Chapter 119 - Allergy, Hypersensitivity, Angioedema, and ... · Allergy, Hypersensitivity,...
17
1543 CHAPTER 119 Allergy, Hypersensitivity, Angioedema, and Anaphylaxis T. Paul Tran and Robert L. Muelleman PERSPECTIVE The human immune system is an assemblage of cellular and humoral components working together in a highly complex, coor- dinated, and elegant fashion to achieve the primary goal of pro- tecting the human host (self) from harmful offenders (nonself). Exposure to danger signals activates the various immune mecha- nisms to bring about immune responses aimed at neutralizing the dangerous nonself while preserving self. 1 The immune system can, however, overreact to otherwise harmless nonself agents, produc- ing inappropriate responses that are harmful to the host, thereby giving rise to allergy or allergic diseases. These hypersensitivity reactions are manifested in clinical symptoms ranging from mildly inconvenient to debilitating to fatal. For practical purposes, the term allergy is used in this chapter to refer to mast cell–mediated hypersensitivity reactions. For most allergic diseases to occur, predisposed individuals need to be exposed to allergens through a process called sensitization. Substances that elicit an allergic reaction are referred to as allergens, and those that elicit an antibody response (activated by B- and T-cell receptors) are called antigens. In this allergic continuum, there are several important allergic syndromes frequently encountered in the emergency department (ED). Urticaria is a common allergic reaction to foods, drugs, or physical stimuli and is clinically characterized by a red itchy rash. Angioedema is the other important allergic syndrome, mediated by either an allergic mechanism in response to exposure to foods, drugs, or physical stimuli or a nonallergic mechanism (e.g., angiotensin-converting enzyme [ACE] inhibitor). Angioedema is characterized by swelling of the subcutaneous tissues, which can cause airway difficulty if the larynx is involved. At the other extreme of this allergic continuum is anaphylaxis, a life-threatening systemic allergic reaction characterized by acute onset and multi- organ involvement. The term anaphylaxis is derived from Greek (ana, against; phylax, guard or protect), meaning “against protec- tion.” Mechanistically, anaphylaxis is a type I hypersensitivity reac- tion (allergic), mediated by immunoglobulin E (IgE). In its most common form, anaphylaxis is precipitated by exposure to aller- gens in previously sensitized individuals. Timely recognition of the syndrome and proper care are essential to bring about benefi- cial outcomes for patients with anaphylaxis. The term anaphylactoid reaction refers to a syndrome clinically similar to anaphylaxis that is not mediated by IgE. Its clinical pre- sentation and treatment are identical to those of anaphylaxis. Ana- phylactoid reactions appear to result from direct degranulation of mast cells (and basophils) and may follow a single, first-time expo- sure to certain inciting agents. In this chapter, we use the term anaphylaxis to refer to both IgE- and non–IgE-mediated reactions, obviating the need for the term anaphylactoid reaction. Epidemiology and Risk Factors The incidence of anaphylaxis has not been determined with cer- tainty, but recent evidence suggests that it is increasing. 2 There are approximately 100,000 attacks of anaphylaxis in the United States per year, of which approximately 60,000 are first-time events and 1000 to 1500 are fatal. 3 Factors affecting the incidence of anaphylaxis include time of the year, age, female sex (adults), higher socioeconomic status, northern locations, route of allergen exposure, and history of atopy (Box 119-1). 2,4 Anaphylactic reactions seem to be more common in the summer and early fall, coincident with the outdoor season; in people of higher socioeconomic status; and in people with a history of atopy. In general, anaphylaxis is more common in adults, but in particular, it is more common in women older than 30 years and in boys younger than 16 years. The dose, fre- quency, duration, and route of administration of a drug also affect the tendency to develop an anaphylactic reaction; the parenteral route is more likely than the oral route to lead to an anaphylactic reaction. One interesting aspect of drug-related anaphylaxis is the constancy of administration. An anaphylactic reaction may not occur in an otherwise susceptible patient as long as a drug is administered at regular intervals. The same patient may, however, experience an anaphylactic reaction if the drug is resumed after an interruption of therapy. 5 Risk factors for increased severity and mortality of an anaphy- laxis reaction include having a recent episode of anaphylaxis, extremes of age, presence of atopy or cardiopulmonary condi- tions, taking medications that may influence timely recognition of the symptoms or impede the treatment of anaphylaxis, and rapid onset of symptoms after exposure (see Box 119-1). 2,6 The more rapid an anaphylaxis reaction is after an exposure, the more likely it is to be severe and potentially fatal. Whereas anaphylaxis in an infant is a rare event, timely recognition of an anaphylactic reac- tion in an infant can be difficult because signs of anaphylaxis, such as flushing, vomiting and diarrhea, lethargy, and dystonia after feeding, can be overlooked as minor reactions. 7 Elders, on the other hand, tend to have worse outcomes in anaphylaxis because of their comorbid conditions, notably heart failure, ischemic heart disease, hypertension, and obstructive lung diseases. A history of asthma and atopy is associated with a more severe or fatal anaphylactic reaction. This is particularly true when the aller- gen is administered by the mucosal route (e.g., food). Atopy does not, however, seem to be a risk factor when the allergen is admin- istered parenterally (e.g., penicillin). Patients with psychiatric dis- orders and individuals taking medications and drugs that may impede prompt recognition of an anaphylaxis reaction are also at increased risks (e.g., recreational drugs, alcohol, tranquilizers, and hypnotics). In addition, two classes of medications concurrently
Transcript of Chapter 119 - Allergy, Hypersensitivity, Angioedema, and ... · Allergy, Hypersensitivity,...
1543
CHAPTER 119
Allergy, Hypersensitivity, Angioedema, and Anaphylaxis
T. Paul Tran and Robert L. Muelleman
PERSPECTIVE
The human immune system is an assemblage of cellular and humoral components working together in a highly complex, coor-dinated, and elegant fashion to achieve the primary goal of pro-tecting the human host (self) from harmful offenders (nonself). Exposure to danger signals activates the various immune mecha-nisms to bring about immune responses aimed at neutralizing the dangerous nonself while preserving self.1 The immune system can, however, overreact to otherwise harmless nonself agents, produc-ing inappropriate responses that are harmful to the host, thereby giving rise to allergy or allergic diseases. These hypersensitivity reactions are manifested in clinical symptoms ranging from mildly inconvenient to debilitating to fatal. For practical purposes, the term allergy is used in this chapter to refer to mast cell–mediated hypersensitivity reactions. For most allergic diseases to occur, predisposed individuals need to be exposed to allergens through a process called sensitization. Substances that elicit an allergic reaction are referred to as allergens, and those that elicit an antibody response (activated by B- and T-cell receptors) are called antigens.
In this allergic continuum, there are several important allergic syndromes frequently encountered in the emergency department (ED). Urticaria is a common allergic reaction to foods, drugs, or physical stimuli and is clinically characterized by a red itchy rash. Angioedema is the other important allergic syndrome, mediated by either an allergic mechanism in response to exposure to foods, drugs, or physical stimuli or a nonallergic mechanism (e.g., angiotensin-converting enzyme [ACE] inhibitor). Angioedema is characterized by swelling of the subcutaneous tissues, which can cause airway difficulty if the larynx is involved. At the other extreme of this allergic continuum is anaphylaxis, a life-threatening systemic allergic reaction characterized by acute onset and multi-organ involvement. The term anaphylaxis is derived from Greek (ana, against; phylax, guard or protect), meaning “against protec-tion.” Mechanistically, anaphylaxis is a type I hypersensitivity reac-tion (allergic), mediated by immunoglobulin E (IgE). In its most common form, anaphylaxis is precipitated by exposure to aller-gens in previously sensitized individuals. Timely recognition of the syndrome and proper care are essential to bring about benefi-cial outcomes for patients with anaphylaxis.
The term anaphylactoid reaction refers to a syndrome clinically similar to anaphylaxis that is not mediated by IgE. Its clinical pre-sentation and treatment are identical to those of anaphylaxis. Ana-phylactoid reactions appear to result from direct degranulation of mast cells (and basophils) and may follow a single, first-time expo-sure to certain inciting agents. In this chapter, we use the term anaphylaxis to refer to both IgE- and non–IgE-mediated reactions, obviating the need for the term anaphylactoid reaction.
Epidemiology and Risk Factors
The incidence of anaphylaxis has not been determined with cer-tainty, but recent evidence suggests that it is increasing.2 There are approximately 100,000 attacks of anaphylaxis in the United States per year, of which approximately 60,000 are first-time events and 1000 to 1500 are fatal.3
Factors affecting the incidence of anaphylaxis include time of the year, age, female sex (adults), higher socioeconomic status, northern locations, route of allergen exposure, and history of atopy (Box 119-1).2,4 Anaphylactic reactions seem to be more common in the summer and early fall, coincident with the outdoor season; in people of higher socioeconomic status; and in people with a history of atopy. In general, anaphylaxis is more common in adults, but in particular, it is more common in women older than 30 years and in boys younger than 16 years. The dose, fre-quency, duration, and route of administration of a drug also affect the tendency to develop an anaphylactic reaction; the parenteral route is more likely than the oral route to lead to an anaphylactic reaction. One interesting aspect of drug-related anaphylaxis is the constancy of administration. An anaphylactic reaction may not occur in an otherwise susceptible patient as long as a drug is administered at regular intervals. The same patient may, however, experience an anaphylactic reaction if the drug is resumed after an interruption of therapy.5
Risk factors for increased severity and mortality of an anaphy-laxis reaction include having a recent episode of anaphylaxis, extremes of age, presence of atopy or cardiopulmonary condi-tions, taking medications that may influence timely recognition of the symptoms or impede the treatment of anaphylaxis, and rapid onset of symptoms after exposure (see Box 119-1).2,6 The more rapid an anaphylaxis reaction is after an exposure, the more likely it is to be severe and potentially fatal. Whereas anaphylaxis in an infant is a rare event, timely recognition of an anaphylactic reac-tion in an infant can be difficult because signs of anaphylaxis, such as flushing, vomiting and diarrhea, lethargy, and dystonia after feeding, can be overlooked as minor reactions.7 Elders, on the other hand, tend to have worse outcomes in anaphylaxis because of their comorbid conditions, notably heart failure, ischemic heart disease, hypertension, and obstructive lung diseases. A history of asthma and atopy is associated with a more severe or fatal anaphylactic reaction. This is particularly true when the aller-gen is administered by the mucosal route (e.g., food). Atopy does not, however, seem to be a risk factor when the allergen is admin-istered parenterally (e.g., penicillin). Patients with psychiatric dis-orders and individuals taking medications and drugs that may impede prompt recognition of an anaphylaxis reaction are also at increased risks (e.g., recreational drugs, alcohol, tranquilizers, and hypnotics). In addition, two classes of medications concurrently

1544 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
more cardiovascular and systemic. Allergic reactions to foodstuffs are more common in children, with incidence ranging from 0.3 to 7.5%.11
Therapeutic and prophylactic use of large quantities of antibi-otics is common in the production of beef cattle, swine, fish, poultry, and sometimes vegetables and fruits. Along with antibiot-ics, sodium and potassium bisulfites and metabisulfites are used as preservatives in foods. Sulfites have been used as antioxidants in the food and restaurant industry to prevent discoloration of vegetables (e.g., salad bars and avocado dips), fruits, and potatoes and to preserve fruit and vegetable juices. They are also used to prevent bacterial contamination and oxidation of wines, beers, and distilled beverages. Sensitivity to ingested sulfites has been well documented, especially among asthmatics.12 Establishment of a particular foodstuff or preservative as the causative agent of anaphylaxis can be difficult.
Antibiotics
Allergic reactions to common antibiotics, such as benzylpenicil-lin, semisynthetic penicillin, and cephalosporins, are well docu-mented; allergy to penicillin is perhaps the most commonly reported medication allergy. Because of their low molecular
taken by patients may increase their risks of anaphylaxis severity. ACE inhibitors can cause an accumulation of kinins and bradyki-nin and thus can exacerbate the angioedema in anaphylaxis. Beta-blockers can oppose the actions of adrenergic agents used in anaphylaxis treatment, potentially leading to protracted hypotension.
Triggers for Anaphylaxis
Virtually any agent that is capable of activating mast cells (or basophils) can potentially precipitate an anaphylactic reaction. In approximately one third of the cases, however, an inciting agent cannot be identified.8 When a cause can be determined, foods, medications, and insect stings are the most common causes of anaphylactic reactions. Box 119-2 lists most common agents by their proposed immunologic mechanism.9 Reactions without identifiable causative agents are classified as physically induced or iatrogenic anaphylaxis.
Foods
Foods are the major identifiable causative agents, accounting for approximately one third of the cases of anaphylaxis.8 A variety of foods have been identified, ranging from the well-known (nuts, shellfish, and eggs) to the obscure (chamomile tea, which may have cross-reactivity with ragweed). Cow’s milk, egg, peanut, soy, wheat, fish, shellfish, and tree nuts are foods that most commonly cause anaphylaxis. Even for a person with a known history of food allergy, it may be difficult to avoid foods that may cause allergic reactions because their identity may be obscured in processing (e.g., consuming wine contaminated with Hymenoptera venom).10 Because allergenic foods are first absorbed transmucosally, symp-toms of food anaphylaxis may first appear localized to the upper airway of the respiratory tract. When anaphylactic allergens are administered parenterally, symptoms of anaphylaxis tend to be
Modified from Lieberman P: Anaphylaxis. Med Clin North Am 90:77-95, 2006, viii; and Simons FE: Anaphylaxis. J Allergy Clin Immunol 125(Suppl 2):S161-S181, 2010.
