Cerebral Atrophy in Infants with Protein Energy · PDF fileCerebral Atrophy in Infants with...
3
434 Cerebral Atrophy in Infants with Protein Energy Malnutrition Samir EI-TatawY ,1 Nadia Badrawi,2 and Amal EI Bishlawy 2 Central nervous system manifestations are common in infants suffering from protein energy malnutrition. Computed tomogra- phy was used to search for pathology in the brain that might explain these symptoms . Subjects were 40 infants with protein malnutrition . All had mental symptoms. The bifrontal index was taken as the best parameter for measuring central atrophy, and the width of the sylvian fissure was used as the parameter for cortical atrophy. Ventricular dilatation and widened sylvian fis- sure of various degrees were found in every patient . The severity of atrophy correlated with the duration of the illness . Protein energy malnutrition is one of the most serious hea lth prob lems in Egypt. It is found predominantly in infant s whose req uirements f or protein have not been met for some time. The age of peak in cidence is 6-30 months [1]. As the human brain grows rapidly from the 11 th week of gestation to the seco nd year of life, malnutrition during this period would be expec ted to impa ir the growt h and fu nct ioning of the brain. Children with prot ein energy malnutrition manifest such sy mpt oms as listlessness, apat hy, irri- tability, weak ness, and in act ivity [2]. The bases for these profound disturbances are co mpl ex and poor ly understood . Computed tomogr ap hy (CT) provides us with a convenient and noninvasive method of exa mining the morphology of the human brain in vivo. We used this technique to searc h for ab norma liti es that might relate to the sy mptoms seen in infant s suffering from protein energy malnutrition. Subjects and Methods Subjects were 40 infants aged 1 2-30 month s with protein energy malnutrition. The dura tion of the disease at the time of the study was 10-70 days. All inf ants had ce ntral nervous system manifes- tations of th e disease (listlessness, apa thy, irritability). Cases were divided into three groups accord ing to the duration of the disease , as follows: group 1, less than 1 month (11 cases); gro up 2, 1- 2 months (10 cases) ; group 3, more than 2 months (19 cases). A fourth group of 10 norma l cont rols was included. All cases were subjec ted to CT head scan using the ACTA 200 FS scanne r at Cairo University Hosp ital. Central atrophy (dilatation of the ventricles) was evaluated by th e bifrontal index (bifrontal diam- eter / tr ansverse diameter of the brain at the same level). Cortical atrophy was evaluated by the width of the sy lvian fissure at its ant eropost er ior diameter. The CT meas ureme nts were scaled to the ac tu al dimensions. Ot her cr it er ia for det ec tion of co rti ca l atr ophy were wide ning of the interhemisphe ri c fissure (6 -11 mm), widening of th e cor ti cal sulci (3-7 mm), and the number of visible cort ical sulci ( 3- 12 / hemisp here). Results Th e results are presented in t ab les 1- 3. Centra l and co rtical atr ophy of various degrees was found in 100% of cases, the severity cor relating with the duration of prot ein deficiency. Re pr esentati ve CT scans of infants suffering from protein energy malnutrition are shown in figur es 1-5. In fo ur cases with severe cortical atrophy, th e atr op hy was loca ll y prominent in the fr ontal region, resulting in an appeara nce identical to localized fro ntal hygroma (fig. 4). These cases had an espec iall y severe clini ca l presentation . Th e bicaudate ind ex (bi caudate diameter / transverse diameter of the brain at the same level) had a mean value of 0.2 (range, 0.15- 0.27 ± 0.03), substantially high er than that of the normal co ntrols (0.14); howeve r, it did not s how signifi ca nt correlation with th e duration of the disease. TABLE 1: Evaluation of Central Atrophy (Dilatation of the Ventricles) by the Bifrontal Index Degree of Atrophy Range Mean Standard Devia- tion Normal <0.28 0.26 0.054 Mild 0 .28-0.32 0.30 0.01 3 Moder ate 0 .33 -0 .37 0.35 0.017 Severe >0 .38 0.41 0.034 Nole .- The bifrontal index is the bifronlal diameter of the brain divided by the transverse diameter at the same level. Values obtained are expressed as ratios. TABLE 2: Evaluation of Cortical Atrophy by the Width of Sylvian Fissure Degree of Atrophy Range (mm) Mean (mm) Standard Devi a- tion (mm) Normal 0- 6 4.7 1.16 Mild ......... . 6-9 7 .8 0.68 Mod erate 9-11 10.4 0.96 Severe > 11 14 .7 2.40 , Department of Radiology, Faculty of Medicine, Cairo University, 166,26 July St., Dokki, Cairo, Egypt. Address reprint reques ts to S. EI -Tatawy. 2 Department of Pediatrics, Faculty of Medicine , Cairo University, Cairo, Egypt. AJNR 4:434-436, May / June 1983 0195-6108 / 83 / 0403-0434 $00.00 © Ameri can Roentgen Ray Society
Transcript of Cerebral Atrophy in Infants with Protein Energy · PDF fileCerebral Atrophy in Infants with...

