
Challenges and Frustrations in the Management of Malignant Glioma Edward R Laws and Colleagues...
56
Successes and Frustrations in the Management of Malignant Gliomas Edward R. Laws and colleagues Brigham & Women’s Hospital
-
Upload
brett-leonard -
Category
Documents
-
view
216 -
download
0
Transcript of Challenges and Frustrations in the Management of Malignant Glioma Edward R Laws and Colleagues...
Successes and Frustrations in the Management of Malignant Gliomas
Edward R. Laws and colleaguesBrigham & Women’s Hospital
Gliomas of the Brain
• 70% of Primary Brain Tumors
• Mean Age at Diagnosis is 55
• 60-70% are Malignant (Glioblastoma)
The Glioma Outcomes Project
Rationale for a Glioma Outcomes Study
• Most Retrospective Studies Show Survival Advantage for Resection when Compared to Biopsy + Adjunctive Therapy
• Very Few Adequate Prospective Studies Exist
• Contemporary Data From An Observational Study Can Provide An Estimate of Survival Differences
Types of Primary Brain Tumors Studied
• Glioblastoma
multiforme
• Anaplastic
oligodendroglioma
• Mixed anaplastic
oligo/astrocytoma
• Anaplastic gliomas (Grade III or IV)
Patient Data
• 788 Malignant Glioma Patients Accrued 1997 - 2000
• 639 Followed At Least 15 Months or Until Death
• 446 With Complete Data
Differences Between Biopsy andResection Cohorts
Age - Biopsy Group Older
Pathology - Resection Group More GBM
KPS - Biopsy Group More KPS <70
Location - All Multifocal (27), More Bilat in Biopsy Group
Size - Larger in Resection Group
Arguments for Radical Resection
CYTOREDUCTION
Decrease the Tumor Burden
Pathologic Diagnosis More Secure
• Sampling Error Reduced
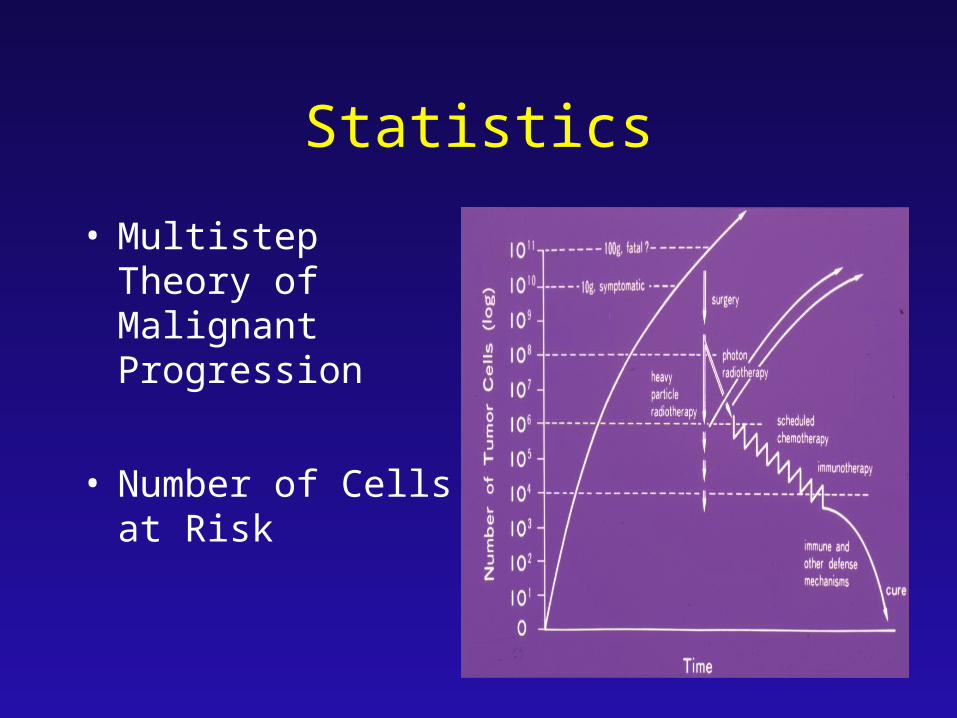
Statistics
• Multistep Theory of Malignant Progression
• Number of Cells at Risk
Intracranial Pressure is Relieved
Neurologic Deficits are Reversed
Seizures are Eliminated

