remove acids
Kidney failure
Urinary tract infection
Vomiting
↓ (acidic)
Diabetic ketoacidosis
Diarrhea
Starvation
Protein: If the kidney is diseased, proteins appear in the urine, even if blood protein
levels are normal.
Clinical:
Biochemical Assessment- Routine Medical Lab Tests Urinalysis27
GLU: Glucose in the urine is called glycosuria or glucosuria: Glucose is not usually found in urine. If it is, further testing is needed.
Ketones: Negative test is normal: if presence is detected patient is ketotic d/t ↓BG (usually uncontrolled DM1)
Blood: Negative test is normal if presence if detected: infx (note: menstruation)
Bilirubin: Negative test is normal if presence if detected: liver or gallbladder disorder
Clinical: Biochemical Assessment- Stress-Related PEM
28
Acute illness or trauma causes an inflammatory response
Hormones and cell-mediated responses trigger the breakdown of lean tissue to produce:
Cytokines
Acute-phase proteins
Lactic acid
WBC
During acute stress/trauma RD cannot rely on traditional labs
Patient metabolized protein very quickly but adding protein to diet does not attenuate this loss.

Clinical: Biochemical Assessment- Stress-Related PEM
29
C-Reactive Protein
Helps to identify when acute hypermetabolicperiod of the inflammatory response wanes and can begin nutrition support
Exact function of CRP is not clear, levels rise 4-6h s/p surgery or trauma
Hepatic acute phase (AP) protein response after trauma in 10 septic and 16 nonseptic patients :
Sganga et al, 1985, American Medical Association

Clinical: Biochemical Assessment- Stress-Related PEM
30
Albumin: Accounts for 60% of total serum proteins. Albumin transports major blood constituents, hormones, enzymes, medications, minerals, ions, FA and amino acids.
Main function is to maintain colloidal osmotic pressure (oncotic pressure) of the plasma.
Albumin has a half-life of 18-21 days so does not reflect current PRO intake
Loss of albumin (protein) can result in edema/ascites
http://youtu.be/BBV-DaLf_n0

Clinical: Biochemical Assessment- Stress-Related PEM
31
Prealbumin (PAB) officially Transthyretin (TTHY)
Half-life of 2 days so a better indicator of current protein status
PAB drop in inflammatory stress and do not usually improve with nutrition support
Clinical: Biochemical Assessment- Nutritional Anemia
32
A reduction in the number of erythrocytes per unit of blood volume
OR
A decrease in hemoglobin content of blood to below the level of usual physiologic need
Anemia is not a disease- it is a symptom:
Blood loss
Blood cell destruction
↓ blood cell formation

Clinical: Biochemical Assessment- Nutritional Anemias
33
Data from the CBC can be used to determine type of anemia and tx
Microcytic anemia (↓ MCV) : iron deficiency
Macrocytic anemia (↑ MCV): Folate or B12 deficient erythropoiesis
Macrocytic anemias include Megaloblastic anemia: folate deficiency
Pernicious anemia: B12 deficient
34
Data from the CBC can be used to determine type of anemia and tx
Hct and Hgb part of routine CBC; used to measure iron status Hct – measure of percentage of RBCs in total blood volume
Ferritin – storage protein that sequesters the iron normally gathered in liver As iron supply increases, intracellular ferritin increases
Positive acute phase protein; synthesis increase in presence of inflammation
Clinical: Biochemical Assessment- Nutritional Anemias
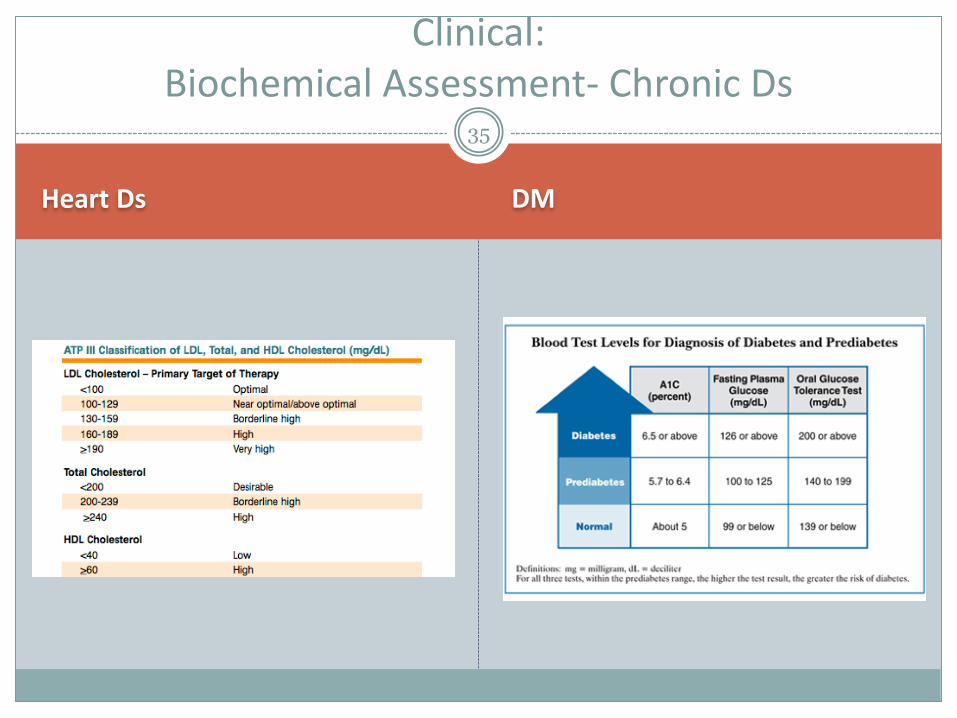
Heart Ds DM
35
Clinical: Biochemical Assessment- Chronic Ds


