434
Cerebral Atrophy in Infants with Protein Energy Malnutrition Samir EI-TatawY ,1 Nadia Badrawi,2 and Amal EI Bish lawy2
Central nervous system manifestations are common in infants suffering from protein energy malnutrition. Computed tomography was used to search for pathology in the brain that might explain these symptoms. Subjects were 40 infants with protein malnutrition. All had mental symptoms. The bifrontal index was taken as the best parameter for measuring central atrophy, and the width of the sylvian fissure was used as the parameter for cortical atrophy. Ventricular dilatation and widened sylvian fissure of various degrees were found in every patient. The severity of atrophy correlated with the duration of the illness.
Protein energy malnutrit ion is one of the most serious health problems in Egypt. It is found predominantly in infants whose requirements for protein have not been met for some time. The age of peak inc idence is 6-30 months [1]. As th e human brain grows rapid ly from the 11 th week of gestation to th e second year of life, malnutrition during this period would be expected to impair the growth and fu nctioning of th e brain. Chi ldren with protein energy malnutrition manifest such symptoms as listlessness, apathy , irritability, weakness, and inact ivi ty [2]. The bases for these profound disturbances are complex and poorly understood .
Computed tomography (CT) provides us with a convenient and noninvasive method of examining th e morphology of the human brain in vivo. We used this technique to search for abnormalities that might re late to the symptoms seen in infants suffer ing from protein energy malnutrition.
Subjects and Methods
Subjects were 40 infants aged 12-30 months with protein energy malnutrition. The duration of the disease at the time of the study was 10-70 days. All infants had central nervous system man ifestations of the disease (listlessness, apathy , irritabi lity). Cases were
d ivided into three groups accord ing to the duration of the disease, as follows: group 1, less than 1 month (11 cases); group 2, 1-2 months (10 cases); group 3, more than 2 months (19 cases). A fourth group of 10 normal controls was inc luded.
All cases were subjected to CT head scan using the ACTA 200FS scanner at Cairo University Hospital. Central atrophy (dilatation of the ventricles) was evaluated by the bifrontal index (bifrontal diameter / transverse diameter of the brain at the same level) . Cortical atrophy was evaluated by the width of th e sylvian fissure at its anteroposterior d iameter. The CT measurements were scaled to th e actu al d imensions. Other criteria for detection of corti ca l atrophy
were widening of the interh emispheric fissu re (6-11 mm), widening of th e cortical sulc i (3-7 mm), and the number of visible cortical sulci (3-12 / hemisphere).
Results
Th e results are presented in tables 1-3. Central and corti ca l atrophy of various degrees was found in 100% of cases, the severity correlatin g with the duration of protein deficiency. Representative CT scans of infants suffering from protein energy malnutrition are shown in figures 1-5.
In four cases with severe cortical atrophy, th e atrophy was locally prominent in the frontal reg ion, resu lting in an appearance identical to localized frontal hyg roma (fig . 4). These cases had an especially severe clinica l presentation .
