CHANGING TIMES Oncology Regulations, Billing and Coding for 2004 Roberta Buell MBA.
73
CHANGING TIMES CHANGING TIMES Oncology Regulations, Billing and Coding for 2004 Oncology Regulations, Billing and Coding for 2004 Roberta Buell MBA Roberta Buell MBA
-
Upload
deborah-weaver -
Category
Documents
-
view
221 -
download
1
Transcript of CHANGING TIMES Oncology Regulations, Billing and Coding for 2004 Roberta Buell MBA.

CHANGING TIMESCHANGING TIMES
Oncology Regulations, Billing and Coding for 2004Oncology Regulations, Billing and Coding for 2004
Roberta Buell MBARoberta Buell MBA

DisclaimerDisclaimer This should not be the only source used for coding and billing.
All coding and billing decisions should be made on a case-by-case basis based upon documentation and insurance guidelines.
All information contained herein is valid for the date of this seminar only. This presentation is based on national guidelines. Your Medicare Carrier may differ.
This presentation is a summary only. For Medicare regulations, see www.cms.hhs.gov or your local Medicare web site.
Nothing in this presentation instructs practices on how to set charges for products and services.

Meeting AgendaMeeting Agenda
Medicare Regulations 2004: Part B Office– Regulations– Commonly Asked Questions
Medicare Regulations 2004: Hospital Outpatient HCPCS Coding 2004 Survival Strategies Your “TO DO” List for First Quarter

Changing TimesChanging Times
“It is change, continuing change, inevitable change, that is the dominant factor in society today. No sensible decision can be made any longer without taking into account not only the world as it is, but the world as it will be.... This, in turn, means that our statesmen, our businessmen, our everyman must take on a science fictional way of thinking.”
Isaac Asimov

Medicare Regulations 2004Office Based Oncology
Passage of The Medicare Prescription Drug Improvement and Modernization Act of 2003
(“DIMA”)

DIMA Regulations DIMA Regulations
DIMA will change the way that you do business regardless of your setting:– It is a temporary fix for office-based Oncologists.– It will shift the your focus from drug distribution to
diversified chemotherapy and cancer services.– It will make you think about coding.– It will make hospitals a more viable cancer option for
the first time in more than three years.

Medicare Physician Fee ScheduleMedicare Physician Fee Schedule Medicare Conversion Factor Bumped Up
– In 2003, this was $36.7856– Was supposed to be reduced by 4.5% due to calculations
in the update factor. This has been corrected in DIMA—increased by 1.5% in 2004 and in 2005.
– $37.3374 is the CF—published 12/31/03 and effective 1/1/04.
Why should you know the conversion factor?– You can use a multiple of it to set your own fees.– You need to know it to negotiate with MCOs.