The Late Effects of Radiation Therapy
Cognitive, Emotional
Demyelination, Necrosis
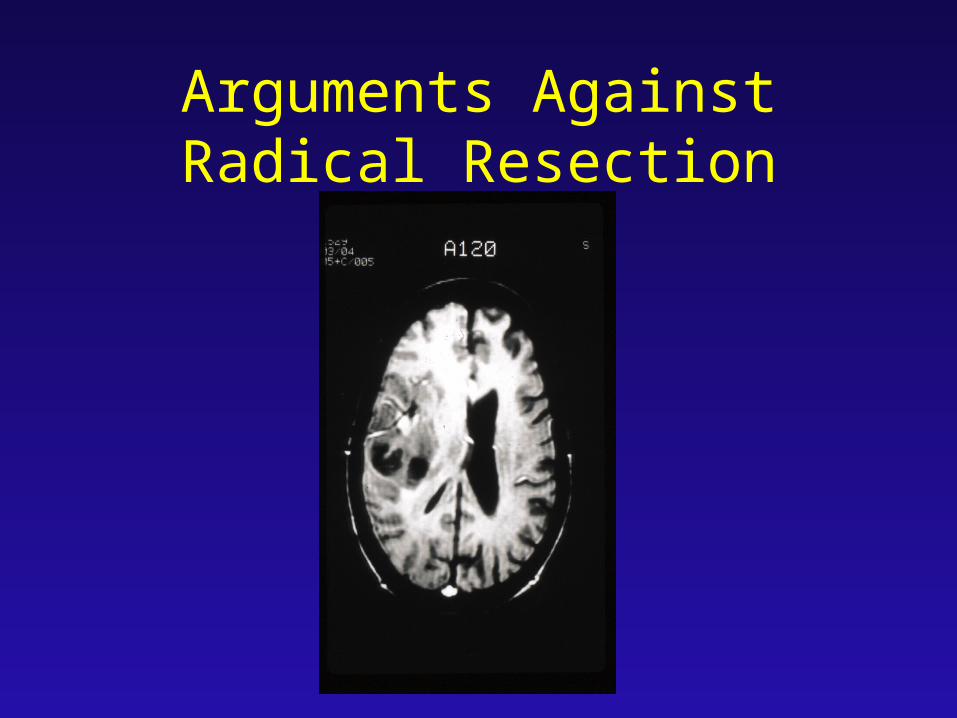
Arguments Against Radical Resection

Inherent Invasiveness of Most Gliomas
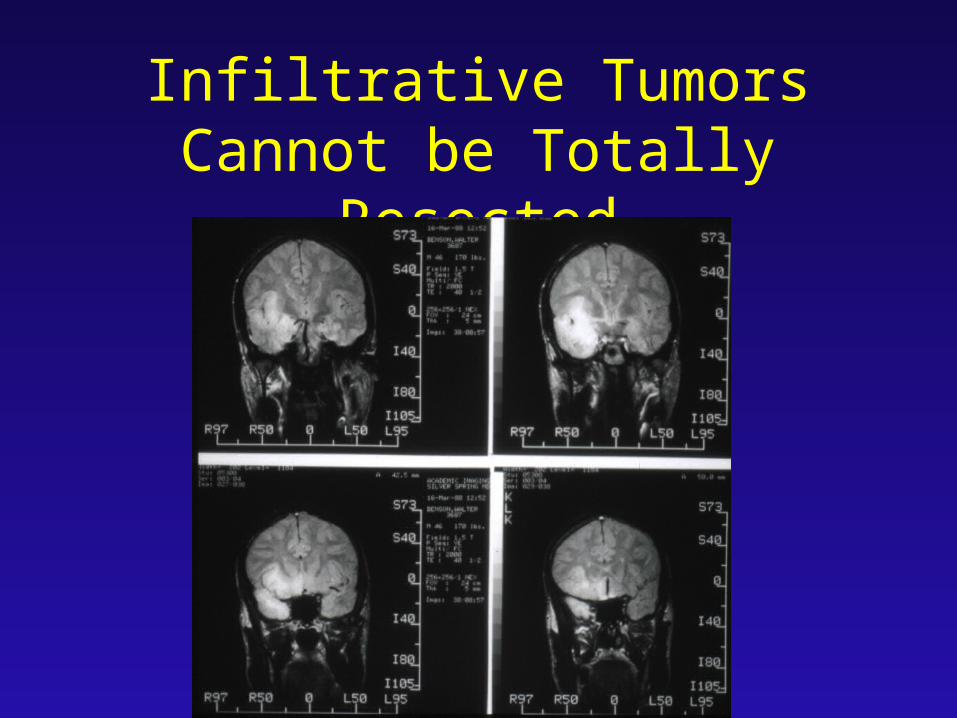
Infiltrative Tumors Cannot be Totally Resected
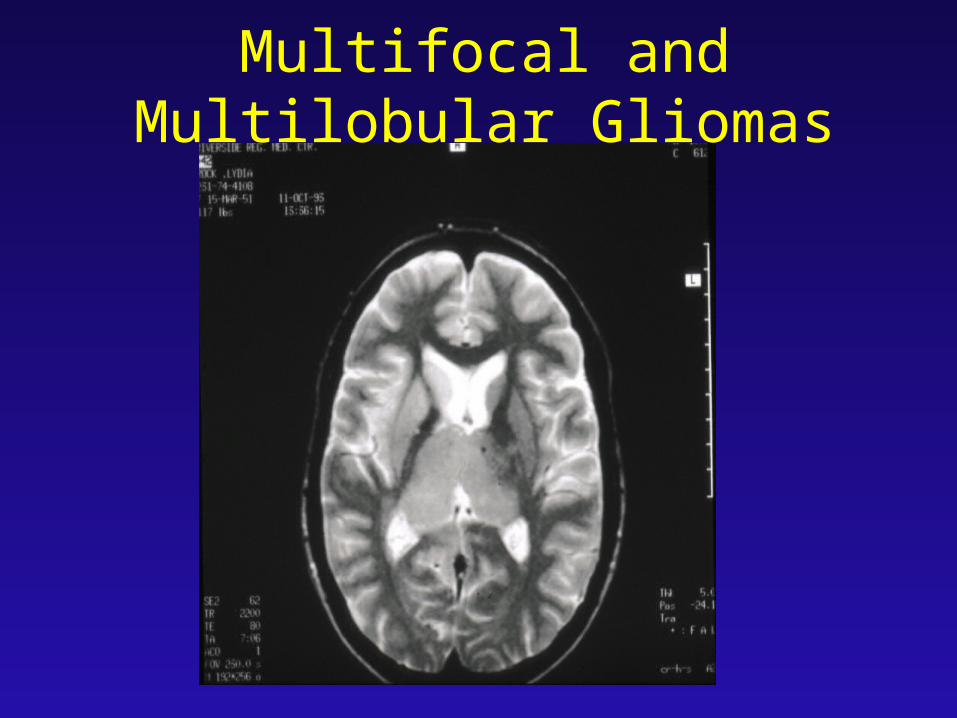
Multifocal and Multilobular Gliomas
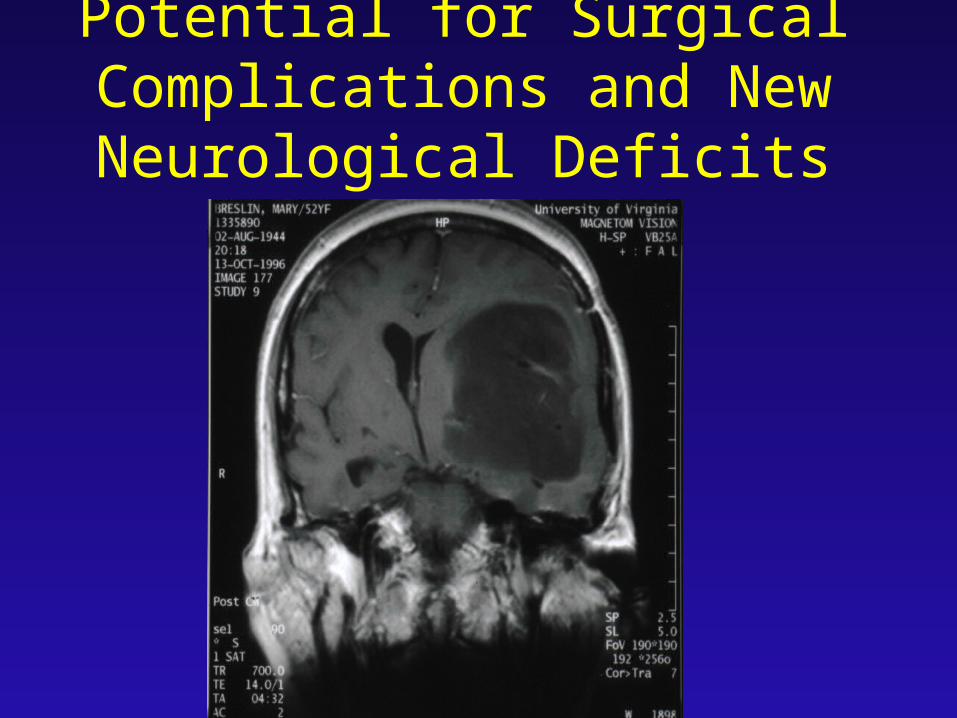
Potential for Surgical Complications and New
Neurological Deficits
Pathology - 446 Patients
GBMF (73%)
Grade III Gliomas (27%)
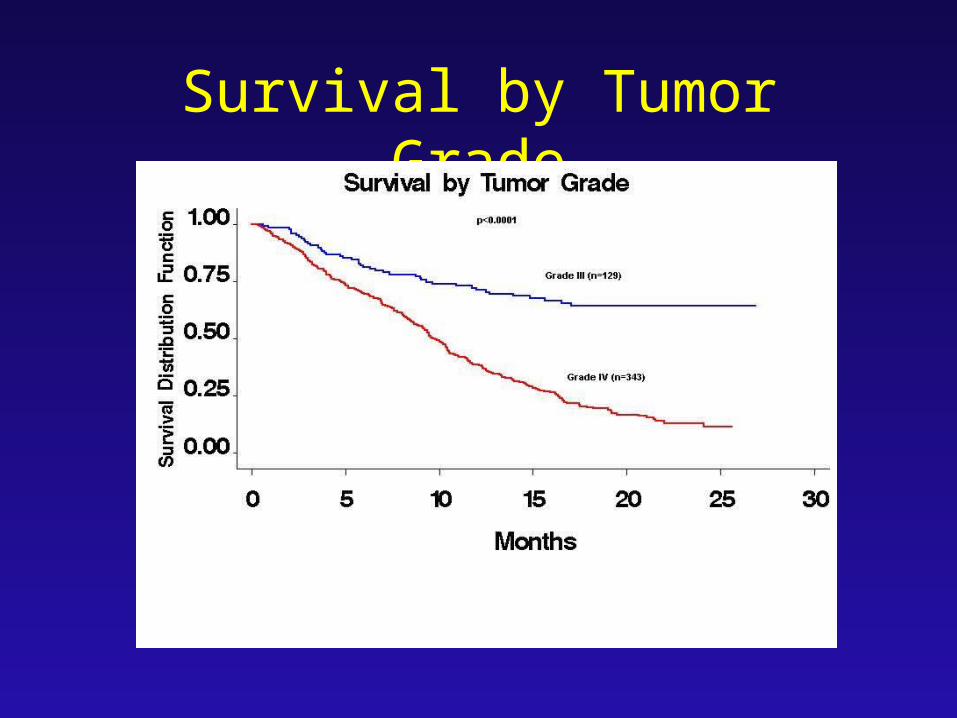
Survival by Tumor Grade
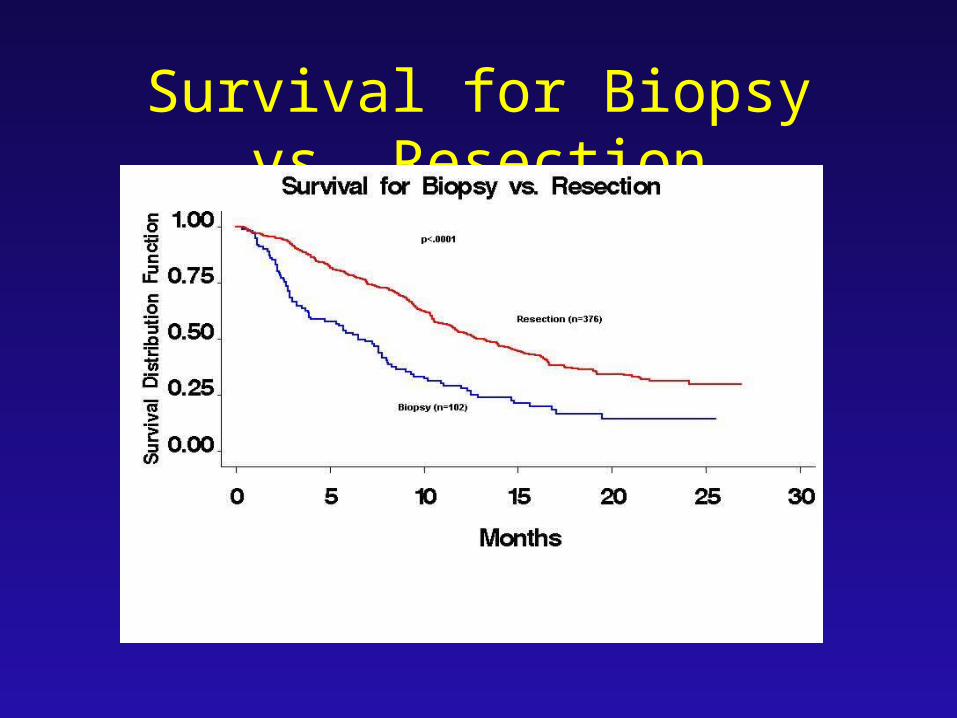
Survival for Biopsy vs. Resection

Favorable Prognostic Factors
Age 20 - 40
Karnofsky Rating 70
Resection
Unfavorable Prognostic Factors
Age 60
Multifocal Tumor
Karnofsky Rating < 70
Biopsy Only
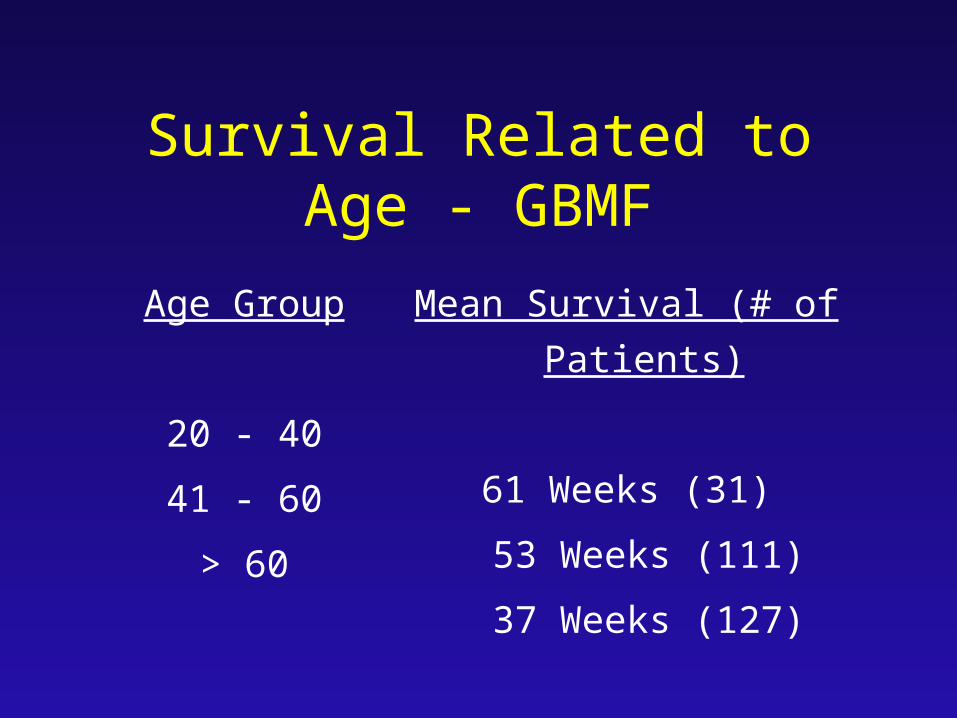
Age Group
20 - 40
41 - 60
> 60
Mean Survival (# of Patients)
