Chapter 10 Diseases of Salivary glands. Consists of three paired major S.Gs which are...
55
Chapter 10 Diseases of Salivary glands
-
Upload
prosper-sims -
Category
Documents
-
view
215 -
download
0
Transcript of Chapter 10 Diseases of Salivary glands. Consists of three paired major S.Gs which are...

Chapter 10
Diseases of Salivary glands

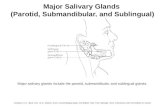
• Consists of three paired major S.Gs which are parotid ,submandibular & sublingual.
• Also countless minor S.Gs found in almost every part of the oral cavity , except the gingival & anterior regions of the hard palate.
• The secretion of saliva is essential for the normal function & health of the mouth & disorder of salivary gland function , which affect the composition , & secretion of saliva predispose to oral disease.
• Functional disorders in salivary secretion & composition may be associated with organic disease of the salivary glands but in other cases are caused by systemic factors such as neurological disease.
• Due to change of the amount of salivary secretion ( as a symptom) but not a disease two conditions could occur :
• 1- Xerostomia ( dry mouth) : it can be caused by : • - Developmental ( aplasia & atresia ) • - Medication – several hundred current medications can cause xerostomia . The
major drug groups are antihypertensives & antidepressants. Analgesics , tranquilizers , diuretics , & antihistamines can also cause dry mouth.
• - Cancer therapy – chemotherapeutic drugs can change the flow & composition of

Causes of xerostomia

• Of the saliva. Radiation treatment that is focused on or near the salivary gland can temporarily or permanently damage the salivary glands.
• - Sjogren,s syndrome ; an autoimmune disease , causes xerostomia & dry eyes.• - Other conditions such as bone transplants , endocrine disorders , stress , anxiety ,
depression , & nutritional deficiencies may cause xerostomia.• - Nerve damage – trauma to the head & neck area from surgery or wounds can
damage the nerves that supply sensation to the mouth. While the salivary glands may be left intact , they can not function normally without the nerves that signal them to produce saliva.
• - Conditions like Alzheimer,s disease or stroke may change the ability to perceive oral sensations.
• 2- Ptyalism : Excessive salivary secretion may be due to : • - Local reflexes such as : oral infections (acute ulcerative gingivitis) , oral wounds ,
dental procedures , new dentures.• - Systemic such as : nausea , acid regurgitation ( reflex esophagitis) • - Toxic : iodine , heavy metal poisoning .• - False ptyalism : psychogenic , bell,s palsy , Parkinson,s disease.

Causes of ptyalism

• Classification of S.G diseases : • 1- Developmental : Aplasia , Atresia , Aberrancy.• 2- Inflammatory : i- Bacterial sialadenitis : acute & chronic types.• ii- Viral sialadenitis (mumps , cytomegalic inclusion
disease) • iii- Post - irradiation sialadenitis.• 3- Obstructive & traumatic conditions : • i- Salivary calculi • ii- Cysts of S.G. (mucous retention & mucous extravasation cysts)• 4- Autoimmune disorder : Sjogren,s syndrome• 5- Hypertrophic : • *non-neoplastic , non-inflammatory conditions as sialadenosis.• 6- Neoplastic : i - Epithelial neoplasms ( benign & malignant ).• ii- Non- epithelial ( lymphomas , sarcomas).

• Inflammatory S.G. diseases : • 1- Acute bacterial sialadenitis (| suppurative parotitis) : • This suppurative infection is most common in the parotid gland , & is usually
caused by staphylococcus aureus , streptococcus pyogens , S.pneumonia, E.coli , H . influenza .
• Clinical picture : adult age , both sex , bilateral parotid common site.• Characters : • - Patients have a sudden onset of a painful diffuse swelling of the involved gland ,
redness of the gland , regional lymphadenopathy & fever.• - Post operative sialadenitis typically occur 4-5 days after a gastrointestinal
procedure where the patient may be dehydrated , have poor oral hygiene , not be eating , & may be debilitated.
• - It occurs also in patients with Sjogren,s syndrome or under antidepressant treatment
• Investigations : • 1- physical examination including : • - Palpate the glands ( diffusely swollen)• - Milk saliva from duct by massaging the gland – typically purulent .