Medicare Physician Fee ScheduleMedicare Physician Fee Schedule
The Geographical Cost Indices were increased!– The minimum work GPCI is now 1.00.– While this may seem really obtuse, it has a very
positive effect for those of you in non-high cost areas.
– Impact on RBRVS services for the better.
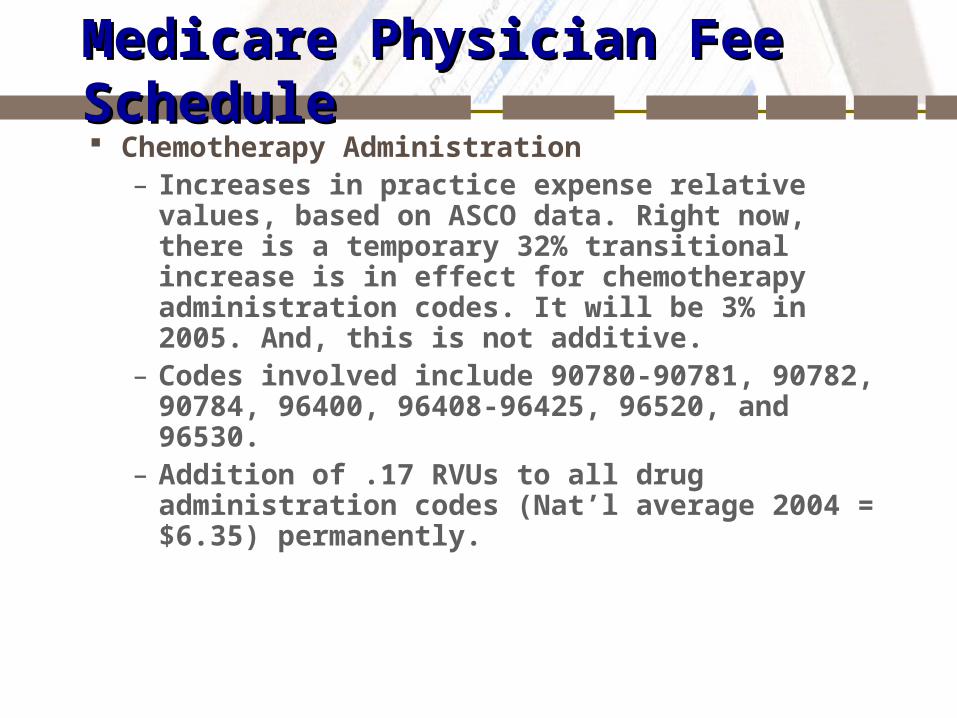
Medicare Physician Fee ScheduleMedicare Physician Fee Schedule Chemotherapy Administration
– Increases in practice expense relative values, based on ASCO data. Right now, there is a temporary 32% transitional increase is in effect for chemotherapy administration codes. It will be 3% in 2005. And, this is not additive.
– Codes involved include 90780-90781, 90782, 90784, 96400, 96408-96425, 96520, and 96530.
– Addition of .17 RVUs to all drug administration codes (Nat’l average 2004 = $6.35) permanently.
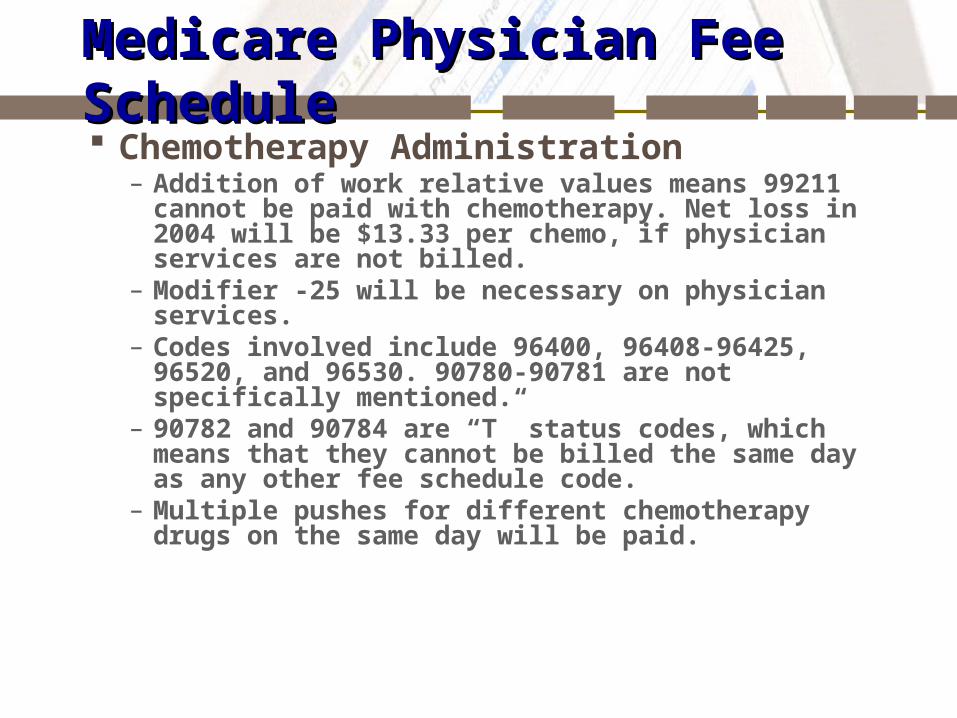
Medicare Physician Fee ScheduleMedicare Physician Fee Schedule Chemotherapy Administration
– Addition of work relative values means 99211 cannot be paid with chemotherapy. Net loss in 2004 will be $13.33 per chemo, if physician services are not billed.
– Modifier -25 will be necessary on physician services.– Codes involved include 96400, 96408-96425, 96520, and
96530. 90780-90781 are not specifically mentioned.– 90782 and 90784 are “T” status codes, which means that
they cannot be billed the same day as any other fee schedule code.
– Multiple pushes for different chemotherapy drugs on the same day will be paid.

Drug Administration ExamplesDrug Administration Examples
Code 2003 $ 2004 Base
2004Trans $
Diff2003 2004
2005Trans $ (estimate)
90780 $42.67 $89.23 $117.79 +$75.12 $91.91
96408 $37.52 $117.54 $154.76 +$117.24 $120.76
96410 $59.22 $164.66 $217.35 +$158.13 $!69.60
96412 $44.14 $36.59 $48.30 +$4.16 $37.69

Drug Payment 2004Drug Payment 2004 Here is what we all know…
– 95% of Average Wholesale Price will only be paid for drugs approved after 4/1/03 and this will last until 2005.
– Until 2005, 85% will be paid for some drugs, but there are 29 exceptions and 23 of them are cancer drugs.
– Oral cancer and oral anti-emetic drugs are supposed to be paid at 85% of AWP with a cost of supplying drug fee. However, this will not happen this year. It will be investigated in 2005.
– The Single Drug Pricer is in effect and has not improved since last year, so 85% is not representative of many multiple source drugs, depending upon what you buy.