61 Weeks (31)
53 Weeks (111)
37 Weeks (127)
Survival Related to Age - GBMF
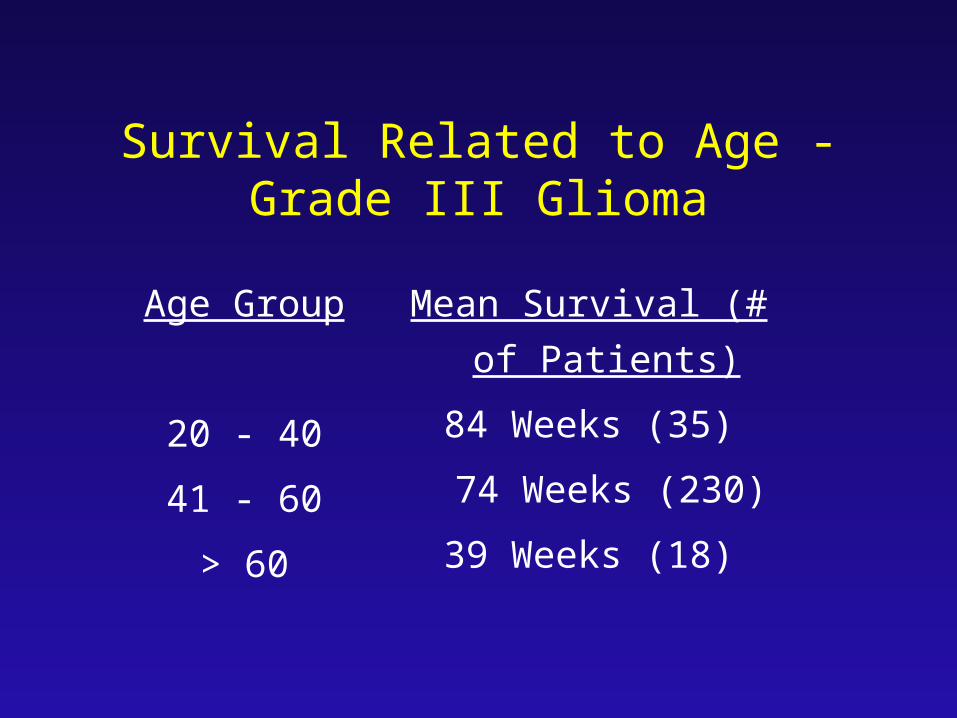
Age Group
20 - 40
41 - 60
> 60
Mean Survival (# of
Patients)
84 Weeks (35)
74 Weeks (230)
39 Weeks (18)
Survival Related to Age - Grade III Glioma
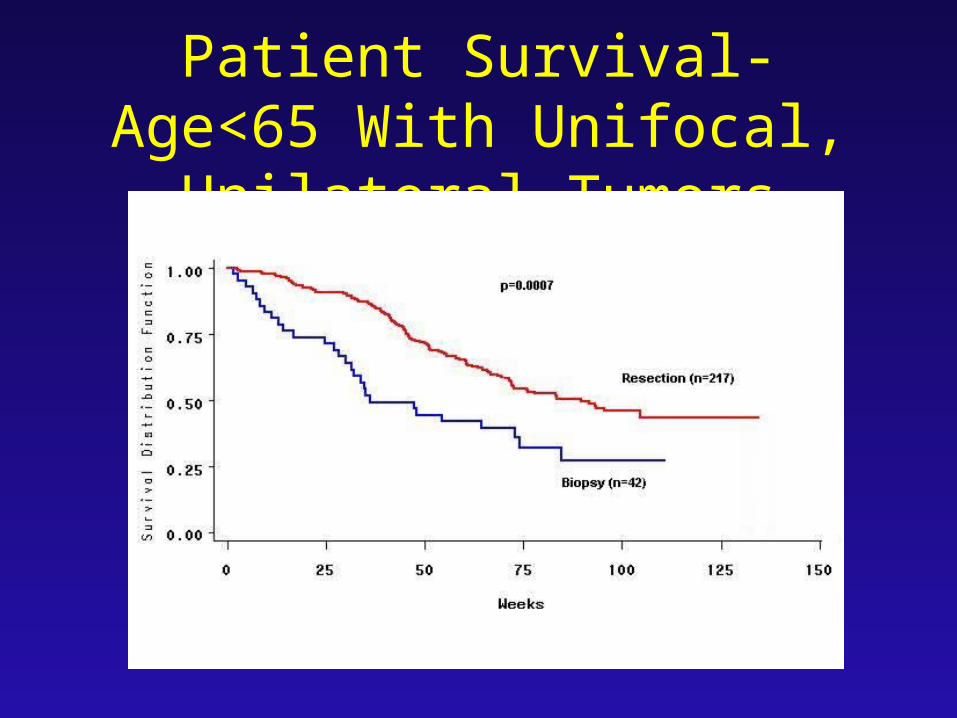
Patient Survival-Age<65 With Unifocal, Unilateral Tumors
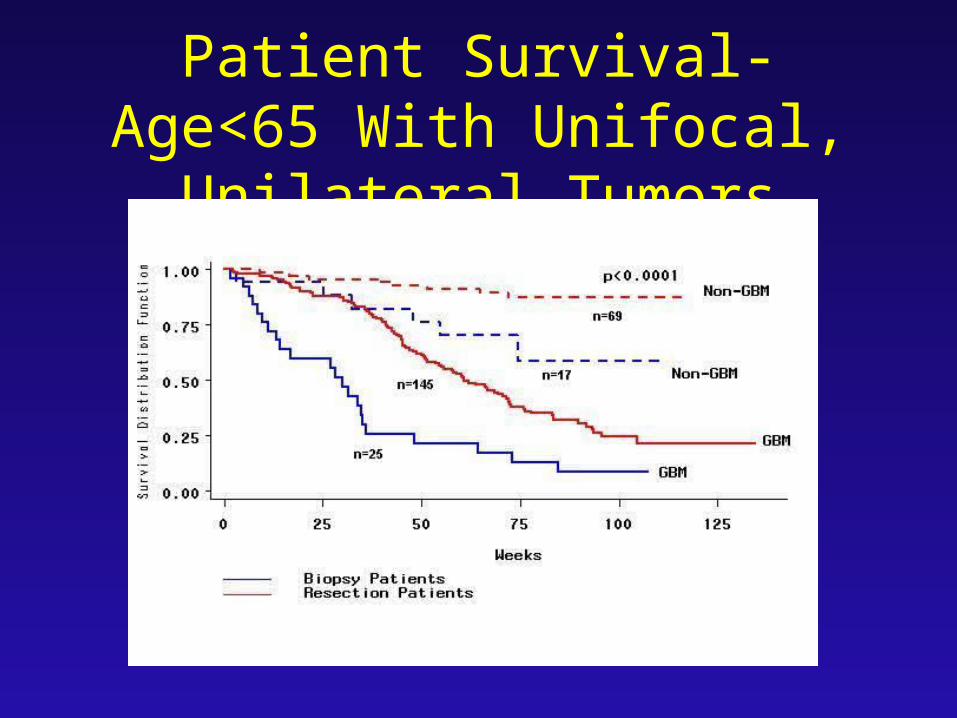
Patient Survival-Age<65 With Unifocal, Unilateral Tumors
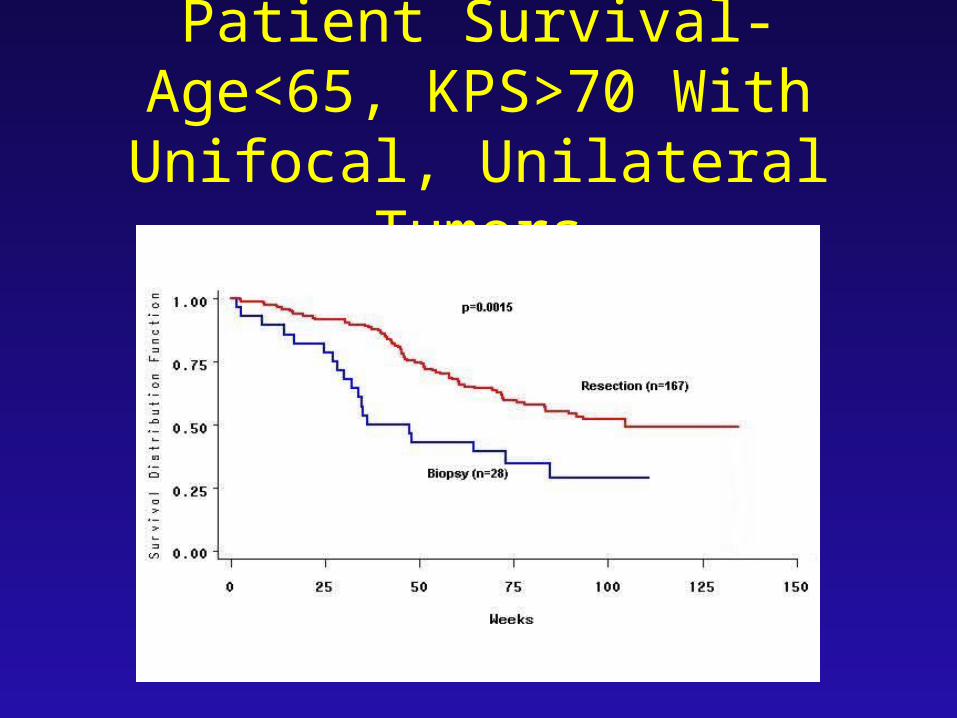
Patient Survival-Age<65, KPS>70 With Unifocal,
Unilateral Tumors
Survival is Improved with Radical Resection
Methods for Improving Radical Resection
• Functional MRI
• Electrophysiological Monitoring
• Image Guided Surgery and Intraoperative Ultrasound Imaging
• Intraoperative MRI
• Metabolic Imaging
• Awake Surgery
Survival for Patients with Malignant Gliomas
Little Changed in 40 years –
Except Perhaps for Quality of Life
