CERVICAL CANCER SCREENING PROGRAM OF BANGLADESH ...
45
1 CERVICAL CANCER SCREENING PROGRAM OF BANGLADESH: EVALUATION & FORMULATION OF QUALITY ASSURANCE STANDARDS & GUIDELINES Dr. Partha Basu Head, Department of Gynecologic Oncology & In Charge, Preventive Oncology program, Chittaranjan National Cancer Institute, India Dr. Murtaza Majid Advisor, Public Health & Quality Assurance, Human Development Research Center, Bangladesh. Study Sponsored by United Nations Population Fund (UNFPA), Bangladesh June 2008
Transcript of CERVICAL CANCER SCREENING PROGRAM OF BANGLADESH ...

1
CERVICAL CANCER SCREENING PROGRAM OF BANGLADESH:
EVALUATION & FORMULATION OF QUALITY ASSURANCE
STANDARDS & GUIDELINES
Dr. Partha Basu
Head, Department of Gynecologic Oncology & In Charge, Preventive
Oncology program, Chittaranjan National Cancer Institute, India
Dr. Murtaza Majid
Advisor, Public Health & Quality Assurance, Human Development
Research Center, Bangladesh.
Study Sponsored by United Nations Population Fund (UNFPA), Bangladesh
June 2008

2
LIST OF CONTENTS
Executive Summary 3
Introduction 6
Objectives 7
Organization of the Cervical Screening Program 8
Principles of Monitoring & Evaluation 10
Methodology Followed for Evaluation 11
Evaluation of the Screening Facilities 12
Evaluation of the Colposcopy Referral Centers 16
Evaluation of Management of Cervical Precancers & Follow Up 18
Recommendations for Internal Monitoring & Quality assurance 20
Quality Standards for Screening
Ensuring Quality Standards for Screening
Quality Standards for Colposcopy & Treatment
Ensuring Quality Standards for Colposcopy & Treatment
Quality Standards for Histology
Ensuring Quality Standards for Histology
Stakeholders & Program Managers 24
Evaluation of Training Program 26
Evaluation of ‘Manual of Screening program – Standards & Guidelines’ 28
Evaluation of IEC Activities 30
Recommendations for IEC Program
Client Satisfaction Survey 32
Conclusions 34
Appendix 1: Screening centers: Reporting & Quality Assurance Form 35
Appendix 2: Colposcopy centers: Reporting & Quality Assurance Form 36
Appendix 3: Check list for consumables and equipment required 37
Appendix 4: Questionnaire for Client Satisfaction Survey 40
Appendix 5: Screening Program Evaluation: Data Collection Form 42
Appendix 6: Compilation format for QA Indicators 44
3
EXECUTIVE SUMMARY
This report is the outcome of an external quality assurance exercise for the cervical
cancer screening program of Bangladesh that is being implemented in phases since 2004.
The specific objectives were to:
• Define the measurable indicators to assess the performance of the program in
achieving the stated targets and goals
• Identify the strengths and weaknesses of the ongoing program and develop a
framework that would help to report and resolve problems at the earliest
• Develop a strategy for continuous improvement in all aspects of service delivery
Consultants who are not directly involved in the strategic planning or implementation of
the program were engaged to review the ongoing activities. They visited different service
delivery setups, collected data using a structured proforma, directly interviewed the
service providers and held discussions with the program managers and health officials
over a period of 10 days. A client-satisfaction survey was also initiated among the
women undergoing VIA test in different clinics.
The review observed that the program at present is based on largely opportunistic
screening with good central coordination and some elements of organized screening.
Broad based public awareness campaign is required to increase the uptake of the program
and improve the spontaneous participation rate. Sensitization of the clinicians and
paramedical staff other than those involved in the program is required so that they can
also disseminate the knowledge in the community.
The structure and content of the training curriculum, the course materials and hand outs,
the competency based evaluation system were found to be of satisfactory quality both for
training in VIA and colposcopy. However, the reviewers felt that the total course duration
may be shortened and the master-trainers can be identified in select district hospitals or
MCWCs to conduct VIA training utilizing the same course modules and the training
materials. This will reduce the workload on the national coordinating center
(Bangabandhu Seikh Mujib Medical University) and will be logistically convenient for
the in-service candidates to attend the training. Training program for clinicians need not

4
be separate for learning VIA and colposcopy. They can be combined together to save
time and expenses.
Screening of women below the age of 30 years should be avoided as much as possible.
The VIA positivity is quite low (below 3%) in some of the screening centers that raises
the concern that some of the cases are being missed. The low positivity is probably due to
the fact that some of the positive cases are being ruled out as normal by the clinician at
the center without resorting to colposcopy. This should be discouraged. There is some
confusion among the providers regarding the test definitions and test criteria that need to
be settled.
The setups where screening is being done are spacious, well equipped and have regular
supply of consumables. The privacy and the comfort of the patients during examination
are being taken care of well by the providers. Pre-test and post-test counseling is being
done appropriately. Some of the centers need to have better focusing lights, preferably
halogen lamps. The knowledge and practice of infection control among the screening
providers were found to be of high quality.
The screen-positive women are being referred to the designated centers (set up in seven
medical colleges) for colposcopy and treatment. At present there is no mechanism to
ensure the compliance of the positive patients to diagnostic evaluation and treatment.
Linkage of screening to treatment is absolutely crucial for the success of the screening
program. Every VIA positive woman should be asked to provide a contact telephone
number. The patients or their relatives should be instructed to report back to the screening
center after colposcopy and/or treatment. The referral Institutions should also generate a
center-wise list of patients seen by them and send the list to the respective screening
centers on quarterly basis. The positive patients’ register maintained at the screening
center has to be updated from this list. The non-compliant patients may be contacted over
telephone or with the help of field workers working in the community.
The referral Institutions are well equipped for colposcopic evaluation and management of
cervical precancer and cancer. The referred women get preferential treatment and further
evaluations are done promptly. However, many patients do not come back for the
histology report and further treatment after colposcopy. To improve compliance to
treatment it is advised to follow ‘see and treat’ policy by doing treatment immediately

5
after colposcopic confirmation of disease. Cryotherapy should be practiced more
frequently as it is a safe, low cost and effective method of treatment for all grades of CIN.
To improve the program efficiency, each district should have a referral colposcopy center
with cryotherapy facility. This should be set up at the medical college hospital or at the
district hospital if there is no medical college in the district.
The computerized database of the referred patients is being maintained at BSMMU.
Effort should be made to maintain such databases in all the referral centers. A system of
giving a unique registration number at the screening center (district code-center code-
year-serial no) should be introduced. This will help to keep track of the positive cases at
all levels of service.
The reviewers have suggested modified quarterly activity report forms that should be
generated at the screening centers and the referral centers. The performance assessment
should be done on the basis of the standards listed in the reviewer’s report. This will
ensure ongoing internal quality control. Steps to ensure good quality service delivery are
enumerated.
The stakeholders for the program are Ministry of Health, Directorate General of Family
Planning, Directorate General of Health Services, BSMMU and other Medical Colleges.
The stakeholders have their roles clearly defined; a greater amount of coordination is
necessary. To ensure more efficient service delivery at the district level it is
recommended that the District Civil Surgeons are designated as Clinical Coordinators
and the Deputy Directors of Family Planning are designated as the IEC & Data
Managers. Each screening and referral center should have a nodal officer who will be
directly responsible for the day to day running of the program.

