Change and improvement managing change in the NHS 2 booklet
24
Managing Change in the NHS Making Informed Decisions on Change KEY POINTS FOR HEALTH CARE MANAGERS AND PROFESSIONALS
Transcript of Change and improvement managing change in the NHS 2 booklet

ManagingChangein the NHS
Making InformedDecisions on Change
KEY POINTS FOR
HEALTH CARE MANAGERS
AND PROFESSIONALS

What is it for?
The booklet aims to encourage managers andclinical professionals to reflect on, and share,learning and experience of what helps andhinders successful change in pursuit of qualityhealth services.
Drawing on a focused summary of selectedmodels, it explores what has been learned so far about the successful management of change. In particular, it considers:• What findings are of most practical use to
those delivering and organising health servicesand to those receiving those services?
• Where can these lessons be found?
The NHS Plan (DOH, 2000) made it clear thatfar-reaching change is needed if the healthservice is to deliver the standards that patientsexpect and staff want to provide. This bookletsupports the work needed at local levels tomake the plan a reality.
Who is it for?
The booklet offers findings of practical interest to all those attempting to bring about change for the benefit of patients. Health professionals,managers and educators at many different levelshelped to develop the material; as didrepresentatives from patient, community anduser groups.
Making InformedDecisions on ChangeThis is a practicallearning resourcefor all thoseplanning andmanaging change in the NHS.
2

ContentsReinventing the wheel?As a manager or a healthprofessional, where can youstart in planning and puttinginto practice effective changeinitiatives?
4
What works?What can you do to helpmake sure that yourmanagement of change isbased on sound evidenceand best practice?
5
Thinking about change: a rough guideThe sheer size and scope ofthe literature on changemanagement can make ithard for practitioners to findtheir way around. Thissection offers:• signposts through the forest• insights into the real-life
experiences of managersand professionals as theybring about change.
6
Change, in practice In practice, what are the mainfactors affecting the waymanagers and professionalsapproach change?
19
Thinking ahead
Where can you look for
evidence, further information,
help? Should you be thinking
about people, published
resources, learning networks?
21
References 23
Acknowledgements 24
Where does it come from?
The NHS Service Delivery and Organisation(SDO) National R & D Programme was launchedin March 2000. The remit of the Programme isto produce, and promote the use of, researchevidence about how the organisation anddelivery of services can be improved to increasethe quality of patient care, ensure better patientoutcomes, and contribute to improved health inthe wider community.
As one of our first activities, we carried out anational listening exercise which broughttogether a wide range of people – includingservice users, health care professionals, healthservice managers and researchers.
One area of common concern was theimplementation and management of change.This concern on the ground chimed with therequirement for change in pursuit of quality setout in the White Paper, A First Class Service(DOH, 1998).
In response to the specific needs identified, we have developed this publication and a longerreview, Organisational Change, under the seriestitle, ‘Managing Change in the NHS’. See backcover for more information.
3

What changes all thetime but stays the same?
According to an influential articlepublished three years ago, there is oneshort answer to the question, ‘Whatchanges all the time but stays thesame?’ That answer is, ‘The NHS’.
The NHS is 50 years old. Everygovernment since 1948 has re-invoked its founding principles,but there is less agreement abouthow services based on theseprinciples should be organised.Alongside remarkable stability in theespoused purpose of the NHS therehas been almost constant structuralchange. [...] There is a papermountain of advice on reforms,restructuring and managing change.Yet many behaviours do not change.The puzzle is why the NHS has beenso unchanging, given the barrage ofattempts to ‘reform’ it.Plamping (1998)
Some of those who use, work in andcare deeply about the health serviceagree with this insight about behavioursremaining the same. Others point tothe significant changes in clinicalinterventions that are constantly takingplace and argue that substantialchange is already a feature of the NHS– and that patients across the countryare benefiting as a result.
There is little disagreement on a coreissue. That, whatever its record onchange so far, the health service needsto transform itself further so that moreand more people have improvedaccess to more effective services – and feel better about the way they aretreated by the health service.
There’s agreement on something elsetoo. That managers, professionals andstaff in the NHS show a growinginterest in understanding how they candevelop the skills and attitudesnecessary for the kind of continuouschange and learning required in amodern health service.
Making sense of thepressures for change ...
When asked to describe what changemeans for them, managers andprofessionals often talk about:• multiple priorities competing for time• changing external pressures• challenging demands on staff.
All these factors may seem to have anadverse impact on patient care.
Many managers and professionals feela need to bring together disconnectedexternal initiatives and internalrequirements into one coherent,manageable approach.
... and planning your next moves
So, as a manager or a healthprofessional, where can you start inplanning and putting into practice aneffective change initiative?
Are you ...• ... about to implement a change in
your unit or organisation and wouldlike to review the range ofapproaches you might take?
• ... in the middle of a change initiative and want to take a little time to reflecton how things are going?
• ... keen to encourage other people in your organisation to do their best toensure that the way they managechange is based on sound theoryand good practice?
Whatever the focus of your currentconcerns, you’re likely to find it usefulto think about the following questions:• What do I know about effective
change management?• What don’t I know?• What do I need to know in order to
initiate and sustain effective change?• Where can I look for evidence, further
information, help? For example,should I be thinking about people,published resources, learningnetworks?
Reinventing the wheel?
4

