Cerebral Siderosis: A Complication of Anticoagulant Therapy? · 2014. 4. 7. · diagnosis of...
3
Cerebral Siderosis: A Complication of Anticoagulant Therapy? N. M. deSouza, J.4 T. C. S. Cox, 1 R. D. Hoare, 2 and C. R. A. Clarke 3 Summary: The authors report a case of cerebral siderosis, a rare disease that generally follows multiple small episodes of subarachnoid hemorrhage from any source, following long-term anticoagulation and minor head injury, and document the fea- tures on MR, which demonstrates characteristic hypointensity in the meninges on T2-weighted scans. Index terms: Subarachnoid space, hemorrhage; Anticoagulants; Brain, magnetic resonance Superficial siderosis first became recognized as a clinicopathologic entity following the reports of Lewey and Govons in the early 1940s. The etiol- ogy is generally accepted to be multiple small episodes of subarachnoid hemorrhage from any source (1 ,2). It is rare: we found approximately 50 cases in the literature . A source of bleeding has been found only in one-half of postmortem cases and was usually a tumor or vascular mal- formation ( 1 ). In the elderly its presence may indicate chronic hemorrhage secondary to amy- loid angiopathy (Jahre C, paper presented at ASNR meeting, June 1991). We are not aware of any reported cases of cerebral siderosis associ- ated with long-term anticoagulation and , there- fore , describe such a case. Case Report A 55-year-old woman presented with headache and vomiting. She had suffered a recent fall and had sustained a minor head injury. A co mput ed tomography (CT) scan w as n orma l. Five years previously she had under go ne two corona ry ar tery bypass operations and had been since then on long-term anti coagu lant s and on a sm all dose of pred- nisolone fo r postcardiotomy sy ndrome. Four months later, she re-presented afte r another fa ll from whi ch she sustained a fractured fe mur . Thi s was fo ll owed by a period of poor anticoagulant co ntrol and a massive bleed into the thigh. At this time, she appeared sleepy on exam ination and had signs of a Parinaud syn- drome. A repeat CT scan was reported as normal. Received April 24, 1992; accepted after revision August 4. 1 Department of Radiology, Guy's Hospit al, London, UK. 2 Department of Magnetic Resonance, Th e Churchill Clinic, London, UK. Tw o months later , she was admitted to the emergency department , sleepy and irritabl e with eye signs as before, neck stiffness , an ex trapyramidal syndrome, and upgoing plantars . Th e international normalized ratio was 2.5. An- ot her CT scan showed blood around the hemispheres and in the cisterns. The anticoagulant therapy was stopped. Selective carotid angiography 4 days later showed normal ca rotid and intracerebral vessels but blocked subclavian arteries bilat erally with reversal of flow down th e verterbral art eries. A lumbar puncture yielded xanthrochromic cere- brospinal fluid at normal pressure. Magnetic resonance (MR) imaging was performed at th e Churchill Clinic. Using a 1 .5- T magnet , proton density and T2-weighted axial and co ronal images and T1-weighted sagittal images were ob- tained. The T1-weighted images were normal. The T2- weighted images showed hypoint ensit y due to hemosiderin deposition around th e middle cerebral artery (Figs. 1 and 2), in th e sylvian fissur es (Figs. 2-4), in the interhemispheri c fissure (Fig. 3), on the undersurfaces of the frontal lobes, and around the temporal poles (Fig. 2), as well as around th e midbrain , pons , and medulla and in the walls of the int erpeduncular cistern (Figs. 3 and 4). Th e ventricular system was normal. There was no sign of any vascular lesion in relation to the circle of Willi s. There was a small left frontal subdural hematoma . Over th e next month , she gradually improved. A CT scan showed slightly enlarged ventricles. She was dis- charged on dex am et hasone 1.5 mg four times a day. Four mo nths later, she had mad e a complete recov ery . Discussion Extracellular deposition of hemosiderin in the leptomeninges is a rare neuropathologic entity thought to result from multiple episodes of chronic subarachnoid hemorrhage of several years' duration (1). Symptoms are caused by the deposition of iron- co ntaining pigments in the cen- tral nervous system (2) resulting in gliosis and neuronal loss. The cardinal feature is the finding of xanthochromic viscous cerebrospinal fluid rich in protein on repeated lumbar punctures. 3 Department of Neurology and Neuros urgery, London Bridge Hospital, London, UK. 4 Addr ess reprint requests to Dr N. deSouza , Department of Radiology , Guys Hospital, St. Thoma s· St. , London SE 1 9RT, UK. AJNR 14:77 4- 776, May/ June 1993 0 1 95-6 I 08 / 93/ 1403-077 4 © American Society of Neuroradiology 774
Transcript of Cerebral Siderosis: A Complication of Anticoagulant Therapy? · 2014. 4. 7. · diagnosis of...

Cerebral Siderosis: A Complication of Anticoagulant Therapy?
N. M . deSouza , J.4 T. C. S. Cox, 1 R. D. Hoare,2 and C. R. A. Clarke3
Summary: The authors report a case of cerebral siderosis, a rare disease that generally follows multiple small episodes of subarachnoid hemorrhage from any source, following long-term anticoagulation and minor head injury, and document the features on MR, which demonstrates characteristic hypointensity in the meninges on T2-weighted scans.
Index terms: Subarachnoid space, hemorrhage; Anticoagulants; Brain, magnetic resonance
Superficial siderosis first became recognized as a clinicopathologic entity following the reports of Lewey and Govons in the early 1940s. The etiology is generally accepted to be multiple small episodes of subarachnoid hemorrhage from any source (1 ,2) . It is rare: we found approximately 50 cases in the literature. A source of bleeding has been found only in one-half of postmortem cases and was usually a tumor or vascular malformation ( 1 ). In the elderly its presence may indicate chronic hemorrhage secondary to amyloid angiopathy (Jahre C, paper presented at ASNR meeting, June 1991). We are not aware of any reported cases of cerebral siderosis associated with long-term anticoagulation and , therefore, describe such a case.
Case Report
A 55-year-old woman presented with headache and vomiting. She had suffered a recent fall and had sustained a minor head injury. A computed tomography (CT) scan was normal. Five years previously she had undergone two corona ry artery bypass opera tions and had been since then on long-term anticoagu lants and on a sm all dose of prednisolone for postcardiotomy syndrome.
Four months later, she re-presented after another fa ll from which she sustained a fractured femur. This was followed by a period of poor anticoagulant contro l and a massive bleed into the thigh. At this time, she appeared sleepy on examination and had signs of a Parinaud syndrome. A repeat CT scan was reported as normal.
Received April 24, 1992; accepted after revision August 4. 1 Department o f Radiology, Guy 's Hospital, London , UK. 2 Department of Magnetic Resonance, The Churchill Clinic, London, UK .
Two months later, she was admitted to the emergency department, sleepy and irritable with eye signs as before, neck stiffness, an extrapyramidal syndrome, and upgoing plantars. The international normalized ratio was 2.5 . Another CT scan showed blood around the hemispheres and in the cisterns. The anticoagulant therapy was stopped. Selective carotid angiography 4 days later showed normal carotid and intracerebral vessels but blocked subclavian arteries bilaterally with reversal of flow down the verterbral arteries. A lumbar puncture yielded xanthrochromic cerebrospinal fluid at normal pressure. Magnetic resonance (MR) imaging was performed at the Churchill Clinic. Using a 1 .5-T magnet, proton density and T2-weighted axial and coronal images and T1-weighted sagittal images were obtained. The T1-weighted images were normal. The T2-weighted images showed hypointensity due to hemosiderin deposition around the middle cerebral artery (Figs. 1 and 2), in the sylvian fissures (Figs. 2-4) , in the interhemispheric fissure (Fig. 3), on the undersurfaces of the frontal lobes, and around the temporal poles (Fig. 2) , as well as around the midbrain , pons, and medulla and in the walls of the interpeduncular cistern (Figs. 3 and 4). The ventricular system was normal. There was no sign of any vascular lesion in relation to the circle of Willi s. There was a small left frontal subdural hematoma.
Over the next month , she gradually improved. A CT scan showed slightly enlarged ventricles. She was discharged on dexam ethasone 1.5 mg four times a day. Four months later, she had made a complete recovery .
Discussion
Extracellular deposition of hemosiderin in the leptomeninges is a rare neuropathologic entity thought to result from multiple episodes of chronic subarachnoid hemorrhage of several years' duration (1). Symptoms are caused by the deposition of iron-containing pigments in the central nervous system (2) resulting in gliosis and neuronal loss. The cardinal feature is the finding of xanthochromic viscous cerebrospinal fluid rich in protein on repeated lumbar punctures.
3 Department of Neurology and Neurosurgery, London Bridge Hospital, London, UK. 4 Address reprint requests to Dr N. deSouza , Department of Radiology, Guys Hospital, St. Thomas· St. , London SE 1 9RT, UK.
AJNR 14:77 4- 776, May/ June 1993 0 195-6 I 08/ 93/ 1403-077 4 © A merican Society of Neuroradiology
774

AJNR: 14, May/ June 1993
2
3 4
The clinical picture in superficial siderosis is quite variable, but one or more of the following clinical signs are usually present: cerebellar ataxia, dementia, nerve deafness, and spasticity. The dementia, if present, occurs in the terminal stage of the disease as a result of necrosis of the cortex due to hemosiderosis. Koeppen and Dentinger (2) observed that minor degrees of subpial hemosiderosis are not infrequent but do not give
CEREBRAL SIDEROSIS 775
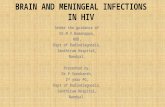
Fig. 1. Axia l spin-echo proton density image (3 .2/ 17 (TR/ TE)) showing hypointensity around the middle cerebral artery (arrows) .
Fig. 2. Ax ial spin-echo T2-weighted image (3 .2/ 90) showing hypointensity around the middle cerebral artery branches in the sylvian fissures (curved arrow) and on the under su rfaces of the frontal lobes and around the temporal poles (straight arrows).
Fig . 3. Coronal spin-echo proton density image (2.5/ 17) showing hypointensity in the sy lvian fissures, in the interhemispheric fissure, in the hippocampal fissures (short arrows) , and around the midbrain , pons, and medulla (open arrows).
Fig. 4. Coronal spin-echo T2-weighted image (2.5/ 90) showing hypointensity in the sylvian fissures and hippocampal and choroidal fissures (long arrows) , in the walls of the interpeduncular c istern (open arrow), and around the midbrian, pons, and medulla (short arrows).
rise to cerebellar ataxia , eighth nerve deafness, or myelopathy , which are the clinical features of the more severe cases. Our patient did not exhibit the classical signs but had an atypical eye movement disorder and parkinsonism.
Antemortem diagnosis has been virtually impossible in the past. However, in the appropriate clinical setting, postcontrast meningeal enhancement on CT may be useful in suggesting the

776 DESOUZA
diagnosis of superficial siderosis (3). Meningeal enhancement is thought to be caused by in- · creased vascular permeability or increased vascularity associated with subsequent arachnoiditis. On MR , hypointensity related to the meninges on T2-weighted images has been observed (4). On the proton density and T2-weighted images in our case there was hypointensity due to hemosiderin mainly at the base of the brain, in the sylvian fissures, and in the ependyma of the fourth ventricle. This distribution of the marginal T2-weighted hypointensity is characteristic for superficial siderosis (2) and is confirmed microscopically in autopsy specimens of young boxers (5), where iron staining of the meninges is seen in brains with naked-eye evidence of previous hemorrhage. Also subependymal deposits of hemosiderin may be observed if the source of the bleeding is intraventricular (2) . Microscopically , there are accumulations of hemosiderin-filled macrophages and fibroblasts w ith a small component due to very fine iron positive particles in astrocytes (2).
Anticoagulant-related subarachnoid hemorrhage is rare and in one series of 76 anticoagulantrelated intracranial extracerebral hemorrhages only seven (1 0 % ) were in the subarachnoid space (6) . In two of these, angiography revealed a bleeding aneurysm, while in the other five , no predisposing factor other than anticoagulation was found . Most patients (42 % ) had been anticoagulated for more than 3 years and only 7 % of intracranial bleeds occurred within 2 weeks of the start of anticoagulants. Our patient had been on warfarin for 5 years prior to presentation. Prothrombin time value does not appear to affect either the course or the severity of the hemorrhage (8) and, at the time of initial presentation , our patient's international normalized ratio was in the desired therapeutic range.
Subarachnoid hemorrhage following trauma (eg, head injury, birth trauma, and violent shaking) is a well- recognized and commonly described entity . Indeed, blunt cranial trauma in an experim ental model was shown to cause subarachnoid
AJNR : 14, May/June 1993
hemorrhage in 100% of cases (7) . In acute severe head injury , traumatic subarachnoid hemorrhage is a frequent occurrence and one large series puts its incidence at 23% (8) . It is likely that the initial minor head injury in our case and the subsequent fall may have predisposed the patient to subclinical bleeding into the subarachnoid space.
Conclusion
Routine long-term anticoagulation rarely causes chronic subarachnoid hemorrhage leading to cerebral siderosis. In the case described, there seems to be little doubt that anticoagulant therapy was the cause of subarachnoid hemorrhage that led to cerebral siderosis, but it is also highly possible that the two traumatic episodes played an etiologic role. The MR appearances with hypointensity related to the meninges are quite characteristic in the distribution of the lesions and the T2-weighted images are vital in making the diagnosis.
References
1. Hughes JT, Oppenheimer DR. Superficial siderosis of the central
nervous system: a report on nine cases with autopsy. Acta Neuro
patho/ (Berl) 1969; 13:56-74
2. Koeppen AHW, Dentinger MP. Brain haemosiderin and superfic ial
siderosis of the central nervous system. J Neuropathol Exp Neurol 1988;47:249-270
3. Pinkston JW, Ballinger WE Jr, Lotz PR, Friedman WA. Superficia l
siderosis: a cause of leptomeningeal enhancement on computed
tomography. J Comput Assist Tomogr 1983;7: 1073- 1076
4. Gomori JM, Grossman Rl , Bilan iuk L T , Zimmerman RA, Goldberg HI.
High field MR imaging of superficial siderosis of the central nervous
system. J Comput Assist Tomogr 1985;9:972- 975. 5. Adams CWM, Bru ton CJ. The cerebral vasculature in dementia
pugil istica. J Neurol Neurosurg Psychiatry 1989;52:600-604
6. Mattei H, Kohler S, Huber P, Rohner M , Steinsieppe KF. Anticoagulant
related intracranial extracerebral haemorrhage. J Neurol Neurosurg
Psychiatry 1989;52:829-837
7. Tornheim PA, Liwnicz BH, Hirsch CH, Brown DL, Mcl aurin RL. Acute
responses to blunt head trauma: experimenta l model and gross
pathology. J Neurosurg 1983;59:431-438
8. Kobayashi S, Nakazawa S, Yokota H, Jsayama K, Vane M, Otsuka T. T rauma tic subarachnoid haemorrhage in acute severe head injury.
No To Shinkei (Japan) 1988;40: 1131- 1135