CHAPTER 2 HUMAN MAXILLARY SINUS FLOOR ELEVATION AS A … · Since the reconstruction of (large)...
26
CHAPTER 2 HUMAN MAXILLARY SINUS FLOOR ELEVATION AS A MODEL FOR BONE REGENERATION ENABLING THE APPLICATION OF ONE-STEP SURGICAL PROCEDURES Tissue Engineering part B 2012,19:69-82 Elisabet Farré-Guasch 1* , Henk-Jan Prins 1,2* , Janice R. Overman 1,2 , Christiaan M. ten Bruggenkate 2 , Engelbert A.J.M. Schulten 2 , Marco N. Helder 3# , Jenneke Klein Nulend 1# 1 2 3 Department of Oral Cell Biology, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University Amsterdam, MOVE Research Institute Amsterdam, The Netherlands Department of Oral and Maxillofacial Surgery, VU University Medical Center/ACTA, MOVE Research Institute Amsterdam, The Netherlands Department of Orthopedic Surgery, VU University Medical Center Amsterdam, MOVE Research Institute Amsterdam, The Netherlands * # Shared first authorship, E. Farré-Guasch and H.J. Prins contributed equally to this manuscript. Shared last authorship, M.N. Helder and J. Klein-Nulend contributed equally to this manuscript.
Transcript of CHAPTER 2 HUMAN MAXILLARY SINUS FLOOR ELEVATION AS A … · Since the reconstruction of (large)...

CHAPTER 2
HUMAN MAXILLARY SINUS FLOOR ELEVATION AS A MODEL FOR BONE REGENERATION ENABLING THE APPLICATION OF
ONE-STEP SURGICAL PROCEDURES
Tissue Engineering part B 2012,19:69-82
Elisabet Farré-Guasch1*, Henk-Jan Prins1,2*, Janice R. Overman1,2, Christiaan M. ten Bruggenkate2, Engelbert A.J.M. Schulten2,
Marco N. Helder3#, Jenneke Klein Nulend1#
1
2
3
Department of Oral Cell Biology, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University Amsterdam, MOVE Research Institute Amsterdam, The Netherlands Department of Oral and Maxillofacial Surgery, VU University Medical Center/ACTA, MOVE Research Institute Amsterdam, The NetherlandsDepartment of Orthopedic Surgery, VU University Medical Center Amsterdam, MOVE Research Institute Amsterdam, The Netherlands
*
#
Shared first authorship, E. Farré-Guasch and H.J. Prins contributed equally to this manuscript. Shared last authorship, M.N. Helder and J. Klein-Nulend contributed equally to this manuscript.

16
ABSTRACT
Bone loss in the oral and maxillofacial region caused by trauma, tumors, congenital disorders or degenerative diseases is a health care problem worldwide. To restore (reconstruct) these bone defects human or animal bone grafts or alloplastic (synthetic) materials have been used. However, several disadvantages are associated with bone graft transplantation, such as limited bone volume, donor-site morbidity, surgical and immune rejection risks, and lack of osseo-integration. Bone tissue engineering is emerging as a valid alternative to treat bone defects allowing the regeneration of lost bony tissue thereby recovering its functionality. During the last decades the increasing aged population worldwide has also raised the prevalence of maxillary atrophy. Maxillary sinus floor elevation (MSFE) has become a standard surgical procedure to overcome the reduced amount of bone, thus enabling the placement of dental implants. MSFE aims to increase bone height in the posterior maxilla, by elevating the Schneiderian membrane and placing graft material into the surgically-created space in the maxillary sinus floor. Importantly, oral bone regeneration during MSFE offers an unique human clinical model in which new cell-based bone tissue engineering applications might be investigated, since biopsies can be taken after MSFE prior to dental implant placement and analyzed at the cellular level. New approaches in oral bone regeneration are focusing on cells, growth factors, and biomaterials. Recently adipose tissue has become interesting as an abundant source of mesenchymal stem cells which might be applied immediately after isolation to the patient allowing a one-step surgical procedure, thereby avoiding expensive cell culture procedures and another surgical operation. In this new cell-based tissue engineering approach, stem cells are combined with an osteoconductive scaffold and growth factors, and applied immediately to the patient. In this review MSFE is discussed as a valid model to test bone tissue engineering approaches, such as the one-step surgical procedure. This procedure might be applied in other regenerative medicine applications as well.
KEY WORDS: Adipose stem cells, oral and maxillofacial bone regeneration, one-step surgical procedure, scaffold, maxillary sinus floor elevation, stromal vascular fraction, growth factors
Chapter 2

17
Human MSFE as a model for bone regeneration
INTRODUCTION
The increasing aged population worldwide has raised the prevalence of maxillary and mandibular atrophy, which is mainly caused by tooth loss. Bone loss in the oral and maxillofacial region can also result from trauma, congenital disorders, ablation of tumors and enucleation of cysts, anatomical events such as pneumatization of the maxillary sinus, and infections.1 A solution to restore the lost oral function in edentulous patients is the placement of dental implants. However, a common problem for implant placement is the lack of sufficient bone height caused by excessive bone resorption, which occurs after tooth loss, particularly in the posterior maxillary bone.2 The maxillary sinus floor elevation (MSFE) procedure aims to increase bone height to allow dental implant placement and obtain initial mechanical stability.3 Since the reconstruction of (large) bone defects in the oral and maxillofacial region is a common challenge, bone tissue engineering has become a promising alternative for bone reconstruction. However, the application of bone tissue engineering approaches in the clinic is hampered by the fact that there is not a good human model available to study these concepts. MSFE could represent an excellent human model to study new bone tissue engineering modalities such as the one-step surgical procedure avoiding the use of autologous bone (Figure 1). In this one-step surgical procedure, adipose tissue is harvested and processed to obtain the stromal vascular fraction (SVF) which contains adipose stem cells (ASCs). These stem cells can be seeded on off-the-shelf scaffolds, to be applied immediately to the patient in an intra-operative concept.4, 5
Maxillary sinus floor elevationThe surgical procedure of MSFE was first performed by Tatum6 and published by Boyne.7 In the procedure described, a window in the lateral wall of the maxillary sinus is made, followed by elevation of the maxillary sinus membrane (Schneiderian membrane) to create a cavity in which a bone graft can be placed (Figure 2). Nowadays, MSFE has become a standard surgical procedure to increase bone height in the posterior maxilla.2, 8 This procedure provides sufficient alveolar bone height for placement of dental implants after the appropriate healing time of the graft and increases implant success.
Bone graft materials in maxillary sinus floor elevationTatum6 introduced the use of allograft or bone from another individual of the same species, and alloplast or synthetic material, besides autograft to fill the space created when elevating the Schneiderian membrane, thereby eliminating the need for a second surgery to obtain an autologous bone graft, and thus also reducing potential complications from an additional surgery.9 The lateral window maxillary sinus floor elevation technique is commonly used nowadays, and still the best results are achieved using autologous bone.3, 10 Bone grafting material such as demineralized bone matrix is also commonly used. It induces bone formation in the human maxillary sinus by providing an osteoconductive matrix that allows migration of precursor cells from the host and differentiation into bone matrix-producing cells8 (Figure 2).

18
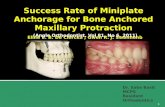
Figure 2. Schematic figure of the MSFE procedure. (A) MSFE is performed via a lateral approach. After reflection of the mucoperiosteal flap, a bony window is created in the lateral wall of the maxillary sinus followed by elevation of the maxillary sinus membrane (Schneiderian membrane) to create a cavity in which the bone substitute is placed. This bone substitute provides a osteoconductive matrix that allows migration of osteoprogenitor cells from the adjacent bone, and bone formation occurs via osteoconduction. (B) The bone substitute is seeded with adipose stem cells. The addition of adipose stem cells with angiogenic and osteogenic potential stimulates osteogenesis, osteoinduction, and vascularization, which enhances bone formation throughout the whole (with bone substitute filled) maxillary sinus. Color images available online at www.liebertpub.com/teb
Chapter 2

