Chapter 4 Review of MAMI guidelines - ennonline.net · notes International guidelines: WHO...
46
48 Chapter 4 Review of MAMI guidelines
Transcript of Chapter 4 Review of MAMI guidelines - ennonline.net · notes International guidelines: WHO...

48
Chapter 4 Review of MAMI guidelines

Management of Acute Malnutrition in Infants (MAMI) Project
49
Chapter 4 Review of MAMI guidelines
Chapter 4: Review of MAMI guidelines
This chapter reviews current guidelines on the management of acute malnutrition, both inpatient and community-based. The chapter looks at similarities and differences on how infants <6m are treated and identifies strengths, weaknesses and gaps in guidance materials.
4.1 Why population burden of disease mattersA review of current recommended approaches to managing acute malnutrition in infants <6m was carriedout to:
• Contextualise and help interpret quantitative feeding programme data (Chapter 5)• Contextualise and help interpret qualitative data from key informant interviews (Chapter 6)• Help set a baseline for future progress in the management of infants <6m malnutrition by:
- Understanding the range of current practices- Understanding the focus and emphasis of current guidelines- Identifying strengths of current guidelines- Identifying gaps in current guidelines
4.2 MethodsSAM and MAM guidelines and protocols (collectively referred to as guidelines from heron) were identified by purposive sampling of:
• Published guidelines available in print and on-line• Final and draft guidelines, obtained via MAMI steering group members and key informants.
Key themes and topics relevant to infants <6m were identified and tabulated. Internationally recognised AGREE (Appraisal of Guidelines for Research and Evaluation) criteria were used to appraise guideline quality130 (see Box 5). A formal AGREE scoring was not applied to each individual guideline, as this was beyond the scope of the MAMI Project. Instead an overview discussion highlights common issues.

Management of Acute Malnutrition in Infants (MAMI) Project
50
4.2 Methods
Scope and Purpose
1. The overall objective(s) of the guideline should be specifically described.
2. The clinical question(s) covered by the guideline should be specifically described.
3. The patients to whom the guideline is meant to apply should be specifically described.
Stakeholder Involvement
4. The guideline development group should include individuals from all the relevant professional
groups.
5. The patients’ views and preferences should be sought.
6. The target users of the guideline should be clearly defined.
7. The guideline should be piloted among end users.
Rigour of Developement
8. Systematic methods should be used to search for evidence.
9. The criteria for selecting the evidence should be clearly described.
10. The methods used for formulating the recommendations should be clearly described.
11. Health benefits, side effects and risks should be considered.
12. There should be an explicit link between recommendations & supporting evidence.
13. The guideline should be externally reviewed by experts prior to publication.
14. A procedure for updating the guideline should be provided.
Clarity and Presentation
15. The recommendations should be specific and unambiguous.
16. Different options for diagnosis and/or treatment of the condition should be presented.
17. Key recommendations should be easily identifiable.
18. The guideline should be supported with tools for application.
Applicability
19. Potential organisational barriers in applying recommendations should be discussed.
20. Potential cost implications of applying the recommendations should be considered.
21. The guideline should presents key review criteria for monitoring and audit purposes
Editorial Independence
22. The guideline should be editorially independent from the funding body.
23. Conflicts of interest of guideline development members should be recorded.
Box 5: ‘AGREE’ CRITERIA (Appraisal of Guidelines for Research & Evaluation)
4.3 Guidelines overviewA total of 37 (14 international and 23 national) guidelines were identified for review. Table 5 presents an overview of the international organizations and countries represented. International guidelines were defined as generic guidelines, owned and written by one lead agency, UN or NGO, and intended for use in multiple settings. National guidelines were focused on one particular setting, often led by a Ministry of Health or other equivalent government body. The list presented is unlikely to be exhaustive. Other guidelines are known to be in development but were not available for this review.
Similarities between guidelinesThe many similarities between documents were striking. This partly reflects common ‘evolutionary origins’.The ‘common ancestor’ of almost all current guidelines is the 1999 WHO guideline on management of SAM.131This formalised the ‘phased’ (stabilisation and rehabilitation) treatment of acute malnutrition and included a description of the ’ten steps’ approach to care (see Figure 8 in chapter 2). Thus WHO (1999) is widely referenced and often directly summarised in subsequent documents. CMAM approaches represent another major step forward in the ‘evolution’ of treatment for SAM and many guidelines also draw on Valid(2006) as a key source.132
This ‘common origins’ finding has several implications. If two programmes use the same guidelines then it is, in theory, possible to compare programme outcomes and assess impact of context factors, such as

Management of Acute Malnutrition in Infants (MAMI) Project
51
4.3 Guidelines overview
quality of implementation or patient profiles. Common terminologies and shared understandings also enable global sharing of ideas and staff exchange. A possible disadvantage of having guidelines that come as a ‘package’, is that individual elements become ‘standard’ and difficult to withhold, even if the underlying evidence for them is slim.
Differences between guidelinesThere are many minor inter-guideline variations. Mostly these are explanations of particular issues, rather than major differences in approach. This makes it difficult to disentangle whether guidelines themselves or other factors (e.g. severity of disease, availability of resources to implement the guidelines, willingness and ability of staff to implement the guidelines, background social circumstances impacting SAM/MAM) are responsible for good or bad patient outcomes. It is especially difficult to infer the effects of multiple minor variations.
IFE Module 2 stands out as different from the other guidelines reviewed here. Whilst created as a training tool, IFE Module 2 provides a ‘stop gap’ in MAMI guidance. Chapter 8 of Module 2 is specifically devoted to the management of SAM in infants <6m, the basis for which is the collation of SAM guidelines and experiences of NGOs, as well as expert authorship from relevant professionals and field teams. Consequently IFE Module 2 content on SAM largely reflects many of the NGO approaches and guidelines reviewed by the MAMI Project, with a strengthened breastfeeding component.
Evolutionary developments across the guidelines The main development since the WHO (1999) inpatient guidelines is that outpatient approaches to SAM treatment are now widely accepted for cases without medical complications. The majority of recent guidelines recognise outpatient-based models of care as complementary to inpatient care.
Also notable is that national SAM/MAM guidelines obtained for this report are very recent, mostly from the last two to three years, the oldest being Burundi in 2002. It is not known whether there were earlier guidelines pre-dating these. Whatever the case, there is evidently a clear trend towards both global rollout of SAM/MAM strategies and increasing national ownership of SAM/MAM guidelines.
Focus on infants <6m in current guidelinesThe majority of guidelines have a separate section focusing explicitly on infants <6m, which varies widely in length. A few, including WHO (1999), recognize infants <6m only indirectly as part of a broader age group, e.g. children <5 years. In the CTC Manual (Valid, 2006), one of the foundation reference materials for CMAM, infants <6m are only referred to in one small section.

Management of Acute Malnutrition in Infants (MAMI) Project
52
4.3 Guidelines overview
Table 5: Overview of available acute malnutrition guidelines
Guideline type Authors / contributors
Region CountryorOrgan-ization
Guideline Date CMAMorInpatientonly
SAMorMAMfocus
language draftorfinal
MoH UNICEF WHO Interna-tional NGOorconsultant
Local NGO orconsul-tant
notes
International guidelines:
WHO Managementof severemalnutrition:a manual forphysicians &other seniorhealthworkers*
1999 Inpatientonly
SAM English,Spanish,French,Portuguese
FIN n/a n/a Y Y n/a available on WHO website http://www.who.int /nutrition/publications/ severemalnutrition/ 9241545119/en/index.html
WHO Guidelines forthe inpatienttreatment ofseverelymalnourishedchildren *
2003 Inpatientonly
SAM English,French,Spanish
FIN n/a n/a Y n/a n/a available on WHO website http://www.who.int/nutrition/publications/severemalnutrition/9241546093/en/index.html
WHO Manual forthe healthcare ofchildren inhumanitarianemergencies
2008 CMAM bothSAMandMAM
English FIN n/a n/a Y n/a n/a available on WHOwebsite:http://whqlibdoc.who.int/publications/2008/9789241596879_eng.pdf
WHO Pocket bookofHospital carefor children(Guidelinesfor themanagementof commonillnesses withlimitedresources)*
2005 Inpatientonly
SAM English,French,Portuguese,Russian
FIN n/a n/a Y Y n/a available on WHO webs http://www.who.int/child_adolescent_health/documents/9241546700/en/index.htmlNoted that this "updates & expands guidelines inWHO 2000 'Management of the child with a serious infection or severemalnutrition'"
WHO HandbookIMCIIntegratedManagementof ChildhoodIllness*
2005 n/a MAM(for SAMguidanceis torefer tohospital)
English,French
FIN n/a Y Y Y n/a available on WHO webhttp://www.who.int/child_adolescent_health/documents/9241546441/en/index.htmlThis is a book focused on all aspects of paediatric care at primary care level, of which assessment & treatment of malnutrition is just one chapter
ActionContre laFaim(ClaudinePrudhon)
Assessment &Treatment ofMalnutritionin EmergencySituations (Manual ofTherapeuticCare & Planningfor a NutritionalProgramme)
2002 Inpatientonly
bothSAMandMAM
English FIN n/a n/a n/a Y n/a Book covering multiple aspects of nutrition: treatment is just one section
MSF NutritionGuidelines(1st edition)
1995 inpatientonly
bothSAMandMAM
English FIN n/a n/a n/a Y n/a Book covering multipleaspects of nutrition: treatment is just one section
Inte
rnat
iona
l

Management of Acute Malnutrition in Infants (MAMI) Project
53
4.3 Guidelines overview
Guideline type Authors / contributors
Region Country orOrganization
Guideline Date CMAMorInpatientonly
SAMorMAMfocus
language draftorfinal
MoH UNICEF WHO Internat-ional NGOorconsultant
Local NGO orconsul-tant
notes
International guidelines:
MSF NutritionGuidelines
May2006
CMAM bothSAMandMAM
English FIN n/a n/a n/a Y n/a Update of 1995guidelines, though available in electronic version rather as a book
MSF GuidelineInfants lessthan 6 monthsold (Benson)MSF - OCBA
Oct2007
n/a SAM English ? n/a n/a n/a Y n/a This is a chapter ocused on infants alone and is one of a wider set of guidelines relating to malnutrition
ValidInternational
Community-basedTherapeuticCare (CTC), Afield manual (first edition)
2006 CMAM bothSAMandMAM
English FIN n/a n/a n/a Y n/a book describing multiple aspects
UNHCR Handbook forEmergencies(thirdedition)
Feb2007
CMAM bothSAMandMAM
English FIN n/a n/a n/a Y n/a Available onlinehttp://www.unhcr.org/publ/PUBL/ 471db4c92.htmlNB Interesting to note that 3rd edition has significantly more IYCF detail than 2nd
UNHCR Themanagementof Nutritionin MajorEmergencies
2000 Inpatientonly
bothSAMandMAM
English FIN n/a n/a Y Y n/a book covering multiple aspects of nutrition
IFE CoreGroup
InfantFeeding inEmergenciesIFE module 2,version 1.1for healthand nutritionworkers inemergencysituations, fortraining,practice andreference
Dec2007
n/a SAM English FIN n/a n/a n/a Y n/a Training modulecovering externsivedetails of IYCF especiallyskilled breastfeedingsupport produced in UNand NGO collaborationwith expert collaboratorsand review. Includes achapter dedicated tomanagement of acutelymalnourished infants <6m (Chapter 8), supported by content in other chapters. Available on ENN website:http://www.ennonline.net/resources/view.aspx?resid=4
ICRC(InternationalCommittee ofthe Red Cross)
NutritionManual forHumanitarianAction
Aug2008
n/a English FIN n/a n/a n/a Y n/a Book covering multiple aspects of nutrition. Includes 1 chapter onTherapeutic Feeding and 1 on Supplementary Feeding Available onICRC website: http://www.icrc.org/web/eng/siteeng0.nsf/html/p0820
Table 5 cont’d
Inte
rnat
iona
l

Management of Acute Malnutrition in Infants (MAMI) Project
54
4.3 Guidelines overview
Guideline type Authors / contributors
Region Country orOrgan-ization
Guideline Date CMAMorInpatientonly
SAMorMAMfocus
language draftorfinal
MoH UNICEF WHO Interna-tional NGOorconsultant
Local NGO orconsult-ant
notes
National guidelines
Burundi ProtocoleNational deNutrition
Aug2002
Inpatientonly
French FIN Y Y Y Y Y
Ethiopia Protocol fortheManagementof SevereAcuteMalnutrition
Mar2007
CMAM SAMonly
English FIN Y Y Y no Y
Madagascar Depistage etprise encharge de lamalnutritionaigue
Sep2007
CMAM bothSAMandMAM
French FIN Y Y Y ? ?
Malawi Guidelines fortheManagementof SevereAcuteMalnutrition(book T3)
2007 Inpatientonly
SAM English FIN Y Y Y Y Y One of a set of guidelines on acutemalnutrition - othersfocus on CMAM.Separate MAM / CMAMguidelines available
Mozambique Manual deOrientacaoparaTratamentodaDesnutricaoAguda Grave
Jun2008
CMAM bothSAMandMAM
Portugese Dr Y Y ? Y Y recently replaced 2007protocol
Tanzania Managementof AcuteMalnutritionNationalGuidelines
2008 CMAM bothSAM(mainfocus)andMAM
English FIN Y Y Y Y Y includes checklist ofSAM management
Uganda IntegratedManagementof AcuteMalnutrition
Nov2006
inpatientonly
bothSAMandMAM
English Dr Y Y ? Y ? reference made toseparate guidelinesfocused on therapeuticfeeding centres
Zambia IntegratedManagementof AcuteMalnutrition
2009 CMAM bothSAM(mainfocus)andMAM
English Dr Y ? ? Y ? includes supervisionchecklist
Zimbabwe Guidelines fortheManagementof SevereAcuteMalnutritionthroughCommunity-basedTherapeuticCare (CTC)
2008 CMAM bothSAM(mainfocus)andMAM
English FIN Y Y n/s Y Y guidelines include: 1) supervision checklist2) indicators forassessing quality &appropriatenessReference also made tothe "Zimbabwetherapeutic feedingprotocol" which outlinesdetails of infant <6mcare
Table 5 cont’d
1. a)
East
ern
Afric
a

Management of Acute Malnutrition in Infants (MAMI) Project
55
4.3 Guidelines overview
Guideline type Authors / contributors
Region Country orOrgan-ization
Guideline Date CMAMorInpatientonly
SAMorMAMfocus
language draftorfinal
MoH UNICEF WHO Interna-tional NGOorconsultant
Local NGO orconsult-ant
notes
National guidelines
DRC ProtocolNational dePrise en Chargede laMalnutritionAigue
Oct2008
CMAM French FIN Y Y ? Y ? Acknowledgements page blank
Sudan(Southern)
Guidelines fortheManagementof Severe AcuteMalnutrition
Jul2008
CMAM SAM English Dr Y Y Y Y ? references WHO(1999), Valid (2006) & Golden & Grellety as sources
Sudan(North)
NationalIntegratedManual on theManagementof Severe AcuteMalnutritionin healthfacilities & atcommunitylevel
Jan2008
CMAM SAM English Dr Y Y Y Y n/s (for medical doctors and senior healthworkers)
Botswana Guidelines fortheManagementof Severe AcuteMalnutrition inChildren
Jun2007
CMAM SAM English Dr Y Y Y Y Y noted that developed in line with WHO reference manuals, 1999, 2003
BurkinaFaso
None yet - indraft
n/s CMAM bothSAMandMAM
French Dr ? ? ? ? ? only draft outline available
CoteD'Ivoire
ProtocoleNational dePrise en chargede lamalnutritionsevere
May2005
Inpatient only(CMAM typehometreatmentnoted inannex
French FIN Y Y Y Y Y
Guinea ProtocoleNational dePrise en Chargede laMalnutritionAigue
May2008
CMAM SAMandMAM
French FIN Y Y ? ? ?
Mali ProtocoleNational de laprise en chargede lamalnutritionaigue
Dec2007
CMAM SAMandMAM
French Dr Y Y Y Y Y
Niger ProtocolNational dePrise en Chargede laMalnutritionAigue
Dec2006
CMAM bothSAMandMAM
French FIN Y Y Y Y Y
Table 5 cont’d
1.b)
Mid
dle A
frica
1.d)
Sout
hern
Afric
a1.
e) W
este
rn A
frica