Why is the search for evidence important?
Many readers will be seeking ananswer to the question ‘Does it work?’in relation to individual models ofchange management. It is important tobear in mind that neither question noranswer is simple or straightforward.
NCCSDO has been working closely withcolleagues across the NHS and outsideto explore the nature of evidence in thefield of change management. Wealready know that managers andprofessionals are keen to learn fromresearch and to base their decisions onevidence. However, substantial numbersof managers and clinical professionalsargue that much of the evidence abouteffective change management is locatedin the heads of practitioners and has yetto find its way into the scholarly journals.
Evidence can usefully guidemanagement decision-making. But, asdiscussed below, many different typesof evidence are used in this field – andeach type of evidence calls for adifferent kind of review and evaluation.
What counts as evidence?
The academic and research literaturedescribes a wide range of approachesto change management, many of themdiffering in emphasis and focus. What’smore, much of the evidence generatedis from a wide variety of organisationsand from diverse methodologiesmarked by varying degrees of rigour.It is important to recognise that thetype of evidence that is useful inchange management may differconsiderably from the scientificevidence that underpinspharmaceutical and technologicaladvances in medicine.
A broad range of research methods,including methods drawn from thesocial sciences, needs to beconsidered in generating evidence thatwill be helpful to those who make useof and those who deliver health careservices (Fulop et al., forthcoming).
Measuring effectivenessis difficult
Nearly all changes have a wide rangeof effects, some planned, someunplanned. When measuring theeffectiveness of the change, you need totake account of the full range of effects.
Change programmes involve analysingthe causes of the presenting problem,designing the change intervention, andimplementing it. This is rarely a linearprocess, moving from point A to B to C.Characteristically, the process involvesjumping ahead, moving sideways orbacktracking – for example, usinglearning from the implementation phaseto re-design aspects of the programme.
Different people involved in the changeprogramme will have different views ofthe event or events that triggered theprogramme, of the underlying causesof the problem, and of the desirableoutcomes of the programme. So youneed to think carefully about whosemeasures of effectiveness are used.
What works?
Example – Learning about, and from, implementing changeA change initiative implemented in mentalhealth services for older people resultedin improved referrals and outcomes forpatients. Those taking forward the initiativebenefited from the support of the ClinicalGovernance Development Programme(see page 21). They highlighted theimportance of others learning the following:• A structured approach – based on a
critical review of models of change• Staff involvement – including a
consultation process to pave the wayfor change, backed up here by amonthly bulletin
• Responsive leadership – with full backing from the clinical managementteam, e.g. when negotiating time forcommunicating the change
• Avoiding change jargon – conveying the change agenda to staff in day-to-day terms
• Openness to unanticipated outcomes – in this case positive, as when staffthemselves identified a case for movingtowards a central access point forreferrals.
Source: Ann McPherson, Service Manager for Older People’s Services, Wakefield and PontefractCommunity NHS Trust.
5

Finding a path through the literature
A large body of thinking about change has been developed over the last fifty years.The sheer size and scope of the literature can make it hard for managers andpractitioners to find their way around. Organisational Change: a Review (see backcover) attempts to create a pathway by grouping models into four main clustersfocused on key questions:1. How can we understand complexity, interdependence and fragmentation?2. Why do we need to change?3. Who and what can change?4. How can we make change happen?
We offer here a selection of models from each cluster. These range from simple toolsand techniques to broad schools of thought to more complex ‘change packages’.
Thinking aboutchange: a rough guide
6
• Weisbord’s Six-Box Organisational Model• 7S Model• PESTELI• Five Whys• Content, Context and Process Model• Soft Systems Methodology• Process modelling
– Process flow– Influence diagram– Theory of Constraints (TOC)
Why do we need to change?
• SWOT
Who and what can change?
• Force field analysis• ‘Sources and potency
of forces’• ‘Readiness and capability’• Commitment, enrolment
and compliance• Organisation-level
change– Total Quality
Management (TQM)– Business Process
Reengineering (BPR)• Group-level change
– Parallel learning structures
– Self-managed teams• Individual-level change
– Innovation research– Securing individual
behaviour change
How can we makechange happen?
• Organisational development (OD)
• Organisational learning and the LearningOrganisation
• Action research• Project management
How can we understand complexity, interdependence and fragmentation?
How can weunderstandcomplexity,interdependenceand fragmentation?
7
What framewords could help?Managers and clinical professionals are likelyto face the following kind of scenario:
“In the situation where I’m trying to achievechange, there are no cut-and-dried solutions.The situation is complex and dynamic. Thismeans that I can’t plan for everything that willhappen. And I need to take into account thefact that any intervention I make may spark offunplanned consequences. What frameworkscan help me to think constructively aboutliving with this kind of complexity?”
Approaches included here range in scopefrom comprehensive methodologies to singletools. All, however, provide insight intopotential ways of understanding and dealingwith multiple priorities and pressures.