19
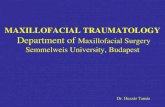
Figure 1. Concept of a maxillary sinus floor elevation (MSFE) with freshly isolated adipose-derived stem cells in a one-step surgical procedure. (A) The plastic surgeon starts harvesting adipose tissue by liposuction. (B) The adipose tissue and liposuction fluid is collected in syringes. (C) The filled syringes are transferred into a Celution 800/CRS system. This device washes, digests, and centrifugates the adipose tissue to obtain the fresh stromal vascular fraction containing the adipose stem cells. After isolation of the stromal vascular fraction, cells can be shortly stimulated with the growth factors before seeding the stimulated cells onto a carrier material. (D) The freshly isolated adipose stem cells are seeded onto the calcium phosphate carrier. Unattached cells are washed off, and the calcium phosphate carrier combined with stem cells (stam= stem cells). (E) During the short attachment period of the cells (30min), the patient is prepared for the MSFE procedure via a lateral approach. After reflection of the mucoperiosteal flap, a bony window is created in the lateral wall of the maxillary sinus and carefully moved and rotated medially toward the maxillary sinus, after dissection of the maxillary sinus mucosa (trap-door technique). (F) The tissue-engineered construct is inserted immediately into the patient, and the space created is filled with the bone substitute combined with the adipose stem cells. (G) Finally, the wound is closed. Color images available online at www.liebertpub.com/teb
A variety of bone grafts are used for MSFE with different degrees of success (Table 1). The bone graft materials applied in MSFE are: 1) autologous bone graft, mostly from the iliac crest or mandibular bone, 2) allograft, 3) xenograft, from bovine or porcine origin, and 4) alloplast materials, such as β-tricalcium phosphate (β-TCP), hydroxyapatite (HA), mixtures of HA/β-TCP (biphasic calcium phosphate; BCP), polymers, and bioactive glasses. Autologous bone graft is still considered as the ‘gold standard’, since it contains osteoblasts and osteoprogenitor cells, and is not only osteoconductive by allowing the migration of progenitor cells, but also osteogenic. 11-13 Since these grafts are from the same individual the tissue is recognized as “self”, and the immune system is not triggered with an immunological response.14 Although it is generally accepted that autologous bone is the ‘gold standard’ for the MSFE procedure, this may not always be the case. Abscesses, fistulas, dehiscences, and large numbers of bacteria can be found in particulated bone collected with suction devices such as bone traps,15 in addition to the disadvantage of limited bone availability and patient morbidity.14 Alternative bone graft materials frequently used are allogenic bone and bone substitutes. Allogenic bone is mostly applied in the form of demineralized freeze-dried bone matrix. The bone morphogenetic proteins (BMPs) present in the matrix of bone allograft are exposed by decalcification leading to induction of osteogenic differentiation of progenitor cells. However, The Sinus Consensus Conference held in Wellesley, MA, USA, in 1996 concluded that demineralized freeze-dried bone is not an appropriate bone substitute, since it always carries the risk of disease transmission and might cause marked bone resorption.11 Other disadvantages, such as lack of osteogenesis and osseointegration, and the risk of immune rejection at the implant site,16, 17 lead to a search for alternative graft materials. Bone substitutes are interesting alternatives because they are available in unlimited quantity and may be used as off-the-shelf products. However, bone substitutes are cell-free and require more time for bone healing than autologous bone grafts.18 It has been shown that maxillary sinus grafting with alloplast materials such as bioactive glass, HA, or β-TCP does not result in increased bone volume compared with autologous bone graft.10, 12 Several attempts
Human MSFE as a model for bone regeneration

20
have been made to apply a cell-based approach using stem cells combined with an osteoconductive biomaterial or scaffold, which is known as cell-based bone tissue engineering.19-23
Bone Tissue Engineering in Maxillary Sinus Floor Elevation: a Potential Model to be Used in Other Surgical DisciplinesFor cell-based bone tissue engineering the choice of osteoprogenitor cells and biomaterials is crucial, as well as the type of growth factor(s) that stimulate osteogenesis and improve osteogenic differentiation of the progenitor cells. Bone regeneration in the oral and maxillofacial region can be used to investigate tissue engineering approaches for later use in other surgical disciplines. Bone biopsies from patients can be taken after an MSFE procedure and prior to dental implant placement. These bone biopsies can then be analyzed by micro-CT, histomorphometry, and histology24-27 and are highly valuable for evaluating new approaches for oral and maxillofacial bone tissue engineering, such as the use of different progenitor cells, growth factors, and biomaterials. Furthermore, the treatment of patients requiring an MFSE procedure at both sites of the maxilla enables the use of a bilateral split-mouth design model, allowing to study simultaneously different conditions in the same patient. Therefore, the MSFE procedure is proposed as a human model for bone regeneration to be used in a so-called one-step surgical procedure. The maxillary sinus represents an excellent model as an osteogenic chamber for bone regeneration.28
The lack of quantitative or histomorphometrical data becomes an important drawback in studies comparing different bone grafts for MSFE.29 Clinically it is difficult and time consuming to analyze a large number of samples,13 and therefore it is desirable to generate a variety of studies with similar approaches, and to combine and compare these results in a meta-analysis.A cell-based approach that uses stem cells combined with an osteoconductive scaffold may become an interesting alternative to conventional procedures, avoiding the major problems associated with bone graft transplantation. However, the paradigm of tissue engineering is to find a suitable human model to investigate the appropriate combination of scaffold and source of osteoprogenitor cells. A limitation for successful application of bone tissue engineering in MSFE is the relative absence of mechanical loading, which is a critical issue for bone regeneration. It has been shown that mechanical loading favours proliferation and osteogenic differentiation of progenitor cells while inhibiting adipogenic differentiation,30 and this should be taken into account to decide the appropriate time for implant loading.
Sources of Stem/Progenitor Cells for Clinical ApplicationIn the late 60s, Friedenstein showed that the mesenchymal stroma from human bone marrow contains a population of cells that proliferate when cultured on plastic, and differentiate to cell lineages derived from the mesoderm, such as chondrocytes and osteoblasts.31 Later these precursor spindle-shape cells are referred to as mesenchymal stem cells (MSCs)32 and shown to differentiate into several lineages in vitro33 and in vivo,34, 35 making them promising candidates for regenerative medicine applications. MSCs grow when adhered to plastic and express specific surface antigens. They also possess multipotent differentiation potential and low immunogenic
Chapter 2

21
Calvarial defects were critical-sized. ABB, anorganic bovine bone; DBM, demineralized bone matrix; FN, fibronectin; CaP, calcium phosphate; HA, hydroxyapatite; ß-TCP, ß-Tricalcium phosphate; BCP, biphasic calcium phosphate (%HA/%ß-TCP); PLA, polylactic acid; PLGA, polylactic-coglycolide copolymers; SVF, stromal vascular fraction; ASCs, adipose stem cells; BM-MSCs, bone marrow-derived mesenchymal stem cells; BMP-2, bone morphogenetic protein-2; PRP, platelet-rich plasma; MSFE, maxillary sinus floor elevation; GBR, guided bone regeneration; n.a., not available.
Human MSFE as a model for bone regeneration
Table 1. (Pre)clinical in vivo studies using mesenchymal stem cells from bone marrow or adipose tissue and stromal vascular fraction from adipose tissue for oral and maxillofacial bone tissue engineering applications in human and animal models: bone volume measurements.

22
potential, according to the minimal criteria to define MSCs, proposed in 2006 by the International Society for Cellular Therapy.36 Their immunosuppressive properties and differentiation potential make MSCs interesting for regenerative medicine clinical applications. The main sources of MSCs for clinical studies in bone tissue engineering are bone marrow and adipose tissue.
Bone marrow-derived mesenchymal stem cellsBone marrow-derived MSCs (BM-MSCs) are widely used in bone regeneration, since they are relatively easy to harvest and show multipotent differentiation potential.33-35, 37 MSCs secrete growth factors and cytokines that inhibit apoptosis and fibrosis or scarring at the site of injury. They also stimulate angiogenesis and proliferation of progenitor cells, and exert an immunomodulatory effect in the organism. These effects, known as “the trophic activity”,38 make them interesting candidates to improve bone regeneration in the MSFE procedure (Table 2). Addition of bone marrow-derived MSCs to bone derivative/substitute materials such as BCP particles enhances bone formation in the maxillary sinus area, with 41% mean percentage of newly formed bone observed at 3 months post-surgery.23 Another study using BCP without cells showed 27% average of bone volume at 6 months post-surgery.25 BM-MSCs applied to calcium phosphate scaffolds for MSFE promote faster bone formation and mineralization in animal models.39-42 One study in rabbits found an increase in bone formation when BM-MSCs were applied to a calcium phosphate scaffold in comparison with scaffold without cells.43 These results suggest that BM-MSCs may improve new bone regeneration in the maxillary sinus. The use of BM-MSCs also has disadvantages, such as pain associated with the harvest procedure and low cell numbers upon harvest, especially in elderly patients.44 Only one MSC per 105 adherent mononuclear cells is obtained upon harvest,33 necessitating an ex vivo expansion step to obtain therapeutic cell numbers, which is time consuming, expensive, and carries the risk of contamination. Long cell culture is associated with loss of differentiation potential and risk of cell transformation.45, 46 The number and concentration of progenitor cells with angiogenic potential in a scaffold are also important for successful bone formation in vivo, since the vascular network is crucial to ensure cell survival.47 These considerations associated with BM-MSCs have led to a search for other sources of progenitor cells for clinical application.
Adipose stem cellsAdipose tissue has gained interest as it contains a population of stem cells with MSC characteristics.48 Adipose tissue, as bone marrow, is derived from adult mesodermal tissue, and after tissue disaggregation, collagenase digestion and cell centrifugation, a pellet is obtained which contains a heterogeneous cell population composed of pre-adipocytes, mast cells, endothelial cells, pericytes, smooth muscle cells, fibroblasts, and multipotent progenitor cells with similar characteristics to BM-MSCs, as well as hematopoietic stem cells.48 This mixture of cells is known as the stromal vascular fraction (SVF). When the pellet is cultured, an adherent cell population is obtained which can be expanded and used in a variety of assays. A wide nomenclature is used to identify this cell population, including adipocyte precursor cells, preadipocytes, adipose-derived adult stem cells, adipose-derived stromal cells, adipose-derived adherent stromal cells, processed lipoaspirate
Chapter 2

23
Human MSFE as a model for bone regeneration
Table 2. (Pre)clinical in vivo studies using autograft, allograft (demineralized bone matrix and mineralized cancellous bone), xenograft (from bovine or from porcine origin), inorganic materials containing calcium phosphate, polymers, and bioglass for oral and maxillofacial bone tissue engineering applications in human and animal models: bone volume measurements.
Calvarial defects were critical-sized. ABB, anorganic bovine bone; MCBA, mineralized cancellous bone allograft; DBM, demineralized bone matrix; CaCO3, calcium carbonate; CaSO4, calcium sulfate; CaP, calcium phosphate; HA, hydroxyapatite; ß-TCP, ß-Tricalcium phosphate; BCP, biphasic calcium phosphate (%HA/%ß-TCP); PLA, polylactic acid; PLGA, polylactic-coglycolide copolymers; VEGF, vascular endothelial growth factor; BMP-2, bone morphogenetic protein-2; BMP-7, bone morphogenetic protein-7; PRP, platelet-rich plasma; GDF-5, growth and differentiation factor-5; MSFE, maxillary sinus floor elevation. n.a.; not available.

