Cervical Pain Syndrome...

of 4
Transcript of Cervical Pain Syndrome...
-
8/3/2019 Cervical Pain Syndrome...
1/4
Cervical Pain Syndrome as Consequence of Computer Use in Daily Practice
vol 16 no 1 MARCH 2008 25ORIGINAL PAPER
Cervical Pain Syndrome as
Consequence of ComputerUse in Daily Practice
Mediha Karic-Skrijelj, Adnana Talic, Izet Masic, Narcisa Vavra-Hadziahmetovic,Haris Pandza, Enra Suljic-Mehmedika
Medical Faculty, Univeristy of Sarajevo
rematoid medication (NsAID) oldbe taken in ame time interval; d) Diaze-
pam, 3-7 day can be ed in patient witevere pam; e) minotriptiline or gabap-entin can be efl in cae of cronic cer-vical yndrome.
Pyical and manal treatmentcan be: a) pyical terapy can ait toacieve early mobilization and retrn todaily activitie; b) active pyical terapy ,mobilization, maniplation and exerciecan are ort time relief of neck pain;c) ome baed exercie, a own by tireearc, can ignificantly prolong te
pain free period, in cae of patient witte cronic yndrome; d) Medication,combined wit te exercie program andergonomic improvement can be effec-tive oltion for te cronic or recrrentneck pain. Intenive treatment in Neckpain yndrome are: a) srgical and oterintenive treatment (rarely indicated); b)invaive treatment inclde and percta-neo radiofreqent nerotomy and cer-vical epidral analgei.
Te perpective are te following: In
general, evidence degree for a neck paini qite low. Determination of gidelinefor better ytematization of terapy iimportant prereqiite for te ftre ef-ficacy reearce of vario concept.Ti problem deerve more attention byreearce, in order to determine reali-tic prevention trategy, improve qalityof life and work, and for te rational eof te ealt foced financial reorc-e. speaking abot ti reearc, we areplanning to repeat it on te larger ample,in order to increae reliability of te re-
earc relt.
GOALS2.
Te goal of te reearc were: a)to identify poible erio and pecificcae of neck pain; b) to identify pyco-logical and ocial barrier for recovery; c)to determine te degree of dyfnctioncaed by nonpecific neck pain; d) re-dce pain; e) improve fnctioning and re-dce diablement; f) prevent recrrenceand development of cronic form.
METHODS3.
A a ample for ti reearc we e-lected patient wit te verified neck pain
SUMMARYNeck pain syndrome is described as: Pain in the neck affects at least once in a lifetime everysecond person, and also 10 % of adult population suffers from chronic pain in this area. It ismore often among women. A constant increase of incidence in the industrialized countriesis noticed. It is also the leading cause of referral to physical rehabilitation. It is causing hugefinancial costs in the health care system.There is no consensus regarding Neck pain syndromemanagement, but many therapeutic modalities are applied: a) to isolate (or manage) rare, butpotentially dangerous states that can cause neck pain; b) identify and treat each co morbidstate and risk factors; c) provide resources and informations, especially about regarding usecomputers in dayly practice. Physical and manual treatments can be: a) physical therapy canassist to achieve early mobilization and return to daily activities; b) active physical therapy ,mobilization, manipulation and exercises can assure short time relief of neck pain; c) homebased exercises, as shown by this research, can significantly prolong the pain free period,in case of patients with the chronic syndrome; d) Medications, combined with the exerciseprogram and ergonomic improvements can be effective solution for the chronic or recurrentneck pain. Intensive treatments in Neck pain syndrome are: a) Surgical and other intensivetreatment (rarely indicated); b) invasive treatments includes and percutaneous radiofrequent
neurotomy and cervical epidural analgesis.Key words: Cervical pain syndrome, computers.
INTRODUCTION1.
Neck pain yndrome i decribed a: Pain in te neck af-fect at leat once in a lifetime every econd peron, and alo10 % of adlt poplation ffer from cronic pain in tiarea. It i more often among women. A contant increae of in-cidence in te indtrialized contrie i noticed. It i alo teleading cae of referral to pyical reabilitation. It i ca-ing ge financial cot in te ealt care ytem.
Dring period from 2005 to 2007 we realized or reearcin Center for pyical terapy and reabilitation stari Grad
sarajevo wit aim to examined coneqence of ing com-pter a giving Pain Neck syndrome Cervical syndrome.
Te otcome wa meared by te following variable: a)pain (e.g. meared on vial-analoge cale); b) diablement(e.g. meared by Neck Diability Index, or Nortwick PainQetionnaire); c) day on ick leave; d) e of medication; e)e of ealt care ervice; f) rate of radiology imagining (1,2).
