Chapter 39: OB US
73
Non-Interpretive Skills Introduction to Pelvic and Obstetric Ultrasound
Transcript of Chapter 39: OB US

Non-Interpretive SkillsIntroduction to Pelvic and Obstetric Ultrasound

Before You Begin
This module is intended primarily for clinical medical students or interns intending to learn or review non-interpretive radiology skills.
Please note that while not integral, this module series assumes some familiarity with basic imaging techniques and interpretive skills. If you wish to learn or review these concepts, please see our “Interpretive Skills” module series.
If material is repeated from another module, it will be outlined as this text is so that you are aware

Objectives
• Explain the advantages of transvaginal ultrasonography compared to a transabdominal pelvic ultrasound
• Construct the appropriate imaging algorithm for: female pelvic pain, vaginal bleeding, suspected ectopic pregnancy
• Estimate the accuracy of ultrasound for pregnancy dating
• Schedule fetal ultrasounds at the appropriate diagnostic intervals
• Describe the limitations of ultrasound for prenatal diagnosis

Outline
• Imaging indications
• Techniques for pelvic imaging
• Pelvic ultrasound
• Premenopausal
• Postmenopausal
• Obstetrical ultrasound• First trimester sonogram • Second trimester sonogram
• Review

1. Ultrasound
2. MRI
3. CT
4. X-ray
Teaching point:US is the first line modality for pelvic imaging
Types of Pelvic Imaging

3 Main Category of Patients
1. Premenopausal2. Postmenopausal3. Pregnant

Indications for Pelvic Ultrasound(2014 AIUM Guidelines)
AIUM: American Institute of Ultrasound in Medicine
• Pelvic Pain• Pelvic Masses• Endocrine abnormalities, including PCOS• Dysmenorrhea (painful menses) or menorrhagia• Amenorrhea• Delayed menses• Evaluation of infertility patients• Limited physical exam• Pelvic Infection• Pelvic abnormality on different imaging modality• Follow-up previous finding• Congenital uterine and lower genital tract abnormalities• IUD location• Screening high-risk patients • Pre or postoperative evaluations
Teaching point:Clinical history is important to help narrow diagnosis.

Ultrasound Approaches

Ultrasound TechniqueLongitudinal View
UT
CX
CX
UT
* Deferred if virgin
RIGHT LEFT
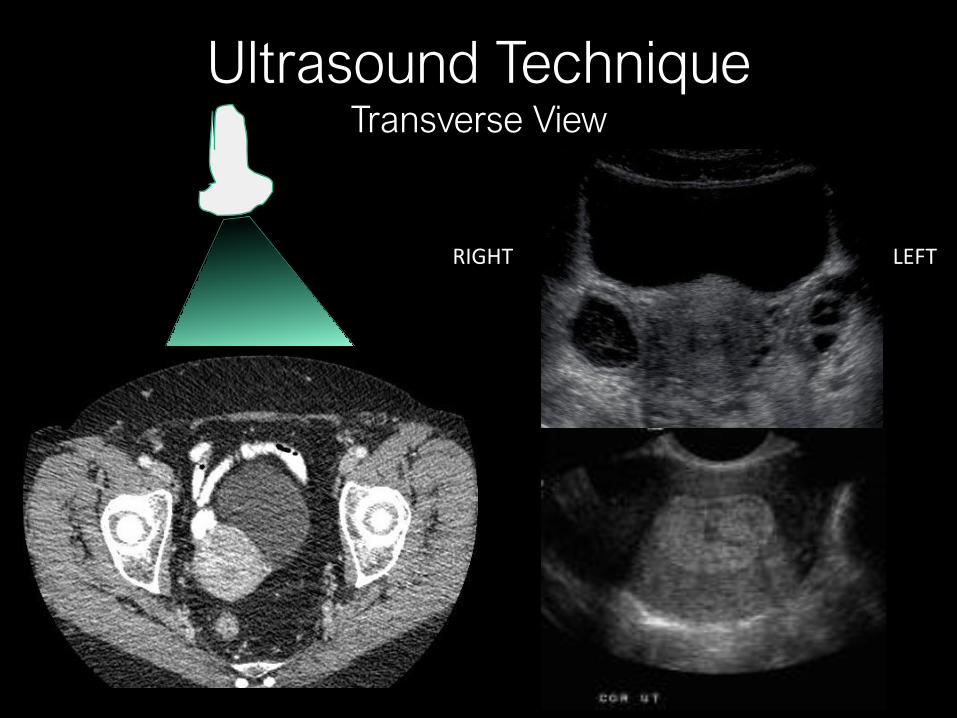
Ultrasound TechniqueTransverse View

