CHAPTER 57 SEPSIS AND SEPTIC SHOCK - University of Manitoba · 2020-02-19 · Sepsis Burns SIRS...
38
P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12 CHAPTER 57 ■ SEPSIS AND SEPTIC SHOCK ANAND KUMAR ASEEM KUMAR Septic shock (shock due to infection) and sepsis-associated mul- tiple organ failure are the dominant cause of death in intensive care units of the industrialized world. As many as 800,000 cases of sepsis are admitted every year to American hospitals (compa- rable to the incidence of first myocardial infarctions), with half of those developing septic shock (1). Historically, the mortality associated with sepsis and septic shock has been approximately 50% to 75% (2–4). The major advance in the therapy of septic shock was the development of antibiotic therapy 50 years ago, which resulted in a reduction in sepsis-associated mortality in the 30% to 50% range (2,3). However, the past 40 years have seen a gradual year-to-year increase in the incidence of sepsis (5). As a result, total deaths in the United States have increased even though the overall mortality rate has fallen from 27.8% to 17.9% during that period (5). At present, the total death toll from sepsis is comparable to that from myocardial infarc- tion and far exceeds the impact of illnesses such as acquired immune deficiency syndrome (AIDS) or breast cancer (1,6). The total number of cases continues to gradually increase due to a burgeoning population of patients with a chronic and high degree of susceptibility to infection (age, AIDS, organ fail- ure with transplant, and other chronic illness); an increased use of invasive medical devices; and increased use of cytotoxic agents for autoimmune disease, transplants, and malignancy for patients at high risk for sepsis. Current estimates suggest a doubling of total United States cases by 2050 but with only a projected increase in population of 33% (1). Until recently, de- spite major advances in technology and constant refinement of our understanding of sepsis pathophysiology, numerous clin- ical trials have failed to produce any new drugs with con- sistent beneficial effects on this patient population. Nonethe- less, the last 50 years have seen a gradual improvement in mortality, perhaps related to improvements in supportive care (5,7). DEFINITIONS Derived from the Greek word “sepo,” meaning “I rot,” the first introduction of the term sepsis occurs in the poems of Homer (circa eighth century B.C.) (8). Over the intervening 2700 years, through Homer, Hippocrates, Aristotle, and Galen to current-day physicians, the term has continued to be used virtually unchanged in meaning. Hugo Schottm ¨ uller modern- ized the term with his 1914 definition, “Septicemia is a state of microbial invasion from a portal of entry into the blood stream which causes signs of illness” (9). From the time of Schottm ¨ uller’s definition of septicemia until recent years, terms such as septicemia, sepsis, toxemia, and bacteremia were all used interchangeably to indicate patients exhibiting systemic responses to infection. A significant problem with the term septicemia (as defined by Schottm ¨ uller) is that most patients with a septic response cannot be documented to have bacteremia/fungemia, and many with bacteremia/fungemia (e.g., endocarditis, catheter-related infection) do not exhibit overt sepsis. Recognizing that future large-scale clinical trials of novel sepsis therapies will require more consistent and precise definitions of the septic response, consensus definitions were developed in 1991 (10). These cri- teria were developed primarily as a tool to enhance the ability to perform clinical sepsis research. However, the terminology soon entered the clinical lexicon. These consensus definitions were revised in 2001 to accommodate the clinician’s perspec- tive (11). Current and previous definitions follow. Infection. A microbial phenomenon characterized by an in- flammatory response to the presence of micro-organisms or the invasion of normally sterile host tissue by these organisms. Bacteremia. The presence of viable bacteria in the blood. The presence of other organisms in the blood should be described in like manner—viremia, fungemia, and so on. Bacteremia can either be transient, sustained, or intermittent. Systemic Inflammatory Response Syndrome (SIRS). The sys- temic inflammatory response to various severe clinical insults, including but not limited to infection. Various other clinical insults include pancreatitis, ischemia, multiple trauma and tis- sue injury, hemorrhagic shock, immune-mediated organ injury, and exogenous administration of inflammatory mediators such as tumor necrosis factor or other cytokines. Previous criteria for SIRS are enumerated in Table 57.1. The more recent re- Table 57.1 vision to sepsis definitions removed these SIRS criteria while retaining the concept. However, some understanding of these criteria remains crucial for the intensivist/clinical researcher, as most trials in the last 15 years have been predicated on patients having three or more of these criteria. Sepsis. The systemic response to infection. This response is similar to SIRS, except that it is considered to result from an infection. The previously accepted definition required at least two of the four SIRS criteria in the presence of documented or suspected infection. The recent revision of the criteria enu- merates multiple potential diagnostic criteria for sepsis (Table 57.2) and no longer specifically requires the discarded elements Table 57.2 of the SIRS criteria. Severe Sepsis. Sepsis associated with organ dysfunction, perfu- sion abnormalities, or hypotension. Organ system dysfunction can be described by organ failure scoring systems (12,13). Septic Shock. Sepsis with hypotension despite adequate fluid resuscitation, in conjunction with perfusion abnormalities. 1
Transcript of CHAPTER 57 SEPSIS AND SEPTIC SHOCK - University of Manitoba · 2020-02-19 · Sepsis Burns SIRS...

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
CHAPTER 57 ■ SEPSIS AND SEPTIC SHOCKANAND KUMAR � ASEEM KUMAR
Septic shock (shock due to infection) and sepsis-associated mul-tiple organ failure are the dominant cause of death in intensivecare units of the industrialized world. As many as 800,000 casesof sepsis are admitted every year to American hospitals (compa-rable to the incidence of first myocardial infarctions), with halfof those developing septic shock (1). Historically, the mortalityassociated with sepsis and septic shock has been approximately50% to 75% (2–4). The major advance in the therapy of septicshock was the development of antibiotic therapy 50 years ago,which resulted in a reduction in sepsis-associated mortality inthe 30% to 50% range (2,3). However, the past 40 years haveseen a gradual year-to-year increase in the incidence of sepsis(5). As a result, total deaths in the United States have increasedeven though the overall mortality rate has fallen from 27.8%to 17.9% during that period (5). At present, the total deathtoll from sepsis is comparable to that from myocardial infarc-tion and far exceeds the impact of illnesses such as acquiredimmune deficiency syndrome (AIDS) or breast cancer (1,6).
The total number of cases continues to gradually increasedue to a burgeoning population of patients with a chronic andhigh degree of susceptibility to infection (age, AIDS, organ fail-ure with transplant, and other chronic illness); an increaseduse of invasive medical devices; and increased use of cytotoxicagents for autoimmune disease, transplants, and malignancyfor patients at high risk for sepsis. Current estimates suggest adoubling of total United States cases by 2050 but with only aprojected increase in population of 33% (1). Until recently, de-spite major advances in technology and constant refinement ofour understanding of sepsis pathophysiology, numerous clin-ical trials have failed to produce any new drugs with con-sistent beneficial effects on this patient population. Nonethe-less, the last 50 years have seen a gradual improvement inmortality, perhaps related to improvements in supportive care(5,7).
DEFINITIONS
Derived from the Greek word “sepo,” meaning “I rot,” thefirst introduction of the term sepsis occurs in the poems ofHomer (circa eighth century B.C.) (8). Over the intervening2700 years, through Homer, Hippocrates, Aristotle, and Galento current-day physicians, the term has continued to be usedvirtually unchanged in meaning. Hugo Schottmuller modern-ized the term with his 1914 definition, “Septicemia is a stateof microbial invasion from a portal of entry into the bloodstream which causes signs of illness” (9). From the time ofSchottmuller’s definition of septicemia until recent years, termssuch as septicemia, sepsis, toxemia, and bacteremia were allused interchangeably to indicate patients exhibiting systemicresponses to infection.
A significant problem with the term septicemia (as definedby Schottmuller) is that most patients with a septic responsecannot be documented to have bacteremia/fungemia, and manywith bacteremia/fungemia (e.g., endocarditis, catheter-relatedinfection) do not exhibit overt sepsis. Recognizing that futurelarge-scale clinical trials of novel sepsis therapies will requiremore consistent and precise definitions of the septic response,consensus definitions were developed in 1991 (10). These cri-teria were developed primarily as a tool to enhance the abilityto perform clinical sepsis research. However, the terminologysoon entered the clinical lexicon. These consensus definitionswere revised in 2001 to accommodate the clinician’s perspec-tive (11). Current and previous definitions follow.
Infection. A microbial phenomenon characterized by an in-flammatory response to the presence of micro-organisms orthe invasion of normally sterile host tissue by these organisms.
Bacteremia. The presence of viable bacteria in the blood. Thepresence of other organisms in the blood should be describedin like manner—viremia, fungemia, and so on. Bacteremia caneither be transient, sustained, or intermittent.
Systemic Inflammatory Response Syndrome (SIRS). The sys-temic inflammatory response to various severe clinical insults,including but not limited to infection. Various other clinicalinsults include pancreatitis, ischemia, multiple trauma and tis-sue injury, hemorrhagic shock, immune-mediated organ injury,and exogenous administration of inflammatory mediators suchas tumor necrosis factor or other cytokines. Previous criteriafor SIRS are enumerated in Table 57.1. The more recent re- Table 57.1vision to sepsis definitions removed these SIRS criteria whileretaining the concept. However, some understanding of thesecriteria remains crucial for the intensivist/clinical researcher, asmost trials in the last 15 years have been predicated on patientshaving three or more of these criteria.
Sepsis. The systemic response to infection. This response issimilar to SIRS, except that it is considered to result from aninfection. The previously accepted definition required at leasttwo of the four SIRS criteria in the presence of documentedor suspected infection. The recent revision of the criteria enu-merates multiple potential diagnostic criteria for sepsis (Table57.2) and no longer specifically requires the discarded elements Table 57.2of the SIRS criteria.
Severe Sepsis. Sepsis associated with organ dysfunction, perfu-sion abnormalities, or hypotension. Organ system dysfunctioncan be described by organ failure scoring systems (12,13).
Septic Shock. Sepsis with hypotension despite adequate fluidresuscitation, in conjunction with perfusion abnormalities.
1

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
2 Section VI: Shock States
TABLE 57.1
DEFINITION OF SYSTEMIC INFLAMMATORYRESPONSE SYNDROME (SIRS)
Systemic inflammatory response syndrome (SIRS): Thesystemic inflammatory response to a wide variety of severeclinical insults manifests by two or more of the followingconditions:
■ Temperature >38◦C or <36◦C■ Heart rate >90 beats per minute (bpm)■ Respiratory rate >20 breaths per minute or PaCO2
AU: Need
Permission?<32 mm Hg
■ White blood cell count >12,000/μL, <4,000/μL, or 10%immature (band) forms
From Bone R. American College of Chest Physicians/Society ofCritical Care Medicine Consensus Conference: definitions for sepsisand organ failure and guidelines for the use of innovative therapies insepsis. Crit Care Med. 1992;20:864–874.
Standard abnormalities in an adult include mean arterial pres-sure (MAP) <60 mm Hg, systolic blood pressure <90 mm Hg,or a drop in drop in systolic blood pressure >40 mm Hg frombaseline.
Multiorgan Dysfunction Syndrome (MODS). The presence ofaltered organ function in an acutely ill patient, such that home-ostasis cannot be maintained without intervention. PrimaryMODS is the direct result of a well-defined insult in whichorgan dysfunction occurs early and can be directly attributableto the insult itself. Secondary MODS develops as a consequenceof a host response and is identified within the context of SIRS.
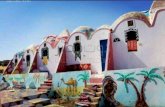
The relationship of many of these conditions to each otheris demonstrated in Figure 57.1. An understanding of sepsis def-Figure 57.1initions has become increasingly important since most clinicaltrials in the last two decades have used the modified version ofthe 1991 sepsis definitions (usually requiring three rather thantwo SIRS criteria) in their entry criteria. The concept of a com-pensatory anti-inflammatory response has also been introducedafter the demonstration that traditional anti-inflammatory me-diators were also elevated during sepsis (14).
EPIDEMIOLOGY
Although the sepsis syndromes (from sepsis to septic shock)have been a major burden on human health in both the de-veloped and undeveloped world, there has been a surprisingdearth of epidemiologic information. In North America, thishas been caused by the earlier lack of consensus definitions ofthese syndromes and, more recently, the absence of syndrome-specific diagnostic codes for sepsis within the InternationalClassification of Disease (ICD) coding system. In the last 20years, the development of consensus definitions and applica-tion of computerized hospital and government administrativedatabases has allowed substantial insight into the problem.
Martin et al. (5) have estimated 660,000 annual cases of sep-sis in the United States during 2000 (adjusted rate 240/100,000population) using an analysis of ICD-9 codes associated withNational Hospital Discharge Survey data. With the exceptionof a single major study with much higher values (1), estimates
TABLE 57.2
REVISED DIAGNOSTIC CRITERIA FOR SEPSIS
Infection,a documented or suspected, and some of thefollowing:b
General variablesFever (core temerpature >38.3◦C)Hypothermia (core temperature <36◦C)Heart rate >90 min or >2 SD above the normal value for
ageTachypneaAltered mental statusSignificant edema or positive fluid balance (>20 mL/kg
over 24 h)Hyperglycemia (plasma glucose >120 mg/dL or
7.7 mmol/L) in the absence of diabetesInflammatory variables
Leukocytosis (WBC count >12,000 μL)Leukopenia (WBC count <4,000 μL)Normal WBC count with >10% immature formsPlasma C-reactive protein >2 SD above the normal valuePlasma procalcitonin >2 SD above the normal value
Hemodynamic variablesArterial hypotensionb (SBP <90 mm Hg, MAP <70, or an
SBP decrease >40 mm Hg in adults or <2 SD belownormal for age)
SvO2 >70%Cardiac index >3.5 L/min/m2
Organ dysfunction variablesArterial hypoxemia (PaO2/FiO2 <300)Acute oliguria (urine output <0.5 mL/kg/h or 45 mmol/L
for ≥2 h)Creatinine increase >0.5 mg/dLCoagulation abnormalities (INR >1.5 or aPTT >60 s)Ileus (absent bowel sounds)Thrombocytopenia (platelet count <100,000 μL)Hyperbilirubinemia (plasma total bilirubin >4 mg/dL or
70 mmol/L)Tissue perfusion variables
Hyperlactatemia (>1 mmol/L)Decreased capillary refill or mottling
WBC, white blood cell; SBP, systolic blood pressure; MAP, meanarterial blood pressure; SvO2, mixed venous oxygen saturation; INR,international normalized ratio; aPTT, activated partial thromboplastintime.a Infection defined as a pathologic process induced by amicro-organism.bSvO2 sat >70% is normal in children (normally, 75%–80%), and CI3.5–5.5 is normal in children; therefore, neither should be used assigns of sepsis in newborns or children.cDiagnostic criteria for sepsis in the pediatric population are signs andsymptoms of inflammation plus infection with hyperthermia orhypothermia (rectal temperature >38.5◦C or <35◦C), tachycardia(may be absent in hypothermic patients), and at least one of thefollowing indications of altered organ function: Altered mental status,hypoxemia, increased serum lactate level, or bounding pulses.From Levy MM, Fink MP, Marshall JC, et al. 2001SCCM/ESICM/ACCP/ATS/SIS International Sepsis DefinitionsConference. Crit Care Med. 2003;31(4):1250–1256.
AU: Please add
c in table or
delete note.
for severe sepsis from sites across North American and Eu-rope have been fairly consistent at 50 to 80/100,000 popula-tion (15–19). These cases account for approximately 10% to15% of all intensive care unit (ICU) admissions (16,17,19–21).Approximately 25% of cases of sepsis (22) and 50% to 75%of cases of severe sepsis progress to septic shock (20). Septic

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 3
Trauma
Infection
SepsisBurns
SIRS
Severe sepsis
Septic shock
Pancreatitis
Post-pump syndrome
FIGURE 57.1. Venn diagram showing the relationship between infec-AU: Order
of
(unnumbered)
hardcopy Figs.
often does not
appear to
match leg-
ends,although
some Figs. do
appear to
match text Fig.
callouts and
descriptions.
Please check all
for match.
tion and other sepsis-associated terms. The intersection of systemicinflammatory response syndrome (SIRS) and infection defines sepsis.Severe sepsis is a subset of sepsis defined by the presence of organ fail-ure. Septic shock is a subset of severe sepsis in which the organ failure iscardiovascular (i.e., shock). Patients with certain inflammatory condi-tions (e.g., extensive burn injury, pancreatitis, major trauma, postpumpsyndrome, and so on) may demonstrate a “septic” appearance withoutthe presence of infection required for a diagnosis of sepsis. (Adaptedfrom Bone R. American College of Chest Physicians/Society of CriticalCare Medicine Consensus Conference: definitions for sepsis and organfailure and guidelines for the use of innovative therapies in sepsis. CritCare Med. 1992;20:864–874.)
shock represents between 5% and 8% of all ICU admissions(21,23). In the United States, the cost of sepsis and severe sepsisranges from $22,000 to $60,000 per episode at a total cost ofapproximately $17 billion annually (1,24). Sepsis and relatedconditions are the tenth leading cause of death in the UnitedStates (6).
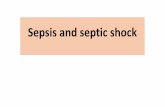
The incidence of sepsis appears to be increasing at a rate ofabout 9% per year in the United States (5) (Fig. 57.2). ReasonsFigure 57.2for this increase include the following: (a) An aging populationwith increased predisposition to illness; (b) increased propor-tion and longevity of the subpopulation with conditions thatpredispose to systemic infection including chronic organ failure(e.g., cirrhosis, renal failure, cardiomyopathy, chronic obstruc-tive pulmonary disease [COPD]), and other conditions (e.g.,diabetes, cancer, AIDS, etc.); (c) extensive use of invasive di-
agnostic and therapeutic modalities (indwelling catheters anddevices), which lead to breakdown of native resistance to infec-tion; and (d) widespread use of immunosuppressive chemother-apies for a wide range of diseases (asthma, inflammatory boweldisease, rheumatoid arthritis, systemic lupus erythematosus,and other autoimmune diseases).
Age is a substantial risk factor for sepsis, severe sepsis, andseptic shock (1,5,25). Patients older than the age of 65 years areapproximately 13-fold more likely to develop sepsis comparedto others (5). Similarly, septic shock is 18 times more likely inthe >80-year age group compared to those in the 20- to 29-year age group (23). Given that the average age of the NorthAmerican population is increasing, and that the incidence of allthe sepsis-related syndromes is markedly elevated in the elderly(23), the fact that the average age of patients with sepsis hasclimbed over the last few decades can be no surprise (1,5). Thefact that septic shock is substantially a geriatric illness is re-flected in the median age of 67 years (25). The persistent 60:40male:female preponderance in sepsis, severe sepsis, and septicshock may have its origins in men’s increased predisposition tosmoking-associated cases of pneumonia and peptic ulcer dis-ease/gastrointestinal malignancy-associated gastric and bowelperforation (1,5,17,20,22,23). Nonwhite racial groups are alsoat substantially increased risk, particularly African Americans(5). However, low socioeconomic status is a substantial riskfactor for septic shock (a fourfold increased risk in the low-est quintile of income compared to any other quintile) (23). Inthis context, it is unclear whether race may be relevant onlyas a marker of socioeconomic status. Comorbidities are com-mon in patients with sepsis, as might be expected given anaverage age of 55 to 65 years for sepsis and perhaps higherfor septic shock (5,19,25–29). Diabetes, COPD, renal failure,congestive heart failure, and malignancy can each be found in10% to 20% of patients with sepsis or septic shock. At least50% of patients with severe sepsis have at least one major med-ical comorbidity (5). Patients with septic shock have an evenhigher incidence (>90%) of major comorbidities. Alcoholismand substance abuse also substantially increases the risk of sep-sis, as well as death from sepsis and septic shock (30).
As might be expected, mortality increases with the severityof the septic syndrome. Mortality is <15% for sepsis, 25% to50% for severe sepsis, and >50% for septic shock (1,5,15–17,20–22,25,31). This mortality rate for septic shock, whilestaggering, nevertheless represents an improvement in survival
225,000
150,000
75,000
25,000
15,000
10,000
5,000
No
. of
case
s o
f se
psi
s
01979 1981 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001
Gram-negative bacteriaGram-positive bacteriaFungi
FIGURE 57.2. Incidence of sepsis in the UnitedStates stratified by organism group. The incidence ofsepsis increased approximately 9% per year between1979 and 2001 with the greatest relative increase infungal infections. In addition, as of the late 1980s,Gram-positive pathogens became numerically dom-inant over Gram-negative organisms. (From Mar-tin GS, Mannino DM, Eaton S, et al. The epi-demiology of sepsis in the United States from 1979through 2000. N Engl J Med. 2003;348(16):1546–1554, with permission.)

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
4 Section VI: Shock States
from 35 years ago when mortality rates frequently exceeded80% (32,33). Early septic mortality (<3 days) appears to be as-sociated most closely with shock and with other deaths withinthe first week due to multiple organ failure. Later deaths tendto be most closely associated with pre-existing comorbidities(34). Of those succumbing to septic shock, approximately 75%are early deaths (within 1 week of shock), primarily due to hy-perdynamic circulatory failure (35).
Throughout recorded history, there has been an evolution ofthe organisms that cause infectious diseases and the associatedclinical syndromes. This phenomenon has become particularlypronounced since the advent of antibiotics in the last half of theprevious century. By the 1960s and 70s, Gram-negative organ-isms had become the dominant pathogens over Staphylococcusaureus and streptococci. During the 1980s, resistant Gram-positive organisms (methicillin-resistant S. aureus, coagulase-negative staphylococci, penicillin-resistant S. pneumoniae, andenterococci) again re-emerged as major pathogens. Gram-positive cocci account for approximately 40% to 50% ofsingle isolates (excluding fungi) in sepsis and septic shock(20,25,31,36–38).
Most recently, yeast and other fungi have demonstrateda remarkable increase in their contribution to sepsis (5% oftotal) and septic shock (8.2% of total), with an increase ofabout 10% per year (5,25,37,38). Candida albicans remainsnumerically dominant (about 60% of total fungal infections),but fluconazole-resistant yeasts are the most rapidly increas-ing species (39–41). Other major concerns in recent years in-clude the emergence of vancomycin-resistant enterococci (42),extended spectrum β-lactamase (ESBL) resistance in Gram-negative organisms (reliably sensitive only to carbapenems)(43), and an endemic strain of virulent, methicillin-resistantS. aureus in the community (44). In addition, concerns regard-ing sporadic cases of vancomycin-resistant S. aureus (VRSA)are growing (45).
PATHOGENESIS OFSEPSIS, SEVERE SEPSIS,
AND SEPTIC SHOCK
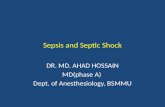
Sepsis and septic shock or sepsis-associated multiple organ fail-ure typically begin with a nidus of infection within the body(e.g., pneumonia, peritonitis, urinary tract infection, abscess).Within that nidus, the organism replicates. Eventually, the in-fection at the inciting focus releases sufficient microbial anti-gens to elicit a systemic inflammatory response designed toeliminate the invading microbes (Fig. 57.3). Many constitu-Figure 57.3tive and/or inducible elements of invasive micro-organisms arecapable of inciting the systemic inflammatory responses thatresult in sepsis and septic shock (Fig. 57.3, Table 57.3). Be-Table 57.3yond endotoxin (lipopolysaccharide; LPS) of Gram-negativebacteria, other major triggers of the systemic inflammatory re-sponse characteristic of sepsis include various exotoxins (allbacteria), peptidoglycans (streptococci), and teichoic acid (S.aureus); lipoarabinomannan of mycobacteria; and mannopro-teins and beta-glucan of fungi (46). Bacterial DNA may possesssufficient antigenic properties (based on unique CG repetitionsand lack of deoxyribonucleic acid [DNA] methylation) to ini-tiate a substantial inflammatory response independent of otherbacterial elements (47–49). Bacterial ribonucleic acid (RNA)
may be able to do the same (50). Recent investigations suggesta surprising commonality of signaling mechanisms in septicshock via Toll-like receptors from a broad range of etiologicagents (48,51–54).
Despite the large number of potential elements of patho-genic micro-organisms that can drive the septic response, endo-toxin of Gram-negative bacteria remains the prototype of suchfactors and the model for subsequent research. This antigen isthought to be central in initiating the powerful host responseduring infection with these organisms (55). LPS and other anti-gens interact with immune cells (particularly macrophages), re-sulting in the induction of proinflammatory cytokines such astumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β) se-creted by monocytes, macrophages, and other cells (Fig. 57.3)(56). These cytokines initiate a complex signaling sequence in-volving the release of secondary mediators (platelet-activatingfactor, leukotrienes, prostaglandins), and monocytes, as wellas endothelial tissue factor expression, inducible nitric oxidesynthetase induction, microvascular coagulation, cell-adhesionmolecule up-regulation, and apoptosis (57–60). To maintainhomeostasis (and likely as part of a feedback mechanism), sev-eral anti-inflammatory mediators are also released, includinginterleukin-10 (IL-10), transforming growth factor-β (TGFβ),and interleukin-1 receptor antagonist (IL-1ra). If homeostasiscannot be maintained, progressive and sequential dysfunctionof various organ systems (i.e., MODS) may occur. If the inflam-matory stimulus is particularly intense, or if there is limitedcardiovascular reserve, effects on the cardiovascular system asmanifested by septic shock may dominate the clinical presen-tation.
Microbial Antigen Signaling
As the prototypical and best-studied microbial antigen, an un-derstanding of the signaling cascade of endotoxin is instruc-tive. Endotoxin is an amphiphilic macromolecule located onthe outer cell wall membrane of Gram-negative bacteria. It iscomposed of lipid A, a diglucosamine-based acylated phospho-lipid, and a polysaccharide side chain (61,62) (Fig. 57.4). The Figure 57.4polysaccharide chain is composed of a short, highly conserved,proximal section (core polysaccharide) and a highly variable,longer distal oligosaccharide side chain. The core polysaccha-ride and lipid A are sometimes referred to as the core glycol-ipid. The highly conserved lipid A moiety is the toxic elementof endotoxin and can reproduce the manifestations of endo-toxic shock when administered alone (62–67). As a circulatingform in the plasma, endotoxin exists in a multimeric aggregateform.
Lipopolysaccharide-binding protein (LBP) is an acute phasereactant protein present in plasma (61,68,69). The levels in-crease with inflammatory stimulation. LBP catalyzes the trans-fer of endotoxin from serum aggregates to either serum lipopro-teins such as high-density lipoprotein (HDL), leading to endo-toxin neutralization or to CD14 receptors (either membrane-bound [mCD14] or soluble [sCD14]), the putative primary LPSreceptor (Fig. 57.5). The degree to which endotoxin is shunted Figure 57.5through either pathway appears to play a significant role inthe phenotypic physiologic response (46). LBP, by forming acomplex with endotoxin monomers, appears to enhance theability of endotoxin to bind CD14 and allows cellular ac-tivation at relatively low endotoxin concentrations (61,69).

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 5
Nidus of InfectionAbscessPneumoniaPeritonitisPyelonephritisCellulitis
Organism
ExotoxinTSST-1Toxin-A
Structural ComponentTeichoic Acid AntigenPeptidoglycan, Endotoxin (LPS)Bacterial DNA
Gut release of endotoxin
Plasma
-Extrinsic/intrinsic pathways-Protein C; S-TFPI-ATIII
Complement Kinins
Coagulation
Monocyte-Macrophage
-Tumor necrosis factor-Interleukins-Interferons-TGF-MIF-HMGB1
Cytokines
Platelet Activating FactorNitric Oxide
Endothelial Cells
Selectins, IcamsRenin-angiotensin systemProstaglandinsLeukotrienesProstacyclinThromboxaneEndothelin
Neutrophils
LysosomesOxygen free radicals (superoxides)Granulocyte Colony Stimulating Factor (G-CSF)
Cellular Dysfunction
Vasculature-Vasodilation-Vasoconstriction-Leukocyte aggregation-Endothelial cell dysfunction
Cellular Dysfunction
Organs-Dysfunction-Metabolic abnormalities
Myocardium-Depression-Dilatation
Shock
Refractory Hypotension Multiple Organ Dysfunction Recovery
Death
Nucleus
LysosomeMitochondriaActin/Myosin
Membranechannel
Membranereceptor
FIGURE 57.3. Pathogenesis of sepsis and septic shock. ATIII, antithrombin III; DNA, deoxyribonucleicacid; HMGB1, high mobility group box 1 protein; LPS, lipopolysaccharide; MIF, macrophage migra-tion inhibitory factor; TFPI, tissue factor pathway inhibitor; TGF, transforming growth factor; Toxin A,Pseudomonas toxin A; TSST-1, toxic shock syndrome toxin 1. (Adapted from Parrillo JE. Pathogenicmechanisms of septic shock. N Engl J Med. 1993;328:1471–1477.)