BOX 119-1
Risk Factors for Having AnaphylaxisAge and sex
Males < 16 years, females > 30 yearsRoute of administration
Parenteral > oralHigher social economic statusTime of the year
Summer and fall (the outdoor seasons)History of atopy
Risk Factors for Increased Anaphylaxis Severity and MortalityExtremes of age
Very young (under-recognition)Elderly (increased risks of mortality from treatment and
venom-induced anaphylaxis)Comorbid conditions
Cardiovascular disease (heart failure, ischemic heart disease, hypertension)
Pulmonary disease (asthma, obstructive airway disease, acute infection)
OthersConcurrent use of beta-blockers and angiotensin-converting
enzyme inhibitorsConcurrent use of cognition-impairing drugs (e.g., alcohol,
recreational drugs, sedatives, tranquilizers)Recent anaphylaxis episode
Risk Factors for Having Anaphylaxis and Increased Anaphylaxis Severity and Mortality
Modified from Kemp SF, Lockey RF: Anaphylaxis: A review of causes and mechanisms. J Allergy Clin Immunol 110:341-348, 2002.
BOX 119-2
IgE-Dependent MechanismFood: egg, peanut, tree nut, milk, fruits, shellfish, shrimp, other
crustaceansAntibiotics: penicillins, cephalosporins, sulfonamides,
nitrofurantoin, tetracycline, streptomycinInsect stings: Hymenoptera venoms, fire ant stingsNatural rubber latexHormones: insulin, methylprednisolone, parathormone,
estradiol, progesterone, corticotropinEnzymes: trypsin, streptokinase, chymotrypsin, chymopapain,
L-asparaginaseOther therapeutics: NSAIDs (some are IgE independent),
methylparaben, human diploid cell rabies vaccine, egg-based vaccines (measles, mumps, rubella), vasopressin, antilymphocyte globulin, heterologous and human sera, local anesthetics (mostly ester family, procaine, tetracaine, benzocaine)
Seminal fluid
IgE-Independent Mechanism (direct mast cell degranulation)Radiocontrast mediaAspirin and NSAIDs (arachidonic acid metabolism)Alcohol, opiates, protamine, polysaccharides (some are IgE
mediated), curare, D-tubocurarineCertain food colorants and additives
Immune Complex MediatedWhole blood (transfusion reaction to formed elements),
immunoglobulins
Physical FactorsExerciseHeat or coldSunlightUltraviolet radiation
MiscellaneousFactitiousUndifferentiated somatoform idiopathic anaphylaxisIdiopathic
Etiologic Agents Causing Anaphylaxis by Immunologic Mechanisms
IgE, immunoglobulin E; NSAIDs, nonsteroidal anti-inflammatory drugs.

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1545
Anesthetic Drugs. Local anesthetics produce occasional adverse reactions.23 Most of these reactions are not allergic in nature but are related to a direct effect of the medication. True allergic reac-tions are uncommon and are most commonly seen with local anesthetics from the ester family (e.g., procaine, tetracaine, and benzocaine). Allergic reactions to local anesthetics belonging to the amide family (e.g., lidocaine, bupivacaine, mepivacaine, and dibucaine) are rare. Multidose vials of lidocaine contain the pre-servative methylparaben, which belongs structurally to the ester family. This preservative has been implicated in allergic reactions in patients with a history of previous lidocaine hypersensitivity.24 Only pure lidocaine (without the methylparaben preservative) should be used in intravenous applications (as in Bier’s block).
Vaccines. Anaphylactic reactions have occurred after the admin-istration of egg embryo–grown vaccines, including the combined measles, mumps, and rubella (MMR), yellow fever, and influenza vaccines. Patients who are able to tolerate eggs orally are likely to tolerate the vaccines.
Blood Products. Anaphylactic-type reactions are an uncommon complication of the administration of whole blood and immuno-globulins. The fixation of antibodies to formed elements such as red blood cells, platelets, and leukocytes and soluble components activates the complement system. This is particularly relevant in IgA-deficient patients exposed to multiple transfusions, who may have produced antibodies to IgA in previous transfusions. With subsequent transfusions, an antigen (IgA)–anti-IgA anti-body (IgG) immune complex forms, leading to subsequent activa-tion of the complement cascade.
Opiates. Many of the opioid analgesics can cause anaphylactic reaction through a direct histamine release mechanism, although some are IgE mediated. It is unclear how much cross-sensitivity is present among these agents.25
weights, these antimicrobials themselves do not possess antigenic properties (they are haptens). They become immunologically active (i.e., elicit an immunologic response) only after they bind to a “carrier” host protein. Although patients often report a history of penicillin allergy, this may not stand up to close scrutiny.13 Studies have shown that up to 90% of individuals with a reported history of penicillin allergy can safely use penicillin; these indi-viduals usually either are mislabeled as penicillin allergic or lose their allergy after years of avoidance.14 Depending on the studies, the frequency of allergic reactions to penicillin varies from 0.01 to 0.05% (1 to 5 reactions per 10,000), with an anaphylactic reaction rate of less than 0.01% and a fatality rate of less than 0.002% (less than 1 fatality per 50,000 penicillin administrations).15 Parenter-ally administered penicillin is responsible for most of the anaphy-lactic reactions. The extensive use of this drug in unsuspected sources such as foods, in which it is used as a bacteriostatic agent, may make it difficult to ascertain historically that penicillin is not the causative agent.
Cephalosporins share the β-lactam ring structure and side chains of the penicillins, and allergic cross-sensitivity has been incriminated in 1 to 8% of patients.16 Patients who have urticaria or anaphylactic reactions after taking penicillin are approximately four times more likely to have an adverse reaction to cephalospo-rins. Even in this setting, the risk of an anaphylactic reaction to cephalosporins is still less than 0.1%, and the first dose of cepha-losporin can be administered orally under medical supervision.17
Insect Stings
Hymenoptera venoms and fire ant stings are responsible for sig-nificant anaphylactic morbidity and mortality.18 The Hymenop-tera venoms are complex mixtures of pharmacologically and biochemically active substances. Honeybee venom contains hyal-uronidase, phospholipase A, and other peptides. Yellow jacket venom contains not only phospholipases A and B and hyaluroni-dase but also kinins. Hornet venom contains acetylcholine in addition to those typical peptides. Fire ant venom is mostly a nonproteinaceous alkaloid suspension containing phospholipase A and hyaluronidase.
Stinging Hymenoptera insects affect up to 13.6 million Ameri-cans annually (c. 1999), accounting for approximately 50 to 100 deaths annually.19 Allergic sensitization to Hymenoptera has been reported in 0.4 to 4% of the general population. The principal offenders (in decreasing order of frequency) are yellow jackets, honeybees, wasps, and yellow and bald-faced hornets. The imported fire ant has become a significant pest responsible for anaphylaxis, spreading from the Atlantic and Gulf coasts inland.20 The introduction of killer (Africanized) bees in Brazil and their subsequent northern migration make them a significant cause of sting-induced anaphylaxis in areas of Texas, Arizona, and the southwestern United States.21
Other Agents
Latex and Medical Products. Latex allergy refers to sensitivity to the proteins or chemicals contained in the latex products. The sensi-tivity reaction can be delayed (type IV) contact dermatitis or an immediate hypersensitivity (type I) reaction (Box 119-3). The most common symptoms of latex allergy include allergic urticaria, rhinitis, conjunctivitis, and occupational asthma. Although latex allergy used to be more common, with the institution of nonpow-dered gloves and nonlatex gloves in hospitals, anaphylactic reac-tion from latex has become an uncommon event.22 Anaphylactic reactions have also occurred against ethylene oxide (ETO), which is used to sterilize hemodialyzers. ETO can bind with human proteins such as human serum albumin (HSA), rendering the ETO-HSA complex allergenic.
BOX 119-3
Type I: Immediate HypersensitivityBinding of multivalent antigens to IgE on the surface of mast cells and basophils leads to degranulation of mediators. In previously sensitized individuals, the reaction develops quickly (minutes). This type of hypersensitivity reaction is seen in allergic diseases (e.g., hay fever, allergic asthma, urticaria, angioedema, and anaphylaxis). Anaphylactoid reaction refers to the direct release of preformed mediators of mast cells independent of IgE.
Type II: Cytotoxic Antibody ReactionAntibody (IgM, IgG) binding of membrane-bound antigens leads to cytotoxicity and cell lysis of cells through the complement or mononuclear cell system (macrophages, neutrophils, and eosinophils). This type of reaction is seen in transfusion reaction and Rh incompatibility.
Type III: Immune Complex–Mediated ReactionBinding of antibody (IgM, IgG) to antigens forms soluble immune complexes, which are deposited on vessel walls, causing a local inflammatory reaction (Arthus reaction) leading to inflammation and tissue injury. This type of reaction is seen in systemic lupus erythematosus and serum sickness (after antithymocyte globulin administration).
Type IV: Cell-Mediated Delayed HypersensitivitySensitized lymphocytes (TH1 cells) recognize the antigen, recruit additional lymphocytes and mononuclear cells to the site, and start the inflammatory reaction. No antibodies are involved. This type of reaction is seen in contact dermatitis, erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis.
Gell and Coombs Classification of Immune Reactions

1546 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
anaphylactic-like incidents.34 The mechanism is unclear, but release of mediators from mast cells and basophils has been impli-cated. Patients with exercise-induced anaphylaxis are generally dedicated athletes who may have a personal or family atopic history. Exercise-induced anaphylaxis has been demonstrated in some cases to depend on previous ingestion of food to which the patient may be subclinically sensitive. Provocative foods, if identi-fied, should be avoided. Patients should discontinue the exercise at the onset of rash or pruritus. When exercise is continued beyond this point, clinical deterioration is likely in susceptible individuals. Prophylactic treatment with an antihistamine as a single agent or in combination with other agents may be helpful. Avoidance of precipitating factors, modification of exercise, and use of a self-injectable epinephrine kit are recommended for patients with exercise-induced anaphylaxis.
Idiopathic Anaphylaxis. In the United States, approximately 20,000 to 47,000 patients annually see allergists for signs and symptoms of idiopathic anaphylaxis (IA).35 The diagnosis of IA is made only after extensive evaluation by the allergist. Although IA may be life-threatening, it is usually responsive to conventional therapies, including antihistamines, sympathomimetics, and espe-cially prednisone.36 Some cases of IA may appear to be caused by the act of kissing but are in fact caused by food or conversion disorders.37 The overall prognosis for IA is good, but certain patients may experience recurrent IA despite intensive prophylac-tic therapy. Sometimes, IA can represent “progesterone” anaphy-laxis.38 Women suffering from this disorder may present with recurrent episodes of anaphylaxis that are temporally related to the menstrual cycle. Other patients may have anaphylactic reac-tions to injection of medroxyprogesterone or luteinizing hormone–releasing hormone.
PRINCIPLES OF DISEASE
Because allergy is intimately related to immunology, a brief review of immunology is included in this chapter. Immunologic responses to antigens in humans are coordinated by two systems: the ancient innate immune system, which humans inherited from inverte-brates; and the recently evolved adaptive immune system, which is present in humans and vertebrates (Fig. 119-1). The innate immune system is considered the first line of defense, character-ized by its nonspecific but rapid responses to offending agents or microbes. Its effector components include resident cells (epithelial cells, mast cells, macrophages, dendritic cells, antimicrobial pro-teins), infiltrative cells (natural killer cells, neutrophils, mono-cytes, dendritic cells), and various proteins (antimicrobial peptides, complements, cytokines, pathogenic pattern recognition receptor [PRR] system). Encoded in the germline, PRRs can recognize pathogen-associated molecular patterns (PAMPs) extracellularly or intracellularly. PAMPs are evolutionarily conserved molecular patterns that are present in microbes but not in humans (except in mitochondrial DNA).39 On exposure of the human host to these PAMPs, the PRR and subsequently the innate system and the inflammatory cascade are activated, leading to the clearance of dangerous PAMPs.40 The innate system responds to the danger signals rapidly and nonspecifically, whereas the adaptive immune system takes time for the antigen-specific cells (B and T cells) to amplify through a process known as clonal expansion to mount a specific immune response. In contrast to the innate system, the adaptive immune system is characterized by the delayed response, immune memory, enormous diversity, and exquisite specificity. The effector components of the adaptive system include B and T lymphocytes and cytokines. T and B cells are capable of recogniz-ing myriad antigens through a vast library of antibodies and receptors (up to 1015). This diversity is accomplished by somatic rearrangement of fewer than 400 genes.41,42
Radiocontrast Media. Radiocontrast media (RCM) represent an important class of drugs that can cause an anaphylactic reaction. Approximately 10 million radiologic studies using RCM are per-formed in the United States annually. Anaphylactic reactions to RCM are largely idiosyncratic, occur within minutes of infusion, and are independent of the dose. The pathophysiologic mecha-nism of anaphylactic reactions to RCM is unknown, but it is believed to be nonimmunologic. Suggested mechanisms include direct histamine release, alternative complement pathway activa-tion, and activation of the contact system. Risk factors for an anaphylactic reaction include a previous adverse reaction to RCM, a history of atopy or allergic disease, asthma, and certain medica-tions. A history of allergy to fish or shellfish is not a contraindica-tion to the use of RCM, nor does it increase the risk of an adverse reaction to RCM.26 Clinically, the risk for severe adverse reaction is 0.16% with ionic contrast materials and 0.03% with nonionic contrast materials. The death rate from RCM reactions is esti-mated at 1 to 3 per 100,000 administrations of contrast material.27 Protocols have been developed to minimize risks of a serious allergic reaction in patients who have had a previous adverse reac-tion to RCM but who still require additional radiographic studies with contrast agents (Box 119-4).