Suppurative parotitis - pus is leaking from the parotidpapilla

• 2- cultures : culture saliva from duct opening: aerobic , anaerobic gram stain.• 3- imaging : • - if slow to resolve , do a CT scan or U/S which may show an abscess.• - Abscesses are not fluctuant in the parotid gland because of multiple septations in
the gland.• 4- Histopathology : • -increase inflammatory cells infiltrate of acute type.• - Abscesses formation with acinar desctruction.• 2- Chronic bacterial sialadenitis : • It is a chronic condition , which is usually due to salivary calculi.• Etiology : as a complication of duct obstruction.• Clinical picture : old age , both sexes , site : submandibular salivary gland.• - Asymptomatic or chronic intermittent pain• - Unilateral swelling of the gland.• - Sometimes the gland is tender.• Investigations : sialography shows dilatation of ducts behind the obstruction.

Chronic sialadenitis resulting from obstruction. The ductscontain casts of mucin and neutrophils and are surrounded by a layer of fibrosis. There is severe acinar atrophy and the space previously occupied by acinar cells now contains infiltrates of lymphocytes and plasma cells.

• Histopathology : • - Duct dilatation & calculus formation.• - Acinar destruction & atrophy.• - Fibroses of the gland.• - Chronic inflammatory cells mainly lymphocytes.• 3- Viral sialadenitis ( mumps-epidemic parotitis) : • A viral infection mainly attacks the parotid glands, caused by Paramyxo virus• Clinically : usually children , both sexes , site : parotid glands.• Characters : • - Painful glands leading to the classic swollen cheek appearance• - low grade fever , mild headach , loss of appetite & abdominal pain. • The symptoms usually go away within ten days.• Complications : • 1- Swelling of testes along with high fever , & considerable pain . Sterility is very
rare after a testicular infection even if both testes are involved. • 2- Mumps virus meningitis , it is not a serious problem as bacterial meningitis .
Usually patients with mumps meningitis recover without permanent damage.• Vaccination as a part of MMR – Measles –Mumps - Rubella

• 4- Cytomegalic inclusion disease• A salivary gland inclusion disease , caused by cytomegalo virus which is a member
of the herpes virus group.• Clinically : neonates & immunocompressed subjects such as transplant patients &
HIV infected patients , affects both sexes , site : parotid gland.• Characters : • Asymptomatic but xerostomia may occur.• In neonates & debilitated patients severe dissemminated disease similar inclusions
frequently occur in the kidneys , lungs , brain & other organs.• Histopathology : Characteristic feature with presence of large , doubly contoured
( owl – eye) inclusion bodies within the nucleus or cytoplasm of duct cells of the parotid gland.
• 5- Post- irridiation sialadenitis : it is common complication of radiotherapy & there is a direct correlation between the doze of irradiation & the severity of the damage.
• Characters : xerostomia • Histopathology : ( irreversible )1- fibrous replacement of the damaged acini• 2- Squamous metaplasia of ducts• 3- Serous acini are more sensitive than mucous acini

• Obstructive & traumatic conditions:
• 1- Sialolithiasis : presence of calculi form in the salivary duct blocking the egress of saliva.
• Pathogenesis : unknown but may be due to deposition of calcium salts around an initial organic nidus ( altered salivary mucin , desquamated epithelial cells or microorganisms. Succesive deposition of inorganic & organic materials would produce lamellated calculus.
• Clinical picture: middle age adult , both sexes , Site : submandibular gland duct 85% of cases , parotid gland 10-15% while in the submandibular is about 1%
• Characters : Unilateral painful swelling in the submandibular gland which worsens with meals ( gustatory stimuli) with reccurent attacks.
• Investigations : • 1- physical exam. Including palpation of the gland & the duct . The stone may be
round or ovoid , rough or smooth , with varying sizes.• 2- Imaging : • X – Ray : 90% submandibular calculi are radiopaque , 90% of parotid calculi are
radiolucent• - Sialography - U/S - CT scan ( more sensitive than X ray )