Normal ovaries and adnexa
It varies with age!
Premenopausal Physiological folliclesAverage size 9-15 ml
Postmenopausal Punctate echo fociAverage size 2-6 ml

Menstrual cycle variation of ovaries
It varies with age!
2 Phases of Menstrual Cycle
1. EstrogenDay 1-9: Small <5 mm folliclesDay 10: Dominant follicle emergesDay 14: Mature ovum with cumulus oophorus
2. Progesterone:Day 14 Midcycle LH surge: Egg rupture and release creates corpus luteumDay 14-27: Remainder of follicles involute
Estrogen Progesterone

Menstrual cycle variation of uterus
It varies with age!Day 14 Ovulation
Teaching point:Best time to obtain pelvic ultrasound is immediately post menses

Pitfall: Imaging at the Wrong PhaseSecretory phase, h/o heavy bleeding
Proliferative phase Sonohysterogram
Teaching point:Best time to obtain pelvic ultrasound is immediately post menses

Limitations of Pelvic US
Transabdominal :• Empty bladder• Body habitus• Bowel gas
Transvaginal:• Neutral lie of the uterus• Bowel gas• Fibroids

Adnexal Masses

Benign Ovarian Masses
Hemorrhagic Cyst Corpus LuteumSimple Cyst
Levine D, Brown DL, Andreotti RF et-al. Radiology. 2010;256 (3): 943-54Corpus luteum: Case courtesy of Dr Matt A. Morgan, Radiopaedia.org, rID: 42531
Endometrioma Dermoid

Benign Extraovarian Masses
Peritoneal Inclusion CystHydrosalpinx
Levine D, Brown DL, Andreotti RF et-al. Radiology. 2010;256 (3): 943-54
Paraovarian cyst

Management of Benign Ovarian masses

Features concerning for Ovarian Neoplasm
Levine D, Brown DL, Andreotti RF et-al. Radiology. 2010;256 (3): 943-54
Thick Septations (> 3mm) Mural Nodule w/ flow Solid

Abnormal Bleeding

Committee Opinion No. 557 ACOG April 2013
Abnormal Uterine Bleeding

Ultrasound Findings for Menorrhagia
Endometrial Polyps Leiomyomas/FibroidsEndometrial Polyps Adenomyosis
Hyperplastic overgrowthsof endometrial glands and
stroma around vascular core
Benign smooth muscle tumor located in the myometrium
Ectopic endometrial glands and stroma in the
myometrium
Teaching Point:Premenopausal causes for abnormal uterine bleeding are most often benign

Ultrasound Findings for Menorrhagia
US
MRI
Endometrial Polyps Leiomyomas/FibroidsEndometrial Polyps Adenomyosis

Abnormal Bleeding:Malpositioned IUD
Leiomyomas/Fibroids
Benign smooth muscle tumor located in the myometrium
Normal Myometrial penetrationand
Inferiorly positioned
Wildemeersch D, Hasskamp T, Goldstuck ND (2016).. Clin Obstet Gynecol Reprod Med 2