24
cells, and adipose-derived stem cells.49 At the Second Annual International Fat Applied Technology Society meeting (October 3-5, 2004, Pittsburgh, PA), consensus was reached to use the term SVF for the freshly isolated stromal vascular fraction, and to refer to the stem cell-like cells within this fraction as ASCs (adipose stromal cells or adipose stem cells). Passaged cells (cells cultured to homogeneity) are also referred to as ASCs. These ASCs can differentiate into multiple mesenchymal tissue cell types, such as osteoblasts, chondrocytes, adipocytes, and myocytes.50
ASCs become an interesting alternative to BM-MSCs, since adipose tissue is easy to access, and its harvesting results in minimal patient discomfort. Furthermore, adipose tissue contains a 100 to 1000-fold higher number of stem cells than bone marrow, and ASCs proliferate faster than BM-MSCs.4, 33, 50, 51 ASCs also secrete growth factors with angiogenic and anti-apoptotic potential, which makes them interesting candidates for bone tissue engineering where blood supply is needed.51-53 These angiogenic properties allow them to survive in low oxygen environments, and make them good candidates for cell-based therapies such as maxillary reconstruction.22 ASCs also abundantly express CD34,54 in contrast with MSCs which lack CD34 expression.36, 55 Cultured ASCs show decreased CD34 expression, which is totally lost after long-term culture.49, 54 The marker CD34, which is also expressed in hematopoietic and endothelial stem cells, is related to angiogenesis and could have important implications in bone tissue engineering, where angiogenesis is crucial.52, 56
Since the amount of bone formed depends at least in part on the number of cells that survive, it is crucial to provide a high number of osteoprogenitor cells per given volume of tissue, to ensure adequate bone formation. A dose-dependent effect on bone formation has been reported for cultured ASCs applied to a calvarium rabbit bone defect.57 ASCs promote healing of critical-sized cranial defects in mice and rabbits,57-60 and have been successfully used in animal models for vertical bone regeneration,57 as well as in MSFE using the SVF containing the ASCs61 (Table 2). ASCs have been used successfully in humans to reconstruct major maxillary defects22 and traumatic calvarial defects.62 Calvarial bone is embryologically, morphologically and physiologically similar to bone in the oral and maxillofacial region. Its high flat surface eases the fixation of titanium osteosynthesis57 making it an interesting model to study oral bone regeneration. Adipose tissue may be an interesting source of progenitor cells for oral and maxillofacial applications, where high cell numbers may be needed for successful bone regeneration. To select the appropriate scaffold for combination with these cells is another critical issue in bone regeneration.
Scaffolds for Oral and Maxillofacial Bone Tissue Engineering Not only the appropriate source of progenitor cells, but also the use of the right type of carrier scaffold with adequate pore size, porosity and composition, is a key issue in bone tissue engineering. The ideal scaffold has a high porosity and interconnected pore network, which is large enough to facilitate vascular invasion and bone development.26 Large pore sizes (>300 µm) promote neo-vascularization and favor mineralized bone ingrowth, whereas smaller pore sizes (90–120 µm) promote endochondral bone formation.63 For tissue engineering the ideal scaffold should be biocompatible with the right porosity and pore size to facilitate neo-vascularization,
Chapter 2

25
and an adequate surface allowing cell adhesion, proliferation, and differentiation. Furthermore the scaffold should be osteoinductive, releasing growth factors that modulate osteoblastic cell functions and enhance bone formation, and the mechanical properties should match those of living bone. Finally the scaffold degradation rate should be tuned with the growth rate of the de novo bone formation, id est the scaffold is totally degraded by the time the injury site is fully regenerated.3, 64 The size of the scaffold is also important for adequate bone regeneration. Particles with a size ranging from 250-500 µm have been shown to increase the volume of mineralized tissue in MSFE showing the presence of lamellar and woven bone.8 Absorbable scaffolds used in bone tissue engineering are divided in biodegradable polymers of synthetic origin, such as polylactic acid (PLA), polyglicolic acid (PGA), polylactic-coglycolide copolymers (PLGA), and Poly(ε-caprolactone) (PCL),65-68 natural polymers such as collagen, hyaluronic acid, fibrin, and silk fibroin,64, 69-72 bioactive glasses with a silica-based osteoinductive surface,73 inorganic materials containing calcium phosphate (ceramics), and finally composite materials, which combine for example calcium phosphates ceramics with polymers.64
Various grafts or combination of graft materials have been used successfully in the oral and maxillofacial region (Table 2). Inorganic materials or ceramics from natural origin, such as calcium carbonate, calcium phosphate, calcium sulfate, bovine-derived or coralline HA, and from synthetic origin, such as synthetic HA or ß-TCP have been widely used in MSFE due totheir good biocompatibility and osteoconductivity,10, 26, 74-79 besides bone grafts,13, 16, 17, 26, 29, 74, 77, 78 polymers28, 78, 80-86 and bioactive glass.78, 87, 88
Synthetic Calcium Phosphate Scaffolds for Oral and Maxillofacial Bone Tissue Engineering HA and ß-TCP have been successfully used for MSFE procedures because of their good biocompatibility and chemical composition, which resembles the composition of natural bone matrix.10, 25, 89, 90 Advantages of using ceramics such as β-TCP is that they support cell in-growth and promote osteogenic differentiation of osteoprogenitor cells.90, 91 However, unlike HA, β-TCP reabsorbs rapidly, but concurrent bone formation does not occur in a 1:1 ratio, and often less bone is produced as compared with the volume of β-TCP absorbed.10 BCP combines the bioactive properties of HA with the good bioresorbability of β-TCP. Due to its high surface area and 3D hierarchical porosity, it supports attachment, proliferation, and osteogenic differentiation of progenitor cells.92, 93 BCP contains a mixture of 60% HA and 40% β-TCP and has been used successfully for MSFE,25-27, 94 with an implant survival >98%27, 89 and bone formation similar to allograft and xenograft.16, 26 The macroporosity (pore diameter 300 to 600 µm) of BCP scaffold allows colonization by osteogenic cells. Osteoclasts attach to BCP surface to resorb biomaterial, stimulating osteoblast differentiation and activity through signaling molecules, while no osteoclast resorption is found on β-TCP material, which is resorbed mainly by chemical dissolution.90, 95 This suggests that BCP material may be promising for use as a scaffold for bone tissue engineering. The favorable clinical results obtained with BCP are similar as those obtained with xenografts, such as inorganic bovine bone,13, 16 or other alloplastic materials such as HA.26 However, significantly less bone formation is observed when compared with autologous bone
Human MSFE as a model for bone regeneration

26
grafts, indicating that autologous bone grafts still remain the ‘gold standard’, showing increased bone formation compared to alloplast material and xenografts.13, 24, 27, 77, 78, 87 In certain augmentation cases, such as maxillary sinus grafting, complete resorption of the bone substitute to be replaced by new bone is not preferable. A long-lasting active osteoconductive guiding scaffold is required to support osseointegrated dental implants without destabilization of bone.74 Therefore the stability of the graft material in the maxillary sinus and height changes of the graft material over time are important issues for successful bone regeneration in MSFE. Calcium phosphates ceramics have also drawbacks, such as lack of osteogenic properties, brittleness and low mechanical stability observed when using ß-TCP, which makes them unsuitable for reconstruction of large bone defects.65, 96 Therefore addition of osteoprogenitor cells might be required to improve the osteogenic properties of the graft, since the ideal bone graft should provide osteogenic cells as well as osteoinductive factors for bone regeneration64 (Table 1). For clinical application of bone tissue engineering, the appropriate source of stem cells together with the adequate scaffold, and the use of growth factors that speed up tissue regeneration are crucial issues for successful clinical application.97, 98
Growth Factors for Oral and Maxillofacial Bone Tissue EngineeringAngiogenesis is extremely important in bone regeneration, since blood vessels carry nutrients which are crucial to ensure the survival of transplanted progenitor cells,99 and vascular development needs to be induced prior to osteogenesis.77, 100 To establish the vascular network, growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β), vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), and those factors present in platelet-rich plasma (PRP), a platelet concentrate obtained from the patient’s own blood, are needed to induce and speed up angiogenesis in the regenerating tissue, and may be used in oral and maxillofacial applications to reduce the healing time and enhance bone formation53, 84, 101-105 (Table 3). These growth factors can be added to all grafting materials. There is controversy in the literature related to the use of PRP in MSFE procedures. Although some studies found an effect of PRP on bone formation in combination with bone substitutes104 and bone grafts,106 other studies did not find such an effect when PRP was combined with a xenograft,29 an autologous bone graft,12 or a synthetic bone substitute.87 Ex vivo seeded ASCs onto a scaffold secrete a high variety of angiogenic growth factors, such as VEGF and FGF-2, which makes them interesting candidates for inducing bone tissue formation.51, 107
One substantial group of growth factors for bone tissue engineering are the bone morphogenetic proteins (BMPs). BMPs have been found in the demineralized bone matrix more than 40 years ago. They belong to the TGF-ß superfamily and promote the differentiation of osteoprogenitor cells and induce osteogenesis.108 An acute increase in the secretion of bone morphogenetic protein-2 (BMP-2) and bone morphogenetic protein-7 (BMP-7), together with bone morphogenetic protein-4 (BMP-4), has been shown when applying ASCs in critical-sized mouse defects,58 which suggests a role of these growth factors in bone regeneration and remodeling. The osteoinductive properties of BMPs make them interesting candidates to promote bone formation in rehabilitation of partially or completely edentulous patients with severe
Chapter 2