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
6 Section VI: Shock States
TABLE 57.3
ELEMENTS OF MICRO-ORGANISMS CAPABLE OFINDUCING A SEPTIC RESPONSE
Micro-organism Component
Gram-negative bacteria LipopolysaccharidePeptidoglycanPorinsLipoproteinsLipopeptidesLipid A–associated proteinsPiliExotoxinsDNA/RNA
Gram-positive bacteria ExotoxinsPeptidoglycanLipoteichoic and teichoic acidsDNA/RNA
Mycobacteria LipoarabinomannanLipomannanMycolylarabinogalactan-
peptidoglycan
Fungi Mannoproteinsβ-glucan
Adapted from Heumann D, Glauser MP, Calandra T. Molecular basisof host-pathogen interaction in septic shock. Curr Opin Microbiol.1998; 1(1):49–55.
Although LBP appears to be a specific carrier molecule forendotoxin, available data suggest that other micro-organismtoxins associated with sepsis may use similar carrier proteins(70,71).
CD14, a glycoprotein receptor, is found primarily in thecells of the myelomonocytic lineage (monocytes, macrophages,polymorphonuclear leukocytes) (72). Although there appearto be several other membrane-associated LPS receptors,membrane-associated CD14 (mCD14) represents the only re-ceptor that is clearly involved in LPS binding and activation ofcellular inflammatory responses. In contrast to the low endo-toxin concentrations required to activate CD14 (an effect me-diated by the LBP-LPS interaction [73]), other receptors such
as CD18 appear to require exceptionally high concentrationsof LPS to elicit a cellular effect, suggesting a lack of physiologicrelevance (74).
Recent data suggest that CD14, far from being uniquely a re-ceptor for LPS, may also bind ligands from various pathogens,including peptidoglycan and lipoteichoic acid of Gram-positivebacteria, lipoarabinomannan of mycobacteria, and chitin offungi (Table 57.4) (46,75). In several of these, binding is serum Table 57.4dependent, suggesting the possibility of serum carrier/bindingproteins similar to LBP (70). This convergence of receptor-signaling mechanisms may explain why downstream intracel-lular signaling events (activation of NF-κB, MAP kinases, etc.)and cellular responses (cytotoxicity, cytokine generation, etc.)appear to be so highly conserved in sepsis due to different eti-ologic agents. Although elements of different micro-organismsbind and activate CD14, limited data suggest that the precisebinding sites vary.
Despite the importance of CD14, the receptor lacks the abil-ity to initiate intracellular signaling on its own because of thelack of an intracytoplasmic-signaling domain. CD14 signal-ing requires the involvement of the most recently discovered(and most central) element of microbial antigen-mediated sig-nal transduction, the Toll-like receptors (TLRs) (52,76–79).The original Toll receptor was initially described as an essentialcomponent of embryogenesis of Drosophila (80). In mammals,various TLRs have been shown to play a crucial role in therecognition of microbial antigens and initiation of the immuneresponse. TLR4 and, to a lesser extent, TLR2 have been im-plicated in signaling associated with endotoxin (53,77–79,81).TLR4 appears to be coexpressed and forms a plasma mem-brane complex with mCD14. mCD14 appears to bind withthe LPS/LBP complex to enable transfer to TLR4 and an ac-cessory protein MD-2 (82). mCD14, acting as a receptor forother non-LPS microbial antigens, also appears to have a rolein TLR2 signaling (83). The exact nature of the CD14-TLR in-teraction is as yet undetermined. However, interaction of CD14and TLR4 stimulates downstream activity of the intracellulardomain of TLR to generate NF-kB and other intracellular me-diators that drive the response to LPS (Fig. 57.5). Notably, theintracellular domain of the TLRs is shared with the IL-1 recep-tor. Several other TLR receptors are known to be involved inmicrobial antigen signaling from various pathogens, includingGram-positive and Gram-negative bacteria, fungi, mycobacte-ria, and viruses (Table 57.5). Table 57.5
Pili
Capsule(K antigen)
Outermembrane
Solidmembrane(peptidoglycan)
Flagellum(H antigen)
LPS (endotoxin: O antigen)
Oligosaccharideside chains
Core polysaccharide
Lipid A
Inner cytoplasmic membrane
FIGURE 57.4. Endotoxin (lipopolysaccharide). Endotoxinis a component of the cell wall of Gram-negative bacilli.(From Young LS, Martin WJ, Meyer RD, et al. Gram-negative rod bacteremia: microbiologic, immunologic, andtherapeutic considerations. Ann Intern Med. 1977;86:456–471, with permission.)

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 7
LPS
LPS
extra- cellular space
cytoplasm
nucleus
LBP
LBP
LPS LBP
Toll4 Toll4
MYD88
IRAK4 IRAK4
TRAF 6
NIK 1KKβ
1κB
NFκB 1κB
NFκB
MYD88
CD14
FIGURE 57.5. Endotoxin signalingpathway related to CD14 and TLR4(Toll-like receptor 4). IκB, inhibi-tory κB; IKK, IκB kinase; IRAK,IL-1R–associated kinase; LBP,lipopolysaccharide-binding protein;LPS, lipopolysaccharide; MYD88, ;
AU: Please
spell out
MYD88.
AU: Please
spell out TRAF
6.
NFκB, nuclear factor-κB; NIK, nuclearfactor κB–inducing kinase; TRAF 6,.
Besides the Toll-like receptor pathways, other importantroutes of microbial antigen signaling exist. In particular, someGram-positive organisms produce potent exotoxins that areimplicated in the pathogenesis of toxic shock syndromes. Theseinclude the toxic shock syndrome toxin-1 associated withstaphylococcal toxic shock and pyrogenic toxins predomi-nantly associated with group A streptococci. These exotoxinsappear to be superantigens in that they are able to activatebroad polyclonal groups of lymphocytes, resulting in massivecytokine generation and toxic shock (84,85).
Cytokines
The concept of a systemic inflammatory response syndrome(SIRS) has already been discussed in the context of sepsis.The notion of an innate anti-inflammatory response, termedcompensatory anti-inflammatory response syndrome (CARS),during sepsis also exists (14). This model suggests that a clin-ical insult (such as infection or injury) initiates a proinflam-
TABLE 57.4
CD14 BINDING-CAPABLE MICROBIAL PRODUCTS
Ligands Origin
Lipopolysaccharide Gram-negative bacteriaPeptidoglycan Gram-positive bacteriaLipoteichoic acid Gram-positive bacteriaLipoarabinomannan Mycobacterium tuberculosisRhamnose-glucose polymers Streptococcus speciesPolyuronic acids BacteriaAcylpolygalactoside Klebsiella pneumoniaeChitin YeastAmphiphilic molecules Staphylococcus aureus
matory response that is countered by an endogenous anti-inflammatory reaction. The aggregate responses produce en-dogenous circulating mediators (cytokines, soluble receptors,adhesion molecules, growth factors, eicosanoids, etc.), gener-ating systemic phenomena such as septic shock or immuno-suppression. Clinical manifestations and patient outcome aredependent on the balance between proinflammatory and anti-inflammatory elements. The predominance of the inflammatoryresponse corresponds to SIRS and may lead to cardiovascularcompromise, shock, and organ dysfunction. However, a pre-dominance of anti-inflammatory mediators produces a state ofimmune paralysis associated with a propensity to infection andinability to fight infection. Both may ultimately lead to death.In patients with sepsis, the duration of monocyte inactivation(a potential manifestation of CARS) correlates with mortality(86). If the counterinflammatory response is able to balance theinflammatory stimuli (while the infecting micro-organism is ef-fectively cleared), homeostasis is achieved and clinical recoverywill occur. In this model, sepsis has a dynamic nature based onthe development and balance of the above-described responses(Fig. 57.6). This interplay is influenced by the nature of the Figure 57.6inflammatory injury and the genetically determined variabilityof the host immune response (87,88).
Proinflammatory cytokines have multiple effects, includ-ing the stimulation of production and release of other proin-flammatory mediators. TNF-α, interleukin-1β (IL-1β), andinterleukin-6 (IL-6) are the best known proinflammatory cy-tokines and have overlapping and synergistic effects in stimu-lating the inflammatory cascade. The next phase in the cytokineresponse to infection is the endogenous counterinflammatorycascade in response to the systemic activity of proinflamma-tory cytokines. Cytokine inhibitors (e.g., IL-1 receptor antag-onist [IL-1ra], soluble TNF receptor) and anti-inflammatorycytokines (e.g., TGFβ, IL-4, IL-10, and IL-13) are involvedin this phase of the response. Other cytokines like HMGB1may be involved even later in the syndrome. Thus, the cy-tokine network in sepsis involves proinflammatory cytokines,

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
8 Section VI: Shock States
TABLE 57.5
MICROBIAL LIGANDS OF THE TOLL-LIKE RECEPTORS (TLRS)
Receptor Microbial ligands Origin
TLR1 Triacyl lipopeptidesSoluble factors
Mycobacteria, bacteriaN. meningitidis
TLR2 Peptidoglycan and LTA Gram-positive bacteriaLipoprotein/lipopeptide Gram-positive bacteriaAtypical LPS Leptospira interrogans and
Porphyromonas gingivalisLipoarabinomannan, cell wall
and lipoproteins/lipopeptidesMycobacteria
Lipoproteins/lipopeptides Borrelia burgdorferiGlycolipids and lipoproteins/ Treponema spp.
lipopeptidesLipoproteins and lipopeptides Mycoplasma spp.Phenol-soluble modulin S. aureusCell wall S. pneumoniaeSoluble factor Group B streptococciPorins Neisseria meningitidisZymosan YeastHeat shock protein Human protein
TLR3 dsRNA Virus
TLR4 LPS Gram-negative bacteriaLTA Gram-positive bacteriaHeat-sensitive compound MycobacteriaHeat shock protein Chlamydia pneumoniaeFusion protein Respiratory syncytial virusGlycolipids Treponema brennaborenseHeat shock protein Human proteinHeat shock protein Human protein
TLR5 Flagellin Bacteria with flagella
TLR6 Diacyl lipopeptides MycoplasmaLipoteichoic acid Gram-positive bacteriaZymosan Fungi
TLR7 ssRNA Virus
TLR8 ssRNA Virus
TLR9 CpG DNA Bacteria
TLR10 Unknown Unknown
TLR11 Unknown Unknown
LTA, lipoteichoic acid; LPS, lipopolysaccharide; dsRNA, double-stranded RNA; ssRNA, single-stranded RNA.Adapted from Leaver SK, Finney SJ, Burke-Gaffney A, et al. Sepsis since the discovery of Toll-like receptors: disease conceptsand therapeutic opportunities. Crit Care Med. 2007;35(5):1404–1410; and Van Amersfoort ES, Van Berkel TJ, Kuiper J, et al.Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clin Micro Rev. 2003;16(3):379–414.
anti-inflammatory cytokines, and cytokine inhibitors (Table57.6). It is the balance between these cytokines at different timeTable 57.6points that determine the clinical manifestations and outcomeof sepsis.
Nitric Oxide
Another important mediator, nitric oxide (NO), has a vital rolein normal intracellular signal transduction (89). NO is synthe-sized by a family of enzymes called NO synthases (NOS) thatincorporate nitrogen from one of the guanidine terminals of L-
arginine with molecular oxygen to form NO and L-citrulline.Three distinct nitric oxide synthases have been purified, cloned,and characterized: (i) Neuronal NOS or nNOS, (ii) inducibleNOS or iNOS, and (iii) endothelial NOS or eNOS, reflectingthe cell types from which they were originally identified.
NO has several important roles in infection, sepsis, and sep-tic shock. The iNOS gene is induced in immunoactivated cells.NO formed by these cells plays a role in host defense againstbacterial, viral, and protozoan infections. Of particular impor-tance in relation to septic shock, nitric oxide is the mediatorthrough which endothelial cells normally cause relaxation ofadjacent smooth muscle (89). Endothelial cells, through eNOS,

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 9
Recovery
Time
INS
UL
T
OrganInjury
SIRS Pro-inflammatory
CARS Anti-inflammatory
FIGURE 57.6. The dynamic cytokine inflammatory response. Sep-sis is associated with an early transient dominance of proinflamma-tory cytokines corresponding to the systemic inflammatory responsesyndrome (SIRS) and the onset of organ damage. After this initialphase, the anti-inflammatory pathways of CARS (compensatory anti-inflammatory response syndrome) become active with the developmentof a refractory state characterized by a decreased capacity of mononu-clear cells to produce proinflammatory cytokines. Recovery occurs ifhomeostasis is re-established (Adapted from van der Poll T, van De-venter SJ. Cytokines and anticytokines in the pathogenesis of sepsis.Infect Dis Clin North Am. 1999;13(2):413–426.).
produce picomolar quantities of nitric oxide in response toseveral vasodilatory stimuli such as shear stress, acetylcholine,and bradykinin. This nitric oxide diffuses to adjacent smoothmuscle and activates guanylate cyclase to produce cyclic GMP,which effects vascular relaxation. Activity of endothelial NOSis regulated and is calcium and calmodulin dependent.
During septic shock, an iNOS capable of producingnanomolar quantities of nitric oxide is generated in endothe-lium and vascular smooth muscle (89,90). Following this gener-ation, the activity of this iNOS is unregulated and constant. Ni-tric oxide–mediated generation of cyclic guanosine monophos-phate (cGMP) explains the profound loss of arterial vascu-lar tone and venodilatation seen in septic shock (90,91) andmay, in part, explain the irreversible vascular collapse seen
late in hemorrhagic shock (92) (Fig. 57.7). A potential role Figure 57.7for NO in inflammation-associated edema and third-spacingduring shock has also been suggested (93). The in vitro my-ocardial depressant effects of TNF-α, IL-1β, and serum fromseptic humans may be mediated by a similar NO- and cGMP-dependent pathway (94,95). TNF-α, IL-1β, and IFN-γ havebeen identified as key mediators of iNOS activation. An al-ternative pathway by which NO may play a role in the car-diovascular pathophysiology of shock and sepsis involves theproduction of peroxynitrite (ONOO−), a highly reactive oxi-dant, from the interaction of superoxide (OH−) and nitric oxide(NO−) (96).
HEMOSTASIS
The coagulation cascade represents a highly conserved antimi-crobial defense mechanism common to even the most primitivecomplex organisms, such as the Limulus horseshoe crab. Thehemolymph of the horseshoe crab, one of the oldest complexorganisms still in existence, clots rapidly in response to minutequantities of endotoxin or beta-(1,3) glucan, a component offungi. Pathogens are immobilized in the clot, allowing subse-quent elimination (97,98). This commonality of purpose andfunction of the coagulation and inflammatory systems in elimi-nating invading microbes has persisted in evolution to present-day mammals including humans (99). These systems, in sharingcommon activation pathways, are inextricably linked.
Although both these systems are normally highly adaptive innature, excessive activity of the coagulation and inflammationpathways can result in vascular injury, aberrant tissue bloodflow, tissue damage, and, ultimately, organ dysfunction. Recentclinical and laboratory investigations have established that, inconjunction with the cytokine cascade, the coagulation systemplays a key role in inflammatory states such as sepsis (100–102)(Fig. 57.8). A critical process in sepsis-induced coagulopathy is Figure 57.8the activation of the extrinsic pathway (100).
During the normal hemostatic response, exposure of bloodto nonvascular cell-bound tissue factor in the subendotheliallayer initiates the extrinsic pathway through the binding of tis-sue factor to activated factor VII. The resulting enzyme com-plex, in turn, activates factor IX of the intrinsic pathway andfactor X of the common pathway. With factor V as a cofactor,
TABLE 57.6
MAJOR PROINFLAMMATORY AND ANTI-INFLAMMATORY CYTOKINES AND RECEPTORS IN SEPSIS
Proinflammatory cytokines Anti-inflammatory cytokines Cytokine inhibitors
Tumor necrosis factor-α (TNF-α) Transforming growth factor (TGF-β) Soluble TNF receptors- Type I-Type II
Interleukin-1β (IL-1β) Interleukin-4 (IL-4) Interleukin-1 receptorantagonist (IL-1ra)
Interleukin-2 (IL-2) Interleukin-6 (IL-6)Interleukin-6 (IL-6) Interleukin-8 (IL-8)Interleukin-12 (IL-12) Interleukin-9 (IL-9)Interferon-γ (IFN-γ ) Interleukin-10 (IL-10)Macrophage migration inhibitory factor (MIF) Interleukin-11 (IL-11)High mobility group 1 protein (HMG-1) Interleukin-13 (IL-13)

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
10 Section VI: Shock States
intravascular space
endothelium
vascular smooth muscle
extravascular space
TNFIL-1
H+ CO2
acetycholinebradykinin
PAFPGE2PG1
TNFIL-1
PGI1PGE2
PAF
macrophage
iNOScGMPcGMP
eNOSeNOS
loss ofloss ofvascular tonevascular tone
iNOS
NONO
OONOOONO--
FIGURE 57.7. Physiologic and pathophysiologic vasodilatoryfactors relevant in sepsis and septic shock. cGMP, cyclic GMP;eNOS, endothelial nitric oxide synthetase; IL-1, interleukin-1β; iNOS, inducible nitric oxide synthetase; NO, nitric oxide;ONOO−, peroxynitrite; PAF, platelet-activating factor; PGE2.prostaglandin E2; PGI2. prostacyclin; TNF, tumor necrosisfactor-α. (Adapted from Kumar A, Parrillo JE. Shock: patho-physiology, classification and approach to management. In: Par-rillo JE, Dellinger RP, eds. Critical Care Medicine: Principles ofDiagnosis and Management in the Adult. 3rd ed. St. Louis, MO:Mosby; 2007:379–422.)
activated factor X cleaves prothrombin to form thrombin.Thrombin then converts fibrinogen to fibrin, which results inclot formation (103).
In sepsis, however, the expression of tissue factor is eitherdirectly or indirectly induced by inflammatory cytokines. Over-expression of proinflammatory cytokines, such as TNF-α, IL-1β, and interleukin-8, are thought to upset the balance to-ward a procoagulant state (60,101,104) (Fig. 57.8). TNF-αand IL-1β, for example, can induce the expression of tissue fac-tor in circulating monocytes and endothelial cells (101). Thevascular endothelial injury resulting from inflammation canalso further expose tissue factor in subendothelial tissue andperivascular cells. Endothelial injury also inhibits the produc-tion and activity of anticoagulants such as proteins C and S, theheparin–antithrombin complex, and thrombomodulin. Loss ofnative anticoagulant function is indicated by decreased activityand circulating levels of protein C (105,106), antithrombin III,(ATIII) (101,106), and tissue factor pathway inhibitor (TFPI)(107,108) in patients with severe sepsis and septic shock.
Current evidence suggests that the pathogenesis of sepsisis associated with (a) systemic activation of coagulation re-
sulting in consumption of coagulant factors, (b) suppressionof the anticoagulant system by the same proinflammatory me-diators that activate coagulation, and (c) early activation fol-lowed by later suppression of fibrinolysis (60,101) (Fig. 57.8).Whereas the coagulation cascade is clearly activated in sep-sis, the specific inciting events and the molecular linkages be-tween inflammation and coagulation remain to be elucidated(60,101–103). Given observational studies demonstrating thedepletion of anticoagulant factors (decreased activity levels ofprotein C [60,102], ATIII [101,103], and TFPI [28]) in patientswith severe sepsis and septic shock, such markers may be usefulas markers of the presence or severity of sepsis in the future.
HOST GENETIC FACTORS
Although the characteristics of the pathogen have much to dowith the occurrence of clinical infection and progression tosepsis and septic shock, a growing body of data suggests thatgenomic variations between patients are equally important.These genomic variations in microbial and cell signaling, innate
Inflammatory Responseto Infection
Thrombotic Responseto Infection
Fibrinolytic Responseto Infection
Endothelium
TAFI
PAI-1
Suppressedfibrinolysis
Neutrophil
Monocyte
IL-6IL-1TNF-#
IL-6
Tissue Factor
Tissue Factor
COAGULATION CASCADE
Factor Va
Factor VIIIa
THROMBIN
FibrinFibrin clot
FIGURE 57.8. Cytokines induce the endothelial cellto shift from an antithrombotic to a prothromboticphenotype. Expression of tissue factor by mono-cytes, and perhaps a subset of endothelial cells, initi-ates coagulation through the extrinsic system in pa-tients with severe sepsis and septic shock. At thesame time, fibrinolysis is inhibited through the releaseof thrombin-activatable fibrinolysis inhibitor (TAFI)and plasminogen activator inhibitor-1 (PAI-1). IL-1, interleukin-1β; IL-6, interleukin-6; TNF-α, tumornecrosis factor-α. (Adapted from Bernard GR, Vin-cent JL, Laterre PF. Efficacy and safety of recombi-nant human activated protein C for severe sepsis. NEngl J Med. 2001;344:699–709.)

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 11
TABLE 57.7
HUMAN GENETIC MARKERS ASSOCIATED WITH RISK OF INFECTION ANDSEPSIS/SEPTIC SHOCK
Gene product group/Gene product Infection/sepsis association
Pattern Recognition ReceptorsTLR2 ■ Tuberculosis
■ Life-threatening bacterial infections■ S. aureus infections
TLR4 ■ Gram-negative infection■ Septic shock
TLR5 ■ Legionella infectionCD14 ■ Septic shock and septic shock mortality
■ Isolation of pathogenic bacteria in infectionMannose-binding lectin ■ Bacterial infections
■ Isolation of pathogenic bacteria in infection
Intracellular ProteinsIRAK4 ■ Recurrent Gram-positive infections
CytokinesTNF-α ■ Sepsis, septic shock, septic mortality
■ Meningococcal mortalityTNF-β ■ Sepsis and septic mortalityIL-6 ■ Septic mortalityIL-10 ■ Sepsis and septic mortality
■ CAP severity and mortality■ Pneumococcal septic shock
IFNγ ■ InfectionMIF ■ Sepsis and sepsis-induced acute lung injuryIL-1Ra ■ Sepsis and septic mortality
Coagulation FactorsPAI-1 ■ Meningococcal sepsis, septic shock, septic mortality,
vascular complications■ Septic mortality
Protein C ■ Septic organ dysfunction and mortalityTAFI ■ Meningococcal and septic mortalityFibrinogen-β ■ Septic mortalityFactor 5 (Leiden) ■ Septic mortality, pressor use, purpura fulminans
TLR, Toll-like receptor;Adapted from Arcaroli J, Fessler MB, Abraham E, et al. Genetic polymorphisms and sepsis. Shock.2005;24(4):300–312; Lin MT, Albertson TE, Lin MT, et al. Genomic polymorphisms in sepsis. Crit CareMed. 2004;32(2):569–579; Texereau J, Pene F, Chiche JD, et al. Importance of hemostatic genepolymorphisms for susceptibility to and outcome of severe sepsis. Crit Care Med. 2004;32(5Suppl):S313–S319; and Papathanassoglou ED, Giannakopoulou MD, Bozas E, et al. Genomic variations
AU: Please
define all other
abbreviations/
acronyms used
in the table per
this format. and susceptibility to sepsis. AACN Adv Crit Care. 2006;17(4):394–422.
immunity, and coagulation and inflammatory stress cytokineresponses appear to explain individual variations in suscepti-bility to infection, sepsis/septic shock, and septic death. Theylikely explain why identical organisms cause fulminant diseasewith septic shock in some but only minimal clinical illness inothers. The importance of inheritable elements in susceptibilityand mortality risk of life-threatening infections is demonstratedby adopted twin studies which demonstrated remarkable con-vergence in the causes of death (including sepsis/infection) ofsuch individuals (109).
The advent of complete gene mapping via high throughputanalysis techniques (e.g., microarray gene chips, etc.) have re-sulted in a rapid expansion of the list of human genetic markersassociated with risk of infection, sepsis/septic shock, and death.These markers fall into several broad groups, including those
involved with microbial ligand binding, intracellular signaling,cytokine generation, and coagulation factor generation/activityas described in Table 57.7. It should be noted that some genetic Table 57.7polymorphisms may be linked to other genetic loci. An asso-ciation between a given polymorphism and susceptibility toinfection, sepsis, septic shock, or septic death does not alwaysimply a direct causal relationship.
BIOENERGETIC FAILURE
The underlying metabolic defect in sepsis and septic shock hasbeen the source of substantial controversy over the last 30years. Most forms of shock are associated with low cardiacoutput (CO) and tissue hypoperfusion leading to overt tissue

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
12 Section VI: Shock States
Normal Sepsis
TissueMicrovascular
Bed
ArterialFlow
flowN
normalmetabolic
VenousFlow
demand
TissueMicrovascular
Bed
normal or ↑metabolic
MVO2N
lactate
VenousFlow
MVO2
lactateN
MVO2
lactate
demandnutrientcapillary
non-nutrientcapillary
(not visible)
no flow
ArterialFlow
nutrientcapillary
non-nutrientcapillary(visible)
↑ flow
↓ flow
MVO2
lactate
N
N
FIGURE 57.9. Microanatomic shunting in sepsis and septic shock. One explanation of the increasedlactatic acidosis and MvO2 found in septic shock is the potential presence of opening of nonnutrientblood vessels between the arterial and venous vascular beds. MvO2, mixed venous oxygen saturation.
ischemia. This results in anaerobic glycolysis with intracellu-lar acidosis, increased lactate, and high-energy phosphate de-pletion in the affected tissues. Blood oxygen extraction ratio(the ratio of oxygen to maintain normal oxygen consumption.During septic shock, the same tissue metabolic phenomenon ofintracellular acidosis and increased lactate production is noted.However, cardiac output and total tissue perfusion is typicallyincreased, and the oxygen extraction ratio falls. The explana-tion for tissue acidosis and lactate production in septic shockin the presence of tissue hyperperfusion is unknown.
Loss of vascular autoregulatory control may explain someof the typical metabolic findings of sepsis and septic shock. Anearly theory postulated the existence of microanatomic shunts
between the arterial and venous circulations (110) (Fig. 57.9). Figure 57.9During sepsis, these shunts were said to result in decreased sys-temic vascular resistance (SVR) and increased mixed venousoxygen saturation (MvO2) (111). The resultant decrease in per-fusion to tissue beds with normal or even increased metabolicdemand could generate tissue ischemia and lactic acid. How-ever, whereas microanatomic shunting has been noted inlocalized areas of inflammation, systemic evidence of this phe-nomenon in sepsis and septic shock is lacking (111–115). An-other theory involving “functional” shunting due to defectsof microcirculatory regulation in sepsis has also been pro-posed (Fig. 57.10) (116,117). Overperfusion of tissues with Figure57.10low metabolic requirements would result in increased MvO2
Normal
Tissue Microvascular
Bed
Tissue Microvascular
Bed
ArterialFlow
flowN
flowN
high metabolic
high metabolic
low metabolic
MVO2N
lactateN
VenousFlow
MVO2N
lactateN
demand
demand
ArterialFlow
flow
flow
low metabolic
MVO2N
lactate
VenousFlow
MVO2
lactateN
MVO2
lactate
demand
demand
MVO2N
lactateN
Sepsis
FIGURE 57.10. Functional shunting in sepsis and septic shock. Loss of ability to appropriately regulatemicrovascular flow according to tissue metabolic demand can lead to overperfusion of low-metabolic-demand tissue beds resulting in increased MvO2 (mixed venous oxygen saturation). Underperfusion ofhigh-metabolic-demand beds can result in tissue ischemia, anaerobic metabolism, and lactic acidosis.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 13
and narrowing of the arteriovenous oxygen content differ-ence. The relative vasoconstriction of vessels supplying moremetabolically active tissues would result in tissue hypoxia andlactate production due to anaerobic metabolism. Observationsthat some capillary beds may be occluded by platelet microag-gregates, leukocytes, fibrin deposits, and endothelial damagesupport this theory (112,116,118). Additional support comesfrom studies that demonstrate evidence of supply-dependentoxygen consumption in sepsis (119–123). Both of these theo-ries of the metabolic defect of energy metabolism in sepsis andseptic shock fall within the category of “stagnant” hypoxia asdescribed by Barcroft in 1920 (124).
A third theory of the metabolic presentation of sepsis andseptic shock suggests that circulating mediators cause an intra-cellular metabolic defect involving substrate use. This resultsin bioenergetic failure with high-energy phosphate (adenosinetriphosphate [ATP] and phosphocreatine) depletion and lactateproduction (125–127). Increased mixed venous oxygen satura-tion could then be explained by perfusion, which is maintainedin excess of tissue oxygen use capability. This phenomenon hasbeen termed histotoxic (124) or cytopathic (127) hypoxia. Po-tential mechanisms to explain this form of hypoxia include im-pairment/ inactivation of pyruvate dehydrogenase; nitric oxideor peroxynitrite-mediated inhibition of mitochondrial respi-ration; uncoupling of oxidative phosphorylation or activationof poly-(ADP-ribosyl)-polymerase (PARP) (127). Observationsdemonstrating preservation of tissue PO2 (128), absence of tis-sue hypoxia (129), and impairment of mitochondrial function(127,130–132) during sepsis and septic shock support this pos-sibility.
In particular, near-infrared spectroscopy (NIRS) has beenused to examine the issue of mitochondrial function in a pri-mate model of septic shock using live Escherichia coli infusion.NIRS demonstrated the presence of mitochondrial dysfunc-tion in skeletal muscle in animals with experimentally inducedsepsis. This was manifested by the impairment of oxidationof cytochrome a,a3 with reperfusion after transient ischemiain septic animals compared to controls (131). Another pri-mate study demonstrated early disturbance of mitochondrialredox state in skeletal muscle and brain in the presence of liveE. coli bacteremia. Of note, these changes occurred before theonset of overt hemodynamic alterations (133). In a limited ob-servational study, uncoupling of tissue oxyhemoglobin levelsand mitochondrial oxygen consumption, as indicated by cy-tochrome a,a3 redox state (indicating mitochondrial oxidativestress), predicted the development of multiple organ failure inpatients with major trauma (134). These data particularly sup-port the possibility of a decreased ability of mitochondria touse oxygen as a potential cause of decreased tissue high-energyphosphate in sepsis.
All these theories of septic bioenergetic metabolism wouldbe expected to result in a deficit of tissue high-energy phos-phates during septic shock. A series of studies using biochem-ical analysis of harvested tissues and nuclear magnetic reso-nance (NMR) spectroscopy of septic animals have suggestedthat high-energy phosphate reserves are decreased in animalmodels of septic or endotoxic shock (125,135,136). It canbe argued that in many of these studies, animals were inad-equately fluid resuscitated, which resulted in tissue hypoperfu-sion. However, animals in at least one study (125) were clearlyadequately resuscitated (cardiac output and tissue oxygen ten-sion were maintained comparable to shams) and demonstrated
similar evidence of high-energy phosphate depletion (skeletalmuscle biopsy) along with an increased lactate/pyruvate ratioduring rat peritonitis induced by cecal ligation and perfora-tion (125). Little human data exist. In one study of criticallyill patients (most of whom were septic), the acetoacetate/β-hydroxybutyrate ratio (a marker of mitochondrial redox state)rose significantly in nonsurvivors compared to survivors (137).Evidence of increased acetoacetate/β-hydroxybutyrate ratioalong with an increase in ATP degradation products in criti-cally ill patients with sepsis also exists (138,139). In addition,independent studies using skeletal muscle biopsies in patientswith sepsis/septic shock observed decreased ATP and phospho-creatine but variable changes in lactate levels in the skeletalmuscle of patients with septic shock (140,141).
In contrast, other animal studies using NMR spectroscopydemonstrate that high-energy phosphates are not depleted inseptic animals as would be expected in these theories of sep-tic bioenergetic failure (142–144). According to these andother studies, cellular ischemia is not the dominant factor inmetabolic dysfunction in sepsis (129,142–147). Rather, circu-lating mediators may result in cellular dysfunction, aerobic gly-colysis, and lactate production in the absence of global ischemia(143). This position is weakened by data suggesting that in-creased lactate in septic shock is also associated with decreasedpH (which would not be expected in aerobic glycolysis) (143).Nonetheless, ongoing controversy of this issue remains.
Cardiac and Vascular Responses
Prior to the introduction of the balloon-tipped pulmonaryartery catheter (PAC) and echocardiography to assess cardio-vascular performance, much of our understanding of septichemodynamics was based on clinical findings. Two distinctclinical presentations of septic shock were proposed: Warmshock characterized with high CO, warm dry skin, boundingpulses and hypotension; and cold shock characterized with lowCO, cold clammy skin, and diminished pulses (148). These twopresentations were thought to represent a progressive contin-uum, starting with warm shock (in the initial hemodynami-cally well-compensated phase) and progressing to cold shock(indicating decompensation), culminating in death. This no-tion was supported by studies showing a correlation betweensurvival and a high cardiac index (CI) (148,149). A major prob-lem with this interpretation was that these studies used centralvenous pressure (CVP) as a reflection of left ventricular end-diastolic volume (LVEDV) and adequacy of fluid resuscitation.The central role of adequacy of intravascular volume statusto CI and survival was suggested in a handful of studies atthat time (150,151). Based on evidence collected over the pastfour decades, CVP is now accepted to be a poor measure ofpreload in critically ill patients, particularly those with sep-sis and septic shock (152). Studies in recent years have clearlyshown that adequately resuscitated septic shock patients typ-ically exhibit a persistent hyperdynamic state, high CO, andlow SVR (153,154). In nonsurvivors, this hyperdynamic stateusually persists until death (Fig. 57.11) (35,155). Figure
57.11More than any other form of shock, distributive and, partic-ularly, septic shock involves substantial elements of the hemo-dynamic characteristics of other shock categories. All formsof distributive shock involve decreased mean peripheral vascu-lar resistance. Before fluid resuscitation, distributive shock also