The bicaudate index (bicaudate diameter / transverse diameter of the brain at the same level) had a mean value of 0 .2 (range, 0.15-0.27 ± 0.03), substantially higher than that of the normal controls (0.14); however, it did not show significant correlation with the duration of the disease.
TABLE 1: Evaluation of Central Atrophy (Dilatation of the Ventricles) by the Bifrontal Index
Degree of Atrophy Range Mean Standard Devia-
tion
Normal < 0 .28 0 .26 0.054 Mild 0 .28-0.32 0 .30 0 .01 3 Moderate 0 .33-0.37 0 .35 0 .017 Severe > 0 .38 0.41 0.034
Nole .- The bifrontal index is the bifronlal diameter of the brain divided by the transverse diameter at the same level. Values obtained are expressed as ratios.
TABLE 2: Evaluation of Cortical Atrophy by the Width of Sylvian Fissure
Degree of Atrophy Range (mm) Mean (mm) Standard Devia-
tion (mm)
Normal 0 - 6 4.7 1.16 Mild ......... . 6-9 7 .8 0.68 Moderate 9-11 10.4 0.96 Severe > 11 14.7 2.40
, Department of Radiology, Faculty of Medicine, Cairo University, 166,26 July St. , Dokki, Cairo, Egypt. Address reprint requests to S. EI-Tatawy. 2 Department of Pediatrics, Faculty of Medicine, Cairo Universi ty, Cairo , Egypt.
AJNR 4:434-436, May / June 1983 0195-6108/ 83 / 0403-0434 $00.00 © American Roentgen Ray Society
AJNR:4, May / June 1983 CT OF THE HEAD 435
Discussion
Although mental changes are one of the diagnostic c riteri a in protein energy malnutrition, few studies have examined the underlying pathologic changes in the brains of affected infants. Elec troencephalographic (EEG) stud ies are few. Taori and Pereira [3) found normal EEG readings in a group of 20 pat ients with the disease. Slowing of the electrica l patterns, particularly over the temporal lobes, was reported in acute protein energy malnutrition by Hansen et al. [2). Engsner et al. [4) studied th e cerebral ventric les by sonog raphy and found a sign ificant dilatation of the ventric les in
TABLE 3 : Severity of Cerebral Atrophy Related to Duration of Protein Energy Malnutrition
Durat ion of Illness (days) Type of Atrophy: Severit y
<30 (n = 11) 30-60 (n = 10) >60 (n = 19)
Central : Mild 54 .5 20.0 10.5 Moderate 27.2 60.0 36.9 Severe 18.2 20.0 52 .6
Cortical : Mild 63 .6 10.0 21 .0 Moderate 27.3 50.0 31 .6 Severe 9.1 40.0 47.4
Nole.- The chi-square lest was used for analysis of covariance. Correlat ion values are expressed as percentages (p < 0.05).