27
maxillary or mandibular atrophy. Favorable regenerative responses to the graft materials containing BMPs in MSFE procedures have been reported.11, 15, 22 BMP-2, BMP-7, and bone morphogenetic protein-14 (BMP-14, known as growth and differentiation factor-5) have been applied in MSFE procedures75, 79, 80, 83, 109 (Table 3). Only recombinant human bone morphogenetic protein-2 (rhBMP-2) and recombinant human bone morphogenetic protein-7 (rhBMP-7) are approved by the food and drug administration (FDA) as medical device.108 Although FDA approval is limited to few orthopaedic applications, other (off-label) applications are considered safe, and may warrant the use of rhBMP-2 and rhBMP-7 clinically in MSFE procedures.
Bone morphogenetic protein-7There are contradictory reports concerning osteoinduction of osteoprogenitor cells by BMP-7. Some studies suggest that BMP-7 is osteoinductive,38, 110 while others suggest that BMP-7 stimulates chondrogenesis.5 This is in contrast to the stimulatory effect of BMP-2 on osteogenic differentiation of progenitor cells.5, 85, 111 BMP-7 applied in MSFE procedure induces bone regeneration.80, 112 However, the use of BMP-7 is associated with swelling and the presence of some granular tissue, which could indicate an inflammatory response.80 This is likely due to the putty component of the BMP-7 preparation which recruits multinucleated giant cells.113
Bone morphogenetic protein-2BMP-2 is a potent osteoinductive molecule that has been shown to increase and speed up osteogenic differentiation, and induce healing of intrabony periodontal defects as well as critical size defects in animals.82, 86, 105, 114 BMP-2 applied to osteoprogenitor cells5, 115, 116 and/or to osteoconductive scaffolds22, 43, 76, 81-86, 105, 114 stimulates osteogenic differentiation in vitro and accelerates bone healing and new bone formation in vivo (Table 3). Carriers combined with BMP-2 have also been shown to induce bone formation when applied in MSFE in sheep,85 rabbit,43, 76,
84 and pig,81 as well as in healing of critical-sized calvarial defects in rats86 and periodontal defects in dogs.82 In an in vivo study in rats using a femoral osteotomy model, a 2 mm femoral gap stabilised by an external fixator device failed to heal within 6 weeks, whereas local application of rhBMP-2 within a blood clot showed proper bone healing with bony bridging.117 This indicates that BMP-2 stimulates osteogenic differentiation of osteoprogenitor cells and might be beneficial for clinical application. The dose of growth factor is also an important issue to take into account in clinical applications. It has been shown that incubation with only 10 ng/ml BMP-2 during 15 min is enough to stimulate osteogenic differentiation of goat derived ASCs.5 This dose of the growth factor is magnitudes lower than the concentration of BMP used in in vivo and clinical studies (0.2–2,5 mg/ml carrier), and may avoid side effects of using mg-range concentrations, such as swelling, ankylosis and calcified seromas, as observed in some studies.80-83, 114,118 It would also avoid the high costs of using high BMP-2 concentrations. BMP-2 supplementation at a low concentration (10 ng/ml) may help to maintain the viability of endothelial cells,100 as well as ASCs (Overman and Farré-Guasch, submitted). Moreover, this rather low and short incubation with BMP-2 could easily fit within a one-step surgical procedure, where autologous stem cells are isolated, triggered with growth factors, and immediately used for bone regeneration within the
Human MSFE as a model for bone regeneration

28
Chapter 2
Table 3. (Pre)clinical in vivo studies combining growth factors with mesenchymal stem cells and/or scaffolds for oral and maxillofacial bone tissue engineering applications in human and animal models: bone volume measurements.
Calvarial defects were critical-sized. ABB, anorganic bovine bone; CaP, calcium phosphate; ß-TCP, ß-Tricalcium phosphate; PLA, polylactic acid; PLGA, polylactic-coglycolide copolymers; BM-MSCs, bone marrow-derived mesenchymal stem cells; BMP-2, bone morphogenetic protein-2; BMP-7, bone morphogenetic protein-7; PDGF, platelet-derived growth factor; VEGF, vascular endothelial growth factor, PDGF, platelet-derived growth factor; PRP, platelet-rich plasma; GDF-5, growth and differentiation factor-5; FGF-2, fibroblast growth factor-2; MSFE, maxillary sinus floor elevation. n.a.; not available.
same surgical procedure (Figure 1).4, 5
One-step Surgical Procedure Approach for Maxillary Sinus Floor ElevationThe stromal vascular fraction (SVF), obtained after collagenase digestion and centrifugation of adipose tissue, has potential for bone tissue engineering, since it contains ASCs with osteogenic potential, among other cell populations.62, 119, 120 For clinical application it would be advantageous to transplant the whole SVF, thereby avoiding expensive and time-consuming in vitro selection and/or expansion steps, loss of differentiation potential, and the risk of contamination. Additionally, the harvesting of human adipose tissue by liposuction is an easy and safe procedure, unlike the harvesting of human bone marrow, which is associated with donor site morbidity.44 Most studies have been performed on cultured ASCs, but before being used clinically, they must overcome

29
prohibitively expensive good manufacturing practice production facilities.55 In addition FDA approval in the USA, or European Agency for the Evaluation of Medicinal Products approval in Europe, is required before use. These limitations hamper the use of cultured stem cells for clinical use. However, using uncultured ASCs in the form of SVF produced via CE-marked devices would overcome at least several of these restrictions.121-123
ASCs in SVF act in coordination with blood cells such as endothelial cells and hematopoietic cells, regulating their undifferentiated state as occurs in the perivascular niche.124 These cells secrete factors that increase proliferation of progenitor cells, such as ASCs, and enhance their osteogenic potential.125 When SVF was co-transplanted on calcium phosphate scaffolds subcutaneously in mice, vascular number and diameter and ectopic mineralization was increased. Therefore, vasculogenesis and osteogenesis may be improved by a synergistic action of ASCs with (pre)vascular cells present in the SVF.126 The synergistic actions of (pre)vascular cells and MSCs may provide an alternative approach for the regeneration of vascular tissues such as bone, where an adequate vascularization is pivotal in effective cell-based bone tissue engineering. For a one-step surgical procedure in MSFE an appropriate amount of adipose tissue would be obtained from the patient. Most patients have an adequate supply of adipose tissue that can be obtained by liposuction using local anesthetics, and the SVF obtained from adipose tissue is a rich source of ASCs readily available for immediate clinical application.121 The freshly isolated SVF can be shortly stimulated with growth factors such as BMP-2 before seeding the stimulated cells onto a carrier material.5 After a short attachment period,127 the tissue-engineered construct is implanted immediately in the patient.4 The feasibility of a one-step procedure relies on the ability of the ASC fraction within the SVF to attach to a scaffold material in sufficient quantities and within a short time frame, which was recently demonstrated to occur. Moreover, it was shown that multidifferentiation potential was maintained, thus likely enhancing angiogenesis and osteogenesis and final clinical outcome.127
Summary and Future DirectionsA cell-based bone tissue engineering approach using stem cells combined with an osteoconductive scaffold and growth factors that stimulate osteogenesis and angiogenesis may become an interesting alternative to the conventional MSFE procedure using autologous bone. Future directions in tissue engineering for MSFE should consider: 1. The need to find the appropriate scaffold for cell-based tissue engineering in MSFE. Calcium phosphate ceramic scaffolds have been widely used in MSFE and support attachment, proliferation, and promote differentiation of osteoprogenitor cells. 2. The appropriate source of stem cells as well as the cell dose to be used in MSFE and study scaffold-cell interactions. The SVF obtained from adipose tissue contains, amongst other cell types, a relatively large number of freshly isolated cells with angiogenic and osteogenic potential, required for vascularisation and osteogenesis in the tissue engineered construct. 3. The delivery method and the appropriate dose of growth factors, such as BMP-2, are critical issues to be considered to enhance bone formation in MSFE. A short (minutes) incubation with a low dose of BMP-2 of 10 ng/ml may avoid the side effects of higher concentrations seen
Human MSFE as a model for bone regeneration