Aspirin and NSAIDs. Aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) are believed to cause anaphylaxis (or anaphylactoid reaction) through interruption of arachidonic acid metabolism.28 The incidence of anaphylaxis to aspirin and NSAIDs varies widely, depending on the population (healthy, atopic, or those with nasal polyps). One study estimated the inci-dence as 2.1 anaphylaxis cases per 100,000 exposed patients.15 Desensitization protocols have been suggested for cardiovascular patients with a history of aspirin allergy.29 For aspirin-induced cutaneous disease, an aspirin desensitization protocol that can be used for cardiovascular patients in the ED is to administer aspirin every 15 minutes, starting with 0.1 mg, up to 325 mg at 135 (FD&C Yellow No. 5), may also cause anaphylaxis through modu-lation of arachidonic acid metabolism.31
Immunotherapy Drugs. Allergen extracts are commonly used in skin testing and in immunotherapy (also known as hyposensitiza-tion or desensitization).32 Exposure to therapeutic pollens, by injection or inhalation, can result in local allergic or systemic anaphylactic reactions. High-dose therapy, too frequent adminis-tration, or inadvertent intravascular injection increases the risk of anaphylaxis with immunotherapy.
Steroids. Although corticosteroids are used in the management of acute allergic syndromes and anaphylaxis, adverse reactions to these medications have been observed after parenteral administra-tion.33 Skin testing may demonstrate the specific class of steroids responsible for hypersensitivity, and substitution of a different class should be considered.
Exercise (Physical)–Induced Anaphylaxis. Thermomechanical and physical factors (heat and cold), especially exercise, have increasingly been recognized as etiologic agents in certain
Modified from Lieberman P: Anaphylaxis. Med Clin North Am 90:77, 2006.
BOX 119-4
Prednisone 50 mg by mouth given 13 hours, 7 hours, and 1 hour before the procedure
Diphenhydramine 50 mg intramuscularly given 1 hour before the procedure
Consider ephedrine 25 mg by mouth given 1 hour before the procedure
Consider an H2 antagonist such as ranitidine 300 mg by mouth given 3 hours before the procedure
A Standard Treatment Protocol for Patients with a History of Radiocontrast-Induced Anaphylaxis

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1547
Figure 119-1. Developmental pathways of the immune and hematopoietic systems. CFU-GEMM, colony-forming unit for granulocyte, erythroid, myeloid, and megakaryocyte.
CFU-GEMM
B cellT cell
Antibodies
Adaptive immune system(delayed response)
Innate immune system(rapid response)
Natural killerT cells
Pattern recognitionreceptor (PRR)
Macrophage
Neutrophil
Erythrocytes
Platelet
Epithelial cells
Dendritic cell
Eosinophil
Mast cell Basophil
CD8+ T cells
CD4+ T cells
Pluripotentstem cellLymphoid
precursor
Development of the Immune System and Mechanism of Immune-Mediated Injury
The adaptive and innate immune systems originate from the common pluripotential hematopoietic stem cells, which are derived from the yolk sac and later reside in the bone marrow. These stem cells differentiate and develop into the lymphoid pre-cursor cells and the colony-forming unit for granulocyte, ery-throid, myeloid, and megakaryocyte (CFU-GEMM) stem cells. The lymphoid precursor cells differentiate into bursa-equivalent lymphocytes (B cells), thymus-derived lymphocytes (T cells), and natural killer cells. The CFU-GEMM cells develop into mast cells, basophils, and others (see Fig. 119-1). When the host encounters a foreign antigen, the cellular components of the adaptive immune system interact with the cellular and protein components of the innate immune system to mount a concerted defense aimed at neutralization of the antigen.
T-Cell Development
Lymphoid precursor cells migrate from the bone marrow into the thymus, where they continue their ontogeny.43 Under regulation by cytokines and cell-cell interaction, these precursors undergo gene rearrangement and positive and negative selection. In the process, T cells acquire the T-cell antigen receptors and various surface markers. Two types of T cells mature and come out of the thymus: CD4+, also called helper T cells (60-70%), and CD8−, also called suppressor T cells (30-40%). Depending on the type of cytokine produced, T helper cells differentiate into type 1 helper cells (TH1) and type 2 helper cells (TH2), with opposing activities. Whereas TH1 cells inhibit IgE production and IgE isotype
switching, TH2 cells stimulate IgE production and IgE isotype switching. The balance of these stimulatory and inhibitory activi-ties of the TH1 and TH2 cells is believed to determine an individ-ual’s propensity to develop allergic disease or atopy and may help explain the increased prevalence of allergy in urbanized and Western societies in the past three decades. Early in utero and soon after birth, naïve T lymphocytes in the infant’s immune system are dominated by the allergy-prone TH2 cells and their associated cytokines (interleukins 4, 5, and 13). These cytokines are impor-tant inducers for production of IgE antibodies. Later, during infancy through early childhood and adolescence, the nonatopic infant’s immune system gradually shifts from this allergy-prone TH2 environment to an allergy-protective TH1 environment. The cytokines associated with this TH1 environment include interleukin-2 and interferon-γ. This shift is thought to be caused by the continual exposure of the young individual’s immune system to allergenic stimuli from the surrounding environment, mainly microbes. Features of Western lifestyles, such as changes in infant diets, widespread use of antibiotics, smaller family size, and cleaner childcare, are believed to reduce this stimulatory anti-genic exposure in an individual’s early years, leading to an envi-ronment in which the immune system is dominated by a persistent allergy-prone TH2 system (the hygiene hypothesis). This imbal-ance between the two immune systems supposedly ultimately leads to atopy and thus an allergy-prone population.44
B-Cell Development and Immunoglobulins
B-cell ontogeny is divided into antigen-independent and antigen-dependent stages.43 During the antigen-independent stage, B cells mature in primary lymphoid organs (bone marrow and fetal liver), where they undergo gene rearrangement in a stochastic
1548 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
Classification of Reactions
The term allergy is commonly used to describe clinical illnesses produced by excessive immune responses by a normal immune system to otherwise innocuous allergens. In this chapter, we adapt the classic Coombs and Gell classification to categorize these hypersensitivity reactions (Box 119-5).
Type I reactions (immediate hypersensitivity) are IgE mediated and account for most allergic and anaphylactic reactions observed in humans. Exposure to sensitizing allergens causes mediators from mast cells and basophils to be released through both IgE-dependent and direct mast cell degranulation (IgE-independent) mechanisms. Rhinitis caused by ragweed pollen and anaphylaxis caused by foods are examples of the IgE-dependent mechanism; anaphylactic reaction to aspirin is an example of the IgE-independent mechanism.
Type II reactions (cytotoxic) denote antibody-mediated cyto-toxic reaction. Complement-fixing IgG (or IgM) engages cell-bound antigen, activating the classic complement pathway and leading to the fixation of membrane attack complexes on the cell surface and subsequent cell lysis. In the process, anaphylatoxins C3a and C5a cause mast cell mediators to be released, producing the same clinical syndrome seen in allergic anaphylaxis.
Type III reactions (immune complex) are IgG or IgM complex mediated. Circulating soluble antigen-antibody immune com-plexes migrate from the circulation to be deposited in the peri-vascular interstitial space, thereby activating the complement system. Anaphylactic reactions to blood transfusions and blood component therapy, including serotherapy (immunoglobulin administration), are examples of the overlap of type II and type
manner and acquire various surface markers. Later during the antigen-dependent stage in the secondary lymphoid organs (lymph nodes and spleen), B cells differentiate into memory B cells and plasma cells and are ready to secrete immunoglobulins. Throughout B-cell ontogeny, B-cell maturation, isotype switch-ing, and immunoglobulin production are driven by activated T cells, cytokines, and interaction with antigen and bone marrow stromal cells.
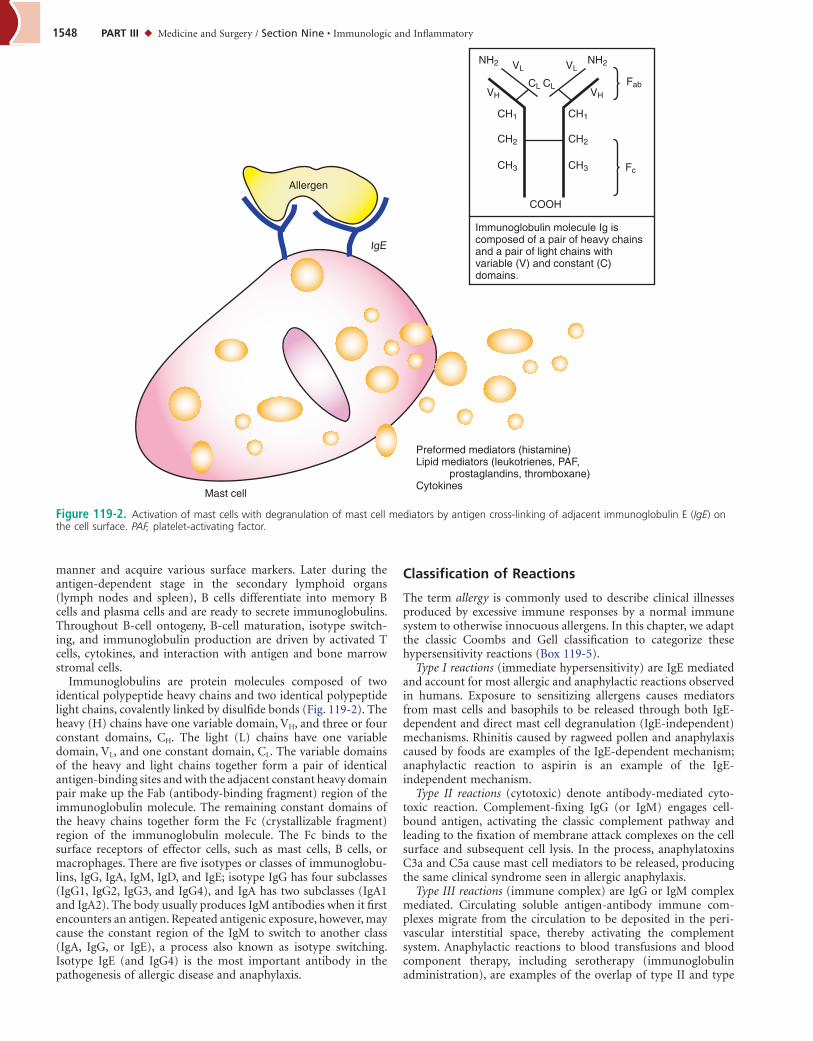
Immunoglobulins are protein molecules composed of two identical polypeptide heavy chains and two identical polypeptide light chains, covalently linked by disulfide bonds (Fig. 119-2). The heavy (H) chains have one variable domain, VH, and three or four constant domains, CH. The light (L) chains have one variable domain, VL, and one constant domain, CL. The variable domains of the heavy and light chains together form a pair of identical antigen-binding sites and with the adjacent constant heavy domain pair make up the Fab (antibody-binding fragment) region of the immunoglobulin molecule. The remaining constant domains of the heavy chains together form the Fc (crystallizable fragment) region of the immunoglobulin molecule. The Fc binds to the surface receptors of effector cells, such as mast cells, B cells, or macrophages. There are five isotypes or classes of immunoglobu-lins, IgG, IgA, IgM, IgD, and IgE; isotype IgG has four subclasses (IgG1, IgG2, IgG3, and IgG4), and IgA has two subclasses (IgA1 and IgA2). The body usually produces IgM antibodies when it first encounters an antigen. Repeated antigenic exposure, however, may cause the constant region of the IgM to switch to another class (IgA, IgG, or IgE), a process also known as isotype switching. Isotype IgE (and IgG4) is the most important antibody in the pathogenesis of allergic disease and anaphylaxis.
Figure 119-2. Activation of mast cells with degranulation of mast cell mediators by antigen cross-linking of adjacent immunoglobulin E (IgE) on the cell surface. PAF, platelet-activating factor.
Preformed mediators (histamine)Lipid mediators (leukotrienes, PAF, prostaglandins, thromboxane)Cytokines
Mast cell
NH2 NH2
VHVH
CH1
CH2
CH3
CH1
CH2
Fc
Fab
CH3
VL VL
CL CL
COOH
Immunoglobulin molecule Ig is composed of a pair of heavy chains and a pair of light chains with variable (V) and constant (C) domains.
IgE
Allergen

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1549
making it difficult to ascribe specific clinical manifestations to any one mediator. Histamine is the most important mediator and responsible for most of the clinical symptoms (Table 119-1). It is an essential mediator in immediate hypersensitivity and inflam-mation, and its infusion has been shown to produce the majority of the clinical features of anaphylaxis syndrome.45 There are three classes of histamine receptors: H1, H2, and H3. H1 receptor stimula-tion produces bronchial, intestinal, and uterine smooth muscle contraction; coronary artery spasm; plaque rupture; and acute myocardial infarction (Kounis syndrome).46 H1 receptor stimula-tion also increases vascular permeability, nasal mucus production, eosinophil and neutrophil chemokinesis, and chemotaxis. H2 receptor stimulation increases the rate and force of ventricular and atrial contraction, gastric acid secretion, airway mucus pro-duction, and vascular permeability while also causing bronchodi-lation and inhibition of basophil histamine release. H3 receptors are found in neurons (in the central nervous system) and periph-eral tissues; these receptors control the synthesis and release of histamine.