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
14 Section VI: Shock States
1
0
2
5
6
Ca
rdia
c In
de
x (L
/min
/m2
)
3
4
1 2 4 7 10 1 2 4 7 10
Time (days)
7
SurvivorsNonsurvivorsAll Patients
FIGURE 57.11. Cardiac index in resuscitated septic shock. The mean(standard error of the mean [SEM]) cardiac index plotted against timefor all patients, survivors, and nonsurvivors. The hatched areas showthe normal range. All groups maintained an elevated cardiac indexthroughout the study period. The difference between the survivors andnonsurvivors was not statistically significant. Open circles, survivors;closed circles, nonsurvivors. (Adapted from Parker MM, ShelhamerJH, Bacharach SL, et al. Profound but reversible myocardial depressionin patients with septic shock. Ann Intern Med. 1984;100:483–490.)
involves a hypovolemic component with decreased central ve-nous and pulmonary artery occlusion pressures. The primarycause of this relative hypovolemia is an increase of the vascularcapacitance due to venodilatation. This phenomenon has beendirectly supported in animal models of sepsis (156–160) and isreinforced by the fact that clinical hypodynamic septic shock(low CO) can usually be converted to hyperdynamic shock(high CO) with adequate fluid resuscitation (35,148,161). Re-laxation of vascular smooth muscle is attributed to several ofthe mediators known to circulate during sepsis. These samemediators also contribute to the second cause of hypovolemiain sepsis: Third-spacing of fluid to the interstitium due to lossof endothelial integrity. Further, decreased oral fluid and saltintake during the course of the illness may play a role. As aconsequence, CO and central/mixed venous oxygen saturationin unresuscitated and poorly resuscitated septic shock patientsis usually decreased (161,162). Septic shock also involves a car-diogenic element. Myocardial depression is common in humansepsis and septic shock (163,164). Circulating substances suchas TNF-α, IL-1β, platelet-activating factor (PAF), leukotrienes,and most recently, IL-6 and macrophage migration inhibitoryfactor have been implicated in this process (95,165–172).
ORGAN SYSTEM DYSFUNCTIONDUE TO SEPSIS AND SEPTIC
SHOCK
Table 57.8 summarizes organ system dysfunction in sepsis andTable 57.8septic shock.
Central Nervous System
Septic encephalopathy is the most common neurologic man-ifestation of sepsis and septic shock, occurring in between8% and 80% of patients with sepsis (173–176). The likelyreason for the divergent frequencies of the syndrome in stud-
TABLE 57.8
ORGAN SYSTEM DYSFUNCTION IN SEPSIS ANDSEPTIC SHOCK
CNS Septic encephalopathyCritical illness polyneuropathy/ myopathy
Heart TachycardiaSupraventricular tachycardiaVentricular ectopyMyocardial depression
Pulmonary Acute respiratory failureAdult respiratory distress syndrome
Kidney Prerenal failureAcute tubular necrosis
GI IleusErosive gastritisPancreatitisAcalculous cholecystitisColonic submucosal hemorrhageTransluminal translocation of
bacteria/antigens
Liver Intrahepatic cholestasis
Hematologic Disseminated intravascular coagulationThrombocytopenia
Metabolic HyperglycemiaGlycogenolysisGluconeogenesisHypertriglyceridemia
Immune System Neutrophil dysfunctionCellular immune (T-cell/macrophage)
depressionHumoral immune depression
CNS, central nervous system; GI, gastrointestinal.
ies is the difficulty of identifying the condition in patientswith superimposed hypotension, sedation, hypoxemia, acido-sis, electrolyte disturbances, hypoglycemia/hyperglycemia, hy-pothermia/hyperthermia, and/or concurrent hepatic/renal fail-ure/encephalopathy. The diagnosis, requiring the presence ofaltered mentation with an extracranial source of infection, isoften one of exclusion. Although deficits can range from im-pairment of higher cognitive functions to delirium or coma,asterixis, myoclonus, and seizure activity are highly atypical(173,176). The diagnosis is best made by electroencephalog-raphy (EEG) (177). The occurrence and severity of septic en-cephalopathy (graded by EEG or Glasgow coma scale) appearsto be associated with increased mortality (as high as 70%)(173,178).
Critical illness-associated neuromuscular syndromes (inclu-sive of critical illness polyneuropathy and myopathy) are themost common cause of neuromuscular problems in the ICU(179). The primary clinical manifestation of this condition ismuscle weakness. Since many patients who are in the ICU withsepsis and septic shock require ventilatory support, the initialovert manifestation may be either respiratory failure or fail-ure to wean from ventilation. Studies have suggested an inci-dence between 35% and 50% based on clinical criteria and40% to 80% based on electromyography (EMG)/nerve con-duction studies (180–182). Although the disorder is commonly

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 15
noted later in the recovery phase of sepsis and septic shock,EMG/nerve conduction data suggest that the onset is muchearlier (concurrent or within days of the onset of septic shock)(183,184). The condition is a predominantly peripheral mo-tor neuropathy in association with the presence of the sys-temic inflammatory response. Physical findings may includedifficulty in weaning from the ventilator, symmetric paresisgreater in the lower extremities, reduced deep tendon reflexes,and ataxia (180). A distal sensory neuropathy is also com-mon. Approximately 25% of patients who are awake after aweek on mechanical ventilation have significant weakness thatlasts at least a week (185). The condition is considered to bean element of and is closely associated with the occurrence ofMODS.
Cardiovascular System
The major clinically apparent manifestations of shock on theheart are due to sympathoadrenal stimulation. Heart rate isalmost universally increased in the absence of disturbances ofcardiac conduction; the degree of increase is predictive of out-come (35). In addition, catecholamine-driven supraventriculartachycardias and ventricular ectopy with ischemic electrocar-diography (ECG) changes, particularly in patients predisposedto myocardial ischemia, may be found.
Like the brain, the blood supply to the heart is autoreg-ulated, rendering it resistant to sympathetically driven vaso-constriction and shock-related hypoperfusion. Perfusion of theheart is unchanged or even increased during sepsis and sep-tic shock (186,187). The occurrence of septic myocardial de-pression has already been addressed. Circulating myocardialdepressant substances contribute to myocardial depression insepsis and septic shock (188,189). This has been linked to de-creased beta-adrenoreceptor affinity and density (190–192), aswell as potential defects of intracellular signal transduction in-volving nitric oxide, G proteins, cyclic adenosine monophos-phate (cAMP), and cGMP (95,193–197).
Although septic myocardial depression is a transient phe-nomenon in survivors, myocardial cell injury as evidenced byincreased troponin levels does occur (198,199). Serum tro-ponin is elevated in almost half of patients with septic shock(without myocardial creatine kinase [CK-MB] elevation or is-chemic ECG changes) (200). A correlation between left ven-tricular (LV) dysfunction and troponin I (TnI) positivity hasbeen shown (199). Serum TnI correlated with left ventriculardysfunction and was an independent predictor of the need forinotropic/vasopressor support, adverse outcome, and mortalityin septic shock patients (200). Whether the clinically inappar-ent myocardial cell injury that is the source of elevated troponincontributes to, or is a consequence of, septic shock is yet to bedetermined. Although troponin is used as a marker of myocar-dial injury (particularly in the context of myocardial ischemia),it does not specifically suggest myocardial infarction in othercontexts.
Respiratory System
Early respiratory responses to sepsis include tachypnea and hy-perventilation. Gas exchange may be mildly abnormal. Laterin the course of sepsis, patients may develop diffuse alveolar
damage consistent with the acute lung injury (ALI) or adultrespiratory distress syndrome (ARDS). Infections account forabout one half of all cases of ARDS. These infections can in-volve local pneumonia or distant foci of infection associatedwith sepsis or septic shock. The risk of ARDS in associationwith sepsis increases with the severity of the syndrome (sep-sis to septic shock) (201). From 40% to 60% of patients withGram-negative septic shock develop ARDS. Sepsis is the sin-gle condition most closely associated with progression to acutelung injury or ARDS, with an incidence of 40% (202). Severalcomorbid factors increase the risk of ARDS, including chronicalcohol abuse, chronic lung disease, and severe acidemia (202).Most patients with septic ARDS also have other organ fail-ure, i.e., MODS. Death is more commonly due to MODS orthe underlying sepsis, although the impact of low tidal vol-ume ventilation in ARDS studies suggest that the lung injurymay still play a significant role (perhaps as a source of per-sistent inflammatory stimulation) (202–204). The mortality ofARDS/MODS is approximately 40%, although some recentreports suggest that it may be decreasing (202,205). Failureto improve in the first week is associated with progression ofthe syndrome and poor prognosis, as are MODS, chronic liverdisease, and age; interestingly, indices of oxygenation and ven-tilation are not predictive (202).
Renal
Acute renal failure (ARF) is a major complication of sepsis andseptic shock and occurs with increasing frequency in relationto the severity of the syndrome, from 16% to 19% with sep-sis to 51% with septic shock (31,201,206). Sepsis has beenthe leading cause of acute tubular necrosis (ATN) in some ICUstudies, accounting for almost 50% of cases (207–209). Sepsis-associated acute renal failure is associated with a substan-tially higher mortality risk (75%) than nonseptic ARF (45%);within this group, septic shock mortality is higher (80%) thanin those with severe sepsis (70%) (208,201). Compared withnon–sepsis-associated ARF, sepsis-related ARF patients are sig-nificantly older, sicker, require mechanical ventilation more of-ten, and present later in the hospital course more frequently(208).
Gastrointestinal
The gut is relatively sensitive to circulatory failure due to theresponsiveness of the splanchnic vasculature to vasoconstric-tive stimulation by extrinsic factors. In addition, gut tissuesmay have increased sensitivity to proinflammatory cytokine-driven inflammatory injury. Typical clinical gut manifestationsof hypoperfusion, sympathetic stimulation, and inflammatoryinjury associated with sepsis and septic shock include ileus, ero-sive gastritis, pancreatitis, acalculous cholecystitis, and colonicsubmucosal hemorrhage (210). In addition, enteric ischemiaproduced by circulatory shock and free radical injury with re-suscitation may breach gut barrier integrity (211,212). Sometheories propose that enteric bacteria and antigens (notably en-dotoxin) may translocate from the gut lumen to the systemiccirculation during gut ischemia, resulting in irreversible shock(213) and MODS (214).

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
16 Section VI: Shock States
Hepatobiliary
Two major forms of organ injury can be seen in the liver withsepsis and septic shock (215,216). “Shock liver” (ischemic hep-atitis) is associated with massive ischemic necrosis and majorelevations of transaminases, which can occur with septic shockand is atypical in the absence of extensive hepatocellular dis-ease (217). When it does occur, it can contribute substantiallyto lactic acidosis since the liver accounts for most serum lac-tate clearance. Hypoglycemia may also be seen. Centrilobularinjury with mild increases of transaminases and lactate dehy-drogenase is much more common. Transaminases usually peakwithin 1 to 3 days of the insult and resolve over 3 to 10 days.In both cases, there are only mild increases in bilirubin andalkaline phosphatase in the early phase. Despite the produc-tion of acute-phase reactants in early sepsis and septic shock,synthetic functions may be impaired, with decreased genera-tion of prealbumin, albumin, and hepatic coagulation factors(increased prothrombin time [PT]). After, or independent of,the occurrence of septic shock, evidence of biliary stasis withincreased bilirubin and alkaline phosphatase may be present(216). Increases in transaminases are modest.
Hematologic
Sepsis and septic shock are associated with a range of hema-tologic disorders including overt disseminated intravascu-lar coagulation (DIC), thrombocytopenia, and coagulopathy.Thrombocytopenia and coagulopathy are multifactorial in na-ture. Bone marrow suppression, consumption, and medica-tions can contribute to thrombocytopenia, whereas consump-tion and decreased liver production of coagulant factors, aswell as malnutrition (leading to depleted vitamin K stores),contribute to coagulopathy. Nonetheless, whenever these find-ings are present, early disseminated intravascular coagulation(DIC) is possible.
Septic shock is the single most common cause of DIC, char-acterized by microangiopathic hemolysis, consumptive throm-bocytopenia, consumptive coagulopathy, and microthrombiwith tissue injury. Overt DIC occurs in one quarter to onehalf of cases of Gram-negative sepsis (218). Although Gram-positive sepsis has been thought to be less closely associ-ated with DIC, the frequency of occurrence is quite similar(218,219). The occurrence of DIC in sepsis is associated with adoubling of projected mortality (218,220). DIC may also rep-resent both a driver and manifestation of MODS. The deposi-tion of microvascular thrombi can cause significant endothelialinjury and inflammatory responses leading to ischemic and in-flammatory tissue injury, the basis of MODS.
A prolonged prothrombin time and partial thromboplastintime, hypofibrinogenemia, elevated level of fibrin split prod-ucts, and the presence of the D-dimer herald the onset ofdisseminated intravascular coagulation. Since it is due to si-multaneous systemic activation of coagulation and fibrinoly-sis cascades, it can be differentiated from the coagulopathyof liver failure by determination of endothelial cell-producedfactor 8 (normal or increased with hepatic dysfunction). Thepathogenesis of this disorder is linked to activation of tissue fac-tor on endothelial cells and macrophages, probably by proin-flammatory cytokines induced by exogenous bacterial toxins(220,221).
Metabolic
Specific, predictable, and overlapping metabolic alterationsoccur in both sepsis and shock. Foremost among these ishyperglycemia. There are two reasons for hyperglycemia insepsis and states of shock. Early in sepsis, when hemody-namic dyshomeostasis initiates compensatory responses, en-dogenous catecholamines are released as a consequence of en-hanced sympathoadrenal stimulation. In addition, increasedrelease of adrenocorticotropic hormone (ACTH), glucocorti-coids, and glucagon with a concomitant decreased release of in-sulin results in glycogenolysis and gluconeogenesis (222,223).Increased epinephrine also results in skeletal muscle insulinresistance, sparing glucose for use by glucose-dependent or-gans such as the heart and brain (224). In addition, proin-flammatory, stress-related cytokines such as TNF-α, IL-1β,and IL-6 contribute to insulin resistance in peripheral tissues(225). Pharmacologic therapies of sepsis and shock, includingcatecholamine vasopressors/inotropes, steroids, and total par-enteral nutrition, can add to these effects. It is notable that,despite insulin resistance, the increased metabolic demands ofsepsis also result in increased overall glucose uptake and uti-lization (226).
With the evolution of sepsis to septic shock, metabolic re-sponses progress. Late in shock, hypoglycemia may develop,possibly due to glycogen depletion or failure of hepatic glucosesynthesis (227). Fatty acids are increased early in sepsis but falllater with hypoperfusion of adipose-containing peripheral tis-sue (226,228). Hypertriglyceridemia is often seen during shockas a consequence of catecholamine stimulation and reducedlipoprotein lipase expression induced by circulating TNF-α (223,226,229). Increased catecholamines, glucocorticoids,and glucagon also increase protein catabolism, resulting in anegative nitrogen balance (223,228).
Endocrine
Endocrine abnormalities are frequently underappreciated insepsis and septic shock. Notable alterations in levels of pitu-itary, adrenal, thyroid, growth, and sex hormones are knownto occur (225,230–236). In recent years, “relative” adrenal in-sufficiency in septic shock has received substantial attention.Few septic patients exhibit overt adrenal insufficiency. Relativebradycardia and a nontoxic appearance in a patient with septicshock is suggestive of this possibility. These are often elderlypatients who have survived an initial episode of septic shockand either fail to fully recover or suffer a relapse. However,a considerable body of literature suggests that a suboptimalcortisol response (within the normal range) to sepsis and septicshock can have deleterious effects, including prolonged pressordependence and increased mortality. Estimates of the frequencyof adrenal insufficiency in septic shock vary wildly from 0% to95% (237,238). In great part, this is due to the use of varyingdefinitions based on baseline or cosyntropin-stimulated cortisollevels or changes in levels from baseline in response to cosyn-tropin. Common definitions in septic shock patients includerandom cortisol of <700 nmol/L (25 μg/dL), peak postcosyn-tropin level of <500 to 550 nmol/L (1–20 μg/dL), or post-cosyntropin change in cortisol of <200 to 250 nmol/L (7–9μg/dL) (230,237,239,240). Interestingly, pituitary dysfunction

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 17
may play a role in many patients with adrenal insufficiency, as85% of critically ill patients have decreased levels of adreno-corticotropic hormone (ACTH) (241).
Abnormalities of thyroid hormones are also present in sep-sis and septic shock, although the clinical significance is lesscertain. In humans, serum T4 and T3 levels fall shortly afterthe onset of severe clinical infection. Euthyroid sick syndromeis manifested by low serum levels of thyroid hormones in clin-ically euthyroid patients with severe nonthyroidal systemic ill-ness. Decreased T3 levels are most common. Patients with moresevere or prolonged illness also have decreased T4 levels. Serumreverse T3 (rT3) is increased. Patients are clinically euthyroidand do not have clinically significant thyroid-stimulating hor-mone (TSH) elevations.
Sepsis and septic shock are clearly associated with perturba-tions of various hormones including insulin, growth hormone,TSH, thyroxin, ACTH, cortisol, growth hormone (242), andsex hormones. Perturbations of hormones of the posterior pi-tuitary should be expected. In addition to abnormal prolactinlevels (243), sepsis and septic shock are accompanied by rel-ative deficiencies of vasopressin/antidiuretic hormone (ADH)levels. Vasopressin, produced in the hypothalamus and storedin the posterior pituitary gland, is released in response to hy-perosmolarity. Hypotension as seen in shock states is an evenmore powerful stimulus for release. Recent human studies havesuggested a relative deficit of circulating vasopressin in patientswith septic shock (relative to those with cardiogenic or hypo-volemic shock). This deficiency may be related to depletion ofneurohypophyseal stores combined with NO-mediated inhi-bition of production (225,235). Clinically, vasopressin exertspowerful vasopressor effects in hypotensive patients, particu-larly those with septic shock. To some extent, this effect appearsto be mediated through re-establishment of reduced sensitivityto catecholamine (244).
DIAGNOSIS OF SEPSIS
Under ideal circumstances, each patient with evidence of sep-sis would undergo a thorough evaluation at presentation priorto the initiation of therapy. In the context of sepsis and septicshock, circumstances are rarely ideal, so an abbreviated ini-tial assessment focusing in critical diagnostic and managementplanning elements is frequently necessary.
To ensure maximally rapid implementation of effective ther-apy, an initial presumptive diagnosis of severe sepsis and septicshock is mandated. The criteria for this presumptive diagno-sis should be highly inclusive and based primarily on clinicalcriteria.
The initial presumptive diagnosis of sepsis with organ dys-function (severe sepsis) may be made in the presence of thefollowing elements:
■ Suspected infection based on a minimal clinical constellationof localizing (e.g., dyspnea, cough, purulent sputum produc-tion, dysuria, pyuria, focal pain, local erythema, etc.) andsystemic signs and/or symptoms of sepsis (Table 57.9)Table 57.9
■ Clinical evidence of organ dysfunction (e.g., hypotensionwith peripheral hypoperfusion, oliguria, hypoxemia, obtun-dation, etc.)
TABLE 57.9
CLINICAL SYMPTOMS/SIGNS FOR PRESUMPTIVEDIAGNOSIS OF SEVERE SEPSIS/SEPTIC SHOCK
Fever or hypothermiaChills, rigorsTachycardiaWidened pulse pressureTachypnea or hyperpneaConfusion, decreased level of consciousness or deliriumDecreased urine outputHypotension
Similarly, an initial diagnosis of septic shock is established inthe presence of suspected infection with sustained hypotensionwithout a definitive alternate explanation.
The initial presumptive diagnosis of severe sepsis or septicshock is based on clinical criteria and does not require micro-biologic, radiographic, or other laboratory evidence of specificinfection or organ injury. Only a clinical suspicion of infec-tion and organ failure is necessary. For the most part, availablelaboratory tests or imaging studies represent supportive, notdiagnostic, elements. This clinical approach allows a parallel,rapid initiation of empiric antimicrobials and supportive mea-sures.
Although a suggestive clinical examination is sufficient forthe presumptive diagnosis of severe sepsis and septic shock,more authoritative investigations (both laboratory and ra-diologic) are generally required for confirmation. For thisreason, the definitive diagnosis of severe sepsis and septicshock involves a broader range of clinical and laboratory ev-idence of sepsis (Table 57.10) and organ dysfunction (arterial Table
57.10hypotension, lactic acidosis, or any organ dysfunction variablesin Table 57.2). Establishment of a definitive diagnosis can helpto more specifically target antimicrobial therapy and triggerspecific therapies such as surgical source control and activatedprotein C.
TABLE 57.10
SUPPORTIVE/CONFIRMATORY FINDINGS FORSEVERE SEPSIS/SEPTIC SHOCK
Leukocytosis, leukopenia, increased immature white bloodcell (WBC) forms, toxic granulation, Dohle bodies
Thrombocytopenia ± increased INR or prothrombin time(PT)
Increased D-dimer or fibrin split productsIncreased serum bilirubin, AST/ALT, C-reactive proteinSerum procalcitonin elevationMetabolic acidosis with anion gapSerum lactate elevationRespiratory alkalosis or acidosisMixed venous saturation >70%Diagnostic imaging findingsPositive microbiologic or pathologic samples for abnormal
presence of micro-organisms, leukocytes, or tissue necrosis
INR, international normalized ratio; AST/ALT, aspartateaminotransferase/alanine aminotransferase.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
18 Section VI: Shock States
History
The initial history should focus on two major areas: The keysymptoms with respect to diagnosis of sepsis and of the specificsite of infection, and key factors that would modify initial em-piric therapies such as antimicrobials, fluid resuscitation, andpossibly, vasopressors/inotropes.
With respect to symptoms, constitutional complaints areentirely nonspecific. The classic pattern of fever, rigors, andchills is common but far from universal. Fatigue, malaise, anx-iety, or confusion may be observed, particularly in the elderly.Occasionally, the elderly, the immunocompromised (nonspe-cific immune dysfunction due to chronic organ failure), andthe immunosuppressed (specific immune defects) may presentwithout such symptoms.
Fever is a common feature of infection and/or sepsis. Feveris caused by a direct effect of inflammatory mediators, such asIL-1β, on the hypothalamus. The fever response may be sup-pressed in septic shock and may be absent in the elderly, im-munocompromised, or immunosuppressed patient. Hypother-mia in septic shock is associated with reduced cardiac outputand portends a poor prognosis (245). Septic encephalopathymanifested by disorientation or confusion is especially com-mon in elderly individuals. Apprehension, anxiety, and agi-tation may all occur early in the course. With severe disease(i.e., septic shock) or progression of sepsis, overt encephalopa-thy with a decreased level of consciousness and coma can oc-cur. Hyperventilation with respiratory alkalosis can manifesteven before the onset of metabolic acidosis as a consequence ofcytokine-mediated stimulation of the respiratory center in themedulla.
Localizing symptoms as described in Table 57.11 may beTable57.11 more helpful in determining the septic cause of the consti-
tutional manifestations of sepsis. The key historical factorsused to modify initial therapies include antimicrobial sensitiv-ities/allergies, recent infections/antimicrobial use, the locale ofinfection acquisition (i.e., nosocomial vs. community), and ma-jor comorbidities. The existence of comorbidities (e.g., AIDS;chemotherapy; hematologic malignancy; neutropenia resultingin immunosuppression or chronic renal, heart, liver, or otherorgan failure; COPD; dementia; inflammatory bowel diseases;diabetes; or via invasive catheters/devices) resulting in immuno-compromise mandate the use of extended-spectrum antimicro-bial therapy. Chronic renal, liver, or heart failure may alsoinfluence the choice and volume/dose of antimicrobials, re-suscitation fluids, and vasopressors. Recent antimicrobial useand nosocomial or institutional acquisition of infection mayalso mandate consideration of extended-spectrum antimicro-bial therapy to adequately cover nosocomial pathogens.
Physical Examination
The physical examination should focus on ensuring that thepatient is stable and on rapid localization of the site of infection.The physical examination should first ensure that the airwayis patent, the patient is breathing satisfactorily, and vital signsand peripheral perfusion are acceptable.
Tachypnea and tachycardia are almost universal. Nor-mothermia and fever are consistent with sepsis, but hy-pothermia should be of concern due to its association withshock/hypoperfusion. All patients with sepsis should be ob-served for signs of hypoperfusion (mottling, pallor, diaphoresis,impaired capillary refill in nail beds). An acutely ill, flushed, andtoxic appearance is common in the septic patient, particularlyearly in the course. In the early stages of sepsis, CO is wellmaintained or even increased, skin and extremities are warm,
TABLE 57.11
LOCALIZING CLINICAL SYMPTOMS AND SIGNS IN SEVERE INFECTIONS
History Physical exam
Central nervous system Headache, neck stiffness, photophobia Meningismus (neck stiffness), focal neurologic signs(weakness, paralysis, paresthesia)
Head and neck Earache, sore throat, sinus pain, or swollenlymph glands
Inflamed or swollen tympanic membranes or ear canal,sinus tenderness, pharyngeal erythema and exudates,inspiratory stridor, and cervical lymphadenopathy
Pulmonary Cough (especially if productive), pleuriticchest pain, and dyspnea
Dullness on percussion, bronchial breath sounds, andlocalized crackles
Cardiovascular Palpitations, syncope New regurgitant valvular murmur
Intra-abdominal Abdominal pain, nausea, vomiting, diarrhea,purulent discharge
Abdominal distention, localized tenderness, guarding orrebound tenderness, and rectal tenderness or swelling
Pelvic/genitourinary Pelvic or flank pain, vaginal or urethraldischarge, and urinary frequency andurgency
Costovertebral angle tenderness, pelvic tenderness, painon cervical motion, and adnexal tenderness
Skin/soft tissue/joint Localized limb pain or tenderness, focalerythema, edema, and swollen joint
Focal erythema or purple discoloration (subcutaneousnecrosis), edema, tenderness, crepitus in necrotizinginfections (Clostridia and Gram-negative infections),petechiae, purpura, erythema, ulceration, andbullous formation and joint effusion
Adapted from Sharma S, Mink S. Septic shock. http://www.emedicine.com/MED/topic2101.htm. 2007.AU: Please add
date accessed.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 19
and capillary refill is normal. As sepsis progresses, venodilationresults in reduced central venous pressure and venous return.Hypovolemic manifestations with hypotension, reduced strokevolume, and CO with signs of tissue hypoperfusion develop.As patients are aggressively fluid resuscitated, a hyperdynamiccirculatory state (albeit with distributive shock) again domi-nates the clinical picture and will usually persist until recoveryor death.
The most common sites of infection causing sepsis and sep-tic shock in order of frequency are respiratory, abdominal, uri-nary, and soft tissue infections. Abdominal infections are moreclosely associated with septic shock whereas urinary infectionsare more common in sepsis. Intravascular catheters are a fre-quently overlooked source of infection and sepsis. A recentstudy suggested that central venous catheters might account foras much as 3.7% of cases of septic shock (25). Similarly, cases ofClostridium difficile–related septic shock are often overlookedin the absence of overt toxic megacolon. Adding to the difficultyof managing the ICU patient with sepsis and/or septic shock isthat many patients have simultaneous infection at more thanone site.
Laboratory Studies
Patients with sepsis require urgent lab testing to help make afirm diagnosis and to evaluate the severity of the illness. Sep-sis and septic shock typically present with somewhat differ-ent, though naturally overlapping, laboratory parameters (seeTable 57.12). Lab tests usually start with a complete bloodTable
57.12 count (CBC). Hemoglobin is often decreased, although this is
usually due to the presence of chronic disease. Hemoglobincan occasionally be increased in patients with substantial in-terstitial third-spacing and relative hypovolemia. The whitecell count is increased in sepsis but may transiently normalizeor even drop below normal range, with progression to septicshock. Although this phenomenon has been linked to Gram-negative septic shock, it can be seen in septic shock due to anypathogen. Leukopenia in this setting has been linked to pooroutcome. Toxic granulation and the presence of Dohle bodiesare also seen more frequently, with progression to more severedisease. Similarly, a marked left shift with increasing immatureforms (bands) is more common in septic shock. Platelets oftenrespond as an acute-phase reactant, with increases early in in-fection/sepsis. However, platelet counts drop, with septic shockreaching a nadir around day 5 in survivors.
In contrast, the international normalized ratio (INR) maybe mildly abnormal at the onset of sepsis (due to malnourish-ment) and is usually most abnormal at onset of septic shock.Fibrinogen is an acute-phase reactant and is usually elevatedwith onset of infection/sepsis. However, levels will drop withseptic shock, especially if DIC intervenes. Fibrin split productsand D-dimers are very sensitive markers of progression of sep-sis and are almost universally elevated with septic shock.
Serum creatinine and blood urea nitrogen (BUN) may ac-tually be decreased due to increased renal blood flow in theearly hyperdynamic phase of sepsis but will increase with theonset of septic shock. An increase in serum creatinine denotesan increased mortality risk even within a few hours of the on-set of septic shock. Similarly, elevated serum lactate is closelycorrelated with increased mortality risk in septic shock.
TABLE 57.12
KEY LABORATORY VALUES IN INFECTION/SEPSIS VERSUS SEPTIC SHOCK
Sepsis Septic shock
Hb N or � (chronic disease) ∗ (hemoconcentration)WBC ∗ + left shift ∗, N or �
-marked left shift with metamyelocytes,toxic granulation, and/or Dohle bodies
platelets N or ∗ N or �
PT/INR N or ∗ (malnutrition) ∗∗fibrinogen N or ∗ N or �
Fibrin split products/D-dimer activity
∗ ∗∗
Glucose N or ∗ ∗∗Cr/BUN N or ∗ ∗∗Bilirubin N, late ∗ ∗, late ∗∗AST/ALT N ∗-∗∗Albumin N or � (malnutrition) �� (endothelial leakage/interstititial
redistribution)ABG respiratory alkalosis metabolic acidosisHCO3
− N �
lactate N ∗-∗∗C-reactive protein ∗ ∗∗procalcitonin ∗ ∗∗Blood culture
positivity5%–10% 30%–40%
∗ increase, ∗∗ marked increase, � decrease, �� marked decrease, N normal. Hb, hemoglobin; WBC, white blood cell count; PT,prothrombin time; INR, international normalized ratio; Cr/BUN, serum creatine and blood urea nitrogen; AST/ALT, serumaspartate transaminase and alanine transaminase; ABG, arterial blood gas; HCO3
−, serum bicarbonate concentration.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
20 Section VI: Shock States
Septic patients should have both site-specific and blood cul-tures drawn prior to initiation of antimicrobial therapy. In thecase of septic shock, however, antimicrobial therapy shouldnever be delayed to accommodate these cultures because of theantimicrobial delay-dependent increase in morality risk (25).Gram stain should be performed on all site samples. Althoughthere are some data to suggest that Gram stain is not usefulin the initial management of certain infections (nosocomialpneumonia, peritonitis due to bowel perforation), a good spec-imen, appropriately interpreted, can provide invaluable infor-mation.
Imaging Studies
Although in most cases the clinical examination will localizethe source of infection with a reasonable degree of confidence,basic radiographic imaging can be very useful in cases wherean obvious site of infection is not apparent. Advanced imagingstudies (computerized axial tomography [CAT], magnetic reso-nance imaging [MRI], ultrasound) rarely yield information re-garding localization of the infection that has not been providedby the clinical examination and basic imaging studies. How-ever, these techniques may be highly useful when definitive orprecise localization and/or delineation of extent of disease arerequired.
A chest radiograph should be obtained in most patients ad-mitted to the hospital with sepsis. Elderly, immunocompro-mised, and immunosuppressed patients with occult sepsis willoften be found to have a pulmonary source on radiographicexamination. Supine and upright or lateral decubitus abdom-inal films are useful if bowel perforation is of concern. In theappropriate clinical context of crepitus, bullae, hemorrhage, orfoul-smelling exudate with intense local pain, evidence of gasin soft tissues on plain extremity radiographs is almost pathog-nomonic of necrotizing soft tissue infection with clostridia orfacultatively anaerobic Gram-negative bacilli.
CT scan with contrast is the preferred imaging modality torule out intra-abdominal, intracranial, epidural, perinephric,and soft tissue abscesses, as well as retroperitoneal abscess ormediastinal infection. They can also be useful for localizingbowel wall injury and assessing necrotizing soft tissue infec-tions (although MRI is preferred for the latter). Ultrasoundis the initial imaging modality of choice for biliary sepsis andobstructive uropathy, although CT scan is also sensitive andspecific.
MANAGEMENT OF SEVERE SEPSISAND SEPTIC SHOCK (I.E., THE
SEPSIS SIX-PACK)
To optimize outcome in sepsis with organ dysfunction (severesepsis), the initiating triggers, amplification cascade, and down-stream organ dysfunction must be addressed; this requiresmonitoring and therapeutic elements. With respect to the ini-tiating triggers, antimicrobials and, where possible, surgicaland nonsurgical source control are mandated. With respect tothe amplification cascade, one new agent (activated protein C)has been developed that directly dampens septic response byexerting both anti-inflammatory and antithrombotic effects,
such that mortality is improved. Organ dysfunction is add-ressed through direct supportive measures. The most immedi-ate of these—fluid and vasopressor/inotropic resuscitation—support the circulatory system. However, mechanical ventila-tion and dialysis have also been shown to improve outcome insevere sepsis and septic shock.
Six major areas in the evaluation and treatment of severesepsis can be identified. These include the following:
1. Fluid resuscitation2. Antimicrobial therapy3. Vasopressors and inotropes4. Invasive and noninvasive monitoring5. Specific therapy6. Supportive therapy
Fluid Resuscitation
The development of shock in patients with sepsis involves dis-turbances of global and regional perfusion. Initially, ventricu-lar filling pressures as reflected by CVP and pulmonary wedgepressure (PWP) are decreased. As a consequence, venous returnfalls, resulting in limitation of CO. Although an increase in in-sensible losses and decreased fluid intake may contribute to thiseffect, nitric oxide–mediated venular dilatation and loss of en-dothelial barrier integrity (resulting in a drop in colloid oncoticpressure from loss of albumin into the interstitium) probablyplay a dominant role (246,247). A significant degree of hypo-volemia is almost universal in early, untreated severe sepsis orseptic shock. Available data suggest that initial isotonic fluiddeficits can exceed 10 L (248).
Management of sepsis requires consideration of both globaland regional perfusion defects, making the establishment ofgoals for therapy more complex than for other forms of shock.Support of global perfusion takes initial precedence. Sincehypovolemia is a major factor in the hypotension and hypop-erfusion of early septic shock, foremost among the appropri-ate initial therapeutic considerations is infusion of intravas-cular fluids. Fluid infusion should be implemented rapidly bylarge-bore peripheral intravenous catheters. Infusion of fluidscan improve global perfusion indices (blood pressure, CO, andMvO2/central venous oxygen saturation [ScvO2]) and may re-veal the presence of regional perfusion disturbances and/or my-ocardial depression that may require therapy with vasopres-sors/inotropes.
The three issues to consider in optimizing fluid resuscitationare the type of fluid used, the rapidity of infusion, and theamount of fluid administered.
Initial resuscitation of septic patients should be aimed at rapidintravascular volume expansion. The view that intravascularfluid depletion plays a central role in the pathogenesis of earlyseptic shock has been recognized since the past midcentury.Several studies suggested that septic shock is associated withreduced total circulating blood volume (149,150). Since almostall untreated patients with severe sepsis or septic shock have asignificant element of hypovolemia, a hypodynamic circulationwith decreased cardiac output is typical prior to fluid resuscita-tion. This hypovolemia is probably the basis of early observa-tions that death in sepsis is associated with decreased cardiacoutput. The patients in those studies were clearly inadequately