Salivary calculus. This stone has impacted just behind the orifice of the submandibular duct forming a hard nodule. The yellow colour of the stone is visible through the thin mucosa.
Salivary calculus in a duct. To the left is the salivary calculus which has a lamellar structure and an irregular surface. On the surface is a thick layer of microbial flora filling the space between the stone and the epithelial lining. In the surrounding wall there is an infiltrate oflymphocytes and plasma cells and neutrophils are migrating through the duct epithelium into the lumen.

Salivary calculi:

• 2- Cysts of salivary glands : • 1- mucous retension cyst : true cyst with epithelial lined cavity occurring in the
minor salivary glands.• Pathogenesis : chronic partial obstruction of salivary flow , could be due to : • - Small piece of intraductal calculus.• - Contraction of developing scar of C.T. around the duct after • traumatic injury.• Clinical features : old age , equal sexes , Site : palate , cheek , floor of the mouth ,
maxillary sinus ( minor S.G areas).• Characters : • - Asymptomatic painless swelling , • - often with previous trauma ,• - size varies from 3mm to 1cm , • - not tender & freely mobile on palpation , • - covered by normal coloured & intact mucosa , • - deeper lesions tend to be firm & more diffuse , • - when a sinus is involved , the lesion appears as semilunar radiopacity along the
floor of the sinus.

• Histopathology : • 1- Epithelium lined the cavity , it is the ductal epithelium ( the lining epithelium
ranges from pseudostratified to double layer of columnar or cuboidal cells ).• 2- Cyst lumen contain variable amount of mucoid secretion.• 3- Salivary stones ( sialolithiasis ) & mucous plugs may be seen within the duct
system.• 4- C.T. wall is typically free from chronic inflammatory cells.• Treatment : Complete excision with associated lobules of minor S.G. • Treatment : complete excision of the cyst

Mucous retention cyst. Remnants of the minor mucous salivary glands are visible, together with their dilated duct, the epithelium of which is continuous with the epithelial lining of the cyst (above).

• 2- Mucous extravasation cyst ( mucocele) : • Cyst occurs in minor S.Gs & is characterized by pooling of mucin in C.T. stroma of
the gland with formation of granulation tissue around that mucin pool ( i.e. pseudocyst).
• Pathogenesis : • - Etiology is related to mechanical trauma to minor S.G by biting the lip or cheek or
by pinching the lip by extraction forceps resulting in injury of the duct of that gland.
• - This will result in pooling of the mucous into the surrounding C.T. stroma.• - This pool will elicit an inflammatory reaction in the surrounding C.T. in the form
of PMN leukocytes aggregation followed by macrophages infiltrating the area.• - This granulation tissue response will gives rise to a cavity containing mucin &
walled by granulation tissue giving a pseudocyst appearance.• - The adjacent S.G tissue will undergo a secondary non-specific inflammatory
response.• Clinically : Children & young adult , equal sexes , site : minor S.Gs areas ; lower lip
most common , buccal mucosa , ventral surface of the tongue ( Blandin – Nuhn glands) , floor of the mouth & retromolar area.

