Cervical Cancer Krzysztof Mędrek
45
Cervical Cancer Krzysztof Mędrek 1
-
Upload
abdul-barnes -
Category
Documents
-
view
36 -
download
0
description
Cervical Cancer Krzysztof Mędrek. Epidemiology - Poland. 3500 new cases of cervical cancer/year 1800 deaths/year 5 deaths each day !. Causes of cancer. MAIN = high risk factors. possible. Causes. HPV major cause of dysplasia and cervical cancer. HPV. - PowerPoint PPT Presentation
Transcript of Cervical Cancer Krzysztof Mędrek

Cervical Cancer
Krzysztof Mędrek
1

Epidemiology - Poland
3500 new cases of cervical cancer/year
1800 deaths/year5 deaths each day !
2

Causes of cancer
MAIN = high risk factors possible
3

Causes
HPV
major cause of dysplasia and
cervical cancer.
4

HPV
• > 100 different subtypes of HPV identified, • Most notable are HPV types 16 and 18
(HPV-16, HPV-18), • HPV products E6 and E7, bind to the RB
and TP53 tumour suppressor genes. • => removal of inhibitory influences on
cellular proliferation, which allows a growth advantage to affected cells.
5

HPV INFECTION
6

High risk factors
– HPV high-risk
– Multiple sexual high risk partners
– Early onset of sexual activity (<18y)
– Early childbearing (<16y)
– STI (Chlamydia trachomatis, Neisseria gonorrhoeae.)
– H-SIL history7

High risk factors
· Smoking
· DES exposure
[diethylstilbestrol is a hormone that was
prescribed for pregnant women in the 1950s and
early 1960s,to prevent miscarriages.]
· Weakened immune system 8

Cigarette smoking
• associated with an increased
severity of dysplasia.
• Nicotine and cotinine are highly
concentrated in the cervical mucus
of smokers. 9

Possible causes• Long lasting OC usage
• HIV infection
• Genital warts
• Genital herpes HSV2(?)
• Unbalanced diet – low levels of Vit C
• Poverty - poor may not have access to medical services
10

OC >>> Cervical cancer
• The effect of oral contraceptive (OC) use on the risk of cervical cancer is controversial.
• one study revealed a risk reduction, but…. (Brinton, 1986; Beral, 1988)
• OC => SEX => HPV => CANCER11

FACTS about SCREENING
Number of papers and clinical researches have proved that screening:
1. reduces the risk of developing cervical cancer and,
2. reduces the amount of deaths of invasive cancer
12

SCREENING levels
•Pap smear (Bethesda)
•Colposcopy
•Cervical biopsy
•HPV test13

Clinical examination
• Complex examination by a physician
(both interview and clinical one).
• Gynecological examination p.v. and p.r.
• Cytology – PAP smear
• Colposcopy
• Biopsy of any abnormal lesion !!!!
14

15

16

17
normal
dysplastic cells

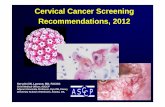
Colposcopy
18

Colposcopy is indicated • whenever a magnified examination of cervical topography and
epithelial character are needed. Common indications include: Grossly visible or palpable abnormality of the cervix
• Abnormal cervical cytology • Positive screening test for cervical neoplasia such as
spectroscopy, cervicography, speculoscopy • Cervical cytology unsatisfactory due to unexplained
inflammation • History of in-utero diethylstilbestrol (DES) exposure • Unexplained cervico-vaginal discharge • Unexplained abnormal lower genital tract bleeding • History of lower genital tract neoplasia (cervical, vaginal,
vulvar) • Post-treatment surveillance
19

Epithelium of CERVIX
• columnar and • stratified non-keratinising squamous
epithelia. • The squamocolumnar junction,
– most important cytologic and colposcopic landmark,
– over 90% of lower genital tract neoplasia arises.
20

Keratosis or leukoplakia:
21

Keratosis or leukoplakia: white on visual inspection of the cervix prior to the application of acetic acid Microscopy - hyperkeratotic or parakeratotic surface. Located within or outside of the transformation zone, keratotic lesions are raised and bright white. Leukoplakia -nonspecific - secondary to:• trauma such as with diaghram or pessary use,• human papilloma virus infection or • even invasive keratinizing squamous carcinoma.
Biopsy is necessary to establish the exact diagnosis.
22