30
in clinical studies, which are shown to be dose-dependent, and may be enough to stimulate an osteogenic response in ASCs. 4. New bone tissue engineering cellular therapeutic approaches have to be evaluated in phase I-IV clinical trials that meet the ATMP Regulation 1394/2007/EC and/or FDA regulations, as well as (local) rules and good clinical practice (GCP) guidelines. In summary, previous studies have shown the importance of scaffolds and growth factors, together with the appropriate source of stem cells, in bone tissue engineering, and have highlighted the need to find an appropriate model for clinical applications. Human MSFE may be a valid model to test bone tissue engineering approaches in a one-step surgical procedure for later use in other surgical disciplines. The comparison of large numbers of patients treated with scaffolds differing in their properties in combination with different cell types and numbers, which are either or not stimulated with different doses of growth factors, will provide critical evidence for future meta-analysis evaluating the safety, efficacy, and outcome measures of clinical trials using new bone tissue engineering approaches.
Chapter 2

31
Human MSFE as a model for bone regeneration
REFERENCES
1.
2.
3.
4.
5.
6.7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
Diaz-Romeral-Bautista, M., Manchon-Miralles, A., Asenjo-Cabezon, J., Cebrian-Carretero, J.L., Torres-Garcia-Denche, J., and Linares-Garcia-Valdecasas, R. Autogenous calvarium bone grafting as a treatment for severe bone resorption in the upper maxilla: a case report. Med Oral Patol Oral Cir Bucal 15, e361, 2010.Hieu, P.D., Chung, J.H., Yim, S.B., and Hong, K.S. A radiographical study on the changes in height of grafting materials after sinus lift: a comparison between two types of xenogenic materials. J Periodontol Implant Sci 40, 25, 2010.Wallace, S.S., and Froum, S.J. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol 8, 328, 2003.Helder, M.N., Knippenberg, M., Klein-Nulend, J., and Wuisman, P.I. Stem cells from adipose tissue allow challenging new concepts for regenerative medicine. Tissue Eng 13, 1799, 2007.Knippenberg, M., Helder, M.N., Zandieh Doulabi, B., Wuisman, P.I., and Klein-Nulend, J. Osteogenesis versus chondrogenesis by BMP-2 and BMP-7 in adipose stem cells. Biochem Biophys Res Commun 342, 902, 2006.Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dental Clin North Am 30, 207, 1986.Boyne, P.J., and James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg 38, 613, 1980.Groeneveld, E.H., van den Bergh, J.P., Holzmann, P., ten Bruggenkate, C.M., Tuinzing, D.B., and Burger, E.H. Mineralization processes in demineralized bone matrix grafts in human maxillary sinus floor elevations. J Biomed Mater Res 48, 393, 1999.Esposito, M., Grusovin, M.G., Rees, J., Karasoulos, D., Felice, P., Alissa, R., Worthington, H.V., and Coulthard, P. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev 17 CD008397, 2010.Zijderveld, S.A., Zerbo, I.R., van den Bergh, J.P., Schulten, E.A., and ten Bruggenkate, C.M. Maxillary sinus floor augmentation using a beta-tricalcium phosphate (Cerasorb) alone compared to autogenous bone grafts. Int J Oral Maxillofac Implants 20, 432, 2005.Browaeys, H., Bouvry, P., and De Bruyn, H. A literature review on biomaterials in sinus augmentation procedures. Clin Implant Dent Relat Res 9, 166, 2007.Klijn, R.J., Meijer, G.J., Bronkhorst, E.M., and Jansen, J.A. A meta-analysis of histomorphometric results and graft healing time of various biomaterials compared to autologous bone used as sinus floor augmentation material in humans. Tissue Eng Part B Rev 16, 493, 2010.Schmitt, C.M., Doering, H., Schmidt, T., Lutz, R., Neukam, F.W., and Schlegel, K.A. Histological results after maxillary sinus augmentation with Straumann® BoneCeramic, Bio-Oss®, Puros®, and autologous bone. A randomized controlled clinical trial. Clin Oral Implants Res, 2012.Ellis, E.E. Surgical reconstruction of defects of the jaws. In: Peterson, J.R., Ellis, E.E., Hupp, J.R., and Tucker, M.R., eds. Contemporary Oral and Maxillofacial Surgery. St Louis, MO: Mosby Inc., 2003, pp. 646-651.Esposito, M., Grusovin, M.G., Coulthard, P., and Worthington, H.V. The efficacy of various bone augmentation procedures for dental implants: a Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants 21, 696, 2006.Cordaro, L., Bosshardt, D.D., Palattella, P., Rao, W., Serino, G., and Chiapasco, M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: histomorphometric results from a randomized controlled multicenter clinical trial. Clin Oral Implants Res 19, 796, 2008.Sohn, D.S., Kim, W.S., An, K.M., Song, K.J., Lee, J.M., and Mun, Y.S. Comparative histomorphometric analysis of maxillary sinus augmentation with and without bone grafting in rabbit. Implant Dent 19, 259, 2010.

32
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.33.
34.
35.
Mummaneni, P.V., Meyer, S.A., and Wu, J.C. Biological approaches to spinal instrumentation and fusion in spinal deformity surgery. Clin Neurosurg 58, 110, 2011.Matsushima, A., Kotobuki, N., Tadokoro, M., Kawate, K., Yajima, H., Takakura, Y., and Ohgushi, H. In vivo osteogenic capability of human mesenchymal cells cultured on hydroxyapatite and on beta-tricalcium phosphate. Artif Organs 33, 474, 2009.Park, J.B. Use of cell-based approaches in maxillary sinus augmentation procedures. J Craniofac Surg 21, 557, 2010.Schmelzeisen, R., Schimming, R., and Sittinger, M. Making bone: implant insertion into tissue-engineered bone for maxillary sinus floor augmentation-a preliminary report. J Craniomaxillofac Surg 31, 34, 2003.Mesimaki, K., Lindroos, B., Tornwall, J., Mauno, J., Lindqvist, C., Kontio, R., Miettinen, S., and Suuronen, R. Novel maxillary reconstruction with ectopic bone formation by GMP adipose stem cells. Int J Oral Maxillofac Surg 38, 201, 2009.Shayesteh, Y.S., Khojasteh, A., Soleimani, M., Alikhasi, M., Khoshzaban, A., and Ahmadbeigi, N. Sinus augmentation using human mesenchymal stem cells loaded into a beta-tricalcium phosphate/hydroxyapatite scaffold. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106, 203, 2008.Zerbo, I.R., de Lange, G.L., Joldersma, M., Bronckers, A.L., and Burger, E.H. Fate of monocortical bone blocks grafted in the human maxilla: a histological and histomorphometric study. Clin Oral Implants Res 14, 759, 2003.Frenken, J.W., Bouwman, W.F., Bravenboer, N., Zijderveld, S.A., Schulten, E.A., and ten Bruggenkate, C.M. The use of Straumann Bone Ceramic in a maxillary sinus floor elevation procedure: a clinical, radiological, histological and histomorphometric evaluation with a 6-month healing period. Clin Oral Implants Res 21, 201, 2010.Iezzi, G., Degidi, M., Piattelli, A., Mangano, C., Scarano, A., Shibli, J.A., and Perrotti, V. Comparative histological results of different biomaterials used in sinus augmentation procedures: a human study at 6 months. Clin Oral Implants Res, 2011.Tosta, M., Cortes, A.R., Correa, L., Pinto, D.D., Jr., Tumenas, I., and Katchburian, E. Histologic and histomorphometric evaluation of a synthetic bone substitute for maxillary sinus grafting in humans. Clin Oral Implants Res, 2011.Mazor, Z., Horowitz, R.A., Del Corso, M., Prasad, H.S., Rohrer, M.D., and Dohan Ehrenfest, D.M. Sinus floor augmentation with simultaneous implant placement using Choukroun’s platelet-rich fibrin as the sole grafting material: a radiologic and histologic study at 6 months. J Periodontol 80, 2056, 2009.Cabbar, F., Guler, N., Kurkcu, M., Iseri, U., and Sencift, K. The effect of bovine bone graft with or without platelet-rich plasma on maxillary sinus floor augmentation. J Oral Maxillofac Surg 69, 2537, 2011.Huang, S.C., Wu, T.C., Yu, H.C., Chen, M.R., Liu, C.M., Chiang, W.S., and Lin, K.M. Mechanical strain modulates age-related changes in the proliferation and differentiation of mouse adipose-derived stromal cells. BMC Cell Biol 11, 18, 2010.Friedenstein, A.J., Piatetzky-Shapiro, II, and Petrakova, K.V. Osteogenesis in transplants of bone marrow cells. J Embryol Exp Morphol 16, 381, 1966.Caplan, A.I. Mesenchymal stem cells. J Orthop Res 9, 641, 1991.Pittenger, M.F., Mackay, A.M., Beck, S.C., Jaiswal, R.K., Douglas, R., Mosca, J.D., Moorman, M.A., Simonetti, D.W., Craig, S., and Marshak, D.R. Multilineage potential of adult human mesenchymal stem cells. Science 284, 143, 1999.Chen, C.H., Wei, H.J., Lin, W.W., Chiu, I., Hwang, S.M., Wang, C.C., Lee, W.Y., Chang, Y., and Sung, H.W. Porous tissue grafts sandwiched with multilayered mesenchymal stromal cell sheets induce tissue regeneration for cardiac repair. Cardiovasc Res 80, 88, 2008.Koga, H., Muneta, T., Nagase, T., Nimura, A., Ju, Y.J., Mochizuki, T., and Sekiya, I. Comparison of mesenchymal tissues-derived stem cells for in vivo chondrogenesis: suitable conditions for cell therapy of cartilage defects in rabbit. Cell Tissue Res 333, 207, 2008.
Chapter 2