In addition to histamine, lipid metabolites elaborated through the prostanoid and leukotriene pathways contribute to the adverse physiologic effects induced by histamine. Prostaglandin D2 (PGD2) is the main arachidonic acid metabolite released by activated mast cells (but not by basophils). PGD2 and thromboxanes are synthe-sized from arachidonic acid by the cyclooxygenase pathway (through both COX-1 and COX-2). PGD2 is responsible for hypo-tension, inhibition of platelet aggregation, and bronchospasm; PGD2 is approximately 30 times more potent than histamine in causing bronchoconstriction. The cysteinyl leukotrienes LTB4, LTC4, LTD4, and LTE4 are synthesized from arachidonic acid through the lipoxygenase pathway. LTB4 and LTC4 are first synthe-sized intracellularly in mast cells and basophils and then secreted; LTC4 is subsequently converted to LTD4 and LTE4 in the extracel-lular space (by γ-glutamyl transpeptidase and dipeptidase). They are involved in cholinergic-independent bronchospasm, increased vascular permeability, and increased mucous gland production. These three leukotrienes have slow onset but potently add to the bronchoconstriction already induced by histamine (LTC4 and LTD4 are 1000 times more potent than histamine).
Platelet-activating factor (PAF) is a phospholipid and the most potent compound known to cause aggregation of human platelets. Its other actions include neutrophil activation and chemotaxis and ileal and parenchymal lung strip smooth muscle contraction. PAF produces many of the important clinical manifestations of ana-phylaxis, including decreased myocardial contractile force, coro-nary vasoconstriction, pulmonary edema, and prolonged increase in total pulmonary resistance with a decrease in dynamic compli-ance.47,48 Indeed, blockage of PAF with experimental antagonists leads to improved cardiac function, suggesting that PAF may be involved in the late cardiac dysfunction and lethality associated with anaphylaxis.49
Recent data have highlighted the important roles that nitric oxide and sphingosine 1-phosphate play in anaphylaxis. Sphingo-sine 1-phosphate can trigger calcium influx, stimulating synthesis of cytokines and mast cell degranulation. Nitric oxide is synthe-sized in vascular endothelium and is a sufficiently potent vasodi-lator to cause hypotension in anaphylaxis. Its action can be increased by histamine, leukotriene, tumor necrosis factor alpha, and PAF.47,50
Physiologic Effects
At the organ and tissue level, mediators released from mast cells and basophils account for the overall pathophysiologic effects of anaphylaxis, which variably are manifested clinically as urticaria and angioedema, rhinorrhea, conjunctivitis, chest pain, breathing difficulty, respiratory insufficiency, headache, syncope,
III reactivity. They have therefore been classified as complement-mediated or immune complex–mediated anaphylaxis.
Type IV reactions (delayed hypersensitivity) are T-cell mediated and have no documented relationship to the pathogenesis of anaphylaxis.
PATHOPHYSIOLOGY
Mast cells, basophils, and their mediators are the central effectors in allergy and anaphylaxis. Exposure of a genetically predisposed individual to an allergen leads to the synthesis and release of allergen-specific IgE by plasma cells into the circulation. Fixation of this allergen-specific IgE to surface receptors on mast cells (FcεRI) completes the process known as sensitization. These IgE-bearing mast cells usually reside in the mucosal surfaces, submu-cosal tissue (around venules), and cutaneous surfaces, and they are capable of becoming activated on reexposure to a specific allergen. Cross-linking of the FcεRI receptors on the mast cells by a specific multivalent allergen sets off a cascade of conformational and bio-chemical events, causing the degranulation of preformed media-tors, subsequent generation and release of arachidonic acid metabolites, elaboration of cytokines and chemokines, and activa-tion of the cellular components by the innate and adaptive systems. These series of events ultimately lead to the clinical syndrome of allergy and anaphylaxis (see Fig 119-2).
Mediators of Anaphylaxis
The numerous mediators released by mast cells and basophils exert overlapping physiologic effects on target organs and tissues,
From Sampson HA, et al: Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 119:391, 1996.*Low systolic blood pressure for children is defined as less than 70 mm Hg from 1 month to 1 year, less than (70 mm Hg + [2 × age]) from 1 to 10 years, and <90 mm Hg from 11 to 17 years.
BOX 119-5
Anaphylaxis is highly likely when any one of the following three criteria is fulfilled:1. Acute onset of an illness (minutes to several hours)
with involvement of the skin, mucosal tissue, or both (e.g., generalized hives, pruritus or flushing, swollen lips-tongue-uvula) and at least one of the following:a. Respiratory compromise (e.g., dyspnea, wheeze-
bronchospasm, stridor, reduced PEF, hypoxemia)b. Reduced BP or associated symptoms of end-organ
dysfunction (e.g., hypotonia [collapse], syncope, incontinence)
2. Two or more of the following occurring rapidly (minutes to several hours) after exposure to a likely allergen for that patient:a. Involvement of the skin-mucosal tissue (e.g., generalized
hives, itch-flush, swollen lips-tongue-uvula)b. Respiratory compromise (e.g., dyspnea, wheeze-
bronchospasm, stridor, reduced PEF, hypoxemia)c. Reduced BP or associated symptoms (e.g., hypotonia
[collapse], syncope, incontinence)d. Persistent gastrointestinal symptoms (e.g., crampy
abdominal pain, vomiting)3. Reduced BP after exposure to known allergen for that
patient (minutes to several hours):a. Infants and children: low systolic BP (age specific) or
greater than 30% decrease in systolic BP*b. Adults: systolic BP of less than 90 mm Hg or greater than
30% decrease from that person’s baseline
Clinical Criteria for Diagnosis of Anaphylaxis
BP, blood pressure; PEF, peak expiratory flow.

1550 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
MEDIATORS PHYSIOLOGIC ACTIVITY CLINICAL MANIFESTATION
Histamine, leukotrienes, thromboxane, prostaglandins, platelet-activating factor, nitric oxide
Vascular permeability, vasodilation, smooth muscle spasm, mucous gland secretion, nociceptor stimulation, myocardial depression
Generalized urticaria and angioedema, pruritus, wheezing, bronchoconstriction, rhinorrhea and bronchorrhea, coryza, conjunctivitis, syncope, tachycardia, hypotension, shock, abdominal pain, nausea, vomiting, diarrhea
Tryptase, carboxypeptidase, chymase, cathepsin G
Activation of complement system, chemoattraction, activation and degranulation of mast cells
Anaphylaxis response is amplified by recruitment and activation of the complement system and further degranulation of mast cell mediators; extent of anaphylaxis may also be limited through opposing effects on conversion of angiotensin I to angiotensin II
Heparin, chondroitin sulfate Antithrombotic, inhibition of the complement system, chemoattraction, activation of the kinin pathway
Tendency for intravascular coagulation is tempered; activation of the kinin system can exacerbate symptoms of anaphylaxis
TNF-α, cytokines, chemokines, eosinophil chemotactic factors
Induction of anti–platelet-activating factor production, control of migration of eosinophils and other inflammatory cells
May be responsible for the intensity, protracted symptoms, and multiphasic reaction of the anaphylaxis attack
TNF-α, tumor necrosis factor alpha.
Table 119-1 Mediators in Anaphylaxis and Their Physiologic Actions
hypotension and hemodynamic instability, nausea, vomiting, diarrhea, and other gastrointestinal symptoms (see Table 119-1). Increased vascular permeability caused by histamine leads to urti-caria, angioedema, laryngeal edema, nasal congestion, or gastro-intestinal swelling with abdominal cramping and vomiting. Vasodilation can lead to flushing, headaches, reduced peripheral vascular resistance, hypotension, and syncope. Contraction of smooth muscle can lead to bronchospasm, abdominal cramping, or diarrhea. Pulmonary vessel vasoconstriction can lead to pul-monary hypertension, pulmonary edema, and decreased cardiac filling pressures. Coronary vasoconstriction can lead to myocar-dial ischemia and decreased myocardial contractile force. Changes in atrial chronotropy and ventricular and atrial isotropy can lead to cardiac dysrhythmias. In addition to the direct actions on the target tissues, these preformed mediators, lipid-derived mediators, and cytokines activate a number of inflammatory pathways, including the complement system, the clotting and clot lysis systems, and the kallikrein-kinin (contact) system, to add to the clinical manifestations of allergy and anaphylaxis. Deaths in anaphylaxis are caused most commonly by acute respiratory failure from laryngeal angioedema and less commonly by cardio-vascular collapse.
Hemodynamic instability in anaphylaxis is typically the result of peripheral vasodilation, enhanced vascular permeability, leakage of plasma, and intravascular volume depletion (the “empty ventricle” syndrome). Up to 50% of intravascular volume can shift to the extravascular space within 10 minutes of exposure.51 In a number of clinical settings, the hypotension in anaphylaxis is also associated with depressed cardiac index and increased pulmonary vascular resistance. The use of pressors alone in anaphylaxis may not improve hemodynamics. Aggressive volume expansion with crystalloid (2-7 L of normal saline) is needed for hypotension in anaphylaxis.6
CLINICAL FEATURES
Anaphylactic reactions vary in duration and severity, affecting organs that are rich in mast cells—the cutaneous, upper and lower respiratory, cardiovascular, neurologic, and gastrointestinal systems. Clinical presentations of anaphylaxis depend on the degree of hypersensitivity; the quantity, route, and rate of antigen exposure; the pattern of mediator release; and the target organ sensitivity and responsiveness. Symptoms of anaphylaxis usually occur minutes after an exposure, although some reactions take longer (>30 minutes). Protracted anaphylaxis may last up to 32
hours.51 Up to 20% of patients may present with biphasic anaphy-laxis, in which clinical symptoms may recur 8 to 24 hours after resolution of symptoms from the index event.52 There are no firmly established factors that can be used to predict which group of patients is at risk for this biphasic attack, although delayed and inadequate administration of epinephrine after the index event and the lack of steroid use have been cited in some studies.53 Fatal cases of anaphylaxis are usually caused by acute respiratory failure due to laryngeal edema and less commonly by cardiovas-cular collapse.
The first clinical manifestation of anaphylaxis usually involves the skin (88%), described as generalized warmth and tingling of the face, mouth, upper chest, palms, soles, or the site of antigenic exposure. Pruritus is a nearly universal feature and may be accom-panied by generalized flushing and urticaria. Patients presenting with angioedema may complain of swelling and a sensation of burning under the skin but no itchy rash. This may be followed by mild to severe respiratory distress. The patient may describe a cough; a sense of chest tightness, dyspnea, and wheeze from bron-chospasm; or throat tightness, dyspnea, odynophagia, or hoarse-ness associated with laryngeal edema or oropharyngeal angioedema. Hypotension or dysrhythmias may be manifested as lightheaded-ness or syncope. Seizure activity caused by decreased cerebral per-fusion may rarely be observed. Any of these clinical patterns may occur independently or in association with nasal congestion and sneezing; ocular itching and tearing; cramping abdominal pain with nausea, vomiting, diarrhea, and tenesmus; incontinence; pelvic pain and uterine cramping; headache; or a sense of impend-ing doom. Although urticaria and angioedema are the most common presenting symptoms in anaphylaxis (88%), fatal ana-phylaxis syndromes with laryngeal edema and circulatory collapse can occur even in the absence of any premonitory warning symp-toms or signs or cutaneous manifestations.6
The physical examination may reveal tachypnea, tachycardia, and hypotension. Laryngeal stridor, hypersalivation, hoarseness, and angioedema indicate upper airway obstruction, whereas coughing, wheezing, rhonchi, and diminished air flow suggest lower respiratory tract bronchoconstriction. Tachycardia and hypotension suggest cardiac insufficiency. Commonly observed dysrhythmias include sinus tachycardia, premature atrial and ven-tricular contractions, nodal rhythm, and atrial fibrillation. Other electrocardiographic changes include nonspecific and ischemic ST-T wave changes, right ventricular strain, and intraventricular conduction defects. The patient may have a depressed level of consciousness because of hypotension; rarely, this may be caused

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1551
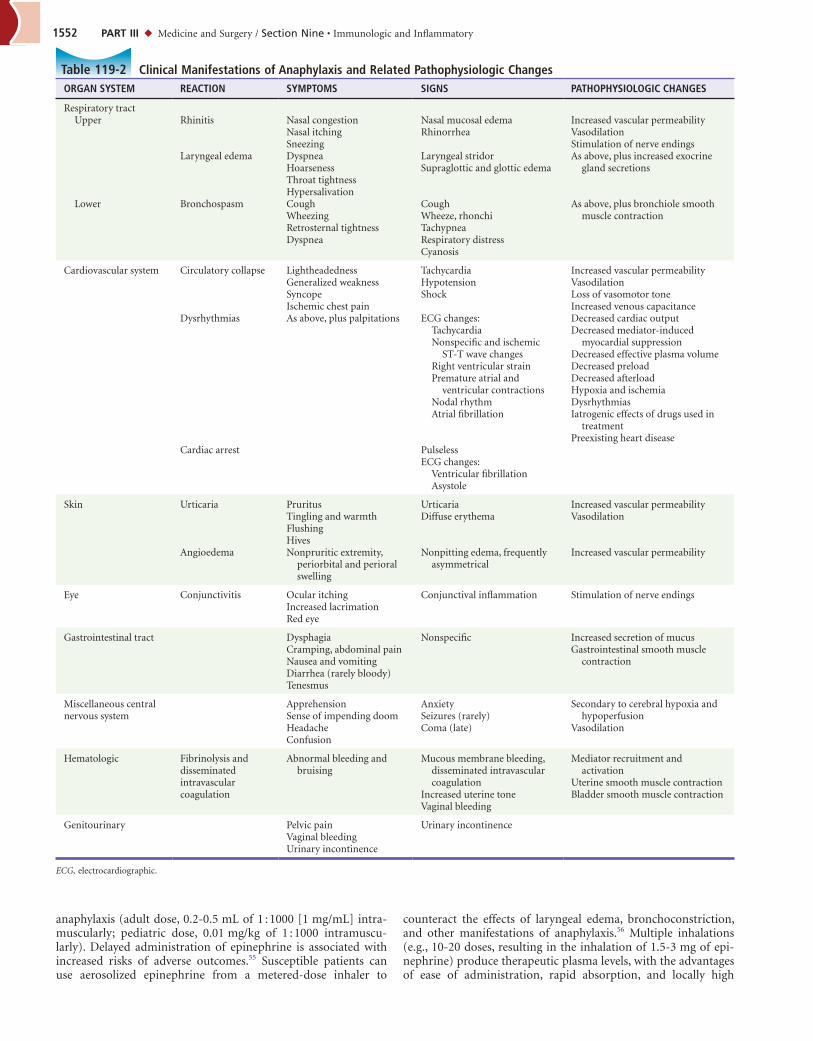
by a postictal state due to seizure activity. Urticaria, angioedema, rhinitis, and conjunctivitis may be evident. A summary of the observed clinical manifestations of anaphylaxis along with their related pathophysiologic changes is presented in Table 119-2.
