Cerebral Monitoring after Asphyxia: Tissue Oxygenation and Cerebral Blood Flow
description

POLYTECHNIC COLLEGE OF DAVAO DEL SUR MacArthur Highway, Digoc City
A CASE STUDY OF Status Post Craniectomy
IN PARTIAL FULFILLMENTOF THE REQUIREMENTS IN
RLE/NCM 102
Presented to Ms. Mary Jane Sulla, RN
Presented by
Radee King R. Corpuz
January, 2009

INTRODUCTION
The brain is enclosed in the skull, which is a rigid, solid bone. Surrounding the brain is a tough, leathery outer covering called the dura (door-uh). The dura attaches to the brain, just beneath the skull bone. The dura normally protects the brain and keeps it nourished with blood and spinal fluid. When a person receives a severe blow to the head, the brain bounces within the cavity.
This movement of the brain structures may cause shearing or tearing of the blood vessels surrounding the brain and dura. When the blood vessels tear, blood accumulates within the space between the dura and the skull. This is known as an epidural hematoma (epi-door-ul hem-a-to-ma), or blood clot at the covering of the brain.
When the blood accumulates between the dura and skull, swelling of the brain occurs. There is no extra room within the skull to allow for the brain to swell and for the blood to accumulate. The only way the brain can compensate is to shift the delicate structures out of the way. This can cause pressure on vital functions, such as eye opening, speech, level of awakeness (or consciousness) or even breathing. Generally, an epidural can cause serious problems and must be removed to prevent increased swelling of the brain. The procedure of choice for removal of an epidural hematoma is surgery to remove the blood clot.
An epidural hematoma can happen to anyone, at any age. Some common causes of epidural hematoma include:
A blow to the head, such as in a motor vehicle crash, assault or bicycle accident, falling down and striking the head and people at particular risk are those who, are elderly and have trouble walking or fall often, take a blood thinner, such as Coumadin
Epidural hematomas may occur in combination with subdural hematomas, or either may occur alone. CT scans reveal subdural or epidural hematomas in 20% of unconscious patients.
In the hallmark of epidural hematoma, patients may regain consciousness during what is called a lucid interval, only to descend suddenly and rapidly into unconsciousness later. The lucid interval, which depends on the extent of the injury, is a key to diagnosing epidural hemorrhage. If the patient is not treated with prompt surgical intervention, death is likely to follow.
Brain damage caused by head injury can have dramatic consequences for those affected; it has been reported in prospective studies that children with a history of CET suffer from twice as many psychiatric and cognitive disorders as controls (2). It has also been reported that CET patients, in particular very serious cases, make normal personality development more difficult, leaving people with serious deficits in areas such as introspection, planning, social judgment, emotional control, empathy and reasoning (3).

In the industrialized countries, physical injury and in particular cranioencephalic trauma (CET), is a significant clinical and social problem of epidemic proportion. According to Kraus (1), epidemiological studies on this pathology are incomplete, since none of them groups all CET patients within a defined population; however, in general it is considered that the annual incidence in the developed countries is from 200 to 300 per 100,000 inhabitants. In the different epidemiological studies, it has been found that the percentages of affected patients of pediatric age is around 20%; the accidents are mainly car crashes and sports falls (bicycles, skate-boards ...) involving a bang on the head in movement on a static surface.

IDENTIFICATION OF THE CASE
A. PERSONAL PROFILE
Name : Lady L.
Address : Asbang, Matanao, Digos, Davao del Sur
Age : 13y/o
Gender : female
Civil status : single
Birth date :
Occupation :helper
Admitting Doctor : Dr. Armando
Admitting Diagnosis : vehicular accident
Religion: Baptist
Nationality: Filipino
Educational Attainment: Grade 6
Father’s name: Mr. E
Occupation: Farmer
Mother’s name: Mrs. V
Occupation: Housewife
Date of admission: January 6, 2009
B. Background/History
DM HPN CA ASTHMA
Maternal
Paternal

C. Medical History
The patient had her complete immunization. According to her
father, she had never been hospitalized. Though she had some fever on
her younger years, hospitalization was not an option for her parents. They
usually use “haplas” and any other herbal medicines for treatment.
D. History of Present Illness
Few minutes prior to admission, the patient was hit by a private
vehicle while riding on a bicycle and was referred to this institution (Davao
Medical Center) for STAT craniectomy.
E. Socio-economic background
Patient L, the eldest of the five siblings was a helper in Digos City.
She has an income of Php. 1000/month which she uses to send herself to
school. Her father works as farmer on a land owned by their neighbor,
while her mother only stays at home taking care of the children.