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 21
resuscitated by current standards (149,150). Additional sup-port for the central importance of functional hypovolemia inearly septic shock comes from a more recent demonstrationthat the venous oxygen saturation is decreased in early prere-suscitation septic shock (consistent with the findings in otherforms of hypodynamic shock) (161).
Aggressive fluid loading is the standard early therapy ofseptic shock and results in the generation of a hyperdynamiccirculatory state in >90% of patients (249). Rapid fluid re-suscitation may reveal severe sepsis without shock in a sig-nificant subset of patients with apparent septic shock (248).Increased total blood volume has been associated with highercardiac output and increased survival in human septic shock(150). Intravascular volume dependence of the hyperdynamiccirculatory state in sepsis has been confirmed in animal mod-els (158). Although the demonstration that resuscitation fromhypovolemia improves outcome in traumatic shock dates backto the early work of Cannon (250) and Cournand et al. (251),clear evidence that early aggressive fluid resuscitation improvesoutcome in septic shock is limited to a small series of pedi-atric septic shock (252) and a recent randomized study of goal-directed resuscitation (253).
Initial fluid resuscitation should be titrated to specific clini-cal endpoints. Aggressive fluid loading in patients with septicshock can increase total blood volume, cardiac output, oxygendelivery, and consumption while reducing lactic acidosis (119).Older studies have suggested that an increased blood volumeassociated with normalization of cardiac output is associatedwith improved survival (149,150).
In the absence of early invasive or echocardiographic mon-itoring, clinical end points can be used for titration of fluidresuscitation. Since both initial heart rate and blood pressurehave been shown to be associated with outcome in septic shockas well as hypovolemic shock (35,254–256), standard goalsmay include the following:
■ Heart rate ≤100 beats/minute■ Systolic blood pressure (≥90 mm Hg)■ Mean arterial pressure (≥60–65 mm Hg)■ Urine output (≥0.5 mL/kg/hour)
It should be noted that these clinical parameters can underes-timate initial resuscitative requirements in critically ill subjectsincluding those with septic shock (257–259).
Mortality in both septic and other forms of shock has alsobeen associated with increased arterial lactate and base deficitlevels (260). Normalization of these parameters can be usedto augment clinical end-points for titration of fluid resuscita-tion (261). However, both parameters represent relatively lateresponses to cellular stress, and resolution may similarly lagfollowing the implementation of effective resuscitation (262).
Initial fluid resuscitation should be achieved using isotoniccrystalloid solutions. Effective fluid resuscitation can be de-livered with either isotonic crystalloid (e.g., normal saline, lac-tated Ringer solution) or colloid solutions (e.g., hydroxyethylstarch, human albumin). All of these solutions are equally ef-fective if titrated to the same clinical end points. Given thedifference in distribution of such compounds, it typically re-quires approximately four times more crystalloid to achievethe same hemodynamic effect as a given amount of colloid(263). Several animal and human studies have pointed out
theoretical advantages to colloids in limiting interstitial fluidaccumulation (which may benefit ARDS) in sepsis and septicshock (264–266). However, no clinical study has suggested im-proved clinical outcomes (morbidity or mortality) with colloidsolutions (267,268). Although the severe sepsis subset of onerecent randomized controlled trial (RCT) trended toward amore favorable outcome with albumin resuscitation (269), an-other (meta-analytic) study suggested an opposite trend towardincreased mortality with albumin use (268,270). In addition,colloids are substantially more expensive than crystalloid solu-tions. For these reasons, isotonic crystalloids are recommendedas the initial resuscitative solution for severe sepsis and septicshock. The development of a hyperchloremic acidosis can beanticipated with use of large volumes of normal saline. Useof lactated Ringer solution may limit this effect. Hypertonicsaline is not recommended for the routine resuscitation of sep-tic shock.
Rapid volume expansion (500 mL isotonic crystalloid every10–30 minutes) should be continued until clinical and physio-logic treatment targets are met. Vasopressor/inotropic supportis required if fluid infusion alone fails to achieve physiologic re-sponse targets. Early aggressive resuscitation to achieve physi-ologically normal hemodynamic goals reduces subsequent mor-bidity and mortality in patients with septic shock. In a pediatricpopulation with septic shock, rapid fluid resuscitation in thefirst hour of presentation to hospital improved survival (252).In an adult study, the effect of early goal-directed resuscitationto normal physiologic values in patients presenting to an emer-gency department with severe sepsis or septic shock was exam-ined (253). All patients (both conventional and goal-directedtherapy groups) were resuscitated in the emergency room forthe first 6 hours to standard hemodynamic end-points of CVP≥8 mm Hg, MAP ≥65 mm Hg, and urine output ≥0.5 mL/kgper hour. The experimental early goal-directed therapy group,in addition, was managed using an experimental protocol toachieve both the standard goals and a central venous oxygensaturation ≥70% (as measured by an oximetric central venouscatheter). During the 6 hours of their protocolized emergencyroom support, the experimental group received 1.5 L more fluidthan the control group, and a substantially larger fraction ofthe patients in the experimental group achieved the physiologicresuscitative goals (99.2% vs. 86.1%). Overall mortality wassignificantly lower in the early goal-directed therapy group.
Antimicrobial Therapy and Source Control
Historically, critically ill patients with overwhelming infectionhave not been considered a unique subgroup comparable toneutropenic patients for purposes of selection of antimicrobialtherapy. However, critically ill patients with severe sepsis andseptic shock, similar to neutropenic patients, are characterizedby distinct differences from the typical infected patient thatimpact on the optimal management strategy. These differencesinclude the following:
■ Marked alterations in antibiotic pharmacokinetics■ Increased frequency of hepatic and renal dysfunction■ High prevalence of unrecognized immune dysfunction■ Predisposition to infection with resistant organisms■ Marked increase in frequency of adverse outcome if there is
a failure of rapid initiation of effective antibiotic therapy

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
22 Section VI: Shock States
Critical management decisions in this patient group must of-ten be made emergently in the absence of definitive data regard-ing the infecting organism and its sensitivity pattern, patientimmune status, and organ function. Since outcomes in severesepsis and septic shock are strongly influenced by the rapidity ofadministration of an appropriate antimicrobial regimen at firstpresentation, a particularly thoughtful and judicious approachto initial empiric antimicrobial therapy is required (271–273).
Empiric antibiotic regimens should approach 100% coverageof pathogens for the suspected source of infection. Initial ad-ministration of inappropriate antimicrobials increases morbid-ity in a wide range of infections. The occurrence of initiationof inadequate antimicrobial therapy may occur as frequentlyas 17.1% in community-acquired and 34.3% in nosocomialbacteremia in patients admitted to the ICU (273). Similarly,18.8% and 28.4% of septic shock cases were initially treatedwith inadequate antimicrobial therapy in another large study(274). Retrospective studies have shown that the risk of deathincreases from 30% to 60% in ICU bacteremia (4,272) to 70%to 100% in Gram-negative shock (4) when the initial empiricregimen fails to cover the inciting pathogen. More recent datasuggest that the relative increase in survival of septic shock withinappropriate initial antimicrobial therapy is reduced approx-imately 5-fold (range 2.5 to 10-fold in selected subgroups) toabout 10% (274). These findings of a sharply increased mortal-ity risk with initial inadequate antimicrobial therapy apply toserious infections caused by Gram-negative and Gram-positivebacteria as well as Candida species (4,274–278).
As a consequence, empiric regimens should err on the sideof overinclusiveness. The most common cause of initiation ofinappropriate antimicrobial therapy is a failure of the clinicianto appreciate the risk of infection with antibiotic-resistant or-ganisms (either otherwise uncommon organisms with increasednative resistance or antibiotic-resistant isolates of common or-ganisms). Selection of an optimal antimicrobial regimen re-quires knowledge of the probable anatomic site of infection;the patient’s immune status, risk factors, and physical environ-ment; and the local microbiologic flora and organism resistancepatterns. Risk factors for infection with resistant organisms in-
clude a prolonged hospital stay, prior hospitalization, and priorcolonization or infection with multiresistant organisms.
Superior empiric coverage can be obtained through theuse of a local antibiogram or via consultation with aninfectious disease specialist (279). Although not routinelyrequired, extended-spectrum Gram-negative regimens, van-comycin, and/or antifungal therapy may be appropriate in spe-cific high-risk cases with severe sepsis (Table 57.13). In addi- Table
57.13tion, given that 90% to 95% of patients with septic shock havecomorbidities or other factors that make them high risk for re-sistant organisms, it may be appropriate to initially treat allpatients with septic shock using a combination of antimicro-bials that result in a broadly expanded spectrum of coveragefor the first few days. This approach should improve the ad-equacy of antimicrobial coverage initially, while ensuring thathigh-risk patients are not inappropriately categorized as lowrisk.
Intravenous administration of broad-spectrum antimicrobialsshould be initiated immediately (preferably <30 minutes) fol-lowing the clinical diagnosis of septic shock. Appropriate in-travenous, empiric broad-spectrum therapy should be initiatedas rapidly as possible in response to clinical suspicion of in-fection in the presence of hypotension, i.e., presumptive septicshock. An assumption that hypotension is caused by anythingother than sepsis in the setting of documented or suspectedinfection should be avoided, unless there is very strong dataindicating a specific alternate cause. Retrospective studies ofhuman bacteremia, pneumonia, and meningitis with sepsis sug-gest that mortality in sepsis increases with delays in antimicro-bial administration (271,278,280–282). One major retrospec-tive analysis of septic shock has suggested that a delay in theinitial administration of effective antimicrobial therapy is thesingle strongest predictor of survival (25). Initiation of effec-tive antimicrobial therapy within the first hour following theonset of septic shock-related hypotension was associated with79.9% survival to hospital discharge (Fig. 57.9). For every ad-ditional hour to effective antimicrobial initiation in the first 6hours post onset of hypotension, survival dropped an averageof 7.6%. With effective antimicrobial initiation between the
TABLE 57.13
INDICATION FOR EXTENDED EMPIRIC ANTIBIOTIC THERAPY OF SEVERE SEPSIS/SEPTICSHOCK
↑ Gram-negative coverage ■ Nosocomial infection■ Neutropenic or immunosuppressed■ Immunocompromised due to chronic organ failure (liver, renal,
lung, heart, etc.)
↑ Gram-positive coverage (vancomycin) ■ High-level endemic MRSA (community or nosocomial)■ Neutropenic patient■ Intravascular catheter infection■ Nosocomial pneumonia
Fungal/yeast coverage (triazole,echinocandin, amphotericin B)
■ Neutropenic fever or other immunosuppressed patientunresponsive to standard antibiotic therapy
■ Prolonged broad-spectrum antibiotic therapy■ Positive relevant fungal cultures■ Consider empiric therapy if high-risk patient with severe shock
MRSA, methicillin-resistant Staphylococcus aureus.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 23
first and second hour post hypotension onset, survival had al-ready dropped to 70.5%. With effective antimicrobial therapydelay to 5 to 6 hours after hypotension onset, survival was just42.0%, and by 9 to 12 hours, 25.4%. The adjusted odds ratioof death was already significantly increased by the second hourpost hypotension onset, and the ratio continued to climb withlonger delays.
Substantial delays before initiation of effective therapy havebeen shown in several studies of serious infections (271,282–284). In septic shock, the median time to delivery of effec-tive antimicrobial therapy following initial onset of recur-rent/persistent hypotension was 6 hours (25).
A potential survival advantage may exist if a pathogenicorganism can be isolated in severe infections, including septicshock. Every effort should be made to obtain appropriate site-specific cultures to allow identification and susceptibility test-ing of the pathogenic organism; however, such efforts shouldnot delay antimicrobial therapy.
Antimicrobial therapy should be initiated with dosing atthe high end of the therapeutic range in all patients withlife-threatening infection. Early optimization of antimicrobialpharmacokinetics can improve the outcome of patients withsevere infection, including septic shock. This is most easilyachieved by initiating antibiotic therapy with high-end dosingregimens.
Early in sepsis, before the onset of hepatic or renal dysfunc-tion, cardiac output is increased in many patients. In associa-tion with increased free drug levels due to decreased albuminlevels, drug clearance can be transiently increased (285). Asthe illness progresses, ICU patients with sepsis or septic shockexhibit substantially increased volumes of distribution and de-creased clearance rates. Consequently, suboptimal dosing ofantibiotics is common in these conditions (286–291). Data ismost well developed in reference to aminoglycosides but alsoexists for fluoroquinolones, β-lactams, and carbapenems (286–291). Failure to achieve targets on initial dosing has been as-sociated with clinical failure with aminoglycosides (292,293).Similarly, clinical success rate for treatment of serious infec-tions tracks with higher peak blood levels of fluoroquinolones(nosocomial pneumonia and other serious infections) (294–296) and aminoglycosides (Gram-negative nosocomial pneu-monia and other serious infections) (297,298). Although thereare extensive data in experimental animals and less serious hu-man infections, data for optimization of outcomes using β-lactams in critically ill, infected patients is relatively limited(299,300). A single recent paper has shown improved survivalin patients with Pseudomonas bacteremia when treated withextended infusions rather than standard intermittent dosing ofpiperacillin/tazobactam (301).
Achievement of optimal serum concentrations of aminogly-cosides (peak antibiotic serum concentration:pathogen mini-mal inhibitory concentration [MIC] ratio of ≥12) and longerperiods of bactericidal β-lactam and carbapenem serum con-centrations (minimum time above MIC in serum of 60% ofdosing interval) are appropriate goals (294,302,303). This canmost easily be attained with once-daily dosing of aminogly-cosides (304). For β-lactams and related antibiotics, increasedfrequency of dosing (given identical total daily dose) is recom-mended. For example, piperacillin/tazobactam can be dosed ateither 4.5 g every 8 hours or 3.375 g every 6 hours for seri-ous infections; all things being equal, the latter would achieve
a higher time above MIC and should be the preferred dosingoption. A similar dosing approach should be used for other β-lactams in critically ill patients with life-threatening infections.Limited data suggest that continuous infusion of β-lactams andrelated drugs may be even more effective, particularly for rela-tively resistant organisms (305–309).
Multidrug antimicrobial therapy is preferred for the initial em-piric therapy of septic shock. Probable pathogens should becovered by at least two antimicrobials with different bacteri-cidal mechanisms. Given that highly resistant organisms areendemic in the critical care environment, multidrug antimicro-bial therapy will reduce the probability of failure to cover theseorganisms. In addition, most patients with septic shock (eventhose without specific pre-existing immune defects) exhibit sig-nificant deficits of neutrophil and monocyte function during thecourse of their illness (310–316). Furthermore, malnutritionand organ dysfunction (e.g., renal or hepatic failure), whichare common in ICU patients, suppress cell-mediated immunity.Based on these data, septic shock patients likely have a reducedability to clear infection and may be best managed with mul-tidrug therapy similar to that recommended for patients withneutropenic sepsis (317,318).
No prospective controlled study has specifically comparedmultiple versus single antimicrobial therapy in a broad rangeof severe sepsis or septic shock patients. Most infectious dis-eases physicians and other experts suggest no advantage tomultidrug therapy in serious infections, including bacteremia(319,320). However, a subgroup analysis of the sickest sub-set of patients with Gram-negative bacteremia, with or with-out shock, has tended to suggest improved survival with theuse of two or more antibiotics to which the causative organ-ism is sensitive (321–324). Similarly, at least two retrospectiveand one prospective analyses of the most severe, critically illpatients with bacteremic pneumococcal pneumonia suggestedimprovement in outcome if two or more effective agents wereused (325–327). This occurred even as patients with pneumo-coccal bacteremia with a lower severity of illness demonstratedno such benefit (325). A recent secondary analysis of a prospec-tive study of community-acquired pneumonia has shown bene-fit with multidrug therapy compared to monotherapy but onlyin the subset of septic shock (328).
Empiric antimicrobial therapy should be adjusted to a nar-rower regimen within 48 to 72 hours if a plausible pathogenis identified or if the patient stabilizes clinically (i.e., resolutionof shock). Although several retrospective studies have demon-strated that inappropriate therapy of bacteremic septic shockyields increased mortality (4,272,276–278), none have sug-gested that early narrowing of antibiotic therapy is detrimen-tal if the organism is identified or if the patient is respondingwell clinically. This approach will maximize appropriate an-tibiotic coverage of inciting pathogens in septic shock whileminimizing selection pressure toward resistant organisms. Al-though it is tempting to continue a broad-spectrum regimen inthe 15% of improving patients who are culture negative for apotential pathogen, intensivists must recognize that a strategyof broad-spectrum initial antimicrobial therapy will be sustain-able only if overuse of these agents can be avoided. Aggressivede-escalation of antimicrobial therapy within 48 to 72 hoursafter initiation is required.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
24 Section VI: Shock States
TABLE 57.14
COMMON SOURCES OF SEVERE SEPSIS/SEPTICSHOCK REQUIRING URGENT SOURCE CONTROL
Toxic megacolon or C. difficile colitis with shockIschemic bowelPerforated viscusIntra-abdominal abscessAscending cholangitisGangrenous cholecystitisNecrotizing pancreatitis with infectionBacterial empyemaMediastinitisPurulent tunnel infectionsPurulent foreign body infectionsObstructive uropathyComplicated pyelonephritis/perinephric abscessNecrotizing soft tissue infections (necrotizing fasciitis)Clostridial myonecrosis
Where possible, early source control should be implementedin patients with severe sepsis, septic shock, and other life-threatening infections. Source control is a critical issue in themanagement of infection associated with severe sepsis. Infec-tions found in ICU patients frequently require source controlfor optimal management. The need for such source control mayinitially be overlooked in many infections commonly found inthe ICU (e.g., pneumonia-associated bacterial empyema, decu-bitus ulcers, C. difficile colitis). Causes of septic shock wheresource control may be required are noted in Table 57.14.Table
57.14 Source control may include removal of implanted or tun-neled devices, open surgical/percutaneous drainage of infectedfluids or abscesses, and surgical resection of infected tissues.In a broader sense, it is inclusive of elimination of incitingchemotherapies (e.g., antibiotics driving C. difficile colitis orchemotherapy causing gut injury). Efforts to identify infectionsrequiring invasive forms of source control frequently requirerapid (<2 hours) radiographic imaging (often CT scan) or, ifclinical status and findings are supportive, direct and immedi-ate surgical intervention without an imaging effort. With rareexceptions, surgical source control should follow aggressiveresuscitative efforts to minimize intraoperative morbidity andmortality. In some cases (e.g., rapidly progressive necrotizingsoft tissue infections, bowel infarction), optimal managementmandates simultaneous aggressive resuscitation and surgicalintervention. Subgroup analysis in at least one large prospec-tive, severe sepsis study has suggested that failure to implementadequate source control is associated with increased mortality(329). Earlier surgical intervention has been shown to have asignificant impact on outcome in certain rapidly progressiveinfections such as necrotizing fasciitis (330,331). In a large ret-rospective study, time from hypotension to implementation ofsource control was found to be highly correlated with outcome(332).
The necessity for or efficacy of source control efforts shouldbe reassessed within 12 to 36 hours following admission and/orsource control efforts should be based on clinical response.
Vasopressors and Inotropes
Following fluid resuscitation, patients with severe sepsis or sep-tic shock may demonstrate persistent vasomotor dysfunction
characterized by regional perfusion deficits with or withoutsystemic hypotension despite normal or increased CO. Clini-cal manifestations may include lactic acidosis and ongoing pro-gression of organ failure.
Until recently, the only available approach to correction ofregional perfusion defects was vasopressor therapy. Unfortu-nately, vasopressors do not represent a specific therapy forthis problem. Their primary use is to increase systemic arterialpressure to a range that potentially sustains the ability of thevasculature to autoregulate flow on a tissue and organ level(333,334), and thus, vital organ perfusion can be supported(potentially at the expense of peripheral perfusion) until defini-tive therapy (infection source control and antibiotics) can beimplemented.
The aim of vasopressor/inotropic therapy in septic shock issimply the optimization of critical organ and tissue perfusion.However, the specific global and/or regional perfusion goalsrequired to achieve this result are complex and controversial.Although specific targets can be suggested, therapy for each pa-tient must be highly individualized and dynamic. Appropriategoals will change over time and should be re-evaluated on acontinuing basis.
If hypotension and/or clinical evidence of tissue hypoperfusionpersist after adequate fluid resuscitation of septic shock, va-sopressor therapy is indicated. Norepinephrine and dopamineare both effective as initial therapy. Initiation of vasopressorsupport is dependent on the patient’s clinical status followingfluid resuscitation. If systemic hypotension in association withevidence of tissue/organ hypoperfusion (oliguria, obtundation,lactic acidosis) persists, vasopressor support is indicated. Se-lection of a vasopressor agent is based on an individualizedassessment of the patient’s needs. The patient’s hemodynamicpresentation, the anticipated cardiovascular effect of each va-soactive agent (based on the distribution of receptor activity),and the physician’s experience and comfort with each drugshould be considered. As a consequence of the variety of fac-tors that may play a role in vasopressor selection, septic shockpatients with a predominantly distributive hemodynamic pat-tern can be appropriately and effectively managed with one ofseveral vasopressors including dopamine, norepinephrine, orphenylephrine.
Ideally, patients should have achieved the targeted intravas-cular volume status prior to initiation of vasopressors. Al-though vasopressors can be used to maintain blood pressurefor brief periods while intravascular volume is repleted, the in-fusion of high=dose vasopressors to volume-depleted patientsmay substantially aggravate ischemic organ injury.
Studies suggesting that norepinephrine is superior todopamine are less than definitive (335–340). No controlledstudy has directly assessed norepinephrine and dopamine interms of survival, and few have compared the two agents withrespect to markers of organ dysfunction. Studies assessing theeffects of these agents on renal and splanchnic perfusion havebeen mixed, with neither agent demonstrating conclusive su-periority (336,337,340–347). Norepinephrine may have morepowerful vasopressor activity than dopamine (348). In addi-tion, its inotropic effects are mediated by direct activity onmyocardial β-adrenoreceptors. Dopamine pressor effects areweaker than those of norepinephrine, and inotropic effects aresubstantially indirect (through stimulation of release of my-ocardial catecholamine stores); excessive tachycardia may be