DIAGNOSTIC STRATEGIES
The diagnosis of anaphylaxis remains clinical. A good history and physical examination offer emergency physicians the best tools in diagnosis of anaphylaxis. The diagnosis of anaphylaxis is “highly likely” in a patient presenting with skin symptoms (itchy urticaria, flushing, and swollen lips, tongue, or throat) and either respiratory difficulty (dyspnea, wheezing, and stridor) or reduced blood pres-sure, after an acute exposure (see Box 119-5).54 Diagnostic labora-tory testing is limited and seldom used in the ED. Anaphylaxis can be confirmed by testing for allergen-specific IgE and serum trypt-ase, serum histamine, or 24-hour urine histamine in select cases. Screening studies are aimed at ruling out of other emergencies (Box 119-6). The initial screening studies can include a complete blood count, complete metabolic panel (hypoglycemia), coagula-tion panel (prothrombin time, partial thromboplastin time, and international normalized ratio), cardiac enzymes, electrocar-diogram, urine analysis, erythrocyte sedimentation rate, and por-table chest radiograph. Serum levels of serotonin and urinary 5-hydroxyindole acetic acid, catecholamines, and vanillylmandelic acid are useful to rule out carcinoid syndrome. Serial arterial blood gas analysis may help monitor clinical response. Blood culture, urine culture, computed tomography of the head and lateral soft tissue of the neck, and indirect and direct laryngoscopy can be considered, depending on the clinical situation.
DIFFERENTIAL DIAGNOSIS
The diagnosis of anaphylaxis is readily apparent in a patient pre-senting with acute rash, respiratory difficulty, or cardiac insuffi-ciency after an allergenic exposure. Considerations for confounders and other diseases with overlapping presentations are shown in Box 119-6.
Urticaria and Angioedema
Generalized urticaria is usually allergic in nature (i.e., mast cell mediated). In half of the cases, it is accompanied by angioedema and may meet the definition for anaphylaxis. Similarly, most cases of angioedema are allergic and usually associated with urticaria. Angioedema caused by bradykinin excess (e.g., hereditary angio-edema or ACE inhibitor) usually is manifested without urticaria. The treatment of this “nonallergic” angioedema is rapidly evolving with ongoing clinical trials and new medications approved by the Food and Drug Administration (FDA). Adverse cutaneous drug reactions (ACDR) comprise a spectrum of skin manifestations due to complications from drug therapy. The majority of these ACDRs are minor allergic reactions (e.g., IgE-mediated urticarial rash to penicillin). Severe, life-threatening ACDRs (e.g., Stevens-Johnson syndrome, toxic epidermal necrolysis, fixed drug erup-tion, drug hypersensitivity syndrome) may mimic drug-induced anaphylaxis.
Flush Syndrome
Flush syndrome refers to a group of diverse clinical entities that are characterized by the onset of redness and a feeling of warmth of the face, neck, trunk, and abdomen. Flushing of the face induced by alcohol is common in Asian patients. Monosodium glutamate (MSG) and its cyclization product pyroglutamate are common seasonings in Chinese foods and can provoke flushing. Scombroi-dosis, a type of histamine poisoning, is caused by the ingestion of
spoiled fish that have a high histidine content (generally dark meat fish such as tuna); histamine and cis-urocanic acid are produced by histidine-decarboxylating bacteria that cleave histamine from histidine when the fish are not properly stored.
Patients usually present with a frightening flush (sunburn like) but no urticaria, palpitations, syncope, nausea, vomiting, or diar-rhea. A number of neoplastic disorders (mastocytosis, carcinoid syndrome, VIPoma, medullary carcinoma of the thyroid) secrete vasoactive substances that are present in anaphylaxis. Harlequin syndrome refers to the hemifacial flushing and sweating induced by exercise.
Respiratory Insufficiency
Epiglottitis, supraglottitis, retropharyngeal and peritonsillar ab-scess, laryngeal spasm, foreign body aspiration, tumor, obstructive lung diseases such as acute asthma, and status asthmaticus can be manifested with acute respiratory difficulty but are usually not associated with other symptoms and signs of anaphylaxis. Exercise-induced anaphylaxis can be differentiated from exercise-induced asthma as the former is usually accompanied by pruritus and other systemic manifestations of anaphylaxis. Patients with acute pulmonary embolism may present with respiratory difficulty and shock but without the cutaneous stigmata of anaphylaxis.
Shock and Cardiovascular System
Patients with anaphylactic shock may present with urticarial rash, angioedema, respiratory insufficiency, hypotension, vasodilation, and signs and symptoms of end-organ hypoperfusion. This form of shock must be differentiated from early presentations of septic shock (end-organ hypoperfusion, rash, vasodilation, hypoten-sion). A history of recent allergenic exposure is helpful in making the diagnosis of anaphylaxis. Spinal shock also presents with hypotension and vasodilation but usually without the urticarial rash and in the setting of significant spinal injury. In all these forms of shock, the skin is usually moist and warm, suggesting a state of decreased peripheral vascular resistance. Cardiogenic, restrictive, hypovolemic, or hemorrhagic shock, on the other hand, would more likely be seen with signs and symptoms of end-organ hypoperfusion and cold, clammy skin, suggesting a state of heightened peripheral vascular resistance. In addition to history, measurement of central venous pressures may add useful data in teasing out the different forms of shock.
Syncope
Vasovagal syncope is the most common differential diagnosis in the patient arriving with collapse as a result of parenteral admin-istration of an antigen. Classically, the patient has bradycardia, hypotension, and pallor as opposed to the tachycardia, hypoten-sion, and flush skin usually associated with anaphylaxis. The absence of any other clinical manifestations of anaphylaxis, along with history of stress, pain, and previous episodes of simple faints, helps point toward the diagnosis of vasovagal syncope. Other causes of syncope, such as seizure, stroke, hypoglycemia, acute coronary syndrome, and cardiac dysrhythmia, also need to be considered. Ordinary allergic reactions and especially anaphylaxis can precipitate an acute coronary syndrome.
MANAGEMENT
Out-of-Hospital Care
When a susceptible patient is reexposed to an antigen to which there has been a previous reaction, self-administered epinephrine is recommended at the first onset of clinical manifestations of
1552 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
ORGAN SYSTEM REACTION SYMPTOMS SIGNS PATHOPHYSIOLOGIC CHANGES
Respiratory tract Upper Rhinitis Nasal congestion
Nasal itchingSneezing
Nasal mucosal edemaRhinorrhea
Increased vascular permeabilityVasodilationStimulation of nerve endings
Laryngeal edema DyspneaHoarsenessThroat tightnessHypersalivation
Laryngeal stridorSupraglottic and glottic edema
As above, plus increased exocrine gland secretions
Lower Bronchospasm CoughWheezingRetrosternal tightnessDyspnea
CoughWheeze, rhonchiTachypneaRespiratory distressCyanosis
As above, plus bronchiole smooth muscle contraction
Cardiovascular system Circulatory collapse LightheadednessGeneralized weaknessSyncopeIschemic chest pain
TachycardiaHypotensionShock
Increased vascular permeabilityVasodilationLoss of vasomotor toneIncreased venous capacitance
Dysrhythmias As above, plus palpitations ECG changes:TachycardiaNonspecific and ischemic
ST-T wave changesRight ventricular strainPremature atrial and
ventricular contractionsNodal rhythmAtrial fibrillation
Decreased cardiac outputDecreased mediator-induced
myocardial suppressionDecreased effective plasma volumeDecreased preloadDecreased afterloadHypoxia and ischemiaDysrhythmiasIatrogenic effects of drugs used in
treatmentPreexisting heart disease
Cardiac arrest PulselessECG changes:
Ventricular fibrillationAsystole
Skin Urticaria PruritusTingling and warmthFlushingHives
UrticariaDiffuse erythema
Increased vascular permeabilityVasodilation
Angioedema Nonpruritic extremity, periorbital and perioral swelling
Nonpitting edema, frequently asymmetrical
Increased vascular permeability
Eye Conjunctivitis Ocular itchingIncreased lacrimationRed eye
Conjunctival inflammation Stimulation of nerve endings
Gastrointestinal tract DysphagiaCramping, abdominal painNausea and vomitingDiarrhea (rarely bloody)Tenesmus
Nonspecific Increased secretion of mucusGastrointestinal smooth muscle
contraction
Miscellaneous central nervous system
ApprehensionSense of impending doomHeadacheConfusion
AnxietySeizures (rarely)Coma (late)
Secondary to cerebral hypoxia and hypoperfusion
Vasodilation
Hematologic Fibrinolysis and disseminated intravascular coagulation
Abnormal bleeding and bruising
Mucous membrane bleeding, disseminated intravascular coagulation
Increased uterine toneVaginal bleeding
Mediator recruitment and activation
Uterine smooth muscle contractionBladder smooth muscle contraction
Genitourinary Pelvic painVaginal bleedingUrinary incontinence
Urinary incontinence
ECG, electrocardiographic.
Table 119-2 Clinical Manifestations of Anaphylaxis and Related Pathophysiologic Changes
anaphylaxis (adult dose, 0.2-0.5 mL of 1 : 1000 [1 mg/mL] intra-muscularly; pediatric dose, 0.01 mg/kg of 1 : 1000 intramuscu-larly). Delayed administration of epinephrine is associated with increased risks of adverse outcomes.55 Susceptible patients can use aerosolized epinephrine from a metered-dose inhaler to
counteract the effects of laryngeal edema, bronchoconstriction, and other manifestations of anaphylaxis.56 Multiple inhalations (e.g., 10-20 doses, resulting in the inhalation of 1.5-3 mg of epi-nephrine) produce therapeutic plasma levels, with the advantages of ease of administration, rapid absorption, and locally high

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1553
Modified from Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology: The diagnosis and management of anaphylaxis: An updated practice parameter. J Allergy Clin Immunol 115(Suppl 2):S483-S523, 2005.
BOX 119-6
Acute generalized urticariaAllergic and nonallergic angioedema (HAE, ACE inhibitor)Adverse cutaneous drug reactionFlush syndrome
Flushing associated with foodAlcoholMonosodium glutamateSulfitesScombroidosis
Carcinoid tumorMedullary carcinoma of thyroidBasophilic leukemiaRed man syndrome (vancomycin)PheochromocytomaMastocytoses (systemic mastocytosis and urticaria
pigmentosa)Vasointestinal peptide tumorsCapillary leak syndromePostmenopausalHydatid cystHarlequin syndrome (exercise induced)Auriculotemporal nerve syndrome (Frey’s syndrome)
Respiratory disordersUpper airway disorders (epiglottitis, Ludwig’s angina, quinsy,
foreign body aspiration, tumor)Status asthmaticus, asthmatic attackObstructive airway diseasesPulmonary embolism
Shock syndromes and cardiacSeptic shockHypovolemic shockCardiogenic shockDistributive shockAcute coronary syndrome
MiscellaneousHypoglycemiaNeurogenic syncope (vasovagal)Acquired and hereditary angioedema (C1 esterase deficiency)Graft-versus-host diseaseProgesterone anaphylaxisNeurologic disorders (seizure, stroke, autonomic epilepsy)Vocal cord dysfunction syndromePanic attacksUndifferentiated somatoform anaphylaxis
Differential Diagnosis of Anaphylaxis
HAE, hereditary angioedema; ACE, angiotensin-converting enzyme.
epinephrine levels in the upper and lower airways. Epinephrine should be used with caution in elders and those with a history of cardiovascular disease or hypertension, but it must be stated that there are no absolute contraindications to the use of epinephrine in anaphylaxis.6 Oral (and parenteral) diphenhydramine (50 mg) can also be administered, but this is only an adjunct therapy.
Out-of-hospital personnel may be required to resuscitate a moribund patient with basic life support. Their first priority is to establish and to maintain ventilation, intravenous access, cardiac monitoring, and administration of supplemental oxygen.