The Enemy
Problems in Glioma Treatment
• Invasion and multifocality – local therapy will never be curative
• Impact of radiotherapy and chemotherapy on quality of life
• Cerebral edema and other reactions to tumor cell death
• Analysis of resected tumor may be misleading
What do we Believe?
• They start monoclonal, but rapidly develop polyclonal instability
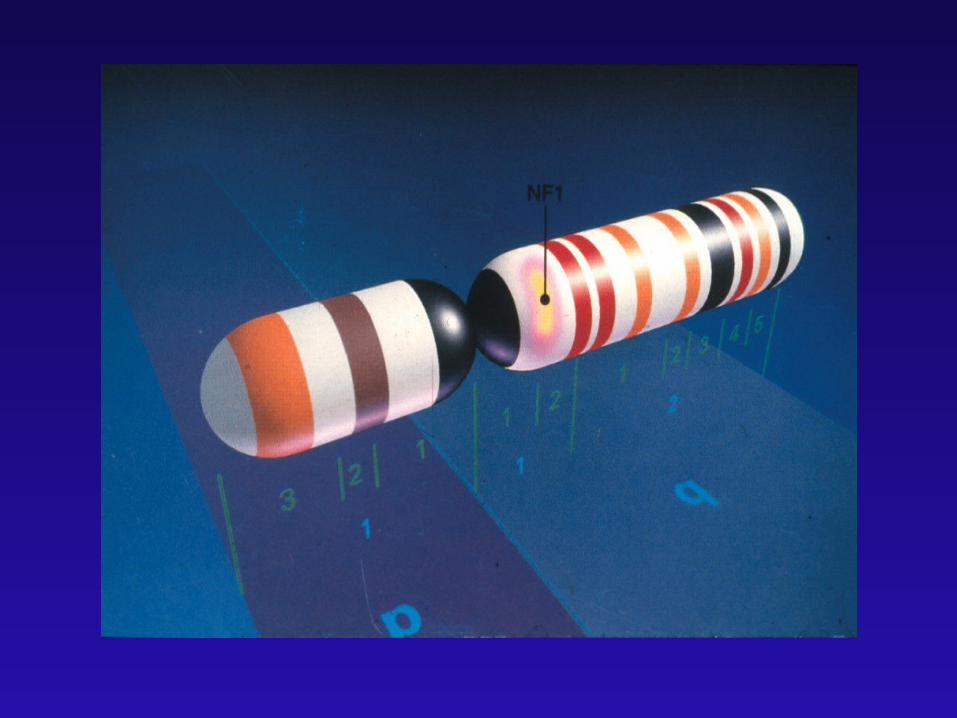
• A sequence of molecular genetic events results in malignancy
• Activation of oncogenes and deletion of suppressor genes play a role in pathogenesis
• Some are malignant de novo; some progress from more benign lesions
More Concepts
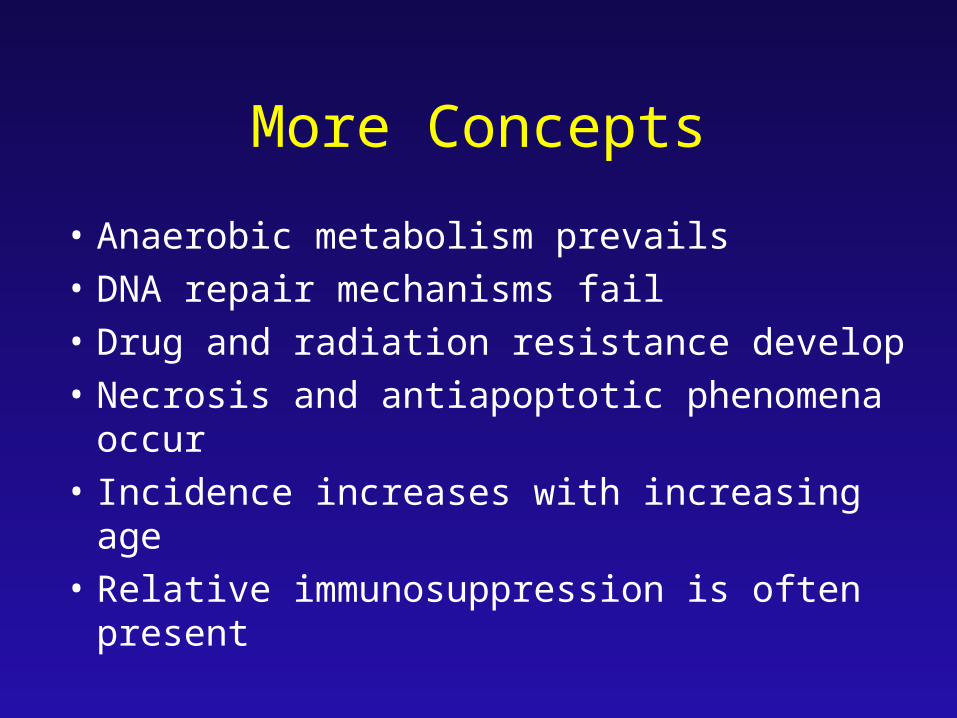
• Anaerobic metabolism prevails
• DNA repair mechanisms fail
• Drug and radiation resistance develop
• Necrosis and antiapoptotic phenomena occur
• Incidence increases with increasing age
• Relative immunosuppression is often present
More Concepts