Content, context and process model
What is it?
This model of strategic change, based onempirical case studies, was developed byPettigrew and Whipp (1991) as a means ofgenerating insight into why some private sectororganisations were better able than others tomanage strategic change and improve theircompetitive performance. It suggests thatsuccessful change is a result of the interactionbetween:• Content or what of change (objectives,
purpose and goals)• Process or how of change (implementation)• Organisational context of change (the internal
and external environment).
It is also a reminder that change is influenced byhistorical, cultural, economic and political factors.The model suggests there are five interrelatedfactors important in shaping a firm’s performance:1. Environmental assessment2. Human resources as assets and liabilities3. Linking strategic and operational change4. Leading change5. Overall coherence.
In use
This model has been widely used in analysingand learning retrospectively from changeprogrammes. It was also extended and tested ina major empirical study of change in the NHS(Pettigrew, Ferlie and McKee, 1992).
Both versions of the model provide diagnosticchecklists which can be used to assess thelikely reception of a particular intervention in aspecific locale. The example (see left) showshow one aspect of the model was used to helpimprove change programme interventions.
Example – Preparing theground for change
Carrying out a situationanalysis – an activity whichidentifies barriers, levers andfacilitators for change – is animportant first step indesigning a changemanagement strategy thatwill meet local needs. Thiswas the finding of a studycomparing nineimplementation projects,undertaken by the SouthThames Evidence BasedPractice (STEP) Project during1997-2000. For instance, asituation analysis of oneproject studied (Promotion ofContinence in People over 65 years in Primary Care)uncovered the followingbarriers and opportunities: no existing policies forcontinence care; trust merger;information systems in theprocess of change; and, notleast, five concurrent auditsbeing undertaken by staff,contributing to a feeling ofoverload. Traininginterventions were developedto help staff respondeffectively to the challengesrevealed by the situationanalysis. Outcomes of theseinterventions were: increasedskills in the identification ofsymptoms; more assessmentsundertaken; more treatmentsinitiated; and more patientsoffered care pathways.
Source: Ross and McLaren (2000).
8
Five Whys
What is it?
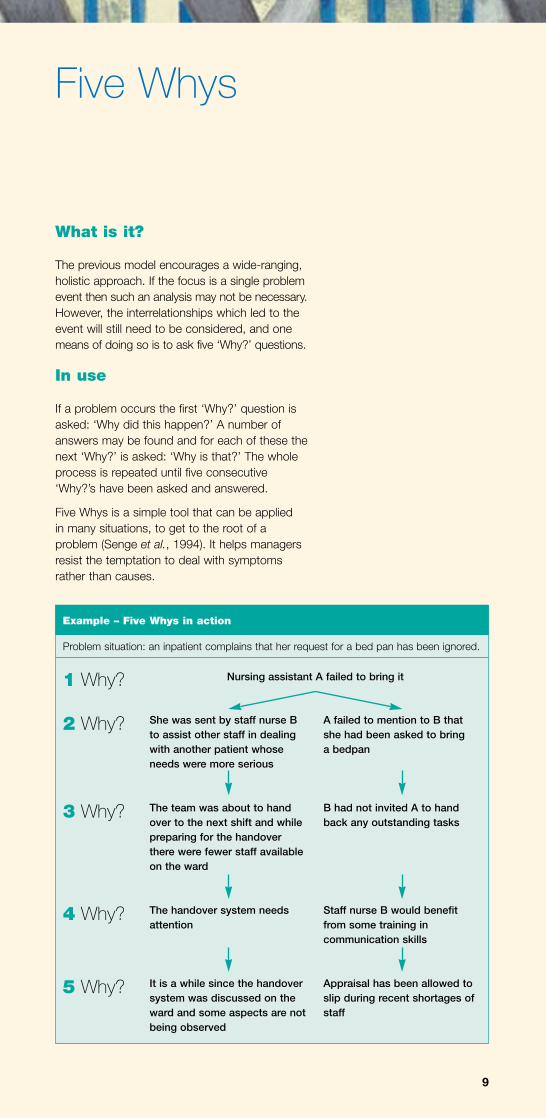
The previous model encourages a wide-ranging,holistic approach. If the focus is a single problemevent then such an analysis may not be necessary.However, the interrelationships which led to theevent will still need to be considered, and onemeans of doing so is to ask five ‘Why?’ questions.
In use
If a problem occurs the first ‘Why?’ question isasked: ‘Why did this happen?’ A number ofanswers may be found and for each of these thenext ‘Why?’ is asked: ‘Why is that?’ The wholeprocess is repeated until five consecutive‘Why?’s have been asked and answered.
Five Whys is a simple tool that can be applied in many situations, to get to the root of aproblem (Senge et al., 1994). It helps managersresist the temptation to deal with symptomsrather than causes.
She was sent by staff nurse Bto assist other staff in dealingwith another patient whoseneeds were more serious
The team was about to handover to the next shift and whilepreparing for the handoverthere were fewer staff availableon the ward
The handover system needsattention
It is a while since the handoversystem was discussed on theward and some aspects are notbeing observed
A failed to mention to B thatshe had been asked to bring a bedpan
B had not invited A to handback any outstanding tasks
Staff nurse B would benefitfrom some training incommunication skills
Appraisal has been allowed toslip during recent shortages ofstaff
Example – Five Whys in action
Nursing assistant A failed to bring it
Problem situation: an inpatient complains that her request for a bed pan has been ignored.
9
1 Why?
2 Why?
3 Why?
4 Why?
5 Why?