6
INTRODUCTION
Population based cervical cancer screening was launched in Bangladesh in 2004 with a
view to implement it in a phased manner. Bangladesh is among the few countries in the
world that have introduced Visual Inspection with Acetic Acid (VIA) as the primary
screening test in a nationwide community based screening program. The middle income
country with a total population of 124 million is divided into 64 districts. Currently the
screening facilities have been set up in 44 districts with Bangabandhu Seikh Mujib
Medical University (BSMMU), Dhaka as the central coordinating body and United
Nations Population Fund (UNFPA), Bangladesh as the major funding agency. Till
December 2007 more than 70,000 women have been screened through the program.
Any organized cervical screening program has the following components: community
awareness; screening; further evaluation and treatment of positive cases; follow up;
human resource development and program monitoring. The screening program of
Bangladesh has to address all these components to ensure that the program has the
desired impact. It is crucial to do systematic auditing of the program so that the
deficiencies can be identified at the earliest and improvement can be suggested.
Continuous proactive monitoring and appropriate corrective measures will ensure
satisfactory performance of the screening program and best utilization of the limited
resources. A team of external reviewers was formed to evaluate the activities in four
districts and in the city of Dhaka where cervical screening activities are going on since
2005. The team also audited the performance of BSMMU as the referral and treatment
center as well as the national training and coordination center. The current document is
based on their observations and recommendations. The document also aims to formulate
a protocol for internal quality-assurance (QA) so that data can be collected from all levels
in a standardized manner, analyzed meaningfully by the program managers and necessary
modifications can be implemented. The screening and management guidelines were
formulated by a national Advisory Board and were already field tested through a pilot
project. The reviewers intended to suggest modifications/improvements in the
implementation of the program within the framework of the recommendations of the
national experts.

7
OBJECTIVES
• Clearly define the measurable indicators that will help assess the performance of
the program in achieving the stated targets and goals
• Provide a framework to identify the strengths and weaknesses of the ongoing
program as well as report and resolve problems at the earliest
• Help continuous improvement in quality for all aspects of cervical screening
service delivery
• Promote continuing professional development and establish a culture of following
evidence based practice

8
ORGANIZATION OF THE CERVICAL SCREENING PROGRAM
Facilities for cervical screening by VIA have been set up in phased manner in 44 districts.
In each district headquarter there is a District Hospital that provides multidisciplinary
care and is under the Directorate of Health Services. The VIA screening services have
been set up in the Department of Obstetrics and Gynecology of the district hospitals. The
nurses have been trained to perform VIA and the Consultant Gynecologists have been
trained to supervise the nurses. In some of the districts the VIA facilities have been made
available in the Department of Obstetrics and Gynecology of the Medical College in
place of or in addition to the district hospitals. Each district has a Maternal and Child
Welfare Center (MCWC) under the Directorate of Family Planning primarily to provide
emergency obstetric care to women. These centers also have been equipped to perform
VIA. The health workers (Female Birth Attendants) along with the Medical Officers of
the centers have been trained. In select urban areas the VIA facilities has been set up in
the Comprehensive Reproductive Health Care Centers (CRHCC) that are run by the
Ministry of Local Government in collaboration with the non-governmental voluntary
organizations. There the nurses have been trained to perform the test under the
supervision of a clinician. As per the country guidelines cervical screening is offered to
women aged 30 years and above at three years interval. The screening test is free of
charge. Screen positive women are asked to attend the referral centers for further
evaluation. A total of 73539 women have been screened from January 2005 till December
2007.
Referral centers with facilities to perform colposcopy and cervical biopsy have been
established in 7 Medical College Hospitals including BSMMU. Treatment by
Cryotherapy and LEEP is available in 3 centers. The locations of the screening and
referral centers are shown in Figure 1. Cervical punch biopsy is performed if any
abnormality is detected on colposcopy. Histology facilities are available in the
Department of Pathology of the referral centers. Treatment is usually done after the
histology reports are available.

9
Figure 1. The locations of the screening and referral centers. [Screening Centers -
Referral Centers - ]
The Department of Obstetrics and Gynecology of BSMMU is the National Coordinating
Center responsible to organize training, identify and set up new screening and referral
facilities and maintain quality assurance of the program.
The United Nations Population Fund (UNFPA), Bangladesh provides technical and fiscal
support to procure equipment for the screening and referral centers, generate IEC and
training materials and conduct periodic quality assurance for the program. The entire
program is under the auspices of the Ministry of Health, Government of Bangladesh.

10
PRINCIPLES OF MONITORING & EVALUATION
The ultimate ‘impact’ of cervical screening program is the reduction of incidence of
cervical cancer and mortality from the disease. Initially the program is likely to detect
many of the undiagnosed prevalent cancers that may be reflected as an apparent increase
in the incidence. There will be a stage-shift of the detected cancer cases with more and
more cases being diagnosed at earlier stages. As the cervical precancers are detected and
treated there will be a gradual reduction in new cases of invasive disease. However,
reduction in incidence and mortality as an impact of screening program will take at least
10 years to be evident. In the meantime, evaluation of the performance of the program
can be done by assessing the following short term performance indicators:
• Access to screening services
• Access to colposcopy and treatment services
• Quality of the services
• Competency of the staff
• Rate of participation to screening specially of those who are hard to reach
Critical information required to assess the above-mentioned parameters have to be
generated in a timely way on regular basis from the screening clinics, referral centers and
from the coordinating Institute. A well organized online Medical Information System
(MIS) capable of maintaining such records and linking all the centers may not be feasible
to set up in a country like Bangladesh. If the data collection forms and registers are
maintained at each level of service properly, the data required for quality assurance
exercise can be retrieved from them and analyzed periodically. The forms and registers
should be similar in content, have the same format and will use common terminologies
across all the screening and referral centers. All service providers including the health
workers should be appropriately trained and should understand the importance of
maintaining legible and accurate records.
The ideal way to study the cervical cancer incidence and mortality among the screened
population is to have a population based cancer registry (PBCR) in the areas where
screening is ongoing. The trend in the incidence and mortality can be linked to the
information about the screening uptake and outcome to get the best evaluation of the

11
screening program. Bangladesh is yet to have a population based cancer registry program.
In absence of a PBCR, the information about the cervical cancer patients can be collected
from all the major hospitals having facilities for cervical cancer treatment using a
uniform proforma. This will provide a rough estimation of the stages of cervical cancers
at detection and also of the number of interval cancers (cancer in screened population).
Both these indicators are important to evaluate performance of screening program.
METHODOLOGY OF CURRENT EVALUATION
The principal funding agency (UNFPA) decided to do an external quality assessment of
the program after it completed three years in May 2008. Consultants not directly involved
in the strategic planning or implementation of the program were engaged to review the
past and ongoing activities. One of the consultants was from outside the country with
expertise and experience in conducting cervical screening programs. The other consultant
was from Bangladesh experienced to perform quality assurance for different public health
programs. They visited different levels of service delivery setups in Dhaka and four
districts (where the program has completed at least one year), collected data using a
structured form (Appendix 5), examined the records, interviewed the service providers
and held discussions with the program managers, health officials and NGO
representatives over a period of 10 days. They interviewed some of the women waiting
for VIA as well as women who have completed the screening test (exit interview). As the
largest national referral center the performance of the colposcopy clinic at BSMMU was
evaluated. The database maintained at BSMMU of the referred patients was analyzed.
The structure of the training program and the teaching aids at BSMMU were assessed.
The observations and the recommendations of the reviewers are described in the
following sections.

12
EVALUATION OF THE SCREENING FACILITIES
Each screening center has designated a separate room in the out-patients’ department
(OPD) where screening by VIA is done on all working days. Women above 30 years of
age attending the OPD due to various ailments and those accompanying the patients are
counseled by the clinicians, nurses and health workers to undergo screening. Women
with symptoms suggestive of lower genital tract infection or of cervical malignancies
(vaginal discharge, abnormal vaginal bleeding, post-coital bleeding) are also sent for
VIA. General practitioners and gynecologists practicing outside the centers also send
such symptomatic patients for VIA. As a result screening is predominantly opportunistic.
Less than 10% of the women undergoing VIA come spontaneously after seeing the
billboards, posters or hearing about the program from community health workers. One
MCWC that works in collaboration with a rural based voluntary organization to motivate
women in the community reported much higher rate of spontaneous screening.
As a result of including mostly symptomatic women a large proportion of them (20-30%)
belong to the age below the recommended age of onset of screening (30 years). Screening
young women with VIA will have a high number of false positives due to the presence of
immature metaplasias at this age and will detect a large number of low grade lesions most
of which would have spontaneously regressed. This will create unnecessary burden on
the program and inconvenience to the women and should be avoided. Under-age women
with symptoms can have speculum examination at the OPD by clinicians and
appropriately advised. If there is any suspicion of malignancy the patient should be
directly referred for colposcopy and management.
VIA is being performed by nurses (at the medical colleges, district hospitals and
CRHCCs) and Female Health Volunteers (at the MCHCs) after they underwent a
certified training course of 15 days at BSMMU. Most of them had reorientation courses
within 6-12 months of the initial training. It is the practice of most providers to get their
findings cross-checked by a clinician specially when they detect a positive case. After
about 50 VIAs done under supervision, the nurses/health workers need not consult the
clinicians except in circumstances where they face difficulties to expose the cervix or
encounter excess bleeding. The cases they feel border-line or doubtful, should be