Management of Acute Malnutrition in Infants (MAMI) Project
56
4.3 Guidelines overview
Guideline type Authors / contributors
Region Country orOrgan-ization
Guideline Date CMAMorInpatientonly
SAMorMAMfocus
language draftorfinal
MoH UNICEF WHO Interna-tional NGOorconsultant
Local NGO orconsult-ant
notes
National guidelines
Senegal Protocole deprise en chargede lamalnutritionaigue
May2008
CMAM bothSAMandMAM
French FIN Y Y Y Y Y
Afghanistan Community-basedManagement ofAcuteMalnutritionprogramme inAqcha andMardyanDistrict ofJawzjanProvinceNorthernAfghanistan(StabilizationCentreGuidelines)
June2008
CMAM SAM English Dr Y Y Y No Y compiled by Savethe Children UK
India Indian Academyof Paeditricsguidelines
2006 Inpatient only SAM English FIN Y Y Y No Y Published injournal 'IndianPaediatrics, (2007: 44: 443-61)
Pakistan Protocol for theinpatienttreatment ofseverelymalnourishedchildren in thePakistanearthquakeemergency
Dec2005
Inpatient only SAM English Dr Y Y Y Y Y based on WHO 1999protocol
Sri Lanka None yet - indraftManagement ofSevere AcuteUndernutrition:Manual forHealth Workersin Sri Lanka
n/s CMAM bothSAMandMAM
French Dr ? ? ? ? ? only draft outline available
Table 5 cont’d
*These WHO resources are the same guideline produced in different formats.
Management of Acute Malnutrition in Infants (MAMI) Project
57
4.4 Guideline Comparisons
4.4 Guideline Comparisons
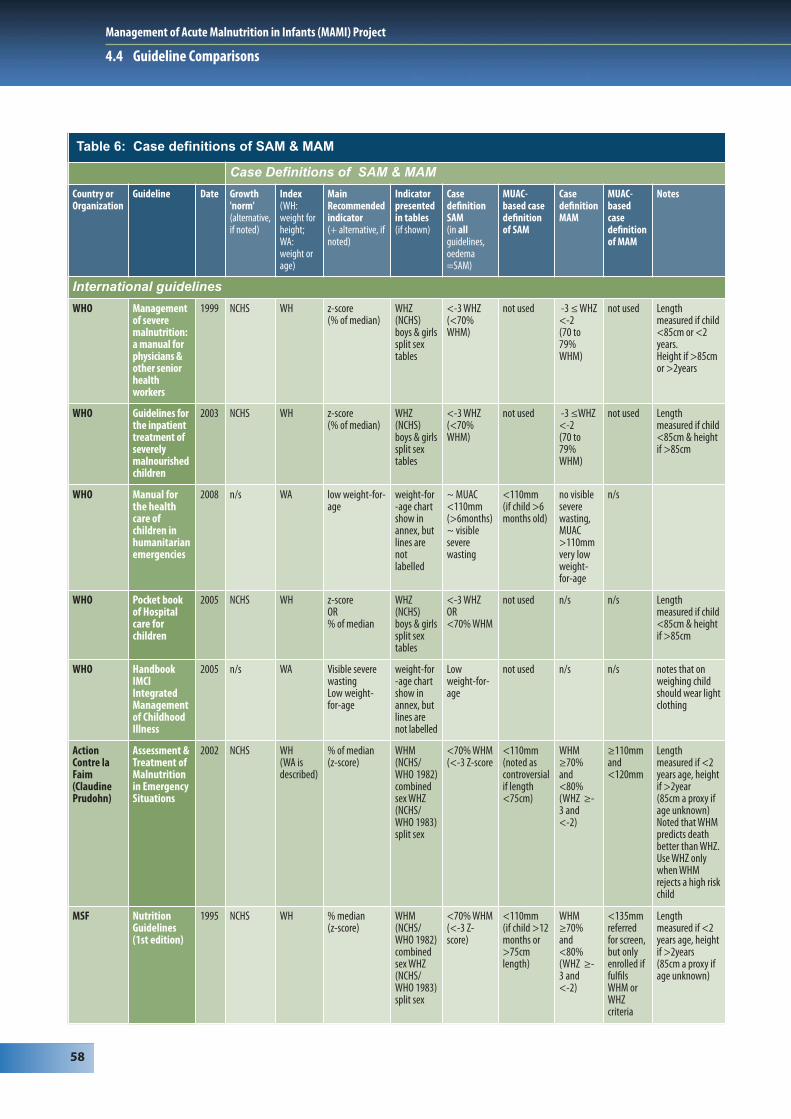
4.4.1 Case definitions of SAM & MAM (general)See Table 6 for an overview of case definitions. All guidelines reviewed use anthropometry as the main indicator for SAM/MAM. All also acknowledge oedematous malnutrition as an indicator of SAM.
Weight-for-height vs. weight-for-ageMost guidelines use weight-for-length criteria as recommended by WHO (1999). Cutoffs for SAM and MAMare also mostly consistent with WHO (1999). Exceptions are the 2008 WHO Manual on healthcare of children in emergencies and IMCI guidelines, which both use weight-for-age as the main indicator (although IMCI also uses visible severe wasting as an alternative). This difference must be addressed.
NCHS vs. WHO-GS (in context of z-score vs. %-of-median)NCHS growth references are still dominant in the guidelines reviewed. Only Sri Lanka and Mozambique explicitly use WHO-GS, though several other guidelines do footnote their availability alongside NCHS. It is only recently, in May 2009 that UNICEF and WHO released a joint statement formally recommending the new WHO-GS for identifying severe acute malnutrition133. It is likely therefore that their use will increase in the coming years. Some of the possible implications of this change for infants are discussed in Chapter 3.
MUACMUAC is increasingly used in SAM/MAM guidelines. It is an independent admission criterion noted alongside weight-for-height, and in a small number or guidelines (Valid 2006, Uganda 2006), it is the major case definition criterion. No guidelines recommend its use in infants <6m.
Management of Acute Malnutrition in Infants (MAMI) Project
58
4.4 Guideline Comparisons
Table 6: Case definitions of SAM & MAM
Case Definitions of SAM & MAM
Country orOrganization
Guideline Date Growth'norm'(alternative,if noted)
Index (WH:weight forheight;WA:weight orage)
MainRecommendedindicator (+ alternative, ifnoted)
Indicatorpresentedin tables(if shown)
CasedefinitionSAM(in allguidelines,oedema=SAM)
MUAC-based casedefinitionof SAM
CasedefinitionMAM
MUAC-basedcasedefinitionof MAM
Notes
International guidelines
WHO Managementof severemalnutrition:a manual forphysicians &other seniorhealthworkers
1999 NCHS WH z-score(% of median)
WHZ(NCHS)boys & girls split sextables
<-3 WHZ (<70%WHM)
not used -3 ≤ WHZ <-2 (70 to79%WHM)
not used Lengthmeasured if child<85cm or <2years.Height if >85cmor >2years
WHO Guidelines forthe inpatienttreatment ofseverelymalnourishedchildren
2003 NCHS WH z-score(% of median)
WHZ(NCHS)boys & girlssplit sextables
<-3 WHZ (<70%WHM)
not used -3 ≤WHZ<-2 (70 to79%WHM)
not used Lengthmeasured if child<85cm & heightif >85cm
WHO Manual forthe healthcare ofchildren inhumanitarianemergencies
2008 n/s WA low weight-for-age
weight-for-age chartshow inannex, butlines arenotlabelled
~ MUAC<110mm(>6months)~ visibleseverewasting
<110mm(if child >6months old)
no visibleseverewasting,MUAC>110mmvery lowweight-for-age
n/s
WHO Pocket bookof Hospitalcare forchildren
2005 NCHS WH z-scoreOR% of median
WHZ(NCHS)boys & girls split sextables
<-3 WHZ OR<70% WHM
not used n/s n/s Lengthmeasured if child<85cm & heightif >85cm
WHO HandbookIMCIIntegratedManagementof ChildhoodIllness
2005 n/s WA Visible severewastingLow weight-for-age
weight-for-age chartshow inannex, butlines arenot labelled
Low weight-for-age
not used n/s n/s notes that onweighing childshould wear lightclothing
ActionContre laFaim(ClaudinePrudohn)
Assessment &Treatment ofMalnutritionin EmergencySituations
2002 NCHS WH (WA isdescribed)
% of median(z-score)
WHM(NCHS/WHO 1982)combinedsex WHZ(NCHS/WHO 1983)split sex
<70% WHM (<-3 Z-score
<110mm(noted ascontroversialif length<75cm)
WHM≥70%and<80% (WHZ ≥-3 and<-2)
≥110mmand<120mm
Lengthmeasured if <2years age, heightif >2year(85cm a proxy ifage unknown) Noted that WHMpredicts deathbetter than WHZ.Use WHZ onlywhen WHMrejects a high riskchild
MSF NutritionGuidelines(1st edition)
1995 NCHS WH % median (z-score)
WHM(NCHS/WHO 1982)combinedsex WHZ(NCHS/WHO 1983)split sex
<70% WHM (<-3 Z-score)
<110mm(if child >12months or>75cmlength)
WHM≥70%and<80% (WHZ ≥-3 and<-2)
<135mmreferredfor screen,but onlyenrolled iffulfilsWHM orWHZcriteria
Lengthmeasured if <2years age, heightif >2years(85cm a proxy ifage unknown)

Management of Acute Malnutrition in Infants (MAMI) Project
59
4.4 Guideline Comparisons
Case Definitions of SAM & MAM
Country orOrganization
Guideline Date Growth'norm'(alternative,if noted)
Index (WH:weight forheight;WA:weight orage)
MainRecommendedindicator (+ alternative, ifnoted)
Indicatorpresentedin tables(if shown)
CasedefinitionSAM(in allguidelines,oedema=SAM)
MUAC-based casedefinitionof SAM
CasedefinitionMAM
MUAC-basedcasedefinitionof MAM
Notes
International guidelines
MSF NutritionGuidelines
May2006
NCHS WH % median(notes z-scoresused in somecountries
n/a <70%WHM (<-3 Z-score)
<110mm(if child >6months old)
WHM≥70%and<80% (WHZ ≥-3 and<-2)
n/s
MSF ProtocolInfants lessthan 6months old(Benson)MSF - OCBA
Oct2007
n/s WH % of median WHM(NCHS/WHO 1982)combinedsex WHZ(NCHS/WHO 1983)split sex
<70%WHM
n/a (focus ison infants<6m)
n/a n/a
ValidInternational
Community-basedTherapeuticCare (CTC), Afield manual(first edition)
2006 NCHS MUAC* UnadjustedMUAC %median or Z-score noted
no tablesshown
<70%WHM<-3WHZ
<110mm (if length>65cm)
WHM≥70% and<80%(WHZ ≥-3 and<-2)
110mm to<125mm
* MUACemphasised asprimarymeasure(WHnoted)
UNHCR Handbook forEmergencies(thirdedition)
Feb2007
NCHS* WH % of medianORz-score
no tablesshown
<70%WHM (or<-3 Z-score)
<110mm(if aged 6 to59months)
70% to79% WHM(-3 to -2WHZ)
110mm to<125mm
also mentionLBW babies (nodetails given) * recognisedWHO & statesthat UNHCR is inprocess ofassessing thenew standards
UNHCR Themanagementof Nutrition inMajorEmergencies
2000 NCHS WA z-score (% of median)
WHZ(NCHS)boys & girls split sextables
<-3 WHZ(<70%WHM)
<-3 ZMUAC-for-age /MUAC-for-height
≥-3 to <-2 WHZ (70 to79% WHM
≥-3 ZMUAC-f-age/MUAC-f-height to<-2z
notes that onweighing childshould wear lightclothing
IFE CoreGroup
InfantFeeding inEmergenciesIFE Module 2,version 1.1
Dec2007
NCHS WH % of median tables notshown
<70%WHM(NCHS)
n/a (focus ison infants<6m)
n/s n/s n/s
ICRC NutritionManual forHumanitarianAction
Aug2008
NCHS WH(describesotherindices,incl WA,MUAC)
z-score (describes otherindicators)
WHZ(NCHS)boys & girls split sextables(MUAC byage Z-scoretables alsogiven)
severaldescribed,including<-3 WHZ(NCHS) andMUAC-for-height <-3z (75%median)
<110mm(<125mmalso referredto as 'severe' inanthro-pometrychapter)
140 or135mm to125mm
Lengthmeasured if <2years age, heightif >2 yearsnotes thatanthropometryshould not bethe only basis ofadmission
National guidelines
Burundi ProtocoleNational deNutrition
Aug2002
NCHS WH % of median combinedsex, WHM(NCHS)
<70%WHM(NCHS)
<110mm(if length>65cm)
between70 to 79%WHM
<125mm height <65cmequated withage <6 monthsno referencegiven for tables
Table 6 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
60
4.4 Guideline Comparisons
Case Definitions of SAM & MAM
Country orOrganization
Guideline Date Growth'norm'(alternative,if noted)
Index (WH:weight forheight;WA:weight orage)
MainRecommendedindicator (+ alternative, ifnoted)
Indicatorpresentedin tables(if shown)
CasedefinitionSAM(in allguidelines,oedema=SAM)
MUAC-based casedefinitionof SAM
CasedefinitionMAM
MUAC-basedcasedefinitionof MAM
Notes
National guidelines
Ethiopia Protocol for theManagementof Severe AcuteMalnutrition
Aug2002
NCHS WH % of median combinedsex, WHM(NCHS)
<70%WHM(NCHS)
<110mm(if length>65cm)
between70 to 79%WHM
<125mm height <65cmequated withage <6 monthsno referencegiven for tables
Madagascar Depistage etprise en chargede lamalnutritionaigue
Sep2007
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(if length>65cm)
70 to 79%WHM
n/s
Malawi Guidelines fortheManagementof Severe AcuteMalnutrition(book T3)
2007 NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(ages 1 to 5years)
70 to 79% 110 to119mm
(NB printed as acard separate tothe book)
Mozambique Manual deOrientacaoparaTratamento daDesnutricaoAguda Grave
Jun2008
WHO-GS(2007protocolusedNCHS)
WH % of median * tablelabelled"% ofmedian(WHO-2004)joint sex
<70%WHM
<110mm 70 to 79%WHM
110 to125mm
* appears tohave calculatedweight cut-offsbased on WHO(2006) boysmedian tables Lengthmeasured if child<85cm & heightif >85cm
Tanzania Managementof AcuteMalnutritionNATIONALGuidelines
2008 NCHS WH % of medianOR z-score
WHZ(NCHS)boys &girls splitsex tables
<70%WHM OR<-3 WHZ
<110mm(6-59m or65 to110cm)
70-79%WHM or<-2SD
110-120mm
Lengthmeasured if child<85cm & heightif >85cm
Uganda IntegratedManagementof AcuteMalnutrition
Nov2006
n/s MUACemphasis-ed
UnadjustedMUAC %median or Z-score noted
no tablesshown
<70%WHM <-3WHZ
<110mm (if length>65cmand/or>6months)
WHM≥70% and<80%(WHZ ≥-3and <-2)
110mm to<125mm
Zambia IntegratedManagementof AcuteMalnutrition
2009 NCHS* WH % of median no tablesshown
<70%WHM OR<-3 WHZ
<110mm(6-59m)
WHM≥70%and <80% (WHZ ≥-3 and<-2)
≥110 and<125mm
*WHO GS notedas a footnote inthe introductionbut notthereafter**z-score notedonce inintroduction butnot thereafter)
Zimbabwe Guidelines fortheManagementof Severe AcuteMalnutritionthroughCommunity-basedTherapeuticCare (CTC)
2008 NCHS WH % of median WHZ(NCHS)boys &girls splitsex tables
<70%WHM
<110 70 to 80% 110 to125mm
Length if <85cmor <2 years,Height ≥85cm or>2years
Table 6 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
61
4.4 Guideline Comparisons
Case Definitions of SAM & MAM
Country orOrganization
Guideline Date Growth'norm'(alternative,if noted)
Index (WH:weight forheight;WA:weight orage)
MainRecommendedindicator (+ alternative, ifnoted)
Indicatorpresentedin tables(if shown)
CasedefinitionSAM(in allguidelines,oedema=SAM)
MUAC-based casedefinitionof SAM
CasedefinitionMAM
MUAC-basedcasedefinitionof MAM
Notes
National guidelines
DRC ProtocolNational dePrise en Chargede laMalnutritionAigue
Oct2008
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(if length>65cm)
70 to79.9%
110 to119mm
Sudan(Southern)
Guidelines fortheManagementof Severe AcuteMalnutrition
Jul2008
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(for height>65cm)
70 to79.9%
n/s Lengthmeasured if child<85cm & heightif >85cm*WHO GS notedas a footnote inthe introductionbut not thereafter** z-score notedonce inintroduction butnot thereafter
Sudan(North)
NationalIntegratedManual on theManagementof Severe AcuteMalnutritionin healthfacilities and atcommunitylevel
Jan2008
NCHS WH % of medianOR z-score
draft - notyetinserted
<70% <110mm(with length>65cm or>1year old)
≥-3 to <-2 WHZ or70 to 79%WHM
n/s Length if <85cmor <2 years,Height ≥85cm or>2years (tablesstate 85cm cutoff,text gives age OR85cm cutoff)
Botswana Guidelines fortheManagementof Severe AcuteMalnutrition inChildren
Jun2007
NCHS WH % of median annexesnotcomplete(draftguidelines)
<70%WHM(NCHS)
<110mm n/s n/s Length measuredif child <85cm &height if >85cmequates age<6months withheight <65cm*z-score notedonce inintroduction butnot thereafter
BurkinaFaso
Guidelines fortheManagementof Severe AcuteMalnutrition inChildren
Jun2007
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm ≥70 to<80%WHM
110 to125mm
equates age<6months withheight <65cm
CoteD'Ivoire
ProtocoleNational dePrise en chargede lamalnutritionsevere
May2005
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm n/s n/s Lengthmeasured if child<85cm & heightif >85cmequates age<6months withheight <65cm
Guinea ProtocoleNational dePrise en Chargede laMalnutritionAigue
May2008
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(if height>65cm)
≥70 to<80%WHM
110 to125mm
Lengthmeasured if child<85cm & heightif >85cm
Table 6 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
62
4.4 Guideline Comparisons
Case Definitions of SAM & MAM
Country orOrganization
Guideline Date Growth'norm'(alternative,if noted)
Index (WH:weight forheight;WA:weight orage)
MainRecommendedindicator (+ alternative, ifnoted)
Indicatorpresentedin tables(if shown)
CasedefinitionSAM(in allguidelines,oedema=SAM)
MUAC-based casedefinitionof SAM
CasedefinitionMAM
MUAC-basedcasedefinitionof MAM
Notes
National guidelines
Mali ProtocoleNational de laprise en chargede lamalnutritionaigue
Dec2007
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NCHS)
<110mm(if height>65cm)
≥70 to<80%WHM
110 to119mm
Length <85cm,Height ≥85cmequates age<6months withheight <65cm
Niger ProtocolNational dePrise en Chargede laMalnutritionAigue
Dec2006
NCHS WH % of median WHM(NCHS)combinedsex
<70%WHM(NHCS)(WHZ<-3WHO isfootnotedas analternativecasedefinition)
<110mm(for height>65cm)
70% to<80%WHM
n/s Length if <85cmor <2 years,Height ≥85cm or>2years
Senegal Protocole deprise en chargede lamalnutritionaigue
May2008
NCHS WH % of medianOR z-score
WHM(NCHS)combinedsex
<70%WHMOR<-3 WHZ
<110mm(if aged 6 to59 months)
≥-3 to <-2 WHZ or70 to 79%WHM
110 to125mm
Length if <2years, Height if>2 years <65cmlength seen asproxy for<6months age
Afghanistan Community-basedManagement ofAcuteMalnutritionprogramme inAqcha andMardyanDistrict ofJawzjanProvinceNorthernAfghanistan
June2008
notspecifited
WH % median(z-score)
annexesnotcomplete(draftguidelines)
<70%WHM(or <-3WHZ)
<110mm n/s n/s Length measuredif child <85cm &height if >85cmif age unknown,<65cm length isproxy for<6months age
India Indian Academyof Paeditricsguidelines
2006 NCHS WH % median(z-score)
not shown <70%WHM(or <-3WHZ)
<110mm n/s n/s
Pakistan Protocol for theinpatienttreatment ofseverelymalnourishedchildren in thePakistanearthquakeemergency
Dec2005
NCHS WH % median(z-score)
not shown(footnotessuggestthat Z-score tableas in WHO1999guidelineslikely to beinserted)
<70%WHM(or <-3WHZ)
not stated n/s n/s Lengthmeasured if child<85cm & heightif >85cm
Sri Lanka Management ofSevere AcuteUndernutrition:Manual forHealth Workersin Sri Lanka
2007 WHO WH z-score WHZ(WHO)split sex
<-3Z WHZ(WHO)
no n/s n/s Lengthmeasured if child<2years &height if >2years
Table 6 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
63
4.4 Guideline Comparisons
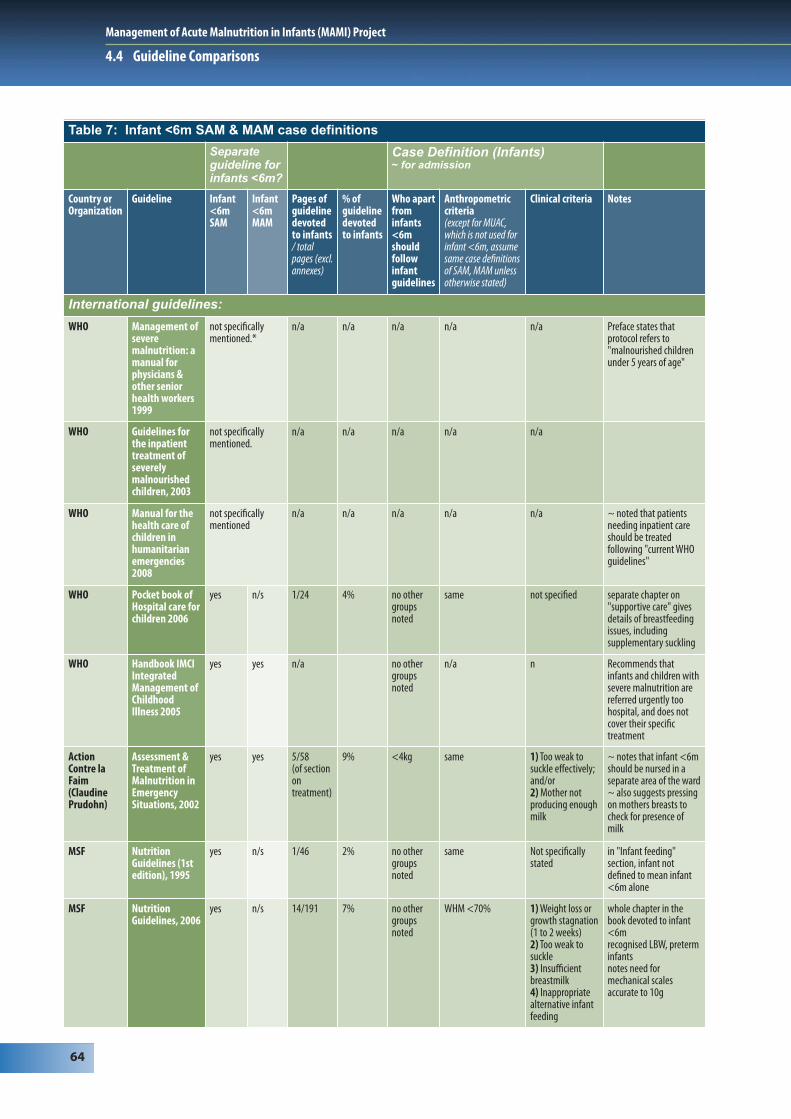
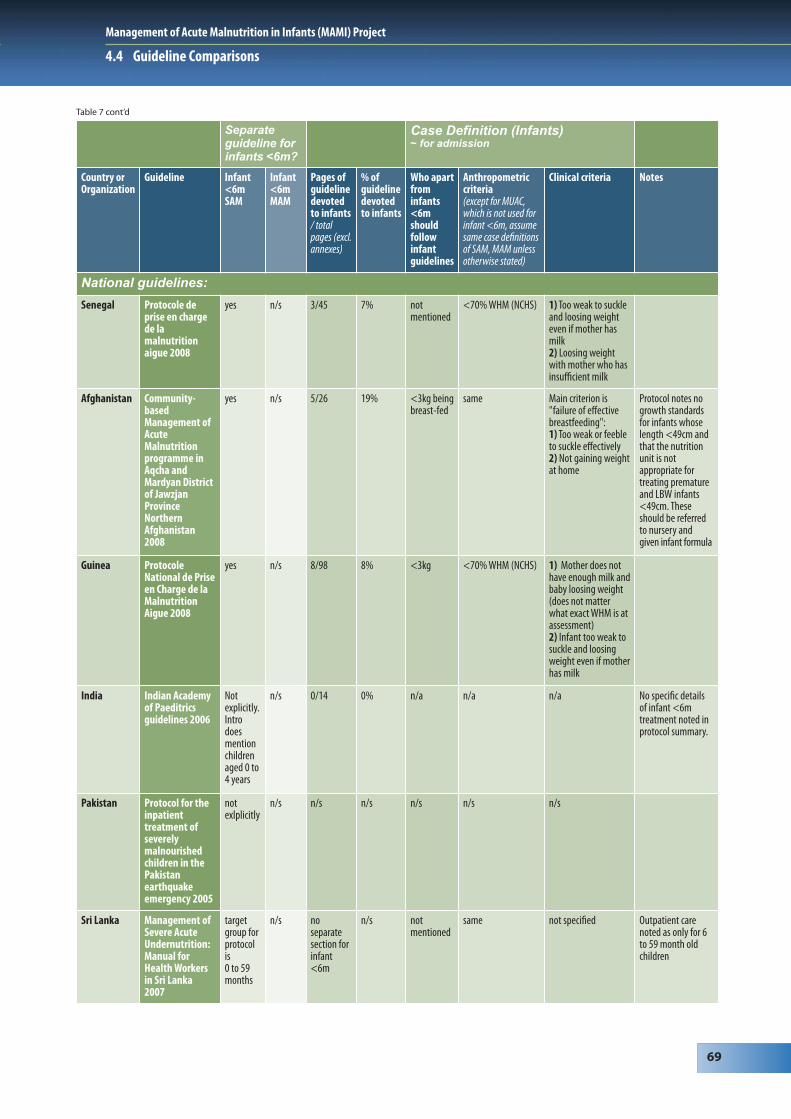
4.4.2 Infant <6m SAM and MAM case definitionsSee Table 7 for overview.
Infant <6m severe acute malnutrition (SAM)In all of the guidelines infants <6m with SAM are treated as inpatients. This includes CMAM guidelines where the management strategy is referral of malnourished infants <6m for inpatient care. Weight-for-length criteria are always the same as for older children, though sometimes this is implied rather than directly stated.
Infants >6m but <3 or 4kgThere is often a ‘secondary criterion’ of a child >6 months but <3 or 4 kg. Some guidelines recommend these should have the same initial treatment as an infant <6m.
Infants <6m and length <65cm Several guidelines implicitly or explicitly equate age <6 months and length <65cm, sometimes using length as a proxy for age. However confusion arises when these measures conflict, e.g. infant is known to be >6 months but length is <65cm. It is not clear which treatment protocol should be applied and if a MUAC measurement is valid if length is <65cms.
Length < 49cmSome guidelines make an allowance for where length <49cm and so W/H cannot be measured. For example, IFE Module 2 recommends “visibly severe thinness” where measurement of W/L is not possible, and mentions that some agencies use a criterion of <2.1kg irrespective of length. WHO-GS go down to 45cm as the minimum length in length-for-height tables. This represents almost -3 z length-for-age at birth: not being able to determine a weight-for-length should therefore be much less of an issue in the future.
Measurement of weight in infants <6mNone of the guidelines draws attention to particular considerations in the anthropometric assessment of infants <6m (see Section 9.3.2). Research has shown weighing scales used in emergencies to be largely unsuitable for weighing infants <6m.134
Assessment of ageSince birth is a recent event in an infant <6m, it is in theory easier to accurately assess age than for older children. None of the guidelines gives details of age assessment of how to best do this e.g. use of calendar to elicit exact age in months.
Infant <6m moderate acute malnutrition (MAM)I dentifying and treating infants <6m with MAM is not specifically dealt with in any of the guidelines except
one (Burkina Faso). Infant MAM is only recognized implicitly, by assuming that the same MAM weight-for-length criteria applicable to older children are applicable to infants. Management therefore requires inference from other sections of the guidelines, e.g. where lactating mothers with infants <6m are admitted to SFP. IFE Module 2 focuses on skilled breastfeeding support for moderately malnourished infants (implicitly including infants <6m).135 Burkina Faso stands out by explicitly stating that infants with MAM should be treated by their mothers receiving SFP rations and health and nutrition education.
Further assessment recommended for infants <6mSome guidelines recommend initial admission to an ‘assessment’ area where breastfeeding can be more closely observed. No current guideline differentiates complicated vs. uncomplicated infant <6m acute malnutrition.
Clinical admission criteria for infants <6mMany guidelines recommend clinical admission criteria, in addition to anthropometry. Common criteria include “an infant who is too weak or feeble to suckle” and “mother not producing enough milk”. Minor variations of emphasis and phrasing (e.g. ‘not enough milk’ with weight loss vs. ‘not enough milk’ alone) make it likely that there are significant inter-programme variations in terms of which infants <6m are admitted to care. It is also not clear whether carer reports or clinician assessments should carry the greaterweight. Inter-user variations in interpreting even the very same guidelines are very likely.
Management of Acute Malnutrition in Infants (MAMI) Project
64
4.4 Guideline Comparisons
Table 7: Infant <6m SAM & MAM case definitions
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
International guidelines:
WHO Management ofseveremalnutrition: amanual forphysicians &other seniorhealth workers 1999
not specificallymentioned.*
n/a n/a n/a n/a n/a Preface states thatprotocol refers to"malnourished childrenunder 5 years of age"
WHO Guidelines forthe inpatienttreatment ofseverelymalnourishedchildren, 2003
not specificallymentioned.
n/a n/a n/a n/a n/a
WHO Manual for thehealth care ofchildren inhumanitarianemergencies2008
not specificallymentioned
n/a n/a n/a n/a n/a ~ noted that patientsneeding inpatient careshould be treatedfollowing "current WHOguidelines"
WHO Pocket book ofHospital care forchildren 2006
yes n/s 1/24 4% no othergroupsnoted
same not specified separate chapter on"supportive care" givesdetails of breastfeedingissues, includingsupplementary suckling
WHO Handbook IMCIIntegratedManagement ofChildhoodIllness 2005
yes yes n/a no othergroupsnoted
n/a n Recommends thatinfants and children withsevere malnutrition arereferred urgently toohospital, and does notcover their specifictreatment
ActionContre laFaim(ClaudinePrudohn)
Assessment &Treatment ofMalnutrition inEmergencySituations, 2002
yes yes 5/58(of sectionontreatment)
9% <4kg same 1) Too weak tosuckle effectively; and/or 2) Mother notproducing enoughmilk
~ notes that infant <6mshould be nursed in aseparate area of the ward~ also suggests pressingon mothers breasts tocheck for presence ofmilk
MSF NutritionGuidelines (1stedition), 1995
yes n/s 1/46 2% no othergroupsnoted
same Not specificallystated
in "Infant feeding"section, infant notdefined to mean infant<6m alone
MSF NutritionGuidelines, 2006
yes n/s 14/191 7% no othergroupsnoted
WHM <70% 1) Weight loss orgrowth stagnation (1 to 2 weeks)2) Too weak tosuckle3) Insufficientbreastmilk4) Inappropriatealternative infantfeeding
whole chapter in thebook devoted to infant<6mrecognised LBW, preterminfantsnotes need formechanical scalesaccurate to 10g