Postmenopausal Bleeding
Causes
Atrophy Polyp Poliferative/Secretory Fibroid Hyperplasia
Atrophy (31%)
Polyp (37%)Atrophy: Endometrial bilayer thickness 4-5 mm or less
Endometrial carcinoma: 7%
Goldstein RB, Bree RL, Benson CB, et al. J Ultrasound Med. 2001 Oct;20(10):1025-36.Van den Bosch, Ameye, Van Schoubroeck, et al. Facts Views Vis Obgyn. 2015; 7(1): 17–24.
ET >20 mm
Teaching Point:Thin postmenopausal endometrium virtually excludes endometrial cancer

SRU Management:Postmenopausal Bleeding
Goldstein RB, Bree RL, Benson CB, et al. J Ultrasound Med. 2001 Oct;20(10):1025-36.

Pelvic Pain

Ultrasound for Acute Pelvic Pain
Not Pregnant
Acute Pelvic Pain
B-Hcg?
PID
Torsion
Appendicitis
Ruptured Cyst
Teaching point: Must obtain pregnancy test prior to ordering a pelvic US
Pregnant
SubchorionicHemorrhage
Pregnancy Failure
Ectopic
Appendicitis

Acute Pelvic Pain in Non-Pregnant Pt
Not Pregnant
PID
Torsion
Appendicitis
Ruptured Cyst
Nl Rt Ov6 year old with LLQ pain, nausea, and vomiting
Torsion of Lt Ov
25 y w fever, CMT, vaginal discharge
TOA Pyosalpinx
Ruptured hemorrhagic cyst
Appendicitis

Which image is a surgical emergency?
PCOS Torsion
Chang H, Bhatt S, Dogra V et-al. Radiographics. Sep 2008, Vol. 28:1355–1368Callen, A.L., Illangasekare, T. & Poder, L. Emerg Radiol (2017) 24: 215.
Ovarian Hyperstimulation
Irregular Menses Nausea, Pelvic Pain Infertility treatment
Teaching point: Clinical history is crucial to accurate diagnosis
Massive Ovarian Edema
Mild painEdema reactive to
Subacute appendicitis
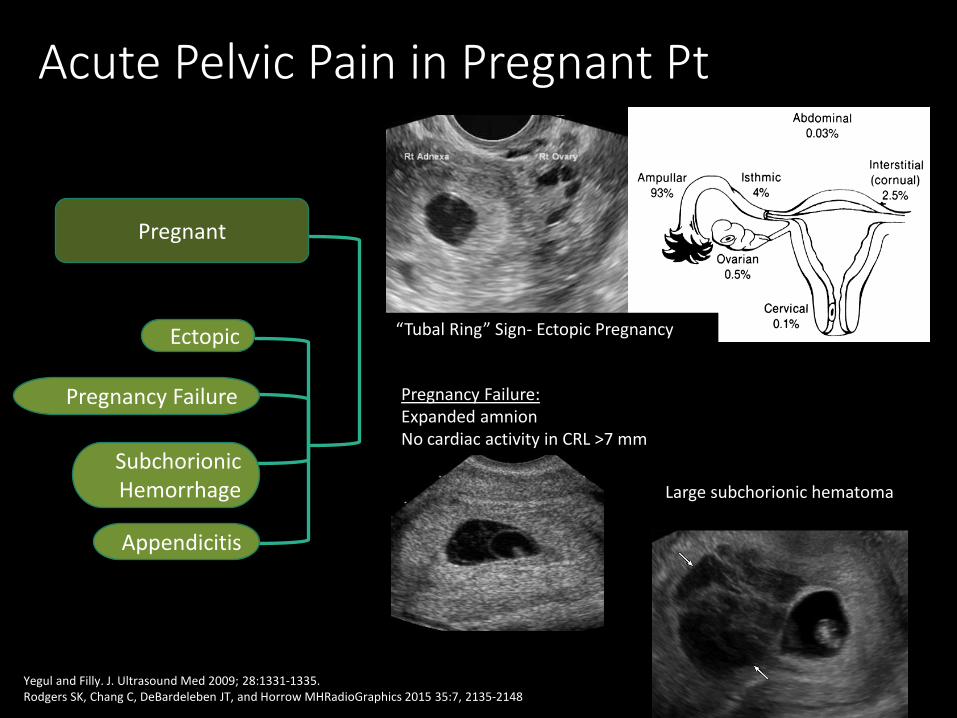
Acute Pelvic Pain in Pregnant Pt
Pregnant
SubchorionicHemorrhage
Pregnancy Failure
Ectopic
Appendicitis
“Tubal Ring” Sign- Ectopic Pregnancy
Yegul and Filly. J. Ultrasound Med 2009; 28:1331-1335.Rodgers SK, Chang C, DeBardeleben JT, and Horrow MHRadioGraphics 2015 35:7, 2135-2148
Pregnancy Failure:Expanded amnionNo cardiac activity in CRL >7 mm
Large subchorionic hematoma