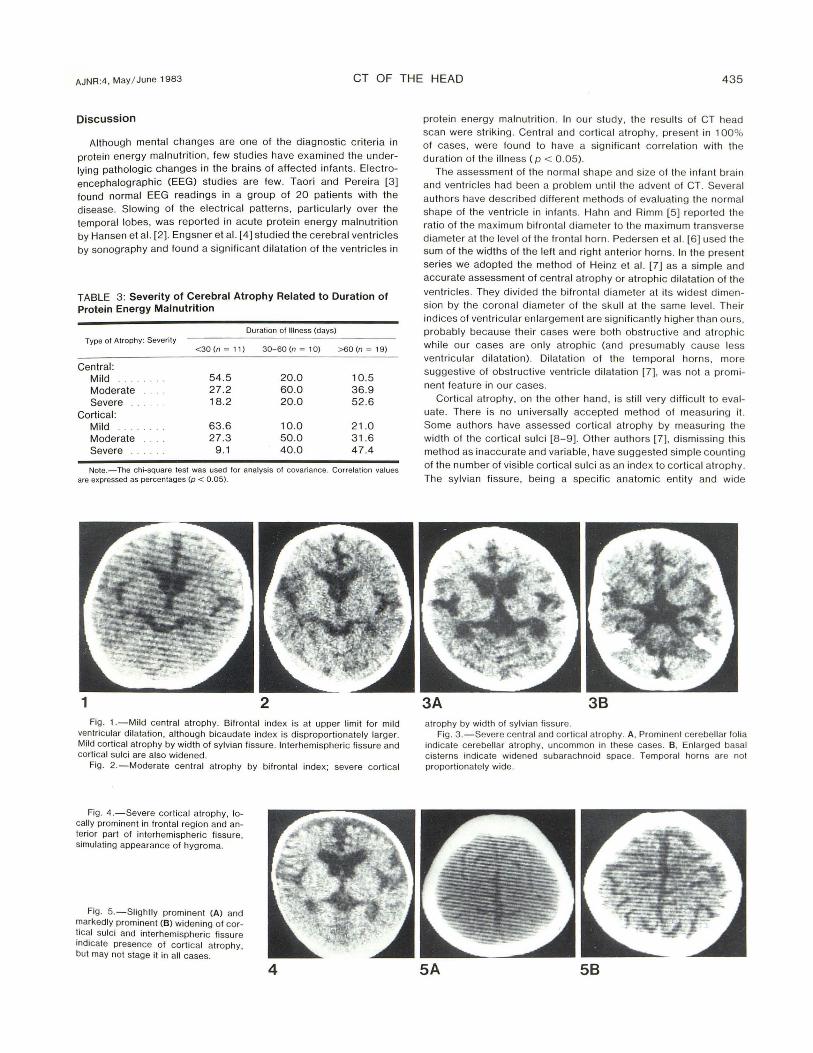
1 2 Fig. 1.-Mild central atrophy. Bifrontal index is at upper limit for mild
ventricular dilatation , although bicaudate index is disproportionately larger. Mild cortical atrophy by width o f sylvian fissure. Interh emispheric fi ssure and cortical sulci are also widened .
Fig . 2. -Moderate central atrophy by bifrontal index: severe cortical
Fig . 4. - Severe corti ca l atrophy, locally prominent in frontal reg ion and anterior part of interhemispheric fissure, simulating appearance of hygroma.
Fig. 5. - Slightly prominent (A) and markedly prominent (B) widen ing o f cortical sulci and interh emispheric fi ssure indicate presence of co rti ca l atroph y, but may not stage it in all cases.
4
protein energy malnutrition. In our stud y, the results of CT head scan were strik ing. Central and corti cal atrophy , present in 100% of cases, were found to have a significant correlation wi th the duration of the illness (p < 0.05).
The assessment of the normal shape and size of the infant brain and ventric les had been a problem until the advent of CT. Several authors have desc ri bed different methods of evaluatin g the normal shape of the vent ri c le in infants. Hahn and Rimm [5) reported the ratio of the maximum bifrontal diameter to the maximum transverse d iameter at the level of the frontal horn . Pedersen et al. [6) used the sum of the widths of the left and right anterior horns. In the present series we adopted the method of Hein z et al. [7) as a simple and accurate assessment of central atrophy or atrophic di latat ion of the
ventricles. They d ivided the bifron tal diameter at its widest d imension by th e coronal diameter of the sku ll at the same level. Their indices of ventricular enlargement are significantly higher than ours, probably because their cases were both obstructi ve and atrophic while our cases are only atrophic (and presumably cause less ventricular dilatat ion). Di latation of the temporal horns, more suggestive of obstructive ventric le dilatation [7) , was not a prominent feature in our cases.
Cortical atrophy, on the other hand , is still very difficu lt to evaluate. There is no universally accepted method of measuring it. Some authors have assessed corti ca l atrophy by measuring the width of the corti ca l sulc i [8-9). Other authors [7) , d ismissing this method as inaccurate and variab le, have suggested simple counting of the number of visible corti cal sulc i as an index to cortical atrophy. The sylvian fissure, being a specific anatomic en ti ty and wide
3A 38 at rophy by width of sy lvian fissure .