What is it?
One way to get a clearer picture of the differentviews and expectations involved in a changeprocess is to use ‘process modelling’. This is atechnique for capturing visually the dynamics ofa situation and articulating how the new one isto be different.
Theory of Constraints is one example. It aims toimprove the performance of any organisationalprocess that involves a series of interdependentsteps. No attempt is made to improve theefficiency of each step in isolation. Instead, theprocess as a whole is analysed, with the goal ofidentifying and addressing bottlenecks – orconstraints – that prevent the process fromincreasing its output.
In use
Theory of Constraints is currently being used inthe NHS – for example, within the RadcliffeInfirmary in Oxford – to tackle waiting lists.
Process modelling –Theory of Constraints
Example – From fragmented to integrated care
In North Tyneside, there was an acknowledgementthat stroke patients were receiving fragmented care.A multidisciplinary audit revealed that baseline datawere not available, there were few agreedoutcomes measures and stroke care was seen aspurely hospital based. A multidisciplinary strokepathway was implemented across the whole of themedical and elderly directorate, followed by acommunity stroke pathway, piloted at a local generalpractice. Evaluation showed consistently high levelsof use of the pathway by professionals. Use of thetool was regarded as one of the major componentsin bringing about what proved to be a successfulchange, reorienting services towards an approachwhich was multidisciplinary, more community-focused, susceptible to audit – and, crucially,centred on the needs of patients and carers.
Source: Richard Curless, Stroke Association District Stroke Services Co-ordinator, North Tyneside Health Care NHS Trust, Report: April 1996-1998.
Process modellingand associatedapproaches stressthe importance ofan integratedapproach tochange and to the planning anddelivery of services.
10

Why do we need to change?
11
What framewords could help?Managers and clinical professionals are likelyto face the following kind of scenario:
“I can’t make the effort that’s needed tobring about effective change if I’m not trulyconvinced it is necessary. The same is true of all the staff in the organisation. Whatframeworks can help me to share anunderstanding of why change is needed?”
In the NHS, as in other complex systems, it is only too easy to look inwards muchmore frequently than outwards – or forattention to be focused on certain types ofdrivers, such as policy directives orperformance indicators. But the real answersto the question, ‘Why do we need tochange?’, lie in identifying and reflecting onthe gaps between what is currently beingoffered and what is likely to be needed in thenext few years. Many models can helppeople to explore either directly or indirectlythe rationale for change.

What is it?
Strengths and weaknesses are internal to theteam or organisation, while opportunities andthreats are external. SWOT analysis focusesattention on the match – or lack of match –between what the team or organisation isgeared up to offer and what the world outsideneeds and wants. In doing so, it encouragespeople to see their own organisation, group orteam from a range of different perspectives.
In use
The SWOT matrix (see below) is one of the mostwidely used strategic planning tools. Evidenceon the relative value of SWOT as a technique isthin on the ground. Some findings suggest thatit can result in over-long lists of factors, generalor meaningless descriptions, a failure to prioritiseissues or no attempt to verify any conclusions.This does not invalidate the use of SWOT butdoes reinforce the point that SWOT needs to beused carefully and with the end in mind ratherthan as a process in its own right.
SWOT analysis
SWOT stands for:
StrengthsWeaknessesOpportunitiesThreats
12
Internal
External
Strengths
Opportunities
Weaknesses
Threats

Who and what can change?
13
What framewords could help?Managers and clinical professionals are likelyto face the following kind of scenario:
“Many different people and processes haveto be involved if change is to be effective. What frameworks can help me to identify thekey areas for my attention?”
Since its earliest days, the NHS has beencharacterised by almost constant structuralchange. Change of this kind has resolvedsome problems, at some times, but has leftmany other deep-seated problems untouched.
There is increasing recognition that people –individuals, teams and workforces – offer thekey to lasting change in the health service.Many will be concerned, therefore, to knowmore about working with others to create anadaptable workforce of the kind described inthe NHS Plan (DOH, 2000) – well led and fitfor practice and purpose. Here we cover twoof the more widely used ‘packages’ thatchange management consultants, amongothers, have used to develop integratedchange programmes.

What is it?
The focus of TQM is on processes of work ratherthan on the workers themselves. Through aprocess of data collection, analysis, hypothesisformation, and hypothesis testing, changes toprocesses can be devised, and the aim is thatthese changes are introduced steadily andforever to improve quality.
In use
In recent years, TQM approaches have beenbrought to health care. These aim to involveclinical staff in quality management, suggestingthat many may need to develop skills in:• working effectively in teams• understanding work as a process• collecting, aggregating, analysing and
displaying data on the outcomes of care and also on the processes of care
• designing work processes• collaborative exchange with patients• working collaboratively with non-medical
managers.
Given the number and complexity of theprocesses involved, TQM approaches haveunderstandably proved difficult to evaluatemethodically. Few empirical studies providecomparative information about the impact ofTQM on health care organisations. Evaluationsof TQM in the NHS have found thatimplementation is often piecemeal, and rarelyfocused on core organisational processes – thatis, clinical practice – concentrating instead onperipheral and administrative activities.
Total QualityManagement (TQM)
TQM refers to a managementprocess directed at establishingorganisedcontinuousimprovementactivities, involvingeveryone in anorganisation in atotally integratedeffort towardimprovingperformance atevery level.
14