Cancer Drug ExceptionsCancer Drug Exceptions Epoetin alfa for non-esrd use
(87%) Leuprolide acetate (81%) Goserelin acetate (80%) Rituximab (81%) Paclitaxel (81%) Docetaxel (80%) Carboplatin (81%) Irinotecan (80%) Gemcitabine (80%) Pamidronate Disodium (85%)
Filgrastim (81%) Granisetron Hcl (80%) Ondansetron (87%) Vinorelbine Tartrate (81%) Sargramostim (80%) Topotecan (84%) Immune Globulin (80%) Leucovorin Calcium (80%) Doxorubicin Hcl (80%) Dexamethosone Sodium (86%) Heparin flush (80%)

Other ExceptionsOther Exceptions Reimbursed at 95% of the October, 2003 AWP
– Blood clotting factor– Drugs without AWP 4/1/2003. – Vaccines– ESRD drugs– Infusion drugs through DME are at 95%, but will go
to ‘competitive acquisition’ cost in 2007.– IVIG paid at 95% of AWP in 2004 and paid
according to ASP beginning in 2005.

Single Drug Pricer (SDP)Single Drug Pricer (SDP) One price for drugs across the country
– Palmetto, Carrier for South Carolina, Ohio, and West Virginia, will maintain a Single fee schedule for drugs
– SDP based on Red Book reported AWP, will be updated quarterly and, to our knowledge, this will not change.
– This means your Carrier fee schedule is the same as the SDP.
– This can have a profound impact on profits, depending upon your drug mix.

Single Drug PricerSingle Drug Pricer October 1, 2004 Update was highly irregular. No
explanation from Medicare. Some of the problems include these allowables:
Bleomycin reduced by 37%. Cisplatin reduced by 62%. Cytarabine reduced by 46%. Doxorubicin reduced by 77%. Etoposide reduced by 84%. Leucovorin reduced by 79%. Mitomycin reduced by 36%.

Single Drug PricerSingle Drug Pricer
Why did this happen?– No formal explanation.– Remember the formula for generic drugs from
BBA1997---the lower of the median AWP or the lowest brand name. This has been applied in a very odd way.
– Generic manufacturers consistently lowering price. This will continue.

SDP—An ExampleSDP—An Example
Mitomycin 5 mg– Brand 1-- 5 mg = $134.11– Brand 2 – 5 mg = $134.11– Generic Brand 5 mg = $67.20– Generic 5 mg = $67.20
SDP = $67.20 (48% of AWP)

Single Drug PricerSingle Drug Pricer How can you analyze this?
– Take the drugs that you buy now.– List them with your cost by NDC on a spread sheet. – Convert cost by NDC to cost by J-code unit. If you need info, call me or look
at the SDP background info at http://www.cms.hhs.gov/providers/drugs/default.asp.
– Compare cost as a percentage of SDP for the drug. Example: your per unit cost is $10 and the SDP is $5. Your cost is 200% of SDP or SDP only covers 50% of your cost and you have a negative margin $5 per unit.
– Multiply the number of J-code units you use by NDC as a percentage of SDP. So, if you give 1000 units per year, you lose $5000.
– Check drugs with negative or very low margins and large impact. Remember—at least one of the generics should be priced at 85% of AWP, unless it is an exception drug.
– Renegotiate contracts.

Medicare 2005Medicare 2005 Pertinent to Oncology in Physicians’ Offices
– 1.5% Fee Schedule increase– Minimum Work RVU GPCI of 1.00– Drug administration transition goes to 3% (and 32% goes
away)– Drug reimbursement based ASP plus 6% or
If adequate data does not for ASP, allowable can be based on WAC or other methodologies as of 11/2003.
ASP may be disregarded if the WAMP exceeds ASP by 5%, But, will not be re-adjusted until 2006.
Or, if WAMP or AMP exceed ASP then allowable can be WAMP or 103% AMP, whichever is lower.
Medicare 2006 and Thereafter?Medicare 2006 and Thereafter? Pertinent to Oncology in Physicians’ Offices
– Conversion factor controlled by sustained growth rate. Could mean negative increases.
– Fee schedule without transition increases, but drug administration RVUs could be developed by then.
– Budget neutrality exemption expires for drug administration increases.
– Phase in of MVI (national “brown bagging”) at the discretion of Oncologists who ‘do not wish to take on the bad debt’ of chemotherapy drugs.