13
categorized as ‘positive’ and referred. This will reduce the number of false-negative
cases.
In most of the centers women detected to have cervical growth (VIA classification –
Cancer) are either categorized as ‘positive’ or are not recorded in the VIA register at all.
The test-providers should be instructed to enter all such cases in VIA positive register as
‘cancer’ and if possible get them clinically staged by a competent clinician before
referral.
Some test providers are categorizing women without visible squamo-columnar junctions
as ‘unsatisfactory’. This is not required in the context of VIA.
If the cervix can not be adequately exposed due to technical difficulties, these cases
should be entered in the card/register as ‘inadequate VIA’ and the number of such cases
should be as low as possible.
The total number of women screened in various centers over the last 12 months has
varied from 778 to 1819 in the district hospitals audited and from 160 to 823 in the
MCWCs audited by the reviewers (Figure 2).
1819
439
778
160
929823 893
259
0200
400600800
100012001400
160018002000
DH MC DH MC DH MC DH MC
DIST A DIST B DIST C DIST D
Figure 2. The number of women screened over last 12 months in the districts evaluated
(DH – District Hospital, MC – MCWC)
The difference of number of screened women between the district hospitals and the
MCWCs is explained by the fact that district hospitals have much higher patient turn outs

14
in the OPD. The district (District C) in which the voluntary organizations are doing
community based awareness had almost equal number of attendees to the district hospital
and to the MCWC. The highest number of women screened in a district over last one year
is 2258. This has to increase substantially as the average estimated number of women in
30-60 years age group in each district is over 300,000. The number of women screened
per year through out the country has a steady upward trend (year 2005 = 11145; year
2006 = 21609; year 2007 = 40785)
The VIA positivity varied from 1.4% to 3.1% in the district hospitals and from 7.3% to
12.7% in the MCWCs evaluated by the expert team. The CRHCC visited had positivity
of 1.5%. The studies performed across the world observed that the range of VIA
positivity is 5-9% in the general population. The test positivity depends on provider
experience (high in the freshly trained), age of the screened women (high in young
women) and screening setup (higher in opportunistic screening). If the test positivity is
below the average there is a possibility of drop in sensitivity and risk of missing some of
the true positive cases. A reason for the low positivity in the district hospital may be the
practice of ruling out some of the VIA positive cases by the gynecologists as normal
without resorting to colposcopy. This should be discouraged.
In the present circumstances, getting accurate and complete data to evaluate the efficacy
of VIA in the conventional way is not feasible. From the BSMMU database colposcopy
and biopsy (if performed) reports were obtained for 1257 women who were VIA positive.
Of them 698 women were normal on colposcopy (55.5%) and did not require biopsy.
There were 152 cases of CIN 1, 100 cases of CIN2/3 and 52 cases of invasive cancer
proved on biopsy. The Positive predictive value of VIA to detect CIN1+ lesions was 24%
and CIN2+ lesions was 12.1%. Similarly calculation from data obtained from
Colposcopy clinic of Rajsahi Medical College (N=179) produced positive predictive
values of 25.2% and 5.6% to detect CIN 1+ and CIN 2+ lesions respectively.
The screening clinics are spacious, clean and ensure adequate privacy of the women. The
consumables supplies are adequate and regular. The container with glacial acetic acid
should be clearly labeled and preferably be kept away from the examination area. 4-5%
acetic acid is prepared daily. All the centers should be provided with a 100ml measuring
cylinder that will make preparation of dilute acetic acid easier.

15
Most of the clinics have good quality focusing light in working condition. The ordinary
bulbs of the spotlights may be replaced by halogen bulbs if feasible. A spare halogen bulb
should be provided. The requirement of cusco’s specula may increase with the increased
turn out of women.
All the screen providers are well aware of the infection control measures and are
practicing as per the guidelines. When the number of clinic attendees will increase the
autoclaved specula may not be adequate. A sterilizer should be provided after assessing
the demand.
The VIA negative women are issued a VIA negative card, reassured and asked to come
for repeat screening after 3 years. The VIA positive women are issued a VIA positive
card, counseled and asked to attend the nearest Colposcopy referral center.
Each center is provided with a VIA register to document the details of all screened
women and a VIA-positive register to record the details of the test positive women. Both
the registers are being filled up appropriately. All efforts should be made to document the
telephone numbers of the screen positive women so that they can be contacted later. The
treatment/follow up records of the referred patients are mostly incomplete as there is no
mechanism at present to get such information unless the patient comes back to the
screening clinic after visiting the referral center.
At the time of referral the patients should be informed about the service charges if any at
the referral center. They should also be told that if necessary they will be treated at the
referral center on the same day of their visit.
Some of the VIA providers commented that doing VIA is adding to their existing heavy
burden of work. Almost all of them agreed that the test was technically simple and easy
to interprete.
16
EVALUATION OF THE COLPOSCOPY REFERRAL CENTERS
Facilities for colposcopic evaluation and management of precancers have been set up in
the Department of Obstetrics and Gynecology of seven medical colleges across the
country. The clinics function on all working days. Gynecologists with post-graduate
degree or diploma have been trained to perform colposcopy, cryotherapy and LEEP at the
training course at BSMMU over 15 days. The charges for colposcopy vary from 0-300
Taka and that for cervical biopsy varies from 0-150 Taka. Treatment of precancers is free
of charges. All the VIA positive women undergo colposcopy and cervical punch biopsies
are obtained at the same sitting if any abnormalities are detected. The biopsy specimen is
carried to the pathology laboratory by the patient or her relatives. The patient is asked to
come back with the biopsy report for further management. The time gap between
colposcopy and obtaining the histology report at BSMMU is 4-12 days.
At present there is no mechanism to evaluate compliance to colposcopy for the VIA
positive women as the records from the screening clinics are not linked to that from the
colposcopy clinics. A major determinant of compliance will obviously be the distance
between the referring center and the colposcopy clinic. The number of women belonging
to Narayangunj district (adjacent to Dhaka) who had colposcopy at BSMMU till
December 2007 closely matched the number of VIA positive women referred from that
district indicating a high compliance rate. The total number of referrals from Bogra
district (200 Km away from Dhaka) during that time was 272 and the number of women
from that district who had colposcopy at BSMMU was only 98 (36%). Some of the
patients from Bogra might have attended the colposcopy clinic at Rajsahi Medical
College that became functional since June 2007.
Of the total referred patients colposcoped at BSMMU 22% were found to be below 30
years of age which explains the high prevalence of CIN 1. Nearly half were found to be
normal on colposcopy and did not require biopsy. If there is a lesion on the ectocervix
and the squamo-columnar junction is not visible the colposcopic diagnosis should be
according to the grade of lesion visible. Presently such cases are being classified as
‘unsatisfactory’.
The details of histology reports of the 1500 patients who had colposcopy at BSMMU
from 2005 till 2007 are shown in Table 1. The proportion of biopsies reported as