What is it?
BPR is a technique for corporate transformationthat came to prominence in the early 1990s, andis defined as:
... the fundamental rethinking and radicalredesign of business processes to achievedramatic improvements in critical,contemporary measures of performancesuch as cost, quality, service and speed.Hammer and Champy (1993)
The main concepts that underpin BPR includethe following.• Organisations should be organised around key
processes rather than specialist functions.• Narrow specialists should be replaced by
multi-skilled workers, often working in self-managed teams.
• In contrast with incremental techniques such as TQM, BPR involves total disassociationfrom current practices and radical rethinking.
• The direction for the requisite radical rethinkingcomes unequivocally from top management.
In use
In the NHS, evaluations at Leicester RoyalInfirmary and at King’s College Hospital, London,found that two of the central principles of BPR –the radical, revolutionary approach to changeand the erasing of historical context – arefundamentally incompatible with the traditions,culture and politics of the NHS.
A more recent evaluation has indicated thatsome reengineering techniques can be usedwithout entailing a whole-organisation approach.For example, the National Patients’ Access Teamincludes among its initiatives the national bookedadmissions programme which makes use ofreengineering or ‘redesign’ techniques. Redesigncan be defined as thinking through the bestprocess to achieve speedy and effective carefrom a patient perspective (Locock, forthcoming).
The guiding principles of TQM and some of thetools of BPR also make a major contribution tothe ‘Breakthrough’ programme of the Institute of Healthcare Improvement. In time this willgenerate valuable evidence in this area.
Business ProcessReengineering (BPR)
Example – Using BPRtechniques as a preludeto change
King’s College Hospital inLondon uses a range ofspecific techniques for itschange programme. Theprogramme includes tacklingoutpatients appointmentssystems and helping staffdeliver bad news to patientsmore effectively. Each projectstarts by ‘mapping’ acommon understanding ofthe current situation. This isoften done by developing aprocess map – of a system,say, or the patient’s journeythrough this. This is done asa team, with facilitation, toreflect not what shouldhappen but what happens inreality. This highly visualmethod has been found toalter individuals’ perceptionsas, for example, doctorssuddenly realise that nursesdo a range of tasks theynever knew about and viceversa. Encouraged by theseinsights, staff are more likelyto buy into the wider changeprogramme.
Source: Kate Grimes, Programme Leader, Transforming Healthcare Delivery, King’sCollege Hospital NHS Trust.
15

How can we make change happen?
16
What framewords could help?Managers and clinical professionals are likelyto face the following kind of scenario:
“I understand the situation. I know why weneed to change. I see who and what needsto change. But how can all this insight beused to create a change initiative that willreally deliver the results that are needed?What frameworks can help me?”
If implementation is thought about quiteseparately from the planning and design of a change initiative, then it is likely that theinitiative will already have failed. Successfulchange initiatives hardly ever follow a simplepattern of ‘thinking’ followed by ‘doing’.Instead, thinking informs doing and doinginforms thinking throughout the process, in an iterative way.
Many change management models and toolscan be used when thinking about how tomake change happen. Here we look at twoinfluential approaches which can be appliedat several different levels. Each suggests indifferent ways the importance of learningfrom change – and using key learning pointsto inform the next steps.

What is it?
Less a model than a school of thought, theconcept of the Learning Organisation (or‘learning company’) is increasingly popular asorganisations, subjected to exhortations tobecome more adaptable and responsive tochange, attempt to develop structures andsystems that nurture innovation.
In use
Much of the literature prescribes howorganisations should be designed and managedto promote effective learning. There is relativelylittle systematic research to support thesesuggestions. However, there is growingconsensus about the features that characterisethe Learning Organisation.
The LearningOrganisation
17
Learning Organisations have flat managerial hierarchies thatenhance opportunities for employee involvement in theorganisation. Members are empowered to make relevantdecisions. Such structures support teamwork, strong lateralrelations, and networking across organisational boundaries bothinternal and external (e.g. project teams).
Learning Organisations require information beyond that used intraditional organisations where information is generally used forcontrol purposes. ‘Transformational change’ requires moresophisticated information systems that facilitate rapidacquisition, processing and sharing of rich, complex informationthat enable effective knowledge management.
People are recognised as the creators and users of organisationallearning. Accordingly, human resource management focuses onprovision and support of individual learning. Appraisal and rewardsystems are concerned to measure long-term performance and topromote the acquisition and sharing of new skills and knowledge.
Learning Organisations have strong cultures that promoteopenness, creativity and experimentation among members.They encourage members to acquire, process and shareinformation, nurture innovation and provide the freedom to trynew things, to risk failure and to learn from mistakes.
Like most interventions aimed at securing significantorganisational change, organisational learning depends heavily oneffective leadership. Leaders model the openness, risk taking andreflection necessary for learning and communicate a compellingvision of the Learning Organisation, providing empathy, supportand personal advocacy needed to lead others towards it.
Structure
Information systems
Human resource practices
Organisational culture
Leadership
The main characteristics of the Learning Organisation

What is it?
This is a form of collaborative, critical inquirydrawing upon organisational learning and usuallyconducted by practitioners and managers, ratherthan expert academic researchers. In the field ofhealth, Donald Berwick advocates the use ofsmall-scale, short-cycle tests based on a Plan-Do-Study-Act learning cycle. He suggests thatthis particular form of action research enableshealth care teams to learn on the basis of actionand its observed effects rather than on the basisof theory alone.
In use
Action research of this kind is now beingenacted in the NHS, for example within theCancer Services Collaborative.
In trying to improve the process of care,wisdom often lies not in accumulating all ofthe information but in acquiring only thatamount of information necessary to supporttaking the next step.Berwick (1998)
Action research has been used successfully in avariety of change programmes. Success hasbeen found to be largely dependent onorganisational context, with difficulties rooted inpolitical and interpersonal conflict betweenresearchers and managers.
Action research
Example – Commitment to sharing learning about change
The West London ResearchNetwork (WeLReN) is aprimary care research networkcovering four London healthauthorities. It aims to producein primary care high-qualityresearch, increased researchcapacity and aims to changethe culture towards reflectiveinquiring practice. A series ofeducational courses helpnovice researchers to developside by side with moreexperienced researchers. Aswell as randomised controlledtrials and qualitative researchprojects WeLReN facilitatesparticipatory action research(PAR) projects. These areparticularly suited toresearching health caresystems. Multidisciplinaryteams explore what needs tochange in differentprofessional groups and theyfeed back this information tothe others involved to producecycles of research, feedbackand action. This helps peopleto understand what they haveto do to implement researchfindings – to move fromresearch to development. PaulThomas, founder of WeLReN,explained: ‘The carrot andstick metaphor is designedfor donkeys undertakingshort journeys. If we wantsustainable development wehave to equip people with theskills and resources for amuch longer journey – and wehave to treat people properly.’
Source: Paul Thomas, Director ofWeLReN, Department of Primary Careand General Practice, Imperial CollegeSchool of Medicine, London.
18

People will have different starting points
In practice, what are the main factors affectingthe way managers and professionals approachchange and change management theory?
Extensive discussion with people working in avariety of organisations and clinical settingssuggests that in everyday situations most peopleare concerned about the following issues.
Who wants the change? and why?• Where is the drive for the change coming from?• How powerful is it?• Is it from within the service or organisation?
or is the change being imposed upon it?• Who is opposed to the change? and why?
Importance for the unit/organisation• How does the change fit in with the other
performance objectives set for the unit ororganisation? What priority should be given tothis initiative?
• How radical is the change needed?• Are we already doing something to address
the issues involved in the initiative?
Performance measurement• Who is measuring the success of the change?• What are their concerns and how do they
measure success?
Consultation with staff• What professional groups are involved in or
affected by the change?• How easy will it be to involve these groups in
discussions and in the development of asolution?
• Are the staff groups concerned already involved with a number of other changes?
Initial questions of the kind outlined above arehelpful in enabling managers and professionalsto orientate themselves in relation to the needfor renewed change, and to start planning andimplementing the change. But as the changeinitiative gets underway, those ‘in charge’ tendto find themselves experiencing and beingdrawn into a range of tensions and dilemmas.
Change, in practice
Example – Respondingcreatively to difference
For every change initiative,including in the same trust orthe same service, people willhave very different startingpoints. In one service in ourtrust, for example, peopleidentified a need to changeand responded positively. In another, the service wasalready seen to be performingwell, so there was resistancefrom key stakeholders.Conducting reviews of bothat the same time gave usvaluable information aboutthe system, as well as helpingus negotiate and disseminatechange strategies moreeffectively.
Source: Ann Lambkin, Head of Midwiferyand Gynaecological Services, West DorsetGeneral Hospital NHS Trust.
Example – How not to winhearts and minds
A senior management teamwent away for a weekendretreat, to look at currentissues and brainstorm aboutthe future. There was a fairamount of disagreementduring the weekend but bythe time they got back to theirorganisation, all storms werespent and they had agreed ona common approach. Theysent memos down the line,telling middle managementwhat to think and do. Whensome middle managers cameback with critical comments,the reaction was ‘Ah ha! Sonow we’ve identified thechange resistors!’
Source: Adapted from Weil (1993).
19

Tensions and dilemmas
Managers and professionals who have spenteven a few years in the health service will havebeen affected by several waves of changeinitiatives. They may well feel that each waveserves mainly to wash away the deposits, goodand bad, left by the one before. Key words mightbe ‘disconnected’, ‘fragmented’ and ‘wary’.
Managers may be familiar too with some of thetensions and dilemmas highlighted (see left).
So, what next?
Many models offer something to those chargedwith managing change. Some are more widelyimplemented, some more rigorously tested.Important lessons for future changemanagement have been learned within andacross different localities. Perhaps the over-arching lessons are:• The importance of analysing the local situation
and planning an intervention accordingly• Every intervention will have some unplanned
consequences as well as the planned ones• Putting evidence into practice is a lengthy and
complicated process• Frontline staff need to be offered benefits and
research must be clearly related to currentpractice (Ywye and McClenahan, 2000).
Managingchange –the reality
Change is often imposed uponmanagers to meet prioritieswhich differ from the prioritiesperceived as most important bythe key opinion formers withinthe unit or organisation – inparticular, the clinicians.
There is a tension between theinstruction to ‘gain ownership’of a particular change initiativeand the instruction to deliverthe change quickly.
Priorities change, and so achange programme may beovertaken by other initiatives.
Amid new initiatives, it is veryeasy to lose sight of theoriginal objectives of achange programme – and onlytoo easy to implement a seriesof actions which may no longerbe the most relevant.
Many staff members arecynical about consultationprocesses, born of experienceof ‘pseudo consultation’ and of change associated withcurbing costs.
Change of any kind inevitablyinvolves some kind of loss,which may need to beaddressed.
There is scepticism aboutchange techniques importedfrom the private sector. Clinicians will value evidenceabout the virtues of a change ina form with which they arefamiliar, but this may not beeither available or appropriate.
There is an opportunity cost,measured in lost patient care,associated with time spentplanning and implementingchange.
Managers tend to stay inpost for shorter periods thantheir clinical colleagues andthus are not able to see achange programme throughfrom start to finish, nor to learnfrom the results.
20

Read? Talk? Listen?
Whatever the focus of your current concerns,you’re likely to find it useful to:• consult the resource and reference tool in the
same series as this booklet – OrganisationalChange (see back cover for further details)
• talk to specialists in change management – inside and outside your own organisation
• link into the NHS Learning Network• seek out further research evidence on
organisational change.
Working with specialists in change management
There are people you can access who haveconsiderable experience and knowledge ofchange management in health care. Often theycan be found in Human Resource (HR)departments, Lifelong Learning teams, orClinical Governance units. If you cannot locatethem in your own organisation, your RegionalOffice of the NHS Executive will be able to pointyou in the direction of a local resource.
What kind of help might be available?See right for some examples of issuesassociated with change management that haveusefully been raised at exploratory meetingsbetween clinicians and change specialists.
Of course, those driving forward change oftenwant to extend their own repertoire of skills andknowledge, as well as make effective use ofchange specialists. In these circumstances, thereis a need for training and development groundedin theory as well as in real life managementissues. The NHS Clinical Governance SupportTeam, based in Leicester, offers an initiative tosupport this kind of development (see page 23).
Thinking ahead
‘Can you help?’
“The success of my changeprogramme depends on peoplefrom different clinicalbackgrounds working togetherwith mutual respect andunderstanding. We’ve a longway to go to achieve this. Canyou help facilitate an initialdiscussion with a range ofprofessionals? Are there anystructured ways of doing thisthat would be helpful?”
“Can you point me in thedirection of someone who hasprepared a good project planbased on a critical path?”
“Can you help our team do aSWOT analysis? We’re prettyclear about our strengths andextremely clear about ourweaknesses, but we’re not soclear about opportunities andthreats. We’ve all got a feelingthat there’s a lot going onoutside the organisation thatwe never get a chance to catchup on.”
“Can you help us evaluate thechanges we are about to make?”
21

Linking into the NHS Learning Network
The NHS Learning Network was developed inresponse to the reality of the pressure on timeexperienced by many NHS staff and managers.Often agendas are full, and there seems little‘headroom’ for learning about how others in thehealth service are facing and tackling commonissues – particularly how to improve andmanage services.
Using a range of approaches, including theinternet and the telephone, the NHS LearningNetwork aims to:• provide busy staff with practical help in
modernising services and raising clinicalstandards
• ensure that the considerable expertise within the NHS is shared and used effectively – forexample, linking into the Learning Networkenables users to share their learning directly aswell as benefit from the experience of others
• provide support to those leading and managing change.
Web: www.doh.gov.uk/learningzone/index.htm
For further information, contact the LearningNetwork Manager, tel 0113 254 6433, or Paul Adams, tel 01225 824120.
Seeking out further research evidence
Databases for exploring further researchevidence on organisational change
Health Management Information Servicesdatabase (HMIC) – contains information on theliterature relating to health systems managementpublished in the UK and internationally –including journals, books, reports, officialpublications, and ‘grey’ literature (unpublisheddocuments). Access via HMIC (HealthManagement Information Consortium).Web: www.silverplatter.com/catalog/hmic.htm
HealthSTAR – a bibliographic database fromthe National Library of Medicine and theAmerican Hospital Association containingrecords of literature relating to health caredelivery. Access via Internet Grateful Med.
22

References
Berwick, D. 1998. Developing andtesting changes in delivery of care.Annals of Internal Medicine, 8: 8,651-6Department of Health (DOH)1998. A First Class Service: Qualityin the New NHS. London: TheStationery OfficeDepartment of Health (DOH)2000. The NHS Plan. London: The Stationery OfficeFulop, N., Allen, P., Clarke, A.and Black, N. (eds) (forthcoming).Studying the Organisation andDelivery of Health Services:Research Methods. London:RoutledgeHammer, M. and Champy, J. 1993.Reengineering the Corporation: aManifesto for Business Revolution.London: Nicholas BrealyLocock, L. (forthcoming). Maps andJourneys: Redesign in the NHSBirmingham: Health ServicesManagement Centre, University ofBirminghamPettigrew, A., Ferlie, E. andMcKee, L. 1992. Shaping StrategicChange. London: SagePlamping, D. 1998. Change andresistance to change in the NHS,British Medical Journal, 4 July, Vol317, pp 69-71Ross, F. and McLaren, S. 2000. An Overview of Aims, Methods andCross-Case Analysis of NineImplementation Projects. The SouthThames Evidence Based Practice(STEP) Project, Kingston Universityand St George’s Hospital MedicalSchool, University of LondonSenge, P., Kleiner, A., Roberts, C., Ross, R. B. and Smith, B. J.1994. The Fifth Discipline Fieldbook:Strategies and Tools for Building aLearning Organisation. New York:DoubledayWeil, S. 1993. ‘Managingfundamental change’, Conferencepaper 7. London: Office for PublicManagementYwye, L. and McClenahan, T.2000. Getting Better with Evidence.Experience of Putting Evidence intoPractice. London: King’s Fund
This resource is also available via CD-ROM andonline hosts.Web: igm.nlm.nih.gov/
Bath Information and Data Services (BIDS) –provides UK academic institutions with abibliographic service and offers links to 2,700full-text electronic journals.Web: www.bids.ac.uk/info/fs_aboutbids.htm
Reviews of evidence relating to health caredelivery and organisation
The Cochrane Effective Practice andOrganisation of Care Group (EPOC) – a Collaborative Review Group of the CochraneCollaboration which aims to inform health carepractice through the production of systematicreviews, including reviews of organisationalinterventions.Web: www.abdn.ac.uk/public_health/hsru/epoc/
The NHS Centre for Reviews andDissemination (CRD) – provides the NHS withinformation on the effectiveness of the deliveryand organisation of health care. Web: www.york.ac.uk/inst/crd/centre.htm
The Campbell Collaboration – an emerginginternational effort to help people make informeddecisions. Prepares and promotes access tosystematic reviews of studies on the effects ofsocial and educational policies and practices.Web: campbell.gse.upenn.edu/
Other useful web sites and contacts
NHS Executive – provides links to RegionalOffices and other organisations:www.doh.gov.uk/nhs.htmNational Patients’ Access Teamwww.health-secure.net/channels/npat/The NHS Clinical Governance Support Teamwww.cgsupport.org/The National Primary Care Development Teamwww.npdt.org/contact.htmNHS Beaconswww.nhsbeacons.org.uk/The Modernisation Agency: Project Manager,Roger Tyrell, email [email protected] or tel 020 7210 5958HR Directors’ Bulletinwww.doh.gov.uk/hrbulletin/
23

Also available
Organisational ChangeA review for health caremanagers, professionals and researchers
by Valerie Iles and Kim Sutherland
• How much is known about what works in change management?
The literature about change management is noteasy to access – it is extensive and spreadacross academic disciplines. This resource andreference tool is designed to bring key changemodels together into one place and takereaders through them.
104 pages
Making Informed Decisions on Change
Researchers and writersMarsaili Cameron and Steve Cranfield, independentconsultants; Valerie Iles,Honorary Senior Lecturer,London School of Hygiene & Tropical Medicine; Jud Stone,independent consultant
Administration and design Margaret Mellor; Sign
Project sponsorsMaureen Dalziel and Naomi Fulop, NCCSDO
Professor Sir John Pattison,Director, NHS SDO R & DProgramme
Project management(NCCSDO)Helena Ward, Gráinne Kavanaghand Pamela Timms
Further copiesKate Thomas, Co-ordinator,NCCSDO, London School ofHygiene & Tropical Medicine, 99 Gower Street, London WC1E 6AZ
Tel: +44 (0) 20 7612 7980Fax: + 44 (0) 20 7612 7979Email: [email protected]
Web: www.sdo.lshtm.ac.uk
Date of issue: May 2001
Copies of Organisational Changecan also be ordered.
AcknowledgementsWe are grateful to the large number of people from differentsectors who contributed to the early development of thisbooklet, particularly those who attended the seminar held inLondon on 12 July 2000 and those who piloted the material.
Our thanks go to:Paul Bate, University of Birmingham; David Bawden,Commission for Health Improvement; Jonathan Boyce, Audit Commission; Cressy Bridgeman, Audit Commission;Donna Covey, Association of CHCs England & Wales; LizaCragg, Greater London Authority; Jennifer Dixon, King’s Fund; Michael Dunning, ImpAct; Debra Humphris, University ofSouthampton; Rod King, King’s College Hospital NHS Trust; Yi Mien Koh, Kensington & Chelsea and Westminster HealthAuthority; Annabelle Mark, Middlesex University; Lucy Moore,NHS Executive London; Matt Muijen, The Sainsbury Centre forMental Health; John Oldham, National Primary Care DevelopmentTeam; Steve O’Neill, NHS Clinical Governance Support Team;David Patterson, Whittington Hospital NHS Trust; Peter Pillay,Parkside Health NHS Trust; Huw Richards, King’s Fund; JohnRiordan, North West London Hospitals NHS Trust; Jenny Secker,King’s College, London; Laura Sharpe, City & Hackney PCG;Joanne Shaw, Audit Commission; Graham Thornicroft, Instituteof Psychiatry; Anne Walker, University of Aberdeen; DawnWakeling, MIND; Laura Wellings, Lewisham Hospital NHS Trust.
PermissionsWe are grateful to the following for their kind permission to usequoted and copyright material, and for providing material for thecase examples.BMJ Publishing Group for the quotation on page 4Richard Curless for ‘From fragmented to integrated care’ Kate Grimes for ‘Using BPR techniques as a prelude to change’Valerie Iles and Kim Sutherland for material from Organisational
ChangeAnn Lambkin for ‘People will have different starting points’Ann McPherson for ‘Learning about, and from, implementing
change’Fiona Ross and Susan McLaren for ‘Preparing the ground
for change’Paul Thomas for ‘Commitment to sharing learning about change’Susan Weil for ‘How not to win hearts and minds’.
Photo montage: FORMAT Photographers (Jacky Chapman,Brenda Prince, Joanne O’Brien, Paula Glassman, Maggie Murray,Ulrike Preuss)
Every effort has been made to identify and contact copyright owners.The publishers would be pleased to hear from anyone whose rightshave been unwittingly infringed.
The SDO R & D Programme is a national research programme managedby the National Co-ordinating Centre for NHS Service Delivery andOrganisation under contract from the NHSE R & D Directorate.
Helping to close thegap between theoryand practice
ManagingChangein the NHS
OrganisationalChangeA REVIEW FOR HEALTH CARE MANAGERS, PROFESSIONALS AND RESEARCHERS
ManagingChangein the NHS
Valerie Iles and Kim Sutherland