
CHAPTER 4 PRE TREATMENT PATIENT SPECIFIC...
12
47 CHAPTER 4 PRE TREATMENT PATIENT SPECIFIC QUALITY ASSURANCE OF RAPIDARC PLANS 4.1 INTRODUCTION Advanced treatment techniques use optimized radiation beam intensities to conform dose distribution to the irregular shaped planning target volume (PTV). This is especially useful when the PTV has a concave shape or if organs at risk (OAR) lie very close to the PTV. When IMRT is delivered by means of a multileaf collimator (MLC), its success strongly depends on the behaviour of the leaves, namely their precise positioning and, in the case of dynamic treatments, the accuracy of the leaf speed control. The dose distribution is very sensitive to a number of factors, among which are the leaf end design, the transmission through the leaves and between two adjacent leaves, and the gap between two opposed leaves. Unlike conformal homogeneous beams, intensity-modulated beams may have areas of high dose gradient anywhere in the field and not at the boundaries so that a correct modelling of the beam penumbra by the treatment planning system (TPS) is especially important. Thus, intensity modulated radiation delivery requires strict quality assurance (QA) hardware tests for MLC and specific patient treatment plan validation procedures. The latter generally involve mapping the plan fields onto a phantom that has been computed tomography scanned, creating a so called hybrid plan, and comparing the results with measurements made on that phantom. It is assumed that the validity of the results for the phantom can be extrapolated to the patient.
Transcript of CHAPTER 4 PRE TREATMENT PATIENT SPECIFIC...
47
CHAPTER 4
PRE TREATMENT PATIENT SPECIFIC QUALITY
ASSURANCE OF RAPIDARC PLANS
4.1 INTRODUCTION
Advanced treatment techniques use optimized radiation beam
intensities to conform dose distribution to the irregular shaped planning target
volume (PTV). This is especially useful when the PTV has a concave shape or
if organs at risk (OAR) lie very close to the PTV. When IMRT is delivered by
means of a multileaf collimator (MLC), its success strongly depends on the
behaviour of the leaves, namely their precise positioning and, in the case of
dynamic treatments, the accuracy of the leaf speed control. The dose
distribution is very sensitive to a number of factors, among which are the leaf
end design, the transmission through the leaves and between two adjacent
leaves, and the gap between two opposed leaves. Unlike conformal
homogeneous beams, intensity-modulated beams may have areas of high dose
gradient anywhere in the field and not at the boundaries so that a correct
modelling of the beam penumbra by the treatment planning system (TPS) is
especially important. Thus, intensity modulated radiation delivery requires
strict quality assurance (QA) hardware tests for MLC and specific patient
treatment plan validation procedures. The latter generally involve mapping
the plan fields onto a phantom that has been computed tomography scanned,
creating a so called hybrid plan, and comparing the results with measurements
made on that phantom. It is assumed that the validity of the results for the
phantom can be extrapolated to the patient.
48
Ionization chambers are the preferred dosimeters for measuring
absorbed dose in intensity modulated radiation therapy deliveries. Although
other methods such as one-dimensional or two-dimensional arrays of
detectors, film, and electronic portal imaging devices, among others, have
proved increasingly useful, they are more suited to the measurement of
relative dose distributions. Dose measurements with ionization chambers
(ICs) reflect the average dose value over their volumes. Since the RapidArc
delivery involves complex treatment delivery procedures like variable dose
rate and variable gantry speed, the patient specific quality assurance for
individual patient should be done. In this paper we present our methodology
for RapidArc pre-treatment patient specific QA procedure for hundred
different cases using semiflex ionization chamber.
4.2 MATERIALS AND METHOD
4.2.1 Pre Treatment Rapid Arc Quality Assurance
Hundred different RapidArc plans conforming to the clinical
standards were selected for the pre treatment patient specific quality
assurances study using semiflex ionization chambers (0.125 cm3). A treatment
plan is considered clinically acceptable if the dose within the PTV is uniform
to within predefined limits, typically ± 5%, and the doses to OARs are lower
than those which would cause unacceptable normal tissue complications.