Pregnant Patient

Types of OB US
FIRST TRIMESTER
“THE BASICS”
- Is pregnancy viable?- Where is it?
SECOND TRIMESTER/THIRD TRIMESTER
“PREPARING FOR DELIVERY”
- Is there contraindication to NSVD?- Fetal anomalies?

First Trimester Sonogram (0-13 wks)
• Goals: • Location of implantation: Intrauterine vs. ectopic
• Dating: If last menstrual period (LMP) uncertain
• Viability: Reaching appropriate milestones, +cardiac motion
• Complications: subchorionic hematoma, ovarian masses
• Genetic Screening: Measurement of nuchal translucency (11-13 wks)
• Components:
Embryonic: Include GS, YS, embryo, measurements, cardiac activity, number, anatomy, nuchal
Maternal: Uterus, adnexae, cul-de-sac
• For multiple gestations:
• Establish FETAL NUMBER
• Establish TYPE of twin pregnancy

TV US Landmark Timeline
Radiology 1986; 161:463-467Bradley et al. Radiology 1982; 143:223-226
LMP
2 wks Menstrual Age: Fertilization
2+ wks Decidual (Endometrial) Changes
3.5-4.5 wks Blastocyst implants into decidua: “Intradecidual Sign”
5 wks Empty gestational sac (mean diameter 10 mm)

Radiology 1986; 161:463-467Bradley et al. Radiology 1982; 143:223-226
J Ultrasound Med 2012; 31:87-95
5w 4d Gestational sac with yolk sac visible
6 wks Gestational sac (MSD 16mm) and yolk sac with adj heart beat and small embryo 3mm
6.7 wks Amnion surrounds embryo
8 wks Embryo with CRL 16 mm with separate amniotic sac and coelomic cavity with yolk sac. Fetal body movements visible, HR 175 bpm
YS Embryo w/HM Amnion
TV US Landmark Timeline

First Trimester Sonogram +Beta HCG, No embryo
Pregnancy of Unknown Location
Appropriate rise in B-hcgFollow-up Ultrasound in 8 days
Next Step in Management?
Teaching point: Follow Beta Curve and repeat ultrasound if IUP not confirmed. Ddx: Normal, Abnormal, or Ectopic Pregnancy

Doubilet et al. NEJM Oct 2013;369:1443-1451.
Transvaginal US for diagnosis –TA US CRL >15mm and w/o heartbeat
If Suspicious –Can get US in 7-10 days