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 25
more common. In addition, dopamine may exert significantimmunosuppressive effects through suppression of prolactinproduction from the hypothalamus (349). Phenylephrine, a rel-atively pure β-adrenergic agonist, has minimal or absent in-otropic effects and tends to cause reflex bradycardia. For thatreason, it can be very useful in the context of excessive tachycar-dia or concurrent tachyarrhythmias. However, phenylephrineconsistently decreases cardiac output and has an increasedpropensity to cause ischemic complications. Despite potent in-otropic and vasopressor activity, epinephrine is not commonlyused as the initial pressor therapy in septic shock because it cangenerate profound tachycardia, tissue ischemia, and metabolicdisturbances.
Dobutamine is indicated for patients with low cardiac index orother evidence of hypoperfusion following achievement of ad-equate blood pressure. Milrinone can be used as an alternateagent if the response to dobutamine is suboptimal. In somecases of septic shock, clinical or laboratory evidence of hy-poperfusion (e.g., oliguria, altered mentation, decreased mixedvenous oxygen saturation, increased lactic acidosis) persists de-spite an adequate blood pressure. In this circumstance, the pa-tient may require a higher blood pressure or assessment of car-diac output (via PAC or echocardiography) to determine theneed for inotropic support. In the small proportion of septicshock patients who manifest overt myocardial depression fol-lowing fluid resuscitation, dobutamine or milrinone may be in-dicated. Dobutamine can increase cardiac index in septic shock,although the inotropic response is frequently blunted relativeto normal subjects (350,351). If catecholamine responsivenessis inadequate, low-dose milrinone may be effective since its in-otropic activity is mediated through an alternate mechanism(352). When using either agent, patients must be adequatelyfluid resuscitated. Severe hypotension can result if intravascu-lar volume is deficient when either dobutamine or milrinone isinitiated (350,352).
Although the aim of inotropic therapy in severe sepsis/septicshock is to improve cardiac output and tissue perfusion, specificgoals for cardiac index have been controversial; the currentlyrecommended target is a CO within the normal range (approx-imately 2.5–4 L/minute per m2). The utility of MvO2/ScvO2 asglobal indices of tissue perfusion adequacy in severe sepsis andseptic shock is also uncertain. Limited studies suggest that anMVO2/ScvO2 below the normal range (65%–70%) may indi-cate inadequacy of resuscitation and/or total perfusion in earlyseptic shock (161). If other hemodynamic targets have beenachieved, an MvO2 <65% may represent an appropriate indi-cation to increase oxygen delivery by starting inotropic agents.Recommendations to increase MvO2 are based on mixed ev-idence. No benefit was noted in a randomized trial of goal-directed therapy using MvO2 in critically ill patients after theonset of organ dysfunction (353,354). On the other hand, earlygoal-directed therapy targeting a ScvO2 of ≥70% was associ-ated with improved outcome in another study (253).
Supranormal hemodynamic goals are not indicated in themanagement of septic shock. Observational studies of medi-cal and surgical critical care patients have demonstrated lowervalues of physiologic variables such as oxygen consumption(VO2), oxygen delivery (DO2), and CI in nonsurvivors rel-ative to survivors of septic shock (355,356). These observa-tions formed the basis of efforts to implement goal-directedtherapy in septic shock to achieve supranormal physiologic
parameters consistent with levels observed in survivors (i.e.,CI ≥4.5 L/min/m2, DO2 ≥600 mL/minute per m2, and VO2
≥170 mL/minute per m2). Although a single clinical trial andat least one meta-analysis have suggested some promise withthis approach (357,358), several large randomized trials havefailed to demonstrate an overall significant benefit of supra-normal oxygen delivery in patients with severe sepsis and sep-tic shock (353,354,359–361). One has suggested increasedmortality when supranormal oxygen delivery was generatedwith dobutamine (354). The absence of a beneficial effect withsupranormal oxygen delivery in patients with severe sepsis andseptic shock has been supported in recent meta-analytic reviews(362).
Continuous infusion of vasopressin (0.01–0.04 U/minute)exerts a strong pressor effect and may be beneficial incatecholamine-resistant septic shock following adequate vol-ume resuscitation. Recently, vasopressin levels in septic shockpatients have been shown to be decreased (363). Further stud-ies have demonstrated that intravenous infusion of vasopressinin patients with septic shock results in a profound pressorresponse (236,364,365), an effect that is absent with evenlarger amounts of vasopressin in normotensive patients (235).A randomized, controlled, double-blind trial of 4-hour infu-sion of norepinephrine and vasopressin in high-dose, pressor-dependent shock has demonstrated significant improvement inurine output and creatinine clearance, along with a concomi-tant reduction in conventional vasopressor requirements in thevasopressin group (365). Another RCT has recently demon-strated that, while vasopressin can spare the need for high dosesof sympathomimetic agents, outcome is not affected (366).
Because of the limited experience with this compound andthe relatively prolonged pharmacologic effect of the drug, va-sopressin should be used only after hemodynamic stabilizationwith standard agents (catecholamines) has been attempted.
At high dose (>0.04 U/minute), vasopressin may produceincreased blood pressure, bradycardia, arrhythmias (prematureatrial contractions, heart block), severe peripheral vasocon-striction, decreased cardiac output, myocardial ischemia, my-ocardial infarction, and cardiac arrest. In patients with vasculardisease, even relatively modest doses can precipitate peripheralvascular insufficiency, mesenteric ischemia, or myocardial in-farction. Given these potential side effects, the minimal amountof vasopressin required should be used to achieve the desiredblood pressure goals. In addition, since vasopressin appears tobe a pure vasopressor in the context of vasodilatory shock, car-diac output will usually decline. Consideration of placement ofan intra-arterial and pulmonary artery catheter (PAC) shouldbe given to all patients receiving vasopressin for shock.
Administration of low- or renal-dose dopamine (1–4 μg/kg perminute) to maintain renal or mesenteric blood flow in sepsisand septic shock is not recommended. Although concurrent in-fusion of low-dose dopamine during human septic shock doesmitigate a decrease in renal perfusion that can occur as a con-sequence of norepinephrine infusion, the clinical benefit of thistherapy is questionable (367,368). Low-dose dopamine infu-sions can cause a mild transient diuresis in the absence of othervasopressors in nonoliguric critically ill patients (369,370).However, low-dose dopamine does not prevent the develop-ment of renal dysfunction in these patients, including thosewith sepsis and septic shock (371,372).

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
26 Section VI: Shock States
Invasive and Noninvasive Monitoring
Controversy exists regarding the most appropriate monitor-ing methods for determining the adequacy of resuscitation inpatients with severe sepsis and septic shock. The range ofmonitoring that must be considered in each patient beginswith observation by specially trained nursing personnel, toroutine noninvasive devices (e.g., continuous electrocardio-graphic monitors, intermittent mechanical sphygmomanome-try, end-tidal carbon dioxide sensors, percutaneous oximetry),to commonly used invasive techniques (arterial, central venous,and pulmonary artery catheters). Prior to the advent of ba-sic hemodynamic monitoring in the 1950s and early 1960s,clinical examination and manual sphygmomanometry were theonly available methods for assessment of cardiovascular status.Clinical judgment correctly predicts the hemodynamic profile(including CO and central venous/pulmonary wedge pressures)of critically ill patients only about half of the time (373,374).
CVP has been considered a useful measure of intravascu-lar volume since the early studies of hypovolemic shock inyoung men following battlefield trauma (250,251). However,CVP may be much less reliable as a reflection of left ventricularpreload in older patients with various cardiopulmonary disor-ders as are typically found in a modern-day ICU (152,375). Al-though low filling pressures may reliably indicate hypovolemiain most patients, the presence of a normal or even elevatedcentral venous pressure can be misleading in patients in whomright ventricular afterload is elevated or right ventricular con-tractility is impaired (376).
The PWP obtained by using a PAC has been consid-ered to reflect intravascular volume more reliably than CVP.In addition, the device allows thermodilution-based deriva-tion of CO (373,374,377). Although the PAC has gainedwidespread acceptance, significant questions about its use havebeen raised. Several studies have questioned the relationship ofPAC-derived, pressure-based estimates of ventricular preloadin specific groups of critically ill patients (375) and, more re-cently, even in normal subjects (378). In addition, the lack ofrandomized trials demonstrating benefit and the association ofPAC with excess mortality in two observational cohort studieshave led to concerns regarding the clinical utility of and safetyof PACs (379,380). Despite these concerns, the PAC remainsthe most commonly used modality for hemodynamic monitor-ing of unstable critically ill patients.
Patients with established septic shock should have continu-ous monitoring of blood pressure, oxygen saturation, electro-cardiogram (ECG), and urine output in a closed ICU staffedwith full-time dedicated intensivists and critical care–trainednurses. Several studies have demonstrated that a reduced mor-tality with decreased length of stay and overall cost for a widerange of individual conditions are obtained when critically illpatients are cared for in closed ICUs staffed with full-time dedi-cated intensivists and nurses (381–385). Similar improvementsin outcome of sepsis and septic shock have been documentedwith the use of dedicated intensivists in closed ICUs (386).Among the practice differences associated with the use of full-time intensivists is a greater use of invasive monitoring (384).
Patients requiring vasopressor agents for a prolonged period orat high dose should be strongly considered for insertion of an
arterial pressure catheter for continuous blood pressure moni-toring, as well as to facilitate frequent measurements of arterialblood gases and chemistry. Accurate, continuous monitoringof blood pressure is required for optimal assessment of sever-ity of shock, response to fluid resuscitation, and titration ofvasopressors and inotropes. However, intense peripheral vaso-constriction may occur during shock as a consequence of thevascular compensatory response to hypotension or due to ad-ministration of vasopressors. Clinical ausculatory and nonin-vasive mechanical methods can be highly inaccurate in thissetting (387,388). Patients with sustained shock, particularlythose requiring vasopressor support, should be assessed forplacement of an intra-arterial catheter for continuous bloodpressure monitoring. However, such catheters should be pref-erentially placed in peripheral sites in non-end arteries (radial,dorsalis pedis), and should be used with caution in patients athigh risk for vascular disease.
If volume resuscitation requirements exceed 2 L, placementof a central venous catheter for monitoring of CVP and forvasopressor/ inotrope infusion should be considered. An ini-tial target CVP of ≥8 mm Hg is recommended. Fluid deficitsduring septic shock in adults typically range from 5 to 10 L(248). In the absence of significant cardiopulmonary dysfunc-tion, central venous pressure should accurately assess intravas-cular volume status. However, cardiopulmonary dysfunction isnot uncommon in patients with septic shock either as an un-derlying predisposition to critical illness/sepsis or as a conse-quence of the injury (ARDS/acute lung injury [ALI], myocardialdepression). Low central venous pressures remain indicativeof hypovolemia; elevated or normal central venous pressuresin this patient group may not necessarily indicate euvolemia.CVP monitoring should be entertained if substantial amountsof fluid resuscitation are required to ensure that overt hypov-olemia is adequately addressed. The initial target CVP shouldbe ≥8 mm Hg, with additional increases indicated by the ef-fect of fluid boluses on cardiac output. The overall goal is toprovide adequate cardiac output and tissue perfusion using thelowest necessary cardiac filling pressures.
Initiation of invasive cardiac monitoring using a pulmonaryartery catheter should be considered if there has been an inad-equate response to fluid resuscitation (3–5 Ls or CVP 8–12 mmHg), if there is clinical suspicion of intravascular fluid volumeoverload, or if the patient has impaired cardiac function. Aninitial target of PWP of 12–15 mm Hg will ensure that hypov-olemia is absent in most patients, but higher pressures may berequired in certain subgroups. Although the maintenance of a
AU: Isadded“mm Hg”what wasintended?
blood pressure adequate for autoregulation of blood flow tovital organs and tissues is the first objective in the resuscitationof septic shock, support of global perfusion is also critical. Ad-equacy of global perfusion cannot always be reliably inferredfrom the clinical examination or CVP/arterial pressure mon-itoring (373,377,389). Patients who respond poorly to fluidresuscitation or are at high risk for fluid resuscitation–relatedcomplications may benefit from pulmonary artery catheteriza-tion. A substantial degree of variability in the relationship be-tween PWP and end-diastolic volumes makes it difficult to spec-ify target PWP goals that ensure adequate cardiac output andtissue perfusion (378,390,391). In general, a PWP titrated toat least 12 to 15 cm H2O will optimize cardiac function (152).If hypotension persists, a higher PWP may be beneficial as

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 27
assessed by measuring the effect of additional fluids on cardiacindex. An elevated PWP may risk the development or aggra-vation of ALI and ARDS (392,393). Specific groups that mayrequire higher PWP include those with congestive heart failure,left ventricular hypertrophy, restrictive or constrictive heart dis-ease, or increased intrathoracic pressures, including those onhigh levels of positive end-expiratory pressure (PEEP).
In patients with vasopressor-requiring shock who develop pro-gressive organ failure or hypoxemic respiratory failure, pul-monary artery catheterization may be a useful clinical manage-ment tool. The information available from a PAC can be usedto help determine the cause of shock and provide a guide forinterventions to maintain an appropriate cardiac output andintravascular volume to limit the risk of further progressionof organ dysfunction/failure. If PACs are beneficial in patientswith sepsis, the most likely candidates may be those in whomresuscitation by clinical assessment or CVP fails to reverse theprogression of organ failure.
Invasive monitoring using a pulmonary artery catheter is notrecommended for routine use in all patients with severe sep-sis. At least one major prospective, nonrandomized multicen-ter study has suggested increased length of stay, costs, and mor-tality in a cohort of risk-matched patients receiving a PAC in thefirst 24 hours after ICU admission (394). A recent multicenterrandomized controlled trial involving 676 subjects with shock(primarily septic), ARDS, or both has demonstrated no differ-ence in organ failure–free days, renal support needs, vasopres-sor requirements, mechanical ventilation, ICU/hospital lengthof stay (14 and 90 day), or mortality between subjects random-ized to pulmonary artery catheterization or controls (395). Asecond, smaller randomized trial of 200 patients (about 100with sepsis) also demonstrated no mortality difference with orwithout the use of PAC (396). Other smaller studies, includ-ing one randomized trial in high-risk operative patients, failedto demonstrate excess mortality with PAC use (397,398). Incontrast, one meta-analysis of RCTs demonstrated a reducedmortality risk in surgical ICU patients treated with PAC butno effect on mortality in medical or mixed ICU patients (399).On the basis of the total data available, routine use of PAC inpatients with sepsis or other critical illness cannot be recom-mended.
Specific Therapy
As discussed, patients with severe sepsis and septic shock mustfirst be treated using the following: (i) Appropriate resuscita-tion, (ii) broad spectrum antimicrobials, (iii) source control,and (iv) physiologic support of organ function in the intensivecare unit. Immunomodulatory therapy has been evaluated onlyin association with adequate treatment based on these four el-ements.
In the last few decades, the dominant hypotheses regardingthe pathogenesis of septic shock and septic organ dysfunctionfocused on inflammatory mediators including TNF α, IL-1β,interleukin-6, and platelet-activating factor. Several clinical tri-als have been performed evaluating both nonspecific inhibitorsof inflammation such as nonsteroidal anti-inflammatory drugsand high-dose glucocorticoids and specific immunomodulatoryagents such as monoclonal antibodies against TNF α and IL-1
receptor antagonist (400,401). Despite an expenditure of >1billion dollars, these studies have failed to demonstrate a sur-vival benefit. No primary immunomodulatory experimentalagent has received regulatory approval.
Recently accepted models of the pathogenesis of sepsis haveemphasized a central role for altered hemostatic/coagulantfunction. Three coagulation modulators have been assessedin large randomized controlled clinical trials: Tissue factorpathway inhibitor, antithrombin III, and drotrecogin alfa (acti-vated) (recombinant human activated protein C). Drotrecoginalfa (activated) is the first and, to date, only specific therapythat has been shown to improve survival in patients with se-vere sepsis and septic shock.
Recombinant human-activated protein C should be adminis-tered in patients with suspected sepsis with organ dysfunction.Acceptable criteria include, but are not necessarily limited to, aminimum of one organ dysfunction with an Acute Physiologyand Chronic Health Evaluation (APACHE) II score ≥25; orif an accurate APACHE 2 score is unavailable, the presenceof two or more organ dysfunctions. Although clinical trials ofmodulation of the coagulation cascade for treatment of sepsishave been performed with several agents (e.g., antithrombinIII [27], tissue factor pathway inhibitor [28]), only drotreco-gin alfa (activated) has been shown to improve mortality (26).The pivotal study was an international multicenter RCT thatcompared drotrecogin alfa (activated) to placebo used in con-junction with standard treatment (antibiotics, physiologic sup-port, and surgical source control) (26). Patients were enteredinto the study if they exhibited acute organ dysfunction dueto a suspected infection (severe sepsis) within a 24-hour win-dow. The study was stopped at a planned interim analysis be-cause of definitive statistical evidence that supported a benefi-cial treatment effect. Using an intention-to-treat analysis, thestudy demonstrated an absolute mortality reduction of 6.5%from 31.3% in the placebo group to 24.8% in the drotrecoginalfa (activated) group, yielding a highly significant 21% relativerisk reduction. Subsequent open-label studies of drotrecoginalfa (activated) using the same criteria as in the pivotal studyhave demonstrated a consistent mortality rate between 25.1%and 26.1% (402,403). A retrospective analysis of an open-label study suggests that earlier initiation of treatment (<24hours after diagnosis of severe sepsis) yields superior outcomes(404).
The original study demonstrated a differential treatment ef-fect based on either APACHE II scores or the number of acuteorgan dysfunctions present at the time of enrollment into thestudy. The absolute reduction in mortality was 1.7% amongpatients with a single dysfunctional organ and 7.4% amongthose with two or more dysfunctional organs (402,405). Sim-ilarly, there was no overall reduction in absolute mortality inthe first 2 quartiles of APACHE score (score <25), whereasthere was a 13% reduction in the last 2 quartiles (score ≥25)(405). A more recent RCT (prematurely terminated for futil-ity) has underlined concerns regarding the utility of drotrecoginalfa (activated) in relatively low-risk (generally APACHE<25or single organ failure) adult patients with a slight trend towardincreased mortality risk in the treatment arm (29). Similarly, astudy of drotrecogin alfa (activated) in pediatric septic shockwith respiratory failure was also prematurely terminated due toits futility, along with evidence of an increased central nervoussystem (CNS) bleeding risk in neonates (406).

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
28 Section VI: Shock States
Drotrecogin alfa (activated) remains approved for manage-ment of high-risk patients with severe sepsis/septic shock, butnew studies are ongoing to validate the continued use of thisagent.
Intravenous immune globulin should be considered for patientssuffering from streptococcal toxic shock syndrome. The po-tential utility of polyclonal immune globulin preparations forsevere sepsis and septic shock in general is uncertain at present.One meta-analysis has suggested that sepsis-related mortal-ity is significantly reduced when intravenous immunoglobulin(IVIG) is used in the management of such patients (407). Asmall randomized controlled trial of trauma patients has alsodemonstrated a reduced incidence of septic complications in-cluding pneumonia and other infections (other than catheter-related infections), although ICU length of stay and mortalitywere not reduced (408). Evidence favoring the use of poly-clonal immunoglobulin for defined invasive streptococcal in-fections, including streptococcal septic shock, is more defini-tive. A case-matching study has demonstrated an improved30-day survival in patients treated with intravenous polyclonalimmune globulin, while a randomized controlled trial (abortedprematurely due to low enrollment) has shown decreased earlysepsis-related organ failure with a trend toward improved sur-vival (409).
Immunosuppressive doses of corticosteroids are contraindi-cated in the management of sepsis and septic shock. In thepast, high-dose steroids had been advocated for sepsis with or-gan failure to dampen inflammatory responses and minimizeorgan dysfunction (410). Several large multicenter randomizedcontrolled trials have definitively demonstrated that adminis-tration of high dose (15–30 mg/kg methylprednisolone equiv-alent) corticosteroids fail to improve outcome in adult septicshock (411–414). In some of these studies, mortality in spe-cific subgroups appeared to be increased with steroid treatment(412).
Supportive Therapy
Although specific therapies for septic shock continue to bedeveloped, general supportive care, in conjunction with an-tibiotics, remains the standard of care. Fluid and vasopres-sor/inotropic support have been addressed in this chapter. Inaddition, there has been an explosion of data in recent yearsregarding the efficacy of other elements of supportive care in-cluding ventilatory strategies, intensity of dialysis, endocrinesupport, and glycemic management. In other key areas (e.g.,nutritional support), definitive data are lacking. Nonetheless,it is likely that an aggressive approach to optimization of sup-portive care, in combination with anti-infective therapy andresuscitative efforts, can improve morbidity and mortality. Forthat reason, application of appropriate support modalities in atimely manner should be the standard of care of septic patientsin all ICUs.
Intensive renal replacement therapy (daily intermittent dialysisor continuous renal replacement therapy) is indicated for se-vere sepsis or septic shock with renal failure. Indications foracute dialysis in the ICU population are not dissimilar to those
for other patients. These indications include volume overload,electrolyte imbalance, acid-base disturbances, elevated bloodurea nitrogen, uremic pericarditis, or uremic encephalopathy.Unfortunately, ICU patients, especially those with acute re-nal failure, may have altered hemodialysis kinetics such thatstandard intermittent dialysis may offer suboptimal urea clear-ance kinetics despite apparently equivalent doses. Comparedto standard intermittent dialysis, daily hemodialysis has beenshown to yield higher urea clearance and improved mortality inICU patients with acute renal failure (415). Similarly, anotherstudy has demonstrated that higher urea clearance with contin-uous venovenous hemodialysis yields reduced mortality (416).Whether these data can be extrapolated to include septic pa-tients with a background of chronic renal failure is unknown.Peritoneal dialysis is not appropriate since even high-frequencyexchanges yield relatively low urea clearance kinetics. A re-cent study of infection-related acute renal failure that includedcases of sepsis demonstrated increased mortality among thosetreated with peritoneal dialysis compared to those treated withhemodialysis (417).
Intensive insulin therapy maintaining a blood glucose of 4.4 to6.1 mmol/L (80–110 mg/dL) may be beneficial in critically illICU patients with severe sepsis. Hyperglycemia is a recognizedrisk factor for increased mortality in the critically ill indepen-dent of the APACHE II score (418). One single-center ran-domized, controlled, nonblinded trial has indicated that tightglycemic control in surgical ICU patients undergoing mechan-ical ventilation (mostly post–coronary artery bypass graft orother cardiovascular surgery) reduces the incidence of severesepsis and decreases mortality, primarily because of a decreasedincidence of multiple organ failure with septic foci (419).These data are consistent with other clinical and experimentalstudies suggesting the presence of granulocyte dysfunction andincreased risk of infection in postoperative surgical patientswith persistent hyperglycemia (420). However, another RCTby the same group has failed to demonstrate similar improve-ments in critically ill medical patients (421). A retrospectivesubgroup analysis, however, suggested mortality improvementin those patients admitted with an ICU length of stay of >3days. In addition, there was a decreased incidence of renal dys-function and critical illness polyneuropathy, with fewer days onventilator support and shorter ICU and hospital length of stay(421,422). No definitive data exist regarding the question ofwhether a tight control strategy is useful in patients who are al-ready septic. In addition, these data should be interpreted withcaution pending replication of these results in other centers.
Stress dose steroids may be administered at presentation to se-lected patients with septic shock pending the result of an ACTHstimulation test. Several previous large randomized, double-blind, multicenter trials have definitively demonstrated that ad-ministration of immunosuppressive (15–30 mg/kg methylpred-nisolone equivalent) corticosteroids fail to improve outcomein adult septic shock (411–414). However, some evidence sug-gests that low “stress-dose” corticosteroids may be beneficial.A relative adrenal insufficiency has been suggested to exist ina substantial subset of patients with septic shock (239,423).Among other deleterious effects, adrenal insufficiency canresult in impairment of catecholamine sensitivity (423–425). Administration of stress-dose steroids (150–300 mg

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 29
hydrocortisone daily equivalent) to patients with septic shockcan decrease pressor requirements while suppressing inflam-matory markers (424,426,427). One recent RCT has demon-strated that 7 days of therapy with hydrocortisone, 50 mg IVevery 6 hours, and fludrocortisone, 50 μg orally once daily,generates a significant reduction in mortality in patients withrelative adrenal insufficiency (428). Subgroup analysis demon-strated that this improvement was restricted to those who failto respond to an ACTH challenge (about 75% of septic shockpatients), with an increase in serum cortisol of ≥250 nmol/L(9 μg/dL). In the recent past, these data were interpreted assuggesting that patients with pressor-dependent septic shockshould undergo ACTH challenge on admission, followed im-mediately by initiation of stress-dose steroid therapy. If theACTH stimulation test was within normal limits, corticos-teroids were discontinued. If the test results indicated relativeadrenal insufficiency, hydrocortisone and fludrocortisone wereoften continued for 7 days or as otherwise clinically indicated.
The major uncertainty with regard to stress-dose steroidtherapy had been the appropriate test and value of serum cor-tisol to indicate adrenal insufficiency. Various studies supportedusing random cortisol levels between 275 and 950 nmol/L (10–35 μg/dL) during the acute stress, or increments of cortisol of250 nmol/L (9 μg/dL) within the first hour following ACTHstimulation (239,423,428). Although no definitive data existedas to which cutoff value was best, many clinicians considered arandom value of <400 nmol/L (15 μg/dL) to be sufficiently sug-gestive of relative adrenal insufficiency during the shock stateto initiate and continue stress-dose therapy. Similarly, a value>950 nmol/L (35 μg/dL) during shock has been thought to besufficiently normal to discontinue stress-dose therapy withoutfurther assessment. Values between those two extremes wereoften interpreted to be an indication for ACTH challenge witha response of <250 nmol/L (9 μg/dL) supporting the need forsteroid therapy. Unfortunately, a recent study has challengedthese accepted cutoffs in the critically ill by questioning thescientific validity of using total as opposed to free serum con-centrations of serum cortisol in such patients (429).
Of most concern, a major multicenter, placebo-controlled,double-blind RCT of septic shock has failed to confirm animprovement in survival regardless of ACTH responsiveness(430). The steroid group did exhibit a reduction in pressor daysbut also had a higher incidence of superinfections and associ-ated sepsis/septic shock events. Confounding these results, thesteroid regimen (hydrocortisone alone) differed from the regi-men used in the previous positive study and could also be im-plemented as late as 72 hours following onset of septic shock.Based on these data, stress-dose or low-dose steroid therapyshould not be considered part of the routine management ofseptic shock pending further definitive trials.
Low-volume (6–8 mL/kg ideal body weight), pressure-limitedventilation is indicated in patients with sepsis-associated acutelung injury or acute respiratory distress syndrome. Animal andhuman studies have suggested that high levels of PEEP and largetidal volumes are associated with increased pulmonary genera-tion of proinflammatory cytokines (431,432) and ventilation-induced lung injury (433). ALI and ARDS represent a mani-festation of MODS that may occur in conjunction with severesepsis and septic shock. Septic patients with bilateral persistent
opacities, in association with an acute and persistent defect ofoxygenation (PaO2/FiO2 ratio of ≤200 for ARDS and ≤300 forALI) and no clinical evidence of left atrial hypertension or a pul-monary wedge pressure of ≥18 mm Hg, fit the criteria for thissyndrome (434). Small randomized studies have supported thepossibility that a lung-protective strategy using low tidal vol-umes and limited airway pressures may decrease pulmonaryinjury and decrease mortality (435). A single large multicenter,randomized controlled trial has demonstrated that ventilationof critically ill patients with ARDS with a low tidal volume(tidal volume of 6–8 mL/kg ideal body weight) reduces all-causeabsolute mortality by 10% (from 40% to 30%; 25% relativerisk reduction). Patients with severe sepsis or septic shock whomeet criteria for ALI or ARDS should be ventilated with alow-volume, pressure-limited strategy. Available evidence sug-gests that ventilation of patients at risk for ALI/ARDS with thisstrategy does not prevent the development of this pulmonarysyndrome (436).
Endotracheal intubation and mechanical ventilation should beconsidered early in the management of all patients with sep-sis and organ failure. Airway intubation is indicated for allpatients with impaired airway protection reflexes (e.g., as aconsequence of cerebral hypoperfusion or septic encephalopa-thy), refractory hypoxemia, respiratory acidosis, or respiratorydistress associated with ongoing hypotension/hypoperfusion.Though not yet addressed by systematic studies, clinical ex-perience suggests that respiratory arrest is a significant risk insuch patients. These observations are consistent with observa-tions of respiratory muscle compromise and respiratory failurein animal models of septic shock (437,438).
Enteral feeding should be considered within 24 hours of admis-sion to the ICU for most patients with sepsis and septic shock.Parenteral feeding should be used only if enteral feeding is notpossible despite best efforts. Recent meta-analyses suggest thatearly enteral feeding lowers the risk of infection and improvessurvival compared to delayed feeding in the critically ill (439).These findings are consistent with animal studies demonstrat-ing that enteral nutrition maintains gut mucosal integrity, de-creases bacterial translocation, and limits the systemic inflam-matory response to bacterial toxins (440). Diminished bowelsounds should not prevent a trial of enteral feeding. Few pa-tients will fail to tolerate enteral feeding if a small bowel tube isused. Studies of parenteral feeding in the ICU have, in general,failed to demonstrate an improvement in mortality in criticallyill patients (441). Other studies demonstrate the superiorityof enteral over parenteral feeding in critically ill patients withrespect to costs and complications, including risk of infection(440,442).
Intravenous administration of sodium bicarbonate is not indi-cated for sepsis-associated metabolic acidosis with a pH ≥7.15.Human investigations demonstrate that intravenous adminis-tration of sodium bicarbonate for lactic acidosis (pH ≥7.15)associated with septic shock does not improve cardiac perfor-mance or reduce vasopressor requirements compared to admin-istration of an equimolar amount of normal saline (443,444).No human data exist in regard to the effect of intravenous bi-carbonate administration for more severe degrees of metabolicacidosis.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12T
AB
LE
57
.15
TIM
EL
INE
OF
IMPL
EM
EN
TA
TIO
NO
FR
EC
OM
ME
ND
ED
DIA
GN
OST
ICA
ND
TH
ER
APE
UT
ICIN
TE
RV
EN
TIO
NS
Res
usci
tati
onA
ntim
icro
bial
sV
asop
ress
ors/
Inot
rope
sM
onit
orin
gSp
ecifi
cT
hera
pySu
ppor
tive
The
rapy
Firs
tho
ur-I
niti
ate
crys
tallo
idflu
idre
susc
itat
ion
(500
mL
ever
y10
–15
min
),ti
trat
ing
toH
R<
100,
MA
P≥6
5m
mH
g,an
dur
ine
outp
ut≥0
.5m
L/h
-Ini
tiat
eem
piri
c,br
oad-
spec
trum
,hig
h-do
sean
tim
icro
bial
ther
apy
wit
htw
oor
mor
eci
dal
drug
sw
here
poss
ible
-Im
plem
ent
cont
inuo
usm
onit
orin
gof
EC
G,
arte
rial
satu
rati
on,
bloo
dpr
essu
rean
dU
O
-Sup
plem
enta
loxy
gen
-Con
side
rin
tuba
tion
and
mec
hani
calv
enti
lati
onpr
ior
toov
ert
resp
irat
ory
dist
ress
1–8
hour
s-T
itra
teflu
idre
susc
itat
ion
toel
imin
atio
nof
base
defic
itan
dno
rmal
izat
ion
ofse
rum
lact
ate
-Ini
tiat
era
diog
raph
icin
vest
igat
ion
for
loca
lizat
ion
and
delin
eati
onof
infe
ctio
n-I
mpl
emen
tso
urce
cont
roli
fne
cess
ary
-Ini
tiat
eva
sopr
esso
rth
erap
yif
circ
ulat
ory
shoc
kpe
rsis
tsfo
llow
ing
adeq
uate
fluid
resu
scit
atio
n-I
niti
ate
inot
rope
sif
CI
orSv
O2
are
pers
iste
ntly
decr
ease
d
-IC
Utr
ansf
erw
ith
full
mon
itor
ing
supp
ort
-Art
eria
lcat
hete
ras
sess
men
t-I
fsh
ock
pers
ists
wit
h>
2L
crys
tallo
idre
susc
itat
ion,
veno
usca
thet
eras
sess
men
t±
plac
emen
t(g
oal
CV
P≥8
mm
Hg)
-Con
side
rlo
w-d
ose
ster
oid
ther
apy
±A
CT
Hst
imul
atio
nte
st
8–24
hour
s-D
ynam
icev
alua
tion
ofre
susc
itat
ive
goal
s(b
ased
oncl
inic
alan
din
vasi
vem
onit
orin
gen
dpo
ints
)
-Con
side
rva
sopr
essi
nif
shoc
kre
frac
tory
tofir
st-l
ine
vaso
pres
sors
pers
ists
-If
pers
iste
ntly
pres
sor
depe
nden
taf
ter
3–5
Lcr
ysta
lloid
infu
sion
,C
VP
≥8ac
hiev
ed,
susp
icio
nof
intr
avas
cula
rvo
lum
ede
plet
ion
orlim
ited
card
iova
scul
arre
serv
e,PA
Cpl
acem
ent
(ini
tial
goal
PWP
12–1
5m
mH
g)-M
aybe
inse
rted
earl
ier
ifcl
inic
ally
indi
cate
d
-Con
side
rin
itia
tion
ofdr
otre
cogi
n-al
fa(a
ctiv
ated
)if
sing
leor
gan
failu
rew
ith
APA
CH
EII
≥25,
two
orm
ore
orga
nfa
ilure
sin
abse
nce
ofA
PAC
HE
scor
e
-Ini
tiat
een
tera
lfee
ding
-Con
side
rin
tens
ive
insu
linth
erap
y
>24
hour
s-N
arro
wan
tim
icro
bial
regi
men
depe
ndin
gon
isol
atio
nof
path
ogen
icor
gani
sms
and/
orcl
inic
alim
prov
emen
t-R
eass
ess
nece
ssit
yfo
ror
effic
acy
ofso
urce
cont
rol
-Con
side
rPA
Cin
vaso
pres
sor-
depe
nden
tpa
tien
tsw
ith
prog
ress
ive
resp
irat
ory,
rena
l,or
mul
tipl
eor
gan
dysf
unct
ion
-Int
ensi
vehe
mod
ialy
sis
ther
apy
for
rena
lfai
lure
-Low
-pre
ssur
e,vo
lum
e-lim
ited
vent
ilati
onfo
rA
RD
S
HR
,hea
rtra
te;M
AP,
mea
nar
teri
albl
ood
pres
sure
;EC
G,e
lect
roen
ceph
alog
raph
;UO
,uri
neou
tput
;Cl,
chlo
rine
;SvO
2,m
ixed
veno
usox
ygen
satu
rati
on;C
VP,
cent
ralv
enou
spr
essu
re;A
CT
H,
adre
noco
rtic
otro
pin
horm
one;
PAC
,pul
mon
ary
arte
ryca
thet
er;P
WP,
pulm
onar
yw
edge
pres
sure
;APA
CH
E,A
cute
Phys
iolo
gyan
dC
hron
icH
ealt
hE
valu
atio
n;A
RD
S,ac
ute
resp
irat
ory
dist
ress
synd
rom
e.
30