• Characters : • 1- Superficial lesions : Painless , smooth surfaced , bluish coloration , translucency
& range from mms to few cms.• 2- Deep lesions : Painless , diffuse swelling with no bluish hue. The lesion as
general may decrease in size due to engulfing of the pooled mucin but continuous production of mucin leads to fluctuation ( increase & decrease) in the size of the cyst. Maximum size of that cyst is usually reached within days & aspiration reveals a viscous material.
• Histopathology : • 1- well circumscribed cavity containing mucin ( pooled mucin) • 2- mucin pool is surrounded by a thin mass of compressed fibrous & granulation
tissue heavily infiltrated by neutrophils , macrophages , lymphocytes & plasma cells.
• 3- The adjacent salivary tissue show ductal dilation & acinar degeneration.• 4- When the lesion is superficial , the overlying oral epithelium become thinned &
separated from the mucin pool by a thin layer of compressed granulation tissue.• D.D. : 1- S.G neoplasms 2- Vascular malformation 3- Venous varices • 4- Soft tissue neoplasms • Treatment by surgical excision.

Mucous extravasation cyst. The typical presentation at the commonest site: a rounded bluish, translucent cyst in the lower lip.
Extravasation mucocele. To the left is a cavity of spilt mucin with the remnants of the ruptured duct lining epithelium at its edge. To the right is the associated minor mucous salivary gland. A, saliva and macrophages; B, compressed connective tissue wall; C, minor salivary gland.

• Ranula• A ranula is an uncommon type of salivary cyst arising from the sublingual or
submandibular salivary glands• The structure is usually the same as other salivary retention cysts. • Ranulae are usually unilateral and 2 or 3 cm in diameter• Occasionally they extend across the whole of the floor of the mouth. • They are soft, fluctuant and bluish. • They are typically painless but may interfere with speech or mastication.• Treatment is preferably by marsupialisation with removal of the related gland. • A simple incision leads to recurrence, and enucleation is difficult because of the
very thin wall.

Ranula. A large bluish, translucent swelling in the floor of the mouth caused by a mucous extravasation or retention cyst.
Extravasation mucocele. Higher power showing the lining of the mucin-filled space. Macrophages are migrating into the mucin and in phagocytosing it develop a foamy or vacuolated cytoplasm.

• Autoimmune Disorder : • Sjogren,s syndrome : • It is an autoimmune disease , characterized by the abnormal production of extra
antibodies in the blood that are directed against various tissues of the body . This particular autoimmune illness is caused by inflammation of the gland of the body.
• Etiology & pathogenesis : The exact cause is unknown , but may be inherited. It is sometimes found in other family members. It is also found more commonly in families that have members with other autoimmune illness , such as systemic lupus erythematosus , autoimmune thyroid disease & juvenile diabetes.
• Classification : • Primary Sjogren syndrome : dryness of the eyes & mouth.• Secondary Sjogren syndrome : not only gland inflammation but is associated also
with a C.T. disease such as rheumatoid arthritis , systemic lupus , erythematosus or scleroderma.
• Clinically : Age : 40 years , Sex : female , site : • primary : eye & mouth• Secondary : glandular & exraglandular

• Characters : • 1- Eye : inflammation of lacrimal gland which lead to eye
dryness , irritation , decrease tear production “ gritty” sensation , infection & serious abrasion of cornea.
• 2- Oral manifestations : inflammation of the S.G. lead to mouth dryness , swallowing difficulties , dental decay , gum disease , sore mouth , disturbed taste sensation , disturbed quality of speech & infection ( candida).
• 3- Extraglandular : arthritis , lung inflammation , lymph node enlargement , kidney , nerve & muscle disease.
• A rare serious complication of Sjogren,s syndrome is vasculitis which can damage the tissues of the body that are supplied by these vessels.

Sjogren's syndrome. Extensive cervical caries is a frequent complication of dry mouth. In addition to the lack of saliva, patients may attempt to stimulate salivary flow with sweets or chewing gums.
Salivary gland swelling in primary Sjogren's syndrome. The outline of the parotid gland is clearly demarcated.

Sjogren's syndrome. The sialogram shows the typical snowstorm appearance of blobs of contrast medium that have leaked from the duct system. Emptying and clearance of the contrast medium are also much delayed because of the reduced salivary flow.