Commonly Asked Questions Can we bill anti-emetics and other supportive care drugs with
96408?
MCM 15400. CHEMOTHERAPY ADMINISTRATION (CODES 96400-96549)
1. General Use of Codes.--Chemotherapy administration codes, 96400 through 96450, 96542, 96545, and 96549, are only to be used when reporting chemotherapy administration when the drug being used is an antineoplastic and the diagnosis is cancer. The administration of other drugs, such as growth factors, saline, and diuretics, to patients with cancer, or the administration of antineoplastics to patients with a diagnosis other than cancer, are reported with codes 90780 through 90784 as appropriate.

Commonly Asked QuestionsCommonly Asked Questions
Can I bill 90784 with chemotherapy administration?
This is a “T” status code. There are RVUs and payment amounts for these services, but they are only paid if there are no other services payable under the physician fee schedule billed on the same date by the same provider. If any other services payable under the physician fee schedule are billed on the same date by the same provider, these services are bundled into the physician services for which payment is made. (MCM 15901)

Commonly Asked QuestionsCommonly Asked Questions Can I bill higher level visits with chemotherapy now that
99211 is gone?
Of course, you may only bill 99212-99215 (with -25) if the physician sees the patient face-to-face. There is no regulation that says you cannot do this. There must be medical necessity for the patient to see the doctor and documentation of services. BUT, remember your utilization patterns are constantly monitored by the Medicare Program and, if patterns change, this can lead to audits and fines, if you are doing this strictly for revenue-maximization purposes.

Commonly Asked QuestionsCommonly Asked Questions Can we still bill 99211 instead of 90782?
Injection and Evaluation and Management Code Billed Separately on Same Day of Service.--Advise physicians that CPT code 99211 cannot be used to report a visit solely for the purpose of receiving an injection which meets the definition of CPT codes 90782, 90783, 90784, or 90788. Do not pay CPT codes 90782, 90783, 90784, or 90788 if any other physician fee schedule service was rendered. (MCM 15502)
This means that this cannot be a ‘drive by’ shooting…
Commonly Asked QuestionsCommonly Asked Questions What documentation do we need for Modifier -25?
CPT Modifier 25-Significant Evaluation and Management Service By Same Physician On Date of Global Procedure.--Pay for an evaluation and management service provided on the day of a procedure with a global fee period if the physician indicates that the service is for a significant, separately identifiable evaluation and management service that is above and beyond the pre- and post-operative work of the procedure. (MCM 15501.1)
This means you need a medically-necessary reason and an Evaluation and Management note for the patient.

Commonly Asked QuestionsCommonly Asked Questions 96530 is covered under the new regulations. Can we now
use it for flushing a port?
MCM 15400.C. Flushing Of Vascular Access Port.--Flushing of a vascular access port prior to administration of chemotherapy is integral to the chemotherapy administration and is not separately billable. If a special visit is made to a physician's office just for the port flushing, code 99211, brief office visit, should be used. Code 96530, refilling and maintenance of implantable pump or reservoir, while a payable service, should not be used to report port flushing.
Commonly Asked QuestionsCommonly Asked Questions
Is Leucovorin billable under 96408?
This is actually less clear than it is for anti-emetics. But, to be conservative, it should not be billed with 96408 because it is technically not a J9xxx code.

Commonly Asked QuestionsCommonly Asked Questions Can I still get paid if I give pre- and post-supportive care meds with chemo?
MCM 15400.E. Chemotherapy Administration and Hydration Therapy.--Do not pay separately for the infusion of saline, an antiemetic, or any other nonchemotherapy drug under codes 90780 and 90781 when these drugs are administered at the same time as chemotherapy infusion, codes 96410, 96412, or 96414. However, pay for the infusion of saline, anti-emetics, or other nonchemotherapy drugs under codes 90780 and 90781 when these drugs are administered on the same day but sequentially to rather than at the same time as chemotherapy infusion, codes 96410, 96412, and 96414. Physicians should use modifier GB (now -59!) to indicate when codes 90780 and 90781 are provided sequentially rather than contemporaneously with codes 96410, 96412, and 96414. Both the chemotherapy and the nonchemotherapy drugs are payable regardless of whether they are administered sequentially or contemporaneously.