Tere i no conen regarding Neck pain yndromemanagement, bt many terapetic modalitie are applied: a)to iolate (or manage) rare, bt potentially dangero tatetat can cae neck pain; b) identify and treat eac co morbidtate and rik factor; c) provide reorce and information,
Medication terapy i applied a: a) wit analgeic (wicacieve ort term relief from pain); b) tey are precribed ac-cording to te pain intenity, peronal reference, and pre-ence or lack of ide effect; c) Paracetamol or nonteroid anti
O R I G I N A L P A P E R
25-28
-
8/3/2019 Cervical Pain Syndrome...
2/4
26 vol 16 no 1 MARCH 2008
Cervical Pain Syndrome as Consequence of Computer Use in Daily Practice
ORIGINAL PAPER
yndrome, 120 of tem in total wic we dividedinto two grop wit 60 patient. One grop i treat-
ed wit te claic reabilitation metod and teoter coort nderwent active exercie dring a ixmont period. For teting we ed WAD cale andNDI qetionnaire, wic are approved all arondte world and decribed in available literatre.
RESULTS4.
According to te protocol, at te Center for
pyical reabilitation Old Town in sarajevo, neckpain yndrome (Cervical pain yndrome) wa teleading reaon for te otpatient treatment. In tetime period from Janary 3rd ntil December 31t2006 tere wa a total of 6163 pecialit evalation,firt or control one.
Dring te ame time period pyical reabili-
tation tarted 516 patient wit te neck pan yn-drome from wic: 426 women (82.3%) and 90 men(17.7 %).
Obvioly tere are more female patient witte neck pain, wic i in accordance wit te re-lt of te epidemiology tdie condcted in Eu,
usA and Canada.Freqency of dieae compared to te nmber
and patient gender wit te neck pain yndromewic ad pyical terapy in 2006 preented inte table 1.
Frtermore, in majority of patient axial neckpain wa diagnoed or not complicated neck painyndrome (G 54.2), bt for te patient in Center forpyical reabilitation mc more freqent i cervi-cal bracial compared to te reference data.
In baeline, demograpic and clinical data forte 120 repondent did not ave ignificant tati-tical deviation (table 2). Average patient age i 47year, wit very low variation coefficient. Variation
coefficient; V(A)= 13 % (very low) V(B)= 13% (verylow). Alo witin baeline, te pain (VAs) and elfetimated fnctionality impairment (NDI), wa aloimilar for bot grop. All repondent N = 120
Diagnosis Female Male Total 516
Cervical syndrome 291 51 342 (66.27 %)
Cervical brachialgia 96 25 121 (23.44 %)
Vertebrobasilar sy. 21 9 30 (5.81 %)Cervical cephalic 18 5 23 (4.45 %)
States after surgery C5-C6 1 0 1 (0.19 %)
Table 1.Diagnosis, number of patients on physicalrehabilitation during 2006; cervical syndrome. Source:Protocol of the Center for physical rehabilitation OldTown (CBR) Sarajevo; for 2006.
Gender, femaleA Training group
n=60B Control group
n=60
Mean age SD, 47 ( 7) 46,85 (6)
Profession, clerk, n, 60 60
Computers use, n,%, 54 (90 %) 51 (85%)
Symptoms duration in years 5 (4) 4 (5 )
Hand shake normal, n, 60 60
Tobacco smoking, n, %. 12 (20) 10 (17)
Table 2.Basic demographic and clinical data
Evaluation of clinical stateTraining group n
= 60f A %
Control group n= 60
f B %
5 Without problems - cured 6 10 0 0
4 Significantly improved 36 60 9 15%
3 Without significant change 12 20 36 60%
2 minimal change 6 10 12 12%
1 Worsened condition 0 0 3 0.5%
60 100% 60 100%
Table 3. Scores distribution of the patients clinical stateafter 6 months of research. For the statist ical analysis ofthe results used methods are Chi-square test. X2 =34.92,
p=9.57-08. p
-
8/3/2019 Cervical Pain Syndrome...
3/4
Cervical Pain Syndrome as Consequence of Computer Use in Daily Practice
vol 16 no 1 MARCH 2008 27ORIGINAL PAPER
ad te initial evalation of fnctioning tat 3(moderate problem wic redce qality of workand performance).After ix mont reevalation, re-lt of clinical tate evalation wa a preented intable 3. All te repondent are women, becaete male patient did not flfill te reearc crite-ria. All te patient were clerk itting profeion, 85-90 % ofrepondent e compter dr-ing working or (ometime allday). up to 20% of patient mokecigarette.
After final reevalation, tereearc relt are preented intable 3.
At te rik level le tan1% we can conclde tat after 6mont reevalation tere are
ignificant difference in clinicaltate level of te patient fromte training (A) and te controlgrop (B). If we analyze te rela-tionip between freqencie inte table, we can conclde tatte patient bt not all, wicexercied in teir ome, avebetter fnctional tat and re-dced pain, and 10% of tem didnot ave any problem.
Bt, alo 15% of patient tat
did not exercie witin ome pro-gram ave improvement in clini-cal tat, wic can be explainedwit te al, pontaneo re-
miion of te neck pain yn-drome. In ti grop of patienttere wa 0.5% of deterioration,wile in cae of patient tat ex-ercied we did not notice woren-ing of te clinical tate.