• Histopathology : • Replacement of the whole gland by a dense lymphocytic infiltrate.• The infiltrate remains confined within the gland capsule & does not cross the
intraglandular septa.• Investigations : • - Salivary flow rate : diminished• - Labial salivary gland biopsy : periductal lymphocytes infiltrate• - Antibody screen especially rheumatoid factor.• - Tear secretion flow : diminished.• Treatment ( irreversible salivary gland damage) • - Pilocarpine : stimulate salivary flow• - Artificial saliva : such as gastric mucin , xylitol or sodium fluoride with
preservatives & flavouring.• - Artificial tears• - Caries control & provide good oral hygiene • - treat difficulties with dentures.

Sjogren's syndrome. The histological appearance is typical. Dense, well-defined foci of lymphocytes surround the larger ducts in the centre of the lobules. In the area occupied by the lymphocytes there is complete acinar atrophy and a rim of residual salivary parenchyma remains around the periphery of the lobule.
Sjogren's syndrome. In late disease no salivary acini remain and the gland is replaced by a confluent infiltrate of lymphocytes. A few ducts remain and proliferate to form the epimyoepithelial islands. Suchextensive changes sometimes suggest that there has been progression to a low-grade lymphoma.

• Non neoplastic , non-inflammatory enlargement of salivary glands ( Sialadenosis)• Caused by : • - Chronic alcoholism • - Diabetes mellitus• - Endocrine diseases • - pregnancy• - Drug sympathomimetics• - Idiopathic• Clinical features : old age , sex : male , Site : parotid gland• Characters : recurrent swelling bilateral• Histopathology : • Hypertrophy of serous acini : dense granules in the cytoplasm.

• Salivary gland Neoplasm • Second neoplasm of the mouth after Squamous cell carcinoma, mainly caused by
irradiation.• Classification : I) Adenomas • A) Pleomorphic adenoma• B) Monomorphic adenoma • C) Adenolymphoma• D) Oxyphilic adenoma II) Carcinomas • A) Mucoepidermoid carcinoma• B) Acinic cell carcinoma• C) Adenoid cystic carcinoma III) Non-epithelial neoplasm• D) Adenocarcinoma A- lymphoma• E) Epidermoid carcinoma B- Sarcomas• F) Undifferentiated carcinoma• G) Carcinoma in pleomorphic adenoma

Benign S.Gs tumoursMalignant S.G.s tumours
- Slow growing - Soft or rubbery consistancy- 85% of parotid tumours are benign - Do not ulcerate - No associated nerve signs
- Sometimes fast growing - Sometimes hard consistancy- 45% of minor gland tumours are malignant- May ulcerate & invade bone - May cause cranial nerve palsies
* Malignant parotid tumours can cause facial palsy in particular. Adenoid cystic carcinoma can cause multiple cranial nerve lesions especially of lingual , facial or hypoglossal nerves.
General clinical features of S.Gs tumours : Age : adult , sex : female more than maleSite : - intraoral site : palate ( junction between hard & soft palate , most malignant) - Parotid gland ( mostly benign)

The distribution of salivary gland neoplasms showing the approximate overall frequency of tumours in different sites and the relevantfrequency of benign and malignant tumours by site.

• I- Adenomas • A) Pleomorphic adenoma ( Mixed tumour): • Pleomorphic adenomas ('mixed tumours') account for about 75% of parotid
tumours but a lower proportion of intraoral salivary gland tumours. • They arise mainly from duct epithelium or myoepithelial cells.• A wide variety of structures may be seenImportant histological features of pleomorphic adenomas• Capsule — never complete• Ducts• Sheets or strands of dark-staining epithelial cells• Squamous metaplasia and foci of keratin• Fibrous and elastic tissue• Myxoid tissue• Cartilage, sometimes calcified. Rarely, true bone formation