Verification plan was created for each treatment plan with the chamber-
phantom combinations CT scanned (Figure 4.1). All plans were aimed to
deliver 200 cGy at the isocentre. All the verification plans has were done
using the Eclipse planning system version 8.6 using the AAA algorithm. All
measurements have been done using Varian 2100 C/D linear accelerator. The
semiflex ionization chamber was inserted inside the Octavius CT phantom
(Octavius Phantom without compensating cavity) in such a way that the
central axis of radiation beam will be coincided with the centre of the
49
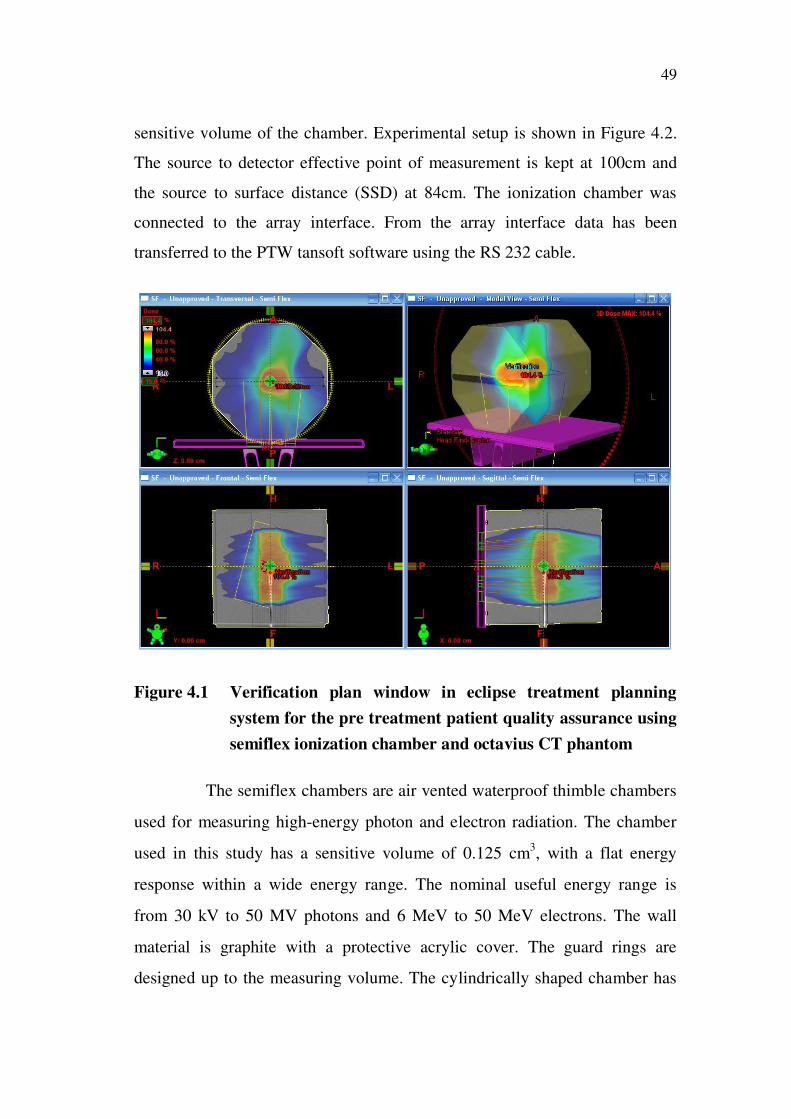
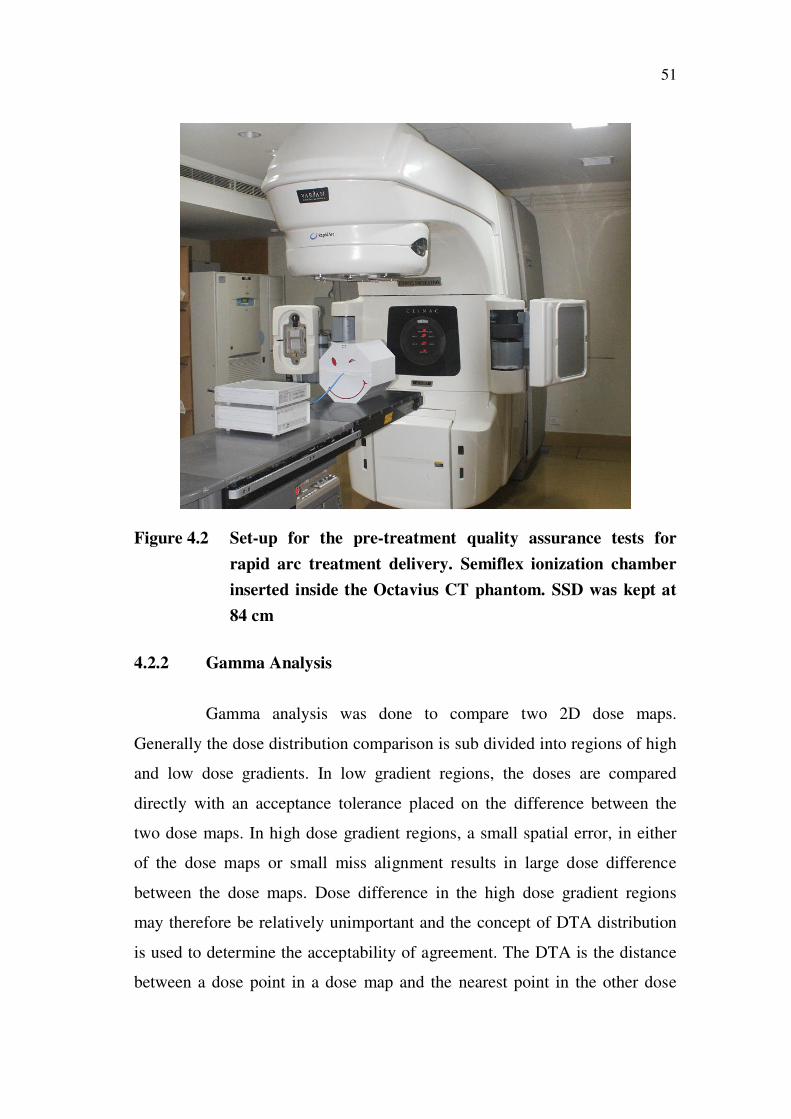
sensitive volume of the chamber. Experimental setup is shown in Figure 4.2.