33
Human MSFE as a model for bone regeneration
36.
37.
38.39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
Dominici, M., Le Blanc, K., Mueller, I., Slaper-Cortenbach, I., Marini, F., Krause, D., Deans, R., Keating, A., Prockop, D., and Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 8, 315, 2006.Szpalski, C., Barbaro, M., Sagebin, F., and Warren, S.M. Bone Tissue Engineering: Current Strategies and Techniques-Part II: Cell Types. Tissue Eng Part B Rev, 2012.Caplan, A.I. Why are MSCs therapeutic? New data: new insight. J Pathol 217, 318, 2009.Sun, X., Zhang, Z.Y., Wang, S.Y., Gittens, S.A., Jiang, X.Q., and Chou, L.L. Maxillary sinus floor elevation using a tissue-engineered bone complex with OsteoBone and bMSCs in rabbits. Clin Oral Implants Res 19, 804, 2008.Zeng, D., Xia, L., Zhang, W., Huang, H., Wei, B., Huang, Q., Wei, J., Liu, C., and Jiang, X. Maxillary sinus floor elevation using a tissue-engineered bone with calcium-magnesium phosphate cement and bone marrow stromal cells in rabbits. Tissue Eng Part A 18, 870, 2012.Zou, D., Guo, L., Lu, J., Zhang, X., Wei, J., Liu, C., Zhang, Z., and Jiang, X. Engineering of bone using porous calcium phosphate cement and bone marrow stromal cells for maxillary sinus augmentation with simultaneous implant placement in goats. Tissue Eng Part A, 2012 (in press).Khojasteh, A., Eslaminejad, M.B., and Nazarian, H. Mesenchymal stem cells enhance bone regeneration in rat calvarial critical size defects more than platelete-rich plasma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106, 356, 2008.Xia, L., Xu, Y., Wei, J., Zeng, D., Ye, D., Liu, C., Zhang, Z., and Jiang, X. Maxillary sinus floor elevation using a tissue-engineered bone with rhBMP-2-loaded porous calcium phosphate cement scaffold and bone marrow stromal cells in rabbits. Cells Tissues Organs 194, 481, 2011.Kennedy, G.A., Morton, J., Western, R., Butler, J., Daly, J., and Durrant, S. Impact of stem cell donation modality on normal donor quality of life: a prospective randomized study. Bone Marrow Transplant 31, 1033, 2003.Rubio, D., Garcia-Castro, J., Martin, M.C., de la Fuente, R., Cigudosa, J.C., Lloyd, A.C., and Bernad, A. Spontaneous human adult stem cell transformation. Cancer Res 65, 3035, 2005.Izadpanah, R., Kaushal, D., Kriedt, C., Tsien, F., Patel, B., Dufour, J., and Bunnell, B.A. Long-term in vitro expansion alters the biology of adult mesenchymal stem cells. Cancer Res 68, 4229, 2008.Madonna, R., and De Caterina, R. In vitro neovasculogenic potential of resident adipose tissue precursors. Am J Physiol Cell Physiol 295, C1271, 2008.Zuk, P.A., Zhu, M., Mizuno, H., Huang, J., Futrell, J.W., Katz, A.J., Benhaim, P., Lorenz, H.P., and Hedrick, M.H. Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng 7, 211, 2001.Mitchell, J.B., McIntosh, K., Zvonic, S., Garrett, S., Floyd, Z.E., Kloster, A., Di Halvorsen, Y., Storms, R.W., Goh, B., Kilroy, G., Wu, X., and Gimble, J.M. Immunophenotype of human adipose-derived cells: temporal changes in stromal-associated and stem cell-associated markers. Stem Cells 24, 376, 2006.Zuk, P.A., Zhu, M., Ashjian, P., De Ugarte, D.A., Huang, J.I., Mizuno, H., Alfonso, Z.C., Fraser, J.K., Benhaim, P., and Hedrick, M.H. Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell 13, 4279, 2002.Ikegame, Y., Yamashita, K., Hayashi, S., Mizuno, H., Tawada, M., You, F., Yamada, K., Tanaka, Y., Egashira, Y., Nakashima, S., Yoshimura, S., and Iwama, T. Comparison of mesenchymal stem cells from adipose tissue and bone marrow for ischemic stroke therapy. Cytotherapy 13, 675, 2011.Miranville, A., Heeschen, C., Sengenes, C., Curat, C.A., Busse, R., and Bouloumie, A. Improvement of postnatal neovascularization by human adipose tissue-derived stem cells. Circulation 110, 349, 2004.Rubina, K., Kalinina, N., Efimenko, A., Lopatina, T., Melikhova, V., Tsokolaeva, Z., Sysoeva, V., Tkachuk, V., and Parfyonova, Y. Adipose stromal cells stimulate angiogenesis via promoting progenitor cell differentiation, secretion of angiogenic factors, and enhancing vessel maturation. Tissue Eng Part A 15, 2039, 2009.Varma, M.J., Breuls, R.G., Schouten, T.E., Jurgens, W.J., Bontkes, H.J., Schuurhuis, G.J., van Ham, S.M., and van Milligen, F.J. Phenotypical and functional characterization of freshly isolated adipose tissue-derived stem cells. Stem Cells Dev 16, 91, 2007.

34
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
Gimble, J.M., Bunnell, B.A., Chiu, E.S., and Guilak, F. Concise review: Adipose-derived stromal vascular fraction cells and stem cells: let’s not get lost in translation. Stem Cells 29, 749, 2011.Traktuev, D.O., Merfeld-Clauss, S., Li, J., Kolonin, M., Arap, W., Pasqualini, R., Johnstone, B.H., and March, K.L. A population of multipotent CD34-positive adipose stromal cells share pericyte and mesenchymal surface markers, reside in a periendothelial location, and stabilize endothelial networks. Circ Res 102, 77, 2008.Pieri, F., Lucarelli, E., Corinaldesi, G., Aldini, N.N., Fini, M., Parrilli, A., Dozza, B., Donati, D., and Marchetti, C. Dose-dependent effect of adipose-derived adult stem cells on vertical bone regeneration in rabbit calvarium. Biomaterials 31, 3527, 2010.Levi, B., James, A.W., Nelson, E.R., Peng, M., Wan, D.C., Commons, G.W., Lee, M., Wu, B., and Longaker, M.T. Acute skeletal injury is necessary for human adipose-derived stromal cell-mediated calvarial regeneration. Plast Reconstr Surg 127, 1118, 2011.Di Bella, C., Farlie, P., and Penington, A.J. Bone regeneration in a rabbit critical-sized skull defect using autologous adipose-derived cells. Tissue Eng Part A 14, 483, 2008.Cowan, C.M., Shi, Y.Y., Aalami, O.O., Chou, Y.F., Mari, C., Thomas, R., Quarto, N., Contag, C.H., Wu, B., and Longaker, M.T. Adipose-derived adult stromal cells heal critical-size mouse calvarial defects. Nature Biotechnol 22, 560, 2004.Rhee, S.C., Ji, Y.H., Gharibjanian, N.A., Dhong, E.S., Park, S H., and Yoon, E.S. In vivo evaluation of mixtures of uncultured freshly isolated adipose-derived stem cells and demineralized bone matrix for bone regeneration in a rat critically sized calvarial defect model. Stem Cells Dev 20, 233, 2011.Lendeckel, S., Jodicke, A., Christophis, P., Heidinger, K., Wolff, J., Fraser, J.K., Hedrick, M.H., Berthold, L., and Howaldt, H.P. Autologous stem cells (adipose) and fibrin glue used to treat widespread traumatic calvarial defects: case report. J Craniomaxillofac Surg 32, 370, 2004.Kuboki, Y., Jin, Q., and Takita, H. Geometry of carriers controlling phenotypic expression in BMP-induced osteogenesis and chondrogenesis. J Bone Joint Surg Am 83-A Suppl 1, S105, 2001.Salgado, A.J., Coutinho, O.P., and Reis, R.L. Bone tissue engineering: state of the art and future trends. Macromol Biosci 4, 743, 2004.Haimi, S., Suuriniemi, N., Haaparanta, A.M., Ella, V., Lindroos, B., Huhtala, H., Raty, S., Kuokkanen, H., Sandor, G.K., Kellomaki, M., Miettinen, S., and Suuronen, R. Growth and osteogenic differentiation of adipose stem cells on PLA/bioactive glass and PLA/beta-TCP scaffolds. Tissue Eng Part A 15, 1473, 2009.Hao, W., Pang, L., Jiang, M., Lv, R., Xiong, Z., and Hu, Y.Y. Skeletal repair in rabbits using a novel biomimetic composite based on adipose-derived stem cells encapsulated in collagen I gel with PLGA-beta-TCP scaffold. J Orthop Res 28, 252, 2010.Wang, L., Dormer, N.H., Bonewald, L.F., and Detamore, M.S. Osteogenic differentiation of human umbilical cord mesenchymal stromal cells in polyglycolic acid scaffolds. Tissue Eng Part A 16, 1937, 2010.Fabbri, P., Bondioli, F., Messori, M., Bartoli, C., Dinucci, D., and Chiellini, F. Porous scaffolds of polycaprolactone reinforced with in situ generated hydroxyapatite for bone tissue engineering. J Mater Sci Mater Med 21, 343, 2010.Kakudo, N., Shimotsuma, A., Miyake, S., Kushida, S., and Kusumoto, K. Bone tissue engineering using human adipose-derived stem cells and honeycomb collagen scaffold. J Biomed Mater Res A 84, 191, 2008.Manferdini, C., Guarino, V., Zini, N., Raucci, M.G., Ferrari, A., Grassi, F., Gabusi, E., Squarzoni, S., Facchini, A., Ambrosio, L., and Lisignoli, G. Mineralization behavior with mesenchymal stromal cells in a biomimetic hyaluronic acid-based scaffold. Biomaterials 31, 3986, 2010.Ahmed, T.A., Dare, E.V., and Hincke, M. Fibrin: a versatile scaffold for tissue engineering applications. Tissue Eng Part B Rev 14, 199, 2008.Kim, H.J., Kim, U.J., Kim, H.S., Li, C., Wada, M., Leisk, G.G., and Kaplan, D.L. Bone tissue engineering with premineralized silk scaffolds. Bone 42, 1226, 2008.
Chapter 2

35
Human MSFE as a model for bone regeneration
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
Haimi, S., Moimas, L., Pirhonen, E., Lindroos, B., Huhtala, H., Raty, S., Kuokkanen, H., Sandor, G.K., Miettinen, S., and Suuronen, R. Calcium phosphate surface treatment of bioactive glass causes a delay in early osteogenic differentiation of adipose stem cells. J Biomed Mater Res A 91, 540, 2009.Zijderveld, S.A., Schulten, E.A., Aartman, I.H., and ten Bruggenkate, C.M. Long-term changes in graft height after maxillary sinus floor elevation with different grafting materials: radiographic evaluation with a minimum follow-up of 4.5 years. Clin Oral Implants Res 20, 691, 2009.Stavropoulos, A., Becker, J., Capsius, B., Acil, Y., Wagner, W., and Terheyden, H. Histological evaluation of maxillary sinus floor augmentation with recombinant human growth and differentiation factor-5-coated beta-tricalcium phosphate: results of a multicenter randomized clinical trial. J Clin Periodontol 38, 966, 2011.Xia, L., Xu, Y., Chang, Q., Sun, X., Zeng, D., Zhang, W., Zhang, X., Zhang, Z., and Jiang, X. Maxillary sinus floor elevation using BMP-2 and Nell-1 gene-modified bone marrow stromal cells and TCP in rabbits. Calcif Tissue Int 89, 53, 2011.Boeck-Neto, R.J., Artese, L., Piattelli, A., Shibli, J.A., Perrotti, V., Piccirilli, M., and Marcantonio, E., Jr. VEGF and MVD expression in sinus augmentation with autologous bone and several graft materials. Oral Dis 15, 148, 2009.Scarano, A., Degidi, M., Iezzi, G., Pecora, G., Piattelli, M., Orsini, G., Caputi, S., Perrotti, V., Mangano, C., and Piattelli, A. Maxillary sinus augmentation with different biomaterials: a comparative histologic and histomorphometric study in man. Implant Dent 15, 197, 2006.Koch, F.P., Becker, J., Terheyden, H., Capsius, B., and Wagner, W.A prospective, randomized pilot study on the safety and efficacy of recombinant human growth and differentiation factor-5 coated onto beta-tricalcium phosphate for sinus lift augmentation. Clin Oral Implants Res 21, 1301, 2010.van den Bergh, J.P., ten Bruggenkate, C.M., Groeneveld, H.H., Burger, E.H., and Tuinzing, D.B. Recombinant human bone morphogenetic protein-7 in maxillary sinus floor elevation surgery in 3 patients compared to autogenous bone grafts. A clinical pilot study. J Clin Periodontol 27, 627, 2000.Lee, J., Susin, C., Rodriguez, N.A., de Stefano, J., Prasad, H.S., Buxton A.N., and Wikesjö, U.M. Sinus augmentation using rhBMP-2/ACS in a mini-pig model: relative efficacy of autogenous fresh particulate iliac bone grafts. Clin Oral Implants Res, 2012.Choi, S.H., Kim, C.K., Cho, K.S., Huh, J.S., Sorensen, R.G., Wozney, J.M., and Wikesjo, U.M. Effect of recombinant human bone morphogenetic protein-2/absorbable collagen sponge (rhBMP-2/ACS) on healing in 3-wall intrabony defects in dogs. J Periodontol 73, 63, 2002.Triplett, R.G., Nevins, M., Marx, R.E., Spagnoli, D.B., Oates, T.W., Moy, P.K., and Boyne, P.J. Pivotal, randomized, parallel evaluation of recombinant human bone morphogenetic protein-2/absorbable collagen sponge and autogenous bone graft for maxillary sinus floor augmentation. J Oral Maxillofac Surg 67, 1947, 2009.Zhang, W., Wang, X., Wang, S., Zhao, J., Xu, L., Zhu, C., Zeng, D., Chen, J., Zhang, Z., Kaplan, D.L., and Jiang, X. The use of injectable sonication-induced silk hydrogel for VEGF(165) and BMP-2 delivery for elevation of the maxillary sinus floor. Biomaterials 32, 9415, 2011.Gutwald, R., Haberstroh, J., Stricker, A., Ruther, E., Otto, F., Xavier, S.P., Oshima, T., Marukawa, E., Seto, I., Enomoto, S., Hoogendijk, C.F., Schmelzeisen, R., and Sauerbier, S. Influence of rhBMP-2 on bone formation and osseointegration in different implant systems after sinus-floor elevation. An in vivo study on sheep. J Craniomaxillofac Surg 38, 571, 2010.Schofer, M.D., Roessler, P.P., Schaefer, J., Theisen, C., Schlimme, S., Heverhagen, J.T., Voelker, M., Dersch, R., Agarwal, S., Fuchs-Winkelmann, S., and Paletta, J.R. Electrospun PLLA nanofiber scaffolds and their use in combination with BMP-2 for reconstruction of bone defects. PLoS One 6, e25462, 2011.Trindade-Suedam, I.K., de Morais, J.A., Faeda, R.S., Leite, F.R., Tosoni, G.M., Neto, C.B., Marcantonio, E., Jr., and Scaf, G. Bioglass associated with leukocyte-poor platelet-rich plasma in the rabbit maxillary sinus: histomorphometric, densitometric, and fractal analysis. J Oral Implantol 36, 333, 2010.