Fig. 3 .- Severe cent ral and cortical atrophy. A, Prom inent cerebellar fo lia indicate cerebellar atrophy, uncommon in these cases. B, Enlarged basal cisterns indicate widened subarachnoid space. Temporal horns are not proportionately wide.
5A 58

436 CT OF THE HEAD AJNR :4 , May / June 1983
enough for convenient measurement , is probably the best parameter of corti ca l atrophy. In our patients, its width showed a significant correlation with the duration of the disease.
Our results are in accordance with the work of Dobbing [1 0], who found th at the mean weight of the brain in undernourished developing animals is less than in a normally nourished age-matched control group. The same author [1 1] found th at malnourished rats show cu rtailment of brain development and permanent defici t in the number of brain ce lls and in the DNA and cholesterol content of the brain . It was also reported [1 2, 13] that the mean brain weight and the numbers of ce lls in cerebrum , cerebellum, and brain stem were significantly fewer in malnourished infants than in well nourished infants. Our observations in vivo support th e postmortem findings.
The brain is presumed to be stunted because of protein energy malnutrition. However, mere underdevelopment of the brain would not be sufficient to account for th e CT appearance within the relatively short course of the d isease. An atrophic process with loss of cerebral ti ssue is probably a contributing factor . It is suggested that the morpholog ical appearance of the brain in protein energy malnutrition depends on the relati ve extent of these two factors. Undergrowth can be corrected while atrophy cannot. Future studies are planned to explore and elaborate upon this theory.
REFERENCES
1. Whitehead RG. The assessment of nutritional status in proteinmalnourished child ren. Proc Nutr Soc 1969;28: 1 -1 6
2. Hansen, JDl, Buchanan N, Pettifor JM. Protein energy malnutrition. In : Macl aren D, Burman D, eds. Textbook of pediatr ic nutrition . New York: Churchill Livingstone, 1976 : 11 8 -1 46
3 . Taori GM , Pereira SM . Electroencephalograms and nerve conduction in survivors of kwashiorkor. Br J Nutr 1974;31 : 59- 65
4. Engsner G, Belete S, Sjog ren I, et al. Brain growth in children with marasmus. A study using head c ircumference measurement , transillumination and ultrasonic echo ventr iculog raphy. Ups J Med Sci 1974;79: 116-1 28
5. Hahn FY, Rimm K. Frontal ventricu lar dimension on normal computed tomography. AJR 1976;126: 593- 596
6. Pedersen H, Gyldensted M , Gyldensted C. Measurement of the normal ventricular system and supratentorial subarachnoid in children with computed tomography. Neuroradiology 1979;17:231-237
7. Heinz ER, Ward A, Drayer BP, Dubois PJ. Distinction between obstructi ve and atrophic dilatation of ventricles in children. J Comput Assist Tomogr 1980;4 : 320-325
8. Huckman MS, Fox JH , Topel J . The validi ty of c riteria for the evaluation of cerebral atrophy by computed tomography. Radio logy 1975 ;11 6:85 - 92
9. Gyldensted C. Measurements of the normal ventricular system and hemispheric sulc i of 100 adults w ith computed tomography. Neuroradio logy 19771 4: 183- 192
10 . Dobbing J. Undernutriti on of the developing brain : the relevance of animal models to the human problem. Am J Dis Child 1970; 1 20: 411 -41 5
11 . Dobbing J. l ater development of the brain and its vu lnerability. In: Dairs JA , Dobbing J , eds. Scientific founda tions of pediatrics. l ondon: Heineman Med ical, 1974 : 565- 567
1 2. Dobbing J. The later growth of th e brain and its vulnerability. Pediatr ics 1974;53:2 - 6
13. World Health Organization. Malnutrition and mental development WHO Chron 1974;28 95-102