Urology EMR Software: Why implementing RevenueXL's Urology EMR is the right choice?
Upload
thitconferenceCategory
view
239download
2description

1
Challenges in Implementing EMR
The Singapore Story
Dr. Chong Yoke SinCEO, IHiS

About Singapore
about Singaporeand IHiS

3
~ 5.4 million people on 707.1 sq km (6,489/km2)Ethnically diverse:
Chinese: 75% Malays: 14% Indians: 9% Others: 2%
40,000+ healthcare providers11,230 hospital beds~450,000 hospital admissionsPublic sector out-patient visits
Specialist Outpatient Clinics ~3.6m A&E ~800k Polyclinics ~4m
Singapore is a small vibrant country

4
IHiS is a healthcare-IT leader, transforming patient care throu gh excellence in technology.
Our healthcare-IT professionals architect and manage the highly integrated systems across Singapore’s Regional Health Systems, public hospitals, national specialty centres and polyclinics.
IHIS played a key role in 7 out of 8 Singapore hospitals and 1 Primary Care facilities becoming among the first public institutions in the Asia Pacific region to achieve HIMSS EMRAM Stage 6, an international benchmark for advanced technology used in patient care.
IHIS works with the healthcare institutions to drive innovation so as to achieve new standards in quality care.
Integrated Health Information Systems

A humble beginning …
A humble beginning …
6
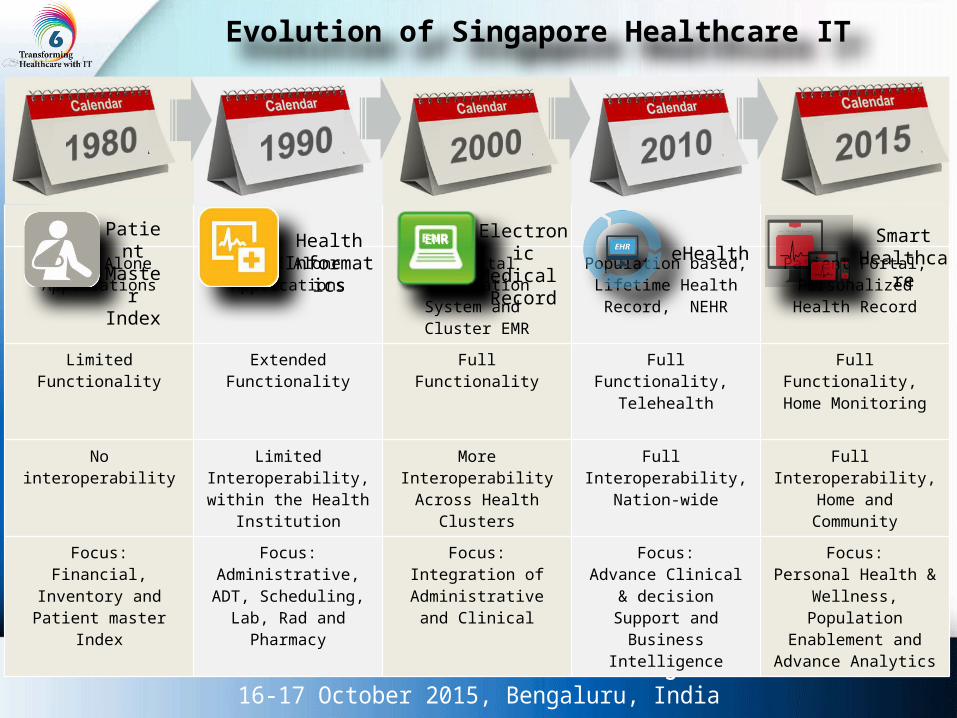
Evolution of Singapore Healthcare IT
Stand Alone Applications
Stand Alone Applications
Hospital Information System and Cluster EMR
Population based, Lifetime Health Record,
NEHR
Patient Portal, Personalized Health
Record
Limited Functionality Extended Functionality Full Functionality Full Functionality, Telehealth
Full Functionality, Home Monitoring
No interoperability Limited Interoperability, within the Health
Institution
MoreInteroperability
Across Health Clusters
Full Interoperability,
Nation-wide
Full Interoperability,
Home and Community
Focus:Financial, Inventory and Patient master
Index
Focus:Administrative, ADT,
Scheduling, Lab, Rad and Pharmacy
Focus:Integration of
Administrative and Clinical
Focus:Advance Clinical &
decision Support and Business Intelligence
Focus:Personal Health &
Wellness, Population Enablement and
Advance Analytics
Patient Master Index
SmartHealthcare
Health Informatics
Electronic Medical Record
EMReHealth

The driving force behind the change …
8
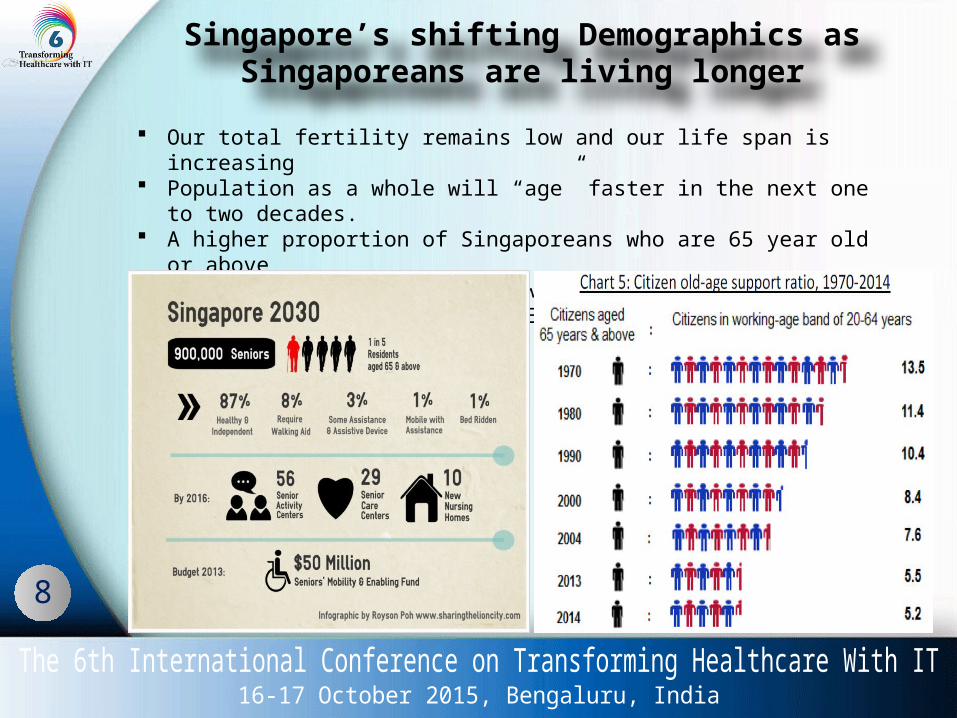
Our total fertility remains low and our life span is increasing Population as a whole will “age” faster in the next one to two decades. A higher proportion of Singaporeans who are 65 year old or above By 2030, one in five of us, will be 65 years and older Fewer Working-Age Adults to Each Citizen Aged 65 and above
Singapore’s shifting Demographics asSingaporeans are living longer

9
?
Healthcare 2020 Master Plan

Our Strategies …
11
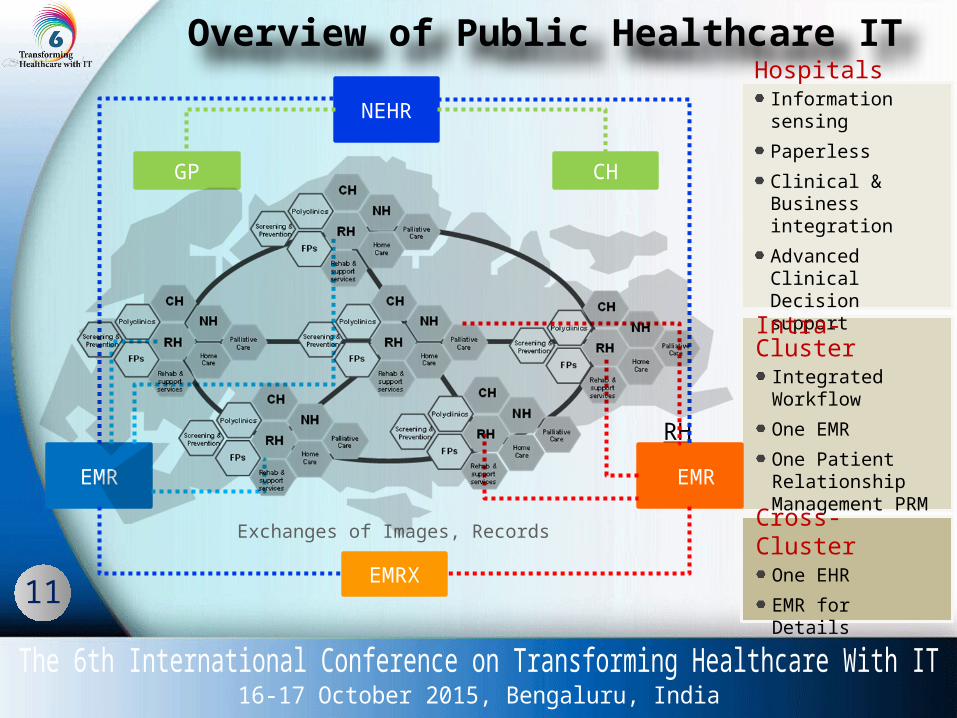
Overview of Public Healthcare ITHospitals
Information sensingPaperlessClinical & Business integrationAdvanced Clinical Decision support
RHEMR EMR
NEHR
GP CH
EMRXExchanges of Images, Records
Intra-ClusterIntegrated WorkflowOne EMROne Patient Relationship Management PRMCross-
ClusterOne EHREMR for Details
12
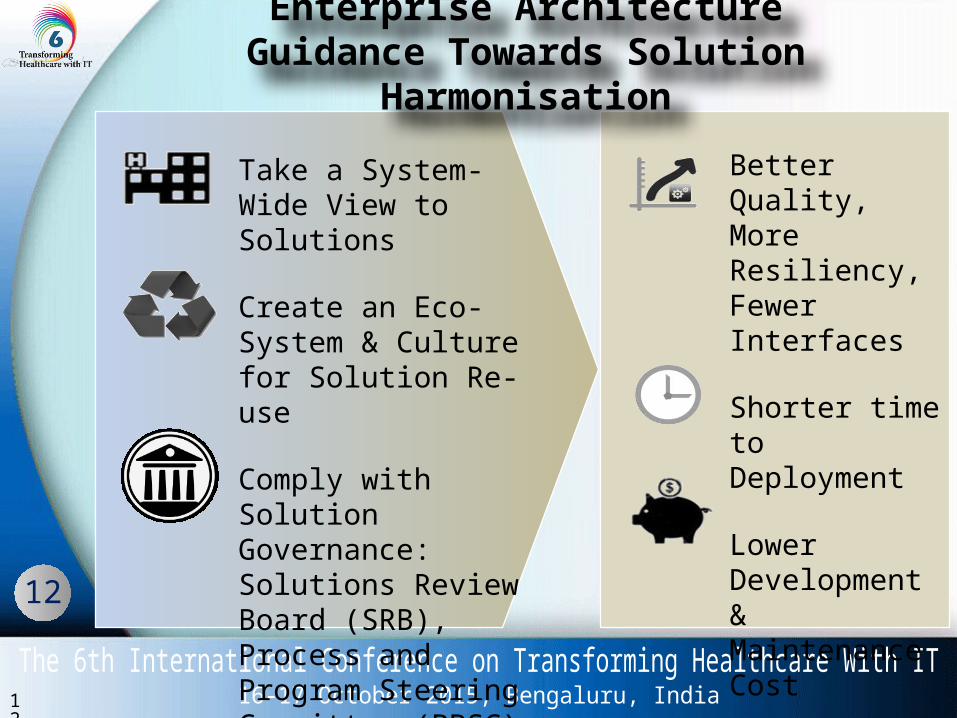
Take a System-Wide View to Solutions
Create an Eco-System & Culture for Solution Re-use
Comply with Solution Governance: Solutions Review Board (SRB), Process and Program Steering Committee (PPSC)
Better Quality, More Resiliency, Fewer Interfaces
Shorter time to Deployment
Lower Development & Maintenance Cost
Enterprise ArchitectureGuidance Towards Solution Harmonisation
12

13
Strategy to achieve Non-Disruptive IT shared Services
Federated Enterprise Architecture
PHI Operating Model
EMRs/NEHR/Clinical systems / Master patient index
Patient Relationship ManagementConnect with AIC, NH, CHs, GPs, etc
Interface through QDX Standardize Integrate and Optimize
Architect the Roadmap
Integrate the Systems
Patient Centric Records

14
ICD 10 AM SNOMED CT LOINC
Structured notes Clinical analytics
Clinical decision support (EMRs, NEHR)
Tele-health
Integrate Analytics across
Continuum
Intervene at the Right Channels
Back to BasicsData Standard and Right Channel
Common Data
Standardized

About IHiS
EMROur EMR Journey …

16
04/28/2023 16©2011 Healthcare Information and Management Systems Society
?
Strategies 2001 2003 2005 2007 2009 2011 2013 2015
Achieving High Quality Integrated Care & Advance Clinical Analytics
BuildingClinical Capabilities, Harvest Full Potential & Benefits of EMR
Consolidation Core Systems, Harmonize Clinical Process & Workflow
20052001
20102006
20152011
Advance Clinical Analytics Proactive and Predictive Alerts Tele-Health, Self-Monitoring & Home Care Mobile Health – Healthcare Social Media Analytics for population care EMRAM Stage 6/7
A common EMR platform & EMRX
Results Reporting and Discharge Summary
Perioperative & ED Notes Cluster eRx, Film-less
Clinical & Nurse Documentation Knowledge-Based Medication
Management CLMM Implementation CPOE/CCOE Implementation eLab & eRad interface to EMR
Cluster’s EMR
The ABC of
digital journey
Our EMR Journey …
17
Cluster EMR Roadmap• Application Landscape• EMR Building Blocks
Implementation Strategies EMR Capabilities Highlights:
• CLMM• CPOE• Clinical Document• Coding Standardization• Statistics
Benefits Challenges & Lessons Learnt
Our EMR Journey …
18
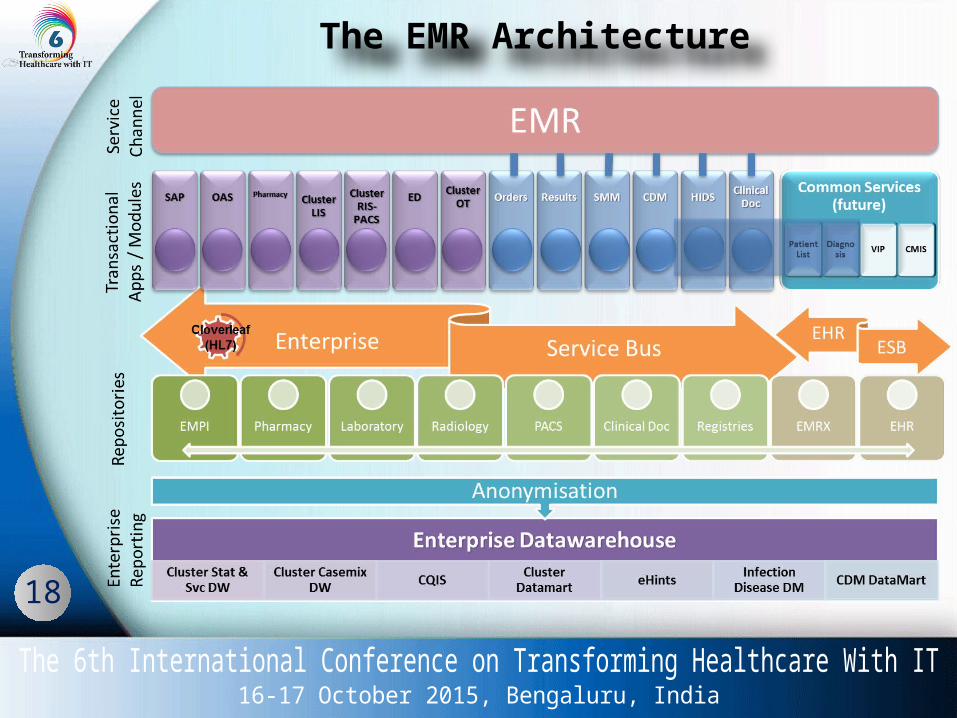
The EMR Architecture
Patient Safety, Our First Priority
Closed Loop Medication Management (CLMM)

20
Value to Patients• Improve patient safety through reducing
medication errors Value to Hospitals / Staff
• Remove waste, improve system efficiency Technology Innovation
• 1st in Asia with a complete end-to-end closed-loop solution
Scalability• Implemented in KKH, NUH and TTSH• Average Unit Dose Serving / year
KKH - 3.9m of unit dose drugs for 65,000 patients NUH - 5.5m of unit dose drugs for 92,000 patients TTSH - 6.6m of unit dose drugs for 110,000 patients
WHY Closed Loop Medication Management
21
WHAT are the CLMM components
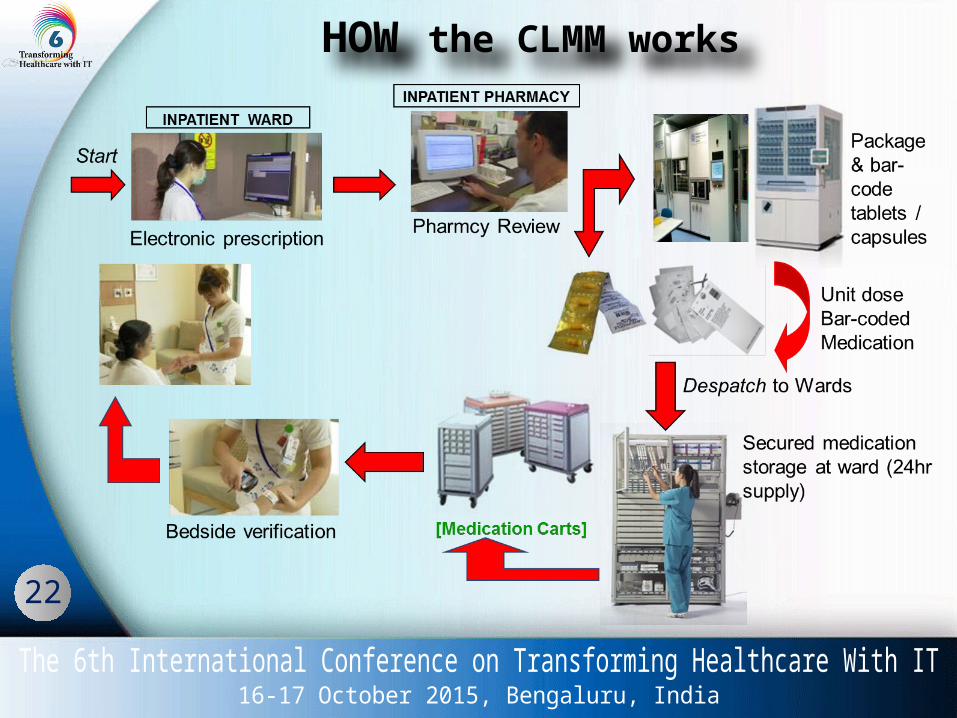
Electronic Prescription System• Patient’s medication prescriptions
Clinical Decision Support System (CDSS)• Enterprise wide Business Intelligence
to support clinical care
Packaging Robot• Unit dose Packaging
Nursing Administration System• Bar-code technology to serve drugs
correctly
22
HOW the CLMM works

23
CLMM ensure 5 RIGHTS
Right patient Right drug
Right dose
Right route
Right time
Enhanced Medication Safety Process
• Improve patient safety
Efficiency of ward processes• Reduce turn around time for
medication stock• On-time, on-demand serving
(urgent medication order) No more faxing of prescription
• Improve the billing process Billing is done upon medication
administration
24
Lessons Learnt• Robot technology for filling medication according to orders from EMR system
eliminate human errors and enhanced patient safety.
• The 2D barcode is capable of storing more information and also ensure higher degree of accuracy compared to one dimensional bar code.
• If the unit dose packaged medication is not consumed or when the doctor change the patient’s medication, it can be returned to pharmacy for the next patient.
• For the medications bundled with a ring, it helps to speed up the cart-fill and enable the pharmacy staff to spend more time for other clinical activities.
• The robot is capable of packing mini-bottle medicine but not big bottles.
• Labeling medications with 2D barcode enables clinicians to scan and verify medication administration at the point of care, helping to ensure the ‘5 rights’ of medication administration.
• Filling the robot for unit dose packing has to be observed very closely for patient safety

Clinical Documentation & Standard
Better Communication, Quality Reporting,
More Effective Patient Care

26
Organization Support• Effective systems to support accurate and concise documentation of practice
in medical records• Appropriate policies and procedures in relation to effective documentation
systems, practices and management of patient health information• The provision of adequate time allocation to document appropriately and
review previous documentation as part of patient care
Leadership• Involve clinical staff in decision making in relation to selecting, implementing
and evaluating documentation systems• Implementing quality improvement processes related to effective
documentation• Promote documentation as an integral and core part of practice and
professional responsibility
Resources• Access to an appropriate physical environment that supports and increases
efficiency and confidentiality of documentation• Reliable, accessible and appropriately maintained equipment
EMRClinical Documentation Implémentation Stratégies
27
• Engage all clinical chiefs and administratorson the new clinical documentation
• Conduct roadshow for all doctors to create awareness
• Set up ‘sandbox’ with feedback system forclinicians to trial the new clinical documentation
• Implement clinical documentation in outpatientsettings first as it is less complex than the inpatient settings
• Implement clinical documentation with a group of related stakeholders
• Deploy additional IT support staff on site during the rollout
EMRClinical Documentation Implémentation Stratégies
28
Benefit of Clinical Documentation
Appropriate documentation promotes
A high standard of clinical care Improved communication and
dissemination of information betweenand across service providers
An accurate account of treatment, intervention and care planning
Improved goal setting and evaluationof care outcomes
Improved early detection of problemsand changes in health status
Evidence of patient care
29
Challenges in Clinical Documentation
Clinicians’ Adoption - Integrated with consultation
workflow - Balance between Structured and
Free Text - Minimal clicks/ data entry - Auto-retrieved Allergy, Health
Issues, Lab / Rad Results and Medication
- Incorporate CPOE into document - Incorporate CDSS into document - Short and concise printout - Reduce duplicate entry

30
Standardisation and Governance
Same Coding standards for Clinical Decision Support and Analytics
Same Data items for same observations in all documentation to facilitate future analytics
e.g. Smoking History, Pain score etc
Same look & feel across institutions for ease of use, particularly for junior doctors rotating from institution to institution
Challenges in Clinical Documentation

31
Improve Clinician EngagementEMR becomes a common platform for information sharing and real-time reporting, resulting in greater communication and partnership among different clinical teams and improved patient outcomes.
AccountabilityDemonstrates the clinician’s accountability and records their professional practice.
CommunicationThe basis for communication between health professionals about the (a) Care provided, (b) treatment, (c) Care plan, (d) outcome
QualityShould be clear, concise, correct, contemporaneous, complete, collaborate, patient-focused
ConfidentialityMust maintain confidentiality
Lessons Learnt
32
Data Standardization
• Adopt SNOMED-CT for Problem List and Diagnosis
• Problem List and Diagnosis can be set as ‘General’, ‘Chart’ and
‘Visit’.
• SNOMED-CT coded Problem List and Diagnosis facilitates Decision Support.
• SNOMED-CT coded Problem List and Diagnosis assist in Analytics

33
Governance Process
Involve clinicians from all institutions for requirement study so that clinical notes for same specialty are standardised across institutions
Change Control Committee (CCC) comprising of IT representatives from different clinical document teams to review data items for new clinical document
Core Clinical Design Team (CCDT) comprising of clinicians, nurses and IT to review the new clinical document