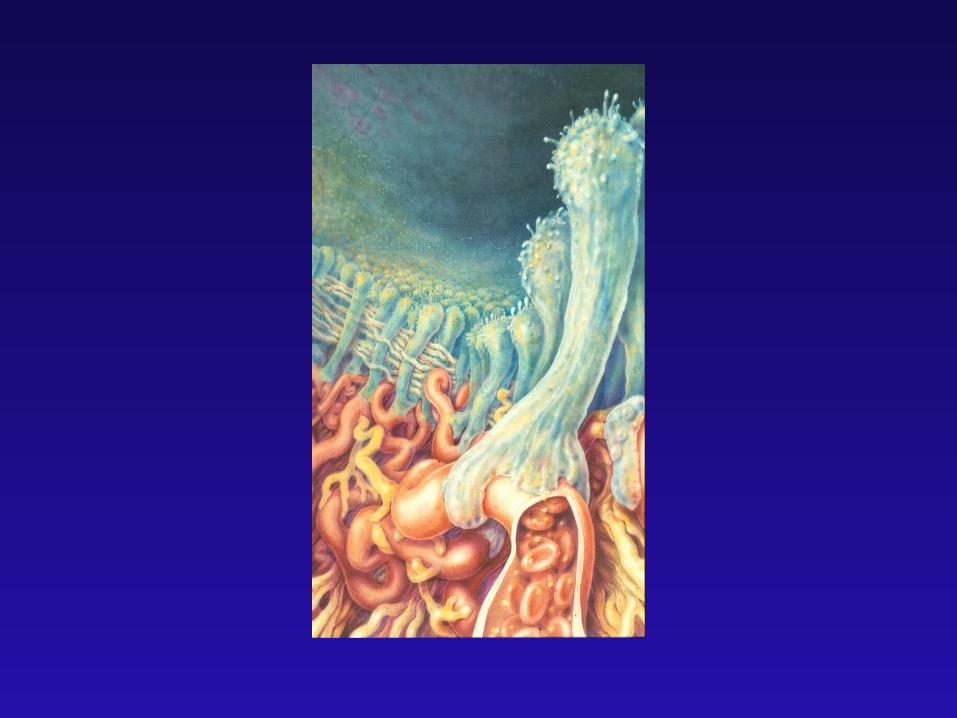
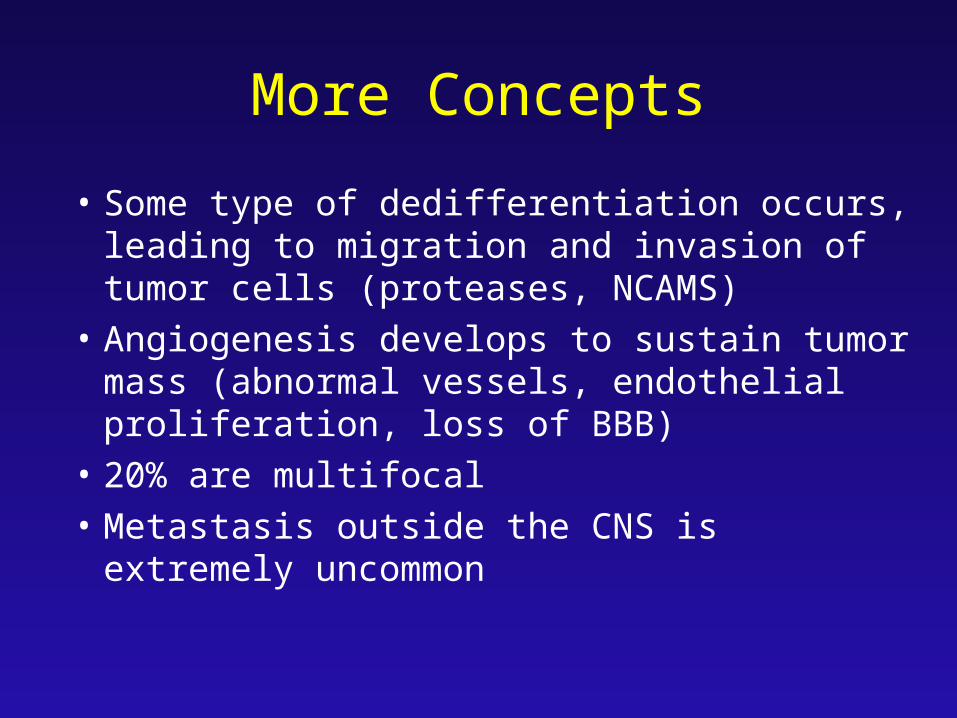
• Some type of dedifferentiation occurs, leading to migration and invasion of tumor cells (proteases, NCAMS)
• Angiogenesis develops to sustain tumor mass (abnormal vessels, endothelial proliferation, loss of BBB)
• 20% are multifocal
• Metastasis outside the CNS is extremely uncommon


Problems in Brain Tumor Therapy
• Polyclonal heterogeneity
• Tumor cell resistance
• Tumor cell metabolism
• Tumor cell invasion and migration
• Tumor oxygenation
Problems in Brain Tumor Therapy
• Characteristics shared with normal brain
• Tumor-brain interface phenomena
• Blood- brain barrier phenomena
• Delivery of toxic agents
• Tumor Stem Cells may Produce Tumors
Unique Characteristics of Tumor
• Growth kinetics• Vascular supply• Glycloytic metabolism• Tumor cell invasion
• Oxygenation• pH• Blood-brain barrier• Peritumoral invasion
Targets for Tumor Cell Destruction
