Centre Jean Perrin - European Society for Medical Oncology · Personalizing the treatment of women...
78
Centre de Lutte contre le Cancer d'Auvergne Clermont-Ferrand - France - Centre Jean Perrin What the clinician needs to know about breast pathology and sample quality Frédérique Penault-Llorca
Transcript of Centre Jean Perrin - European Society for Medical Oncology · Personalizing the treatment of women...

Centre de Lutte contre le Cancer d'AuvergneClermont-Ferrand - France -
Centre Jean Perrin
What the clinician needs to know about breast pathology and sample quality
Frédérique Penault-Llorca

Breast cancer• Classical biomarkers• Proliferation • Prediction of response• Molecular classification• Molecular signature• Importance of quality assurance in breast cancer

Basically for the pathologist, the missions did ot ha ge….
• What is it, is benign, at risk or malignant?• If it is at risk, which follow up ?• If it is malignant, is it aggressive or quiet ? • How do I treat? • Did I remove everything ?
To try to answer to 5 major questions

Answers • What is it, is benign, at risk or malignant?• If it is at risk, which follow up ?• If it is malignant, is it aggressive or quiet ? • How do I treat? • Did I remove everything ?

Priceless Information is Given by the Pathologist, AND will Never be Given by Molecular Testing!

TNM
But we also have classical prognosis and predictive factors• Age• Grade • Histological subtypes• ER/PR and HER2 status• Ki67 +/- mitotic index• Vascular invasion• Tumor margins
Oldies but goldies

TNM parameters: • Pros – Treatment decisions are based on T size – Node involvement is a major prognosis factor – Micrometastasis can be detected in sentinel lymph node by IHC
• Cons– TNM is decreasing because of mass screening (69%of T1 in France in 2015)– 70% of N0 in France in 2015– SLN: axillary dissection is debatable in case of Nano/micromets

Clarification of the AJCC 7th editionStaging multiple tumors• If in same breast:
– T category is based on single largest tumor focus – Do ’t i lude satellite fo i whe easuri g tu or size – If multiple foci of microinvasion, report the # of foci and the size of the largest focus do ’t o i e – Use (m) modifier
• If bilateral: – Stage each side separately

Clarification of the AJCC 7th edition in the 8th edition• Correlate gross, microscopic and imaging findings to assign correct pT when necessary. - For small tumors diagnosed by core biopsy, measuring only the residual tumor in the excision may result in understaging. • Example:
– 6 mm mass by imaging; largest focus in biopsy core – 4 mm – 2 mm focus of residual carcinoma in excision: categorize as pT1b (not pT1a) – No residual cancer in excision: categorize as pT1a (not pTX)
• Same rule applies when tumor is present in multiple fragments: Use clinical and imaging findings to assign pT• pTX should rarely be used

Grade I
Grade II
Grade III8,9
SBR grade modified by Elston and Ellis• Standardization of tumor grading• France 2010: Gr I 25%, Gr II 50% , Gr III 25% • Genomic grade : not confirmed
SBR grade and RFS in operable BC (57% N-) treated by adjuvant therapy

VASCULAR EMBOLI
Lymphovascular invasion and BCSS in N-operable BC treated by adjuvant therapy (from Lee)

Group 3 - Average prognosis:Medullary, classical lobular, lobular mixed
Group 1 - Excellent prognosis: Tubular, invasive cribriform, mucinous Group 2 - Good prognosis:Tubular mixed, mixed ductal NST and special type like adenoid cystic, secretory
Group 4 - Poor prognosisDuctal NST, solid lobular, mixed ductal NST and lobular, micropapillary
18 Histological types: morphology matters!

Special types « The heterogeneous « Triple negative » subtype includes adenoid cystic, juvenile secretory (good prognosis), medullary (intermediate prognosis), and metaplasic (either low grade, with good prognosis; or high grade, with poor prognosis) carcinomas, for which no generalizations can be proposed) »

Medullary features and BCSSFrom medullary
Tubular Non tubular
Tubular carcinoma and DFS (Rakha)

Special types Tubular and cribriform carcinoma may be suitable for observation without therapy or for endocrine therapy alone

Special types rare variant of lobular carcinoma (e.g. pleomorphic) (up to 25% HER2+) and apocrine carcinoma require treatment according to their biological features in a manner analogous to that used for ductal carcinoma
Pleiomorphic lobular carcinoma
E CADH HER2

Prediction


HER2
Negative predictive value
(<5% chance to respond to anti-estrogens or trastuzumab)
HIGH 95%Positive predictive value
30-50%
Breast CancerER/PGR
What is the level of prediction accuracy clinically useful?Cut off 1%

Ki67 why?• Definition of luminal A and B• Decision of CT for ER+, Grade II tumors