First Trimester Sonogram Findings diagnostic for Pregnancy Failure
Mean GS diameter >25 mm, no embryo
CRL >/= 7 mm, no heart beat
Doubilet et al. NEJM Oct 2013;369:1443-1451
Other diagnostic findings:No embryo with heartbeat, 1. >/= 2 weeks after a scan with GS, no YSOr2. >/= 11 days after scan with GS and YS
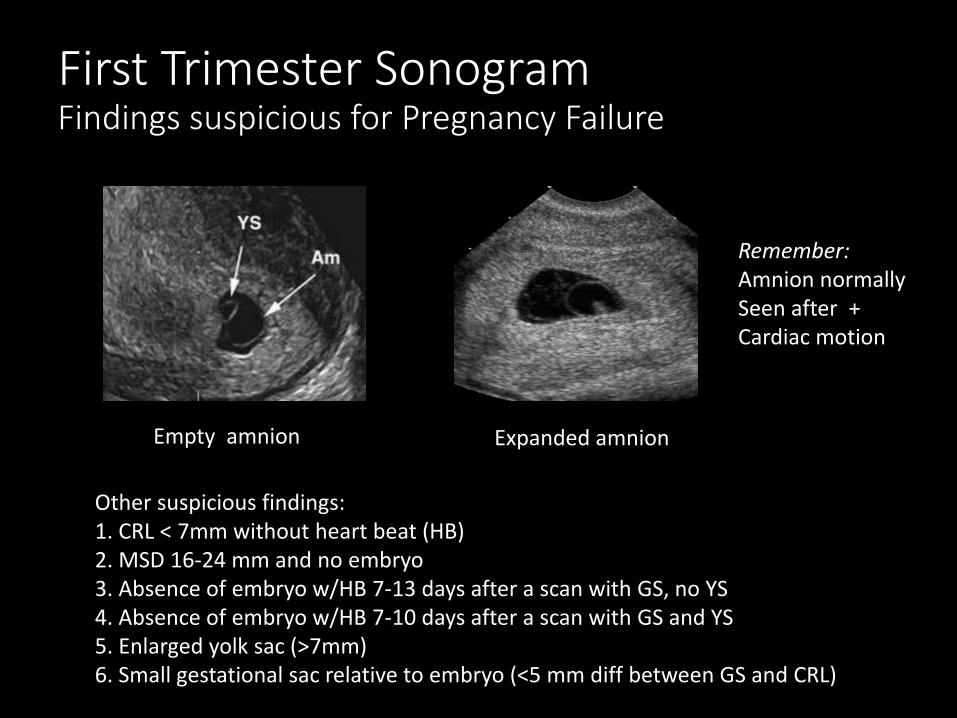
First Trimester Sonogram Findings suspicious for Pregnancy Failure
Empty amnion Expanded amnion
Remember:Amnion normallySeen after +Cardiac motion
Other suspicious findings:1. CRL < 7mm without heart beat (HB)2. MSD 16-24 mm and no embryo3. Absence of embryo w/HB 7-13 days after a scan with GS, no YS4. Absence of embryo w/HB 7-10 days after a scan with GS and YS5. Enlarged yolk sac (>7mm)6. Small gestational sac relative to embryo (<5 mm diff between GS and CRL)

“Bunch of grapes” =
Gestational trophoblastic disease
Molar pregnancy
First Trimester Sonogram +Beta HCG, No embryo

First Trimester Sonogram Ectopic Pregnancy
• Locations: Majority are Tubal 95%Cesarean section Scar Heterotopic (ectopic and intrauterine)
• Present with Vaginal bleeding and Pain
• Risk Factors: Abnormal fallopian tube: PID, prior tubal ligationH/O prior ectopic pregnancyIUDH/O C-sectionFertility Treatment

Ectopic Pregnancy

Determine type of multiple in First Tri US
MonozygoticBrown sisters
of San Francisco
DizygoticScarlett & Hunter
Johansson
(*some monozygotics can be Di/Di)
ConjoinedChang & Eng Bunker
“Siamese Twins”

Chorions = # placentasAmnions = # yolk sacs
Teaching point: Determine type of twin gestation in the first trimesters as management is quite different. May not be able to distinguish later in gestation