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 31
CONCLUSION
Severe sepsis and septic shock continue to be a major causeof mortality and morbidity among patients requiring ICU sup-port. In recent years, both basic and clinical research in the fieldhave accelerated substantially. This has led to the publicationof several studies with major implications regarding the appro-priate management of patients with these conditions. Many ofthese new studies relate to optimization of supportive care.Although controversial, a single specific therapy, drotrecoginalfa (activated), has been shown to improve mortality in se-vere sepsis and septic shock. Few major studies in the areas offluid resuscitation, vasopressors/inotropes, invasive and non-invasive monitoring, or antimicrobial therapy have been pub-lished in recent years. Nonetheless, outcome can most likely beimproved by taking a systematic approach to therapy as de-scribed in Table 57.15. Although significant improvements inTable
57.15 outcome have been made possible by new pharmacologic ther-apies, recent studies focusing on antimicrobial and supportiveelements clearly demonstrate that close attention to establishedtherapies can have a substantial impact on survival in severesepsis and septic shock.
References
1. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severesepsis in the United States: analysis of incidence, outcome, and associatedcosts of care. Crit Care Med. 2001;29(7):1303–1310.
2. Finland M, Jones WF, Barnes MW. Occurence of serious bacterial infectionssince the introduction of antibacterial agents. JAMA. 1959;84:2188–2197.
3. Hemminki E, Paakkulainen A. Effect of antibiotics on mortality from infec-tious diseases in Sweden and Finland. Am J Public Health. 1976;66:1180–1184.
4. Kreger BE, Craven DE, McCabe WR. Gram-negative bacteremia. IV. Re-evaluation of clinical features and treatment in 612 patients. Am J Med.1980;68(3):344–355.
5. Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in theUnited States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–1554.
6. Minino AM, Heron MP, Smith BL. Deaths: preliminary data for 2004. NatlVital Stat Rep. 2006;54(19):1–49.
7. Friedman G, Silva E, Vincent JL. Has the mortality of septic shock changedwith time? Crit Care Med. 1998;26(12):2078–2086.
8. Geroulanos S, Douka ET. Historical perspective of the word “sepsis”. In-tensive Care Med. 2006;32:2077.
9. Budelmann G. Hugo Schottmuller, 1867–1936. The problem of sepsis [inGerman]. Internist (Berl). 1969;10(3):92–101.
10. Bone R. American College of Chest Physicians/Society of Critical CareMedicine Consensus Conference: definitions for sepsis and organ failureand guidelines for the use of innovative therapies in sepsis. Crit Care Med.1992;20:864–874.
11. Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250–1256.
12. Marshall JC, Cook DJ, Christou NV, et al. Multiple organ dysfunctionscore: a reliable descriptor of a complex clinical outcome. Crit Care Med.1995;23(10):1638–1652.
13. Ferreira FL, Bota DP, Bross A, et al. Serial evaluation of the SOFA score topredict outcome in critically ill patients. JAMA. 2001;286(14):1754–1758.
14. Bone RC, Bone RC. Immunologic dissonance: a continuing evolution inour understanding of the systemic inflammatory response syndrome (SIRS)and the multiple organ dysfunction syndrome (MODS). Ann Intern Med.1996;125(8):680–687.
15. Padkin A, Goldfrad C, Brady AR, et al. Epidemiology of severe sepsis oc-curring in the first 24 hrs in intensive care units in England, Wales, andNorthern Ireland. Crit Care Med. 2003;31(9):2332–2338.
16. Finfer SBR, Bellomo R, Lipman J, et al. Adult-population incidence of severesepsis in Australian and New Zealand intensive care units. Intensive CareMed. 2004;30:589–596.
17. Brun-Buisson C, Meshaka P, Pinton P, et al. EPISEPSIS: a reappraisal of theepidemiology and outcome of severe sepsis in French intensive care units.Intensive Care Med. 2004;30(4):580–588.
18. Sundararajan V, Macisaac CM, Presneill JJ, et al. Epidemiology of sepsisin Victoria, Australia. Crit Care Med. 2005;33(1):71–80.
19. Danai P, Martin GS. Epidemiology of sepsis: recent advances. Curr InfectDis Rep. 2005;7:329–334.
20. Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and out-come of severe sepsis and septic shock in adults. A multicenter prospectivestudy in intensive care units. French ICU Group for Severe Sepsis. JAMA.1995;274:968–974.
21. Annane D, Aegerter P, Jars-Guincestre MC, et al. Current epidemiol-ogy of septic shock: the CUB-Rea Network. Am J Resp Crit Care Med.2003;168(2):165–172.
22. Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndromein 8 academic medical centers. JAMA. 1997;278(3):234–240.
23. Pakhale S, Roberts D, Light B, et al. A geographically and temporally com-prehensive analysis of septic shock: impact of age, sex and socioeconomicstatus. Crit Care Med. 2005;33:A79.
24. Zhan C, Miller MR. Excess length of stay, charges, and mortalityattributable to medical injuries during hospitalization. JAMA. 2003;290(14):1868–1874.
25. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension be-fore initiation of effective antimicrobial therapy is the critical determi-nant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596.
26. Bernard GR, Vincent JL, Laterre PF. Efficacy and safety of recombinanthuman activated protein C for severe sepsis. N Engl J Med. 2001;344:699–709.
27. Warren BL, Eid A, Singer P, et al. High-dose antithrombin III in se-vere sepsis: a randomized controlled trial. JAMA. 2001;286(15):1869–1878.
28. Abraham E, Reinhart K, Opal S, et al. Efficacy and safety of tifacogin(recombinant tissue factor pathway inhibitor) in severe sepsis: a randomizedcontrolled trial. JAMA. 2003;290(2):238–247.
29. Abraham E, Laterre PF, Garg R, et al. Drotrecogin alfa (activated) foradults with severe sepsis and a low risk of death. N Engl J Med. 2005;353(13):1332–1341.
30. O’Brien JM Jr, Lu B, Ali NA, et al. Alcohol dependence is independentlyassociated with sepsis, septic shock, and hospital mortality among adultintensive care unit patients. Crit Care Med. 2007;35(2):345–350.
31. Rangel-Frausto MS, Pittet D, Costigan M, et al. The natural history ofthe systemic inflammatory response syndrome (SIRS). A prospective study[comment]. JAMA. 1995;273(2):117–123.
32. Loeb HS, Cruz A, Teng CY, et al. Haemodynamic studies in shock associ-ated with infection. Br Heart J. 1967;29(6):883–894.
33. Weil MH, Shubin H, Biddle M. Shock caused by gram-negative microor-ganisms. Ann Intern Med. 1964;60:384–400.
34. Kasal J, Jovanovic Z, Clermont G, et al. Comparison of Cox and Gray’ssurvival models in severe sepsis. Crit Care Med. 2004;32(3):700–707.
35. Parker MM, Shelhamer JH, Natanson C, et al. Serial cardiovascular vari-ables in survivors and nonsurvivors of human septic shock: Heart rate asan early predictor of prognosis. Crit Care Med. 1987;15:923–929.
36. Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsis andinfection in ICU patients from an international multicentre cohort study.Intensive Care Med. 2002;28(2):108–121.
37. Richards MJ, Edwards JR, Culver DH, et al. Nosocomial infections in medi-cal intensive care units in the United States. National Nosocomial InfectionsSurveillance System. Crit Care Med. 1999;27(5):887–892.
38. Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstreaminfections in US hospitals: analysis of. 24,179 cases from a prospectivenationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317.
39. Macphail GL, Taylor GD, Buchanan-Chell M, et al. Epidemiology, treat-ment and outcome of candidemia: a five-year review at three Canadianhospitals. Mycoses. 2002;45(5-6):141–145.
40. Berrouane YF, Herwaldt LA, Pfaller MA, et al. Trends in antifungal useand epidemiology of nosocomial yeast infections in a university hospital. JClin Microbiol. 1999;37(3):531–537.
41. Abi-Said D, Anaissie E, Uzun O, et al. The epidemiology of hematoge-nous candidiasis caused by different Candida species. Clin Infect Dis. 1997;24(6):1122–1128.
42. Murray BE, Murray BE. Vancomycin-resistant enterococcal infections. NEngl J Med. 2000;342(10):710–721.
43. Giamarellou H. Multidrug resistance in Gram-negative bacteria that pro-duce extended-spectrum beta-lactamases (ESBLs). Clin Microbiol Infect.2005;11(Suppl 4):1–16.
44. Miller LG, Perdreau-Remington F, Rieg G, et al. Necrotizing fasciitis causedby community-associated methicillin-resistant Staphylococcus aureus inLos Angeles. N Engl J Med. 2005;352(14):1445–1453.
45. From the Centers for Disease Control. Staphylococcus aureus resistant tovancomycin–United States, 2002. JAMA. 2002;288(7):824–825.
46. Heumann D, Glauser MP, Calandra T. Molecular basis of host-pathogeninteraction in septic shock. Curr Opin Microbiol. 1998;1(1):49–55.
47. Hemmi H, Takeuchi O, Kawai T, et al. A Toll-like receptor recognizesbacterial DNA. Nature. 2000;408(6813):740–745.
48. Bauer S, Kirschning CJ, Hacker H, et al. Human TLR9 confers respon-siveness to bacterial DNA via species-specific CpG motif recognition. ProcNatl Acad Sci U S A. 2001;98(16):9237–9242.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
32 Section VI: Shock States
49. Sparwasser T, Miethke T, Lipford G, et al. Bacterial DNA causes septicshock. Nature. 1997;386(6623):336–337.
50. Alexopoulou L, Holt AC, Medzhitov R, et al. Recognition of double-stranded RNA and activation of NF-kappaB by Toll-like receptor 3. Nature.2001;413(6857):732–738.
51. Dziarski R, Wang Q, Miyake K, et al. MD-2 enables Toll-like receptor2 (TLR2)-mediated responses to lipopolysaccharide and enhances TLR2-mediated responses to Gram-positive and Gram-negative bacteria and theircell wall components. J Immunol. 2001;166(3):1938–1944.
52. Yang RB, Mark MR, Gray A, et al. Toll-like receptor-2 mediateslipopolysaccharide-induced cellular signalling. Nature. 1998;395(6699):284–288.
53. Lien E, Sellati TJ, Yoshimura A, et al. Toll-like receptor 2 functions as apattern recognition receptor for diverse bacterial products. J Biol Chem.1999;274(47):33419–33425.
54. Schwandner R, Dziarski R, Wesche H, et al. Peptidoglycan- and lipoteichoicacid-induced cell activation is mediated by toll-like receptor 2. J Biol Chem.1999;274(25):17406–17409.
55. Manocha S, Feinstein D, Kumar A, et al. Novel therapies for sepsis: antien-dotoxin therapies. Exp Opin Invest Drugs. 2002;11(12):1795–1812.
56. Martich GD, Boujoukos AJ, Suffredini AF. Response of man to endotoxin.Immunobiology. 1993;187(3–5):403–416.
57. Ing DJ, Zang J, Dzau VJ, et al. Modulation of cytokine-induced cardiacmyocyte apoptosis by nitric oxide, Bak, and Bcl-x. Circ Res. 1999;84:21–33.
58. Albelda SM, Smith CW, Ward PA. Adhesion molecules and inflammatoryinjury. FASEB J. 1994;8:504–512.
59. Balligand JL, Ungureanu-Longrois D, Simmons WW, et al. Cytokine-inducible nitric oxide synthase (iNOS) expression in cardiac myocytes. JBiol Chem. 1994;269:27580–27588.
60. Esmon CT. Role of coagulation inhibitors in inflammation. ThrombHaemost. 2001;86(1):51–56.
61. Heumann D. CD14 and LBP in endotoxemia and infections caused byGram-negative bacteria. J Endotoxin Res. 2001;7(6):439–441.
62. Raetz CR, Ulevitch RJ, Wright SD, et al. Gram-negative endotoxin: anextraordinary lipid with profound effects on eukaryotic signal transduction.FASEB J. 1991;5(12):2652–2660.
63. Rietschel ET, Kirikae T, Schade FU, et al. Bacterial endotoxin: molecularrelationships of structure to activity and function. FASEB J. 1994;8(2):217–225.
64. Hellman J, Warren HS. Antiendotoxin strategies. Infect Dis Clin NorthAm. 1999;13(2):371–386.
65. Kumar A, Zanotti S, Bunnell G, et al. Interleukin-10 blunts the humaninflammatory response to lipopolysaccharide without affecting the cardio-vascular response. Crit Care Med. 2005;33(2):331–340.
66. Kumar A, Bunnell E, Lynn M, et al. Experimental human endotox-emia is associated with depression of load-independent contractility in-dices: prevention by the lipid a analogue E5531. Chest. 2004;126(3):860–867.
67. Suffredini AF, Reda D, Banks SM, et al. Effects of recombinant dimericTNF receptor on human inflammatory responses following intravenousendotoxin administration. J Immunol. 1995;155(10):5038–5045.
68. Le Roy D, Di Padova F, Tees R, et al. Monoclonal antibodies to murinelipopolysaccharide (LPS)-binding protein (LBP) protect mice from lethal en-dotoxemia by blocking either the binding of LPS to LBP or the presentationof LPS/LBP complexes to CD14. J Immunol. 1999;162(12):7454–7460.
69. Schumann RR, Leong SR, Flaggs GW, et al. Structure and function oflipopolysaccharide binding protein. Science. 1990;249(4975):1429–1431.
70. Heumann D, Barras C, Severin A, et al. Gram-positive cell walls stimu-late synthesis of tumor necrosis factor alpha and interleukin-6 by humanmonocytes. Infect Immun. 1994;62(7):2715–2721.
71. Mattsson E, Rollof J, Verhoef J, et al. Serum-induced potentiation of tu-mor necrosis factor alpha production by human monocytes in responseto staphylococcal peptidoglycan: involvement of different serum factors.Infect Immun. 1994;62(9):3837–3843.
72. Wright SD, Ramos RA, Tobias PS, et al. CD14, a receptor for com-plexes of lipopolysaccharide (LPS) and LPS binding protein. Science. 1990;249(4975):1431–1433.
73. Hailman E, Lichenstein HS, Wurfel MM, et al. Lipopolysaccharide (LPS)-binding protein accelerates the binding of LPS to CD14. J Exp Med. 1994;179(1):269–277.
74. Ingalls RR, Golenbock DT, Ingalls RR, et al. CD11c/CD18, a trans-membrane signaling receptor for lipopolysaccharide. J Exp Med. 1995;181(4):1473–1479.
75. Kusunoki T, Hailman E, Juan TS, et al. Molecules from Staphylococcusaureus that bind CD14 and stimulate innate immune responses. J Exp Med.1995;182(6):1673–1682.
76. Kirschning CJ, Wesche H, Merrill AT, et al. Human toll-like recep-tor 2 confers responsiveness to bacterial lipopolysaccharide. J Exp Med.1998;188(11):2091–2097.
77. Hoshino K, Takeuchi O, Kawai T, et al. Cutting edge: Toll-like recep-tor 4 (TLR4)-deficient mice are hyporesponsive to lipopolysaccharide: ev-idence for TLR4 as the Lps gene product. J Immunol. 1999;162(7):3749–3752.
78. Takeuchi O, Hoshino K, Kawai T, et al. Differential roles of TLR2 and
TLR4 in recognition of gram-negative and gram-positive bacterial cell wallcomponents. Immunity. 1999;11(4):443–451.
79. Chow JC, Young DW, Golenbock D, et al. Toll-like receptor-4 medi-ates lipopolysaccharide-induced signal transduction. J Biol Chem. 1999;274(16):10689–10692.
80. Tauszig S, Jouanguy E, Hoffmann JA, et al. Toll-related receptors and thecontrol of antimicrobial peptide expression in Drosophila. Proc Natl AcadSci U S A. 2000;97(19):10520–10525.
81. Lien E, Means TK, Heine H, et al. Toll-like receptor 4 imparts ligand-specific recognition of bacterial lipopolysaccharide. J Clin Invest. 2000;105(4):497–504.
82. Muroi M, Ohnishi T, Tanamoto K, et al. MD-2, a novel accessory molecule,is involved in species-specific actions of Salmonella lipid A. Infect Immun.2002;70(7):3546–3550.
83. Muroi M, Ohnishi T, Tanamoto K, et al. Regions of the mouse CD14molecule required for toll-like receptor. 2- and 4-mediated activation ofNF-kappa B. J Biol Chem. 2002;277(44):42372–42379.
84. Muller-Alouf H, Alouf JE, Gerlach D, et al. Human pro- and anti-inflammatory cytokine patterns induced by Streptococcus pyogenes ery-throgenic (pyrogenic) exotoxin A and C superantigens. Infect Immun.1996;64(4):1450–1453.
85. Cohen J. The immunopathogenesis of sepsis. Review. Nature. 2002;420(6917):885–891.
86. Docke WD, Randow F, Syrbe U, et al. Monocyte deactivation in septic pa-tients: restoration by IFN-gamma treatment. Nature Med. 1997;3(6):678–681.
87. Mira JP, Cariou A, Grall F, et al. Association of TNF2, a TNF-alpha pro-moter polymorphism, with septic shock susceptibility and mortality: a mul-ticenter study. JAMA. 1999;282(6):561–568.
88. Holmes CL, Russell JA, Walley KR. Genetic polymorphisms in sepsis andseptic shock: role in prognosis and potential for therapy. Chest. 2003;124:1103–1115.
89. Nathan C. Nitric oxide as a secretory product of mammalian cells. FASEBJ. 1992;6:3051–3064.
90. Lorente JA, Landin L, Renes E, et al. Role of nitric oxide in the hemody-namic changes of sepsis. Crit Care Med. 1993;21:759–767.
91. Kilbourn RG, Gross SS, Jubran A, et al. N-methyl-L-arginine inhibits tumornecrosis factor-induced hypotension: implications for the involvement ofnitric oxide. Proc Natl Acad Sci U S A. 1990;87:3629–3623.
92. Thiemermann C, Szabo C, Mitchell JA, et al. Vascular hyporeactivity tovasoconstrictor agents and hemodynamic decompensation in hemorrhagicshock is mediated by nitric oxide. Proc Natl Acad Sci U S A. 1993;90:267–271.
93. Kubes P. Nitric oxide modulates microvascular permeability. Am J Physiol.1992;262(2):H611–H615.
94. Kumar A, Thota V, Dee L, et al. Tumor necrosis factor-alpha andinterleukin-1 beta are responsible for depression of in vitro myocardialcell contractility induced by serum from humans with septic shock. J ExpMed. 1996;183:949–958.
95. Kumar A, Krieger A, Symeoneides S, et al. Myocardial dysfunction in septicshock, II: role of cytokines and nitric oxide. J Cardiovasc Thorac Anesth.2001;15(4):485–511.
96. Beckman JS, Beckman TW, Chen J, et al. Apparent hydroxyl radicalproduction by peroxynitrite: implications for endothelial injury from ni-tric oxide and superoxide. Proc Natl Acad Sci U S A. 1990;87(4):1620–1624.
97. Muta T, Iwanaga S, Muta T, et al. Clotting and immune defense in Limul-idae. Progr Molec Subcell Biol. 1996;15:154–189.
98. Nachum R, Nachum R. Antimicrobial defense mechanisms in Limuluspolyphemus. Progr Clin Biol Res U S A. 1979;29:513–524.
99. McGilvray ID, Rotstein OD, McGilvray ID, et al. Role of the coagulationsystem in the local and systemic inflammatory response. World J Surg.1998;22(2):179–186.
100. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl JMed. 1999;340:207–214.
101. Gando S, Nanzaki S, Sasaki S. Activation of the extrinsic coagulationpathway in patients with severe sepsis and septic shock. Crit Care Med.1998;26:2005–2009.
102. Mesters R, Helterbrand J, Utterback BG. Prognostic value of protein Cconcentrations in neutropenic patients at high risk of severe septic compli-cations. Crit Care Med. 2000;28:2209–2216.
103. Rosenberg RD, Aird WC. Vascular-bed-specific hemostasis and hypercoag-ulable states. N Engl J Med. 1999;340:1555–1564.
104. van der Poll T, Bueller HR, ten Cate H, et al. Activation of coagulationafter administration of tumor necrosis factor to normal subjects. N Engl JMed. 1990;322:1622–1627.
105. Esmon NL, Esmon CT. Protein C and the endothelium. Semin ThrombHemost. 1988;14:210–215.
106. Mesters R, Mannucci PM, Coppola E. Factor VIIA and anti-thrombin IIIactivity during severe sepsis and septic shock in neutropenic patients. Blood.1996;88:881–886.
107. Abraham E. Tissue factor inhibition and clinical trial results of tissue factorpathway inhibitor in sepsis. Crit Care Med. 2000;28(9 Suppl):S31–S33.
108. Abraham E, Reinhart K, Svoboda P, et al. Assessment of the safety ofrecombinant tissue factor pathway inhibitor in patients with severe sepsis:

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 33
a multicenter, randomized, placebo-controlled, single-blind, dose escalationstudy. Crit Care Med. 2001;29(11):2081–2089.
109. Sorensen TI, Nielsen GG, Andersen PK, et al. Genetic and environmentalinfluences on premature death in adult adoptees. N Engl J Med. 1988;318(12):727–732.
110. Udhoji VN, Weil MH. Hemodynamic and metabolic studies on shock as-sociated with bacteremia. Ann Intern Med. 1965;62:966–978.
111. Cohn JD, Greenspan M, Goldstein CR, et al. Arteriovenous shunting in highcardiac output shock syndromes. Surg Gynecol Obstet. 1968;127:282–288.
112. Thijs LG, Groenveld ABJ. Peripheral circulation in septic shock. Appl Car-diopul, Pathol. 1988;2:203–214.
113. Wright CJ, Duff JH, McLean APH, et al. Regional capillary blood flow andoxygen uptake in severe sepsis. Surg Gynecol Obstet. 1971;132:637–644.
114. Finley RJ, Duff JH, Holliday RL, et al. Capillary muscle blood flow inhuman sepsis. Surgery. 1975;78:87–94.
115. Cronenwett JL, Lindenauer SM. Direct measurement of arteriovenous anas-tomic blood flow in the septic canine hindlimb. Surgery. 1979;85:275–282.
116. Dantzker D. Oxygen delivery and utilization in sepsis. Crit Care Clin. 1989;5:81–98.
117. Wolf YG, Cotev S, Perel A, et al. Dependence of oxygen consumption oncardiac output in sepsis. Crit Care Med. 1987;15:198–203.
118. Shoemaker WC, Chang P, Czer L, et al. Cardiorespiratory monitoring inpostoperative patients, I: prediction of outcome and severity of illness. CritCare Med. 1979;7:237–242.
119. Haupt MT, Gilbert EM, Carlson RW. Fluid loading increases oxygenconsumption in septic patients with lactic acidosis. Am Rev Respir Dis.1985;131:912–916.
120. Samsel RW, Nelson DP, Sanders WM, et al. Effect of endotoxin on systemicand skeletal muscle oxygen extraction. J Appl Physiol. 1988;65:1377–1382.
121. Vincent JL, Roman A, DeBacker D, et al. Oxygen uptake/supply depen-dency: effects of short-term dobutamine infusion. Am Rev Respir Dis.1990;142:2–8.
122. Fenwick JC, Dodek PM, Ronco JJ, et al. Increased concentrations of plasmalactate predict pathological dependence of oxygen consumption on oxygendelivery in patients with adult respiratory distress syndrome. J Crit Care.1990;5:81–87.
123. Gutierrez G, Pohil RJ. Oxygen consumption is linearly related to oxygensupply in critically ill patients. J Crit Care. 1986;1:45–53.
124. Barcroft J. On anoxaemia. Lancet. 1920;2:485–492.125. Astiz M, Rackow EC, Weil MH, et al. Early impairment of oxidative
metabolism and energy production in severe sepsis. Circ Shock. 1988;26:311–320.
126. Mizock B. Septic shock: a metabolic perspective. Arch Intern Med. 1984;144:579–585.
127. Fink MP. Cytopathic hypoxia. Mitochondrial dysfunction as mechanismcontributing to organ dysfunction in sepsis. Crit Care Clin. 2001;17(1):219–237.
128. VanderMeer TJ, Wang H, Fink MP. Endotoxemia causes ileal mucosal aci-dosis in the absence of mucosal hypoxia in a normodynamic porcine modelof septic shock. Crit Care Med. 1995;23(7):1217–1226.
129. Hotchkiss RS, Rust RS, Dence CS, et al. Evaluation of the role of cellularhypoxia in sepsis by the hypoxic marker [18F] fluoromisonidazole. Am JPhysiol. 1991;261:R965–R972.
130. King CJ, Tytgat S, Delude RL, et al. Ileal mucosal oxygen consumption isdecreased in endotoxemic rats but is restored toward normal by treatmentwith aminoguanidine. Crit Care Med. 1999;27(11):2518–2524.
131. Simonson SG, Welty-Wolf K, Huang YT, et al. Altered mitochondrialredox responses in gram negative septic shock in primates. Circ Shock.1994;43(1):34–43.
132. Brealey D, Brand M, Hargreaves I, et al. Association between mito-chondrial dysfunction and severity and outcome of septic shock. Lancet.2002;360(9328):219–223.
133. Griebel JA, Moore FA, Piantadosi CA. In-vivo responses of mitochon-drial redox levels to Escherichia coli bacteremia in primates. J Crit Care.1990;5:1–9.
134. Cairns CB, Moore FA, Haenel JB, et al. Evidence for early supply inde-pendent mitochondrial dysfunction in patients developing multiple organfailure after trauma. J Trauma. 1997;42(3):532–536.
135. Mori E, Hasebe M, Kobayashi K, et al. Alterations in metabolite levels incarbohydrate and energy metabolism of rat in hemororrhagic shock andsepsis. Metabolism. 1987;36:14–20.
136. Tanaka J, Sato T, Kamiyama Y, et al. Bacteremic shock: aspects of high-energy metabolism of rat liver following Escherichia coli injection. J SurgRes. 1982;33:49–57.
137. Yassen KA, Galley HF, Lee A, et al. Mitochondrial redox state in the criti-cally ill. Br J Anaesth. 1999;83(2):325–327.
138. Grum CM, Simon RH, Dantzker D, et al. Evidence for adenosine triphos-phate degradation in critically ill patients. Chest. 1985;88:763–767.
139. Ozawa K, Aoyama H, Yasuda K, et al. Metabolic abnormalities associatedwith postoperative organ failure. A redox theory. Arch Surg. 1983;118(11):1245–1251.
140. Bergstrom J, Bostrom H, Furst P, et al. Preliminary studies of energy-richphosphagens in muscle from severely ill patients. Crit Care Med. 1976;4(4):197–204.
141. Liaw KY, Askanazi J, Michelson CB, et al. Effect of injury and sepsis onhigh-energy phosphates in muscle and red cells. J Trauma. 1980;20(9):755–759.
142. Song SK, Hotchkiss RS, Karl IE, et al. Concurrent quantification of tis-sue metabolism and blood flow via 2H/31P NMR in vivo, III: alterationsof muscle blood flow and metabolism during sepsis. Magn Reson Med.1992;25:67–77.
143. Hotchkiss RS, Karl IE. Reevaluation of the role of cellular hypoxia andbioenergetic failure in sepsis. JAMA. 1992;267:1503–1510.
144. Solomon MA, Correa R, Alexander HR, et al. Myocardial energymetabolism and morphology in a canine model of sepsis. Am J Physiol.1994;266:H757–H768.
145. Hotchkiss RS, Song SK, Neil JJ, et al. Sepsis does not impair tricarboxylicacid cycle in the heart. Am J Physiol. 1991;260:C50–C57.
146. Chaudry IH, Wichterman KA, Baue AE. Effect of sepsis on tissue adeninenucleotide levels. Surgery. 1979;85:205–211.
147. Geller ER, Tankauskas S, Kirpatrick JR. Mitochondrial death in sepsis: afailed concept. J Surg Res. 1986;40:514–517.
148. MacLean LD, Mulligan WG, McLean APH, et al. Patterns of septic shockin man: a detailed study of 56 patients. Ann Surg. 1967;166:543–562.
149. Nishijima H, Weil MH, Shubin H, et al. Hemodynamic and metabolicstudies on shock associated with gram-negative bacteremia. Medicine (Bal-timore). 1973;52:287–294.
150. Weil MH, Nishijima H. Cardiac output in bacterial shock. Am J Med.1978;64:920–922.
151. Blain CM, Anderson TO, Pietras RJ, et al. Immediate hemodynamic effectsof gram-negative vs gram-positive bacteremia in man. Arch Intern Med.1970;126:260–265.
152. Packman MI, Rackow EC. Optimum left heart filling pressure during fluidresuscitation of patients with hypovolemic and septic shock. Crit Care Med.1983;11:165–169.
153. Winslow EJ, Loeb HS, Rahimtoola SH, et al. Hemodynamic studies andresults of therapy in 50 patients with bacteremic shock. Am J Med. 1973;54:421–432.
154. Krausz MM, Perel A, Eimerl D, et al. Cardiopulmonary effects of volumeloading in patients with septic shock. Ann Surg. 1977;185:429–434.
155. Parker MM, Suffredini AF, Natanson C, et al. Responses of left ventricu-lar function in surviviors and non-survivors of septic shock. J Crit Care.1989;4:19–25.
156. Teule GJJ, Van Lingen A, Verweij-van Vught MA, et al. Role of periph-eral pooling in porcine Escherichia coli sepsis. Circ Shock. 1984;12:115–123.
157. Natanson C, Fink MP, Ballantyne HK, et al. Gram-negative bacteremiaproduces both severe systolic and diastolic cardiac dysfunction in a caninemodel that simulates human septic shock. J Clin Invest. 1986;78:259–270.
158. Carroll GC, Snyder JV. Hyperdynamic severe intravascular sepsis de-pends on fluid administration in cynomolgus monkey. Am J Physiol. 1982;243:131–141.
159. Teule GJJ, Den Hollander W, Bronsveld W, et al. Effect of volume load-ing and dopamine on hemodynamics and red cell distribution in canineendotoxic shock. Circ Shock. 1983;10:41–50.
160. Magder S, Vanelli G. Circuit factors in the high cardiac output of sepsis. JCrit Care. 1996;11(4):155–166.
161. Donnino M, Nguyen HB, Rivers EP. A hemodynamic comparison of earlyand late phase severe sepsis and septic shock. Chest. 2002;122:4S.
162. Kumar A, Haery C, Parrillo JE. Myocardial dysfunction in septic shock,I: clinical manifestation of cardiovascular dysfunction. J Cardiothor VascAnesth. 2001;15(3):364–376.
163. Ognibene FP, Parker MM, Natanson, et al. Depressed left ventricular per- AU:Initial?formance. Response to volume infusion in patients with sepsis and septic
shock. Chest. 1988;93:903–910.164. Parker MM, Shelhamer JH, Bacharach SL, et al. Profound but reversible
myocardial depression in patients with septic shock. Ann Intern Med.1984;100:483–490.
165. Garner LB, Willis MS, Carlson DL, et al. Macrophage migration inhibitoryfactor is a cardiac-derived myocardial depressant factor. Am J Physiol.2003;285(6):H2500–H2509.
166. Eichenholz PW, Eichacker PQ, Hoffman WD, et al. Tumor necrosis factorchallenges in canines: patterns of cardiovascular dysfunction. Am J Physiol.1992;263:H668–H675.
167. Vincent JL, Bakker J, Marecaux G, et al. Administration of anti-TNF anti-body improves left ventricular function in septic shock patients: results ofa pilot study. Chest. 1992;101:810–815.
168. Hosenpud JD, Campbell SM, Mendelson DJ. Interleukin-1-induced my-ocardial depression in an isolated beating heart preparation. J Heart Trans-plant. 1989;8:460–464.
169. Massey CV, Kohout TR, Gaa ST, et al. Molecular and cellular actions ofplatelet-activating factor in rat heart cells. J Clin Invest. 1991;88:2106–2116.
170. Schutzer KM, Haglund U, Falk A. Cardiopulmonary dysfunction in a felineseptic model: possible role of leukotrienes. Circ Shock. 1989;29:13–25.
171. Werdan K, Muller U, Reithmann C. “Negative inotropic cascades” in car-diomyocytes triggered by substances relevant to sepsis. In: Schlag G, RedlH, eds. Pathophysiology of Shock, Sepsis and Organ Failure. Berlin, Ger-many: Springer-Verlag; 1993:787–834.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
34 Section VI: Shock States
172. Pathan N, Hemingway CA, Alizadeh AA, et al. Role of interleukin 6in myocardial dysfunction of meningococcal septic shock. Lancet. 2004;363(9404):203–209.
173. Papadopoulos MC, Davies DC, Moss R, et al. Pathophysiology of septicencephalopathy: a review. Crit Care Med. 2000;28(8):3019–3024.
174. Sprung CL, Peduzzi PN, Shatney CH, et al. Impact of encephalopathy onmortality in the sepsis syndrome. The Veterans Administration SystemicSepsis Cooperative Study Group. Crit Care Med. 1990;18(8):801–806.
175. Pine RW, Wertz MJ, Lennard ES, et al. Determinants of organ malfunctionor death in patients with intra-abdominal sepsis. A discriminant analysis.Arch Surg. 1983;118(2):242–249.
176. Young GB, Bolton CF, Austin TW, et al. The encephalopathy associatedwith septic illness. Clin Invest Med. 1990;13(6):297–304.
177. Young GB, Bolton CF, Archibald Y, et al. The electroencephalogram insepsis-associated encephalopathy. J Clin Neurophysiol. 1992;9(1):145–152.
178. Kollef MH, Sherman G. Acquired organ system derangements and hos-pital mortality: are all organ systems created equally? Am J Crit Care.1999;8(3):180–188.
179. De Jonghe B, Lacherade JC, Durand MC, et al. Critical illness neuromus-cular syndromes. Crit Care Clin. 2006;22(4):805–818.
180. Leijten FS, Harinck-de Weerd JE, Poortvliet DC, et al. The role of polyneu-ropathy in motor convalescence after prolonged mechanical ventilation.JAMA. 1995;274(15):1221–1225.
181. Bercker S, Weber-Carstens S, Deja M, et al. Critical illness polyneuropathyand myopathy in patients with acute respiratory distress syndrome. CritCare Med. 2005;33(4):711–715.
182. Lorin S, Sivak M, Nierman DM. Critical illness polyneuropathy: what tolook for in at-risk patients. J Crit Illness. 1998;13(10):608–612.
183. Tennila A, Salmi T, Pettila V, et al. Early signs of critical illness polyneu-ropathy in ICU patients with systemic inflammatory response syndrome orsepsis [see comment]. Intensive Care Med. 2000;26(9):1360–1363.
184. Tepper M, Rakic S, Haas JA, et al. Incidence and onset of critical illnesspolyneuropathy in patients with septic shock. Neth J Med. 2000;56(6):211–214.
185. De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquired in the inten-sive care unit: a prospective multicenter study. JAMA. 2002;288(22):2859–2867.
186. Cunnion RE, Schaer GL, Parker MM, et al. The coronary circulation inhuman septic shock. Circulation. 1986;73:637–644.
187. Dhainaut JF, Huyghebaert MF, Monsallier JF, et al. Coronary hemo-dynamics and myocardial metabolism of lactate, free fatty acids, glu-cose, and ketones in patients with septic shock. Circulation. 1987;75:533–541.
188. Reilly JM, Cunnion RE, Burch-Whitman C, et al. A circulating myocardialdepressant substance is associated with cardiac dysfunction and periph-eral hypoperfusion (lactic acidemia) in patients with septic shock. Chest.1989;95:1072–1080.
189. Parrillo JE, Burch C, Shelhamer JH, et al. A circulating myocardial depres-sant substance in humans with septic shock. Septic shock patients with areduced ejection fraction have a circulating factor that depresses in vitromyocardial cell performance. J Clin Invest. 1985;76:1539–1553.
190. Jones SB, Romano RD. Myocardial beta adrenergic receptor coupling toadenylate cyclase during developing septic shock. Circ Shock. 1990;30:51–61.
191. Bristow MR, Ginsburg R, Minobe W, et al. Decreased catecholamine sensi-tivity and beta adrenergic receptor density in failing human hearts. N EnglJ Med. 1982;307:205–210.
192. Silverman HJ, Penaranda R, Orens JB, et al. Impaired beta-adrenergic re-ceptor stimulation of cyclic adenosine monophosphate in human septicshock: association with myocardial hyporesponsiveness to catecholamines.Crit Care Med. 1993;21:31–39.
193. Kumar A, Brar R, Wang P, et al. The role of nitric oxide and cyclic GMP inhuman septic serum-induced depression of cardiac myocyte contractility.Am J Physiol. 1999;276:R265–R276.
194. Kumar A, Paladugu B, Mensing J, et al., Nitric oxide-dependent and -independent mechanisms are involved in TNFa-induced depression of car-diac myocyte contractility. Am J Physiol. 2007;292:R1900–R1906.
195. Anel R, Paladugu B, Makkena R, et al. TNFa induces a proximal defectof beta-adrenoreceptor signal transduction in cardiac myocytes. Crit CareMed. 1999;27:A95.
196. Gulick T, Chung MK, Pieper SJ, et al. Interleukin-1 and tumor necrosisfactor inhibit cardiac myocyte adrenergic responsiveness. Proc Natl AcadSci.U S A. 1989;86:6753–6757.
197. Chung MK, Gulick TS, Rotondo R, et al. Mechanism of cytokine inhibi-tion of beta-adrenergic agonist stimulation of cyclic AMP in rat cardiacmyoctyes: impairment of signal transduction. Circ Res. 1990;67:753–763.
198. Turner A, Tsamitros M, Bellomo R. Myocardial cell injury in septic shock.Crit Care Med. 1999;27(9):1775–1780.
199. ver Elst KM, Spapen HD, Nguyen DN, et al. Cardiac troponins I and Tare biological markers of left ventricular dysfunction in septic shock. ClinChem. 2000;46(5):650–657.
200. Mehta NJ, Khan IA, Gupta V, et al. Cardiac troponin I predicts my-ocardial dysfunction and adverse outcome in septic shock. Intl J Cardiol.2004;95(1):13–17.
201. Schrier RW, Wang W. Acute renal failure and sepsis [see comment]. N EnglJ Med. 2004;351(2):159–169.
202. Ware LB, Matthay MA, Ware LB, et al. The acute respiratory distress syn-drome. N Engl J Med. 2000;342(18):1334–1349.
203. Sevransky JE, Levy MM, Marini JJ, et al. Mechanical ventilation in sepsis-induced acute lung injury/acute respiratory distress syndrome: an evidence-based review. Crit Care Med. 2004;32(11 Suppl):S548–S553.
204. The Acute Respiratory Distress Syndrome Network. Ventilation with lowertidal volumes as compared with traditional tidal volumes for acute lunginjury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308.
205. Piantadosi CA, Schwartz DA, Piantadosi CA, et al. The acute respiratorydistress syndrome. Ann Intern Med. 2004;141(6):460–470.
206. Hoste EA, Lameire NH, Vanholder RC, et al. Acute renal failure in patientswith sepsis in a surgical ICU: predictive factors, incidence, comorbidity, andoutcome. J Am Soc Nephrol. 2003;14(4):1022–1030.
207. Rasmussen HH, Ibels LS. Acute renal failure. Multivariate analysis of causesand risk factors. Am J Med. 1982;73:211–218.
208. Neveu H, Kleinknecht D, Brivet F, et al. Prognostic factors in acute re-nal failure due to sepsis. Results of a prospective multicentre study. TheFrench Study Group on Acute Renal Failure. Nephrol Dial Transplant.1996;11(2):293–299.
209. Brivet FG, Kleinknecht DJ, Loirat, et al. Acute renal failure in intensive AU:Initial?care units–causes, outcome, and prognostic factors of hospital mortality; a
prospective, multicenter study. French Study Group on Acute Renal Failure.Crit Care Med. 1996;24(2):192–198.
210. Astiz ME, Rackow EC, Weil MH. Pathophysiology and treatment of circu-latory shock. Crit Care Clin. 1993;9:183–203.
211. Deitch E, Bridges W, Baker J, et al. Hemorrhagic shock-induced bacterialtranslocation is reduced by xanthine oxidase inhibition or inactivation.Surgery. 1988;104:191–198.
212. Mainous MR, Deitch EA. Bacterial translocation. In: Schlag G, Redl H,eds. Pathophysiology of Shock, Sepsis and Organ Failure. Berlin, Germany:Springer-Verlag; 1993:265–278.
213. Lillehei RC, MacLean LD. The intestinal factor in irreversible endotoxinshock. Ann Surg. 1958;148:513–519.
214. Meakins JL, Marshall JC. The gut as the motor of multiple organ failure. In:Marston A, Bulkley GB, Fiddian-Green RG, et al., eds. Splanchnic Ischemiaand Multiple Organ Failure. London, England: Edward Arnold; 1989:339.
215. Marrero J, Martinez FJ, Hyzy R, et al. Advances in critical care hepatology.Am J Resp Crit Care Med. 2003;168(12):1421–1426.
216. Moseley RH. Sepsis and cholestasis. Clin Liver Disease. 1999;3:465–475.217. Champion HR, Jones RT, Trump BF, et al. A clinicopathologic study of
hepatic dysfunction following shock. Surg Gynecol Obstet. 1976;142:657–663.
218. Levi M, ten Cate H, Levi M, et al. Disseminated intravascularcoagulation.[see comment]. N Engl J Med. 1999;341(8):586–592.
219. Bone RC. Gram positive organisms and sepsis. Arch Intern Med. 1994;154:26–34.
220. Zeerleder S, Hack CE, Wuillemin WA, et al. Disseminated intravascularcoagulation in sepsis. Chest. 2005;128(4):2864–2875.
221. ten Cate H. Pathophysiology of disseminated intravascular coagulation insepsis. Crit Care Med. 2000;28(9 Suppl):S9–S11.
222. Woolf PD. Endocrinology of shock. Ann Emerg Med. 1986;15:1401–1405.
223. Arnold J, Leinhardt D, Little RA. Metabolic response to trauma. In: SchlagG, Redl H, eds. Pathophysiology of Shock Sepsis and Organ Failure. Berlin,Germany: Springer-Verlag; 1993: 145–160.
224. Bessey PQ, Brooks DC, Black PR, et al. Epinephrine acutely mediates skele-tal muscle insulin resistance. Surgery. 1983;94:172–179.
225. Brierre S, Kumari R, Deboisblanc BP, et al. The endocrine system duringsepsis. Am J Med Sci. 2004;328(4):238–247.
226. Mizock B. Metabolic derangements in sepsis and septic shock. Crit CareClin. 2000;16(2):319–336.
227. Naylor JM, Kronfeld DS. In-vivo studies of hypoglycemia and lactic acidosisin endotoxic shock. Am J Physiol. 1985;248:E309–E316.
228. Daniel AM, Pierce CH, Shizgal HM, et al. Protein and fat utilization inshock. Surgery. 1978;84:588–594.
229. Bagby GJ, Spitzer JA. Decreased myocardial extracellular and musclelipoprotein lipase activities in endotoxin-treated rats. Proc Soc Exp BiolMed. 1981;168:395–398.
230. Ho HC, Chapital AD, Yu M, et al. Hypothyroidism and adrenal insuffi-ciency in sepsis and hemorrhagic shock. Arch Surg. 2004;139(11):1199–1203.
231. Gardelis JG, Hatzis TD, Stamogiannou L, et al. Activity of the growthhormone/insulin-like growth factor-I axis in critically ill children. J PediatrEndocrinol. 2005;18(4):363–372.
232. Beishuizen A, Thijs LG, Beishuizen A, et al. Endotoxin and thehypothalamo-pituitary-adrenal (HPA) axis. J Endotoxin Res. 2003;9(1):3–24.
233. Heemskerk VH, Daemen MA, Buurman WA, et al. Insulin-like growthfactor-1 (IGF-1) and growth hormone (GH) in immunity and inflammation.Cytokine Growth Factor Rev. 1999;10(1):5–14.
234. Woods RJ, David J, Baigent S, et al. Elevated levels of corticotrophin-

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 35
releasing factor binding protein in the blood of patients suffering fromarthritis and septicaemia and the presence of novel ligands in synovial fluid.Br J Rheumatol. 1996;35(2):120–124.
235. Holmes CL, Patel BM, Russell J, et al. Physiology of vasopressin relevantto management of septic shock. Chest. 2001;120(3):989–1002.
236. Landry DW, Levin HR, Gallant EM, et al. Vasopressin deficiency con-tributes to the vasodilatation of septic shock. Circulation. 1997;95:1122–1125.
237. Marik PE, Zaloga GP. Adrenal insufficiency during septic shock. Crit CareMed. 2003;31(1):141–145.
238. Zaloga GP, Marik P. Hypothalamic-pituitary-adrenal insufficiency. CritCare Clin. 2001;17(1):25–42.
239. Annane D, Sebille V, Troche G, et al. A 3-level prognostic classification inseptic shock based on cortisol levels and cortisol response to corticotropin.JAMA. 2000;283(8):1038–1045.
240. Manglik S, Flores E, Lubarsky L, et al. Glucocorticoid insufficiency in pa-tients who present to the hospital with severe sepsis: a prospective clinicaltrial [see comment]. Crit Care Med. 2003;31(6):1668–1675.
241. Marik P, Rotello L, Zaloga G. Secondary adrenal insufficiency is commonin critically ill patients. Crit Care Med. 2001;29:A163.
242. de Groof F, Joosten KF, Janssen JA, et al. Acute stress response inchildren with meningococcal sepsis: important differences in the growthhormone/insulin-like growth factor I axis between nonsurvivors and sur-vivors. J Clin Endocrinol Metab. 2002;87(7):3118–3124.
243. Felmet KA, Hall MW, Clark RS, et al. Prolonged lymphopenia, lymphoiddepletion, and hypoprolactinemia in children with nosocomial sepsis andmultiple organ failure. J Immunol. 2005;174(6):3765–3772.
244. Medina P, Noguera I, Aldasoro M, et al. Enhancement by vasopressin ofadrenergic responses in human mesenteric arteries. Am J Physiol. 1997;272(3 Pt 2):H1087–H1093.
245. Peres BD, Lopes FF, Melot C, et al. Body temperature alterations in thecritically ill. Intensive Care Med. 2004;30(5):811–816.
246. Gomez-Jimenez J, Salgado A, Mourelle M, et al. L-arginine: nitric oxidepathway in endotoxemia and human septic shock. Crit Care Med. 1995;23:253–258.
247. Kubes P. Nitric oxide affects microvascular permeability in the intact in-flamed vasculature. Microcirculation. 1995;2(3):235–244.
248. Rackow EC, Kaufman BS, Falk JL, et al. Hemodynamic response to fluidrepletion in patients with septic shock: evidence for early depression ofcardiac performance. Circ Shock. 1987;22:11–22.
249. Parrillo JE, Parker MM, Natanson C, et al. Septic shock in humans. Ad-vances in the understanding of pathogenesis, cardiovascular dysfunction,and therapy. Ann Intern Med. 1990;113:227–242.
250. Cannon WB. Traumatic Shock. New York, NY: Appleton; 1923.251. Cournand A, Riley RL, Bradley SE, et al. Studies of the circulation in clinical
shock. Surgery. 1943;13:964–995.252. Carcillo JA, Davis AL, Zaritsky A. Role of early fluid resuscitation in pe-
diatric septic shock. JAMA. 1991;266(9):1242–1245.253. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the
treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377.
254. Levraut J, Ichai C, Petit I, et al. Low exogenous lactate clearance as an earlypredictor of mortality in normolactatemic critically ill septic patients. CritCare Med. 2003;31(3):705–710.
255. Abramson D, Scalea TM, Hitchcock R, et al. Lactate clearance and survivalfollowing injury. J Trauma. 1993;35(4):584–588.
256. Davis JW, Shackford SR, Mackersie RC, et al. Base deficit as a guide tovolume resuscitation. J Trauma. 1988;28(10):1464–1467.
257. Oud L, Haupt MT. Persistent gastric intramucosal ischemia in patients withsepsis following resuscitation from shock. Chest. 1999;115(5):1390–1396.
258. Wo CC, Shoemaker WC, Appel PL, et al. Unreliability of blood pressureand heart rate to evaluate cardiac output in emergency resuscitation andcritical illness. Crit Care Med. 1993;21(2):218–223.
259. Ward KR, Ivatury RR, Barbee WR. Endpoints of resuscitation for the victimof trauma. Intensive Care Med. 2001;16(2):55–75.
260. Bakker J, Coffemils M, Leon M, et al. Blood lactate levels are superiorto oxygen-derived variables in predicting outcome in human septic shock.Chest. 1992;99:956–962.
261. Nguyen HB, Rivers EP, Knoblich BP, et al. Early lactate clearance is asso-ciated with improved outcome in severe sepsis and septic shock. Crit CareMed. 2004;32(8):1637–1642.
262. James JH, Luchette FA, McCarter FD, et al. Lactate is an unreliable indica-tor of tissue hypoxia in injury or sepsis. Lancet. 1999;354(9177):505–508.
263. Ernest D, Belzberg AS, Dodek PM. Distribution of normal saline and 5%albumin infusions in septic patients. Crit Care Med. 1999;27(1):46–50.
264. Rackow EC, Falk JL, Fein IA, et al. Fluid resuscitation in circulatory shock:a comparison of the cardiorespiratory effects of albumin, hetastarch, andsaline solutions in patients with hypovolemic and septic shock. Crit CareMed. 1983;11:839–850.
265. Haupt MT, Teerapong P, Green D, et al. Increased pulmonary edema withcrystalloid compared to colloid resuscitation of shock associated with in-creased vascular permeability. Circ Shock. 1984;12:213–224.
266. Haupt MT, Rackow EC. Colloid osmotic pressure and fluid resuscita-tion with hetastarch, albumin, and saline solutions. Crit Care Med. 1982;10:159–162.
267. Wilkes MM, Navickis RJ. Patient survival after human albumin adminis-tration. A meta-analysis of randomized, controlled trials. Ann Intern Med.2001;135(3):149–164.
268. Alderson P, Bunn F, Lefebvre C, et al. Human albumin solution for resus-citation and volume expansion in critically ill patients. Cochrane DatabaseSyst Rev. 2002;(1):CD001208.
269. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and salinefor fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350(22):2247–2256.
270. Schierhout G, Roberts I. Fluid resuscitation with colloid or crystalloid so-lutions in critically ill patients: a systematic review of randomised trials [seecomment]. BMJ. 1998;316(7136):961–964.
271. Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, andoutcomes in elderly patients with pneumonia. JAMA. 1997;278(23):2080–2084.
272. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate an-timicrobial treatment of bloodstream infections on patient outcomes in theICU setting [see comment]. Chest. 2000;118(1):146–155.
273. Kollef MH, Sherman G, Ward S, et al. Inadequate antimicrobial treatmentof infections: a risk factor for hospital mortality among critically ill patients.Chest. 1999;115(2):462–474.
274. Kumar A, Ellis P, et al. The impact of initiation of inadequate antimicrobial AU: Pleaseprovidename ofthirdauthor ordelete ”etal.”
therapy on survival in human septic shock. Antimicrob Agents Chemother.2007;111:271.
275. Young LS, Martin WJ, Meyer RD, et al. Gram-negative rod bacteremia:Microbiologic, immunologic, and therapeutic considerations. Ann InternMed. 1977;86:456–471.
276. Romero-Vivas J, Rubio M, Fernandez C, et al. Mortality associated withnosocomial bacteremia due to methicillin-resistant Staphylococcus aureus.Clin Infect Dis. 1995;21(6):1417–1423.
277. Nguyen MH, Peacock JE Jr, Tanner DC, et al. Therapeutic approaches inpatients with candidemia. Evaluation in a multicenter, prospective, obser-vational study. Arch Intern Med. 1995;155(22):2429–2435.
278. Vergis EN, Hayden MK, Chow JW, et al. Determinants of vancomycinresistance and mortality rates in enterococcal bacteremia. a prospectivemulticenter study. Ann Intern Med. 2001;135(7):484–492.
279. Byl B, Clevenbergh P, Jacobs F, et al. Impact of infectious diseases specialistsand microbiological data on the appropriateness of antimicrobial therapyfor bacteremia [see comment]. Clin Infect Dis. 1999;29(1):60–66.
280. Aronin SI, Peduzzi P, Quagliarello VJ. Community-acquired bacterialmeningitis: risk stratification for adverse clinical outcome and effect of an-tibiotic timing. Ann Intern Med. 1998;129(11):862–869.
281. Miner JR, Heegaard W, Mapes A, et al. Presentation, time to antibiotics,and mortality of patients with bacterial meningitis at an urban county med-ical center. J Emerg Med. 2001;21(4):387–392.
282. Proulx N, Frechette D, Toye B, et al. Delays in the administration of antibi-otics are associated with mortality from adult acute bacterial meningitis.QJM. 2005;98(4):291–298.
283. Houck PM, Bratzler DW, Nsa W, et al. Timing of antibiotic administrationand outcomes for Medicare patients hospitalized with community-acquiredpneumonia. Arch Intern Med. 2004;164(6):637–644.
284. Natsch S, Kullberg BJ, Van der Meer JW, et al. Delay in administeringthe first dose of antibiotics in patients admitted to hospital with seriousinfections. Eur J Clin Microbiol Infect Dis. 1998;17(10):681–684.
285. Pinder M, Bellomo R, Lipman, et al. Pharmacological principles of an-tibiotic prescription in the critically ill. Anaesth Intensive Care. 2002;30(2):134–144.
286. Pimentel FL, Abelha F, Trigo MA, et al. Determination of plasma con-centrations of amikacin in patients of an intensive care unit. J Chemother.1995;7(1):45–49.
287. Whipple JK, Ausman RK, Franson T, et al. Effect of individualized pharma-cokinetic dosing on patient outcome. Crit Care Med. 1991;19(12):1480–1485.
288. Joukhadar C, Frossard M, Mayer BX, et al. Impaired target site penetrationof beta-lactams may account for therapeutic failure in patients with septicshock. Crit Care Med. 2001;29(2):385–391.
289. Franson TR, Quebbeman EJ, Whipple J, et al. Prospective comparison oftraditional and pharmacokinetic aminoglycoside dosing methods. Crit CareMed. 1988;16(9):840–843.
290. Chelluri L, Jastremski MS. Inadequacy of standard aminoglycoside loadingdoses in acutely ill patients. Crit Care Med. 1987;15(12):1143–1145.
291. Tegeder I, Schmidtko A, Brautigam L, et al. Tissue distribution of imipenemin critically ill patients. Clin Pharmacol Ther. 2002;71(5):325–333.
292. Moore RD, Smith CR, Lietman PS. The association of aminoglycosideplasma levels with mortality in patients with gram-negative bacteremia.J Infect Dis. 1984;149(3):443–448.
293. Moore RD, Smith CR, Lietman PS. Association of aminoglycoside plasmalevels with therapeutic outcome in gram-negative pneumonia. Am J Med.1984;77(4):657–662.
294. Forrest A, Nix DE, Ballow CH, et al. Pharmacodynamics of intravenousciprofloxacin in seriously ill patients. Antimicrob Agents Chemother.1993;37(5):1073–1081.
295. Preston SL, Drusano GL, Berman AL, et al. Pharmacodynamics of lev-ofloxacin: a new paradigm for early clinical trials. JAMA. 1998;279(2):125–129.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
36 Section VI: Shock States
296. Drusano GL, Preston SL, Fowler C, et al. Relationship between flu-oroquinolone area under the curve: minimum inhibitory concentrationratio and the probability of eradication of the infecting pathogen, inpatients with nosocomial pneumonia. J Infect Dis. 2004;189(9):1590–1597.
297. Moore RD, Lietman PS, Smith CR. Clinical response to aminoglycosidetherapy: importance of the ratio of peak concentration to minimal in-hibitory concentration. J Infect Dis. 1987;155(1):93–99.
298. Kashuba AD, Nafziger AN, Drusano GL, et al. Optimizing aminoglyco-side therapy for nosocomial pneumonia caused by gram-negative bacteria.Antimicrob Agents Chemother. 1999;43(3):623–629.
299. Schentag JJ, Smith IL, Swanson DJ, et al. Role for dual individualizationwith cefmenoxime. Am J Med. 1984;77(6A):43–50.
300. Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale forantibacterial dosing of mice and men. Clin Infect Dis. 1998;26(1):1–10.
301. Lodise TP, Lomaestro BM, Drusano GL. Piperacillin-tazobactam forPseudomonas aeruginosa infection: Clinical implications of an extended-infusion dosing strategy. Clin Infect Dis. 2007;44:357–363.
302. Craig WA, Ebert SC. Continuous infusion of beta-lactam antibiotics. An-timicrob Agents Chemother. 1992;36(12):2577–2583.
303. Craig WA. Once-daily versus multiple-daily dosing of aminoglycosides. JChemother. 1995;7(Suppl 2):47–52.
304. Kashuba AD, Bertino JS Jr, Nafziger AN. Dosing of aminoglycosides torapidly attain pharmacodynamic goals and hasten therapeutic response byusing individualized pharmacokinetic monitoring of patients with pneu-monia caused by gram-negative organisms. Antimicrob Agents Chemother.1998;42(7):1842–1844.
305. Bodey GP, Ketchel SJ, Rodriguez V. A randomized study of carbenicillinplus cefamandole or tobramycin in the treatment of febrile episodes incancer patients. Am J Med. 1979;67(4):608–616.
306. Daenen S, Vries-Hospers H. Cure of Pseudomonas aeruginosa infectionin neutropenic patients by continuous infusion of ceftazidime. Lancet.1988;1(8591):937.
307. Egerer G, Goldschmidt H, Hensel M, et al. Continuous infusion of cef-tazidime for patients with breast cancer and multiple myeloma receivinghigh-dose chemotherapy and peripheral blood stem cell transplantation.Bone Marrow Transplant. 2002;30(7):427–431.
308. Benko AS, Cappelletty DM, Kruse JA, et al. Continuous infusion ver-sus intermittent administration of ceftazidime in critically ill patients withsuspected gram-negative infections. Antimicrob Agents Chemother. 1996;40(3):691–695.
309. Thalhammer F, Traunmuller F, El Manyawi I, et al. Continuous infusionversus intermittent administration of meropenem in critically ill patients. JAntimicrob Chemother. 1999;43(4):523–527.
310. Sfeir T, Saha DC, Astiz M, et al. Role of interleukin-10 in monocyte hypore-sponsiveness associated with septic shock. Crit Care Med. 2001;29(1):129–133.
311. Haupt W, Riese J, Mehler C, et al. Monocyte function before and aftersurgical trauma. Dig Surg. 1998;15(2):102–104.
312. Brandtzaeg P, Osnes L, Ovstebo R, et al. Net inflammatory capacity of hu-man septic shock plasma evaluated by a monocyte-based target cell assay:identification of interleukin-10 as a major functional deactivator of hu-man monocytes. [Erratum in J Exp Med. 1996;184(5):2075.]. J Exp Med.1996;184(1):51–60.
313. Williams MA, Withington S, Newland AC, et al. Monocyte anergy in sep-tic shock is associated with a predilection to apoptosis and is reversed bygranulocyte-macrophage colony-stimulating factor ex vivo. J Infect Dis.1998;178(5):1421–1433.
314. Tavares-Murta BM, Zaparoli M, Ferreira RB, et al. Failure of neutrophilchemotactic function in septic patients. Crit Care Med. 2002;30(5):1056–1061.
315. Holzer K, Konietzny P, Wilhelm K, et al. Phagocytosis by emigrated, intra-abdominal neutrophils is depressed during human secondary peritonitis.Eur Surg Res. 2002;34(4):275–284.
316. Benjamim CF, Ferreira SH, Cunha FQ. Role of nitric oxide in the failureof neutrophil migration in sepsis. J Infect Dis. 2000;182(1):214–223.
317. Barriere SL. Monotherapy versus combination antimicrobial therapy: a re-view. Pharmacotherapy. 1991;11(2 Pt 2):64S–71S.
318. Hughes WT, Armstrong D, Bodey GP, et al. 2002 guidelines for the useof antimicrobial agents in neutropenic patients with cancer [see comment].Clin Infect Dis. 2002;34(6):730–751.
319. Bochud PY, Glauser MP, Calandra T, et al. Antibiotics in sepsis. IntensiveCare Med. 2001;27(Suppl 1):S33–S48.
320. Safdar N, Handelsman J, Maki DG, et al. Does combination antimicrobialtherapy reduce mortality in Gram-negative bacteraemia? A meta-analysis[see comment]. Lancet Infect Dis. 2004;4(8):519–527.
321. Hilf M, Yu VL, Sharp J, et al. Antibiotic therapy for Pseudomonas aerug-inosa bacteremia: outcome correlations in a prospective study of. 200 pa-tients. Am J Med. 1989;87(5):540–546.
322. Chow JW, Fine MJ, Shlaes DM, et al. Enterobacter bacteremia: clinical fea-tures and emergence of antibiotic resistance during therapy [see comment].Ann Intern Med. 1991;115(8):585–590.
323. Korvick JA, Bryan CS, Farber B, et al. Prospective observational study ofKlebsiella bacteremia in. 230 patients: outcome for antibiotic combinations
versus monotherapy. Antimicrob Agents Chemother. 1992;36(12):2639–2644.
324. Anderson ET, Young LS, Hewitt WL. Antimicrobial synergism in the ther-apy of gram-negative rod bacteremia. Chemotherapy. 1978;24(1):45–54.
325. Baddour LM, Yu VL, Klugman KP, et al. Combination antibiotic therapylowers mortality among severely ill patients with pneumococcal bacteremia.Am J Resp Crit Care Med. 2004;170(4):440–4.
326. Waterer GW, Somes GW, Wunderink RG. Monotherapy may be subop-timal for severe bacteremic pneumococcal pneumonia. Arch Intern Med.2001;161(15):1837–1842.
327. Martinez JA, Horcajada JP, Almela M, et al. Addition of a macrolide to abeta-lactam-based empirical antibiotic regimen is associated with lower in-hospital mortality for patients with bacteremic pneumococcal pneumonia[see comment]. Clin Infect Dis. 2003;36(4):389–395.
328. Rodriguez A, Mendia A, Sirvent JM, et al. Combination antibiotic therapyimproves survival in patients with community-acquired pneumonia andshock. Crit Care Med. 2007;35(6):1493–1498.
329. Sprung CL, Finch RG, Thijs LG, et al. International sepsis trial (INTER-SEPT): role and impact of a clinical evaluation committee. Crit Care Med.1996;24(9):1441–1447.
330. Sudarsky LA, Laschinger JC, Coppa GF, et al. Improved results from astandardized approach in treating patients with necrotizing fasciitis. AnnSurg. 1987;206(5):661–665.
331. Moss RL, Musemeche CA, Kosloske AM. Necrotizing fasciitis in children:prompt recognition and aggressive therapy improve survival. J Pediatr Surg.1996;31(8):1142–1146.
332. Kumar A, Wood K, Gurka D, et al. Outcome of septic shock correlates withduration of hypotension prior to source control implementation. ICAACProceedings. 2004;350:K–1222.
333. Kumar A, Parrillo JE. Shock: pathophysiology, classification and approachto management. In: Parrillo JE, Dellinger RP, eds. Critical Care Medicine:Principles of Diagnosis and Management in the Adult. 3rd ed. St. Louis,MO: Mosby; 2007:379–422.
334. Bond RF. Peripheral macro- and microcirculation. In: Schlag G, Redl H,eds. Pathophysiology of Shock, Sepsis and Organ Failure. Berlin, Germany:Springer-Verlag; 1993:893–907.
335. Desjars P, Pinaud M, Potel G, et al. A reappraisal of norepinephrine therapyin human septic shock. Crit Care Med. 1987;15(2):134–137.
336. Desjars P, Pinaud M, Bugnon D, et al. Norepinephrine therapy has no dele-terious renal effects in human septic shock. Crit Care Med. 1989;17(5):426–429.
337. Fukuoka T, Nishimura M, Imanaka H, et al. Effects of norepinephrine onrenal function in septic patients with normal and elevated serum lactatelevels. Crit Care Med. 1989;17(11):1104–1107.
338. Hesselvik JF, Brodin B. Low dose norepinephrine in patients with septicshock and oliguria: effects on afterload, urine flow, and oxygen transport.Crit Care Med. 1989;17(2):179–180.
339. Meadows D, Edwards JD, Wilkins RG, et al. Reversal of intractable sep-tic shock with norepinephrine therapy. Crit Care Med. 1988;16(7):663–666.
340. Redl-Wenzl EM, Armbruster C, Edelmann G, et al. The effects of nore-pinephrine on hemodynamics and renal function in severe septic shockstates [see comment]. Intensive Care Med. 1993;19(3):151–154.
341. Neviere R, Mathieu D, Chagnon JL, et al. The contrasting effects ofdobutamine and dopamine on gastric mucosal perfusion in septic patients.Am J Resp Crit Care Med. 1996;154(6 Pt 1):1684–1688.
342. Marin C, Eon B, Saux P, et al. Renal effects of norepinephrine used to treatseptic shock patients. Crit Care Med. 1990;18(3):282–285.
343. Marik PE, Mohedin M. The contrasting effects of dopamine and nore-pinephrine on systemic and splanchnic oxygen utilization in hyperdynamicsepsis. JAMA. 1994;272(17):1354–1357.
344. Ruokonen E, Takala J, Kari A, et al. Regional blood flow and oxygentransport in septic shock. Crit Care Med. 1993;21(9):1296–1303.
345. Meier-Hellmann A, Specht M, Hannemann L, et al. Splanchnic blood flowis greater in septic shock treated with norepinephrine than in severe sepsis.Intensive Care Med. 1996;22(12):1354–1359.
346. Levy B, Bollaert PE, Charpentier C, et al. Comparison of norepinephrineand dobutamine to epinephrine for hemodynamics, lactate metabolism,and gastric tonometric variables in septic shock: a prospective, randomizedstudy [see comment]. Intensive Care Med. 1997;23(3):282–287.
347. De Backer D, Creteur J, Silva E, et al. Effects of dopamine, norepinephrine,and epinephrine on the splanchnic circulation in septic shock: which is best?Crit Care Med. 2003;31(6):1659–1667.
348. Martin C, Papazian L, Perrin G, et al. Norepinephrine or dopamine for thetreatment of hyperdynamic septic shock? Chest. 1993;103(6):1826–1831.
349. Devins SS, Miller A, Herndon BL, et al. The effects of dopamine on T-cellproliferative response and serum prolactin in critically ill patients. Crit CareMed. 1992;20:1644–1649.
350. Kumar A, Schupp E, Bunnell E, et al. The cardiovascular response to dobu-tamine in septic shock. Clin Invest Med. 1994;17, B18 #107. AU: Please
clarify “17,B18 #107”and, ifpossible,put intostandardjournalformat.
351. Rhodes A, Lamb FJ, Malagon R, et al. A prospective study of the use ofa dobutamine stress test to identify outcome in patients with sepsis, severesepsis or septic shock. Crit Care Med. 1999;27(11):2361–2366.
352. Barton P, Garcia J, Kouatli A, et al. Hemodynamic effects of i.v.milrinone lactate in pediatric patients with septic shock. A prospec-