Local measures to decrease antigen absorption from an extrem-ity include dependent positioning of the extremity, ice to vasocon-strict locally, and application of a loose tourniquet to obstruct the venous and lymphatic circulation. The tourniquet should be released for 1 minute of every 10 minutes and should never be applied continuously for more than 2 hours. If an insect stinger
remains in the wound, the wound should not be squeezed because the stinger may inject more venom into the patient; the stinger should be removed gently with instruments, avoiding disturbance of the venom apparatus.
Emergency Department
Because most of the morbidity and mortality associated with ana-phylaxis are caused by acute respiratory failure or cardiovascular collapse, the treatment of anaphylaxis focuses on the triad of providing a patent airway, expanding intravascular volume with crystalloid (or colloid), and early administration of epinephrine. Antihistamines (H1 and H2) and steroids are commonly given in cases of anaphylaxis, although there is no objective evidence that they will improve the outcome.57,58 Box 119-7 summarizes the treatment algorithm in anaphylaxis.
Airway
Patients at risk of losing their airway are preoxygenated while the airway is assessed. Because upper airway obstruction from laryn-geal angioedema can progress rapidly, preparations for a difficult airway, including a surgical airway, must be made early. Premedi-cation with nebulized epinephrine may help maximize visualiza-tion. The success rate of intubation is improved when it is performed early, before significant soft tissue swelling from oro-laryngeal angioedema occurs.
Volume Expansion
Along with airway preparation, start aggressive fluid resuscitation, which may include 1 to 2 L of normal saline (NS) infused rapidly through large-bore (e.g., 16-gauge) intravenous lines (5 to 10 mL/kg in first 5 minutes). NS is preferred to lactated Ringer’s solution, which has the potential to exacerbate metabolic acidosis.6 The use of a colloid solution (e.g., 5% albumin) in addition to NS may be helpful because of the increased vascular permeability in anaphy-laxis. Large volumes of NS (2-7 L) may be required to reverse the fluid lost to extravascular space in anaphylaxis. Patients with heart failure or renal failure should be monitored closely for signs of volume overload.
Epinephrine
Epinephrine is the drug of choice and the first drug to be given at the first suspicion of an anaphylactic reaction.6 The dose of aqueous epinephrine is 0.2 to 0.5 mL of 1 : 1000 (1 mg/mL) intra-muscularly for adults and 0.01 mg/kg of 1 : 1000 intramuscularly for pediatric patients, repeated every 5 minutes as needed. The intramuscular route allows shorter time to peak plasma epineph-rine concentration (8 minutes) versus subcutaneous administra-tion (34 minutes).6
Epinephrine derives its therapeutic value from its combined alpha-adrenergic and beta-adrenergic actions. Its alpha1-adrenergic stimulation increases vasoconstriction, increases peripheral vascu-lar resistance, and decreases mucosal edema. Its beta1-adrenergic stimulation brings about positive inotropic and chronotropic cardiac activity, and its beta2-adrenergic stimulation results in sta-bilization of mast cells and basophils and bronchodilation.2 As a result, epinephrine decreases mediator release from mast cells (and basophils), improves hives and bronchospasm, decreases mucosa edema and swelling, and reverses systemic hypotension. Epinephrine therefore works directly to improve the clinical fea-tures most commonly observed in a fatal anaphylactic reaction.
Epinephrine can, however, produce untoward side effects, such as palpitations, anxiety, and headache. Excessive alpha-agonist activity (as in overdose) can result in a hypertensive crisis and

1554 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
BOX 119-7
Emergency Measures (taken simultaneously)Remove any triggering agent. If the patient had a sting or
immunization injection, place a loose tourniquet proximal to the site; if the reaction site is on an extremity, place the extremity in dependent position.
Place patient in the Trendelenburg position if hypotensive.Begin cardiac monitoring, pulse oximetry, and blood pressure
autonomic monitoring; apply oxygen non-rebreather mask, establish large-bore intravenous lines, draw blood, obtain stat electrocardiogram and portable chest radiograph.
Establish a patent airway.Open the airway by head tilt/chin lift or jaw thrust as clinically
appropriate.Be prepared for endotracheal intubation with or without rapid
sequence intubation.Be prepared to use adjunct airway technique (laryngeal mask
airway, fiberoptic, jet ventilation, surgical airway) as per local custom.
Administer racemic epinephrine (L-epinephrine acceptable) 0.5 mL of 2.25% solution in 2.5 mL of NS by nebulizer while awaiting definitive airway management.
Start rapid infusion of isotonic crystalloid (NS): 500 mL in the first 5 minutes in the adult; several liters of NS may be required.
Antianaphylactic DrugsEpinephrine is the first-choice drug, to be given simultaneously
with the above general emergency measures, at the first suspicion of an anaphylactic reaction.Intramuscular (1 : 1000 concentration)
Adult: 0.3-0.5 mL every 5 minutes, more often as clinically indicated, titrated to effects
Pediatric: 0.01 mL/kg, every 5 minutes as necessary, titrated to effects
Alternatively, epinephrine (EpiPen, 0.3 mL; or EpiPen Jr, 0.15 mL) can be administered into anterolateral thigh. Removal of clothing is unnecessary.
Intravenous (1 : 100,000 concentration; 0.1 mL of 1 : 1000 epinephrine in 10 mL of NS)Continuous hemodynamic monitoring required10 mL of 1 : 100,000 during 10 minutes, titrated to effects;
repeat as necessaryAntihistamines
Diphenhydramine: intravenous (intramuscular acceptable)Adult: 50 mg, up to 400 mg/24 hr, titrated to effectsPediatric: 1 mg/kg, up to 300 mg/24 hr, titrated to effects
Ranitidine: intravenousAdult: 50 mg IV (150 mg oral)Pediatric: 1 mg/kg IV or oral
Aerosolized beta-agonistsAdult
Albuterol: 2.5 mg, diluted to 3 mL of NS; may be given continuously
Levalbuterol: 0.625-1.25 mg, diluted to 3 mL of NS; may be given continuously
Ipratropium: 0.5 mg in 3 mL of NS; repeat as necessaryPediatric
Albuterol: 2.5 mg, diluted to 3 mL of NS; may be given continuously
Levalbuterol: 0.31-0.625 mg, diluted to 3 mL of NS; may be given continuously
Ipratropium: 0.25 mg in 3 mL of NS; repeat as necessaryMethylprednisolone
Adult: 125-250 mg IVPediatric: 1-2 mg/kg IV
Special SituationsRefractory HypotensionConsider continuous epinephrine drips
Dilute 1 mg (1 mL 1 : 1000) in 250 mL D5W to yield a concentration of 4 µg/mL
Infuse this diluted solution at 1 to 4 µg/min, up to 10 µg/min, titrated to effects
Glucagon: 1-5 mg IV during 5 minutes, followed by 5-15 µg/min continuous infusion
Consider vasopressors:Dopamine, 5-20 µg/kg/min continuous infusion and/or
dobutamine 5-20 µg/kg/min continuous infusion, titrated to effects
Norepinephrine: 8-12 µg/min (2-3 mL/min; 4 mg added to 1000 mL of D5W provides a concentration of 4 µg/mL), titrated to effects
Phenylephrine, 40-180 µg/min, titrated to effectsVasopressin, 2-4 IU/hr, titrated to effects
Patients Receiving Beta-BlockadeGlucagon: 1-5 mg IV during 5 minutes, followed by 5-15 µg/min
continuous infusionTranscutaneous pacing for bradycardiaAtropine for bradycardia
Adult: 0.3-0.5 mg IV or subcutaneous, to a maximum of 3 mgPediatric: 0.02 mg/kg IV or subcutaneous, to a maximum of
2 mg
Treatment Options for Anaphylaxis
D5W, 5% dextrose in water; NS, normal saline.
intracerebral bleeding; worsen myocardial oxygen consumption through increased wall tension, contractility, and chronotropism; and cause myocardial ischemia, myocardial infarction, and pul-monary edema. Increased automaticity and chronotropism can produce hemodynamically significant supraventricular and ven-tricular tachydysrhythmia. Despite these concerns, the benefits of early administration of epinephrine in anaphylaxis far outweigh any of the stated risks. Serious adverse effects of epinephrine administration, such as myocardial ischemia and pulmonary edema, are usually attributable to an overdose or inappropriately rapid intravenous infusion.59 There are no absolute contraindica-tions to the use of epinephrine, and it is the drug of first choice in anaphylaxis and anaphylactic shock.6
If the patient remains hypotensive after multiple doses of intra-muscular epinephrine and aggressive volume expansion, intrave-nous epinephrine should be considered.6 Intravenous epinephrine infusion increases the risks of cardiac dysrhythmias, thus requir-ing continuous cardiac and hemodynamic monitoring. Dilution and slow administration are recommended to reduce untoward
effects by epinephrine. The initial intravenous dose is 10 mL of a 1 : 100,000 dilution of aqueous epinephrine during 10 minutes. This is done by dilution of 0.1 mL of 1 : 1000 epinephrine in 10 mL of NS and infusion during 10 minutes (i.e., 100 µg epi-nephrine infusion given intravenously during 10 minutes at 10 µg/min). If no improvement is observed, a continuous infusion can be set up by mixing 1 mg of epinephrine (i.e., 1 mL of 1 : 1000 epinephrine) in 250 mL of 5% dextrose in water, giving a concen-tration 4 µg/mL. This solution can be started at 1 µg/min and titrated to effects or 10 µg/min.6 In children and infants, an infu-sion rate of 0.1 µg/kg/min is advised, increasing in increments of 0.1 µg/kg/min to a maximum of 1.5 µg/kg/min. A convenient dosing method for pediatric patients is the “rule of 6”: 0.6 × body weight (in kilograms) = milligrams of epinephrine to be diluted to 100 mL NS; then 1 mL/hr of this solution delivers 0.1 µg/kg/min.6 Central line access is usually recommended for intravenous administration of epinephrine because of the risk of tissue necro-sis from possible extravasation. Extravasation of epinephrine from peripheral access is treated with phentolamine. In addition to

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1555
helpful in patients who are receiving beta-blockers and who do not respond to epinephrine and other standard treatment modali-ties.6 Glucagon is thought to effect positive inotropism by aug-menting cyclic adenosine monophosphate synthesis through a nonadrenergic pathway. The initial dose is 1 to 5 mg for adults and 20 to 30 µg/kg (maximum dose 1 mg) for children intrave-nously, followed by an infusion of 1 to 5 mg/hr.6 Side effects include nausea, vomiting, hypokalemia, and hyperglycemia. Atropine can be tried as second-line therapy for symptomatic bradycardia.
DISPOSITION
Most patients with anaphylaxis respond to aggressive manage-ment and can be safely discharged to home. Patients with mild to moderate anaphylaxis who completely respond to treatment are appropriate for discharge after an observation period (2-6 hours) in the ED. Advise these patients about symptoms of biphasic ana-phylaxis and to return to the ED at the earliest onset of symptoms in the next 72 hours.61 There are established clinical predictors for biphasic response; severity of the initial presentation, hypoten-sion, laryngeal edema, delayed or inadequate dosage of epineph-rine, and chronic beta-blocker medication use have been advanced as risk factors for a biphasic attack.52,62 Patients with these clinical features may thus be candidates for hospital observation. Those going home are commonly prescribed a 7-day course of an oral H1 antihistamine (either first or second generation, e.g., diphen-hydramine hydrochloride 50 mg every 6 hours) and H2 antihista-mine (e.g., ranitidine 150 mg every day).55 The select patients who present with moderate anaphylaxis symptoms may benefit from outpatient steroid therapy (prednisone 1 mg/kg/day for 7 to 10 days). Consider hospital admission for patients who present with protracted anaphylaxis, hypotension, airway involvement, pro-longed bronchospasm, and poor social support and for those who may be at risk for biphasic anaphylaxis.
Prevention
Emergency physicians can take an active role in educating patients under their care about allergy and anaphylaxis, arranging for specialty care follow-up, and prescribing epinephrine for self-administration in case of allergic emergency. The SAFE acronym (Seek support, Allergen identification and avoidance, Follow-up for specialty care, and Epinephrine for emergencies) is a useful reminder tool to use in providing care for patients with anaphy-laxis in the ED.63 Physicians should spend a few minutes to advise patients of risks for future anaphylactic attacks and the need to seek emergency care as quickly as possible at the first signs of another anaphylactic reaction. Discharge planning includes referral to a primary care physician or allergist for further diag-nostic workups and allergy management, a prescription for self-injectable epinephrine kits including education on how and when to self-administer, and a recommendation to carry a warning identification stating the hypersensitivity (MedicAlert bracelet or wallet card).
URTICARIA AND ANGIOEDEMA
Clinical Features
Urticaria and angioedema are common allergic presentations encountered in the ED.64,65 Urticaria (hives) is the clinical mani-festation of a wheal and flare (allergic) reaction, appearing as papules or wheals that are nonpitting, edematous, pruritic, slightly erythematous, and raised circular or annular; they range in size from millimeters to several centimeters (Fig. 119-3). The centers of the wheals are usually clear while the borders are erythematous,
the intramuscular route of administration for epinephrine, successful administration of epinephrine through the intraosse-ous, sublingual, intraglossal, and endotracheal routes has been reported anecdotally, although only the parenteral route is recommended in the 2010 anaphylaxis treatment guidelines.6 The dosage and concentration guidelines for these routes of adminis-tration of epinephrine are the same as those for intravenous administration.