Commonly Asked QuestionsCommonly Asked Questions
Drugs given in a pump are still paid at 95% of AWP. Can I give them in the office and be paid for these?
Drugs given in a pump are only billable (as are the pump and the pump supplies) through the DMERC. Plus, drugs paid at 95% are limited.
Commonly Asked QuestionsCommonly Asked Questions How do I bill multiple pushes? With multiple units or
with differing line items?
While most Carriers have not printed guidelines for this, I agree with ASCO in that, without specific and exceptional guidance in the regulation, you will bill for multiple units in Box 24G. Line item billing with a modifier would not be very practical—but this is still not explicit. Also, remember to have as many drugs on the claim as units in the box.

Commonly Asked QuestionsCommonly Asked Questions Can I bill 99211 with 90780? ASCO says maybe I can…
The reason that they are saying ‘maybe’ (and that they will check with CMS) is that it is not DIRECTLY mentioned in the regs. Here’s what it says:“Currently, section 15010 of the Medicare Carriers Manual (MCM) does not allow payment for CPT codes 90782, 90783, 90784 and 90788 unless these are the only physician fee schedule services provided on that day. We do pay separately for cancer chemotherapy injections (CPT codes 96400-96549) in addition to an office visit (CPT codes 99211-99215) furnished on the same day by the same physician. CPT code 99211 does not require a face-to-face encounter between the physician and the patient like other office visit services (CPT codes 99212-99215) and can be used be physicians supervising a nurse performing chemotherapy administration…We believe that adding physician work to the drug administration services will subsume the supervision that physicians billing for a 99211 on the same day are typically providing. Therefore, we will no longer allow for 99211 to be billed on the same day as a chemotherapy administration service. “
BUT, .17 relative values were added to 90780, just like they were to 964xx codes, so my guess is that inevitably 99211 WILL BE DENIED. Check with your Carrier.

Commonly Asked QuestionsCommonly Asked Questions
Can I bill two units of 90782?
There is nothing legally to prevent you from doing this. But, Medicare has not allowed multiple units of this since the late 1980s.

OIG Proposed Rule on ChargesOIG Proposed Rule on Charges The proposed rule states that the OIG can use its exclusion
powers against anyone who charges Medicare over 120% more than any other payer.
Only includes drugs, lab, and durable medical equipment. May be average price or median price—but brown bagging could
bring either down. Payers must constitute over 10% of your business. This includes net charges to Managed Care Organizations,
indemnity payers, TRICARE, etc. This also includes amounts charged to patients with no
insurance.

Hospital Outpatient Prospective PaymentHospital Outpatient Prospective Payment
General Principles from 2000– Drugs are not paid separately– New drugs are paid at 95% of AWP as the total
allowable, but that is for 2-3 years.– 10 Cancer Hospitals are ‘held harmless’

Medicare HOPPS Before DIMAMedicare HOPPS Before DIMA
Under OPPS, payment for drugs should be bundled with the procedure (e.g., infusion) into Ambulatory Payment Classifications (APCs)
APCs are paid at a prospectively determined rate for all APCs delivered on one day.
Drugs without J-codes are not paid until they get a temporary code.
Exception are pass-through drugs paid at 95% of the AWP for the first 2-3 years and then reduced reserved for new drugs and drugs whose cost is “not insignificant” temporary status lasting from 2 to 3 years Once status expires, drugs costing more than $50 per episode (as of
2004) receive unique APCs Loads of drugs are not paid!
HOPPS for 2004HOPPS for 2004 DIMA
– “Specified covered outpatient drugs” will be paid. These are drugs which meets these criteria It is a covered drug under Section 1927(k)(2) of the Social
Security Act. It is a drug which has a separate APC. It is a drug which was paid by pass-through before 12/31/2002.
– Exceptions are drugs first paid on pass-through on 1/1/2003; drugs without codes; and, 2004-2005 orphan drugs as defined by Medicare. Blood, blood products and certain vaccines are also exceptions.

HOPPS 2004--DIMAHOPPS 2004--DIMA Drugs that are covered are classified as follows by
manufacturers Medicaid rebate definitions with ceilings and floors:– Sole Source will be paid at a floor of 88% and a ceiling of
95% of AWP;– Innovator Multiple Source Drugs will be paid with no floor and
a ceiling of 68% of AWP;– Non-innovator Multiple Source will be paid with no floor and a
ceiling of 46% of AWP. These are applied to the 11/7/04 HOPPS rule and based on
RED BOOK of May 1, 2003.

HOPPS 2005-2006HOPPS 2005-2006 For 2005:
– Sole Source will be paid at a floor of 83% and a ceiling of 95% of AWP;
– Innovator Multiple Source Drugs will be paid with no floor and a ceiling of 68% of AWP;
– Non-innovator Multiple Source will be paid with no floor and a ceiling of 46% of AWP.
For 2006 and beyond– Paid at acquisition cost.