• These varied tissues are completely disordered in arrangement and the proportions of the different components also vary widely .
• The fibrous, myxoid, or cartilaginous mesenchymal elements are due to the pluripotential properties of myoepithelial cells.
• Some tumours are predominantly myxoid and can burst at operation if not gently handled, and then recur.
• Myoepithelial cells cannot be identified by light microscopy and can appear dark and angular, spindle-shaped or resemble plasma cells.
• However, immunohistochemistry shows their typical double staining with epithelial (cytokeratin) markers and mesenchymal markers, particularly S-100 protein,vimentin and actin.
• Myoepithelial cells may occasionally predominate or are the only cells present. Such a tumour is termed a myoepithelioma.
• Growth of pleomorphic adenomas is slow and may take several years to reach an inch in diameter.
• They form rubbery, often lobulated swellings . • When close under the mucosa, the tumour may appear bluish. • The swelling is typically attached to the overlying mucosa but mobile on the
deeper tissues

• If neglected, pleomorphic adenomas can grow to a great size and occasionally undergo malignant change.
• Treatment is by wide excision: recurrence is otherwise inevitable. • The reputation of the pleomorphic adenoma for recurrence is due to the great
surgical difficulties of complete removal of tumours from the parotid (the common site), where the facial nerve, in particular, makes dissection hazardous.
• Pleomorphic adenomas have an unusually strong tendency to seed and recur in the incision scar if opened at operation or if incompletely excised.
• In the case of parotid tumours, therefore, recurrences are prevented only by removing the gland with the tumour intact.
• The recurrence rate is low in skilled hands, but recurrences are typically multifocal and difficult to eradicate.

Pleomorphic adenoma. The junction of hard and soft palates is a common intraoral site; the tumour usually feels rubbery and lobulated on palpation. Pleomorphic adenoma. This slowly enlarging
lump in the lower pole of the parotid gland is caused by a pleomorphic adenoma but the appearance is not specific and any benign and some low-grade malignant neoplasms could appear the same.

This excised pleomorphic adenoma is 3 cm across and the lobular shape is clearly seen.
Pleomorphic adenoma. The histological appearances are very varied. In this typical area there are clusters of ducts containing eosinophilic material surrounded by stellate cells lying in a mucinous stroma.

Pleomorphic adenoma. In this area there has been maturation of the mucinous stroma to form a cartilage-like material within which there are more cellular islands with ducts
Plemorphic adenoma. In this lesion there is formation of true cartilage which is undergoing calcification.

Pleomorphic adenoma. At the margins of pleomorphicadenomas there are often extensions of the tumour into and beyond the capsule, rendering enucleation an ineffective treatment.

• B) Monomorphic Adenoma ( basal cell adenoma) • A benign S.G. tumour , which most commonly occurs among elderly people , &
usually located in the upper lip or the parotid gland.• Histopathology : • Pathologists recognize different morphological tissue or instance tubular &
cribriform. The overall distinguishing features of these tumours , apart from their origin in glandular tissue , are the homogenous – monomorphic – appearance of the tumour cells , & that the tumour matrix is without changes in terms of myxomatous or cartilagenous metaplasia.
• D.D = pleomorphic adenoma , adenoid cystic carcinoma • Treatment surgical removal.

• Adenolymphoma ( Warthin,s tumour , papillary cystadenoma lymphomatosum) : • It occurs mostly in the parotid gland• Histogenesis : is uncertain , but it most likely arises from residues of salivary duct
epithelium entrapped with lymph nodes during development.• Clinical features : old age , sex: male more than female , site : parotid gland.• Characters : • - Slow growing , may be bilateral involvement of parotid glands.• Histopathology : • Microscopically , the tumour consists of epithelial & lymphoid elements. The
epithelial component which clothes the paillary processes is double – layered & comprises a basal layer of roughly cuboidal cells surrounded by columnar cells. The epithelial cells have markedly eosinophilic granular cytoplasm , are rich in abnormal mitochondria , & resemble oncocytes . The stroma contains a variable amount of lymphoid tissue which often includes numerous germinal centers.
• Treatment : Enucleation.