Antihistamines
In addition to epinephrine, antihistamines are routinely used in the treatment of anaphylaxis. Through competitive blockade of circulating histamines at target tissue cell receptors, they theoreti-cally decrease symptoms of histaminemia such as itching, flush and rhinorrhea, and myocardial contractility, although they have no role in decreasing mediator release and have no effect on the leukotrienes. Diphenhydramine hydrochloride is the most com-monly used H1 antihistamine (50 mg intravenously or orally every 4 to 6 hours in adults or 1 to 2 mg/kg in children). Ranitidine (50 mg intravenously in adults, 1 mg/kg in children) and cimeti-dine (300 mg intravenously every 6 hours) are commonly used H2 blockers. Antihistamines should be not given as lone agents in the treatment of true anaphylaxis.
Corticosteroids
Along with epinephrine and antihistamines, systemic corticoste-roids are commonly administered in the treatment of anaphylaxis. A typical regimen involves an initial intravenous loading dose of methylprednisolone (Solu-Medrol, 125 to 250 mg) or oral pred-nisone (0.5-1 mg/kg). Steroids have an onset of action of approxi-mately 4 to 6 hours after administration and therefore are of limited benefit in the acute treatment. They are most useful for protracted symptoms and may confer theoretic benefits in pre-venting the biphasic reaction. Rare cases of deterioration after corticosteroid administration may be the result of the patient’s hypersensitivity reaction to steroid.
Aerosolized Beta-Agonists
Bronchospasm in anaphylaxis refractory to epinephrine may respond to a nebulized beta-agonist.6 Continuous nebulization of the beta-agonists (albuterol sulfate, levalbuterol) may be helpful for persistent bronchospasm. The use of anticholinergic therapy with ipratropium bromide (Atrovent, 0.5 mg [2.5 mL of a 0.02% solution]) is an additional option in the management of acute bronchospasm. Anticholinergic medications decrease cyclic gua-nosine monophosphate levels, thereby decreasing mediator release and reversing the action of mediators on target tissue cells.6
Vasopressors
Patients with persistent hypotension despite adequate epinephrine injections require aggressive volume expansion with crystalloid fluids. Large volumes of NS (>2 L) are often infused quickly, at a rate of 5 to 10 mL/kg for the first 5 minutes.6 Watch for signs of volume overload in patients with a history of reduced cardiac function, renal insufficiency, or congestive heart failure.6 As a last resort, dopamine, vasopressors (e.g., norepinephrine, phenyleph-rine), or vasopressin infusion (2-4 IU/hr) should be considered for refractory hypotension.6,60
Patients Receiving Beta-Blockade
Glucagon, with positive inotropic and chronotropic cardiac effects mediated independently of alpha and beta receptors, may be

1556 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
deficiency or functional deficiency, which is biochemically con-firmed by low levels of C4 and C1 esterase inhibitor activity.68 This ultimately results in intermittent elevated bradykinin levels and other mediators, resulting in angioedema. The cardinal symptoms and signs of HAE include edema of the airway, face, genitalia, or extremities and abdominal pain associated with nausea, vomiting, and diarrhea. These clinical manifestations may occur singly or in combination. Trauma and stress are common precipitating factors. There is usually a family history.
ACID is clinically indistinguishable from HAE attacks and is often associated with underlying lymphoproliferative diseases. The underlying disease results in consumption of C1 inhibitor or the development of anti–C1 inhibitor autoantibodies. It is less common than HAE, it typically involves older patients, and a family history is usually absent.
ACE inhibitor–induced angioedema has an incidence of 0.1 to 0.7% and has a predilection for the tongue, lips, and laryngeal soft tissue.69 The highest incidence occurs in the first month of therapy, but it can occur as many as 10 years after therapy is started. Increased risk factors include African American race, smoking, older age, and female gender. Diabetes decreases the risk. The pathophysiologic mechanism is thought to be related to decreased metabolism of bradykinin and substance P, both of which are potent mediators of tissue inflammation. Most patients who have angioedema while receiving ACE inhibitors should be able to tol-erate angiotensin receptor blocker drugs.
The clinical evaluation of angioedema starts with a focused search for emergency conditions, followed by a detailed history aimed at identification of the underlying cause. Life-threatening airway compromise can occur if the angioedema involves the upper airway. HAE, ACID, ACE inhibitors, thermal burn, and local allergic reaction to inhaled drugs (e.g., Quincke’s disease) tend to cause glossopharyngeal angioedema, resulting in upper airway obstruction, dysphagia, or both.70 The detailed history is aimed at eliciting exposures to foods, drugs, physical stimuli, infection (especially viral hepatitis), occupational elements, and insect stings.
Diagnostic Strategies
Diagnostic considerations are vast and include evolving anaphy-laxis syndrome, erythema multiforme minor, bullous pemphigoid and dermatitis herpetiformis, urticarial vasculitis, mastocytosis, HAE (C1 esterase deficiency), ACID, ACE inhibitor–associated angioedema, and serum sickness, among others. The constellation of pruritus, urticarial rash or angioedema, hypotension, and wheezing after exercise should raise the possibility of exercise-induced anaphylaxis. Angioedema of the upper extremity raises the possibility of superior vena cava syndrome. Brawny edema and shock raise the possibility of capillary leak syndrome.
Management
Angioedema with Urticaria
Management of allergic angioedema that occurs in conjunction with urticaria (mast cell related) is first focused on stabilization of respiratory insufficiency and hemodynamic instability. Antihista-mines (both H1 and H2) are the first-line therapeutic drugs. Epi-nephrine can be considered for moderate to severe cases but should be used with caution in patients older than 35 years to minimize the risk of precipitating an acute coronary syndrome. Steroids may be helpful in preventing recurrence. In the longer term, the most effective treatment of urticaria and angioedema involves removal of the etiologic factors. Second-generation H1
raised, and serpiginous. The erythema is due to dilation of blood vessels in the dermal layer of the skin, and the edematous wheals are due to transudation from these blood vessels. Urticaria favors the extremities and trunk and is usually transient, with crops of hives spontaneously appearing and resolving as often as every few hours.
Angioedema refers to abrupt vasodilation and edema and resul-tant swelling of the deeper dermal and subcutaneous layers of the skin. Because the swelling is located in the deeper layers of the skin, the skin may appear normal color (or pink) and pruritus is variable. Instead of itch, patients may complain of pain associ-ated with angioedema. Angioedema commonly involves the face, mouth, lips, tongue, extremities, and genitalia. Angioedema of the larynx can cause an acute upper airway obstruction and is a medical emergency. Recurrent episodes of angioedema and urticaria that last less than 6 weeks are considered acute (90%), and those that persist longer than 6 weeks are classified as chronic (10%).
Urticaria and angioedema represent clinical symptoms and signs of potentially distinct underlying disease entities. Similar to anaphylaxis, the majority of cases of acute urticaria and angio-edema are hypersensitivity reactions, commonly triggered by allergens (e.g., foods, drugs, RCM, Hymenoptera venoms) and, rarely, by physical stimuli (e.g., heat, wet, cold, vibratory, exercise). Angioedema caused by an allergic mechanism is called allergic angioedema. Nonallergic angioedema is caused by bradykinin excess, either by reduced degradation of bradykinin by ACE inhib-itors or by excessive bradykinin production by a genetic defect as in hereditary angioedema (HAE). Differentiation of the two forms of angioedema is crucial to successful therapy.
Nonallergic angioedema (angioedema without urticaria and pruritus) is usually kinin related; its causes include HAE, acquired C1 inhibitor deficiency (ACID), and ACE inhibitors. All three result in elevated bradykinin levels.66 In the case of HAE and ACID, the deficiency of C1 inhibitor causes activation of the kallikrein-kinin system, with consumption of kininogen, and results in increased production of bradykinin. In the case of ACE inhibitor drugs, the inhibition of ACE, one of the main inactiva-tors of bradykinin, results in increased bradykinin levels.67 Sub-stance P is also thought to play a role in ACE inhibitor–associated angioedema.
HAE affects fewer than 200,000 people in the United States and may account for 15,000 to 30,000 ED visits annually. It is an autosomal dominant condition caused by C1 esterase inhibitor
Figure 119-3. Acute urticaria. (Copyright © 2001-2003, Johns Hopkins University School of Medicine. http://dermatlas.med.jhmi.edu/derm.)

Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1557
MASTOCYTOSIS
Mastocytosis is a rare disorder caused by an abnormal prolifera-tion of mast cells (hyperplasia) in the body. There are two forms of mastocytosis. Cutaneous mastocytosis, also called urticaria pig-mentosa, occurs when mast cell hyperplasia is in the skin. Cutane-ous mastocytosis is more common and affects mostly children. Systemic mastocytosis refers to the clinical syndrome caused by mast cell hyperplasia in bone marrow, gut mucosa, liver, or spleen. Pathologic fractures, osteoblastic lesions on skeletal radiographs, cutaneous pigmented lesions, abdominal pain, diarrhea, hepato-splenomegaly, lymphadenopathy, headache, flushing, anemia, and, rarely, vascular collapse (from released vasoactive substances) are common clinical findings in systemic mastocytosis. The diagnosis is made by a 24-hour urine collection for histamine or its metabo-lites, PGD2, or serum tryptase level. Adjunct diagnostic measures include bone scans, skeletal surveys, and upper gastrointestinal workup (upper gastrointestinal series, small bowel radiograph, computed tomography scan, and endoscopy). A skin or bone marrow biopsy helps confirm the diagnosis. Treatment options include avoidance of agents that precipitate a mediator release (such as aspirin, NSAIDs, opioids, and RCM) and referral to an allergist. Temporizing treatment in the ED includes H1 and H2 antihistamines for pruritus, flush, and gastrointestinal symptoms; potent topical steroids (class 1) can also be used for limited cuta-neous mastocytosis.
antihistamines such as cetirizine, loratadine, and fexofenadine, at increased doses (up to fourfold the conventional doses for aller-gic rhinitis), are the first-line drugs.71 The older antihistamines (hydroxyzine and diphenhydramine) can be tried when the newer H1 antihistamines are ineffective. Because 85% of histamine recep-tors in the skin are H1 and 15% are H2, the addition of an H2 antihistamine (e.g., ranitidine or cimetidine) benefits a histamine-induced urticarial reaction. Besides those common antihistamines, low-dose tricyclics (e.g., doxepin 25-100 mg/day) have both H1 and H2 activity and are used as second-line drugs, especially in cases of chronic urticaria.72 Heavy sedating effects limit the useful-ness of doxepin, however. The addition of a short course of cor-ticosteroids (0.5 mg/kg daily, up to 1 week) may shorten the duration of acute urticaria.71
Angioedema without Urticaria
Management of angioedema that occurs without urticaria (kinin related) is somewhat more of a problem with fewer therapeutic options.73,74 Life-threatening acute attacks of kinin-related angio-edema do not usually respond satisfactorily to treatment with epinephrine, antihistamines, or steroids.75,76 Active airway man-agement is the mainstay of treatment. Aerosolized racemic epi-nephrine (l-epinephrine is acceptable) may help stabilize the airway edema. Several new agents have recently been approved by the FDA for use in the United States; several others either are being used in other countries or are under clinical trial for the treatment of HAE.
For HAE, fresh frozen plasma (FFP), which contains C1 inhibi-tor, has been reported to be effective in abolishing acute attacks; however, there are rare reports of exacerbation of the angioedema by FFP. Steroids have not been shown to be helpful during acute attacks of HAE and should not be used.68
The use of C1 inhibitor replacement protein (C1-INHRP), a product of pooled human plasma, is the recommended treatment of HAE.73 Currently, two C1-INHRP drugs are approved by the FDA for the treatment of HAE: Berinert (20 units/kg intra-venously) and Cinryze (1000 units intravenously for patient weighing 50 to 100 kg).73 Recombinant C1-INHRP has been developed and is under review in North America for the treatment of HAE. Both types of products have been shown to shorten time to relief of symptoms, but the recombinant product has a shorter half-life.
Ecallantide (Kalbitor, 30 mg subcutaneously) is a small peptide kallikrein inhibitor and prevents the generation of bradykinin.73 It has been approved for use in the United States since 2009. It should not be used intravenously because of a reported 3.9% risk of anaphylaxis. A bradykinin receptor-2 antagonist (Icatibant) has been approved by the European Medicines Agency for use in the European Union but has not been approved for use in North America.
For ACE inhibitor–induced angioedema, the treatment is mainly supportive. There is a report of FFP being used with success in severe cases of ACE inhibitor–induced angioedema.77 It is thought that the benefits conferred by FFP are due to the effect of kininase II in breaking down the accumulated bradykinin. Because elevation in bradykinin is observed in both ACE inhibitor–induced angioedema and HAE (among others), perhaps the bra-dykinin receptor blocker class of drug that is being evaluated for HAE may also be found to be effective in the treatment of ACE inhibitor–induced angioedema.
■ Anaphylaxis is a life-threatening systemic allergic reaction of acute onset and multiorgan involvement; timely recognition and treatment are essential to maximize good outcomes.
■ A history of sudden urticarial rash after an exposure, accompanied by either respiratory difficulty or hypotension, strongly favors the diagnosis of anaphylaxis.
■ The treatment triad in anaphylaxis includes establishment of a patent airway, early treatment with epinephrine, and aggressive volume expansion with normal saline.
■ H1 and H2 antihistamines seem helpful in reducing pruritus, rhinorrhea, and the flush syndrome in anaphylaxis. Corticosteroids can be helpful in reducing the risks of a protracted anaphylactic reaction and biphasic anaphylaxis.