The source to detector effective point of measurement is kept at 100cm and
the source to surface distance (SSD) at 84cm. The ionization chamber was
connected to the array interface. From the array interface data has been
transferred to the PTW tansoft software using the RS 232 cable.
Figure 4.1 Verification plan window in eclipse treatment planning
system for the pre treatment patient quality assurance using
semiflex ionization chamber and octavius CT phantom
The semiflex chambers are air vented waterproof thimble chambers
used for measuring high-energy photon and electron radiation. The chamber
used in this study has a sensitive volume of 0.125 cm3, with a flat energy
response within a wide energy range. The nominal useful energy range is
from 30 kV to 50 MV photons and 6 MeV to 50 MeV electrons. The wall
material is graphite with a protective acrylic cover. The guard rings are
designed up to the measuring volume. The cylindrically shaped chamber has
50
an inner diameter of 5.5 mm. The 0.125 cm3 chamber is ideal for 3D
dosimetry, since the measuring volume is approximately spherical resulting in
a flat angular response over an angle of ± 160° and a uniform spatial
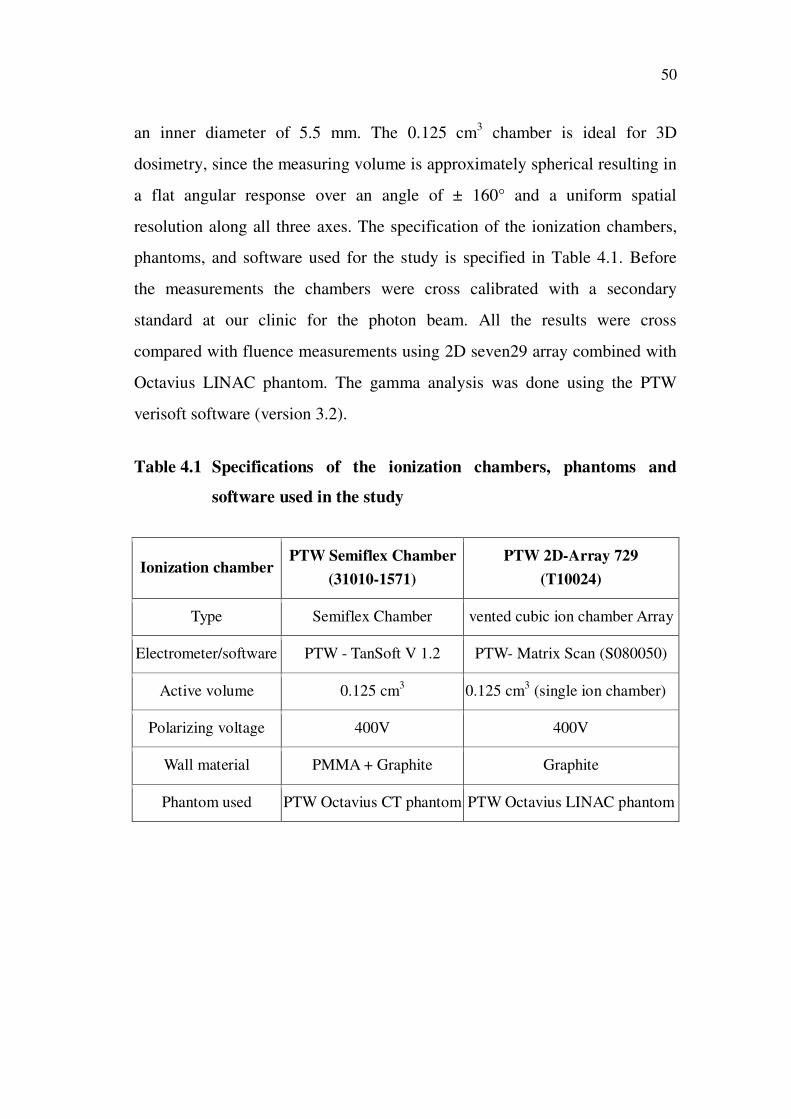
resolution along all three axes. The specification of the ionization chambers,
phantoms, and software used for the study is specified in Table 4.1. Before
the measurements the chambers were cross calibrated with a secondary
standard at our clinic for the photon beam. All the results were cross
compared with fluence measurements using 2D seven29 array combined with
Octavius LINAC phantom. The gamma analysis was done using the PTW
verisoft software (version 3.2).