HOPPS 2004--DIMAHOPPS 2004--DIMA Pass-through drugs are paid as Part B drugs. That is, they
will be paid on the Single Drug Pricer at 85% this year; ASP plus 6% next year; and thereafter at ASP plus 6% or brown-bagged.
Exceptions are– Drugs not approved as of 4/1/03. They will be paid at 95% of
AWP.– Drugs that are appealed by manufacturers as being
reimbursed at levels below widely available prices.– Blood, blood products, and vaccines.

HOPPS 2004HOPPS 2004 More good news for hospitals:
– Drugs without HCPCS codes will now be paid, but will not qualify for outlier status (DIMA).
– Functional equivalence will not be applied hereafter (DIMA). But, it is there for PROCRIT and ARANESP.
– Q0085 has been deleted. You can now bill Q0083 and Q0084 on the same day.
– If multiple injections are done in multiple visits in a day, they can be billed as long as the visits are separate. Check with your FI as to how this will be implemented.

DIMA Comparison 2004—Q1DIMA Comparison 2004—Q1
Drug 2004 MD $
2004 HOPPS
1/1/2003 HOPPS1
Amifostine (ETHYOL)
$405.29 $419.59 $234.98
Darbepoetin,5 mcg
$21.20 $19.40 $11.85
Leucovorin $3.00 NO APC Not paid separately
Anzemet $13.85 NO APC Not paid separately
Zofran $5.58 No APC Not paid separately
Aredia/ Pamidronate
$237.88 $128.74 $170.29
Adriamycin $8.67 $4.69 Not paid separately
Cisplatin, 10 mg $13.56 $7.73 $22.23
Taxotere $301.40 $331.53 $203.14 Gemzar $101.90 $112.09 $67.71 Taxol/ Paclitaxel $139.90 $79.04 $120.77
Procrit $11.62 $11.76 $9.10
1 This was the rate in the 10/31/02 Federal Register for 2003. This may have been updated during the year 2003.

HCPCS Codes 2004HCPCS Codes 2004
Since many issues are not discussed here, this is not meant to replace your careful review of the official coding manuals. You should always refer to these manuals for specific questions and to select the proper code for services provided.Also, please note that all CPT codes are published and copyrighted by the American Medical Association.

CPT for Cancer CareCPT for Cancer Care
New Codes– 36555-36556: Insertion of Non-Tunneled Central Venous Catheter.– 36557-36566: Insertion of Tunneled Venous Access Device– 36568-36571: Insertion of PICC Lines– 36575-36576: Repair of Central Venous Access Device– 36578-36585: Replacement of Central Venous Access Devices– 36589-36590: Removal of Central Venous Access Device– 36595-36596: Mechanical Removal of Obstructive Material– 36597: Reposition of Central Venous Catheter under Fluoroscopic
Guidance
HCPCS 2004 (1/1/2004)HCPCS 2004 (1/1/2004)– J2353—Sandostatin LAR, 1 mg– J2354—Sandostatin, non-depot, 1 mg– J2505—Neulasta, 6 mg– J9098—Cytarabine, liposome, 10 mg– J9178—Epirubicin, 2 mg (Changed)– J9263—Eloxatin, 0.5 mg– J9395—Faslodex, 25 mg– Q0137—Aranesp, 1 mcg (Non-ESRD)– Q4054—Aranesp, 1 mcg for ESRD– Q4055—Epoetin alfa 1000 units for ESRD

Aranesp (Darbepoetin Alfa)Aranesp (Darbepoetin Alfa)
Per Transmittal 36, Change Request 3037– For IN OFFICE, non-dialysis patients J0880 is re-
instated. This does NOT apply to dialysis patients.– Removes ‘non-payable’ status from J0880.– Physicians have the option of using EITHER code
that they want to. Both are valid.– For dialysis, Q4054 will be used.
AranespAranesp
In ESRD on dialysis, Per Medicare Transmittal 39, Change Request 2963– For patients ON DIALYSIS only!– Does away with Q99xx codes– Q4054 for 1 mcg. goes into effect January 1. Q4055
for Epogen goes into effect January 1, 2004.– Payment will be based on SDP.– Must have hematocrit in Box 19.