Management of Acute Malnutrition in Infants (MAMI) Project
65
4.4 Guideline Comparisons
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
International guidelines:
MSF ProtocolInfants lessthan 6months old(Benson)MSF – OCBA2007
yes n/s (10/10) (100%) <3kg beingbreast-fed
WHM <70% 1) Infant tooweak or feebleto suckleeffectively(independent ofWHM)
one chapter from a widerset of guidelines notesneed for a 'breastfeedingcorner'notes no growthstandards for infants whoselength <49cm and that thenutrition unit is notappropraite for treatingpremature and LBW infants<49cm. These should bereferred to nursery forappropriate care
ValidInternational
Community-basedTherapeuticCare (CTC), Afield manual(first edition)2006
yes n/s 0.5/13pages oninpatientcare
4% no othergroupsnoted
WHM <70% visible wasting Guideline does not attemptto directly address infant<6m treatment, referringinstead to other guidelines,notably the 2001Operational Guidance onInfant & Young ChildFeeding in Emergencies,volume 1
UNHCR Handbook forEmergencies(third edition)2007
yes notdirectly
infant U6mmentionedin severalparagraphsmixed inmain text
no othergroupsnoted
same "visible severewasting inconjunction withdifficulties in BF"
- notes that infantsU6 SAMtreatment is based onpromotion of BF (ifpossible)- details not described
UNHCR Themanagementof Nutrition inMajorEmergencies2000
infant <6mmalnutritionrecognised, but notsplit into SAM &MAM
1/24 4% no othergroupsnoted
same not specificallystated
States that "formalnourished infants<6m, it is the mother whoshould be included, NOTthe infants (infants shouldbe exclusively breastfed)"
IFE CoreGroup
InfantFeeding inEmergenciesIFE Module 2,version 1.12007
yes yes 17/114pagesfocus juston infantwith SAM(see notes)
(15%) >6monthsold but<65cm~ 4kg
WHM <70% failure to gainweight at homeor undermanagement ata breastfeedingcorner
One chapter (8) focusesexclusively on infant <6msevere malnutrition.Chapter 5 adrresses lowbirth weight infants,”visiblythin”/moderatelymalnourished infants andmalnourished mothers. Thewhole 223 page manualdirectly or indirectlyaddresses this age groupthrough guidance onskilled assessment andsupport for breastfeeding.
ICRC NutritionManual forHumanitarianAction 2008
no(notesTFP oftenrestrictedto<5years)
no n/a n/a n/a n/a n/a no separate section for careof infant <6m. Does however have aparagraph on BF. Notes it asan "absolute priority, andevery effort should bemade to encourage orrestore it"
Table 7 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
66
4.4 Guideline Comparisons
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
National guidelines:
Burundi ProtocoleNational deNutrition2002
yes n/s 5/33 15% <6m or<3kg beingBF
same 1) Mother doesnot have enoughmilk AND infantloosing weight2) Infant tooweak to suckleand loosingweight even ifmother does havemilk
Ethiopia Protocol fortheManagementof SevereAcuteMalnutrition2007
yes n/s 8/81 10% no othergroupsnoted
WHM <70% too weak orfeeble to suckleeffectively(any WH)
Protocol notes no growthstandards for infantswhose length <49cm andthat the nutrition unit isnot appropriate fortreating premature andLBW infants <49cm. Theseshould be referred tonursery and given infantformula.
Madagascar Depistage etprise encharge de lamalnutritionaigue 2007
yes n/s 3/52 6% <3.5kg WHM <70% 1) Too weak orfeeble to suckleeffectively or2) Mother doesnot have enoughmilk and infant isloosing weight
Malawi Guidelinesfor theManagementof SevereAcuteMalnutrition(book T3)2007
yes yes (ingroup'infants<6m withnutritionproblemsbut notSAM')
10/38 26% <3kg WHM <70% 1) Infant notgaining or loosingweight but notSAM or2) Motherreportsinsufficient BM or3) Weak or feebleand not sucklingwell but not SAM
Protocol notes no growthstandards for infantswhose length <49cm andthat the nutrition unit isnot appropriate fortreating premature andLBW infants <49cm -should be referred tonursery for appropriatecare
Mozambique Manual deOrientacaoparaTratamentodaDesnutricaoAguda Grave2008
yes n/s 8/91 9% <3kg WHM <70% 1) Too weak orfeeble to suckleeffectively or2) Not gainingweight at home
Tanzania Managementof AcuteMalnutritionNATIONALGuidelines2008
yes n/s 1/67 1% - same not stated Protocol has only 1paragraph which states "Ifthe mother isbreastfeeding, assist her tobreastfeed or expressbreastmilk. Give theprescribed amount of F75in addition to thebreastmilk"
Table 7 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
67
4.4 Guideline Comparisons
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
National guidelines:
Uganda IntegratedManagementof AcuteMalnutrition2006
yes n/s 1/53 2% 2% same not stated reference made toseparate guidelinesfocused on therapeuticfeeding centres referencealso make to link withIMCI guidelines
Zambia IntegratedManagementof AcuteMalnutrition2009
yes(but seenotes)
n/s 1/35 3% <3kg WHM <70% 1) Infant <6munable tobreastfeed
~ Though infant <6mSAM recognised briefly as"special cases", statedelsewhere that theseguidelines are targeted at6 to 59m children. Thusno separate section orchapter for infant <6m.~ Also referencesseparate "Nationalguidelines" for fulldetails of treatmentduring (inpatient)stabilisation
Zimbabwe Guidelines fortheManagementof Severe AcuteMalnutritionthroughCommunity-basedTherapeuticCare (CTC) 2008
yes(but seenotes)
n/s 1/56 2% n/s n/s not stated ~ reference made toseparate guidelinesfocused on therapeuticfeeding centres~ infants <6m nototherwise focused on inthis guideline in thechapter on "StabilisationCentre" care
DRC GuidelineNational dePrise en Chargede laMalnutritionAigue 2008
yes n/s 5/68 7% <3.5kg <70% WHM 1) Too weak orfeeble to suckleeffectively (anyWH) or2) Mother does nothave enough milkto feed her child or3) Not gaining (orloosing) weight athome
Sudan(Southern)
Guidelines fortheManagementof Severe AcuteMalnutrition2008
yes n/s 7/103 7% <3kg beingbreast-fed
<70% WHM 1) Too weak orfeeble to suckleeffectively (any WH)2) Not gaining (orloosing) weight athome
noted that RUTFinappropriate as "reflexof swallowing is not yetpresent"
Sudan(North)
NationalIntegratedManual on theManagementof Severe AcuteMalnutritionin healthfacilities and atcommunitylevel 2008
yes n/s 7/103 7% <3kgbeingbreast-fed
<70% WHM 1) Too weak orfeeble to suckleeffectively (anyWH)2) Not gainingweight at home
notes that infant <6mshould be ideally benursed in a separate areaof the ward
Table 7 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
68
4.4 Guideline Comparisons
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
National guidelines:
Botswana Guidelinesfor theManagementof SevereAcuteMalnutritionin Children2007
yes n/s 6/28 21% <3kg beingbreast-fed
same 1) Too weak or feebleto suckle effectively(any WH) or2) Mother does nothave enough milk tofeed her child
Protocol notes no growthstandards for infantswhose length <49cmand that the nutritionunit is not appropriate fortreating premature andLBW infants <49cm.These should be referredto nursery and giveninfant formula.
Burkina Faso None yet - indraft
yes yes 5/57 9% <3kg ORlength<65cm (aproxy forage)
same 1) Mother does nothave enough milk andbaby loosing weight2)Infant too weak tosuckle and loosingweight even ifmother has milk
SFP recommended formothers of MAM infants<6m. General health andnutrition education alsorecommended
Cote D'Ivoire ProtocoleNational dePrise encharge de lamalnutritionsevere 2005
yes n/s 10/65 15% <3kg ORlength<65cm (aproxy forage)
<70% WHM (NCHS)(for non-breastfedinfant)
1) Mother does nothave enough milkand baby loosingweight (does notmatter what exactWHM is atassessment)2)Infant too weak tosuckle and loosingweight even ifmother has milk
Protocol notes no growthstandards for infantswhose length <49cmand that the nutritionunit is not appropriate fortreating premature andLBW infants <49cm.These should be referredto nursery and giveninfant formula
Guinea ProtocoleNational dePrise enCharge de laMalnutritionAigue 2008
yes n/s 8/98 8% <3kg <70% WHM (NCHS) 1) Mother does nothave enough milkand baby loosingweight (does notmatter what exactWHM is atassessment)2) Infant too weak tosuckle and loosingweight even ifmother has milk
Mali ProtocoleNational dela prise encharge de lamalnutritionaigue 2007
yes n/s 4/97 4% <3kg <70% WHM (NCHS) 1) Mother does nothave enough milk andbaby loosing weight2) Infant too weak tosuckle and loosingweight even ifmother has milk
noted that RUTFinappropriate as "reflexof swallowing is not yetpresent"
Niger Protocole deprise encharge de lamalnutritionaigue 2008
yes yes(motherreferred to SFP)
7/93 8% <3kg <70% WHM (NCHS) Main criterion is"failure of effectivebreastfeeding":1) Tooweak or feeble tosuckle effectively (nomatter what weight-for-height)2) Notgaining (or loosing)weight at home
notes that infant <6mshould be nursed in aseparate area of the ward
Table 7 cont’d
Management of Acute Malnutrition in Infants (MAMI) Project
69
4.4 Guideline Comparisons
Separateguideline forinfants <6m?
Case Definition (Infants) ~ for admission
Country orOrganization
Guideline Infant <6mSAM
Infant <6mMAM
Pages ofguidelinedevotedto infants / totalpages (excl.annexes)
% ofguidelinedevotedto infants
Who apartfrominfants<6mshouldfollowinfantguidelines
Anthropometriccriteria(except for MUAC,which is not used forinfant <6m, assumesame case definitionsof SAM, MAM unlessotherwise stated)
Clinical criteria Notes
National guidelines:
Senegal Protocole deprise en chargede lamalnutritionaigue 2008
yes n/s 3/45 7% notmentioned
<70% WHM (NCHS) 1) Too weak to suckleand loosing weighteven if mother hasmilk2) Loosing weightwith mother who hasinsufficient milk
Afghanistan Community-basedManagement ofAcuteMalnutritionprogramme inAqcha andMardyan Districtof JawzjanProvinceNorthernAfghanistan2008
yes n/s 5/26 19% <3kg beingbreast-fed
same Main criterion is"failure of effectivebreastfeeding":1) Too weak or feebleto suckle effectively2) Not gaining weightat home
Protocol notes nogrowth standards for infants whoselength <49cm andthat the nutritionunit is notappropriate fortreating prematureand LBW infants<49cm. Theseshould be referred to nursery and given infant formula
Guinea ProtocoleNational de Priseen Charge de laMalnutritionAigue 2008
yes n/s 8/98 8% <3kg <70% WHM (NCHS) 1) Mother does nothave enough milk andbaby loosing weight(does not matterwhat exact WHM is atassessment)2) Infant too weak tosuckle and loosingweight even if motherhas milk
India Indian Academyof Paeditricsguidelines 2006
Notexplicitly.Introdoesmentionchildrenaged 0 to4 years
n/s 0/14 0% n/a n/a n/a No specific detailsof infant <6mtreatment noted inprotocol summary.
Pakistan Protocol for theinpatienttreatment ofseverelymalnourishedchildren in thePakistanearthquakeemergency 2005
notexlplicitly
n/s n/s n/s n/s n/s n/s
Sri Lanka Management ofSevere AcuteUndernutrition:Manual forHealth Workersin Sri Lanka2007
targetgroup forprotocolis 0 to 59months
n/s noseparatesection forinfant<6m
n/s notmentioned
same not specified Outpatient carenoted as only for 6to 59 month oldchildren
Table 7 cont’d
Management of Acute Malnutrition in Infants (MAMI) Project
70
4.4 Guideline Comparisons
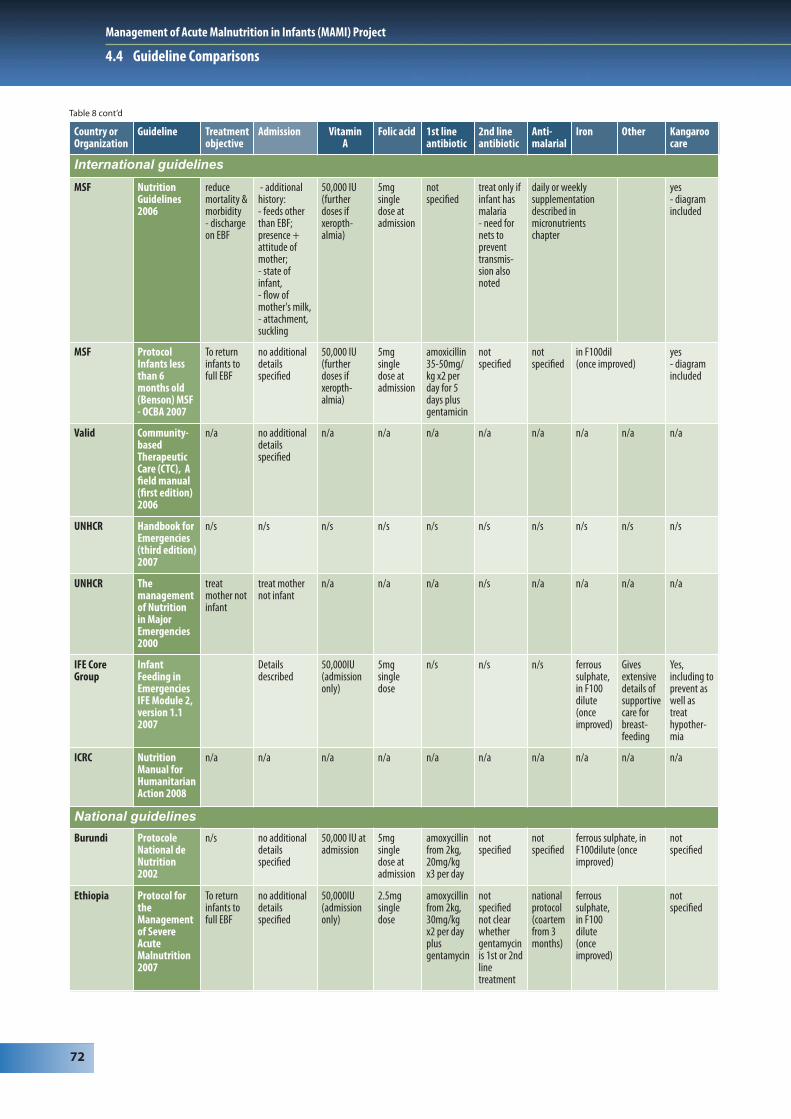
4.4.3 Key medical treatments for infants <6mSee Table 8 for overview.
Admission proceduresAdmission procedures for SAM and MAM include a basic medical history and clinical examination. Some guidelines annex a template ‘history/examination’ proforma, thereby standardizing admission practices. Few guidelines suggest significant extra or different admission procedures for infants <6m. Exceptions and possible models for future guidelines include:
• IFE Module 2 provides the most detail of various aspects of presentation, including recognizing low birth weight infants, infant feeding status (e.g. breastfed or not) and full assessment of breastfeeding (with dedicated sections and a standard checklist).
• MSF 2006 highlights “Additional history, including feedings other than EBF; presence and attitude of the mother, state of the infant, flow of mother’s milk and attachment and suckling.”
• Botswana’s national guidelines note the need to observe breastfeeding “position, attachment, suckling,breast conditions”
• Cote d’Ivoire suggests that suck can be assessed by inserting a finger into the infant’s mouth. Adequacy of current admission procedures will be reviewed in detail in Chapter 9.
Treatment guidelinesAll guidelines recognize a phased approach to care. Many go into significantly more detail on the WHO (1999) ‘ten steps’. There is, however, no specific focus on infants <6m with the exception of IFE Module 2.
Specific treatmentsWhere sections on infant <6m exist in guidelines, they commonly recommend vitamin A, folic acid, iron (usually mixed into the therapeutic milk, but only once the child has improved and is in recovery phase) at appropriate doses. For malaria, local guidelines are referred to. Antibiotics are universally recommended. The most common first line therapy is amoxicillin, with several minor variations in dose/ dose regimen. Second line therapy is often not directly covered in the infant section of the guideline. If noted, initial ampicillin (with switch after two days to oral amoxicillin) plus gentamycin is common.
Kangaroo careii for nursing young / small infants is noted in many guidelines, but often only as a treatment for hypothermia rather than as a default ‘ideal’ position for infants <6m. One exception is IFE Module 2, where Kangaroo care is recommended to “prevent or treat hypothermia” in severely malnourished infants, and also as the default treatment of low birth weight infants, supported by detailed content136.
HIVDetails of HIV-related issues are limited in most guidelines. Those written most recently seem to have greater detail, which probably reflects increased availability of antiretroviral treatments. Where HIV is mentioned, explicit links and references to local HIV-specific guidelines are not made. This is an area for future developers to address, to ensure closer links between services (see Section 9.9 for more HIV considerations).
ii Kangaroo care is a technique where the infant is held in continuous skin-to-skin contact with an adult, usually the mother. It facilitates temperature regulation, reduces infant stress, and helps establish and maintain breastfeeding.