Table 4.1 Specifications of the ionization chambers, phantoms and
software used in the study
Ionization chamber PTW Semiflex Chamber
(31010-1571)
PTW 2D-Array 729
(T10024)
Type Semiflex Chamber vented cubic ion chamber Array
Electrometer/software PTW - TanSoft V 1.2 PTW- Matrix Scan (S080050)
Active volume 0.125 cm3 0.125 cm
3 (single ion chamber)
Polarizing voltage 400V 400V
Wall material PMMA + Graphite Graphite
Phantom used PTW Octavius CT phantom PTW Octavius LINAC phantom
51
Figure 4.2 Set-up for the pre-treatment quality assurance tests for
rapid arc treatment delivery. Semiflex ionization chamber
inserted inside the Octavius CT phantom. SSD was kept at
84 cm
4.2.2 Gamma Analysis
Gamma analysis was done to compare two 2D dose maps.
Generally the dose distribution comparison is sub divided into regions of high
and low dose gradients. In low gradient regions, the doses are compared
directly with an acceptance tolerance placed on the difference between the
two dose maps. In high dose gradient regions, a small spatial error, in either
of the dose maps or small miss alignment results in large dose difference
between the dose maps. Dose difference in the high dose gradient regions
may therefore be relatively unimportant and the concept of DTA distribution
is used to determine the acceptability of agreement. The DTA is the distance
between a dose point in a dose map and the nearest point in the other dose
52
map that exhibits the same dose. The dose difference and DTA evaluations
complement each other when used as determinants of agreement accuracy
between the dose maps. The simultaneous use of DTA and a percent dose
difference (DD) is proposed by Daniel A Low et al (1998). These parameters
can help evaluate the agreement of the two distributions in terms of
misalignment and difference, respectively. So in this study the various gamma
index constraints which are a combination of particular DTA value with
specific dose difference tolerance value were used.
4.3 RESULTS
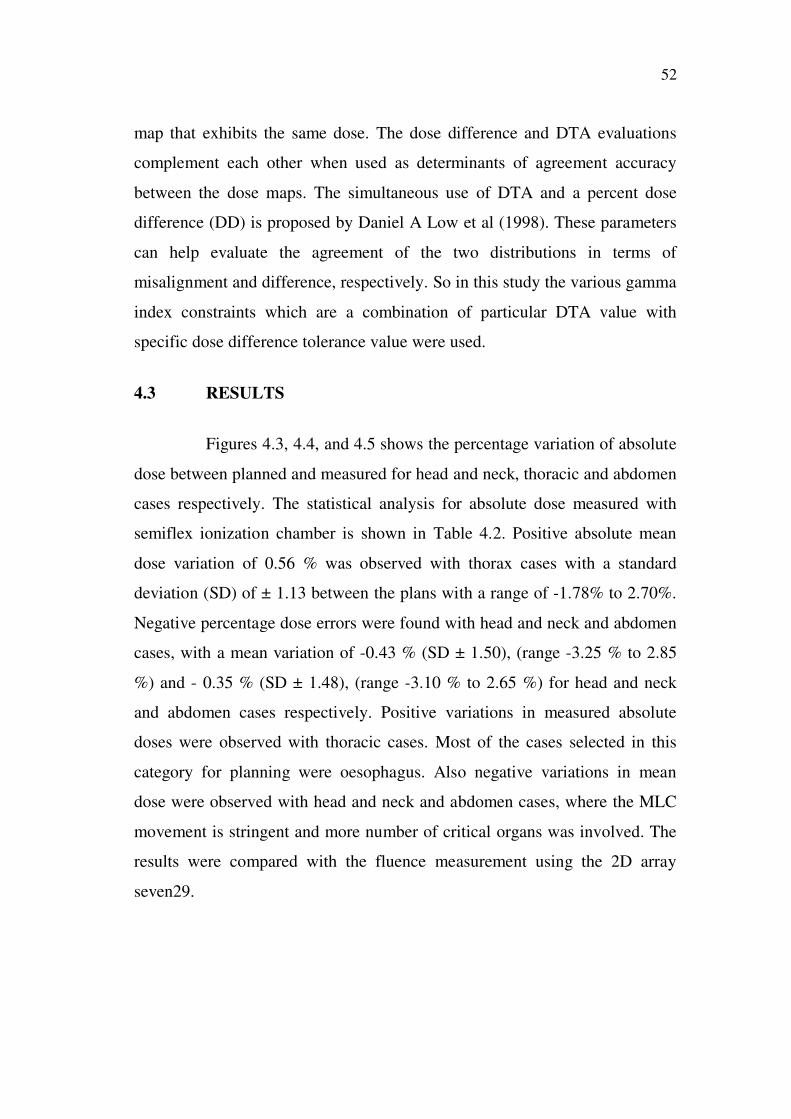