17
inadequate tissue for evaluation is quite low indicating that the appropriate punch biopsy
forceps are being used. In 16.2% cases the report is not available as the patients did not
come back after colposcopy and naturally did not have further management. VIA picked
up 5 cases of adenocarcinoma that comprised 12% of all cancers for which types were
specified. Stages of cancers detected at BSMMU Colposcopy clinic: Stage I-IIa – 30 ;
Stage IIB+ - 22; Unstaged – 32. More cases have been detected at earlier stage than
would have been expected without screening.
HISTOLOGY NUMBER PERCENT
Biopsy not done 698 46.5
Normal & others 252 16.8
CIN 1 152 10.1
CIN 2 81 5.4
CIN 3 19 1.3
Sq cell Carcinoma 38 2.5
Adeno Carcinoma 5 0.3
Cancer Type Unspecified 9 0.6
Tissue Inadequate 3 0.2
Report not available 243 16.2
TOTAL 1500 100.0
Table 1. Details of histology reports from BSMMU colposcopy clinic
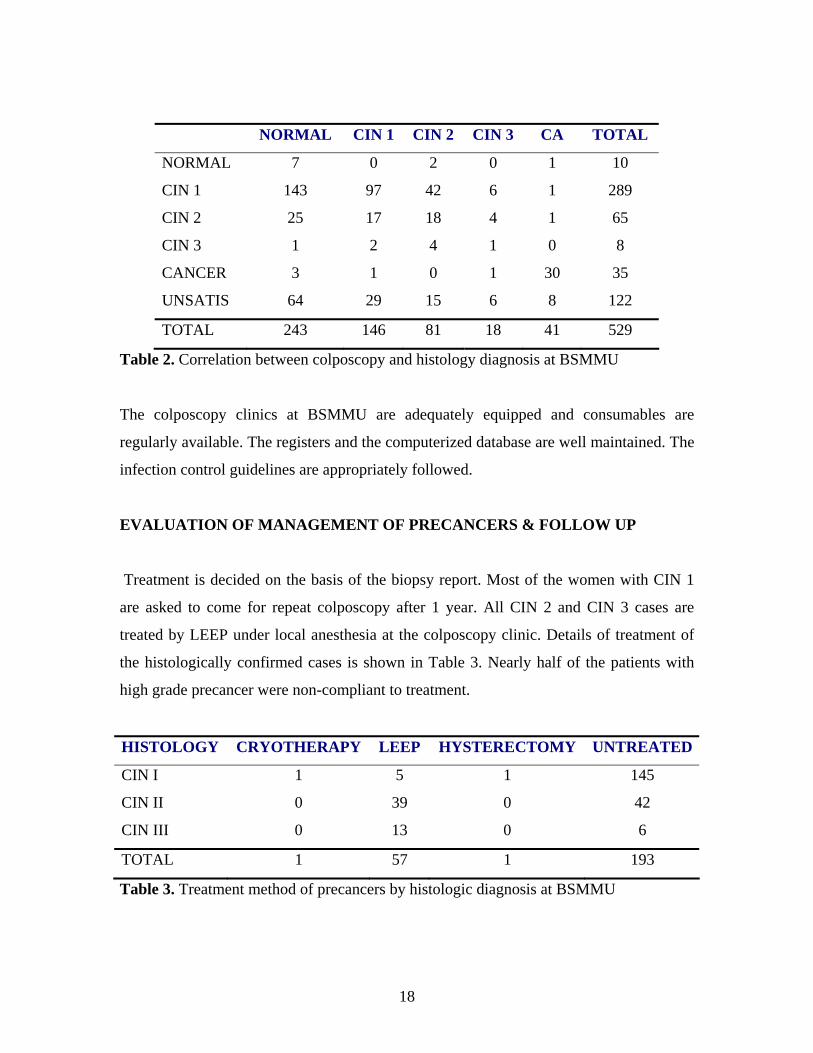
The correlation between colposcopy diagnosis and histology diagnosis at BSMMU is
shown in Table 2. The predictive value of colposcopic diagnosis of CIN 2+ lesions was
55%.
The colposcopist repeats VIA before doing colposcopy. The result of VIA by
colposcopist should be entered in the colposcopy register. This will help to assess the
VIA performance by calculating the agreement between VIA done by paramedics and
VIA done by expert clinicians.
18
NORMAL CIN 1 CIN 2 CIN 3 CA TOTAL
NORMAL 7 0 2 0 1 10
CIN 1 143 97 42 6 1 289
CIN 2 25 17 18 4 1 65
CIN 3 1 2 4 1 0 8
CANCER 3 1 0 1 30 35
UNSATIS 64 29 15 6 8 122
TOTAL 243 146 81 18 41 529
Table 2. Correlation between colposcopy and histology diagnosis at BSMMU
The colposcopy clinics at BSMMU are adequately equipped and consumables are
regularly available. The registers and the computerized database are well maintained. The
infection control guidelines are appropriately followed.
EVALUATION OF MANAGEMENT OF PRECANCERS & FOLLOW UP
Treatment is decided on the basis of the biopsy report. Most of the women with CIN 1
are asked to come for repeat colposcopy after 1 year. All CIN 2 and CIN 3 cases are
treated by LEEP under local anesthesia at the colposcopy clinic. Details of treatment of
the histologically confirmed cases is shown in Table 3. Nearly half of the patients with
high grade precancer were non-compliant to treatment.
HISTOLOGY CRYOTHERAPY LEEP HYSTERECTOMY UNTREATED
CIN I 1 5 1 145
CIN II 0 39 0 42
CIN III 0 13 0 6
TOTAL 1 57 1 193
Table 3. Treatment method of precancers by histologic diagnosis at BSMMU

19
Patients are kept admitted for few hours and are allowed to go home in the afternoon. Till
date no patient required general anesthesia for treatment. Only one patient came back
with complication later. An informed consent form should be administered before
treatment.
Cryotherapy has been proved to be a safe and effective method of treating all grades of
CIN provided the lesion does not occupy more than 75% of the transformation zone, can
be covered by the cryo-probe and does not have endo-cervical extension. It is an easy
technique to learn and the immediate and long term complications are very minimal. The
recurrent cost of cryo-therapy is also much less as compared to LEEP. It is advisable to
use cryotherapy more frequently for the screening program as the equipment is available
in all the colposcopy centers.
The follow up of the CIN 1 lesions can not be ensured in the present set up and is
logistically inconvenient both for the patient and the program. All CIN 1 patients should
be assessed for suitability of cryotherapy and offered treatment if found appropriate.
Colposcopy followed by treatment at the same sitting (‘see and treat’) is an accepted
norm for treating CIN and should be practiced provided the patient is willing. Although
there will be some over-treatment, the compliance to treatment will be high. It is obvious
from the BSMMU records that a significant number of patients do not return for biopsy
report/treatment. If the treatment is done by cryotherapy, punch biopsy should be
obtained prior to that.
The followup recommendations for patients treated by cryotherapy and LEEP are
different that may be difficult to adhere to. There is no record of any patient having
follow-up VIA at the screening centers evaluated.

20
RECOMMENDATIONS FOR INTERNAL MONITORING & QA
For the screening program to be effective and efficient, a regular ongoing quality control
plan in-built in the program is necessary. The quality assurance program should cover all
levels of services – screening facilities, colposcopy and treatment facilities, pathology
laboratories and training program. Presently it is not very structured and well defined,
specially in terms of how frequently it should be done and by whom. The expected
standards at various levels of service delivery conditions need to be delineated. The
following section defines the quality standards and suggests the means to achieve that.
Quality Standards for Screening
• Women should be screened from 30 years onwards. The national guidelines for
upper limit of age for screening should be fixed. For VIA based screening it is
generally recommended to limit the upper age at 60 years.
• Screening interval should not be less than 3 years
• Considering the logistic constraints it will be impractical to fix a coverage rate at
the present scenario. The number of women screened per center per month has to
increase significantly. A realistic target may be set depending on the capacity of
the screening center. All efforts should be made to increase the proportion of
spontaneous screening and reduce that of opportunistic screening.
• VIA should be done by certified providers only
• VIA positivity should be 5-9%
• All VIA positive women should be referred for colposcopy and at least 80% of
them should be able to reach colposcopy clinic within a month of referral
• Appropriate infection control and sterilization procedures should be practiced
Ensuring Quality Standards for Screening
• Each screening clinic will generate quarterly report as per the Screening Center
Reporting and QA form (Appendix 2) and send to BSMMU
• Each screening clinic will have a Nodal Officer responsible for generating report
and take appropriate action in case there is ay deviation from standard.