Management of Acute Malnutrition in Infants (MAMI) Project
71
4.4 Guideline Comparisons
Table 8: Key medical treatments recommended for infants <6m
Country orOrganization
Guideline Treatmentobjective
Admission Vitamin A
Folic acid 1st lineantibiotic
2nd lineantibiotic
Anti-malarial
Iron Other Kangaroocare
International guidelines
WHO Managementof severemalnutrition:a manual forphysicians &other seniorhealthworkers1999
n/a Clinicalassessment
50,000IU (onadmission)followedby smalldaily doses
5mg doseatadmission,then dailydose of1mg
cotrimoxazolex2 per dayfor 5 days
ampicillin (50mg/kg/6hrs im for 2 days)then amoxicillin 15mg/kg/8hrs orally for 5daysplus gentamycin7.5mg/kg daily for 7 days
Recommendsfollowingnationalguidelines
all get irononcompletionofstabilisationphase
notspecified
WHO Guidelines forthe inpatienttreatment ofseverelymalnourishedchildren,2003
n/a Clinicalassessment
50,000IU (onadmission)followedby smalldaily doses
50,000IU (onadmission)followedby smalldailydoses
If no complicationscotrimoxazolex2 per dayfor 5 daysif complications amp +gent as above
not specified 3mg/kd/day(onceimproved)
notspecified
WHO Manual forthe healthcare ofchildren inhumanitarianemergencies2008
n/a n/a 50,000IU (onadmission)
notroutinely
amoxicillin notspecified
according tonationalguideline
notroutinely
notspecified
WHO Pocket bookof Hospitalcare forchildren 2005
n/s Clinicalassessment
50,000IU (onadmission)then smalldaily dose
5mg onadmissionthen1mg/day
cotrimoxazolex2 per dayfor 5 days
as above not specified 3mg/kg/day (onceimproved)
alsonotes2mg/kg/day zinc and 0.3mg/kg/day copper
notspecified
WHO HandbookIMCIIntegratedManagementof ChildhoodIllness 2005
n/a n/a n/a n/a n/a n/s n/a n/a n/a n/a
ACF Assessment &Treatment ofMalnutritionin EmergencySituations 2002
Increasemothersmilk supplyuntil BMalonesufficientfor growth
clinicalexaminationmentionedbut nodetailsgiven
50,000IUon days1,2 and atdischarge
5mgsingledose atadmission
amoxicillin20mg/kgx3 per dayfor 10 days
notspecified
according tonationalprotocol
in F100dilute(onceimproved)
noted aspart ofhypo-thermiaprevention
MSF NutritionGuidelines(1st edition)1995
stated thatBF shouldbepromotedandcontinuedduring thewholetreatmentcourse
noadditionaldetailsspecified
notes thatvit Ashould notbe givendue topossibletoxicity
no specificdetailsgiven
no specificdetails given
notspecified
no specificdetails given
no specificdetailsgiven
notspecified
Management of Acute Malnutrition in Infants (MAMI) Project
72
4.4 Guideline Comparisons
Country orOrganization
Guideline Treatmentobjective
Admission Vitamin A
Folic acid 1st lineantibiotic
2nd lineantibiotic
Anti-malarial
Iron Other Kangaroocare
International guidelines
MSF NutritionGuidelines2006
reducemortality &morbidity- dischargeon EBF
- additionalhistory:- feeds otherthan EBF;presence +attitude ofmother; - state ofinfant, - flow ofmother's milk, - attachment,suckling
50,000 IU(furtherdoses ifxeropth-almia)
5mgsingledose atadmission
notspecified
treat only ifinfant hasmalaria- need fornets topreventtransmis-sion alsonoted
daily or weeklysupplementationdescribed inmicronutrientschapter
yes- diagramincluded
MSF ProtocolInfants lessthan 6months old(Benson) MSF- OCBA 2007
To returninfants tofull EBF
no additionaldetailsspecified
50,000 IU(furtherdoses ifxeropth-almia)
5mgsingledose atadmission
amoxicillin35-50mg/kg x2 perday for 5days plusgentamicin
notspecified
notspecified
in F100dil(once improved)
yes- diagramincluded
Valid Community-basedTherapeuticCare (CTC), Afield manual(first edition)2006
n/a no additionaldetailsspecified
n/a n/a n/a n/a n/a n/a n/a n/a
UNHCR Handbook forEmergencies(third edition)2007
n/s n/s n/s n/s n/s n/s n/s n/s n/s n/s
UNHCR Themanagementof Nutritionin MajorEmergencies2000
treatmother notinfant
treat mothernot infant
n/a n/a n/a n/s n/a n/a n/a n/a
IFE CoreGroup
InfantFeeding inEmergenciesIFE Module 2,version 1.12007
Detailsdescribed
50,000IU(admissiononly)
5mgsingledose
n/s n/s n/s ferroussulphate,in F100dilute(onceimproved)
Givesextensivedetails ofsupportivecare forbreast-feeding
Yes,including toprevent aswell astreathypother-mia
ICRC NutritionManual forHumanitarianAction 2008
n/a n/a n/a n/a n/a n/a n/a n/a n/a n/a
National guidelines
Burundi ProtocoleNational deNutrition2002
n/s no additionaldetailsspecified
50,000 IU atadmission
5mgsingledose atadmission
amoxycillinfrom 2kg,20mg/kgx3 per day
notspecified
notspecified
ferrous sulphate, inF100dilute (onceimproved)
notspecified
Ethiopia Protocol fortheManagementof SevereAcuteMalnutrition2007
To returninfants tofull EBF
no additionaldetailsspecified
50,000IU(admissiononly)
2.5mgsingledose
amoxycillinfrom 2kg,30mg/kgx2 per dayplusgentamycin
notspecifiednot clearwhethergentamycinis 1st or 2ndlinetreatment
nationalprotocol(coartemfrom 3months)
ferroussulphate,in F100dilute(onceimproved)
notspecified
Table 8 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
73
4.4 Guideline Comparisons
Country orOrganization
Guideline Treatmentobjective
Admission Vitamin A
Folicacid
1st lineantibiotic
2nd lineantibiotic
Anti-malarial
Iron Other Kangaroocare
National guidelines
Madagascar Depistage etprise encharge de lamalnutritionaigue2007
To ensuremother canproduce milkof sufficientquantity andquality forinfant togrownormally
no additionaldetailsspecified
notspecified
notspecified
notspecified
notspecified
notspecified
notspecified
noted ingeneralsection onhypothermia
Malawi Guidelinesfor theManagementof SevereAcuteMalnutrition(book T3)2007
To stimulateBF untilsufficient toallow theinfant togrowproperly
no additionaldetailsspecified
50,000IU(admissiononly)
5mgsingledose
amoxycillin15mg/kgx3 / day,phase 1 +4 daysextra)
ampicillinivandgentamycinim
notspecified
in F100dil(onceimproved)
noted astreatmentforhypothermiain generalsection
Mozambique Manual deOrientacaoparaTratamentodaDesnutricaoAguda Grave2008
n/s no additionaldetailsspecified
notspecified
5mgsingledose
amoxycillin20mg/kgx3 per dayplusgentamycin
notspecified
notspecified
in F100dil(onceimproved)
HIV-relatedtreatmentsnoted forexposedinfants
noted ingeneralsection onhypothermia
Tanzania Managementof AcuteMalnutritionNATIONALGuidelines2008
n/s not stated 50,000 IUd1 (+d2,d14 ifclinicalsignsdeficiency)
5mgsingledose
amoxycillin15mg/kgx3 per dayfor 5 days
ampicillin plusgentamycin7.5mg/kgdaily for 7days
notspecified
3mg/kg/day elementaliron once improved
noted as atreatmentforhypothermiain generalsection
Uganda IntegratedManagementof AcuteMalnutrition2006
n/s n/a n/a n/a n/a n/a n/a n/a n/a n/a
Zambia IntegratedManagementof AcuteMalnutrition2009
n/s no additionaldetailsspecified
50,000IUatadmission
notspecified
notspecified
notspecified
notspecified
notspecified
notspecified
not specified
Zimbabwe Guidelinesfor theManagementof SevereAcuteMalnutritionthroughCommunity-basedTherapeuticCare (CTC)2008
n/s n/s 50,000IUatadmission
5mg atadmission
amoxycillin from 2kg,20mg/kg x3 per dayfor 7-10 days
not for<4kginfants
notspecified
notspecified
not specified
DRC ProtocolNational dePrise enCharge de laMalnutritionAigue 2008
n/s no additionaldetailsspecified
50,000 IUatadmissiononly(not ifoedema)
notspecified
amoxycillinfrom 2kg,30mg/kgx2 per day
notspecified
notspecified
notspecified
Notes'healtheducationand socialcare' (forallchildren)
not specified
Table 8 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
74
4.4 Guideline Comparisons
Country orOrganization
Guideline Treatmentobjective
Admission Vitamin A
Folic acid 1st lineantibiotic
2nd lineantibiotic
Anti-malarial
Iron Other Kangaroocare
National guidelines
Sudan(Southern)
Guidelinesfor theManagementof SevereAcuteMalnutrition2008
To improve orre-establishBF
no additionaldetailsspecified(thoughdisability,maternalillness,maternaltrauma notedas problemwhich canaffect infantfeeding)
50,000 IUatadmissiononly
2.5mgsingledose atadmission
amoxycillinfrom 2kg,30mg/kgx2 per dayplusgentamycin
notspecified
notspecified
ferrous sulphate, inF100dilute, onceimproved
notspecified
Sudan NationalIntegratedManual ontheManagementof SevereAcuteMalnutritionin healthfacilities andatcommunitylevel 2008
To returninfants to fullEBF
no additionaldetailsspecified
50,000 IUatadmissiononly
2.5mgsingledose atadmission
amoxycillinfrom 2kg,30mg/kgx2 per dayplusgentamycin
notspecified
notspecified
ferrous sulphate, inF100dilute, onceimproved
noted astreatmentforhypother-mia ingeneralsection
Botswana Guidelinesfor theManagementof SevereAcuteMalnutritionin Children2007
~ Treat SAM~ Restore tohealth~ Reducemortality~ Treatcomplications& associateddiseases~ Maintainor improvematernalmilkproduction
~ Observebreastfeeding(position,attachment,suckling,breastconditions)~ medicalconsultation(history,examination)
50,000 IUatadmissiononly
2.5mgsingledoseatadmission
amoxycillinfrom 2kg,20mg/kgx3 per day
notspecified
accordingto nationalguidelines
ferroussulphate6mgelementaliron/kg/day (onceimproved,growing)
Brieflymentions'healtheducationand socialcare' (for allchildren)
noted as atreatmentforhypother-mia ingeneralsection
Burkina Faso None yet - indraft
To increasethe qualityand quantityof BF
no additionaldetailsspecified
50,000 IUatadmissiononly
5mgsingledose atadmission
amoxycillin,from 2kg25mg/kgx3 per day
notspecified
notspecified
ferrous sulphate(once improved)
notspecified
Cote D'Ivoire ProtocoleNational dePrise encharge de lamalnutritionsevere2005
To re-establisheffective EBF(NOTnecessarily toregain 85%WHM)
Note~ Whetherpreterm ~ Birthweight~ Feeds(aside fromBM) ~ Strength ofinfant suck(by insertingfinger intomouth)
notspecified
5mgsingledose atadmission
amoxycillinfrom 2kg,20mg/kgx3 per day
notspecified
notreatmentif testsnegative7 daysartesunateif positive
in F100dil(onceimproved)
Notes thatrisk ofhypother-mia &hypoglycae-mia high ==>infants to benursed closetogetherandmonitoredclosely
notspecified
Guinea ProtocoleNational dePrise enCharge de laMalnutritionAigue 2005
Tosupplementmaternal BFand get tothe pointwhere infantgrowing wellon BF alone
no additionaldetailsspecified
50,000 IUatadmissiononly
2.5mgsingledose atadmission
amoxycillin,from 2kg30mg/kgx2 per day+gentamycin
notspecified
notspecified
in F100dil(onceimproved)
noted as atreatmentforhypother-mia ingeneralsection
Table 8 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
75
4.4 Guideline Comparisons
Country orOrganization
Guideline Treatmentobjective
Admission Vitamin A
Folic acid 1st lineantibiotic
2nd lineantibiotic
Anti-malarial
Iron Other Kangaroocare
National guidelines
Mali ProtocoleNational de laprise encharge de lamalnutritionaigue 2007
n/s noadditionaldetailsspecified
50,000 IUatadmissiononly
2.5mgsingledose atadmission
amoxycillin, from 2kg20mg/kgx3 per day
notspecified
in F100dil(once improved)
noted as atreatment forhypothermiain generalsection
Niger ProtocolNational dePrise enCharge de laMalnutritionAigue 2006
To returninfants tofull EBF
noadditionaldetailsspecified
50,000 IUatadmissiononly
2.5mgsingledose atadmission
amoxycillin,from 2kg30mg/kgx2 per day
notspecified
notspecified
in F100dil(once improved)
not specified
Senegal Protocole deprise encharge de lamalnutritionaigue 2008
To returninfants tofull EBF
noadditionaldetailsspecified
not noted 2.5mgsingledose atadmission
amoxycillinfrom 2kg,20mg/kgx2 per dayfor 7 days
notspecified
notspecified
notspecified
not specified
Afghanistan Community-basedManagementof AcuteMalnutritionprogrammein Aqcha andMardyanDistrict ofJawzjanProvinceNorthernAfghanistan(StabilizationCentreGuidelines)2008
To returninfants tofull EBF
noadditionaldetailsspecified
50,000 IUatadmissiononly
2.5mgsingledoseatadmission
amoxycillinfrom 2kg,30mg/kgx2 per day
addgentamycin(do not usechloram- phenicol)
accordingtonationalguidelines
in F100dil(once improved)
noted insection onhypothermia,withimplicationthat isrecommendedfor all children
India IndianAcademy ofPaeditricsguidelines2006
n/s n/a n/a n/a n/a n/a n/a n/a n/a n/a
Pakistan Protocol forthe inpatienttreatment ofseverelymalnourishedchildren inthe Pakistanearthquakeemergency2005
n/s n/a n/a n/a n/a n/a n/a n/a n/a n/a
Sri Lanka Managementof SevereAcute Under-nutrition:Manual forHealthWorkers in SriLanka2007
n/s noadditionaldetailsspecified
"accordingtonationalprotocol"
notspecified
amoxycillin15mg/kgx3 per dayfor 5 days
gentamycin7.5mg/kgfor 7 daysplusampicillin ivfor 2 daysthen
notspecified
3mg/kg/day onceimproving/gainingweight
noted insection onhypothermiaas prevention/treatment
Table 8 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
76
4.4 Guideline Comparisons
“Careful attention to infant feeding and support for good practice can save lives.Preserving breastfeeding, in particular, is important not just for the duration of anyemergency, but may have lifelong impacts on child health and on women’s futurefeeding decisions.
Every group of people has customs and traditions about feeding infants and youngchildren. It is important to understand these and work with them sensitively whilepromoting best practice.”
Operational Guidance on IFE, v2.1, 2007 &UNHCR Handbook for Emergencies, 3rd Edition
4.4.4 Nutritional treatments for infants <6m
See Table 9 for summary. Most guidelines divide infants into those who have the opportunity to breastfeed and those who do not. These will be dealt with in turn.
Treatment objective‘Restoration of effective exclusive breastfeeding’ (or similar phrasing implying the same) is a commonly stated treatment objective for infants <6m. This differs from the goal for older children, who aim for a nutritional ‘cure’ (commonly >80 or 85% weight-for-height / >-2 or -1 z-scores).
Breastfed infantsMost guidelines encourage the continuation of breastfeeding. However, details of breastfeeding support are rarely described. Exceptions are IFE Module 2 and the WHO pocket handbook of hospital care (2005). For infants <6m who can breastfeed, three hourly breastfeeding of ten to 20 minutes is generally recommended in guidelines. Some encourage more frequent feeds as demanded by the infant. Practical details of how to support and optimize breastfeeding are very limited. This makes prior specialist skills necessary to be able to implement and build on guidelines. Existing materials on breastfeeding support are rarely referenced.
All guidelines imply that infants <6m admitted to treatment would need at least short term supplemental feeds, with the exception of IFE Module 2 that gives the option of breastfeeding/expressed breastmilk alone where an infant is suckling and breastmilk supply is adequate. Diluted F100 was the most frequently recommended supplemental milk. Some guidelines mention F75 for infants with oedema. IFE Module 2 includes commercial infant formula as an option and advises against ‘home prepared’ F75 in thisage-group.
The supplementary suckling (SS) technique as a means of supplemental feeding is widely referenced and thoroughly described in guidelines, including with pictures and diagrams in many137. Using SS, weight gain criteria (20g per day cited by many guidelines) are used to signify that breastmilk production is improving. After a few days with good weight gain, the volume of supplemental milk is reduced. If weight gain continues, supplemental milk is stopped entirely and the infant is monitored to see whether he/she continues to gain weight on exclusive breastfeeding alone.
A minimum admission length is sometimes specified (e.g. nine to 11 days minimum, which includes two to three days each for phase one and two, plus five days for exclusive breastfeeding). Other guidelines urge a short as possible admission, depending on weight gain. All emphasise a need to ensure the infant is gaining adequate weight and is clinically well on exclusive breastfeeding alone, prior to discharge.
Non-breastfed infantsPossible reasons for not breastfeeding are not generally listed, with the exception of IFE Module 2. Thoughrare, none of the guidelines reviewed mention medical contra-indications to breastfeeding 138. The same supplemental milk recommended for breastfed infants is often recommended for this group: dilutedF100 or sometimes F75 for infants with oedema, fed by cup. Only a small number of guidelines explicitly warn of the hygiene risks of bottle/teat feeding.
The major difference for non-breastfed infants <6m arises in the rehabilitation phase of treatment. Here, volume of supplemental milk doubles to enable catch-up growth. Non-breastfed infants may also require transition to an appropriate breastmilk substitute, e.g. transition from diluted F100 to a commercial infant