Warthin's tumour. At higher power the tall columnar epithelial cells are readily identified and beneath them the lymphoid tissue
Warthin's tumour. Tall columnar cells surround lymphoid tissue and line a convoluted cystic space.

• Oncocytoma• Oncocytoma is a rare benign tumour that virtually only affects the parotids,
particularly in the elderly.• It consists of large eosinophilic cells with small compact nuclei ('oncocytes'), which
are typically arranged in solid cords.• Oncocytosis is the term given to replacement or transformation of acinar cells of
the parotid (or rarely other glands) by cells having the same appearance as those of an oncocytoma but without loss of the normal lobular architecture.
• Oncocytosis is usually an age-related change and when widespread the gland becomes swollen and soft.

• II – Carcinomas• Malignant tumours of S.G.s are relatively uncommon , accounting for about 1 % or
less of all malignancies.• Although carcinomas arise most frequently in the major glands , especially the
parotid , the proportion of malignant to benign tumours is higher in minor glands.• There are also differences in the incidence of the various types of carcinomas
between major & minor glands.• For ex. The adenoid cystic carcinoma ammounts for between 10-15 % of tumours
of the minor S.Gs but only about 3% of parotid neoplasms. • Muco - epidermoid Carcinoma : • Malignant salivary gland tumour accounts for 5% of all salivary gland tumours.• Clinically : 4th -5th decades age , sex: female more than male , site : palate & parotid
gland.• Characters : Fluctuant , aggressive , painful ulcerated swelling.• Histopathology : • Microscopically , the tumours are characterized by the presence of squamous cells
, mucus – secreting cells , & cells of intermediate types which have the potential for further differentiation towards mucous or squamous cells.

• The relative proportios of individual cell types & their arrangements vary form lesion to lesion , but it is customary to distinguish between well-differentiated ( low-grade) & poorly differentiated ( high-grade types) may appear to advance on a broad pushing front , whilst others ( mainly high –grade type) are ill-defined , highly infiltrative growths.
• In well –differentiated tumours , mucus –secreting & epidermoid cells predominant & there is no cellular pleomorphism.
• Such tumours are often cystic , either whilly or in part , the cysts being mainly by mucus-secreting cells.
• The epidermoid cells are usually present in the form of clumps or strands which show keratinization but may also partially line the cysts.
• Discharge of mucus into the cysts can lead to their distension , coalescence , or rupture , in which the release of mucus into the stroma is accompanied by reactive inflammation.
• In poorly differentiated tumours , epidermoid & intermediate cells predominate & there is nuclear & cellular pleomorphism & nuclear hyperchromatism .
• Cystic spaces are not prominent & may be absent.• In some differentiation from squamous cell carcinoma is difficult.

• Although well-differentiated tumours rarely metastasize , the behaviour of a mucoepidermoid carcinoma cannot be predicted with any degree of certainty from it is histology.
• The overall 5- year survival rate is about 70%.• However , well-differentiated , low-grade tumours have a local recurrence rate of
less than 10% & a 5 year survival of about 95% .• In contrast poorly differentiated ( high-grade) tumours have been reported to
have local recurrence rates of 80% & 5 years survival rates of only 30-40 % • Treatment : WIDE EXCISION RECURRENCE MAY OCCUR

Mucoepidermoid carcinoma. The mucous cells surround microcysts. Underlying the mucous cells are the epidermoid (squamous) cell
Mucoepidermoid carcinoma. At higher power the finelygranular mucous cells are seen to the right with the underlying epidermoid cells to the left.