Second Trimester Ultrasound(14-26 weeks)
• Routinely done at about 18-22 weeks
• Level 1 and 2
• Level 1: Basic screening
• Level 2: Targeted, High Risk
• Limited
Components1. Fetal presentation
2. Fetal number
3. Cardiac activity
4. Amniotic Fluid Volume
5. Gestational age assessmnt
6. Fetal Weight est
7. Fetal anatomy
8. Placental and cord
9. Maternal anatomy, incl cervix

Fetal Presentation
Vertex (cephalic presentation)
Head located above Cx
Cervix
Fetal Head

Cervical Length
Closed Cervical length
Less than 24 weeks: >/= 2.5 cm
Abnormal: Funneled and Short

Placenta Location
Posterior Placenta
Concerning: Placenta Previa
Complete Previa
Cx
• Placenta overlies internal cervical os
• Increased bleeding risk• C-section delivery at
36 w – 37w6d

Placental Cord Insertion & Placental Types
Placenta
Cord Insertions
Vasa Previa
Bilobed Placenta Succenturiate Lobe
Teaching point: Screen for Vasa Previa due to high risk of bleeding

Amniotic Fluid Volume• Qualitative vs Quantitative
• Qualitative: Subjective
• Quantitative: 1. Amniotic fluid Index
Sum 4 quadrantsNormal 8-24 cmOligohydramnios <5 cmPolyhydramnios >24 cm
2. Deepest vertical pocket (DVP)Normal 2-8 cmOligohydramnios <2 cmPolyhydramnios >8 cm
Reddy UM, Abuhamad AZ, Levine D, et al. Obstet Gynecol. 2014;123(5):1070.

Abnormal Amniotic Fluid Volume
OligohydramniosNormal
DVP
Polyhydramnios

Gestational Age/Fetal BiometryBiparietal Diameter : Head Circumference
Abdominal Circumference Femur Length

Estimated Fetal Weight

Fetal Anatomy
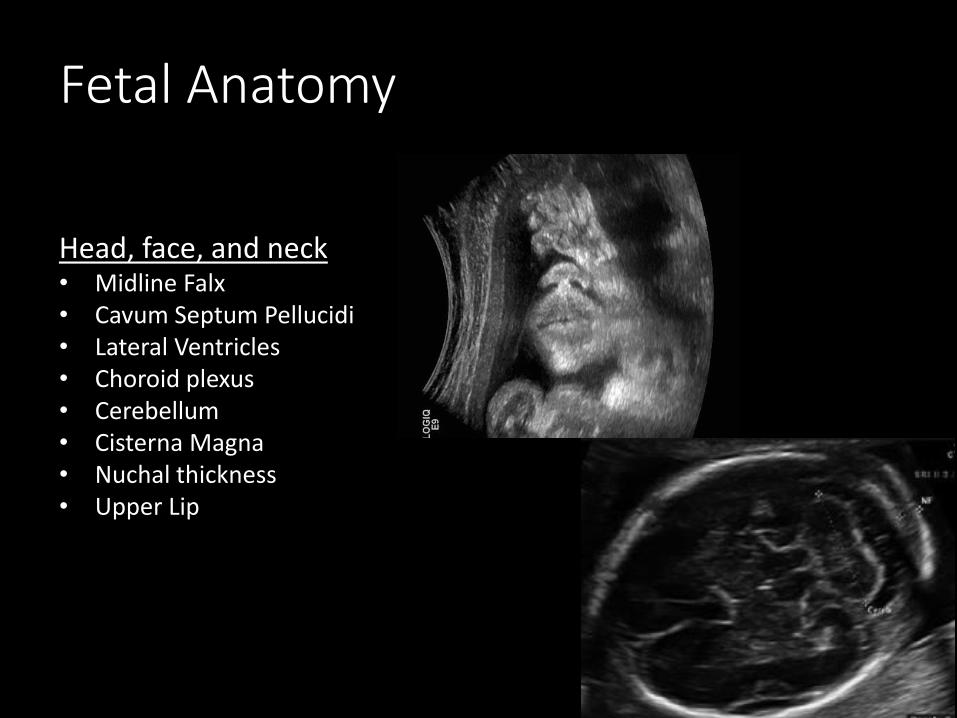
Head, face, and neck• Midline Falx• Cavum Septum Pellucidi• Lateral Ventricles• Choroid plexus• Cerebellum• Cisterna Magna• Nuchal thickness• Upper Lip
Chest• Four Chamber Heart• Outflow Tracts
Abdomen• Stomach• Kidneys• Urinary bladder• Abdominal cord insertion• Umbilical cord vessel
number
Spine
Extremities
Genitalia
Fetal Anatomy
Head, face, and neck• Midline Falx• Cavum Septum Pellucidi• Lateral Ventricles• Choroid plexus• Cerebellum• Cisterna Magna• Nuchal thickness• Upper Lip