21
• The National Program Coordinator at BSMMU should check the reports at least
twice a year and will guide the Nodal Officers when necessary.
• The screening coverage and rate of spontaneous screening can be improved by
doing broad based awareness program in the community and by making the
facilities accessible to the rural population. Involving the voluntary grass-root
level organizations will also help to disseminate the knowledge and information.
The screening clinics may be set up at the Upazilla Primary Health Complexes.
These issues have been discussed in details later.
• The VIA providers should counsel the VIA positive women along with their
family members and ensure that they understand properly why and where to go
for colposcopy. They should be advised to report back to the screening center
with the card within a month of completion of colposcopy/treatment. The VIA
positive register has to be kept updated about the information on colposcopy and
treatment.
• The referral centers will generate a quarterly report showing the district-wise list
of women colposcoped and treated by them. This list will be sent to the district
coordinators who will ensure that the VIA-positive registers are updated at the
screening centers.
• The defaulter women should be given a reminder over telephone or through field
workers when feasible.
• To simplify tracking of the positive women a uniform system of assigning a
unique registration number to each woman should be started. The Number will
contain a district code, center code, year of registration and registration number.
The codes will be provided by the National coordinating center at BSMMU.
Quality Standards for Colposcopy & Treatment
• All VIA positive women referred to the colposcopy center must have colposcopy
on the day of first visit
• VIA should be repeated before colposcopy. The concordance between VIA report
from the screening clinic and VIA report from the colposcopy clinic should be
>80%

22
• The colposcopist should have the certified training at BSMMU and should be
doing at least 15 colposcopies per month
• All cases suspected to have CIN on colposcopy should have biopsy unless an
excisional treatment is planned at the same sitting. If biopsy is not done the reason
should be written down
• Colposcopic features along with colposcopic impression of lesion grade should be
documented
• More than 90% of the biopsies should be suitable for histological interpretation
• The histology report should be available within 2 weeks of colposcopy
• The predictive value of colposcopy diagnosis of CIN2+ lesions should be >60%
• >90% of the histology/colposcopy proved high grade lesions should be treated
within two months
• Appropriate infection control and sterilization procedures should be practiced
Ensuring Quality Standards for Colposcopy & Treatment
• Each Colposcopy clinic will generate quarterly report as per the Colposcopy
Center: Reporting and QA form (Appendix 2) and send it to BSMMU
• Each Colposcopy clinic will have a Clinic-in-charge responsible for generating
report and taking appropriate action in case there is any deviation from standard.
• The National Program Coordinator at BSMMU should check the reports at least
twice a year and will take necessary actions
• Information regarding investigations and treatment of the patients should be
communicated to the referring centers periodically
• More stress should be given to teach cryotherapy to the clinicians
• ‘See and treat’ policy should be followed more frequently
• There should be definite guidelines for management of complications of treatment
• Efforts should be made to set up colposcopy and cryotherapy facilities in each
district that in the long run will help to improve compliance to colposcopy and
treatment.
Quality Standards for Histology
23
• Histology reports of all patients who had biopsy should be available to the
colposcopy clinic within 15 days
• The proportion of inadequate biopsies should be less than 10%
• Histology report should follow the CIN system of reporting and the grades of CIN
should be clearly mentioned
• Histology reports of LEEP specimens should comment on the margin status (both
endo and ecto cervical)
Ensuring quality standards for Histology
• If the number of inadequate biopsies goes up the punch biopsy forceps at the
colposcopy clinic need to be sharpened/replaced.
• If feasible the histology laboratory should be asked to send a copy of cervical
histology reports to the colposcopy clinics. Otherwise the reports need to be
retrieved every month from the laboratory registers.
• As an external quality control exercise randomly selected 10% of the negative
slides and 20% of the positive slides may be reviewed by a second pathologist.
• A certified training course for pathologist may also be considered
A compilation format for Quality Assurance Indicators has been included in
Appendix 6. The National Program Coordinator has to fill up this form annually
from the reports generated from the screening and colposcopy centers. He/she can
evaluate the performance of the entire program by comparing the national
indicators with the standards enumerated in this document.

24
STAKEHOLDERS AND PROGRAM MANAGERS
As the ambit of the program increases, it is of paramount importance that there should be
responsibility fixation at each managerial and service delivery level. BSMMU being the
national coordinating center must identify one National Program Coordinator who will be
responsible for:
• Ensuring that written protocols based on recommended national guidelines are in
place and are followed
• Ensuring that the protocols are regularly reviewed
• Ensuring that the defined quality assurance standards are being met
• Ensuring that regular audit of the services takes place
• Liaising with those responsible for providing the facilities to ensure that the
services are adequately staffed by appropriately trained individuals and the
service needs can be met in a timely and consumer friendly manner
• Coordinating training and facilitating the maintenance of continued certification
of practising service providers at various levels
• Informing Program Directors of any shortcomings of any aspect of the ability of
the screening and colposcopy services so that appropriate corrective actions can
be initiated
• Conducting regular dialogue with users, providers and other stakeholders to
ensure that service and development are both appropriate and meet with the needs
of the local population.
Such person should have adequate expertise in cervical screening paradigm, be
committed to the cervical screening service and be ready to take responsibility for it.
Organizational as well as training skills are also essential.
A tentative organizational flowchart for the entire program with representations from all
major stakeholders is depicted in Figure 3.

25
DIRECTORDGFP
DIRECTORPHC
PROGRAM CO-ORDINATORBSMMU
DDFP(IEC & DATA MANAGER)
CIVIL SURGEON/ SUPTDT(CLINICAL COORDINATOR)
HOD, OB & GYNMEDICAL COLL
NODAL OFFICERMCWC
CERVICAL SCREENING PROGRAMMINISTRY OF HEALTH
NODAL OFFICERMEDICAL COLL
NODAL OFFICERDISTRICT HOSP
NODAL OFFICERUPHCP
DIRECTORDGFP
DIRECTORPHC
PROGRAM CO-ORDINATORBSMMU
DDFP(IEC & DATA MANAGER)
CIVIL SURGEON/ SUPTDT(CLINICAL COORDINATOR)
HOD, OB & GYNMEDICAL COLL
NODAL OFFICERMCWC
CERVICAL SCREENING PROGRAMMINISTRY OF HEALTH
NODAL OFFICERMEDICAL COLL
NODAL OFFICERDISTRICT HOSP
NODAL OFFICERUPHCP
Figure 3. Proposed Organizational Flowchart for the Cervical Cancer Screening Program
At the district level the Deputy Director of Family Planning (DDFP) may be entrusted to
conduct the IEC for the program and data management in addition to supervision of the
MCWCs and the UPHCPs. The Civil Surgeon or Superintendent of district hospital will
be responsible for organizing the clinical services and staff deployment for the District
hospital as well as for the Medical College in consultation with the Head, Department of
Obstetrics and Gynecology of the district medical college. Each screening/referral facility
should have a nodal officer directly responsible for implementation of the cervical
screening program. A team meeting should be arranged at least once a year to review the
entire program.
Orientation of Field staff & Doctors
Orientation of Field staff & Doctors

26
EVALUATION OF TRAINING PROGRAM
Curriculum development and training of a critical number of service providers is a
significant achievement of the VIA program. The training modules are primarily aimed
at teaching VIA to nurses, health workers and clinicians and colposcopy and precancer
management to gynecologists. They are as follows:
a. Basic training on VIA
b. Training on colposcopy & precancer management
c. Refresher course on VIA
d. Combined training on VIA and Clinical Breast Examination (CBE)
Initially, the Department of Obstetrics and Gynaecology of BSMMU with support from
other institutes and Medical Colleges trained 25 Gynecologists as master trainers in 2004.
They then trained 113 service providers from 16 districts and 12 UH&FWCs in 2004 &
2005 at BSMMU. These service providers included Medical Officers and FWVs from
MCWCs, Consultants, Medical Officers and Nurses from Obs/Gynae deptt. of District
Hospitals (DHs), and FWVs from selected unions. Then in 2006, after extension of the
programme, 100 more service providers from 14 districts were trained on VIA. In 2007,
134 service providers from 28 districts were trained. For development of referral centres
in various medical college, 37 Gynaecologists were trained on Colposcopy in the year
2006 and 2007. Thus, colposcopy centers were developed for VIA+ cases in BSMMU,
Chittagong, Sir Salimullah, Rajshahi, Khulna and Mymensingh Medical College
Hospitals. A joint curriculum on “Cervical and Breast Cancer Screening Programme:
Standard and Guidelines” was developed in both English and Bengali language. The
training materials developed till date are:
a. Cervical and Breast Cancer Trainer’s Handbook (in English)
b. Cervical and Breast Cancer Screening Programme: Trainee’s Logbook (in English
& Bengali)
c. Cervical and Breast Cancer Screening Programme: Standard and Guidelines (in
English & Bengali
d. Training Curriculum (in English & Bengali)
e. Training materials in CD-ROMs