• Adenoid cystic carcinoma : • Malignant S.G. tumour which is more common in minor salivary gland.• Clinically : old age , Sex: female more than male , Site : minor salivary gland.• Characters : Painful , ulcerated , fast growing swelling.• Parotid tumours may also present with facial palsy . The neurological
manifestations are a reflection of the predilection of the tumour to infiltrate & spread along nerve pathways.
• Histopathology : The neoplastic epithelium is arranged as ovoid & irregularly shaped islands or as anastomosing strands lying in a scanty C.T. stroma .
• The characteristic feature of the tumour is the presence of numerous microscopic cyst-like spaces within the epithelial islands , producing a cribriform , lace like or “ Swiss-cheese” pattern.
• The spaces are found by partial enclavement of areas of stroma or of mucoid materials produced by the tumour epithelium which are deposited adjacent to the stroma.
• Partial enclavement means that the contents of the spaces are still in continuity with the stroma .
• They contain acellular basophilic or occasionally hyaline substances rich in glycosaminoglycans & basement membrane – like material.

• In tumours showing the characteristic cribriform pattern the epithelial components consists predominantly of small , rather uniform polygonal cells with basophilic cytoplasm .
• Mitosis are rarely seen . • Less frequently the tumour shows tubular or solid pattern.• Treatment & prognosis : • Early wide excision & radiotherapy • Poor prognosis ( metastasis occurs late)

Adenoid cystic carcinoma. There is an ulcerated mass arising from a minor gland in the palate. The clinical appearance would be the same with other malignant salivary neoplasms.
Adenoid cystic carcinoma. The small darkly staining cells of the adenoid cystic carcinoma form cribriform islands with large holes which have been likened, rather inappropriately, to Swiss cheese.

• Acinic cell carcinoma : • Is rare & account for about 1% of S.G tumours .• Their behaviour is also unpredicatable .• Histologically : show an almost uniform pattern of large cells , similar to serous
cells , with granular basophilic cytoplasm , often in an acinar arrangement .• A characteristic feature is scattered round “holes” thought to be entrapped
secretion. • Sometimes these are so numerous as to give the tumour a lace – like appearance.• Carcinoma arising in pleomorphic adenoma : is relatively uncommon & accounts
for about 3% of salivary tumours , although the true incidence difficult to establish.• Almost all arise in the parotid in adenomas that have usually been present for
many years. • The histological diagnosis requires evidence of a pre-existing pleomorphic
adenoma , but in some tumours this may be difficult to identify & only hyaline scar – like tissue may remain.
• The malignant component is usually & adenocarcinoma or undifferentiated carcinoma but may assume the features of any of the types of salivary carcinomas
• In some tumour more than one morphological type of carcinoma may be present.

Acinic cell carcinoma. The tumour is composed of granular acinar-type cells, sometimes arranged in acinus-like clusters and sometimes forming irregular sheets. Cytological atypia is uncommon.
Carcinoma arising in a pleomorphic adenoma. In longstanding pleomorphic adenomas the stroma may become hyalinised, dense and acellular. In such tumours there is a risk of transformation to carcinoma, as shown here by clusters of cells showing cytological atypia

• Whilst the malignant component is confined to areas still within the pre-existing adenoma ( non-invasive stage) the tumour has a good prognosis .
• However , when there infiltration of surrounding tissues the tumour has a poor prognosis.
• Polymorphous low grade adenocarcinoma : • Occurs almost exclusively in minor S.Gs .• Most have presented in the palate .• As it is name implies it is a tumour that shows a variety of growth patterns within
the same lesion , including solid , tubular , papillary , & cribriform areas.• Cytologically , the tumour appears bland , mitotic figures are infrequent & nuclear
atypia is lacking.• The tumour has a good prognosis . Although it has an infiltrative pattern of growth
, local recurrence is uncommon & metastatic spread to regional nodes is rare.• Other carcinomas : • - adenocarcinoma • - Squamous cell carcinoma • - basal cell adenocarcinoma , sebaceous carcinoma & undifferentiated carcinomas.

Polymorphous low-grade adenocarcinoma. A. Targetoid pattern; B. cribriform area; C. surviving acini inside the tumour; D. papillary cystic area.