DEFINITION OF TERMS
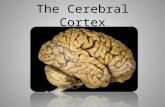
Cerebrum or telencephalon – together with the diencephalon, constitute the forebrain. It is the most anterior or, especially in humans, most superior region of the vertebrate central nervous system. "Telencephalon" refers to the embryonic structure, from which the mature "cerebrum" develops. The dorsal telencephalon, or pallium, develops into the cerebral cortex, and the ventral telencephalon, or subpallium, becomes the basal ganglia. The cerebrum is also divided into symmetric left and right cerebral hemispheres
CerebralConcussion – from the Latin concutere ("to shake violently"),[1] is the most common type of traumatic brain injury. The terms mild brain injury, mild traumatic brain injury (MTBI), mild head injury (MHI), and minor head trauma and concussion may be used interchangeably, although the latter is often treated as a narrower category. The term 'concussion' has been used for centuries and is still commonly used in sports medicine, while 'MTBI' is a technical term used more commonly nowadays in general medical contexts. Frequently defined as a head injury with a transient loss of brain function, concussion can cause a variety of physical, cognitive, and emotional symptoms.
Craniectomy – is a neurosurgical procedure in which part of the skull is removed to allow a swelling brain room to expand without being squeezed. It is performed on victims of traumatic brain injury and stroke. Use of the surgery is controversial.[1] Though the procedure is considered a last resort, some evidence suggests that it does improve outcomes by lowering intracranial pressure (ICP), the pressure within the skull.
Epidural hematoma (EDH) occurs outside the brain and is usually caused by a damaged artery. Arteries carry blood under high pressure; therefore, a large EDH can cause pressure to build up within minutes, even seconds. This condition requires immediate surgery to relieve pressure and prevent severe permanent damage or death
Glasgow Coma Scale or GCS – is a neurological scale which aims to give a reliable, objective way of recording the conscious state of a person, for initial as well as continuing assessment. A patient is assessed against the criteria of the scale, and the resulting points give a patient score between 3 (indicating deep unconsciousness) and either 14 (original scale) or 15 (the more widely used modified or revised scale).

ANATOMY AND PHYSIOLOGY
The cerebrum consists of two cerebral hemispheres connected by a bundle of
nerve fibers, the corpus callosum. The largest and most visible part of the brain, the

cerebrum, appears as folded ridges and grooves, called convolutions. The following
terms are used to describe the convolutions:
A gyrus (plural, gyri) is an elevated ridge among the convolutions.
A sulcus (plural, sulci) is a shallow groove among the convolutions.
A fissure is a deep groove among the convolutions.
The deeper fissures divide the cerebrum into five lobes (most named after bordering
skull bones)—the frontal lobe, the parietal love, the temporal lobe, the occipital lobe,
and the insula. All but the insula are visible from the outside surface of the brain.
A cross section of the cerebrum shows three distinct layers of nervous tissue:
The cerebral cortex is a thin outer layer of gray matter. Such activities as
speech, evaluation of stimuli, conscious thinking, and control of skeletal
muscles occur here. These activities are grouped into motor areas, sensory
areas, and association areas.
The cerebral white matter underlies the cerebral cortex. It contains mostly
myelinated axons that connect cerebral hemispheres (association fibers),
connect gyri within hemispheres (commissural fibers), or connect the cerebrum
to the spinal cord (projection fibers). The corpus callosum is a major
assemblage of association fibers that forms a nerve tract that connects the two
cerebral hemispheres.
Basal ganglia (basal nuclei) are several pockets of gray matter located deep
inside the cerebral white matter. The major regions in the basal ganglia—the
caudate nuclei, the putamen, and the globus pallidus—are involved in relaying
and modifying nerve impulses passing from the cerebral cortex to the spinal
cord. Arm swinging while walking, for example, is controlled here.
The diencephalon connects the cerebrum to the brain stem. It consists of the
following major regions:
The thalamus is a relay station for sensory nerve impulses traveling from the
spinal cord to the cerebrum. Some nerve impulses are sorted and grouped here
before being transmitted to the cerebrum. Certain sensations, such as pain,
pressure, and temperature, are evaluated here also.