Survival Strategies Survival Strategies
The DIMA regulation states that Oncology practices will break even in terms of revenue THIS YEAR. $510 million was taken out of drug reimbursement and $510 million was replaced. Next year, 29% of drug administration money will be removed from Medicare reimbursement.
What will you do?
Survival StrategiesSurvival Strategies
Three aspects to your strategy:– Top Line– Bottom Line– Leadership

Top LineTop Line
At least, three product lines in your practice:– Drug Administration– Evaluation and Management– Provision of Drugs

Top Line—Drug AdministrationTop Line—Drug Administration Can you enhance this product line?
– Provide nursing staff with education on the new rules ASAP. Use this Power Point. Use ASCO FAQ.
– Audit for the following: Lost infusion hours. Lost pushes (at least, after March 1) A push being billed instead of an infusion. 90780-90781-59 Lost 99211’s prior to 12/31/03
– Enlist your Nurses to call physicians in when possible to see patients in the chemo room who have questions or side effects.

Top Line—Evaluation & ManagementTop Line—Evaluation & Management
Documentation of Evaluation and Management Services
Review of systems (H)Examination of systems (P)Review of ancillaries/medical
records/treatment plan and options (DM)Counseling (for more than 50% of the visit)
Time of counseling

Top Line—E&MTop Line—E&M
Documentation of counseling & coordination of care:
An example from MCM 15501.C--A cancer patient has had all preliminary studies completed and a medical decision to implement chemotherapy. At an office visit the physician discusses the treatment options and subsequent lifestyle effects of treatment the patient may encounter or is experiencing. The physician need not complete a history and physical examination in order to select the level of service. The time spent in counseling/coordination of care and medical decision-making will determine the level of service billed.
Top Line—E&MTop Line—E&M Counseling from MCM 15501
The code selection is based on the total time of the face-to-face encounter or floor time, not just the counseling time. The medical record must be documented in sufficient detail to justify the selection of the specific code if time is the basis for selection of the code.
In the office and other outpatient setting, counseling and/or coordination of care must be provided in the presence of the patient if the time spent providing those services is used to determine the level of service reported. Face-to-face time refers to the time with the physician only. Counseling by other staff is not considered to be part of the face-to-face physician/patient encounter time. Therefore, the time spent by the other staff is not considered in selecting the appropriate level of service. The code used depends upon the physician service provided.

Top Line—E&MTop Line—E&M Counseling…what this means
– Document the time of the visit (face-to-face)– Document the time spent counseling– Document the reason for counseling– Visit times
99212 = 10 minutes 99213 = 15 minutes 99214 = 25 minutes 99215 = 40 minutes

Top Line—E&MTop Line—E&M
Consultations are a focused area of the OIG this year!!!– Not every new patient is a consult…
Must be a documented referral from another physician. Must be a written report back to the referring physician. Must not be a second opinion (unless you code it
Confirmatory Consultation 99271-99275) Must not be a referral from another Oncologist for
treatment (ie.winter guests)
Top Line--EM Services To ConsiderTop Line--EM Services To Consider
EM services will be more important in the future. Discuss these in your practice….– 2004 Fee Schedule Allowables (National Average weight = 1)
Home Health Certification/Recertification (G0180, G0179)--$73.93 and $57.13
CPOS* (G0181-G0182)--$123.96-$131.05 99239 (discharge, more than 30 minutes) --$95.21
* For non-Medicare, use CPT codes (99374-99380).

Top Line--CPOSTop Line--CPOS From 15513 of MCM Nature of Services.--Care plan oversight is the physician
supervision of patients under the care of home health agencies or hospices that require complex or multidisciplinary care modalities involving regular physician development and/or revision of care plans, review of subsequent reports of patient status, review of related laboratory and other studies, communication with other health professionals not employed in the same practice who are involved in the patient's care, integration of new information into the medical treatment plan, and/or adjustment of medical therapy.
.
Top Line--CPOSTop Line--CPOS
Services not countable toward the 30 minutes threshold that must be provided in order to bill for CPO include, but are not limited to, time associated with discussions with the patient, his or her family or friends to adjust medication or treatment, time spent by staff getting or filing charts, travel time, and/or physician’s time spent telephoning prescriptions in to the pharmacist unless the telephone conversation involves discussions of pharmaceutical therapies—MCM 15513

Top Line—Prolonged ServicesTop Line—Prolonged Services MCM 15511
– Required Companion Codes.--Pay prolonged services codes 99354-99355 when they are billed on the same day by the same physician as the companion evaluation and management codes and: The companion codes for 99354 are 99201-
99205, 99212-99215, 99241-99245; or 99341- 99345; 99347 - 99350 to be used;
The companion codes for 99355 are 99354 and one of the evaluation and management codes required for 99354 to be used;

Top Line—Prolonged ServicesTop Line—Prolonged Services– Requirement for Physician Presence.--Advise
physicians to count only the duration of direct face-to-face contact between the physician and the patient (whether the service was continuous or not) beyond the typical time of the visit code billed to determine whether prolonged services can be billed and to determine the prolonged services codes that are allowable. In the case of prolonged office services, time spent by office staff with the patient, or time the patient remains unaccompanied in the office cannot be billed. In the case of prolonged hospital services, time spent waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities cannot be billed as prolonged services.