27
These were finalized in consensus meetings involving experts from DGHS, DGFP,
UNFPA, WHO, OGSB and BSMMU.
During the Program Evaluation the training materials and training methodology were also
observed and service providers interviewed to ferret out the gap with the existing health
and family planning program of the country and recommend suggestions. The gaps
identified and steps suggested are as follows-
1. Currently, the clinicians and the paramedics are called in same batch for training
on “Cervical Cancer and Breast Screening” and the clinicians are again called for
separate training on “Colposcopy”. As the roles of these two categories of service
providers in the program are different and their background knowledge and
competence also differ, their training modules and sessions should be separate.
All the clinicians selected for training are gynecologists (Post-graduate
degree/diploma/certificate holders). They should be taught screening (including
VIA) and colposcopy in a combined module.
2. The present course modules (both for VIA and Colposcopy) require 15 days of
training and after inclusion of the holidays the total course duration extends to 17-
20 days. As all the trainees are from in-service, staying away from their routine
work for such an extended period hampers the regular service of their respective
centers. It is suggested that the training should be made more compact to
accommodate within 10 days. With the current patient turnout at BSMMU it is
feasible.
3. The training on VIA of the FWVs and nurses should be gradually decentralized
and provided at the medical colleges and select district hospitals/MCWCs through
creation of some new master-trainers at those level. The adequacy of patient
turnout at the center should be assessed before designating it as training center.
The master-trainers should be provided with all the teaching aids including the
electronic materials.
4. Department of Obstetrics and Gynaecology of BSMMU should focus on
providing training for the Gynaecologists on Cervical Screening, Colposcopy and
Management of Cervical Precancers, ensuring the quality standards of the
teaching programs in the other centers and developing appropriate teaching
materials incorporating the recent developments in the area.

28
5. All the trained VIA providers should be supervised by the trained clinicians for
first 6 months or till they complete 50 cases, whichever is earlier, for the quality
of their performance and provided refresher training at least once every year.
Duration of refresher course should not exceed 5 days and preferably be arranged
in the district.
6. Efforts should be made to retain the trained staff at their respective
centers/hospital or to post them at centers/hospitals where their expertise in
VIA/Colposcopy can be utilized.
7. If the cervical screening methods (including VIA) are included in the training
curriculum of the undergraduate and postgraduate (Ob & Gyn) medical students,
the nurses and the paramedics that will pay dividend in the long run.
EVALUATION OF THE ‘MANUAL OF SCREENING PROGRAM STANDARDS
& GUIDELINES’
The reviewers felt that the following modifications in the manual may be incorporated in
the next edition after consultation with the national experts.
Appendix III; Page 104: The classification of VIA findings may be the same as followed
by International Agency for Research on Cancer (IARC, Lyon). According to that
classification system VIA is categorized as negative when any of the following are
observed:
• No acetowhite lesions, or faint, ill-defined, bluish white or doubtful lesions
• Acetowhitening on cervical polyps or on nabothian cysts
• Dot- or streak-like acetowhitening on the cervix
• White line-like prominent squamocolumnar junction (SCJ) after application of
acetic acid
• Angular or geographic acetowhite lesions far away from the SCJ or the external
os, if SCJ was not visible
VIA is categorized as positive when any of the following are observed:
• Well-defined, opaque, acetowhite lesions touching the SCJ or the external os, if
SCJ is not visible

29
• A large circumferential acetowhite lesion surrounding the external os
• Pre-existing wart or leukoplakia turning intensely white after application of acetic
acid
An ulceroproliferative growth on the cervix is categorized as Cancer.
The present classification is of ‘high threshold’ that may also be the reason for low VIA
positivity.
Page 59: Management of VIA +ve cases. Repeat VIA is not necessary after antibiotics
treatment. All positive cases should be referred.
Page 64: Follow up after treatment. Post-cryotherapy patients may be followed up in the
same way as post-LEEP patients.
Option for ‘see and treat’ should be discussed in the management section.
Management of post-treatment complications specially secondary hemorrhage need to be
discussed more elaborately.
There is no guideline for management of cases where colposcopy suspects high grade
lesion but punch biopsy turns out to be CIN 1 or no CIN.

30
EVALUATION OF INFORMATION, EDUCATION AND COMMUNICATION
(IEC) ACTIVITIES
Dissemination of information to the target population is among the most important
determinants of success of the program. The Department of Obstetrics and Gynaecology
of BSMMU with other institutes have developed IEC materials (Posters, Brochure and
Flip Chart) and distributed in project areas after approval of Ministry of Health and
family Welfare. Twenty orientation meetings among health service doctors, FWVs and
FWAs were held at district level so far to create awareness on cervical cancer and VIA.
The VIA program is till using an opportunistic drive for IEC. Where all the women above
30 years should be invited for VIA, only the women attending the MCWCs, District
Hospitals, Medical College Hospitals and specified UHFWCs and UPHCP clinics for
general health, gynecology or family planning services are being informed and called for
VIA. The billboards and posters prepared for VIA are also used for this purpose
predominantly in front of the hospitals and clinics mentioned above. The field workers
making home visits for several other health programs have not been actively involved to
educate the target women. As a result, a large part of women above 30 years are staying
outside the IEC of VIA and the clinic attendances are quite low. Interestingly, the
clinicians, the general practitioners and gynecologists and obstetricians who are not
directly involved with the program have little information about the new national
program.
The recommendations for broad based IEC program are as follows:
1. The general practitioners and gynecologists (both government service-holders and
private practitioners) should be informed of the need of examining all the women
above 30 years for the prevention of cervical cancer, the screening program taken
up by the government, and the hospitals and clinics where the services are
provided. Orientation programs can be organized with the help of national
professional organizations and their local branches eg. Bangladesh Medical
Association, Private Practitioner’s Association and Obstetrics and Gynecological
Society of Bangladeh.

31
2. Both electronic (radio & TV) and print media should be utilized to disseminate
the knowledge to the population. The content, packaging and communication
strategies should be determined with the help of expert professionals in this area.
3. All the FWVs, FWAs, HAs and SBAs of the VIA service providing districts
should be informed of the program, so that they can motivate the women above
30 years age for VIA in the nearby facilities. They should be provided with low
cost leaflets describing the screening test to be distributed in the villages.
4. The doctors, health and family planning managers, FWVs, FWAs, HAs and SBAs
at the district and upazilla level can be informed through monthly meetings by
CS, DDFP and upazilla level managers.
5. The NGOs and other voluntary organizations working for women’s health and
development at the community level have a key role to play in the program.
Active partnership should be developed with them to educate women through
house to house campaigns or group awareness meetings.
6. The local politicians, teachers and religious leaders should be sensitized to form
local peer groups whose help can be sought from time to time to arrange group
meetings. Such meetings should also involve the husbands and other family
members.
7. The posters and billboards should be more widely displayed.
8. The IEC activities should be implemented and regularly monitored by the DDFPs
of the districts.