The epithalamus contains the pineal gland. The pineal gland secretes
melatonin, a hormone that helps regulate the biological clock (sleep-wake
cycles).
The hypothalamus regulates numerous important body activities. It controls
the autonomic nervous system and regulates emotion, behavior, hunger, thirst,
body temperature, and the biological clock. It also produces two hormones
(ADH and oxytocin) and various releasing hormones that control hormone
production in the anterior pituitary gland.
The following structures are either included or associated with the hypothalamus.
The mammillary bodies relay sensations of smell.
The infundibulum connects the pituitary gland to the hypothalamus.
The optic chiasma passes between the hypothalamus and the pituitary gland.
Here, portions of the optic nerve from each eye cross over to the cerebral
hemisphere on the opposite side of the brain.
The brain stem connects the diencephalon to the spinal cord. The brain stem
resembles the spinal cord in that both consist of white matter fiber tracts surrounding
a core of gray matter. The brain stem consists of the following four regions, all of
which provide connections between various parts of the brain and between the brain
and the spinal cord.

The midbrain is the uppermost part of the brain stem.
The pons is the bulging region in the middle of the brain stem.
The medulla oblongata (medulla) is the lower portion of the brain stem that
merges with the spinal cord at the foramen magnum.
The reticular formation consists of small clusters of gray matter interspersed
within the white matter of the brain stem and certain regions of the spinal cord,
diencephalon, and cerebellum. The reticular activation system (RAS), one
component of the reticular formation, is responsible for maintaining
wakefulness and alertness and for filtering out unimportant sensory information.
Other components of the reticular formation are responsible for maintaining
muscle tone and regulating visceral motor muscles.
The cerebellum consists of a central region, the vermis, and two winglike lobes, the
cerebellar hemispheres. Like that of the cerebrum, the surface of the cerebellum is
convoluted, but the gyri, called folia, are parallel and give a pleated appearance. The

cerebellum evaluates and coordinates motor movements by comparing actual skeletal
movements to the movement that was intended.
The limbic system is a network of neurons that extends over a wide range of areas of the
brain. The limbic system imposes an emotional aspect to behaviors, experiences, and
memories. Emotions such as pleasure, fear, anger, sorrow, and affection are imparted to
events and experiences. The limbic system accomplishes this by a system of fiber tracts
(white matter) and gray matter that pervades the diencephalon and encircles the inside
border of the cerebrum. The following components are included:
The hippocampus (located in the cerebral hemisphere)
The denate gyrus (located in cerebral hemisphere)
The amygdala (amygdaloid body) (an almond-shaped body associated with the
caudate nucleus of the basal ganglia)
The mammillary bodies (in the hypothalamus)
The anterior thalamic nuclei (in the thalamus)
The fornix (a bundle of fiber tracts that links components of the limbic system)

ETIOLOGY AND SYMPTOMATOLOGY
Etiology
Ideal Actual JustificationLocation (+) The location varies a lot in incidence
number of the Vehicular Accident. Those people who live nearby from the highways are more prone to those people that are away from the highway. In our pt, their house is near the highway.
Weather (+) Weather does also have a large effect of most vehicular accident such as rain which may interferes or blocks the visualization of those who are involve.
Age (+) Younger ones have lots of playtime than the old ones making them more at risk in any form of Accidents.
Symptomatology
Ideal Actual Justificationdizziness (+) -Pt. manifested
Lightheadedness or dizziness because dizziness happens when there is not enough blood getting to the brain. This can happen if there is a sudden drop in your blood pressure
Confusion (+) -because of Low levels of oxygen, Concussion, Fever Fluid and electrolyte imbalance, Head trauma or head injury or a sudden drop of temperature
Different Size Pupils (+) -due to bleeding inside the skull caused by head injury
Shock(+)
- because of Low blood volume secondary to bleeding

COMPLICATION
Post-Concussion Syndrome
Post-concussion syndrome (PCS) is a common but controversial disorder that presents with variety of symptoms including- but not limited to- headache, dizziness, fatigue, and personality changes. PCS occurs in approximately 23-93% of persons with mild to severe head injuries.
Seizure
A seizure is a sudden change in behavior characterized by changes in sensory perception (sense of feeling) or motor activity (movement) due to an abnormal firing of nerve cells in the brain. Epilepsy is a condition characterized by recurrent seizures that may include repetitive muscle jerking called convulsions
Infectionis the detrimental colonization of a host organism by a foreign species. In
an infection, the infecting organism seeks to utilize the host's resources to multiply (usually at the expense of the host). The infecting organism, or pathogen, interferes with the normal functioning of the host and can lead to chronic wounds, gangrene, loss of an infected limb, and even death
Chronic Head Injuriesoccurs when an outside force traumatically injures the brain. TBI can be
classified based on severity (mild, moderate, or severe), mechanism (closed or penetrating head injury), or other features (e.g. occurring in a specific location or over a widespread area). Head injury usually refers to TBI, but is a broader category because it can involve damage to structures other than the brain, such as the scalp and skull.

PATHOPHYSIOLOGY
Epidural Hematoma is acquired through many causes. One of these
causes is the vehicular accident because during a vehicular accident, one’s head
maybe injured.
Predisposing factorsAgeAccident prone area
Vehicular Accident
Precipitating factorsWorkAwarenessType(s) of vehicle
Head Injury
Skull fracture
Rupture or laceration of theMiddle meningeal artery
HEMORRHAGE
Blood collect in the epiduralSpace between the skull and dura
Epidural HematomaInc. ICP
S/Sx* momentary loss of
ConsciousnessInterval apparent
Recovery or lucid recovery
CRANIECTOMY
Good prognosis

After a head injury, blood may collect in the epidural space between the
skull and the dura. This can result from a skull fracture that causes a rupture or
laceration of the middle meningeal artery, the artery that runs between the dura
and the skull inferior to a thin portion of temporal bone. Hemorrhage from this
artery causes rapid pressure on the brain.
Symptoms are caused by the expanding hematoma. Usually, a
momentary loss of consiousness occurs at the time of injury, followed by an
interval apparent recovery. Although the lucid interval is considered a classic
characteristics of an epidural hematoma, no lucid interval has been reported in
many patients with this lesion and therefore it should not be considered a critical
defining criterion.
An epidural hematoma is considered an extreme emergency; marked
neurologic deficit or even respiratory arrest can occur within minutes. Treatment
consists of making openings through the skull (burr holes) to decrease ICP
emergently, remove the clot, and control the bleeding. A craniotomy may be
required to remove the clot and control the bleeding. A drain is usually inserted
after creation of burr holes or a craniotomy to prevent reaccumulation of blood
But on the other hand, if treatment is being applied, there is great chance
of recovery through what we so call surgery and to be more specific, the
procedure called craniectomy. Craniectomy is a neurosurgical procedure in
which part of the skull is removed to allow a swelling brain room to expand
without being squeezed. Through this procedure the Increase intracranial
Pressure due to pain will be relieve or be lowered because increase intracranial
pressure is very fatal to the brain since it compresses the brain and restricted the
cerebral blood flow. When surgery is being done, it is still very important to follow
any medication being prescribe t him by the doctor. If this medical management
will be done to the patient correctly, it is pretty sure that the recovery of the
patient will be great and fast and the most desirable thing that everyone who’s
sick would like to have, TOTAL RECOVERY or BEING WEL

MEDICAL MANAGEMENT
01/06/09
Referred to Dr. Armando
8:30am For repeat cranial CT scan STAT Monitor NVS every hour and record Refer
01/07/0910:30am
NPO Start Ranitidine 50mg IVTT every 8 hours Shave full head Refer
01/08/09
May have DAT Continue medz Continue IVF: PLR 1L to run at 130cc/hr D/C PNSS D/C omepirazole Open dressing Keep Jackson’s Pratt drain in negative
5:55pm D/C all medz Change dressing Refer
01/09/095:30
DAT Continue medz Change dressing Keep Jackson’s Pratt Drain in negative Full body bath Remove FBC
01/10/09
DAT with SAP ROM:
Laboratory

Test ResultNormal Values
Clinical Significance
Remarks
CBC Hemoglobin – 142
115-155 -normal range-
Hematocrit – 0.41
0.30-0.48 Normal volume of Red Blood Cells
-normal range-
RBC – 5.00 4.20-6.10 Adequate number of Red Blood Cell primarily to ferry oxygen in blood to all cells of the body
-normal range
WBC – H 13.77
5.0-10.0 Infection, leukemia, tissue necrosis
-increased-
Neutrophil – 90
55-75 Infection, ischemic neurosis, metabolic d/o acute gout
-increased-
Lymphocytes – L4
0.2-.35 TB, hepatitis, infectious mononucleosis, mumps, rubella, lymphocytic leukemia
-increased-
Monocytes – 6
2-10 -normal range-
Eosinophil – L0
1-8 Cushings’s syn. -decresed-
Basophil – 0 0-1 -normal range-Platelet – 257x10^3/uL
150-400
Glucose-RBS – 5.4
3.90-6.8 -normal range-
Creatinine – L27.00 Umol/L
53.00-115.00 Kidney dysfunction -decreased-
CT-scan(+)Epidural hematoma, Right parietotemporal convixities

NURSING ASSESSMENT
B. Physical Assessment
Assessment Normal Findings Yes No
Body Build,
Height and
Weight
Proportionate, varies with
lifestyle
Posture and Gait Clean, neat
Body and Breath
odor
No body or breath odor
Signs of Distress No distress noted
Signs of Health
or Illness
Healthy appearance
Attitude Cooperative
Affect/Mood Appropriate to situation
Quantity, Quality
and Organization
of Speech
Understandable,
moderate pace, exhibits
thought association
Relevance and
Organization of
Thoughts
Logical sequence, makes
sense, has sense of reality

Assessment Normal Findings Yes Poor
Uniformity of
skin color
Uniformity except in
areas exposed to the sun
Edema No edema
Skin Lesions No freckles, No
birthmarks, no abrasions
or lesions
Skin Moisture Moisture in skin folds
and the axillae
Skin
Temperature
Uniform, within normal
range
Skin Turgor Skin springs back to
previous state when
pinched
Assessment Normal Findings Yes No
Scalp Evenly distributed
Hair Thickness Thick hair
Hair Texture Silky, resilient hair
Amount of Body
Hair
Variable
Assessment Normal Findings Yes No

Nail Plate Shape Convex curvature
Texture Smooth
Nail Bed Color Highly vascular, pink,
prompt return of pink
color
Assessme
nt
Normal
Findings
Good Fair Poor
A. Skull and Face
Head Rounded,
symmetrical,
smooth skull
contour, no
nodule
B. Eyes and Vision
Eyebrows Hair evenly
distributed,
symmetrical,
skin intact
Eyelid Skin intact, no
discharges, no
discolorations,
symmetrical
Eyelashes Equally
distributed,
slightly curved
outward
Conjunctiv Transparent,

a sometimes
appear white,
shiny, smooth,
pink or red
Lacrimal
Gland
No edema or
tearing
Cornea Transparent,
shiny and
smooth, blinks
when cornea is
touched
Pupils Black color,
equal size
Near
Vision
Able to read
newsprint
C. Ears and Hearing
Auricles Color is uniform,
symmetric,
mobile, firm,
pinna recoils
when folded
Response
to Normal
Voice
Tone
Normal voice
tone audible
D. Nose and Sinuses
Nares Symmetric and
straight, no
discharges, no
swelling,
uniform color,

not tender
Lining of
nose
Nasal septum in
midline
E. Mouth
Lips
Buccal
Mucosa
Uniform pink,
soft, symmetrical
Teeth and
Gums
Complete child
teeth, smooth,
white tiny tooth
enamel, pink
gums, moist,
firm, no
retractions
Tongue Centrally
located, pink in
color, freely
movable
Palates,
Uvula,
Tonsils
Light pink,
smooth, no
discharges,
present gag
reflex
Assessment Normal Findings Good Fair Poor
Shape and
Symmetry
Symmetrical
Spinal
Deformities
Spine vertically aligned
Assessment Normal Findings Good Fair Poor
Inspect Neck
Muscles
Symmetrical with head
centered
Observe Head
Movement
Coordinated, smooth,
movement with no
discomfort, equal strength

Assessment Normal Findings Good Fair Poor
Muscle Size is symmetrical, no
contracture, normally firm
Movement Smooth coordinated
movements, equal strength
Bones No deformities, no
swelling or tenderness
Joints No swelling, tenderness
Range of motion Varies to some degree

NURSING MANAGEMENT
Ideal
Goal Responsibilities
Maintain Patent Airway Check the orders for and aaply
supplemental Oxygen. Assess RR and
depth, ease of respirations, oxygen
saturation, and breath sounds.
Encourage patient to turn frequently
and take deep breath and cough at
least every two hours.
-Administer pain medication to permit
more effective coughing; suction
patient as needed.
Maintain Cardiovascular stability -Monitor cardiovascular stability by
assessing patients mental status; vital
sings; cardiac rhythm; skin
temperature, color and moisture; and
urine output.
-Assess patency of all intravenous line.
-Assess output from wound drainage
system and amount of bloody drainage
on the surgical dressing frequently.
Mark and time spots of drainage; report

excess drainage or fresh blood to
surgeon immediately.
-Observe the surgical site for bleeding,
type and integrity of dressing , and
drain (eg, Jackson-pratt)
Assessing and Managing pain -Assess pain level using a verbal or
visual analog scale, and assess the
characteristics of the pain.
-Discuss options in pain relief
measures with patient to determine the
best medication. Assess effectiveness
of medication periodically beginning 30
minutes after administration.
-Provide other pain relief measures
(changing patients position, using
distraction, applying cool washcloths to
the face, and rubbing the back with a
soothing lotion) to relieve general
discomfort temporarily.
Maintain normal body temperature -Monitor body system function and vital
sings with temperature every 4 hours
and every shift thereafter.
-Report sings of hypothermia to
physician.
-Maintain the room at a comfortable
temperature, and provide blankets to
prevent chilling.
-Monitor patient for cardiac
dysrhythmias.
-Take efforts to identify malignant

hyperthermia and to treat it early.
Assess mental status -Assess mental status (level of
consciousness, speech, and
orientation) and compare to pre-
operative baseline; change maybe
related to anxiety, pain, medications,
oxygen deficit, or hemorrhage.
-Address source of discomfort, and
report signs of complication for
immediate treatment.
Promote nutrition and fluid balance - Assess patient to return to normal
dietary intake gradually at a pace set
by patient (liquid first then soft foods
such as milk and creamed soak are
added gradually)
-Eat nutritious food and take and
instruct patient to take multivitamins,
Iron and Vitamin C as prescribe.
-Assess potency and intravenous lines,
ensuring that appropriate fluids are
administered at prescribe rate.
-Record intake and output.

HEALTH TEACHINGS
PRIMARY
1. Instruct the patient to have a proper diet that she can tolerate, such as fruits, to help promote wellness.
2. Instruct the patient to have deep breathing exercise, to promote non-pharmacological treatment
3. Advice the patient to have fluid intake or adequate hydration, to help her body re-hydrate to prevent fluid imbalance.
4. Assist patient to perform self-care activities she cannot tolerate, to help her maintain her activities of daily living.
5. Encourage patient to perform self care activities within her level of own ability.
6. Initiate and encourage patient to perform bed exercises to improve circulation ( ROM to arms, hands and fingers, feet and legs; leg flexion and leg lifting; abdominal and gluteal contraction)
7. Ask patient to perform as much as possible and then to call for assistance. Collaborate with patient for progressive activity before and after schedule activity.
SECONDARY
1. Administer medications as ordered by the physician2. Advice patient to have proper nutrition to enhance immune system
TERTIARY
1. Instruct patient to comply for medication regimen2. Discuss the importance of having a regular check-up with his physician

DISCHARGE PLAN
When the doctor noted that the patient is for discharge it is very important
to continue the medication depending on the duration the doctor ordered for the
total recovery of the patient. Patient with epidural hematoma and undergone post
craniectomy needs to have a light exercise such as motor development in both
arms and feet, clear verbalization and spontaneous with the duration of 10-15
minutes and must get enough rest. It is also important to maintain proper hygiene
to prevent further infection that may happen to the patient because she was
undergone surgery; the operated site is very susceptible to any diseases. He
also needs to minimized smoking and drinking alcoholic beverages.
She also need to stop her school because to much exposed to a pressure
and positive atmosphere can be a high risk factor that may cause severity of her
condition. The diet of the patient is also a factor for fast recovery. She is
encourage to eat nutritious foods such as juices that are rich in Vitamin C. the
family of the patient plays a big role for the fast recovery.
Regular consultation to the physician can be factor for recovery to assess
and monitor her condition

PROGNOSIS
Good Fair Poor JustificationDuration of Illness -
Duration of illness is good since the incident was stat and she was given ample treatment.
Onset of Illness
-
The onset is stat since right after the she was diagnosed, she was automatically brought to the Operating room for a stat craniectomy.
Compliance to Medication
-
Patient can afford to sustain the needed laboratory exams and the feasibility of having a surgery.
Family Support -
The family members supported the patient both financially and emotionally.
Environment
-
The hospital setting is not well ventilated and may promote for further infection of the patient’s current situation.
Age - Patient is 13 years old therefore she has a greater chance of recovering for her immune system is still generating in the process of

development.Precipitating Factors
-
The patient manifested all the factors that may lead to epidural hematoma which urged the health care team to bring her for an operation.
EVALUATION
Through our hardship in preparing for this research, tried to interact
and communicate our patient in good manner for us to gather the specific and
accurate data that we need that could help us in studying the disease which
could lead us into successful research.
The patient’s condition is in recovery period as she had already
undergone surgery, which thereby prevented occurrence of complications
They are financially capable in sustaining such surgery and the
medications after. Her father is the one taking good care of her in throughout
her hospitalization.

IMPLICATION
Nursing Practice
- this can be used as a guide for practice by other nurses. They may get many relevant ideas in giving proper care and interventions to patients with related illness or those who have the same illness (Epidural hematoma, Brain Injury)
Nursing Education
- this study may serve as a helpful learning tool for student nurses. They may utilize this complied study as their reference for research; this will also give them good examples on nursing managements, and nursing diagnoses, which will be a very useful guide when they will be making their own Nursing Care Plans.
Nursing Research
- students may use this compilation as their guide for research. This will hand them good views and factual ideas which will be very essential for their added learning an knowledge for Epidural hematoma, Brain Injury

REFERENCES
http://www.neurologychannel.com/tbi/types.shtml
http://en.wikipedia.org/wiki/Cerebrum
http://en.wikipedia.org/wiki/Glascow_Coma_Scale
http://en.wikipedia.org/wiki/Infection
http://www.alasbimnjournal.cl/revistas/8/ceballos.html
http://www.muhealth.org/neuromed/epidural.shtml