Management of Acute Malnutrition in Infants (MAMI) Project
77
4.4 Guideline Comparisons
formula. Rather than an ‘adequate weight gain’ discharge criterion, the non-breastfed infant is typically expected to reach the same anthropometric targets as older children prior to discharge (>80% or >85% weight-for-length).
Very few guidelines go into details about the challenges of long term use of infant formula, follow-up needs and resources required, and how to source supplies. Likewise, few note alternatives, such as wet nursing or modified animal milks. No guideline suggests that complementary foods or RUTF be started before six months.
Infant and young child feeding support in older age-groupThe lack of breastfeeding-specific guidance in current guidelines also has implications for older severely malnourished children, where breastmilk should continue to contribute significantly to their energy and nutrient intake. This compromises achievement of the Sphere indicator “as much attention is attached to breastfeeding and psychosocial support, hygiene and community outreach as to clinical care” (Correction of malnutrition standard 2: severe malnutrition).

Management of Acute Malnutrition in Infants (MAMI) Project
78
4.4 Guideline Comparisons
Tab
le 9
: N
utr
itio
nal
tre
atm
ents
fo
r in
fan
ts <
6m
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Divi
sion
into
'bre
ast-
fed'
and
'non
-BF'
Brea
st fe
edin
gBr
east
feed
ing
(det
ails)
Supp
lem
enta
lm
ilks
(BF i
nfan
t)
Supp
lem
enta
l m
ilk ro
ute
(BF i
nf.a
nt)
Supp
lem
enta
l m
ilk fe
edfre
quen
cy(B
F inf
ant)
Supp
lem
enta
l fe
ed
amou
nt(B
F inf
ant)
reha
b ph
ase
(BF i
nfan
t)du
ratio
nof
pha
ses
(BF i
nfan
t)
Disc
harg
e(B
F inf
ant)
No m
ater
nal
brea
stfe
edin
gav
aila
ble
Inte
rnat
ion
al g
uid
elin
es
WHO
Man
agem
ent o
fse
vere
mal
nutr
ition
,19
99
n/a
"sho
uld be
cont
inued
"No
ted i
n sec
tion
on pr
epar
ation
for d
ischa
rge
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
WHO
Guid
elin
es fo
r the
inpa
tient
trea
tmen
t of
seve
rely
mal
nour
ished
child
ren,
2003
n/a
"bre
astfe
ed as
ofte
nas
child
wan
ts"no
ted i
n sec
tion
on pr
epar
ation
for d
ischa
rge
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
WHO
Man
ual f
or th
ehe
alth
care
ofch
ildre
n in
hum
anita
rian
emer
genc
ies 2
008
n/a
not n
oted
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
WHO
Pock
et b
ook o
fHo
spita
l car
e for
child
ren
2005
no"if
child
is br
eastf
ed,
cont
inue w
ith th
is"se
para
tech
apte
r on
supp
ortiv
e car
eha
s det
ails o
nsu
ppor
ting B
F
In or
der o
fpr
efere
nce:
1)BM
alon
e 2)
Infan
tfo
rmula
3)
F100
dilut
e
not s
pecifi
ed(S
S des
cribe
din
differ
ent
chap
ter)
8 tim
es pe
r day
deta
ils no
tsp
ecifi
edde
tails
not s
pecifi
ed
not
spec
ified
not s
pecifi
edex
pres
sed
brea
stmilk
(ifav
ailab
le);
form
ula m
ilk or
infan
t for
mula
;m
odifie
dan
imal
milk
ACF
Asse
ssm
ent &
Trea
t-men
t of
Mal
nutr
ition
inEm
erge
ncy
Situ
atio
ns 20
02
>6m
onth
but <
4kg
infan
ts ar
ese
para
te
Ever
y 3 ho
urs
~ BF
for 1
0-20
mins
~ G
ive BM
S one
hour
afte
r BF
Dilut
ed F1
00su
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg
/day
)
~ if
weigh
tinc
reasin
g for
15 da
ysth
en ha
lf am
ount
F100
dil ~
stop
SSaf
ter f
urth
er 3
days
mini
mum
stay w
ould
be 15
+ 3
+ 5
= 23
days
Once
gaini
ngwe
ight f
or 5
days
with
out
SS
Dilut
ed F1
00*
(pro
toco
l for
>6m
onth
but
<4k
g inf
ants)
MSF
Nutr
ition
Guid
elin
es (1
sted
ition
) 199
5
yes
"shou
ld be
prom
oted
and
cont
inued
durin
g the
whole
of tr
eatm
ent"
BMS A
FTER
each
sessi
on on
the b
reas
t
Reco
nstit
uted
enric
hed
form
ula m
ilk(re
cipie
given
)
small
spoo
n or
syrin
ge5-
6 tim
es pe
rda
y10
5kc
al/kg
/day
no sp
ecifi
c det
ails
not
spec
ified
not s
pecifi
edEn
riche
dfo
rmula
milk
(recip
e give
n)
MSF
Nutr
ition
Guid
elin
es20
06
yes
Ever
y 3 ho
urs
Ever
y 2 ho
urs f
or<
1.5kg
mor
e ofte
nif i
nfan
t wan
ts
~ BF
for 1
0-20
mins
~ G
ive BM
S one
hour
afte
r BF
SDTM
(ther
apeu
ticm
ilk)
supp
lemen
tary
suck
ling
8 tim
es pe
r day
100-
120
kcal/
kg/d
aysta
rt Tra
nsiti
on on
day 1
0 (m
ax d.
15).
Whe
n BM
outp
ut in
creas
es,
weigh
t incre
asing
,de
creas
e STD
M by
50%
. If st
ill ga
ining
weigh
t by 5
g/kg
/day
,sto
p SDT
M
phas
e 110
-15 d
ays
then
acco
rding
to pr
ogre
ss
Once
gaini
ngwe
ight f
or 5
days
with
out
SS
SDTM
(ther
apeu
ticm
ilk)

Management of Acute Malnutrition in Infants (MAMI) Project
79
4.4 Guideline Comparisons
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Divi
sion
into
'bre
ast-
fed'
and
'non
-BF'
Brea
stfe
edin
gBr
east
feed
ing
(det
ails)
Supp
lem
enta
lm
ilks
(BF i
nfan
t)
Supp
lem
enta
l m
ilk ro
ute
(BF i
nf.a
nt)
Supp
lem
enta
l m
ilk fe
edfre
quen
cy(B
F inf
ant)
Supp
lem
enta
l fe
ed am
ount
(BF i
nfan
t)
reha
b ph
ase
(BF i
nfan
t)du
ratio
n of
phas
es(B
F inf
ant)
Disc
harg
e(B
F inf
ant)
No m
ater
nal
brea
stfe
edin
gav
aila
ble
Inte
rnat
ion
al g
uid
elin
es
MSF
Prot
ocol
Infa
nts
less
than
6 m
onth
sol
d (B
enso
n) M
SF -
OCBA
2007
yes
Ever
y 3ho
urs
mor
eof
ten i
finf
ant
want
s
~ BF
for 1
0-20
mins
~ G
ive BM
S 30-
60m
ins af
ter B
F
F100
dil(F
75 if
oede
ma)
supp
lemen
tary
suck
ling
8 tim
es pe
r day
100-
120
kcal/
kg/d
ayde
creas
e to 5
0% of
main
tena
nce o
nce
baby
gaini
ng 20
g/da
ysto
p com
plete
ly on
cega
ining
>10
g/da
y
acco
rding
topr
ogre
ssfew
mor
e day
swi
thou
t SS
- can
also
goon
ce ch
ild BF
gree
dly if
mot
her w
ishes
F100
dilut
e OR F
75fo
r mar
asm
usf7
5 for
kwas
hiorko
r
Valid
Hand
book
for
Emer
genc
ies(t
hird
editi
on) 2
007
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
UNHC
RM
anua
l for
the
heal
th ca
re of
child
ren
inhu
man
itaria
nem
erge
ncie
s 200
8
reco
gnise
dbu
t not
descr
ibed i
nde
tail
yes
"trea
tmen
t sho
uldinc
lude s
uppo
rt fo
rBF
n/s
n/s
n/s
n/s
n/s
n/s
n/s
n/s
UNHC
RTh
e man
agem
ent
of N
utrit
ion
inM
ajor
Emer
genc
ies
2000
non B
Finf
ants
not
reco
gnise
d
discu
ssed
in an
nex
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
IFE C
ore
Grou
pIn
fant
Feed
ing
inEm
erge
ncie
s IFE
Mod
ule 2
, ver
sion
1.1 2
007
yes
yes
Exte
nsive
discu
ssion
of BF
issu
es. B
reas
tfee
ding o
r exp
resse
dbr
eastm
ilk gi
ven a
stre
atm
ent o
ption
.Su
pplem
enta
ryfee
ds m
ay be
indica
ted.
F75 o
rF1
00 di
lute o
rIn
fant f
orm
ula
supp
lemen
tary
suck
ling
at le
ast 8
x /da
yvo
lume p
er kg
varie
sac
cord
ing to
weigh
t(ta
bles g
iven)
if inf
ant g
aining
weigh
t for
2-3d
ays,
atlea
st 20
g/ da
y the
nre
duce
SS by
1/3 a
ndfee
d for
furth
er 2-
3da
ys. C
ontin
ue to
redu
ce vo
lumes
ifinf
ant g
aining
weig
ht.
if gain
ingwe
ight,
each
redu
ction
ofBM
S volu
me
by 1/
3 oc
curs
ever
y2-
3 day
s
Once
gaini
ngwe
ight f
or 5
days
on BF
alone
F75 (
prefe
rred
optio
n)F1
00dil
or fo
rmula
also O
K
ICRC
Nutr
ition
Man
ual
for H
uman
itaria
nAc
tion
2008
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
Nat
ion
al g
uid
elin
es
Buru
ndi
Prot
ocol
e Nat
iona
lde
Nut
ritio
n 20
02ye
sEv
ery 3
hour
s~
BF fo
r 20 m
ins~
Give
BMS o
neho
ur af
ter B
F
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
ofm
ainte
nanc
e onc
eba
by ga
ining
20g/
day
not s
pecifi
edOn
ce ga
ining
weigh
t for
5da
ys w
ithou
t SS
F100
dilut
e OR F
75fo
r mar
asm
usf7
5 for
kwas
hiorko
r
Ethi
opia
Prot
ocol
for t
heM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
2007
yes
Ever
y 3ho
urs
~ BF
for a
t lea
st 20
mins
~ BF
mor
e ofte
n if
infan
t wan
ts~
Give
BMS 3
0 to
60m
in af
ter B
F
F100
dilut
eor
com
mer
cial
form
ula(F
75 fo
r infan
tswi
th oe
dem
a)
supp
lemen
tal
suck
ling
(des
cribe
d)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg
/day
)
decre
ase t
o 50%
ofm
ainte
nanc
e onc
eba
by ga
ining
20g/
day,
stop c
omple
tely
once
gaini
ng>
10g/
day
"as s
hort
aspo
ssible
"On
ce ga
ining
weigh
t on B
Malo
ne
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Table 9 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
80
4.4 Guideline Comparisons
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Divi
sion
into
'bre
ast-
fed'
and
'non
-BF'
Brea
stfe
edin
gBr
east
feed
ing
(det
ails)
Supp
lem
enta
lm
ilks
(BF i
nfan
t)
Supp
lem
enta
l m
ilk ro
ute
(BF i
nf.a
nt)
Supp
lem
enta
l m
ilk fe
edfre
quen
cy(B
F inf
ant)
Supp
lem
enta
l fe
ed am
ount
(BF i
nfan
t)
reha
b ph
ase
(BF i
nfan
t)du
ratio
n of
phas
es(B
F inf
ant)
Disc
harg
e(B
F inf
ant)
No m
ater
nal
brea
stfe
edin
gav
aila
ble
Inte
rnat
ion
al g
uid
elin
es
Mad
agas
car
Depi
stag
e et p
rise
en ch
arge
de l
am
alnu
triti
on ai
gue
2007
Reco
gnise
d but
not d
etail
edEv
ery 3
hour
s~
BF fo
r 20 m
ins~
Give
BMS o
neho
ur af
ter B
F
F100
dilut
esu
pplem
enta
rysu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
ofm
ainte
nanc
e onc
eba
by ga
ining
20g/
day
stop c
omple
tely
once
gaini
ng >
10g/
day
not s
pecifi
edOn
cega
ining
weigh
t for
5da
yswi
thou
t SS
Relac
tatio
n of
othe
r fem
ale ca
rer
(e.g
aunt
)re
com
men
ded)
Mal
awi
Guid
elin
es fo
r the
Man
agem
ent o
fSe
vere
Acu
teM
alnu
triti
on(b
ook T
3) 20
07
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
n if
infan
t wan
ts~
Give
BMS o
neho
ur af
ter B
F
F100
dilut
esu
pplem
enta
rysu
cklin
g(d
escri
bed)
9 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase F
100 d
ilute
by 1/
3 the
main
tena
nce o
nce
baby
gaini
ng20
g/da
y, de
creas
e by
a fur
ther
1/3 i
f stil
lga
ining
weig
ht af
ter
2-3 d
ays,
stop
F100
dilut
e if s
till
gaini
ng w
eight
~ "a
s sho
rtas
possi
ble"
~ 2-
3 day
sfo
r eac
hre
ducti
on of
1/3
F100
dilut
em
ainte
nanc
e
Once
gaini
ngwe
ight f
or 5
days
with
out S
S
F75
Moz
ambi
que
Man
ual d
eOr
ient
acao
par
aTr
atam
ento
da
Desn
utric
ao A
guda
Grav
e 200
8
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
n if
infan
t wan
ts~
Give
supp
lemen
tal fe
edon
e hou
r afte
r BF
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
supp
lemen
tary
suck
ling
(des
cribe
d)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
ofm
ainte
nanc
e onc
eba
by ga
ining
20g/
day
stop c
omple
tely
once
gaini
ng >
10g/
day
not s
pecifi
edOn
cega
ining
weigh
t for
5da
yswi
thou
t SS
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Tanz
ania
Man
agem
ent o
fAc
ute M
alnu
triti
onNA
TION
ALGu
idel
ines
2008
no Relac
tatio
n of
othe
r fem
aleca
rer (
e.g au
nt)
reco
mm
ende
d)
"assi
st to
brea
stfee
dor
expr
ess
brea
stmilk
"
Give
pres
cribe
dam
ount
of F-
75 in
addit
ionto
brea
stmilk
not s
pecifi
ed8 t
imes
per d
ayas
per F
75pr
otoc
olEn
cour
age m
othe
rs to
BF. G
ive ad
dition
aldil
uted
F-10
0. As
BMpr
oduc
tion i
ncre
ases
,gr
adua
lly re
duce
amou
nt di
luted
F100
not s
pecifi
edas
for o
lder
child
ren,
>85
%W
HMor
>-1
WHZ
or M
UAC
>12
5mm
not s
epar
ately
deta
iled
Ugan
daIn
tegr
ated
Man
agem
ent o
fAc
ute M
alnu
triti
on20
06
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
Zam
bia
Inte
grat
edM
anag
emen
t of
Acut
e Mal
nutr
ition
2009
not s
pecifi
edno
tsp
ecifi
edno
t spe
cified
Infan
t for
mula
OR F1
00 di
lute
(F75
dilut
e for
infan
ts wi
thoe
dem
a)
not s
pecifi
ed8 t
imes
per d
ayno
t spe
cified
not s
pecifi
edno
t spe
cified
not
spec
ified
not s
pecifi
ed
Zim
babw
eGu
idel
ines
for t
heM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
thro
ugh
CTC 2
008
not s
pecifi
edno
tsp
ecifi
edno
t spe
cified
not s
pecifi
edno
t spe
cified
not s
pecifi
edno
t spe
cified
not s
pecifi
edno
t spe
cified
not
spec
ified
not s
pecifi
ed
Table 9 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
81
4.4 Guideline Comparisons
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Divi
sion
into
'bre
ast-
fed'
and
'non
-BF'
Brea
stfe
edin
gBr
east
feed
ing
(det
ails)
Supp
lem
enta
lm
ilks
(BF i
nfan
t)
Supp
lem
enta
l m
ilk ro
ute
(BF i
nf.a
nt)
Supp
lem
enta
l m
ilk fe
edfre
quen
cy(B
F inf
ant)
Supp
lem
enta
l fe
ed am
ount
(BF i
nfan
t)
reha
b ph
ase
(BF i
nfan
t)du
ratio
n of
phas
es(B
F inf
ant)
Disc
harg
e(B
F inf
ant)
No m
ater
nal
brea
stfe
edin
gav
aila
ble
Inte
rnat
ion
al g
uid
elin
es
DRC
Prot
ocol
Nat
iona
lde
Pris
e en
Char
gede
la M
alnu
triti
onAi
gue 2
008
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
supp
lemen
tal
feed o
ne ho
uraf
ter B
F
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
supp
lemen
tary
suck
ling
(des
cribe
d)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg
/day
)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
byga
ining
20g/
day.
stop c
omple
tely
once
gaini
ng>
10g/
day
not s
pecifi
edOn
ce ga
ining
weig
ht on
EBF a
lone
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Suda
n(S
outh
ern)
Guid
elin
es fo
r the
Man
agem
ent o
fSe
vere
Acu
teM
alnu
triti
on 20
08
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
supp
lemen
tal
feed o
ne ho
uraf
ter B
F
F100
dilut
esu
pplem
enta
rysu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
byga
ining
20g/
day
stop c
omple
tely
once
gaini
ng>
10g/
day
not s
pecifi
edOn
ce ga
ining
weig
ht on
EBF a
lone
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Suda
n(N
orth
)Na
tiona
lIn
tegr
ated
Man
ual
on th
eM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
in h
ealth
facil
ities
and
at co
mm
unity
leve
l 200
8
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
supp
lemen
tal
feed 3
0-60
mins
afte
r BF
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
supp
lemen
tary
suck
ling
(des
cribe
d)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
byga
ining
20g/
day
stop c
omple
tely
once
gaini
ng>
10g/
day
as sh
ort a
spo
ssible
Once
gaini
ng w
eight
onEB
F alon
eF1
00 di
lute
(F75
for in
fants
with
oede
ma)
Bots
wan
aGu
idel
ines
for t
heM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
inCh
ildre
n 20
07
yes
as of
ten
as possi
ble /
frequ
ently
"Edu
cate
and
dem
onstr
ate
prop
er BF
tech
nique
"
F100
dilut
esu
pplem
enta
rysu
cklin
g8 t
imes
per d
ay14
0ml/k
g/da
y70
ml/k
g/da
y10
-15 d
ays
intial
phas
e2 d
ays r
ehab
phas
eM
inim
um 4
days
final
phas
e
Whe
n gain
ing w
eight
(5 to
10g/
kg/d
ay) o
n EBF
alon
efo
r 5 co
nsec
utive
days
afte
rSS
stop
ped
NB so
me d
iscre
panc
y in
differ
ent s
ectio
ns of
guide
line a
s to l
engt
hs of
stay r
ecom
men
ded
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Burk
ina F
aso
None
yet -
in d
raft
noEv
ery 3
hour
s~
BF fo
r 20 m
ins~
Give
supp
lemen
tal
feed o
ne ho
uraf
ter B
F
dilut
ed F1
00su
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
byga
ining
20g/
day
Not
spec
ified
Once
gaini
ng w
eight
for 5
days
with
out S
Sno
t spe
cified
Cote
D'Iv
oire
Prot
ocol
e Nat
iona
lde
Pris
e en
Char
gede
la M
alnu
triti
onAi
gue 2
005
yes
Ever
y 3ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
BMS 3
0-60
mins
afte
r BF
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
byga
ining
20g/
day
"as s
hort
aspo
ssible
"On
ce ga
ining
weig
ht on
EBF a
lone
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Table 9 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
82
4.4 Guideline ComparisonsCo
untr
y or
Orga
niza
tion
Guid
elin
eDi
visio
nin
to'b
reas
t-fe
d' an
d'n
on-B
F'
Brea
st fe
edin
gBr
east
feed
ing
(det
ails)
Supp
lem
enta
lm
ilks
(BF i
nfan
t)
Supp
lem
enta
l m
ilk ro
ute
(BF i
nf.a
nt)
Supp
lem
enta
l m
ilk fe
edfre
quen
cy(B
F inf
ant)
Supp
lem
enta
l fe
ed am
ount
(BF i
nfan
t)
reha
b ph
ase
(BF i
nfan
t)du
ratio
n of
phas
es(B
F inf
ant)
Disc
harg
e(B
F inf
ant)
No m
ater
nal
brea
stfe
edin
gav
aila
ble
Nat
ion
al g
uid
elin
es
Guin
eaPr
otoc
ole N
atio
nal d
e Pris
een
Char
ge d
e la M
alnu
triti
onAi
gue 2
005
yes
Ever
y 3 ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
BMS 3
0-60
mins
afte
r BF
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg
/day
)
decre
ase t
o 50%
of
main
tena
nce
once
baby
gaini
ng20
g/da
y
"as s
hort
aspo
ssible
"On
cega
ining
weigh
t on
EBF a
lone
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Mal
iPr
otoc
ole N
atio
nal d
e la
prise
en ch
arge
de l
am
alnu
triti
on ai
gue 2
007
yes
Ever
y 3 ho
urs
~ BF
for 2
0 mins
~ G
ive BM
S60
mins
afte
r BF
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of
main
tena
nce
once
baby
gaini
ng20
g/da
y, sto
pco
mple
tely
once
gaini
ng >
10g/
day
not
spec
ified
Once
gaini
ngwe
ight f
or 5
days
with
out S
S
F100
dilut
e
Nige
r Pr
otoc
ol N
atio
nal d
e Pris
een
Char
ge d
e la M
alnu
triti
onAi
gue 2
006
yes
~ no
n-BF
prot
ocol
descr
ibes
findin
g wet
-nu
rse if
possi
ble
Ever
y 3 ho
urs
~ BF
for 2
0 mins
~ BF
mor
e ofte
nif i
nfan
t wan
ts~
Give
supp
lemen
tal
feed 6
0mins
afte
r BF
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of
main
tena
nce
once
baby
gaini
ng20
g/da
y, sto
pco
mple
tely
once
gaini
ng >
10g/
day
not
spec
ified
Once
gaini
ngwe
ight f
or a
few da
yswi
thou
t SS
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Sene
gal
Prot
ocol
e de p
rise e
n ch
arge
de la
mal
nutr
ition
aigu
e200
8
noEv
ery 3
hour
s~
BF fo
r 20
mins
~ G
ivesu
pplem
enta
lfee
d 60m
insaf
ter B
F
F100
dilut
esu
pplem
enta
lsu
cklin
g(d
escri
bed)
8 tim
es pe
r day
130m
l/kg/
day
(=10
0kca
l/kg/
day)
decre
ase t
o 50%
of
main
tena
nce
once
baby
gaini
ng20
g/da
y, sto
pco
mple
tely
once
gaini
ng >
10g/
day
as sh
ort a
spo
ssible
tom
inim
iseris
k of
noso
com
ialinf
ectio
n
Once
gaini
ngwe
ight f
or 5
days
with
out S
S
not d
etail
ed
Afgh
anist
anCo
mm
unity
-bas
edM
anag
emen
t of A
cute
Mal
nutri
tion p
rogr
amm
e in
Aqch
a and
Mar
dyan
Dist
rict
of Ja
wzja
n Pro
vince
Nor
ther
nAf
ghan
istan
(Sta
biliz
atio
nCe
ntre
Gui
delin
es) 2
008
noEv
ery 3
hour
s~
for a
t lea
st20
mins
~ m
ore o
ften i
fch
ild w
ants
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Supp
lemen
tary
suck
ling
8 x pe
r day
(0.5
to 1
hraf
ter B
F)
130m
l/kd/
day
(100
kcal/
kg/
day)
(am
ount
NO
T inc
reas
ed
as in
fant g
ains
weigh
t)
decre
ase t
o 50%
of m
ainte
nanc
eon
ce ba
by ga
ining
20g/
day
if weig
htga
inm
ainta
ined,
then
stop
SS
Whe
nga
ining
weigh
t on
EBF a
lone
(no m
atte
rwh
at we
ight
or W
FL)
F100
dilut
e(F
75 fo
r infan
tswi
th oe
dem
a)
Indi
aIn
dian
Aca
dem
y of
Paed
iatr
ics g
uide
lines
onho
spita
l bas
ed m
anag
emen
tof
Seve
rely
Mal
nour
ished
Child
ren
2006
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
Paki
stan
Prot
ocol
for t
he in
patie
nttr
eat-m
ent o
f sev
erel
ym
alno
urish
ed ch
ildre
n in
the P
akist
an ea
rthq
uake
emer
genc
y 200
5
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
n/a
Sri L
anka
Man
agem
ent o
f Sev
ere
Acut
e Und
ernu
triti
on:
Man
ual f
or H
ealth
Wor
kers
in Sr
i Lan
ka 20
07
nono
ted t
hat "
BFsh
ould
beco
ntinu
ed fo
rall
infan
ts &
youn
g chil
dren
"
no ot
her d
etail
sno
t spe
cified
.By
impli
catio
n,inf
ant U
6 will
be tr
eate
d with
F75
n/a
n/a
n/a
n/a
n/a
n/a
n/a
Table 9 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
83
4.4 Guideline Comparisons
4.4.5 Maternal care, preparation for discharge & follow-upSee Table 10 for overview.
Maternal dietMany guidelines recommend that lactating mothers receive increased food rations to give a total intake of2500kcal/day, and increased fluid intake to >2 litres/day. Vitamin A for the mother is recommended by many guidelines as a single large dose if the infant is <2 months old. Mothers of older infants may be pregnant so either it is withheld or a course of low dose Vitamin A is given. A small number of guidelines mention that general maternal micronutrient stores should be replenished though a high quality diet during breastfeeding.
Psychosocial carePlay therapy and psychosocial support of the malnourished child is one of WHO’s essential ten treatment steps. It is still recognized in many guidelines, often in dedicated sections, but none focus specifically on infants <6m.
The impact of severe infant malnutrition on feeding-associated interactions and feeding cues between a mother and her infant <6m, e.g. reduced demands for breastfeeding, and how to manage these are not generally addressed. IFE Module 2 does include content on this in the section concerned with breastfeeding support in malnourished infants but not specifically in the SAM chapter.
Specific psychosocial care for the mother/carergiver of either infants <6m or children, including assessment and treatment, is not included in the guidelines apart from general statements about ‘being supportive’, explaining treatments and avoiding blame for the infant’s malnutrition. The exception is IFE Module 2 that gives a more practical description of assessment and care for mothers. Given the relevance of psychosocial aspects of care to MAMI, Chapter 8 of this report undertakes a detailed review.
Follow-up care and supplementary feedingFollow-up on discharge from a TFP (inpatient or community-based) is almost universally recommended. SFP referral (if available) on discharge is almost universal and, by implication, this includes infants <6m where the mother benefits from supplementary food rations.
Promoting optimal infant and young child feedingTaking advantage of a captive ‘in-programme’ audience to work towards prevention of future malnutrition has obvious potential. Many guidelines highlight ‘health and nutrition education’ as part of the discharge package, but few are specific on what topics should be covered. Very few guidelines take advantage of thelarge body of IYCF literature available.
Feeding programmes for pregnant & lactating mothersSFP target groups frequently include pregnant women (in last trimester of pregnancy) and lactating women who are malnourished. However it is often not clear in guidelines whether the mothers of malnourished infants <6m should be admitted to SFPs, independent of the nutritional status of themother.