• Cell surface/nuclear receptors
• Cell membrane/nuclear/mitochondrial membranes
• Mitochondria-energy production
• Cytoskeleton
• Protein synthesis – cytoplasm/nucleus
• Signal transduction processes
Mechanisms of Tumor Cell Destruction
• Free radicals – oxygen, peroxide, hydroxyl
• Direct ionizing reactions
• Alkylation/carbamylation of bases
• Inhibition of enzyme action
• Alterations of nucleic acid structure & function
• Angiogenesis inhibition
• Immunotherapy
Malignant Gliomas – What is Effective
• Surgical Resection
• Conventional Fractionated Radiotherapy
• Nitrosoureas (marginally)
• Temazolamide – in some (MGMT methylation)
Malignant Gliomas – What is Ineffective (So Far)
• Hyperfractionation, Hypofractionation, Radiation Sensitizers, Oxygenation
• Brachytherapy, Radiosurgery, BNCT• Photoradiation, Hyperthermia• Gene Therapy• Monoclonal Antibodies, Immunotherapy• Angiogenesis Inhibitors, Protease Inhibitors, Signal
Transduction Blockers, Cytokines• Hormone, Steroid, Vitamin Based Therapy
Other Ineffective Therapies
• In vitro chemotherapy testing• Differentiation therapy• Stem Cells• Chemotherapy ( iv,intrarterial,intrathecal, BBBD, Polymer, Convection, BM rescue)
Why Have We Failed
• Wrong treatment strategies – focal therapies for a diffuse disease
• Wrong tissue studied – resected tissue may not represent what is left behind
• Poor or misleading models
• Inadequate understanding of developmental neurobiology

Proposal for Management
• Maximally resect
• Analyze tumor margin to guide therapy
• Inhibit invasion/migration
• Use radiotherapy judiciously
• Consider immunotherapy and vaccination strategies
For Incomplete Resection
• Maximize quality of life and cognitive function
• Judicious radiotherapy – Focal +
• Antiangiogenesis agents
• Antimetabolites
The Enemy
Peter Bent Brigham Hospital


