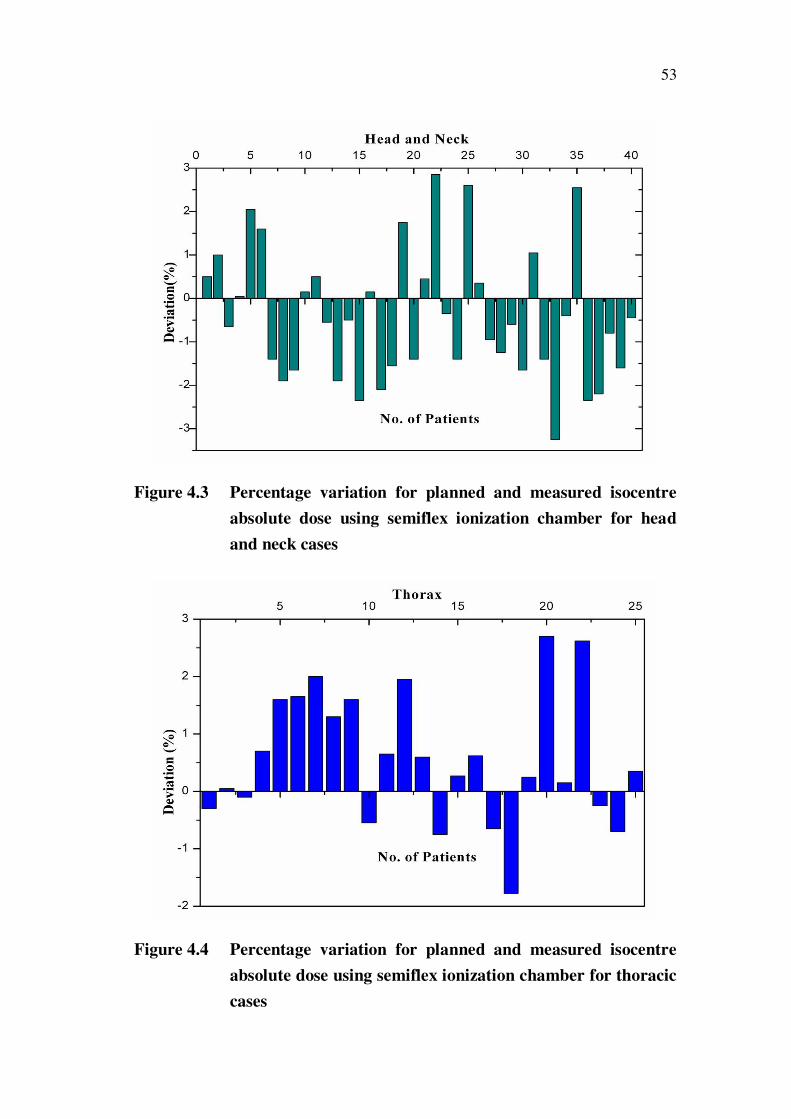
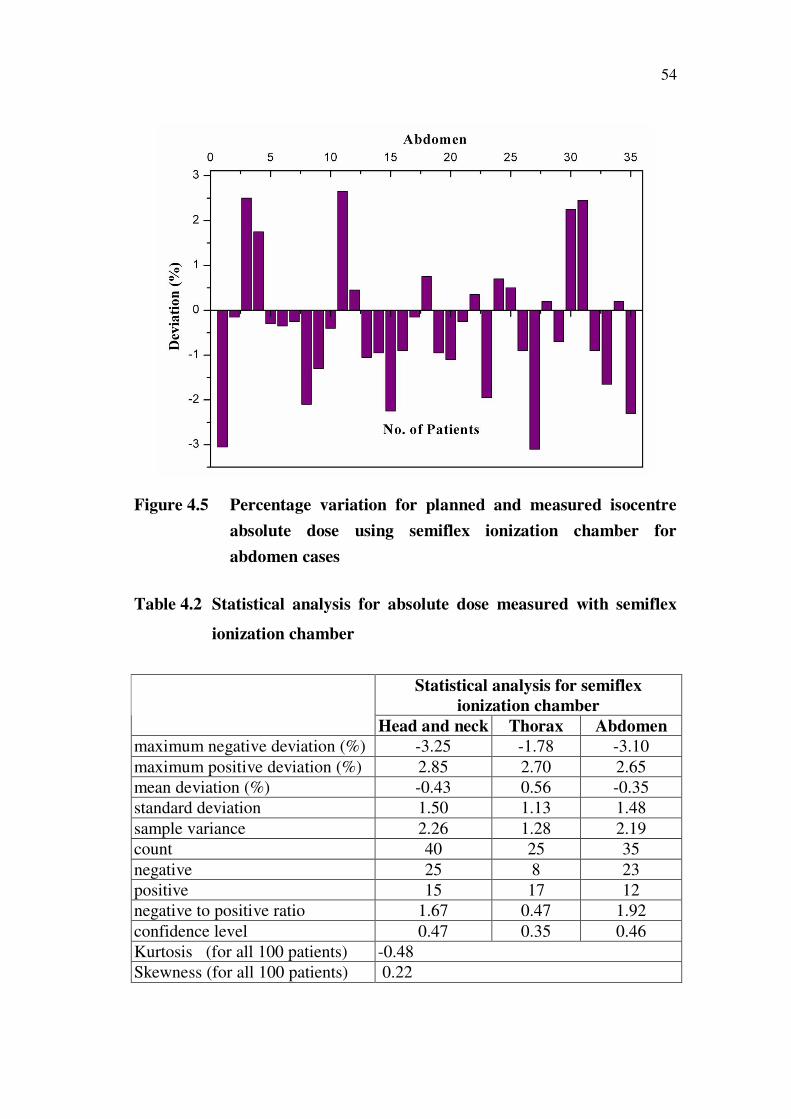
Figures 4.3, 4.4, and 4.5 shows the percentage variation of absolute
dose between planned and measured for head and neck, thoracic and abdomen
cases respectively. The statistical analysis for absolute dose measured with
semiflex ionization chamber is shown in Table 4.2. Positive absolute mean
dose variation of 0.56 % was observed with thorax cases with a standard
deviation (SD) of ± 1.13 between the plans with a range of -1.78% to 2.70%.
Negative percentage dose errors were found with head and neck and abdomen
cases, with a mean variation of -0.43 % (SD ± 1.50), (range -3.25 % to 2.85
%) and - 0.35 % (SD ± 1.48), (range -3.10 % to 2.65 %) for head and neck
and abdomen cases respectively. Positive variations in measured absolute
doses were observed with thoracic cases. Most of the cases selected in this
category for planning were oesophagus. Also negative variations in mean
dose were observed with head and neck and abdomen cases, where the MLC
movement is stringent and more number of critical organs was involved. The
results were compared with the fluence measurement using the 2D array
seven29.
53
Figure 4.3 Percentage variation for planned and measured isocentre
absolute dose using semiflex ionization chamber for head
and neck cases
Figure 4.4 Percentage variation for planned and measured isocentre
absolute dose using semiflex ionization chamber for thoracic
cases
54
Figure 4.5 Percentage variation for planned and measured isocentre
absolute dose using semiflex ionization chamber for
abdomen cases
Table 4.2 Statistical analysis for absolute dose measured with semiflex
ionization chamber
Statistical analysis for semiflex
ionization chamber
Head and neck Thorax Abdomen
maximum negative deviation (%) -3.25 -1.78 -3.10
maximum positive deviation (%) 2.85 2.70 2.65
mean deviation (%) -0.43 0.56 -0.35
standard deviation 1.50 1.13 1.48
sample variance 2.26 1.28 2.19
count 40 25 35
negative 25 8 23
positive 15 17 12
negative to positive ratio 1.67 0.47 1.92