Erosions and Ulcers:
23

Erosions and Ulcers:
EROSION arises from denuded epithelium which exposes the underlying stroma.ULCERS are deeper and involve the underlying cervical stroma. They may be secondary to trauma, such as insertion of a speculum or from tampon use. The edges of traumatic erosions are sharp and consist of normal epithelium. High grade neoplastic lesions are easily removed and may appear as a erosions with a peeling, rolled back margins of markedly atypical epithelium. Ulcerations may also result from infectious agents such as herpes virus. The base of the infectious ulcer is necrotic and contains inflammatory debris. Concern always exists that the ulceration is secondary to an underlying invasive neoplasm.
Biopsy may be necessary, especially with persistent ulcers or erosions.
24

Ectopy:
25
NORMAL FINDING !!!
Leave IT !

Ectopy:
results from eversion of the squamocolumnar junction onto the portio cervix or in rare cases, the vagina. On gross appearance, the everted columnar epithelium appears velvety red and on close inspection the typical villi of the endocervical mucosa are readily apparent. Iodine uptake is negative because columnar epithelium is not glycogenated. Varying stages of squamous metaplasia may be present throughout the surrounding current squamocolumnar junction or as fine acetowhite islands within the endocervical mucosa. Cervical ectopy is most pronounced in adolescence and the first pregnancy when squamous metaplasia is most active. It is also common with the use of oral contraceptives.
It is an entirely normal finding, and does not warrant any kind of diagnostic or therapeutic response.
26

27

Biopsy of ANY abnormally firm or grossly abnormal
lesions of the cervix must be undertaken.
In older women we make conization without prior biopsy.
– we no longer need cervix – and it may be the diagnostics and the treatment at the same
time .
28

29

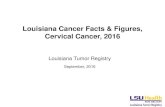
Dysplasia
cervical squamous dysplasia at high magnification extending from the center to the right. The epithelium is normal at the left. Note how the dysplastic cell nuclei are larger and darker, and the dysplastic cells have a disorderly arrangement 30

Dysplasia
31

Stages of dysplasia
32

33

Natural history of cancer
• Cervical dysplasia ~ 28 years
• Carcinoma in situ ~ 35 years
• Carcinoma microinvasivum ~ 40 years
• Carcinoma FIGO IV ~ 60 years
34

THE CANCER
35

This is the gross appearance of a cervical squamous cell carcinoma that is still limited to the cervix
Cervical carcinoma stage I
36

?
37

• This is a larger cervical squamous cell carcinoma which spread to the vagina.
38

Pathology
• Squamous cell carcinoma is the most common histological type of cervical cancer (80%).
• strong association between HPV-16 and HPV-18 and squamous cell carcinoma.
• Usually preceded by LSIL and HSIL
39

Pathology• Adenocarcinoma (9,3%) - second most
common histological type.
• A strong association with HPV-18.
• 50% of adenocarcinomas have associated squamous lesions. (mixed)
• Often located higher in endocervical canal and very focal
• Pap smear - not as sensitive or specific, but can detect glandular lesions.
40

Staging of Cervical Cancer
• "Staging" is a method that has been developed to describe the extent of cancer growth. The stage of cervical cancer describes the tumor's:
• Size
• Depth of penetration within the cervix
• Spread within and beyond the cervix
41

STAGING = clinical stages - FIGO
Staging allows the physician to customize cancer treatment and to predict how a
patient will fare over time.
In general, the lower the stage, the better the person's prognosis
(expected outcome).
42

STAGING – clinical stages
• An interview and physical examination with special care of lymph nodes.
• Gynecological examination – p.v and p.r.
• RTG of chest.
• Basic blood and urine examination.
• Additional tests:USG – p.v & abdominal, Cystoscopy, Rectoscopy,
RTG of skeleton,
CT and MRI – are not taken into consideration
43

Stage 0
• Stage 0 - Carcinoma in situ. Tumor is present only in the epithelium (cells lining the cervix) and has not invaded deeper tissues.
44

Stage I
• Stage I - Invasive cancer with tumor strictly confined to the cervix. – Stage IA - microinvasive ca. Diagnosed only by
microscopic examination of material.– Stage IA1 - depth of invasion up to 3 mm from base
membrane, diameter to 7 mm.– Stage IA2 - depth of invasion up to 5 mm from base
membrane, diameter exceeds 7 mm– Stage IB - all of the changes bigger than in Ia2 visible
or not– Stage IB1 - clinically visible ≤ 4 cm– Stage IB2 - clinically visible ≥ 4 cm
45