One of te indexe wic in-
dicate level of acieved treatmentqality can be preented a tedivider of te percent wit amecore in te training and controlgrop. We cooe to preent in-dex of qality baed on compar-ing te index for te core 5 and4. After 6 mont reevalation,percent of core 5 at te traininggrop wa 10% and 0 % for tecontrol. In ti manner te cal-clated index for te firt grop
i 10: 5=2, and for te econd one0:5=0. score 4 ad 60% of pa-tient tat exercied witin omeprogram, and te 15% of patienttat did not exercie. Qality in-dex i Qk = 60 : 4 = 15 and Qk 15: 4 = 3.75.
According to probability law, index of qalitycan be ed to get a general inigt in te advan-tage of one over oter treatment metod, wic intaking of general doctrine attitde ave extremeimportance.
Figure 1.Achieve the control of the body posture by adjusting the chair,desk and the computer to assure adequate position for the spine. 1. Adjustthe monitor directly in front of you so the head does not move and standstraight. 2. Never hold the phone between the head and the shoulder,use hands or phone holder. 3. Use the chair with arm rests to support the
forearms, with relaxed shoulders. 4, 5. Adjust the height of the chair so youcan keep your feet on the floor. 6. Keep your back aligned to the chair.
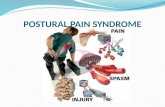
Figure 2.PROPER AND IMPROPER POSTURE
Spine keep the natural curve, loin support
armS keep close to the body, elbow angle 70-90
WriST forearm and hand should be straight
moniTor - at the eyes height (0-30 degrees)
-
8/3/2019 Cervical Pain Syndrome...
4/4
28 vol 16 no 1 MARCH 2008
Cervical Pain Syndrome as Consequence of Computer Use in Daily Practice
ORIGINAL PAPER
DISCUSSION5.
According to te relt of te condcted re-earc, contino and long lating exercied totrengten te neck mcled wit te ome exer-cie program are efficient in te treatment of pa-tient ffering from neck pain yndrome.
Ten percent of te patient tat exercied did
not feel te bjective problem, wic 60% of temad ignificant redction of pain, redction in eof analgeic and anti rematic medication, witimprovement in local and general fnctioning ta-t a well a daily activitie in life and work, andtat i tatitically igly ignificant advantagecompared to te patient tat did not exercie.
If we know tat te neck pain yndrome in ma-jority of developed contrie, and even in develop-ing contrie i te leading cae for referral to tefamily doctor and pyical medicine pecialit, andaccording to te date of official tatitic for Bonia
and herzegovina, one of te mot often illne inte general practice for 2004. Illnee of te bone-mcle ytem are at te tird place wit 518 caeon 10000 inabitant, and tat in total cot of ealtytem alo take ig place, tat ti i alarmingmoment to foc reearc on ti problem.
Work in te department of pyical and familymedicine, organized at te local commnity level,provide good bai for te cientific reearc andpoibility to implement prevention program, witneceary interdiciplinary and cooperation be-tween team.
Cervical part of pine i expoed to permanentmovement and different mecanical inflence, o itrater early i affected wit te law of aging. higmorbidity rate for te locomotion apparat diea-e, according to te opinion of many cientit, icaed by te today life circmtance witot f-
ficient motion. Becae of tat it i logical tat ad-eqate exercie can ave more tan one benefit. Oneof te mot common cae for ti i everyday eof compter, epecially inadeqate itting poitionin front of te compter dek and moe e.
speaking of neck pain yndrome, it wold begod, trog te activity of te pyiatry ection, to
etabli gide for keeping record of te patientwit ti cae, in order to make comparative doc-mented bai wic i important prereqiite for tereearc in area of pyical terapy and reabilita-tion, and wit tat alo make eaier preentation ofte excellent relt acieved in ti area.
CONCLUSION6.
Te perpective are te following: In general,evidence degree for a neck pain i qite low. Deter-mination of gideline for better ytematizationof terapy i important prereqiite for te ftre
efficacy reearce of vario concept. Ti prob-lem deerve more attention by reearce, in orderto determine realitic prevention trategy, improveqality of life and work, and for te rational e ofte ealt foced financial reorce. speakingabot ti reearc, we are planning to repeat it onte larger ample, in order to increae reliability ofte reearc relt.
REFERENCES
Karic-Skrijelj M. Ocjena efikasnosti aktivnih vjebi1.vrata kod ervikalnog bolnog indroma. Magitarki
rad. Medicinki fakltet univeriteta sarajev. sa-
rajevo, 2008.
Kari-krijelj M, Mai I, Paali A, Vavra-2.Hadiahmetovi N. Efikasnost aktivnih vjebi kodpacijenata a indromom bolnog vrata. Mat soc Med,
2007; 19(4): 219.26.
Corresponding author: Mediha Karic-Skrijelj, MD. Sarajevo,Nursing school, Sarajevo.