32
CLIENT SATISFACTION SURVEY
In cervical cancer screening program the asymptomatic women are invited to undergo a
medical examination for which the benefits are not immediately apparent to them. To
ensure adequate spontaneous participation of the target women it is absolutely essential
that they are satisfied with the service delivery. The counselling of the women before and
after the test has to be proper so that the women comply with subsequent
recommendations (repeat screening for negative women and colposcopy for positive
women). As the screening program in Bangladesh is still in its formative stage, the
feedbacks from the clients can be a useful tool to assess the performance and suggest
improvements. The specific issues to be addressed by such survey in the context of the
cervical cancer screening program will be:
To assess the awareness of the target women about
• Cervical cancer is a significant cause of morbidity and death
• Cervical cancer can be prevented through screening
• Screening services available
• Timings and location of the services
• Procedure and examination
• Significance of the test results
• Necessity to get treatment and follow up if advised
To assess if the women perceive that
• The service providers are efficient
• The quality of the services is acceptable
• Their privacy has been adequately maintained
• Service providers have spent adequate time
• Time spent in travelling to the clinic is acceptable
• Time spent waiting for the test is acceptable
• Their concerns have been adequately addressed to
• They can refer their friends/relatives to the clinic
The Client Satisfaction Survey should be done (preferably by persons not directly
connected to the program to avoid Social Acceptability Bias) once a year. The target area,
33
timing of such survey and the sample size will be determined by the National Program
Co-ordinator. A client satisfaction survey questionnaire has been designed by the
reviewers and included in Appendix 4 for future use.
Some of the key observations of the reviewers related to the issue of client satisfaction
collected through interviews of women waiting for VIA and undergone VIA in the
hospitals and clinics.
• In most of the facilities the women were counseled and sent for VIA by their
doctors and gynaecologists.
• Most of them were waiting for 1-2 hours. Those waiting for 2 hours or more
asked for quicker service.
• Among them who came from rural areas felt that similar service closer to their
home would have been better.
• Those waiting for VIA most of them knew that cervical cancer was a dangerous
disease and the test was to detect the disease early.
• Some of them were scared of the instruments and thought the test would be
painful
• Those who received VIA service, most of them were satisfied in general
• In one of the centres women informed that they didn’t get the colposcopy service
after going to the referral centre as the doctor was not available that day.
• They also asked for colposcopy service at nearby centre in their own district.
34
CONCLUSIONS
The limitations of the present evaluation study are:
The evaluation was done on the basis of observations of the activities of non-
randomly selected samples of the centers where screening activities are ongoing
The data on colposcopy and management were obtained from BSMMU, the
national training and co-ordination center whose performance may not reflect that
of other colposcopy centers
There was no structured way of collecting data before the evaluation and some of
the essential information are missing
Even at international level, the quality standards for a VIA based national
program are not yet well defined
The evaluation has done an in-depth assessment of the VIA based screening program for
the first time and more importantly has formulated a guideline to follow for ongoing
quality assurance. There was not much heterogeneity among the screening centers
evaluated in various districts. It is likely that the assessment of the selected sample will
reflect more or less the true picture of the national program.
The VIA based screening program is being up-scaled gradually. Currently most of the
services (screening and referral) are limited to the district headquarters and have less
reach to the rural sector. Even in those centers the utilization of the services is sub-
optimal. A broad based IEC program will improve the clinic attendances. Undeniably, an
expansion of the program is required. At the same time the program needs to consolidate
the existing facilities and ensure maintenance of appropriate quality standards at all
levels. The current evaluation document has suggested several
modifications/improvements that need to be prioritized depending on the feasibility,
logistics and fiscal resources. The program managers can set the immediate, short term
and long term goals based on the recommendations and formulate an action plan to deal
with issues in close cooperation with all the stakeholders.

35
APPENDIX 1: SCREENING CENTER: REPORTING & QUALITY ASSURANCE FORM
CENTER: DISTRICT: CODE:
REPORT YEAR: REPORT QR: Jan-Mar / Apr-Jun / July-Sept / Oct-Dec
VIA: Total: Positive: Cancer:
Inadequate: Repeat: <30 yrs
LIST OF VIA +VE CASES REGISTERED IN PREVIOUS QUARTER BUT COLPO/TREATMENT NOT YET DONE / INFORMATION UMKNOWN
REMINDER REGN NO. NAME CONTACT NO.
FW/TEL NO
Consumables & Stationeries required:
Equipment required/to be repaired:
VIA PROVIDERS: NAME DESIGNATION BASIC COURSE ON REFRESHER ON
IEC ACTIVITIES: Awareness meet: Field Worker orientation: Other:
COMMENTS:

36
APPENDIX 2: COLPOSCOPY CENTER: REPORTING & QUALITY ASSURANCE FORM
CENTER: DISTRICT: CODE:
REPORT YEAR: REPORT QR: Jan-Mar / Apr-Jun / July-Sept / Oct-Dec
COLPOSCOPY: Total: CIN 1: CIN 2/3:
Cancer: Normal/Other:
VIA: Positive/Cancer: Negative:
BIOPSSIES: No. of biopsies for CIN/CA: Inadequate:
HISTO REPORT: Unknown: CIN 1: CIN 2/3:
Sq CA: Adeno CA: CA unsp.: Normal/Other:
CRYOTHERAPY: Total: CIN 1: CIN 2/3:
Cancer: Normal/Other:
LEEP: Total: CIN 1: CIN 2/3:
Cancer: Normal/Other:
HYSTERECTOMY: Total: CIN 1: CIN 2/3:
SEE & TREAT: LEEP CRYO:
LIST OF CIN2+ PATIENTS DETECTED >1 MONTH BACK & TREATMENT PENDING
REGN NO. NAME CONTACT NO. DIAGNOSIS
COMMENTS:

37
Appendix 3: Check List of Equipment and Consumables for Screening/Colpo Clinic
Community Based IEC Equipment/Instruments Consumables Stationeries
• None • None • IEC Leaflets
• Flipcharts
• FWA Registers
Screening Centers Equipment/Instruments Consumables Stationeries
• Examination bed • Glacial acetic acid • Flipchart
• Spotlight • Cotton • Posters
• Instrument trolley • Gloves • VIA –ve cards
• Autoclave • Gauze pieces • VIA +ve cards
• Spare bulb • Bleaching powder • VIA register
• Cusco’s specula • Detergent • VIA +ve register
• Sponge holding forceps • Reporting forms
• Bowls/ galipot • Check list
• Trays
• Instrument drum
• Buckets
• Measuring cylinder
• Container for acetic acid
Referral Centers (Colposcopy) Equipment/Instruments Consumables Stationeries
• Examination bed • Glacial acetic acid • Colposcopy register
• Colposcope • Distilled water • Reporting forms
• Spotlight • Cotton
• Instrument trolley • Gloves
• Autoclave • Gauze pieces
• Spare bulb (colpo) • Bleaching powder
• Cusco’s specula • Detergent
• Sponge holding forceps • Monsel’s paste

38
• Punch biopsy forceps • Vaginal packs
• Endocervical forceps • Potassium iodide
• Bowls/ galipot • Iodine crystals
• Trays
• Instrument drum • Formalin Solution
• Buckets • Container for biopsy
• Measuring cylinder
• Container for acetic acid
Referral Centers (Additional requirement for cryotherapy) Equipment/Instruments Consumables Stationeries
• Cryotherapy machine • Filled up cylinder • Consent form
• cryo probes • KY jelly
• NO2 Cylinder
• Cylinder holder
Referral Centers (Additional requirement for LEEP) Equipment/Instruments Consumables Stationeries
• Electrosurgical unit • Large Loops • Consent form
• Suction machine • Dental syringe & needle
• Insulated Cusco’s specula • Inj Lignocaine
• • Lignocaine+Adrenaline
Persons to be contacted for supply:
Persons to contact for repair:

39
:CONTINUED:

40
APPENDIX 4 : QUESTIONNAIRE FOR CLIENT SATISFACTION SURVEY Date of Interview: Sl. No.
Respondent Category:
Randomly selected woman (>29yrs & married) in the community Randomly selected woman (>29yrs & married) at a health facility Woman waiting for VIA Woman who had VIA in last 1 month and tested negative Woman who had VIA in last 1 month and tested positive
1. Identification of respondent
Name: Age:
Vill/Ward: Union: Upazilla: Dist:
Married for: yrs Number of children:
2. Access to health care
2.1 Where do you usually go for treatment if you fall sick?
• Union Health & FWC
• Upazilla Health Complex
• District Hospital
• MCWC
• Private clinic/doctor
• Other (specify)
2.2 If you have any problem commonly seen in women (white discharge, abnormal periods etc.)
where will you go?
• Union Health & FWC
• Upazilla Health Complex
• District Hospital
• MCWC
• Private clinic/doctor
• Other (specify)
2.3 How far is the nearest hospital/health center from your house? ____ Km/Unknown
2.4 Did any FWA/HA visit your house in last 3 months? No / Yes / Don’t know
3. Knowledge about cervical cancer and its prevention?
3.1 Have you ever heard of cervical cancer (use Bengali term)? No / Yes
Skip Q3.2 – Q3.4 if response to Q3.1 is NO
3.2 Could you please describe what you understand about the disease?
_______________________________________________________
3.3 Do you know that this disease can be prevented? No / Yes
3.4 If yes, do you know how it can be prevented?
________________________________________________________
3.5 Have you heard of VIA test? No / Yes
3.6 If yes, where did you hear it from?