Management of Acute Malnutrition in Infants (MAMI) Project
84
4.4 Guideline Comparisons
Tab
le 1
0: M
ater
nal
car
e, p
rep
arat
ion
fo
r d
isch
arg
e an
d f
ollo
w-u
p
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Mat
erna
l die
tM
ater
nal
(care
give
r) ps
ycho
-so
cial i
ssue
s
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
y IY
CFgu
idan
ceFe
eds
for
preg
nant
&lac
tatin
g wo
men
Inte
rnat
ion
al G
uid
elin
es
WHO
Man
agem
ent o
fse
vere
mal
nutr
ition
: am
anua
l for
phys
ician
s & ot
her
seni
or h
ealth
work
ers 1
999
not s
pecifi
edno
t spe
cified
not
spec
ified
Ensu
re ch
ild fu
lly im
mun
ized
Ensu
re m
othe
r or c
arer
:~
able
to fe
ed ch
ildap
prop
riate
ly~
able
to m
ake a
ppro
priat
eto
ys &
play
with
child
~
know
s how
to gi
ve ho
me
treat
men
t & re
cogn
ise si
gns
to se
ek m
edica
l assi
stanc
e
Yes:
~ ‘sh
ould
not b
e don
ero
utine
ly’; ~
‘HIV
stat
usha
s no r
ole in
man
agem
ent’;
~
‘resu
lt sh
ould
beco
nfide
ntial
, not
reve
aled t
o sta
ff
Yes
1 wee
k, 2 w
eeks
, 1m
onth
, 3m
onth
s & 6
mon
ths a
fter
disch
arge
not n
oted
none
not d
escri
bed
WHO
Guid
elin
es fo
r the
inpa
tient
trea
tmen
t of
seve
rely
mal
nour
ished
child
ren,
2003
not s
pecifi
edno
t spe
cified
Show
pare
nt/ca
rer t
o:~
feed
freq
uent
ly wi
then
ergy
and n
utrie
nt de
nse
food
s~
give
stru
cture
d play
ther
apy
Yes:
"reco
very
may
take
longe
r & tr
eatm
ent
failur
e is m
ore
com
mon
’~
‘trea
tmen
t sam
e as
for H
IV ne
g. ch
ild’
Yes
"regu
lar fo
llow-
up ch
ecks
"ad
vised
not n
oted
None
not d
escri
bed
WHO
M
anua
l for
the
heal
th ca
re of
child
ren
inhu
man
itaria
nem
erge
ncie
s 200
8
not s
pecifi
edm
enta
l hea
lth an
dps
ycho
socia
l sup
port
discu
ssed i
n sep
arat
ech
apte
r
not s
pecifi
edot
her c
hapt
er or
man
ual is
devo
ted t
oHI
V
not s
pecifi
edno
t spe
cified
Note
d, bu
t rea
der
refer
red e
lsewh
ere
for d
etail
s
not d
escri
bed
WHO
Pock
et b
ook o
fHo
spita
l car
e for
child
ren
2005
not s
pecifi
edim
porta
nce o
fps
ycho
logica
l facto
rsno
ted
Show
pare
nt/ca
rer t
o:~
feed
freq
uent
ly wi
then
ergy
and n
utrie
nt de
nse
food
s~
give
stru
cture
d play
ther
apy
Yes
Sepa
rate
chap
ter o
fbo
ok de
tails
HIV
issu
es
yes
1 wee
k, 2 w
eeks
, 1m
onth
, the
nm
onth
ly fo
r6m
onth
s
not n
oted
brea
stfee
ding a
ndyo
ung c
hild f
eedin
gde
scribe
d~
WHO
IYCF
docu
men
t not
refer
ence
d
not d
escri
bed
WHO
Hand
book
IMCI
Inte
grat
edM
anag
emen
t of
Child
hood
Illn
ess
2005
n/a
n/a
n/a
n/a
n/a
n/a
n/a
deta
iled s
ectio
n on
infan
t fee
ding
not d
escri
bed
ACF
Asse
ssm
ent &
Trea
tmen
t of
Mal
nutr
ition
inEm
erge
ncy
Situ
atio
ns 2
002
~ D
rink ≥
2l w
ater
per d
ay~
Eat ~
2600
kcal/
day
~ Su
pplem
ent w
ithvit
amins
& m
inera
ls(e
nsur
e typ
e 1nu
trien
t sto
res
adeq
uate
)
To su
ppor
t BF:
1) Li
sten t
o any
prob
lems
2) As
sess
BF3)
Help
durin
g BF
If gain
ing w
t 15d
ays:
-->ha
lve m
ilk --
>sto
p BM
S aftr
3da
ys --
->ke
ep fo
r 5 m
ore
days
to en
sure
prog
ress
main
taine
d
Yes n
otes
that
:~
field
treat
men
ts ar
ege
nera
lly in
adeq
uate
~ re
-feed
ing tr
eatm
ent
is sa
me
yes,
to~
weig
h inf
ant,
~ pr
ovide
supp
lemen
tary
food
to m
othe
r
week
ly(1
500k
cal/d
ay)
1st m
onth
;fo
rtnigh
t(7
00kc
al/da
y)2n
d mon
th;
mon
thly
(350
kcal/
day)
3-6m
onth
s
ch2.2
: Bre
ast m
ilk,
The p
racti
ce of
BF;
BMS;
Asse
ssing
feedin
g pra
ctice
s
Refer
ral t
o SFP
(but
evide
nce o
feff
ectiv
enes
sdis
cusse
d)

Management of Acute Malnutrition in Infants (MAMI) Project
85
4.4 Guideline ComparisonsCo
untr
y or
Orga
niza
tion
Guid
elin
eM
ater
nal d
iet
Mat
erna
l(ca
regi
ver)
psyc
ho-so
cial
issue
s
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
yIY
CF g
uida
nce
Feed
s fo
rpr
egna
nt &
lact
atin
gwo
men
Inte
rnat
ion
al G
uid
elin
es
MSF
Nutr
ition
Guid
elin
es (1
sted
ition
) 199
5
~ m
entio
ns ne
ed fo
r ext
ra0.5
to 1
litre
fluids
/day
~ el
igible
for S
FP if
one i
sav
ailab
le
Stat
es "s
tress
isim
porta
nt fa
ctor
redu
cing t
hequ
antit
y of b
reas
tm
ilk;
Prot
ocol
note
s:~
need
for
psyc
hoso
cial
stim
ulatio
n
yes
~ no
ted th
at th
isdo
es no
t alte
rth
e trea
tmen
tstr
ategy
not
spec
ified
infan
ts ar
eeli
gbile
for
SFP a
fter T
FPca
re
None
SFP
(in pa
rticu
lar ca
ses
of fo
od in
secu
rity)
MSF
Nutr
ition
Guid
elin
es20
06
~ D
rink ≥
2l w
ater
per d
ay~
Eat 2
500k
cal/d
ayno
tes
psyc
holog
ical
supp
ort a
nden
cour
agem
ent t
om
othe
rs; al
so th
ene
ed fo
r priv
acy
and r
est
~ sti
mula
teem
otion
al an
dph
ysica
lde
velop
men
t~
prep
are pa
tient
for no
tmal
feedin
g prac
tices
1) Se
ction
onHI
V/AI
Ds,
focu
ses o
nnu
tritio
n;2)
Descr
ibed i
ninf
ant f
eedin
g &HI
V sec
tion
part
of in
fant
chap
ter d
escri
bes
supp
ort f
or BF
+alt
erna
tives
to BF
SFP o
r TFP
orsu
ppor
tive f
eedin
g(a
ccord
ing to
situa
tion)
MSF
Pr
otoc
ol In
fant
sle
ss th
an 6
mon
ths o
ld(B
enso
n) M
SF -
OCBA
2007
~ D
rink ≥
2l w
ater
per d
ay;
~ Ea
t 250
0kca
l per
day
~ Su
pplem
ent w
ith vi
tam
ins+
mine
rals
(ens
ure t
ype 1
nutri
ent s
tore
s ade
quat
e)~
Vit A
: 200
,000 I
U (si
ngle
dose
) if in
fant <
2mon
ths;
else 2
5,000
(wee
kly)
~ ne
ed to
enga
gem
othe
r with
treat
men
tpr
ogra
mm
ede
scribe
d~
need
to re
assu
re&
supp
ort
descr
ibed
Need
to nu
rse in
fants
in qu
iet,
sepa
rate
room
note
d no
t spe
cified
inth
is ch
apte
rno
t disc
usse
d in
this
chap
ter
not
spec
ified
inth
isch
apte
r
not s
pecifi
edin
this
chap
ter
not s
pecifi
ed in
this
chap
ter
not d
escri
bed
Valid
Inte
rnat
iona
lCo
mm
unity
-ba
sed
Ther
apeu
tic
Care
(CTC
), A
field
man
ual (
first
editi
on) 2
006
note
s nee
d for
nutri
tiona
lca
re of
mot
hers
(det
ails n
otsp
ecifi
ed)
note
s nee
d for
psyc
holog
ical c
are
of m
othe
rs (d
etail
sno
t spe
cified
)
n/a
yes
secti
on in
"futu
rede
velop
men
ts"ch
apte
rdis
cusse
s HIV
not
spec
ified
SFP i
fav
ailab
leIYC
F not
ed, b
utre
ader
refer
red
elsew
here
for
deta
ils
SFP i
f:~
MUA
C <21
0mm
& pr
egna
nt (3
rdtri
mes
ter)
~ M
UAC <
210m
m&
infan
t <6m
UNHC
RHa
ndbo
ok fo
rEm
erge
ncie
s(th
ird ed
ition
)20
07
n/s
n/s
n/s
yesd
etail
s abo
utHI
V and
nutri
tion
descr
ibed
n/s
SFP f
or al
ldis
char
ged
SAM
patie
nts
Has d
etail
edou
tlinin
g IYC
Fiss
ues,
includ
ingus
e of m
ilk pr
oduc
ts
targ
eted
SFP i
fM
UAC<
22cm
;bla
nket
SFP
othe
rwise
UNHC
RTh
em
anag
emen
t of
Nutr
ition
inM
ajor
Emer
genc
ies
2000
Addit
ional
supp
lemen
tary
ratio
n (no
t spe
cified
)su
gges
ted
Tnot
es th
atm
othe
rs/ca
rers
may
need
help
and
enco
urag
emen
t
Notes
: "W
hen a
mot
her is
seve
rely
maln
oursi
hed o
r suff
ering
from
seve
re inf
ectio
n or o
verw
ork,
she
may
prod
uce i
nade
quate
brea
stmilk
,lea
ding t
o maln
utrit
ion of
infan
t.Br
eastm
ilk pr
oduc
tion m
ay al
so be
affec
ted by
psyc
hoso
cial fa
ctors
n/a
yes
~ di
scusse
d in
deta
il in a
nnex
,inc
luding
issu
esof
BF &
HIV
n/a
SFP i
fav
ailab
leGu
iding
Princ
iples
for f
eedin
g inf
ants
and y
oung
child
ren
durin
g em
erge
ncies
refer
ence
d
SFP
deta
ils de
pend
onth
e situ
ation
IFE C
ore
Grou
pIn
fant
Feed
ing
inEm
erge
ncie
s IFE
Mod
ule 2
,ve
rsio
n 1.
120
07
~ D
rink e
xtra
1l w
ater
per
day
~ Ea
t ~ 25
00kc
al/da
y
Sepa
rate
chap
ter is
on "m
othe
rtra
umat
ised,
inem
otion
al cri
sis or
rejec
ting i
nfan
t"
seve
ral ch
apter
s foc
us on
care
form
othe
rW
hen B
F well
(if
BF)
Mot
her t
raine
dto
give
BMS
corre
ctly (
non-
BFinf
ants)
note
d in o
ther
chap
ters,
but
not i
n sec
tion o
nm
alnou
rishe
dinf
ant
at le
ast
week
ly fo
ra m
inium
umof
3 m
onth
SFP i
fav
ailab
leM
any c
hapt
ers o
fm
anua
l focu
s on
good
IYCF
prac
tices
refer
ence
to ot
her
guide
lines
give
n
Table 10 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
86
4.4 Guideline ComparisonsCo
untr
y or
Orga
niza
tion
Guid
elin
eM
ater
nal d
iet
Mat
erna
l(ca
regi
ver)
psyc
ho-
socia
l iss
ues
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
y IY
CFgu
idan
ceFe
eds
for p
regn
ant
& la
ctat
ing
wom
en
Inte
rnat
ion
al G
uid
elin
es
ICRC
Nutr
ition
Man
ual
for H
uman
itaria
nAc
tion
2008
Secti
on on
psyc
holog
ical
supp
ort f
ocus
es on
child
rath
er th
anca
rer
~ im
mun
izatio
ns up
to da
teye
sCh
apte
r is de
vote
dto
feed
ing in
fants
and s
mall
child
ren
acco
rding
tonu
tritio
nal s
tate
Nat
ion
al G
uid
elin
es
Buru
ndi
Prot
ocol
eNa
tiona
l de
Nutr
ition
2002
~ D
rink ≥
2l w
ater
per d
ay~
Eat ~
2500
kcal/
day
~ Su
pplem
ent w
ith vi
tam
ins &
mine
rals
(ens
ure t
ype 1
nutri
ent s
tore
s ade
quat
e)~
Vit A
: 200
,000 I
U (si
ngle
dose
) if in
fant <
2mon
ths;
25,00
0 (we
ekly
if >2m
onth
s)
~ ne
ed to
enga
gem
othe
r with
treat
men
tpr
ogra
mm
ede
scribe
d~
need
to re
assu
re &
supp
ort m
othe
rde
scribe
d
impo
rtanc
e of
good
war
den
viron
men
tde
scribe
d
~ ha
s had
healt
hed
ucat
ion~
imm
uniza
tions
upto
date
noat
leas
t 3m
onth
sfo
llow-
upat
healt
hce
ntre
leve
l
Has m
essa
ges o
n:EB
F; co
ntinu
ed BF
until
2 ye
ars a
ge;
appr
opria
teco
mple
men
tary
food
s; ke
y chil
dcar
epr
actic
es
SF fo
r:pr
egna
nt w
oman
in3r
d trim
este
r if M
UAC
<21
0mm
; also
wom
en w
ith in
fant
<6m
if M
UAC
<21
0mm
Ethi
opia
Prot
ocol
for t
heM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
2007
~ D
rink ≥
2l w
ater
per d
ay~
Eat ~
2500
kcal/
day
~ Su
pplem
ent w
ith vi
tam
ins &
mine
rals
(ens
ure t
ype 1
nutri
ent s
tore
s ade
quat
e)~
Vit A
: 200
,000 I
U (si
ngle
dose
) if in
fant <
2mon
ths
~ Ex
plain
aim of
treat
men
t/wha
t is
expe
cted;
reas
sure
SS w
orks
; be
atte
ntive
to m
othe
r&
intro
duce
her t
oot
her m
othe
rs
no sp
ecifi
c det
ails
yes.
Deta
ilsinc
lude:
1)Ne
ed fo
rte
sting
; 2)
TB co
-infec
tion
3)AR
V & st
art o
fAR
V
~ m
onth
lyfo
llow-
upun
til ag
ed 6
mon
ths
Mot
her in
SFP ~
mon
thly
until
6mon
ths a
ge
Anne
x 12 g
ives 9
key B
F mes
sage
s; An
nex 1
3 give
s 7ke
y mes
sage
s on
nutri
tion &
grow
th
not d
escri
bed
Mad
agas
car
Depi
stag
e et p
rise
en ch
arge
de l
am
alnu
triti
onai
gue 2
007
not s
pecifi
edno
t spe
cified
~ H
ealth
& nu
tritio
ned
ucat
ionno
spec
ific
infan
tfo
llow-
upno
t not
ed
Refer
ral t
o SFP
reco
mm
ende
dfo
r all
disch
arge
d SAM
patie
nts
briefl
y not
ed in
a lis
tof
healt
h and
nutri
tion e
duca
tion
topic
s
SFP f
or:
~ pr
egna
nt (3
rdtri
mes
ter)
& lac
tatin
gwo
men
with
MUA
C<
210m
m
Mal
awi
Guid
elin
es fo
r the
Man
agem
ent o
fSe
vere
Acu
teM
alnu
triti
on(b
ook T
3)20
07
~ D
rink a
t lea
st 2l
wate
r per
day
~ Ea
t ~ 25
00kc
al/da
y~
If inf
ant <
2 mon
ths,
mot
her
shou
ld ha
ve Vi
t A 20
0,000
IU
need
to re
assu
rem
othe
r not
edIf E
BF no
tpo
ssible
,alt
erna
tives
liste
d inc
lude:
- mod
ified
cow
or go
at m
ilk- i
nfan
t for
mula
~ ne
ed fo
r lov
ing ca
re,pla
y and
stim
ulatio
nno
ted
~ If
EBF n
ot po
ssible
,alt
erna
tives
liste
dinc
lude:
mod
ified
cow
or go
atm
ilk, in
fant f
orm
ula
note
d in l
ist of
caus
es of
failu
reto
resp
ond t
otre
atm
ent
refer
ral fo
rgr
owth
mon
itorin
gno
ted
Refer
ral t
o SFP
reco
mm
ende
dfo
r all
disch
arge
d SAM
patie
nts
none
SFP f
or:
~ pr
egna
nt &
lacta
ting w
omen
, up
to 6
mon
ths a
fter
birth
, with
MUA
C<
210m
m
Moz
ambi
que
Man
ual d
eOr
ient
acao
par
aTr
atam
ento
da
Desn
utric
aoAg
uda G
rave
2008
~ D
rink a
t lea
st 2l
wate
r per
day
~ Ea
t ~ 25
00kc
al/da
y~
If inf
ant <
2 mon
ths,
mot
her
shou
ld ha
ve Vi
t A 20
0,000
IU; if
<2m
onth
s, th
en25
,000IU
/wee
k~
Nee
d to r
eplen
ish ty
pe I
micr
onut
rient
stor
es no
ted
need
to re
assu
rem
othe
r and
expla
intre
atm
ents
note
d
~ H
as de
taile
d cha
pter
on ps
ycho
-socia
lsti
mula
tion &
care
yes
Who
le ch
apte
rde
vote
d to H
IViss
ues
for 3
mon
ths
afte
rdis
char
ge
Refer
ral t
o SFP
reco
mm
ende
dfo
r all
disch
arge
d SAM
patie
nts
has d
etail
ed se
ction
in an
nexe
s out
lining
IYCF i
ssues
SFP r
eferra
l for:
~ pr
egna
nt &
lacta
ting w
omen
with
MUA
C <22
0mm
Table 10 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
87
4.4 Guideline Comparisons
Coun
try o
rOr
gani
zatio
nGu
idel
ine
Mat
erna
l die
tM
ater
nal
(care
give
r)ps
ycho
-socia
liss
ues
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
y IY
CFgu
idan
ceFe
eds
for p
regn
ant &
lact
atin
g wo
men
Nat
ion
al G
uid
elin
es
Tanz
ania
Man
agem
ent
of A
cute
Mal
nutr
ition
NATI
ONAL
Guid
elin
es20
08
not s
pecifi
edno
t spe
cified
not s
pecifi
edPr
otoc
ol de
scribe
s:~
Ensu
reim
mun
izatio
nsdo
ne~
Play
ther
apy &
sens
ory s
timula
tion
men
tione
d in
histo
ry; H
IVscr
eenin
g is
"nec
essa
rylab
orat
ory
inves
tigat
ion"
ever
y 2 m
onth
s for
6 m
onth
s (co
ntinu
e/co
mple
te an
ym
edica
tions
;co
ntinu
e BF i
f ch
ild BF
)
not s
pecifi
edNo
neno
t des
cribe
d
Ugan
daIn
tegr
ated
Man
agem
ent
of A
cute
Mal
nutr
ition
2006
not s
pecifi
edno
t spe
cified
Prot
ocol
focus
es on
RUTF
-relat
edm
essa
ges f
or ol
der
child
ren
yes, W
hole
chap
ter d
evot
edto
HIV
issu
es,
with
sepa
rate
guide
lines
for
HIV+
patie
nts.
(NB f
ocus
ed at
>6m
onth
olds
)
not s
pecifi
edRe
ferra
l to S
FPre
com
men
ded
for a
lldis
char
ged
SAM
patie
nts
Need
to lin
k with
othe
r nat
ional
child
healt
h and
nutri
tion
prog
ram
mes
note
d
SFP r
eferra
l
Zam
bia
Inte
grat
edM
anag
emen
tof
Acu
teM
alnu
triti
on20
09
not s
pecifi
edno
t spe
cified
Prot
ocol
note
s:~ba
sic he
alth
educ
ation
mes
sage
s
yes
not s
pecifi
edRe
ferra
l to S
FPre
com
men
ded
for a
lldis
char
ged
SAM
patie
nts
None
SFP
for:
~ All
preg
nant
(3rd
trim
ester
)& la
ctatin
gwo
men
(with
infan
t<6
m &
child
ren on
PMTC
T com
ing fro
m fo
odins
ecur
e hou
seho
lds~
MUAC
<22
5mm
Zim
babw
eGu
idel
ines
for t
heM
anag
emen
tof
Seve
reAc
ute
Mal
nutr
ition
thro
ugh
CTC
2008
not s
pecifi
edno
t spe
cified
~ H
ealth
&nu
tritio
n edu
catio
n~
Link
s with
instit
ution
s,or
ganiz
ation
s &su
ppor
t gro
ups
(e.g.
socia
l welf
are,
hom
e bas
ed ca
re)
yes
deta
ils gi
ven
n/s
not s
pecifi
edNo
neSP
F for
P&L w
ithM
UAC<
185m
m;
OTP f
or M
UAC <
185m
m
DRC
Prot
ocol
Natio
nal d
ePr
ise en
Char
ge d
e la
Mal
nutr
ition
Aigu
e 200
8
~ Ea
t ~25
00kc
al/da
y~
Vit A
: 200
,000 I
U(si
ngle
dose
) if
infan
t <2m
onth
s
need
to re
assu
rean
d sup
port
mot
her s
tate
d
Prot
ocol
descr
ibes:
~ H
ealth
and
nutri
tion e
duca
tion
~ Pl
ay th
erap
y &ps
ycho
socia
lsu
ppor
t
noSp
ecifi
c inf
ant
follo
w-up
not
deta
iled
Refer
ral t
o SFP
reco
mm
ende
dfo
r all
disch
arge
dSA
M pa
tient
s.
briefl
y not
ed in
a lis
t of
healt
h and
nutri
tion
educ
ation
topic
s, als
ono
tes th
at fee
ding
bottl
es an
d arti
ficial
teats
shou
ld be
bann
ed
SFP f
or:
~ m
othe
rs of
infan
tswi
th M
AM~
lacta
ting w
omen
with
MUA
C <21
0mm
Suda
n(S
outh
ern)
Guid
elin
esfo
r the
Man
agem
ent
of Se
vere
Acut
eM
alnu
triti
on20
08
~ D
rink ≥
2l w
ater
per d
ay~
Eat ~
2500
kcal/
day
~ Su
pplem
ent w
ithm
icron
utrie
nts
~ Vi
t A 20
0,000
IU if
infan
t <2 m
onth
s
para
grap
h on
supp
ortiv
e car
efo
r mot
hers
men
tions
men
tal
and e
mot
ional
supp
ort f
ortra
uma /
depr
essio
n
Prot
ocol
descr
ibes:
~ H
ealth
and
nutri
tion e
duca
tion
~ Pl
ay th
erap
y &ps
ycho
socia
lsu
ppor
t~
Imm
uniza
tions
up-to
-dat
e
yes
deta
ils gi
ven
yes
"At r
egula
r inte
rvals
follo
wing
disch
arg
Refer
ral t
o SFP
reco
mm
ende
dfo
r all
disch
arge
dSA
M pa
tient
s.
IYCF n
oted
, but
read
erre
ferre
d else
wher
e for
deta
ils
not d
escri
bed
Table 10 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
88
4.4 Guideline ComparisonsCo
untr
y or
Orga
niza
tion
Guid
elin
eM
ater
nal d
iet
Mat
erna
l (ca
regi
ver)
psyc
ho-
socia
l iss
ues
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
y IY
CFgu
idan
ceFe
eds
for p
regn
ant &
lact
atin
g wo
men
Nat
ion
al G
uid
elin
es
Suda
n(N
orth
)Na
tiona
lIn
tegr
ated
Man
ual o
n th
eM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
in h
ealth
facil
ities
and
at co
mm
unity
leve
l 200
8
~ D
rink ≥
2l w
ater
per
day
~ Ea
t ~ 25
00kc
al/da
y~
Supp
lemen
t with
micr
onut
rient
s~
Vit A
200,0
00IU
ifinf
ant <
2 mon
ths,
2500
0IU w
eekly
othe
rwise
need
to re
assu
re an
d sup
port
mot
her s
tate
d~
ensu
re ch
ild is
fully
re-in
tegr
ated
in fam
ily &
com
mun
ity~
fully
imm
unize
d~
healt
h and
nutri
tion e
duca
tion
note
d in
list o
fm
ultipl
eca
uses
oftre
atm
ent
failur
e
~af
ter 1
wee
k, 2
week
s, 1 m
onth
, 3m
onth
s and
6mon
ths
Refer
ral t
o SFP
reco
mm
ende
d for
all di
schar
ged
SAM
patie
nts.
(SFP
for m
othe
r inca
se of
infan
t<
6m)
None
not d
escri
bed
Bots
wan
aGu
idel
ines
for t
heM
anag
emen
t of
Seve
re A
cute
Mal
nutr
ition
inCh
ildre
n 20
07
~ D
rink ≥
2l w
ater
per
day
~ Ea
t ~ 25
00kc
al/da
y~
Supp
lemen
t with
vitam
ins &
mine
rals
(ens
ure t
ype 1
nutri
ent
store
s ade
quat
e)
need
to re
assu
re an
d sup
port
mot
her (
e.g. 'b
e atte
ntive
')em
phas
ised
Mot
her s
hould
rece
ive m
edica
ltre
atm
ent i
f nee
ded
~ co
unse
lling a
ndhe
ath ed
ucati
onco
mple
ted~
imm
uniza
tion
up-to
-date
~ arr
ange
men
tsm
ade f
or fo
llow-
up
note
d in
list o
f 6ca
uses
ofpo
orwe
ight
gain
~ w
eekly
for 1
mon
th~
fortn
ightly
next
mon
th~
mon
thly
for n
ext 2
mon
ths
~ as
need
edth
erea
fter
no no
ted
Says
"fee
d fre
quen
tlywi
th en
ergy
and
nutri
ent d
ense
food
s"Fe
eding
bottl
es an
dar
tificia
l tea
ts sh
ould
be ba
nned
not d
escri
bed
Burk
ina
Faso
None
yet -
in d
raft
~ D
rink ≥
2l w
ater
per
day
~ Ea
t ~ 25
00kc
al/da
y~
Supp
lemen
t with
vitam
ins &
mine
rals
(ens
ure t
ype 1
nutri
ent
store
s ade
quat
e)~
Vit A
200,0
00IU
;Iro
n&fo
late
(60m
g+40
0mcg
) for
3m
onth
s afte
r adm
ission
~ ne
ed to
enga
ge m
othe
r with
treat
men
t pro
gram
me d
escri
bed
~ ne
ed to
reas
sure
& su
ppor
tm
othe
r des
cribe
d~
impo
rtanc
e of g
ood
envir
onm
ent d
escri
bed
~ ne
ed to
enga
ge m
othe
r with
treat
men
t pro
gram
me d
escri
bed
~ ne
ed to
reas
sure
& su
ppor
tm
othe
r des
cribe
d~
impo
rtanc
e of g
ood
envir
onm
ent d
escri
bed
Prot
ocol
men
tions
:~
Child
care
prac
tices
~ Pa
rent
ingca
pacit
y~
Play
ther
apy
nofo
llow
up no
ted b
utno
t det
ailed
Refer
ral t
o SFP
reco
mm
ende
d for
all di
schar
ged
SAM
patie
nts.
None
SFP i
f MUA
C <21
0mm
or if
her in
fant <
6mha
s MAM
Cote
D'Iv
oire
Prot
ocol
eNa
tiona
l de P
rise
en ch
arge
de l
am
alnu
triti
onse
vere
2005
~ D
rink a
t lea
st 2l
wate
r per
day
~ Ra
t ~ 25
00kc
al/da
y~
Mot
her s
hould
bead
equa
tely
supp
lemen
ted w
ithvit
amins
& m
inera
ls(ty
pe 1
nutri
ent s
tore
sad
equa
te) -
Vit A
200,0
00IU
2 pag
es of
prot
ocol
devo
ted t
ops
ycho
socia
l car
e & su
ppor
t~
coun
sellin
g and
heat
h edu
catio
nco
mple
ted (
good
child
care
prac
tices
are d
escri
bed i
nde
tail)
~ im
mun
izatio
nup
-to-d
ate
~ ar
rang
emen
tsm
ade f
or fo
llow-
up
yes
follo
w up
for a
t lea
st3 m
onth
s pos
t-dis
char
ge
~ M
othe
r sho
uldha
vesu
pplem
enta
ryfee
ds to
main
tain
quan
tity a
ndqu
ality
of m
ilksu
pply
None
not d
escri
bed
Guin
eaPr
otoc
ole
Natio
nal d
e Pris
een
Char
ge d
e la
Mal
nutr
ition
Aigu
e 200
5
~ Ea
t ~ 25
00kc
al/da
y~
Vit A
: 200
,000 I
U(si
ngle
dose
) if in
fant
<2m
onth
s
need
to re
assu
re an
d sup
port
mot
her s
tate
dPr
otoc
ol de
scribe
s:~
Hea
lth an
dnu
tritio
n edu
catio
n~
Play
ther
apy &
psyc
hoso
cial
supp
ort
noSp
ecifi
c inf
ant f
ollow
-up
not d
etail
edRe
ferra
l to S
FPre
com
men
ded f
orall
disch
arge
dSA
M pa
tient
s.
briefl
y not
ed in
a lis
t of
healt
h and
nutri
tion
educ
ation
topic
s, als
ono
tes th
at fee
ding
bottl
es an
d arti
ficial
teats
shou
ld be
bann
ed
SFP f
or:
~ m
othe
rs of
infan
tswi
th M
AM~
lacta
ting w
omen
with
MUA
C <21
0mm
Table 10 cont’d