■ Continuous intravenous infusion of epinephrine may be needed in refractory anaphylactic shock after adequate volume expansion and multiple doses of intramuscular epinephrine. Prolonged treatment with epinephrine or glucagon may be required for patients receiving beta-adrenergic blockade.
■ Consider hospitalization or prolonged observation for patients who have experienced hypotension, upper airway involvement, and prolonged bronchospasm.
■ The SAFE acronym (Seek support, Allergen identification and avoidance, Follow-up for specialty care, and Epinephrine for emergencies) is a useful framework for discharge planning.
■ Nonallergic angioedema is treated with supportive therapy. FFP has been used with varying success in HAE, ACID, and ACE inhibitor–induced angioedema. New drugs, including Berinert and Cinryze, and ecallantide have been approved for use in HAE-induced angioedema.
KEY CONCEPTS
The references for this chapter can be found online by accessing the accompanying Expert Consult website.
Chapter 119 / Allergy, Hypersensitivity, Angioedema, and Anaphylaxis 1557.e1
References
1. Matzinger P: Tolerance, danger, and the extended family. Annu Rev Immunol 1994; 12:991-1045.
2. Simons FE: Anaphylaxis. J Allergy Clin Immunol 2010; 125(Suppl 2):S161-S181.
3. Golden DB: What is anaphylaxis? Curr Opin Allergy Clin Immunol 2007; 7:331-336.
4. Lieberman P: Epidemiology of anaphylaxis. Curr Opin Allergy Clin Immunol 2008; 8:316-320.
5. Lieberman P: Anaphylaxis. Med Clin North Am 2006; 90:77-95, viii.6. Lieberman P, et al: The diagnosis and management of anaphylaxis
practice parameter: 2010 update. J Allergy Clin Immunol 2010; 126:477-480.
7. Simons FE: Anaphylaxis in infants: Can recognition and management be improved? J Allergy Clin Immunol 2007; 120:537-540.
8. Kemp SF, Lockey RF, Wolf BL, Lieberman P: Anaphylaxis. A review of 266 cases [see comments]. Arch Intern Med 1995; 155:1749-1754.
9. Kemp SF, Lockey RF: Anaphylaxis: A review of causes and mechanisms. J Allergy Clin Immunol 2002; 110:341-348.
10. Armentia A, Pineda F, Fernández S: Wine-induced anaphylaxis and sensitization to Hymenoptera venom. N Engl J Med 2007; 357:719-720.
11. Castillo R, Delgado J, Quiralte J, Blanco C, Carrillo T: Food hypersensitivity among adult patients: Epidemiological and clinical aspects. Allergol Immunopathol (Madr) 1996; 24:93-97.
12. Wuthrich B, Ballmer-Weber BK: Food-induced anaphylaxis. Allergy 2001; 56(Suppl 67):102-104.
13. Salkind AR, Cuddy PG, Foxworth JW: The rational clinical examination. Is this patient allergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. JAMA 2001; 285:2498-2505.
14. Gadde J, Spence M, Wheeler B, Adkinson NF Jr: Clinical experience with penicillin skin testing in a large inner-city STD clinic. JAMA 1993; 270:2456-2463.
15. Kaufman DW: Risk of anaphylaxis in a hospital population in relation to the use of various drugs: An international study. Pharmacoepidemiol Drug Saf 2003; 12:195-202.
16. Mayorga C, Torres MJ, Blanca M: Cephalosporin allergy. N Engl J Med 2002; 346:380-381.
17. Goodman EJ, et al: Cephalosporins can be given to penicillin-allergic patients who do not exhibit an anaphylactic response. J Clin Anesth 2001; 13:561-564.
18. Freeman TM: Clinical practice. Hypersensitivity to Hymenoptera stings. N Engl J Med 2004; 351:1978-1984.
19. Neugut AI, Ghatak AT, Miller RL: Anaphylaxis in the United States: An investigation into its epidemiology. Arch Intern Med 2001; 161:15-21.
20. Rhoades R: Stinging ants. Curr Opin Allergy Clin Immunol 2001; 1:343-348.
21. Schumacher MJ, Egen NB: Significance of Africanized bees for public health. A review. Arch Intern Med 1995; 155:2038-2043.
22. Decker WW, et al: The etiology and incidence of anaphylaxis in Rochester, Minnesota: A report from the Rochester Epidemiology Project. J Allergy Clin Immunol 2008; 122:1161-1165.
23. Fisher M: Anaphylaxis to anaesthetic drugs. Novartis Found Symp 2004; 257:193-202.
24. Kajimoto Y, et al: Anaphylactoid skin reactions after intravenous regional anaesthesia using 0.5% prilocaine with or without preservative—a double-blind study. Acta Anaesthesiol Scand 1995; 39:782-784.
25. Fisher MM, Harle DG, Baldo BA: Anaphylactoid reactions to narcotic analgesics. Clin Rev Allergy 1991; 9:309-318.
26. Huang SW: Seafood and iodine: An analysis of a medical myth. Allergy Asthma Proc 2005; 26:468-469.
27. Cochran ST: Anaphylactoid reactions to radiocontrast media. Curr Allergy Asthma Rep 2005; 5:28-31.
28. Kong JS, Teuber SS, Gershwin ME: Aspirin and nonsteroidal anti-inflammatory drug hypersensitivity. Clin Rev Allergy Immunol 2007; 32:97-110.
29. Ramanuja S, Breall JA, Kalaria VG: Approach to “aspirin allergy” in cardiovascular patients. Circulation 2004; 110:e1-e4.
30. Wong JT, Nagy CS, Krinzman SJ, Maclean JA, Bloch KJ: Rapid oral challenge-desensitization for patients with aspirin-related urticaria-angioedema. J Allergy Clin Immunol 2000; 105:997-1001.
31. Simon RA: Adverse reactions to food additives. N Engl Reg Allergy Proc 1986; 7:533-542.
32. Borchers AT, Keen CL, Gershwin ME: Fatalities following allergen immunotherapy. Clin Rev Allergy Immunol 2004; 27:147-158.
33. Butani L: Corticosteroid-induced hypersensitivity reactions. Ann Allergy Asthma Immunol 2002; 89:439-445.
34. Robson-Ansley P, Toit GD: Pathophysiology, diagnosis and management of exercise-induced anaphylaxis. Curr Opin Allergy Clin Immunol 2010; 10:312-317.
35. Patterson R, Hogan MB, Yarnold PR, Harris KE: Idiopathic anaphylaxis. An attempt to estimate the incidence in the United States. Arch Intern Med 1995; 155:869-871.
36. Greenberger PA: Idiopathic anaphylaxis. Immunol Allergy Clin North Am 2007; 27:273-293, vii-viii.
37. Fischer A, Groneberg DA, Moehring R, Hallett R, Teuber SS: Kissing and food reactions. N Engl J Med 2002; 347:1210.
38. Webb LM, Lieberman P: Anaphylaxis: A review of 601 cases. Ann Allergy Asthma Immunol 2006; 97:39-43.
39. Zhang Q, et al: Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature 2010; 464:104-107.
40. Janeway CA Jr: Approaching the asymptote? Evolution and revolution in immunology. Cold Spring Harb Symp Quant Biol 1989; 54(Pt 1):1-13.
41. Delves PJ, Roitt IM: The immune system. Second of two parts. N Engl J Med 2000; 343:108-117.
42. Delves PJ, Roitt IM: The immune system. First of two parts. N Engl J Med 2000; 343:37-49.
43. Chaplin DD: Overview of the immune response. J Allergy Clin Immunol 2010; 125(Suppl 2):S3-S23.
44. Weiss ST: Eat dirt—the hygiene hypothesis and allergic diseases. N Engl J Med 2002; 347:930-931.
45. Kaliner M, Shelhamer JH, Ottesen EA: Effects of infused histamine: Correlation of plasma histamine levels and symptoms. J Allergy Clin Immunol 1982; 69:283-289.
46. Constantinides P: Infiltrates of activated mast cells at the site of coronary atheromatous erosion or rupture in myocardial infarction. Circulation 1995; 92:1083.
47. Incorvaia C, Mauro M, Pravettoni V, Incorvaia S, Riario-Sforza GG: Anaphylaxis: An update on its understanding and management. Recent Pat Inflamm Allergy Drug Discov 2010; 4:124-129.
48. Yost CC, Weyrich AS, Zimmerman GA: The platelet activating factor (PAF) signaling cascade in systemic inflammatory responses. Biochimie 2010; 92:692-697.
49. Felix SB, et al: Characterization of cardiovascular events mediated by platelet activating factor during systemic anaphylaxis. J Cardiovasc Pharmacol 1990; 15:987-997.
50. Peavy RD, Metcalfe DD: Understanding the mechanisms of anaphylaxis. Curr Opin Allergy Clin Immunol 2008; 8:310-315.
51. The diagnosis and management of anaphylaxis: An updated practice parameter. J Allergy Clin Immunol 2005; 115(Suppl 2):S483-S523.
52. Tole JW, Lieberman P: Biphasic anaphylaxis: Review of incidence, clinical predictors, and observation recommendations. Immunol Allergy Clin North Am 2007; 27:309-326, viii.
53. Ellis AK, Day JH: Incidence and characteristics of biphasic anaphylaxis: A prospective evaluation of 103 patients. Ann Allergy Asthma Immunol 2007; 98:64-69.
54. Sampson HA, et al: Symposium on the definition and management of anaphylaxis: Summary report. J Allergy Clin Immunol 2005; 115:584-591.
55. Simons FE, Simons KJ: Epinephrine (adrenaline) in anaphylaxis. Chem Immunol Allergy 2010; 95:211-222.
56. Heilborn H, Hjemdahl P, Daleskog M, Adamsson U: Comparison of subcutaneous injection and high-dose inhalation of epinephrine—implications for self-treatment to prevent anaphylaxis. J Allergy Clin Immunol 1986; 78:1174-1179.
57. Choo KJ, Simons E, Sheikh A: Glucocorticoids for the treatment of anaphylaxis: Cochrane systematic review. Allergy 2010; 65:1205-1211.
58. Sheikh A, ten Broek V, Brown SG, Simons FE: H1-antihistamines for the treatment of anaphylaxis with and without shock. Cochrane Database Syst Rev 2007; 1:CD006160.
59. Simons FE: Anaphylaxis: Recent advances in assessment and treatment. J Allergy Clin Immunol 2009; 124:625-636.
60. Schummer C, Wirsing M, Schummer W: The pivotal role of vasopressin in refractory anaphylactic shock. Anesth Analg 2008; 107:620-624.
61. Kemp SF: The post-anaphylaxis dilemma: How long is long enough to observe a patient after resolution of symptoms? Curr Allergy Asthma Rep 2008; 8:45-48.
62. Brady WJ Jr, Luber S, Carter CT, Guertler A, Lindbeck G: Multiphasic anaphylaxis: An uncommon event in the emergency department. Acad Emerg Med 1997; 4:193-197.
63. Lieberman P, et al: SAFE: A multidisciplinary approach to anaphylaxis education in the emergency department. Ann Allergy Asthma Immunol 2007; 98:519-523.
64. Dibbern DA Jr: Urticaria: Selected highlights and recent advances. Med Clin North Am 2006; 90:187-209.

1557.e2 PART III ◆ Medicine and Surgery / Section Nine • Immunologic and Inflammatory
65. Kaplan AP, Greaves MW: Angioedema. J Am Acad Dermatol 2005; 53:373-388.
66. Cugno M, Nussberger J, Cicardi M, Agostoni A: Bradykinin and the pathophysiology of angioedema. Int Immunopharmacol 2003; 3:311-317.
67. Byrd JB, Adam A, Brown NJ: Angiotensin-converting enzyme inhibitor–associated angioedema. Immunol Allergy Clin North Am 2006; 26:725-737.
68. Zuraw BL: Clinical practice. Hereditary angioedema. N Engl J Med 2008; 359:1027-1036.
69. Slater EE, et al: Clinical profile of angioedema associated with angiotensin converting-enzyme inhibition. JAMA 1988; 260:967-970.
70. Kestler A, Keyes L: Images in clinical medicine. Uvular angioedema (Quincke’s disease). N Engl J Med 2003; 349:867.
71. Zuberbier T, et al: EAACI/GA2LEN/EDF/WAO guideline: Management of urticaria. Allergy 2009; 64:1427-1443.
72. Greene SL, Reed CE, Schroeter AL: Double-blind crossover study comparing doxepin with diphenhydramine for the treatment of chronic urticaria. J Am Acad Dermatol 1985; 12:669-675.
73. Bowen T, et al: 2010 International consensus algorithm for the diagnosis, therapy and management of hereditary angioedema. Allergy Asthma Clin Immunol 2010; 6:24.
74. Bowen T: Hereditary angioedema: Beyond international consensus—circa December 2010. Allergy Asthma Clin Immunol 2011; 7:1.
75. Nielsen EW, Gramstad S: Angioedema from angiotensin-converting enzyme (ACE) inhibitor treated with complement 1 (C1) inhibitor concentrate. Acta Anaesthesiol Scand 2006; 50:120-122.
76. Caballero T, et al: Consensus statement on the diagnosis, management, and treatment of angioedema mediated by bradykinin. Part I. Classification, epidemiology, pathophysiology, genetics, clinical symptoms, and diagnosis. J Investig Allergol Clin Immunol 2011; 21:333-347.
77. Warrier MR, Copilevitz CA, Dykewicz MS, Slavin RG: Fresh frozen plasma in the treatment of resistant angiotensin-converting enzyme inhibitor angioedema. Ann Allergy Asthma Immunol 2004; 92:573-575.