Top Line—Prolonged ServicesTop Line—Prolonged Services– Documentation.--Do not require
documentation to accompany the bill for prolonged services unless the physician has been targeted for medical review. Advise physicians that to support billing for prolonged services, the medical record must document the duration and content of the evaluation and management code billed and that the physician have personally furnished at least 30 minutes of direct service after the typical time of the evaluation and management service had been exceeded by at least 30 minutes.
– Threshold Times for Codes 99354 and 99355.--If the total direct face-to-face time equals or exceeds the threshold time for code 99354, but is less than the threshold time for code 99355, the physician should bill the visit and code 99354. Do not accept more than 1 unit of code 99354. If the total direct face-to-face time equals or exceeds the threshold time for code 99355 by no more than 29 minutes, the physician should bill the visit code 99354 and one unit of code 99355. One additional unit of code 99355 is billed for each additional increment of 30 minutes extended duration. Use the following threshold times to determine if the prolonged services codes 99354 and/or 99355 can be billed with the office/outpatient visit and consultation codes.

Top Line—DrugsTop Line—Drugs
Clinical Trials Do not depend upon the whims of reimbursement Routine costs, if an acceptable Medicare trial, are
billable (-QV and V70.5) Just make sure not to double bill. This includes
Lab tests E & M Drugs

Bottom LineBottom Line
Chemotherapy Administration– How many hours of Nursing do you need per week?– How many hours of Nursing PTO do need per week?– Can you flex your staffing?– Can you contract for staff?– Will NPPs extend your hours or days available?
Bottom LineBottom Line Drugs
– Get deeply involved with the SDP. This will sneak up on you if you do not. You need to look at NDCs, not J-codes EACH QUARTER.
– Ask drug companies to estimate the ASP for you as soon as possible.
– Make logical choices about chemo in the office versus the hospital. Remember patients go on and off therapies.

Bottom LineBottom Line
“You Have To Spend $$$ to Make $$$”– Electronic Medical Records– Better Billing Systems (less bodies)– Electronic prescriptions– Collection agencies– Contractors

Bottom LineBottom Line The worst hit to your bottom line will be ‘take backs’ Medicare. Areas of
focus by OIG include:– Consults– Coding of level of E&M services– Use of Modifier -25– Use of Modifiers with CCI edits– Place of Service Errors– CPOS– Billing for Diagnostic Tests– Radiation Therapy– Services/supplies Incident to Physicians’ Services– “Long Distance” Physician Claims
Let’s be careful out there!

LeadershipLeadership
“Leadership is the art of getting someone else to do something you want done
because he wants to do it." -Dwight. D. Eisenhower
LeadershipLeadership Manage Managed Care
– Find all of those contracts– Look at the fee schedule—are they on 2004 RVUs?– Look at the drug pricing basis.– Assess their contractual adjustment.– Ascertain their collection rate.– Find out the number of patients in treatment.– Do you want to keep them if better terms cannot be
reached?

LeadershipLeadership Bring in Every Possible $ This Year in Cash
– Get rid of old Receivables– Look at Collection Policies and Procedures– Collect cash for uncovered services—nutrition, counseling,
meditation, etc.– Re-assess your charges, if you have more than 10%
indemnity or lab.– Collect co-pays on less complex or more standard services at
treatment. – Take charge and/or debit cards.

LeadershipLeadership
Assess Every Patient’s Situation Prior to Treatment– Deductible– Co-pay– Drug benefits at all sites of service– Referral requirements– Stop losses– Catastrophic benefits– COB

2004 Quarter 1 Checklist2004 Quarter 1 Checklist In-service your Nurses on the new regulations if you have not done so
already. Check every chemotherapy and drug administration EOB to be sure that
you are being paid correctly. Go through the Single Drug Pricer, particularly for multi-source drugs and
ensure that you are not being paid below cost. Update your Superbill for new codes and modifiers. Get non-Medicare payers to use 2004 RVUs. Audit E&M coding for opportunities and problems. For forms, call me or
see www.donself.com. Audit chemotherapy charts and billed services in late March (if not before
then) to see if everyone gets it! Seek new practice opportunities. And, as always, participate in the struggle!
Contact InformationContact Information
Here is my contact information:
Bobbi [email protected]
800-795-2633650-854-5615650-618-8621 (FAX)