41
• FWA/ HA
• Doctor/SACMO
• Nurse/FWV
• Relative/neighbour
• Billboards/posters
• TV
• Newspaper
• Other (specify)
4.0 Knowledge about the VIA services (Only for those who responded Yes to Q3.5)
4.2 Could you please tell me the opening and closing hours of the VIA clinic?
_________________________________________________________
4.3 Has it been explained to you how the test will be done? No / Yes
4.4 Can you please tell me what it means if the result of the test is negative?
__________________________________________________________
4.5 Can you please tell me what it means if the result of the test is positive?
__________________________________________________________
4.6 Do you know that you will be sent to a higher center if the test is positive? No / Yes
5.0 Experience after going through the test
5.1 You were examined by a trained nurse/FWV. Do you think?
• She was good at her job and you are satisfied
• She was good but a doctor would have been better
• A doctor should have seen you
5.2 Was the examination center neat and clean? No / Yes
5.3 Was your privacy during examination adequately maintained? No / Yes
5.4 Did the nurse/FWV explain to you before and after the test? No / Yes
5.5 How much time did you spend to travel from your home to the center? _____Hr
5.6 How much time did you have to wait before the test at the center? _____Hr
5.7 How will you rate the overall experience you had at the center?
• Very bad
• Bad
• Neither good or bad
• Good, could be better
• Good
• Very good
5.8 Do you have any suggestions to improve the service?
_______________________________________________________
5.9 Will you advice your friend/relatives to go for the VIA test? No / Yes
5.10 If you were referred to a higher center did you go there? No / Yes
5.11 If not, why didn’t you go? _____________________________________________

42
APPENDIX 5: SCREENING PROGRAM EVALUATION: DATA COLLECTION FORM
Name of center: District
Status: Coordinating center / Medical College / District Hospital / MCWC / Other
Nodal officer:
Facilities available:
Screening
Colposcopy
Histology lab
Cryotherapy
LEEP
Training
Cancer Therapy
Other
Staff involved in Cervical Screening
Number Qualifications Responsibilities
Field staff (FWA/HA):
Health workers:
Nurses
Medical officers
Gynecologists
Pathologists:
Others:
Screening program initiated on:
Target Area:
Target population (30-60 yr):
IEC activities:
Total number screened
30-60 yr: Beyond 30-60 yr: Repeat screen:
Opportunistic: Spontaneous:
Monthly breakup last one yr:
VIA: Positive Negative Cancer Abandoned
Number of VIA +ve who had colposcopy:
Colpo diagnosis:
CIN 1 CIN 2/3 Inv Normal & others

43
Reasons for not having colposcopy:
Number of women who had biopsy:
Refusal for biopsy:
Average time required for histology reporting:
Mechanism for delivery of reports:
Histology diagnosis:
CIN 1 CIN 2/3 Micro-inv Inv Other
Treatment:
Cryo LEEP Hysterectomy Rad hyst RT
Number of untreated cases of CIN2+:
Reasons for no treatment:
Records maintained at the center:
Forms:
Registers
Computerized database
Consumables and supplies:
Adequate & regular / Requirement __________________________
Equipment
Adequate & working / Requirement _________________________
Sterilization & disinfection procedures
Appropriate / Requirement ________________________________
Ensuring competency of the screeners and colposcopists
Training
Supervised VIA/Colposcopy
Refresher courses
Mechanism of QA
Responsible Officer
Periodic checking of records
Periodic performance report
Laboratory QC
COMMENTS:
44
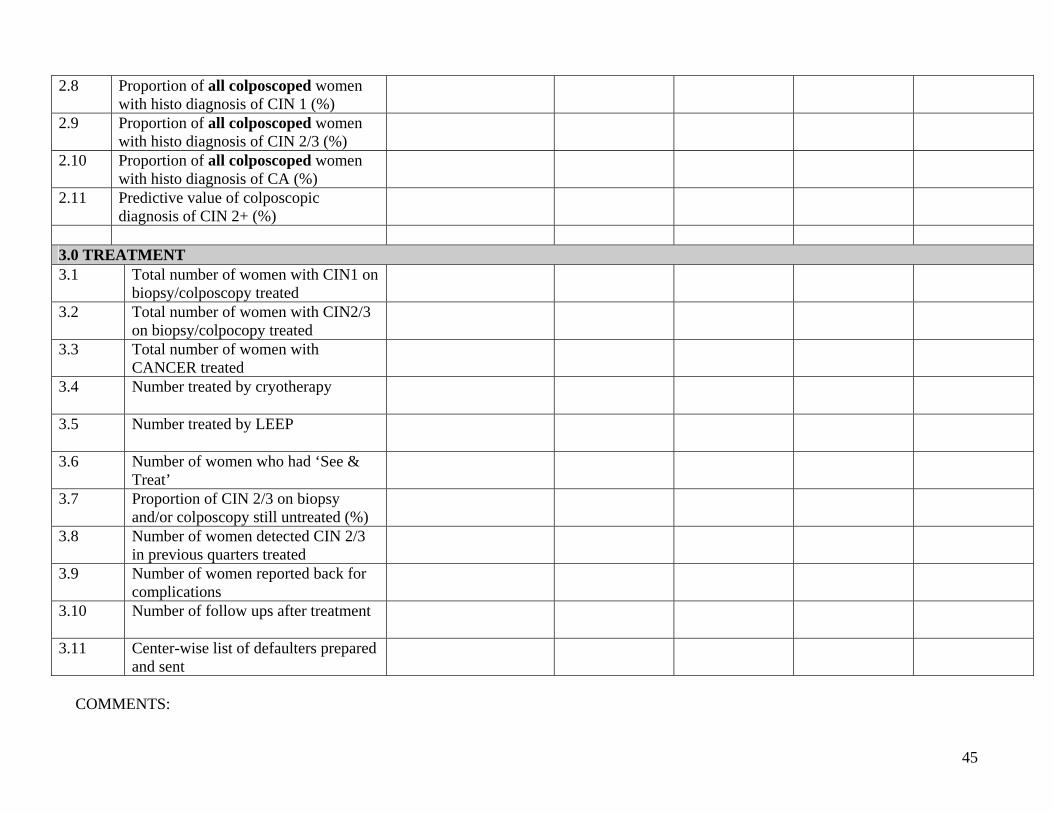
APPENDIX 6: CERVICAL CANCER SCREENING PROGRAM COMPILATION FORMAT FOR QUALITY ASSURANCE INDICATORS
DATE: DATE: DATE: DATE: DATE: INDICATOR BASELINE STATUS 1ST QUARTER 2ND QUARTER 3RD QUARTER 4TH QUARTER
1.0 SCREENING 1.1 Number of women screened
1.2 Proportion of women screened below 30 years (%)
1.3 Number of certified providers of VIA
1.4 VIA positivity (%)
1.5 Proportion of referred women attended referral centers (%)
2.0 COLPOSCOPY 2.1 Number of women colposcoped
2.2 Proportion of VIA+ve women found to be VIA+ve at before colposcopy (%)
2.3 Proportion of women with colposcopic diagnosis of CIN 1 (%)
2.4 Proportion of women with colposcopic diagnosis of CIN 2/3 (%)
2.5 Proportion of women with colposcopic diagnosis of CANCER (%)
2.6 Proportion of women with CIN1+ on colposcopy who had biopsies (%)
2.7 Proportion of inadequate biopsies (%)
45
2.8 Proportion of all colposcoped women with histo diagnosis of CIN 1 (%)
2.9 Proportion of all colposcoped women with histo diagnosis of CIN 2/3 (%)
2.10 Proportion of all colposcoped women with histo diagnosis of CA (%)
2.11 Predictive value of colposcopic diagnosis of CIN 2+ (%)
3.0 TREATMENT 3.1 Total number of women with CIN1 on
biopsy/colposcopy treated
3.2 Total number of women with CIN2/3 on biopsy/colpocopy treated
3.3 Total number of women with CANCER treated
3.4 Number treated by cryotherapy
3.5 Number treated by LEEP
3.6 Number of women who had ‘See & Treat’
3.7 Proportion of CIN 2/3 on biopsy and/or colposcopy still untreated (%)
3.8 Number of women detected CIN 2/3 in previous quarters treated
3.9 Number of women reported back for complications
3.10 Number of follow ups after treatment
3.11 Center-wise list of defaulters prepared and sent
COMMENTS: