
Implementation of Thin Layer Agar for Mycobacterium culture in rural Kenya Médecins Sans Frontières.
Upload
katherine-lloydCategory
view
216download
0
Challenges in adapting chronic HIV/TB services to high mobile populations in Southern Africa
Eric Goemaere, MD Médecins Sans Frontières
IAS Washington , July 25th 2011
OWN, SCALE-UP & SUSTAINThe 16th International Conference on AIDS & STIs in Africa
4 to 8 December 2011, Addis Ababawww.icasa2011addis.org

High mobility , high HIV and TB prevalence
• High regional mobility• Different patterns of migration • Mobility = survival• Chronic care designed for
residents• Migrants
– Hardly attending health facility– Fear of deportation, health
system barriers, xenophobia – Access to treatment often
denied due to fears about adherence and continuity of care

Failure to identify migrants at ART initiation triggers a high rate of loss to follow-up
• Multivariate analysis -> AHR for LTFU in migrants at one year 6.69 ( 3.18-14.09)
Trends in loss to follow-up among migrant workers on ART in a community cohort in Lesotho Helen Bygrave1*, and all , Plos One , October 2010 | Volume 5 | Issue 10 | e13198
14 % of migrants amongst ART initiations

Cd4 results collection among migrants testing HIV(+) Central Methodist Church, Johannesburg , 2009-2010
• Central Methodist Church is a shelter for up to 3000 homeless mostly Zimbabwean migrants in central Johannesburg
• MSF opened a clinic in CMC in 2008
• Cd4 testing was initially implemented in a traditional passive way
• After implementing a testing campaign and active case tracing, outcomes where significantly increased

Defining the problem
• HIV/TB care designed for resident population
• Mobility = survival for migrants • Different treatment protocols in
different countries• Medications & documents
frequently stolen or lossed during irregular crossings
• No cross-border information‘s on where and how to access services
• Fear of arrest /deportation• Staff attitude towards migrants• Illegal fees

Establishing mobile HIV/Tb units, Musina border, Limpopo, South Africa
21,000 living on commercial farms along border
Circular seasonal migration
Decentralized MSF/DOH nurse based mobile clinics on farms, offering PHC services but referral for integrated HIV/TB initiation .
SOUTH AFRICA
MUSINA

Initial outcomes : continuum of HIV care in farms
ART eligible380
Pre-treatment
steps
CD4 results given 951 (44%)
CD4 count sample
provided2171
Initiated ART193 51%
95% CI 46%-56%
HIV+ diagnosed population
Testing to etsablish eligibility
ART eligibility to ART initiation

Adapting services to integrated HIV/Tb care
ART and TB treatment initiation offered on the spot in farm
Point of care CD4 Peer education network on
farms (HIV awareness, linkage to care, adherence to ART/TB, defaulter tracing..)

Adapted strategyfor providing HIV/TB care to "migrant" patients
• Each visit, patient asked about travel plan and documented
• Health passports + alternative treatment points

When time to go , issued with a ‘travel pack’
• Temporary Transfer Out (TTFO): = plans to return (circular migration)
• 3 months ARV supply + tail protection
• If not intention to return, self addressed stamped envelope signed by receiving sites

Impact of adapted strategy on continuum of HIV care
ART eligible
380
226Pre-
treatment steps
CD4 results given
951 (44%)
594 (81%)
CD4 count sample
provided2171735
Initiated ART193 ( 51% )
95% CI 46%-56%18883%
95% CI 78%-88%
HIV+ diagnosed population
Testing to etsablish eligibility
ART eligibility to ART initiation
37%
32%
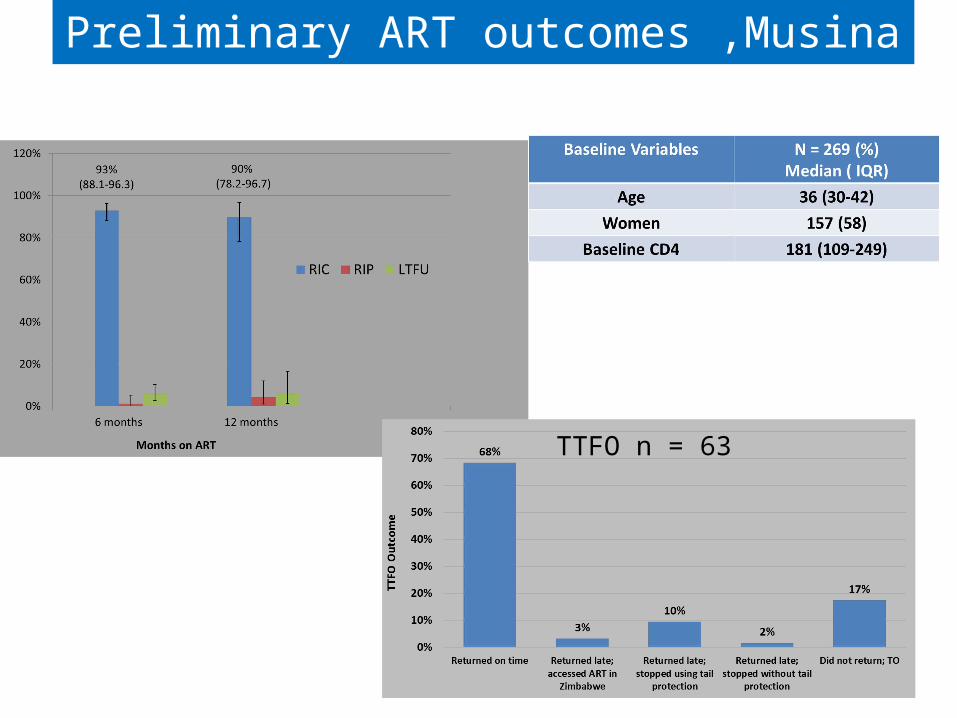
Preliminary ART outcomes ,Musina
TTFO n = 63

Conclusions
• HIV/TB care can be successfully adapted to migrant population pending :• clear regulations in terms of
access to health care for non-nationals , including ART and TB
• Access to be free of charge • Adapting health service to
provide acceptable access • Harmonize ART practices, regimen &
documentation -> Regional ART/TB health passport• Achievements of R9 global fund grant
( 12 M $) with SADC secretariat in Gaborone?

Acknowledgements
• Tambu Matambo , Helen Bygrave, Gilles Van Cutsem
• Mobile MSF/DOH teams in Musina
• Department of Health, Limpopo , South Africa
• People living with HIV in Musina






![Salvadoran refugee ampS in HonduraS 1988...Laurence Binet - Médecins Sans Frontières [January 2005 - November 2013] - “Violence against Kosovar Albanians, NATO’s Intervention](https://static.fdocuments.us/doc/165x107/60ab811016d6a05be04000c4/salvadoran-refugee-amps-in-honduras-1988-laurence-binet-mdecins-sans-frontires.jpg)