36
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.98.99.
100.
101.
102.
103.
104.
105.
106.
107.
Stavropoulos, A., Sima, C., Sima, A., Nyengaard, J., Karring, T., and Sculean, A. Histological evaluation of healing after transalveolar maxillary sinus augmentation with bioglass and autogenous bone. Clin Oral Implants Res 23, 125, 2012.Lee, J.H., Jung, U.W., Kim, C.S., Choi, S.H., and Cho, K.S. Histologic and clinical evaluation for maxillary sinus augmentation using macroporous biphasic calcium phosphate in human. Clin Oral Implants Res 19, 767, 2008.Zerbo, I.R., Bronckers, A.L., de Lange, G., and Burger, E.H. Localisation of osteogenic and osteoclastic cells in porous beta-tricalcium phosphate particles used for human maxillary sinus floor elevation. Biomaterials 26, 1445, 2005.E, L.L., Xu, L.L., Wu, X., Wang, D.S., Lv, Y., Wang, J.Z., and Liu, H.C. The interactions between rat-adipose-derived stromal cells, recombinant human bone morphogenetic protein-2, and beta-tricalcium phosphate play an important role in bone tissue engineering. Tissue Eng Part A 16, 2927, 2010.Guha, A.K., Singh, S., Kumaresan, R., Nayar, S., and Sinha, A. Mesenchymal cell response to nanosized biphasic calcium phosphate composites. Colloids Surf B Biointerfaces 73, 146, 2009.Saldana, L., Sanchez-Salcedo, S., Izquierdo-Barba, I., Bensiamar, F., Munuera, L., Vallet-Regi, M., and Vilaboa, N. Calcium phosphate-based particles influence osteogenic maturation of human mesenchymal stem cells. Acta Biomater 5, 1294, 2009.Friedmann, A., Dard, M., Kleber, B.M., Bernimoulin, J.P., and Bosshardt, D.D. Ridge augmentation and maxillary sinus grafting with a biphasic calcium phosphate: histologic and histomorphometric observations. Clin Oral Implants Res 20, 708, 2009.Detsch, R., Schaefer, S., Deisinger, U., Ziegler, G., Seitz, H., and Leukers, B. In vitro: osteoclastic activity studies on surfaces of 3D printed calcium phosphate scaffolds. J Biomater Appl 26, 359, 2011.Blattert, T.R., Jestaedt, L., and Weckbach, A. Suitability of a calcium phosphate cement in osteoporotic vertebral body fracture augmentation: a controlled, randomized, clinical trial of balloon kyphoplasty comparing calcium phosphate versus polymethylmethacrylate. Spine (Phila Pa 1976) 34, 108, 2009.Langer, R., and Vacanti, J.P. Tissue engineering. Science 260, 920, 1993.Service, R.F. Tissue engineers build new bone. Science 289, 1498, 2000.Trueta, J., and Buhr, A.J. The vascular contribution to osteogenesis. V. The vasculature supplying the epiphysial cartilage in rachitic rats. J Bone Joint Surg Br 45, 572, 1963.Correia, C., Grayson, W.L., Park, M., Hutton, D., Zhou, B., Guo, X.E., Niklason, L., Sousa, R.A., Reis, R.L., and Vunjak-Novakovic, G. In vitro model of vascularized bone: synergizing vascular development and osteogenesis. PLoS One 6, e28352, 2011.Chang, P.C., Seol, Y.J., Cirelli, J.A., Pellegrini, G., Jin, Q., Franco, L.M., Goldstein, S.A., Chandler, L.A., Sosnowski, B., and Giannobile, W.V. PDGF-B gene therapy accelerates bone engineering and oral implant osseointegration. Gene Ther 17, 95, 2010.Kwan, M.D., Sellmyer, M.A., Quarto, N., Ho, A.M., Wandless, T.J., and Longaker, M.T. Chemical control of FGF-2 release for promoting calvarial healing with adipose stem cells. J Biol Chem 286, 11307, 2011.Ohya, M., Yamada, Y., Ozawa, R., Ito, K., Takahashi, M., and Ueda, M. Sinus floor elevation applied tissue-engineered bone. Comparative study between mesenchymal stem cells/platelet-rich plasma (PRP) and autogenous bone with PRP complexes in rabbits. Clin Oral Implants Res 16, 622, 2005.Wiltfang, J., Schlegel, K.A., Schultze-Mosgau, S., Nkenke, E., Zimmermann, R., and Kessler, P. Sinus floor augmentation with beta-tricalciumphosphate (beta-TCP): does platelet-rich plasma promote its osseous integration and degradation? Clin Oral Implants Res 14, 213, 2003.Behr, B., Sorkin, M., Lehnhardt, M., Renda, A., Longaker, M.T., and Quarto, N.A Comparative Analysis of the Osteogenic Effects of BMP-2, FGF-2, and VEGFA in a Calvarial Defect Model. Tissue Eng Part A 18, 1079, 2012.Roldan, J.C., Knueppel, H., Schmidt, C., Jepsen, S., Zimmermann, C., and Terheyden, H. Single-stage sinus augmentation with cancellous iliac bone and anorganic bovine bone in the presence of platelet-rich plasma in the miniature pig. Clin Oral Implants Res 19, 373, 2008.Tobita, M., and Mizuno, H. Adipose-derived stem cells for periodontal tissue regeneration. Methods Mol Biol 702, 461, 2011.
Chapter 2

37
Human MSFE as a model for bone regeneration
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
Gautschi, O.P., Frey, S.P., and Zellweger, R. Bone morphogenetic proteins in clinical applications. ANZ J Surg 77, 626, 2007.Park, J.B. Use of bone morphogenetic proteins in sinus augmentation procedure. J Craniofac Surg 20, 1501, 2009.Gruber, R., Kandler, B., Fuerst, G., Fischer, M.B., and Watzek, G. Porcine sinus mucosa holds cells that respond to bone morphogenetic protein (BMP)-6 and BMP-7 with increased osteogenic differentiation in vitro. Clin Oral Implants Res 15, 575, 2004.Cowan, C.M., Aalami, O.O., Shi, Y.Y., Chou, Y.F., Mari, C., Thomas, R., Quarto, N., Nacamuli, R.P., Contag, C.H., Wu, B., and Longaker, M.T. Bone morphogenetic protein 2 and retinoic acid accelerate in vivo bone formation, osteoclast recruitment, and bone turnover. Tissue Eng 11, 645, 2005.Ho, S.K., Peel, S.A., Hu, Z.M., Sandor, G.K., and Clokie, C.M. Augmentation of the maxillary sinus: comparison of bioimplants containing bone morphogenetic protein and autogenous bone in a rabbit model. J Can Dent Assoc 76, a108, 2010.Mullender, M.G., Krijnen, M.R., Helder, M.N., Smit, T.H., Everts, V., and Wuisman, P.I. Lumbar body fusion with a bioresorbable cage in a goat model is delayed by the use of a carboxymethylcellulose-stabilized collagenous rhOP-1 device. J Orthop Res 25, 132, 2007.He, D., Genecov, D.G., Herbert, M., Barcelo, R., Elsalanty, M.E., Weprin, B.E., and Opperman, L.A. Effect of recombinant human bone morphogenetic protein-2 on bone regeneration in large defects of the growing canine skull after dura mater replacement with a dura mater substitute. J Neurosurg 112, 319, 2010.Maegawa, N., Kawamura, K., Hirose, M., Yajima, H., Takakura, Y., and Ohgushi, H. Enhancement of osteoblastic differentiation of mesenchymal stromal cells cultured by selective combination of bone morphogenetic protein-2 (BMP-2) and fibroblast growth factor-2 (FGF-2). J Tissue Eng Regen Med 1, 306, 2007.Miyazaki, M., Zuk, P.A., Zou, J., Yoon, S.H., Wei, F., Morishita, Y., Sintuu, C., and Wang, J.C. Comparison of human mesenchymal stem cells derived from adipose tissue and bone marrow for ex vivo gene therapy in rat spinal fusion model. Spine (Phila Pa 1976) 33, 863, 2008.Preininger, B., Gerigk, H., Bruckner, J., Perka, C., Schell, H., Ellinghaus, A., Schmidt-Bleek, K., and Duda, G. An experimental setup to evaluate innovative therapy options for the enhancement of bone healing using BMP as a benchmark - a pilot study. Eur Cell Mater 23, 262, 2012.Carragee, E.J., Hurwitz, E.L., and Weiner, B.K. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J 11, 471, 2011.Elabd, C., Chiellini, C., Massoudi, A., Cochet, O., Zaragosi, L.E., Trojani, C., Michiels, J.F., Weiss, P., Carle, G., Rochet, N., Dechesne, C.A., Ailhaud, G., Dani, C., and Amri, E.Z. Human adipose tissue-derived multipotent stem cells differentiate in vitro and in vivo into osteocyte-like cells. Biochem Biophys Res Commun 361, 342, 2007.Rada, T., Reis, R.L., and Gomes, M.E. Adipose tissue-derived stem cells and their application in bone and cartilage tissue engineering. Tissue Eng Part B Rev 15, 113, 2009.Astori, G., Vignati, F., Bardelli, S., Tubio, M., Gola, M., Albertini, V., Bambi, F., Scali, G., Castelli, D., Rasini, V., Soldati, G., and Moccetti, T. “In vitro” and multicolor phenotypic characterization of cell subpopulations identified in fresh human adipose tissue stromal vascular fraction and in the derived mesenchymal stem cells. J Transl Med 5, 55, 2007.Vidal, M.A., Kilroy, G.E., Lopez, M.J., Johnson, J.R., Moore, R.M., and Gimble, J.M. Characterization of equine adipose tissue-derived stromal cells: adipogenic and osteogenic capacity and comparison with bone marrow-derived mesenchymal stromal cells. Vet Surg 36, 613, 2007.Yoshimura, K., Shigeura, T., Matsumoto, D., Sato, T., Takaki, Y., Aiba-Kojima, E., Sato, K., Inoue, K., Nagase, T., Koshima, I., and Gonda, K. Characterization of freshly isolated and cultured cells derived from the fatty and fluid portions of liposuction aspirates. J Cell Physiol 208, 64, 2006.

38
124.
125.
126.
127.
Mendez-Ferrer, S., Michurina, T.V., Ferraro, F., Mazloom, A.R., Macarthur, B. D., Lira, S.A., Scadden, D.T., Ma’ayan, A., Enikolopov, G.N., and Frenette, P. S. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature 466, 829, 2010.Saleh, F.A., Whyte, M., Ashton, P., and Genever, P.G. Regulation of mesenchymal stem cell activity by endothelial cells. Stem Cells Dev 20, 391, 2011.Moioli, E.K., Clark, P.A., Chen, M., Dennis, J.E., Erickson, H.P., Gerson, S.L., and Mao, J.J. Synergistic actions of hematopoietic and mesenchymal stem/progenitor cells in vascularizing bioengineered tissues. PLoS One 3, e3922, 2008.Jurgens, W.J., Kroeze, R.J., Bank, R.A., Ritt, M.J., and Helder, M.N. Rapid attachment of adipose stromal cells on resorbable polymeric scaffolds facilitates the one-step surgical procedure for cartilage and bone tissue engineering purposes. J Orthop Res 29, 853, 2011.
Chapter 2