Changing - Overdiagnosis 3… · Changing Overdiagnosis the Cultureof GOAL RESULTS Three common...
1
Changing Overdiagnosis the Culture of GOAL RESULTS Three common cancers affecting varied populations and screening rates were chosen as our test measures. Cervical, breast and prostate cancer all have tests used to identify early tumors with the goal of detecting these in the curable stage. The first two have well established publicly reported metrics used in accountabil- ity frameworks through the National Committee for Quality Assurance (NCQA); Prostate cancer screening using a PSA is actually recommended to NOT do, with the US Public Services Task Force (USPSTF) citing this as a “D” recommenda- tion – screening does more harm than good. For each topic we: 1. Created a shared vision with clinical experts, leading with the “why” of how appropriate care benefited patients 2. Built and leveraged trusted peer networks enabling effective behavior and belief change, 3. Developed innovative data and measurement to assess progress, and 4. Empowered both clinicians and patients with skills and tools to support new behaviors. By leveraging the model, we have been able to shift from a belief that “more care is better care” to “the right care is the best care” at a broad scale. Created home-grown measures in KP to understand how effectively we are adhering to evidence based care in a learning environment has helped our clinicians move their thinking about care delivery. Starting with our vision that we have an ethical responsibility to practice evidence based medicine, sharing decisions between the clinical expert (the physician) and the context expert (the patient), we were able to gain alignment on initial topics to measure by different clinical groups. By convening chiefs of specialty together across the KP delivery system, individuals with common backgrounds and interests have gotten to know and trust each other, and were able to identify areas of variation in practices across our geographies. With the vision and trust in place, data was our key barrier to enabling cultural change. Developing credible, relevant data useful at a system level created an appetite at the local sites for data at an actionable level. The trust the individuals have developed in working together create the platform of social networks that allow facile spread. The groups commissioned or created tools and trainings that were adopted rapidly across the network. Our members are getting more appropriate care in breast, cervical and prostate cancer screening. By driving less unnecessary procedures and testing we are avoiding patient harm and cost, and increasing access for people in need of care. By developing a shared vision with trusted clinicians, supporting development of peer networks, providing data and tools we are helping KP be a nidus to change the culture of overdiagnosis in the United States. What started as an exercise to measure Goldilocks care with cancer screening has now been leveraged to measure care elements important to many specialists. By building out innovative performance data, we’ve allowed our clinician networks to know if a change is an improvement. We have unleashed the power of our sys- tem to optimize the potential of the right care for the right patient at the right time. METHODS CONCLUSION A chief of gynecology from one state told another from a different state that her patients would see a shift away from annual to every 3-5 year cervical cancer screening as ‘withholding care’. the second gynecol- ogist shared the education and words used to ensure patient’s knew his sole purpose in coming to work was to save lives, and he would never put a woman’s health at risk for cost. The skeptical chief reflected back the words, borrowed the physician and patient education tools, and led her department to a drop in over screening in the next two years. Peer networks enable idea brokerage across geographies, enabling practice change: an anecdotal example 11Q4 12Q1 12Q2 12Q3 12Q4 13Q1 13Q2 13Q3 13Q4 3.00 % 6.00 % 9.00 % 12.00 % 15.00 % Kaiser Permanente Region A Region B Region C Region D Region E Region F % Male 70+ Urology: % Male 70+ W/PSA (Excluding those w/ prior diagnosis of prostate cancer in past 5 yrs) To change the culture of excessive testing in a systematic way across the 18,000 physicians caring for the 9.5 million patients of Kaiser Permanente. 50% 40% 20% 30% 10% 12Q1 12Q2 12Q3 12Q4 13Q1 13Q2 13Q3 13Q4 14Q1 0% % KP women age 21-65 Kaiser Permanente Region A Region B Region C Region D Region E Region F Period 2014Q1 SCAL:9.77% 12.33% CO: 22.04% Low KP High OBGYN: % women age 21-65 with at least one pap smear in period specified and any prior pap smear within 12 and 30 months of most recent pap smear Amy Compton-Phillips, MD, The Permanente Federation, Chief Quality Officer Linda Radler, MBA, The Permanente Federation, Director of Quality Analysis Alvina Sundang, The Permanente Federation, Reporting and Analytic Manager Angela Wong, The Permanente Federation, Reporting Analyst / Developer 10% 15% 20% 5% 0% % women with mammograms Period Low KP High 42 HI: 0.19% 0.25% NW: 0.33% OBGYN: % women with mammograms done within n months of last mammogram Kaiser Permanente Region A Region B Region C Region D Region E Region F 01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 00 02 04 06 08 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 Just Right Over Under 70% 12% 18% 2012-2013 Mammo All Female 42-74 Linda_Overdiagnosis Poster.indd 1 9/3/2014 9:09:45 AM
Transcript of Changing - Overdiagnosis 3… · Changing Overdiagnosis the Cultureof GOAL RESULTS Three common...