Management of Acute Malnutrition in Infants (MAMI) Project
89
4.4 Guideline ComparisonsCo
untr
y or
Orga
niza
tion
Guid
elin
eM
ater
nal d
iet
Mat
erna
l(ca
regi
ver)
psyc
ho-so
cial
issue
s
Othe
rPr
epar
atio
n fo
r disc
harg
e(g
ener
al)
HIV
note
dFo
llow
–up
visit
sEx
tra h
ome
food
ratio
n?De
tails
of an
yIY
CF g
uida
nce
Feed
s fo
rpr
egna
nt &
lact
atin
gwo
men
Nat
ion
al G
uid
elin
es
Mal
iPr
otoc
ole N
atio
nal d
e la p
rise
en ch
arge
de l
a mal
nutr
ition
aigu
e 200
7
~ Dr
ink ≥
2l w
ater p
er da
y~
Eat ~
2500
kcal/
day
~ Su
pplem
ent w
ithvit
amins
& m
ineral
s~
Vit A
200,0
00IU
if inf
ant
<6 w
eeks
has p
arag
raph
on ps
ycho
socia
len
viron
men
t
Prot
ocol
men
tions
:~
play
ther
apy
~ he
alth a
nd nu
tritio
ned
ucat
ion
yes
~ A
chap
ter is
devo
ted t
o HIV
&re
lated
issu
es
as fo
r olde
r chil
dren
:for
3 m
onth
s~
week
ly for
1m
onth
~ for
tnigh
tlyth
ereaft
er
Refer
ral t
o SFP
reco
mm
ende
d for
all di
schar
ged
SAM
patie
nts.
note
d with
in lis
t of
healt
h and
educ
ation
topic
s for
com
mun
ity he
alth
worke
rs to
cove
r
SFP i
f MUA
C<
210m
m
Nige
r Pr
otoc
ol N
atio
nal d
e Pris
e en
Char
ge d
e la M
alnu
triti
onAi
gue 2
006
~ Dr
ink ≥
2l w
ater p
er da
y;~
Eat ~
2500
kcal/
day
~ Su
pplem
ent w
ith vi
tamins
& m
ineral
s (en
sure
type 1
nutri
ent s
tores
adeq
uate)
~ Vit
A 20
0,000
IU if
infan
t<2
mon
ths o
ld; Ir
on &
folat
e(6
0mg+
400m
cg) fo
r 3m
onth
s afte
r adm
ission
~ ne
ed to
enga
ge m
othe
rwi
th tr
eatm
ent
prog
ram
me
descr
ibed
~ ne
ed to
re
assu
re &
su
ppor
t mot
her
descr
ibed
Prot
ocol
men
tions
:~
play t
herap
y~
healt
h and
nutri
tion
educ
ation
yes
~ D
etail
s of H
IV an
dre
lated
issu
esdis
cusse
d
need
for r
egula
rfo
llow-
upem
phas
ised
Refer
ral t
o SFP
reco
mm
ende
d for
all di
schar
ged
SAM
patie
nts.
None
SFP f
orpr
egna
nt an
dlac
tatin
gwo
men
(with
infan
t <6m
) if
MUA
C <21
0mm
Sene
gal
Prot
ocol
e de p
rise e
n ch
arge
de la
mal
nutr
ition
aigu
e20
08
~ D
rink ≥
2l w
ater
per d
ay~
Eat ~
2500
kcal/
day
~ ne
ed to
enga
ge m
othe
rwi
th tr
eatm
ent
prog
ram
me
descr
ibed
Prot
ocol
men
tions
:~ pl
ayth
erapy
~ nu
tritio
nal
advic
e to m
othe
r~en
sure
mot
her c
anrec
ognis
e 'da
nger
signs
'of
clinic
al de
terior
ation
yes
not s
pecifi
edre
ferra
l to S
FP (i
fav
ailab
le)re
com
men
ded f
orall
disch
arge
dSA
M pa
tient
s
None
SFP f
orpr
egna
nt an
dlac
tatin
gwo
men
(with
infan
t <6m
) if
MUA
C <21
0mm
Afgh
anist
anCo
mm
unity
-bas
edM
anag
emen
t of A
cute
Mal
nutr
ition
pro
gram
me i
nAq
cha a
nd M
ardy
an D
istric
tof
Jaw
zjan
Prov
ince
Nor
ther
nAf
ghan
istan
(Sta
biliz
atio
nCe
ntre
Gui
delin
es) 2
008
Mot
her s
hould
bead
equa
tely
supp
lemen
ted
with
vita
mins
& m
inera
ls(ty
pe 1
nutri
ent s
tore
sad
equa
te)
not s
pecifi
edno
t spe
cified
nom
onth
ly un
til ag
ed6 m
onth
sNo
neno
t des
cribe
d
Indi
aIn
dian
Aca
dem
y of P
aedi
trics
guid
elin
es on
hos
pita
l bas
edm
anag
emen
t of S
ever
ely
Mal
nour
ished
Child
ren
2006
not s
pecifi
edno
t spe
cified
Prot
ocol
descr
ibes:
~ H
ealth
and n
utrit
ioned
ucat
ion~
Play
ther
apy &
psyc
hoso
cial s
uppo
rt
noSp
ecifi
c inf
ant
follo
w-up
not
deta
iled
not s
pecifi
edbr
iefly n
oted
in a
list
of he
alth a
ndnu
tritio
n edu
catio
nto
pics,
also n
otes
that
feedin
g bot
tles
and a
rtific
ial te
atssh
ould
be ba
nned
not d
escri
bed
Paki
stan
Prot
ocol
for t
he in
patie
nttr
eatm
ent o
f sev
erel
ym
alno
urish
ed ch
ildre
n in
the
Paki
stan
eart
hqua
keem
erge
ncy 2
005
not s
pecifi
edno
t spe
cified
Prot
ocol
men
tions
:~
com
pletin
gim
mun
izatio
ns~
sens
itizin
g car
ers t
oho
me c
are
~ pl
ay th
erap
y
yes:
~ no
ted th
at "re
cove
rym
ay ta
ke lo
nger
and
treatm
ent f
ailur
e is
mor
e com
mon
~ tre
atmen
t sho
uld be
sam
e as f
or H
IV
yes
~ w
eekly
for 1
mon
th~
fortn
ightly
for 2
mon
ths
~ m
onth
ly fo
r 3m
onth
s
not s
pecifi
edNo
neno
t des
cribe
d
Sri L
anka
Man
agem
ent o
f Sev
ere A
cute
Unde
rnut
ritio
n: M
anua
l for
Heal
th W
orke
rs in
Sri L
anka
2007
not s
pecifi
edno
t spe
cified
anne
x has
secti
on on
play t
hera
pyno
refer
ral fo
r foll
ow-
up no
ted
guide
to fa
mily
food
s for
child
ren
aged
1 to
5 ye
ars
given
in an
nex
None
not d
escri
bed
Table 10 cont’d
Management of Acute Malnutrition in Infants (MAMI) Project
90
4.5 An ‘AGREE’ appraisal of current guidelines
4.5 An ‘AGREE’ appraisal of current guidelinesUsing the ‘AGREE’ appraisal framework (boxed), these are the common issues identified in this review:
a) Scope and purpose of guidelines in addressing infant <6m malnutrition
Guideline objectives to address child malnutrition are generally well stated. Titles alone are often enough to determine whether all types of acute malnutrition or only SAM is the focus.
Guidelines are generally much poorer at explicitly stating the needs of infants <6m. Infant <6m MAM is almost universally neglected (except by Burkina Faso guideline and IFE Module 2). In some guidelines infants <6m are only indirectly addressed, including in the WHO 1999 and 2003 guidelines. Some guidelines usefully state the objective of infant treatment (e.g. “to restore exclusive breastfeeding”). As infant <6m management is different from that of older infants and children it seems sensible that future guidelines deal with it specifically.
b) Stakeholder involvement
1. The overall objective(s) of the guideline should be specifically described.
2. The clinical question(s) covered by the guideline should be specifically described.
3. The patients to whom the guideline is meant to apply should be specifically described.
It is not possible to say which professional groups had inputs into guideline writing without detailedprobing with guideline sources. Many current guidelines have minimal detail of how to clinically assessinfants <6m and focus heavily on supplemental feeds as the core treatment option. This possibly reflectspredominantly nutrition-focused writing groups. Other professionals that may be relevant in the writingof future guidelines on infants <6m include dieticians, paediatricians, obstetricians, nurses, midwives,speech & language therapists, HIV specialists, lactation specialists, psychologists and community healthworkers.
4. The guideline development group should include individuals from all the relevant
professional groups.
IYCF is a family affair and a severely malnourished infant <6m needs involvement of not just the mother orprimary caregiver, but the father, family and community to support treatment. It is clearly difficult forinternational guidelines to include users, however, this should certainly be a feature of national guidelines.Some CMAM guidelines note the importance of ‘community engagement’ as an essential element ofSAM/MAM management. This should be encouraged and made universal. Even basic understanding oflocal context factors influencing malnutrition may make big differences to acceptance and acceptability oftreatments.
5. The patients’ views and preferences should be sought.
Target users are often not clear in guidelines reviewed. Many guidelines, for example, combine details ofclinical management with details of programme management, which can confuse content. Future authorsshould consider and ideally research the pros and cons of a ‘comprehensive’ vs. ‘targeted’ approach. Forexample, small, clinically focused ‘case management’ pocket size handbooks are often liked by front lineclinical staff. Managers, meanwhile, might appreciate a large file with step-by-step instructions abouttroubleshooting programme databases.
6. The target users of the guideline should be clearly defined.
Management of Acute Malnutrition in Infants (MAMI) Project
91
4.5 An ‘AGREE’ appraisal of current guidelines
8. Systematic methods should be used to search for evidence.
9. The criteria for selecting the evidence should be clearly described.
10. The methods used for formulating the recommendations should be clearly described.
11. Health benefits, side effects and risks should be considered.
12. There should be an explicit link between recommendations & supporting evidence.
13. The guideline should be externally reviewed by experts prior to publication.
Guidelines reviewed are ‘end-products’. Separate documents outlining the guideline development processand articulating the underlying evidence base behind individual recommendations were not available. A2004 WHO consultation to ‘Review the literature on Severe Malnutrition’139 is probably reflective of mostcurrent approaches to malnutrition guideline development. Expert consultations and critical reviews areused to identify, interpret and translate available research into policy. Guidelines for the development ofguidelines (e.g. GRADE140 and SIGN141) could be used in future.
In considering “health benefits, side effects and risks”, it is important to consider the implications oftherapeutic treatment of infants <6m amongst the wider infant population. For example, are there risksthat ‘supplemental’ feeding’ of malnourished breastfed infants <6m will carry mixed messages to thecaregiver and community regarding causes of malnutrition and benefits of exclusive breastfeeding? And,if so, how should these risks be managed? None of the guidelines reviewed address these broader issuesof ‘spillover’ and population impact. Locating strategies to treat SAM and MAM in infants <6m within abroader infant and young child feeding framework (see Chapter 2) can help to identify wider risks andinform risk management.
No guideline noted its ‘expiry date’. This probably reflects the short term and uncertain nature of fundingin international nutrition. However, for optimal future impact, regular guideline updates are needed andprocesses for this should be clearly stated.
d) Clarity & presentation
14. A procedure for updating the guideline should be provided.
15. The recommendations should be specific and unambiguous.
16. Different options for diagnosis and/or treatment of the condition should be presented.
17. Key recommendations should be easily identifiable.
There were considerable variations in how easy guidelines were to follow and how much detail theycontained. Varying formats made guideline comparisons difficult, with some recommendations often hardto find. Management of infants <6m was sometimes explicitly stated, (e.g. antibiotic choice), other timesnot, e.g. diagnosis of fluid overload. This issue needs to be addressed in future guidelines by statingexplicitly when and how infants <6m should be treated differently throughout and when treatment is thesame.
There is a clear ‘evolution’ of guidelines, which suggests a process of testing and refining. However, resultsof piloting and testing are not clearly stated in any of the guidelines reviewed. This would be helpful forusers and could be housed in a, probably web-based, repository of guidelines and evaluations for othersto learn from.
c) Rigour of Development
7. The guideline should be piloted among end users.

Management of Acute Malnutrition in Infants (MAMI) Project
92
4.6 Summary findings and recommendations
A key strength of WHO 1999 and its wide acceptance and use is that it was accompanied by a trainingprogramme to aid implementation. Limited information was available as to whether reviewed guidelineswere actively promoted to target audiences and if tools were given to aid rollout.
Chapter 8 of IFE Module 2 is actually a training resource that has become a guidance material, due to thegap in formal guidance. An evaluation of IFE Module 2 amongst users (2006) found that content on SAM<6m was typically used as reference material for programmes more than a training content142.
e) Applicability
19. Potential organisational barriers in applying recommendations should be discussed.20. Potential cost implications of applying the recommendations should be considered.
These were not directly addressed in the majority of guidelines reviewed. This is most probably becauseall guidelines identified were primarily targeted at front-line field staff rather than policy-makers decidingon whether or not they wanted to implement the programme in the first place.
21. The guideline should presents key review criteria for monitoring and audit purposes
18. The guideline should be supported with tools for application.
A few recent guidelines (e.g. Tanzania, Zambia, Zimbabwe) include a ‘checklist’ to help programmemanagers to ensure that all factors relevant to high quality care were being considered. There is someevidence that ‘checklist’ strategies can have a positive impact on patient outcomes143, so this might beuseful for other guidelines to replicate in future. Ideally research should be done to develop an evidence-based checklist for infant <6m malnutrition, as well as for child malnutrition.
f) Editorial Independence
22. The guideline should be editorially independent from the funding body.23. Conflicts of interest of guideline development members should be recorded.
Organizations like WHO and UNICEF often play dual roles as both funders of guideline development andtechnical experts advising on guideline details. UNICEF also contributes funds and resources to inpatientprogrammes in some settings. Any risk of conflicts of interest can be minimized by having independentindividuals on the guideline writing team. This is currently the case for many national guidelines, whichhave a variety of authors involved. It would be good practice for future guidelines to name all contributingindividuals and organizations.
Future guidelines would be improved by aiming towards AGREE standards at the time of writing. This willrequire more person-time resources for writing / guideline development but may have positive impacts interms of individual outcomes.
4.6 Summary findings and recommendationsSummary findingsA total of 37 guidelines (14 international and 23 national) were identified for review. Most share a commonorigin in the WHO 1999 guideline and describe the ’ten steps’ approach to care.
Community-based management of Acute Malnutrition (CMAM) is rapidly being recognised as the ‘norm’ for the management of acute malnutrition for children aged 6 to59m. The Valid International field manual (2006) is a key reference.

Management of Acute Malnutrition in Infants (MAMI) Project
93
4.6 Summary findings and recommendations
MUAC is frequently used in the guidelines as an independent admission criterion, though in no guidelines is it recommended for use in infants <6m.
There is wide variation in how current guidelines address acute malnutrition in infants <6m and some onlyimplicitly recognise the problem.
There is inconsistency in age, weight and length cut-offs used to identify infants <6m for admission and their subsequent treatment.
All guidelines recommend inpatient care for SAM in infants <6m and focus on nutritional treatments with the aim of restoring exclusive breastfeeding. Very few guidelines give details of the MAM in infants <6m.
Few guidelines include details of IYCF/breastfeeding support. MSF guidelines 2006, ACF Assessment and Treatment of Malnutrition, 2002 and IFE Module 2 are important exceptions.
Summary recommendationsFuture guidelines and guideline updates should build on and expand MAMI guidance, both SAM and MAM, and should give more details on IYCF/ breastfeeding support.
The following three guidelines could be considered a good reference/ template for future MAMI guidelines: MSF guidelines 2006, ACF Assessment and Treatment of Malnutrition, 2002 and IFE Module 2
Strategies with potential to improve outcomes of infant <6m SAM include implementation of routine kangaroo care144 for inpatient ‘complicated’ cases of SAM.
MAMI strategies should be located within a framework of safe and appropriate IYCF; synergies in programming between <6m and 6 to 24m age groups must be better reflected in the guidelines.
In the context of international rollout of CMAM programmes, it is noteworthy that MAMI is predominantly inpatient-focused. Options for outpatient based care in infants <6m should be considered in future guidelines.
Greater clarity is needed on anthropometric criteria, measurement cut-offs and age assessment for SAM & MAM infants <6m.
More resources should be devoted to future guideline development. Tools such as GRADE and AGREE should be used to better enhance the quality of future guidelines. An open access online ‘guideline library’might facilitate development of future documents.
130 http://www.gradeworkinggroup.org/131 WHO (1999) Management of severe malnutrition: a manual for physicians and other senior health workers. World Health Organisation.
Geneva: World Health Organisation. 132 Valid International (2006) Community-based Therapeutic Care (CTC). A Field Manual. Oxford: Valid International. 133 WHO & UNICEF (2009) WHO child growth standards and the identification of severe acute malnutrition in infants and children. A joint
statement by the World Health Organization and the United Nations Children's Fund. May 2009.134 Angood, C. (2006) Weighing scales for young infants: a survey of relief workers. Field Exchange. 2006(29):11-2.135 IFE Core Group (2007) Chapter 5. Section 5.3 Babies who are visibly thin or underweight. IFE Module 2. Oxford: Emergency Nutrition
Network. 136 IFE Core Group (2007) Chapter 5. IFE Module 2. Oxford: Emergency Nutrition Network.137 SS involves an initial attempt at normal BF. 30 to 60 minutes later the infant tries suckling again. But the breast this time has a small
nasogastric tube taped near to the nipple. The idea is that the process of suckling helps stimulate progressively increasing breastmilk production. Acknowledging that this takes time - but that infantU6m nutritional needs are urgent - BMS provides maintenance nutrients at 100kcal/kg/day.
138 WHO (2009) Acceptable medical reasons for use of breast-milk substitutes. WHO/NMH/NDH/09.01. Available via http://www.who.int/nutrition/publications/infantfeeding/WHO_NMH_NHD_09.01_eng.pdf
139 WHO. (2004) Severe malnutrition: Report of a consultation to review current literature. Geneva, Switzerland, 06 - 07 September, 2004.140 Jaeschke, R., Guyatt, G.H., Dellinger, P., Schunemann, H., Levy, M.M., Kunz, R., et al. (2008) Use of GRADE grid to reach decisions on
clinical practice guidelines when consensus is elusive. BMJ. 2008;337:a744.141 SIGN. Scottish Intercollegiate Guidelines Network. Available from: http://www.sign.ac.uk/.142 IFE Core Group (2007) Chapter 5. IFE Module 2. Oxford: Emergency Nutrition Network.143 Haynes, A.B., Weiser, T.G., Berry, W.R., Lipsitz, S.R., Breizat, A-H.S., Dellinger, E.P., et al. (2009) A Surgical Safety Checklist to Reduce
Morbidity and Mortality in a Global Population. N Engl J Med. 2009 January 29, 2009;360(5):491-9.144 Kangaroo care consists of skin-to skin contact between mother and infant. Key features are continuous and prolonged skin-to-skin contact
between the mother and baby, accomplished by the baby being firmly attached to the mother chest both day and night, allowing frequentand exclusive breastfeeding (or breastmilk substitute if required).
Endnotes