confidence level 0.47 0.35 0.46
Kurtosis (for all 100 patients) -0.48
Skewness (for all 100 patients) 0.22
55
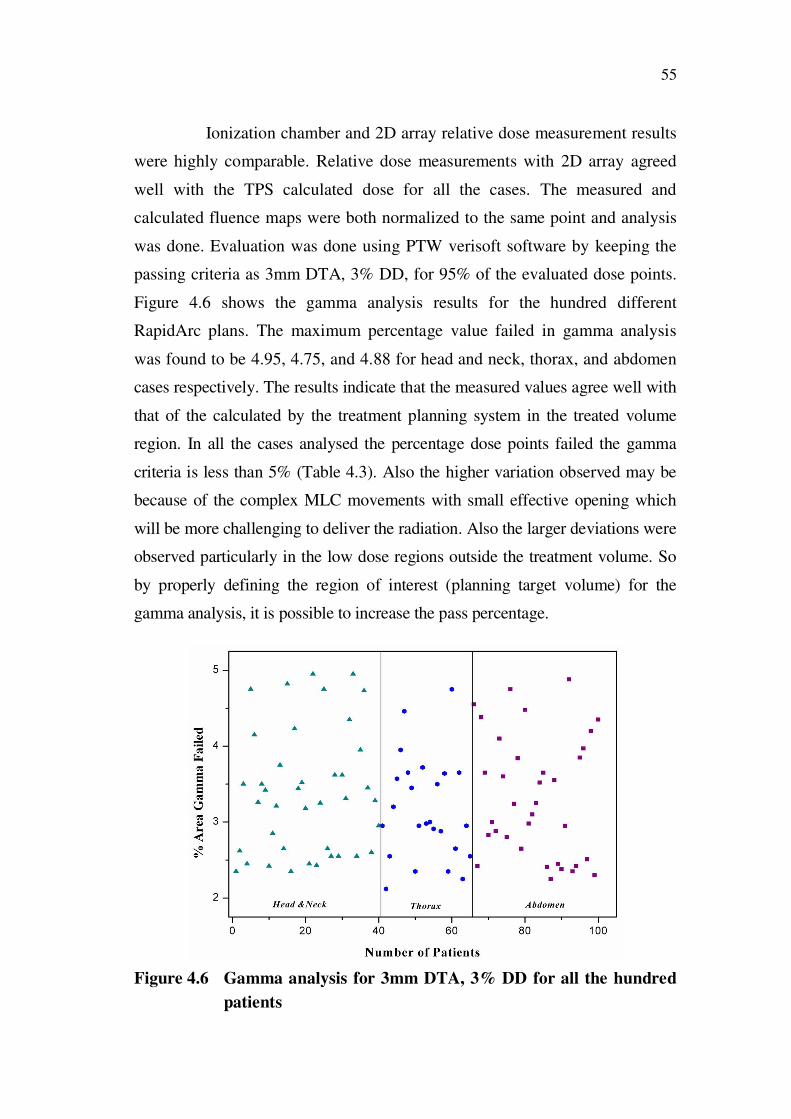
Ionization chamber and 2D array relative dose measurement results
were highly comparable. Relative dose measurements with 2D array agreed
well with the TPS calculated dose for all the cases. The measured and
calculated fluence maps were both normalized to the same point and analysis
was done. Evaluation was done using PTW verisoft software by keeping the
passing criteria as 3mm DTA, 3% DD, for 95% of the evaluated dose points.
Figure 4.6 shows the gamma analysis results for the hundred different
RapidArc plans. The maximum percentage value failed in gamma analysis
was found to be 4.95, 4.75, and 4.88 for head and neck, thorax, and abdomen
cases respectively. The results indicate that the measured values agree well with
that of the calculated by the treatment planning system in the treated volume
region. In all the cases analysed the percentage dose points failed the gamma
criteria is less than 5% (Table 4.3). Also the higher variation observed may be
because of the complex MLC movements with small effective opening which
will be more challenging to deliver the radiation. Also the larger deviations were
observed particularly in the low dose regions outside the treatment volume. So
by properly defining the region of interest (planning target volume) for the
gamma analysis, it is possible to increase the pass percentage.
Figure 4.6 Gamma analysis for 3mm DTA, 3% DD for all the hundred
patients
56
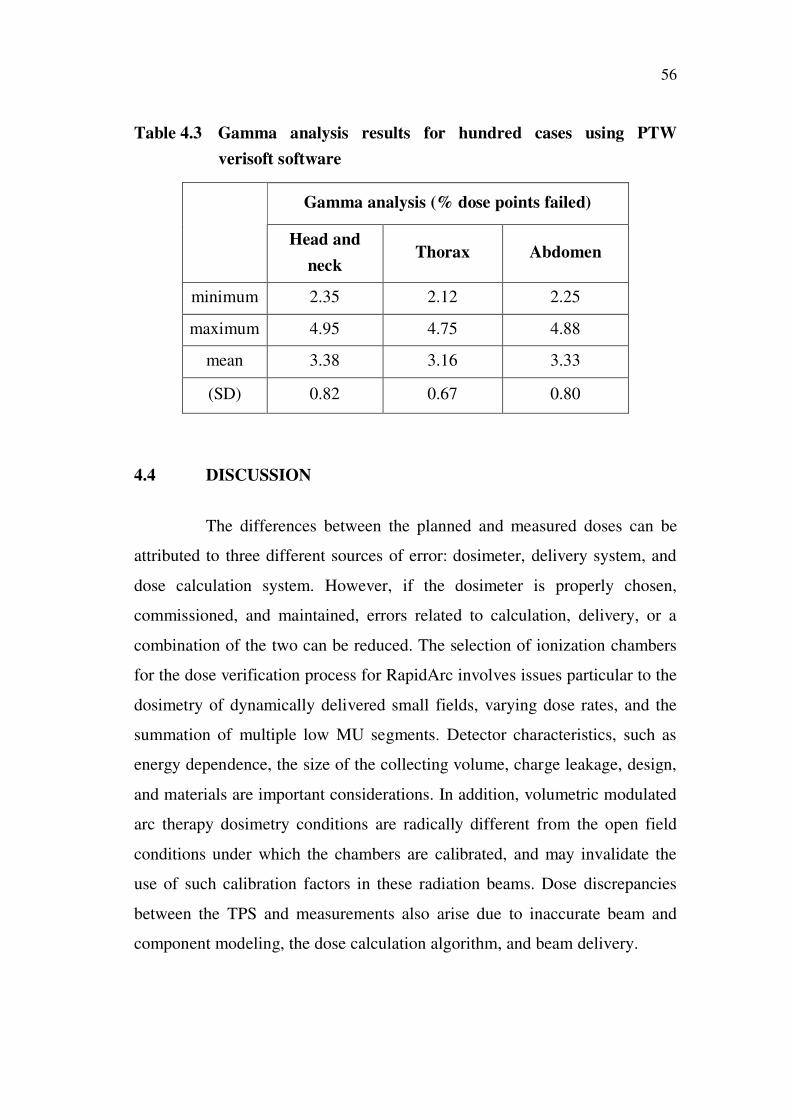
Table 4.3 Gamma analysis results for hundred cases using PTW
verisoft software
Gamma analysis (% dose points failed)
Head and
neck Thorax Abdomen
minimum 2.35 2.12 2.25
maximum 4.95 4.75 4.88
mean 3.38 3.16 3.33
(SD) 0.82 0.67 0.80
4.4 DISCUSSION
The differences between the planned and measured doses can be
attributed to three different sources of error: dosimeter, delivery system, and
dose calculation system. However, if the dosimeter is properly chosen,