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
Chapter 57: Sepsis and Septic Shock 37
tive, double-blinded, randomized, placebo-controlled, interventional study.Chest. 1996;109:1302–1312.
353. Gattinoni L, Brazzi L, Pelosi P, et al. A trial of goal-oriented hemodynamictherapy in critically ill patients. SvO2 Collaborative Group. N Engl J Med.1995;333:1025–1032.
354. Hayes MA, Timmins AC, Yau EHS, et al. Elevation of systemic oxygendelivery in the treatment of critically ill patients. N Engl J Med. 1994;330:1717–1722.
355. Shoemaker WC, Appel PL, Kram HB, et al. Temporal hemodynamic andoxygen transport patterns in medical patients. Septic shock. Chest. 1993;104(5):1529–1536.
356. Shoemaker WC, Appel PL, Kram HB, et al. Sequence of physiologic patternsin surgical septic shock. Crit Care Med. 1993;21(12):1876–1889.
357. Ivanov R, Allen J, Calvin JE. The incidence of major morbidity in criticallyill patients managed with pulmonary artery catheters: a meta-analysis [seecomment]. Crit Care Med. 2000;28(3):615–619.
358. Tuchschmidt J, Fried J, Astiz M, et al. Elevation of cardiac output andoxygen delivery improves outcome in septic shock. Chest. 1992;102:216–220.
359. Yu M, Levy MM, Smith P, et al. Effect of maximizing oxygen deliveryon morbidity and mortality rates in critically ill patients: a prospective,randomized, controlled study. Crit Care Med. 1993;21(6):830–838.
360. Yu M, Burchell S, Hasaniya NW, et al. Relationship of mortality to in-creasing oxygen delivery in patients > or = 50 years of age: a prospective,randomized trial. Crit Care Med. 1998;26(6):1011–1019.
361. Alia I, Esteban A, Gordo F, et al. A randomized and controlled trial of theeffect of treatment aimed at maximizing oxygen delivery in patients withsevere sepsis or septic shock. Chest. 1999;115(2):453–461.
362. Heyland DK, Cook DJ, King D, et al. Maximizing oxygen delivery in crit-ically ill patients: a methodologic appraisal of the evidence [see comment].Crit Care Med. 1996;24(3):517–524.
363. Bussolino F, Camussi G, Baglioni C. Synthesis and release of platelet activat-ing factor by human vascular endothelial cells treated with tumor necrosisfactor or interleukin-1. J Biol Chem. 1988;263:11856–11861.
364. Landry DW, Levin HR, Gallant EM, et al. Vasopressin pressor sensitivityin vasodilatory septic shock. Crit Care Med. 1997;25:1279–1282.
365. Patel BM, Chittock DR, Russell JA, et al. Beneficial effects of short-termvasopressin infusion during severe septic shock. Anesthesiology. 2002;96(3):576–582.
366. Russell JA, Walley KR, Singer J, et al. A randomised controlled trial oflow dose vasopressin versus norepinephrine infusion in patients who haveseptic shock. American J Resp Crit Care Med. 2007;175:A508.
367. Schaer GL, Fink MP, Parrillo JE. Norepinephrine alone versus nore-pinephrine plus low-dose dopamine: enhanced renal blood flow with com-bination pressor therapy. Crit Care Med. 1985;13:492–496.
368. Hoogenberg K, Smit AJ, Girbes AR. Effects of low-dose dopamine on renaland systemic hemodynamics during incremental norepinephrine infusion inhealthy volunteers. Crit Care Med. 1998;26(2):260–265.
369. Olson D, Pohlman A, Hall JB. Administration of low-dose dopamine tononoliguric patients with sepsis syndrome does not raise intramucosalgastric pH nor improve creatinine clearance. Am J Resp Crit Care Med.1996;154(6 Pt 1):1664–1670.
370. Ichai C, Passeron C, Carles M, et al. Prolonged low-dose dopamine infusioninduces a transient improvement in renal function in hemodynamically sta-ble, critically ill patients: a single-blind, prospective, controlled study [seecomment]. Crit Care Med. 2000;28(5):1329–1335.
371. Bellomo R, Chapman M, Finfer S, et al. Low-dose dopamine in patients withearly renal dysfunction: a placebo-controlled randomised trial. AustraliaNew Zealand Intensive Care Society (ANZICS) Clinical Trials Group [seecomment]. Lancet. 2000;356(9248):2139–2143.
372. Marik PE, Iglesias J. Low-dose dopamine does not prevent acute renalfailure in patients with septic shock and oliguria. NORASEPT II StudyInvestigators. Am J Med. 1999;107(4):387–390.
373. Mimoz O, Rauss A, Rekik N, et al. Pulmonary artery catheterization in criti-cally ill patients: a prospective analysis of outcome changes associated withcatheter-prompted changes in therapy. Crit Care Med. 1994;22(4):573–579.
374. Connors AF Jr, McCaffree DR, Gray BA. Evaluation of right-heart catheter-ization in the critically ill patient without acute myocardial infarction. NEngl J Med. 1983;308:263–267.
375. Weisel RD, Vito L, Dennis RC, et al. Myocardial depression during sepsis.Am J Surg. 1977;133:512–521.
376. Cohn JN. Central venous pressure as a guide to volume expansion. AnnIntern Med. 1967;66(6):1283–1287.
377. Connors AF Jr, Dawson NV, Shaw PK, et al. Hemodynamic status incritically ill patients with and without acute heart disease. Chest. 1990;98(5):1200–1206.
378. Kumar A, Anel R, Bunnell E, et al. Pulmonary artery occlusion pressure andcentral venous pressure fail to predict ventricular filling volume, cardiacperformance, or the response to volume infusion in normal subjects. CritCare Med. 2004;32(3):691–9.
379. Robin ED. The cult of the Swan-Ganz catheter. Overuse and abuse of pul-monary flow catheters. Ann Intern Med. 1985;103(3):445–449.
380. Dalen JE, Bone RC. Is it time to pull the pulmonary artery catheter [seecomment]? JAMA. 1996;276(11):916–918.
381. Pronovost PJ, Jenckes MW, Dorman T, et al. Organizational characteristicsof intensive care units related to outcomes of abdominal aortic surgery [seecomments]. JAMA. 1999;281:1310–1317.
382. Carson SS, Stocking C, Podsadecki T, et al. Effects of organizational changein the medical intensive care unit of a teaching hospital: a comparison of’open’ and ’closed’ formats. JAMA. 1996;276:322–328.
383. Pronovost PJ, Angus DC, Dorman T, et al. Physician staffing patternsand clinical outcomes in critically ill patients: a systematic review. JAMA.2002;288(17):2151–2162.
384. Li TC, Phillips MC, Shaw L, et al. On-site physician staffing in a communityhospital intensive care unit. Impact on test and procedure use and on patientoutcome. JAMA. 1984;252(15):2023–2027.
385. Pollack MM, Katz RW, Ruttimann UE, et al. Improving the outcome andefficiency of intensive care: the impact of an intensivist. Crit Care Med.1988;16(1):11–17.
386. Reynolds HN, Haupt MT, Thill-Baharozian MC, et al. Impact of criticalcare physician staffing on patients with septic shock in a university hospitalmedical intensive care unit. JAMA. 1988;260:3446–3450.
387. Hutton P, Dye J, Prys-Roberts C. An assessment of the Dinamap. Anaes-thesia. 1984;39:261–267.
388. Cohn JN. Blood pressure measurement in shock. Mechanism of inaccuracyin ausculatory and palpatory methods. JAMA. 1967;199(13):118–122.
389. Connors AF Jr, Dawson NV, McCaffree DR, et al. Assessing hemodynamicstatus in critically ill patients: do physicians use clinical information opti-mally? J Crit Care. 1987;2:174–180.
390. Michard F, Teboul JL. Predicting fluid responsiveness in ICU patients: acritical analysis of the evidence. Chest. 2002;121(6):2000–2008.
391. Marik PE. Pulmonary artery catheterization and esophageal Doppler mon-itoring in the ICU. Chest. 1999;116(4):1085–1091.
392. Humphrey H, Hall J, Sznajder I, et al. Improved survival in ARDS patientsassociated with a reduction in pulmonary capillary wedge pressure [seecomment]. Chest. 1990;97(5):1176–1180.
393. Mitchell JP, Schuller D, Calandrino FS, et al. Improved outcome basedon fluid management in critically ill patients requiring pulmonary arterycatheterization. Am Rev Resp Dis. 1992;145(5):990–998.
394. Connors AF Jr, Speroff T, Dawson NV, et al. The effectiveness of rightheart catheterization in the initial care of critically ill patients. JAMA.1996;276:889–897.
395. Richard C, Warszawski J, Anguel N, et al. Early use of the pulmonary arterycatheter and outcomes in patients with shock and acute respiratory dis-tress syndrome: a randomized controlled trial. JAMA. 2003;290(20):2713–2720.
396. Rhodes A, Cusack RJ, Newman PJ, et al. A randomised, controlled trial ofthe pulmonary artery catheter in critically ill patients. Intensive Care Med.2002;28(3):256–264.
397. Polanczyk CA, Rohde LE, Goldman L, et al. Right heart catheterizationand cardiac complications in patients undergoing noncardiac surgery: anobservational study. JAMA. 2001;286(3):309–314.
398. Sandham JD, Hull RD, Brant RF, et al. A randomized, controlled trial ofthe use of pulmonary-artery catheters in high-risk surgical patients. N EnglJ Med. 2003;348(1):5–14.
399. Ivanov RI, Allen J, Sandham JD, et al. Pulmonary artery catheterization: anarrative and systematic critique of randomized controlled trials and rec-ommendations for the future. New Horiz. 1997;5(3):268–276.
400. Zanotti S, Kumar A, Kumar A. Cytokine modulation in sepsis and septicshock. Expert Opin Investig Drugs. 2002;11(8):1061–1075.
401. Anel RL, Kumar A. Experimental and emerging therapies for sepsis andseptic shock. Expert Opin Investig Drugs. 2001;10(8):1471–1485.
402. Ely EW, Bernard GR, Vincent JL. Activated protein C for severe sepsis [seecomment]. N Engl J Med. 2002;347(13):1035–1036.
403. Beale R, Wright TJ, Wong K, et al. Safety of drotrecogin alfa (activated)in adult patients with severe sepsis: comparison of global ENHANCE toPROWESS. Chest. 2003;124:102S.
404. Vincent JL, Bernard GR, Beale R, et al. Drotrecogin alfa (activated) treat-ment in severe sepsis from the global open-label trial ENHANCE: furtherevidence for survival and safety and implications for early treatment. CritCare Med. 2005;33(10):2266–2277.
405. Siegel JP. Assessing the use of activated protein C in the treatment of severesepsis. N Engl J Med. 2002;347(13):1030–1034.
406. Nadel S, Goldstein B, Williams MD, et al. Drotrecogin alfa (activated) inchildren with severe sepsis: a multicentre phase III randomised controlledtrial [see comment]. Lancet. 2007;369(9564):836–843.
407. Alejandria MM, Lansang MA, Dans LF, et al. Intravenous immunoglobulinfor treating sepsis and septic shock. Cochrane Database Syst Rev. 2002;(1):CD001090.
408. Douzinas EE, Pitaridis MT, Louris G, et al. Prevention of infection in multi-ple trauma patients by high-dose intravenous immunoglobulins. Crit CareMed. 2000;28(1):8–15.
409. Darenberg J, Ihendyane N, Sjolin J, et al. Intravenous immunoglobulin Gtherapy in streptococcal toxic shock syndrome: a European randomized,double-blind, placebo-controlled trial. Clin Infect Dis. 2003;37(3):333–340.
410. Pitcairn M, Schuler J, Erve PR, et al. Glucocorticoid and antibiotic effecton experimental gram-negative bacteremic shock. Arch Surg. 1975;110(8):1012–1015.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-57 GRBT291-3318G GRBT291-Gabrielli-v2.cls March 14, 2008 13:12
38 Section VI: Shock States
411. Sprung CL, Caralis PV, Marcial EH, et al. The effects of high-dose corti-costeroids in patients with septic shock. A prospective, controlled study. NEngl J Med. 1984;311(18):1137–1143.
412. Bone RC, Fisher CJ Jr, Clemmer TP, et al. A controlled clinical trial ofhigh-dose methylprednisolone in the treatment of severe sepsis and septicshock. N Engl J Med. 1987;317(11):653–658.
413. Luce JM, Montgomery AB, Marks JD, et al. Ineffectiveness of high-dosemethylprednisolone in preventing parenchymal lung injury and improvingmortality in patients with septic shock. Am Rev Resp Dis. 1988;138(1):62–68.
414. The Veterans Administration Systemic Sepsis Cooperative Study Group.Effect of high-dose glucocorticoid therapy on mortality in patients withclinical signs of systemic sepsis. N Engl J Med. 1987;317(11):659–665.
415. Schiffl H, Lang SM, Fischer R. Daily hemodialysis and the outcome of acuterenal failure. N Engl J Med. 2002;346(5):305–310.
416. Ronco C, Bellomo R, Homel P, et al. Effects of different doses in contin-uous veno-venous haemofiltration on outcomes of acute renal failure: aprospective randomised trial. Lancet. 2000;356(9223):26–30.
417. Phu NH, Hien TT, Mai NT, et al. Hemofiltration and peritoneal dialysisin infection-associated acute renal failure in Vietnam. N Engl J Med. 2002;347(12):895–902.
418. Krinsley JS. Association between hyperglycemia and increased hospitalmortality in a heterogeneous population of critically ill patients. Mayo ClinProc. 2003;78(12):1471–8.
419. Van den BG, Wouters P, Weekers F, et al. Intensive insulin therapy in thecritically ill patients. N Engl J Med. 2001;345(19):1359–1367.
420. Latham R, Lancaster AD, Covington JF, et al. The association of dia-betes and glucose control with surgical-site infections among cardiotho-racic surgery patients. Infect Control Hosp Epidemiol. 2001;22(10):607–612.
421. Van den BG, Wilmer A, Hermans G, et al. Intensive insulin therapy in themedical ICU. N Engl J Med. 2006;354(5):449–461.
422. Hermans G, Wilmer A, Meersseman W, et al. Impact of intensive insulintherapy on neuromuscular complications and ventilator dependency in themedical intensive care unit. Am J Resp Crit Care Med. 2007;175(5):480–489.
423. Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients.N Engl J Med. 2003;348(8):727–734.
424. Annane D, Bellissant E, Sebille V, et al. Impaired pressor sensitivity tonoradrenaline in septic shock patients with and without impaired adrenalfunction reserve. Br J Clin Pharmacol. 1998;46:589–597.
425. Briegel J, Forst H, Haller M, et al. Stress doses of hydrocortisone reversebyperdynamic septic shock: a prospective randomized, double-blind, single-center study. Crit Care Med. 1999;27(4):723–732.
426. Bollaert PE, Charpentier C, Levy B, et al. Reversal of late septic shock withsupraphysiologic doses of hydrocortisone. Crit Care Med. 1998;26(4):645–650.
427. Keh D, Boehnke T, Weber-Cartens S, et al. Immunologic and hemodynamiceffects of “low-dose” hydrocortisone in septic shock: a double-blind, ran-domized, placebo-controlled, crossover study. Am J Resp Crit Care Med.2003;167(4):512–520.
428. Annane D, Sebille V, Charpentier C, et al. Effect of treatment with lowdoses of hydrocortisone and fludrocortisone on mortality in patients withseptic shock. JAMA. 2002;288(7):862–871.
429. Hamrahian AH, Oseni TS, Arafah BM. Measurements of serum free cortisolin critically ill patients. N Engl J Med. 2004;350(16):1629–1638.
430. Sprung C, Annane D, Briegel J, et al. Corticosteroid therapy of septic shock(CORTICUS). Am J Resp Crit Care Med. 2007;175:A507.
431. Ranieri VM, Suter PM, Tortorella C, et al. Effect of mechanical venti-lation on inflammatory mediators in patients with acute respiratory dis-tress syndrome: a randomized controlled trial [see comment]. JAMA.1999;282(1):54–61.
432. Tremblay L, Valenza F, Ribeiro SP, et al. Injurious ventilatory strategiesincrease cytokines and c-fos m-RNA expression in an isolated rat lungmodel. J Clin Invest. 1997;99(5):944–952.
433. International consensus conferences in intensive care medicine: Ventilator-associated Lung Injury in ARDS. This official conference report was cospon-sored by the American Thoracic Society, The European Society of IntensiveCare Medicine, and The Societe de Reanimation de Langue Francaise, andwas approved by the ATS Board of Directors, July, 1999. Am J Resp CritCare Med. 1999;160(6):2118–2124.
434. Bernard GR, Artigas A, Brigham KL, et al. The American-European Con-sensus Conference on ARDS. Definitions, mechanisms, relevant outcomes,and clinical trial coordination. Am J Resp Crit Care Med. 1994;149(3 Pt 1):818–824.
435. Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome[see comment]. N Engl J Med. 1998;338(6):347–354.
436. Stewart TE, Meade MO, Cook DJ, et al. Evaluation of a ventilation strategyto prevent barotrauma in patients at high risk for acute respiratory distresssyndrome. Pressure- and Volume-Limited Ventilation Strategy Group. NEngl J Med. 1998;338(6):355–361.
437. Hussain SN, Graham R, Rutledge F, et al. Respiratory muscle energeticsduring endotoxic shock in dogs. J Appl Physiol. 1986;60(2):486–493.
438. Leon A, Boczkowski J, Dureuil B, et al. Effects of endotoxic shock ondiaphragmatic function in mechanically ventilated rats. J Appl Physiol.1992;72(4):1466–1472.
439. Marik PE, Zaloga GP. Early enteral nutrition in acutely ill patients: a sys-tematic review. Crit Care Med. 2001;29(12):2264–2270.
440. Heyland DK. Nutritional support in the critically ill patients. A criticalreview of the evidence. Crit Care Clin. 1998;14(3):423–440.
441. Heyland DK, MacDonald S, Keefe L, et al. Total parenteral nutritionin the critically ill patient: a meta-analysis. JAMA. 1998;280(23):2013–2019.
442. Moore FA, Feliciano DV, Andrassy RJ, et al. Early enteral feeding, com-pared with parenteral, reduces postoperative septic complications. The re-sults of a meta-analysis. Ann Surg. 1992;216(2):172–183.
443. Cooper DJ, Walley KR, Wiggs BR, et al. Bicarbonate does not improvehemodynamics in critically ill patients who have lactic acidosis. A prospec-tive, controlled clinical study Ann Intern Med. 1990;112:492–498.
444. Mathieu D, Neviere R, Billard V, et al. Effects of bicarbonate therapy onhemodynamics and tissue oxygenation in patients with lactic acidosis: aprospective, controlled clinical study. Crit Care Med. 1991;19(11):1352–1356.
445. van der Poll T, van Deventer SJ. Cytokines and anticytokines in the patho-genesis of sepsis. Infect Dis Clin North Am. 1999;13(2):413–426.
446. Leaver SK, Finney SJ, Burke-Gaffney A, et al. Sepsis since the discoveryof Toll-like receptors: disease concepts and therapeutic opportunities. CritCare Med. 2007;35(5):1404–1410.
447. Van Amersfoort ES, Van Berkel TJ, Kuiper J, et al. Receptors, mediators,and mechanisms involved in bacterial sepsis and septic shock. Clin MicroRev. 2003;16(3):379–414.
448. Arcaroli J, Fessler MB, Abraham E, et al. Genetic polymorphisms and sepsis.Shock. 2005;24(4):300–312.
449. Lin MT, Albertson TE, Lin MT, et al. Genomic polymorphisms in sepsis.Crit Care Med. 2004;32(2):569–579.
450. Texereau J, Pene F, Chiche JD, et al. Importance of hemostatic gene poly-morphisms for susceptibility to and outcome of severe sepsis. Crit CareMed. 2004;32(5 Suppl):S313–S319.
451. Papathanassoglou ED, Giannakopoulou MD, Bozas E, et al. Genomicvariations and susceptibility to sepsis. AACN Advanced Critical Care.2006;17(4):394–422.
452. Sharma S, Mink S. Septic shock. http://www.emedicine.com/MED/topic2101.htm. 2007. AU: Please
add dateaccessed.