Fetal Anatomy
Chest• Four Chamber Heart• Outflow Tracts
RVOT
LVOT

Fetal Anatomy
Abdomen• Stomach• Kidneys• Urinary bladder• Umbilical cord vessel
number• Abdominal cord insertion

Fetal Anatomy
Spine
Extremities
Genitalia

Fetal Anomalies
Cleft Lip
Myelomeningocele
Anencephaly
Gastroschisis

Questions

Question 1
The best first imaging test for a pelvic mass in a female patients is:
a) MRI
b) CT
c) Ultrasound
d) PET scan

The best first imaging test for a pelvic mass in a female patients is:
a) MRI
b) CT
c) Ultrasound
d) PET scan
Question 1

A patient presents with first trimester bleeding. What ultrasound finding would be reassuring for a potentially viable pregnancy?
a) An adnexal mass
b) Gestational sac with embryo within the uterus
c) Normal uterus without a gestational sac or embryo
d) Free fluid in the pelvis
Question 2

A patient presents with first trimester bleeding. What ultrasound finding would be reassuring for a potentially viable pregnancy?
a) An adnexal mass
b) Gestational sac with embryo within the uterus
c) Normal uterus without a gestational sac or embryo
d) Free fluid in the pelvis
Question 2

For a twin pregnancy, when is ultrasound most accurate for determining the chorionicity and amnionicity of the pregnancy?
a) Second trimester
b) First trimester
c) It makes no difference, measurement is easy and accurate at any point in the pregnancy
d) Right before delivery
Question 3

For a twin pregnancy, when is ultrasound most accurate for determining the chorionicity and amnionicity of the pregnancy?
a) Second trimester
b) First trimester
c) It makes no difference, measurement is easy and accurate at any point in the pregnancy
d) Right before delivery
Question 3

Which of the following fetal assessments is commonly performed on a first trimester ultrasound?
a) Sonographic age
b) Fetal anatomy
c) Amniotic fluid volume
d) Placental position
Question 4

Which of the following fetal assessments is commonly performed on a first trimester ultrasound?
a) Sonographic age
b) Fetal anatomy
c) Amniotic fluid volume
d) Placental position
Question 4

Which of the following is most important in evaluating whether the thickness of the endometrium is abnormal?
a) Parity
b) Phase of menstrual cycle
c) History of C section
d) Presence of fibroids
Question 5

Which of the following is most important in evaluating whether the thickness of the endometrium is abnormal?
a) Parity
b) Phase of menstrual cycle
c) History of C section
d) Presence of fibroids
Question 5

END



![Ob US MRI Correlation.ppt - mc.vanderbilt.edu … · T1 and T2 Values for Brain Tissues at 1.5 Tesla ... • congenital infarction. ... Ob US MRI Correlation.ppt [Compatibility Mode]](https://static.fdocuments.us/doc/165x107/5af8a69a7f8b9a5f588d07ea/ob-us-mri-mcvanderbiltedu-t1-and-t2-values-for-brain-tissues-at-15-tesla.jpg)