commissioned, and maintained, errors related to calculation, delivery, or a
combination of the two can be reduced. The selection of ionization chambers
for the dose verification process for RapidArc involves issues particular to the
dosimetry of dynamically delivered small fields, varying dose rates, and the
summation of multiple low MU segments. Detector characteristics, such as
energy dependence, the size of the collecting volume, charge leakage, design,
and materials are important considerations. In addition, volumetric modulated
arc therapy dosimetry conditions are radically different from the open field
conditions under which the chambers are calibrated, and may invalidate the
use of such calibration factors in these radiation beams. Dose discrepancies
between the TPS and measurements also arise due to inaccurate beam and
component modeling, the dose calculation algorithm, and beam delivery.
57
During RapidArc delivery, the detector is often located either
outside of the field or in penumbra regions, resulting in volume averaging
which is especially important over gradient regions. To overcome this
problem suitable volume chambers are suggested for RapidArc absolute dose
measurements. Semiflex ionization chamber with 0.125 cm3 proved to be
ideal for RapidArc absolute dosimetry. Also in gamma analysis the
percentage of passing points depends on choice of normalization point. The
requirements for dosimetric accuracy in gamma analysis are highest in
regions of low dose gradient and that the requirements for geometric accuracy
are highest in regions of high dose gradient. There are therefore two criteria
for accuracy. Dose points situated in the penumbra region were found to be
responsible for low passing criteria. Study published by Danielle Fraser et al
(2009) suggests that the degree of underestimation was the greatest for the
smallest volume chamber for intensity modulated type of radiation delivery.
Ion chamber based detector arrays are known to have insignificant