ChangingOverdiagnosis
the Culture of
GOAL
RESULTS
Three common cancers affecting varied populations and screening rates were chosen as our test measures. Cervical, breast and prostate cancer all have tests used to identify early tumors with the goal of detecting these in the curable stage. The first two have well established publicly reported metrics used in accountabil-ity frameworks through the National Committee for Quality Assurance (NCQA); Prostate cancer screening using a PSA is actually recommended to NOT do, with the US Public Services Task Force (USPSTF) citing this as a “D” recommenda-tion – screening does more harm than good.
For each topic we: 1. Created a shared vision with clinical experts, leading with the “why” of how appropriate care benefited patients 2. Built and leveraged trusted peer networks enabling effective behavior and belief change, 3. Developed innovative data and measurement to assess progress, and 4. Empowered both clinicians and patients with skills and tools to support new behaviors.
By leveraging the model, we have been able to shift from a belief that “more care is better care” to “the right care is the best care” at a broad scale.
Created home-grown measures in KP to understand how effectively we are adhering to evidence based care in a learning environment has helped our clinicians move their thinking about care delivery. Starting with our vision that we have an ethical responsibility to practice evidence based medicine, sharing decisions between the clinical expert (the physician) and the context expert (the patient), we were able to gain alignment on initial topics to measure by different clinical groups. By convening chiefs of specialty together across the KP delivery system, individuals with common backgrounds and interests have gotten to know and trust each other, and were able to identify areas of variation in practices across our geographies. With the vision and trust in place, data was our key barrier to enabling cultural change. Developing credible, relevant data useful at a system level created an appetite at the local sites for data at an actionable level. The trust the individuals have developed in working together create the platform of social networks that allow facile spread. The groups commissioned or created tools and trainings that were adopted rapidly across the network.
Our members are getting more appropriate care in breast, cervical and prostate cancer screening. By driving less unnecessary procedures and testing we are avoiding patient harm and cost, and increasing access for people in need of care.
By developing a shared vision with trusted clinicians, supporting development of peer networks, providing data and tools we are helping KP be a nidus to change the culture of overdiagnosis in the United States. What started as an exercise to measure Goldilocks care with cancer screening has now been leveraged to measure care elements important to many specialists. By building out innovative performance data, we’ve allowed our clinician networks to know if a change is an improvement. We have unleashed the power of our sys-tem to optimize the potential of the right care for the right patient at the right time.
METHODS
CONCLUSION
A chief of gynecology from one state told another from a different state that her patients would see a shift away from annual to every 3-5 year cervical cancer screening as ‘withholding care’. the second gynecol-ogist shared the education and words used to ensure patient’s knew his sole purpose in coming to work was to save lives, and he would never put a woman’s health at risk for cost. The skeptical chief reflected back the words, borrowed the physician and patient education tools, and led her department to a drop in over screening in the next two years.
Peer networks enable idea brokerage across geographies, enabling practice change: an anecdotal example
11Q4 12Q1 12Q2 12Q3 12Q4 13Q1 13Q2 13Q3 13Q4
3.00 %
6.00 %
9.00 %
12.00 %
15.00 % Kaiser PermanenteRegion ARegion BRegion CRegion DRegion ERegion F
% M
ale
70+
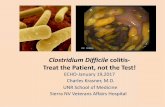
Urology: % Male 70+ W/PSA (Excluding those w/ prior diagnosis of prostate cancer in past 5 yrs)
To change the culture of excessive testing in a systematic way across the 18,000 physicians caring for the 9.5 million patients of Kaiser Permanente.
50%
40%
20%
30%
10%
12Q1 12Q2 12Q3 12Q4 13Q1 13Q2 13Q3 13Q4 14Q10%
% K
P w
omen
age
21-
65
Kaiser PermanenteRegion ARegion BRegion CRegion DRegion ERegion F
Period2014Q1 SCAL:9.77% 12.33% CO: 22.04%
Low KP High
OBGYN: % women age 21-65 with at least one pap smear in period specified and any prior pap smear within 12 and 30 months of most recent pap smear
Amy Compton-Phillips, MD, The Permanente Federation, Chief Quality OfficerLinda Radler, MBA, The Permanente Federation, Director of Quality AnalysisAlvina Sundang, The Permanente Federation, Reporting and Analytic ManagerAngela Wong, The Permanente Federation, Reporting Analyst / Developer
10%
15%
20%
5%
0%
% w
omen
with
mam
mog
ram
s
Period Low KP High42 HI: 0.19% 0.25% NW: 0.33%
OBGYN: % women with mammograms done within n months of last mammogram
Kaiser PermanenteRegion ARegion BRegion CRegion DRegion ERegion F
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 4100 02 04 06 08 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42
2012-2013 MammoAll Female 42-74
Just RightOverUnder70%
12%
18%
2012-2013 Mammo All Female 42-74
Linda_Overdiagnosis Poster.indd 1 9/3/2014 9:09:45 AM