energy and dose-rate dependence for megavoltage photon beams, but required
a large sensitive volume, with diameter of the order of 5mm for each
chamber, to gain signal and will therefore exhibit a volume averaging effect
in steep dose gradient regions. Therefore the 2D array was used for fluence
measurement rather than the absolute point dose measurement in the present
study. For point dose measurements, the semiflex ionization chamber was
kept inside the Octavius CT phantom without the compensating cavity.
A trend for measured dose values to be lower than the calculated
ones was observed mainly with head and neck cases. This observation may be
explained by the leaves shielding the ICs from the primary beam during a
fraction of the irradiation. Others potential cause for under response may be
the ionization chamber leakage. Leakage is more marked for small volume
ionization chambers, because chamber sensitivity is proportional to volume.
58
In practice, absolute dose discrepancy between a treatment planning system
and measurement can be clinically accounted by applying TPS correction
factor that adjusts the analytical algorithm to better match systematically
different intensity modulated measurements. Alternatively, treatment plan
specific correction factors can be applied to ionization chamber to account for
fluence perturbation effects in RapidArc delivery. In this study the average
discrepancy between TPS calculated and measured remains within ICRU
Report 24 recommendations for clinical accuracy of ± 5%. Also it is important
to normalize the dose distribution in the high dose region and exclude the area
receiving a dose less than a certain minimum dose for the RapidArc QA
analysis.
4.5 CONCLUSION
On the basis of the studies performed, it can be concluded that the
semiflex ionization chamber having a volume of 0.125cm3 can be used
efficiently for performing the pre-treatment quality assurance of RapidArc
plans for all the sites. The results provide an overall accuracy when compared
to fluence measurement done using 2D array seven29.


