Towards a simplified taxonomy of breast cancer? « definition of intrinsic subtypes has proven efficient in defining prognosis for breast cancer patients »RE neg RE pos
C Perou & T Sorlie

Surrogate definition of intrinsic subtypes of breast cancer«basal-like»• ER and PgR absent• HER2 negative• Approximately 80% overlap between « triple negative » and intrinsic « basal-like »• But « triple negative » also include good prognosis special types such as medullary and adenoid cystic carcinoma • Staining for basal keratin is considered insufficiently reproducible for general use

Basal-likeTriple-negative
Triple negative BC by IHC and molecular subtypes: a 80% concordance
Medullary
Adenoid cystic
Low grade squamous
Secretory carcinoma
TNBC subtypes of excellent prognosis

Ki67 = Not standardized

St. Gallen 2013

Personalizing the treatment of women with early breast
cancer: highlights of the St Gallen International Expert
Consensus on the Primary Therapy of Early Breast Cancer 2013
Luminal A all of:ER and PR positiveHER2 negativeKi-67 lowRecurrence risk low based onmulti-gene-expression assay (if available)Luminal B ER positiveHER2 negativeand at least one of:Ki-67 highPR negative or lowRecurrence risk high based onmulti-gene-expression assay (if available)

Personalizing the treatment of women with early breast
cancer: highlights of the St Gallen International Expert
Consensus on the Primary Therapy of Early Breast Cancer 2013
Luminal A Endocrine therapy often used alone.Cytotoxics may be added in selected patients.• High risk status with gene signature, if available;• Grade 3 disease;• Involvement of four or more lymph nodes;• Young age (<35 years)
Luminal B Endocrine therapy for all patientsCytotoxic therapy for most.

TNM
Classical prognosis and predictive factors• Age• Grade • Histological subtypes• ER/PR and HER2 status• Ki67 +/- mitotic index• Vascular invasion• Tumor margins
Oldies but goldies

FOCUS ON HER2 GUIDELINES

THERE IS A CHANGE IN HER2+ DEFINITION

Evolution of HER2 guidelines• Scoring on biopsies• Eligibility criteria to trastuzumab=> for IHC a step back to FDA criteria– accept >10% of 3+ or amplified cells as a definition of HER2 positivity – For amplification
• Dual probes HER2/CEP17 >= 2• Single color HER2>= 6• Equivocal cases (between >=4 and < 6) to retest and/or eventually to treat if still equivocal

Heterogeneity: Where to count?
3+0
2+

≤ % of TC> 10% of tumorcells
> 10% of tumor cells
How to answer in the PR after ISH?• 1 - HER2 negative or «non amplified» : < 4 HER2 copies / nuclei• 2 - HER2 positive :
– «amplified» ≥ HER2 copies / nuclei– «eligible» ≥ 4 HER2 copies / nuclei & ratio HER /CEP ≥ 2
• 3 - HER2 ambiguous or «eligible for Multidisciplinarytumor boards»: – ≥ opies HER / nuclei– ≥ 4 HER opies / nuclei & ratio HER /CEP ≥
– ≥ 4 HER opies / nuclei & ratio HER2/CEP17 <2

Key Recommendations: Oncologists• Should delay decision to recommend HER2-targeted therapy if HER2 status cannot be confirmed as positive or negative after separate HER2 tests (HER2 test result or results Equivocal).• If the HER2 test result is ultimately deemed to be Equivocal, even after reflex testing with an alternative assay, the oncologist may consider HER2-targeted therapy.
www.asco.org/guidelines/ © American Society of Clinical Oncology®. All rights reserved.

For the equivocal cases• Discussion in tumor boards• Integration of HER2 results to– Patient age– Tumor size– Grade– ER, PR status– Proliferation– Molecular tests ???

QUALITY ASSURANCE

Sources of variation in biomarkers testingTime to slicing and
fixation Method of tissue
processing
Type of
fixation
Equipment
calibration
Laboratory
procedures
Time of
fixation
Assay
validation
Staff
competenceType of antigen
retrieval
Test
reagents
Control
materials
Assay
conditions
Use of
image
analysis
Interpretation
criteria
Reporting
elements
Scoring
system
Wolff et al 2007
IHC, ISH
testing
variables
Post-analytical Pre-analytical
Analytical

Interlaboratory discrepancies
All the HER2+ patients are not inditentied for treatment
Key Insight
CAC
PRIVE
CHU/AP
CHG/CH
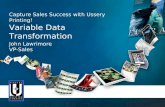
FRANCEOverexpression Rate EBC
10,7%
11,5%
15,6%
10,9%
15,0%
11,5%
13,0%
14,0%
10,3%
13,0%
14,8%
10,0%
12,0%
11,0%
23,0%
13,0%
10,8%11,0%
23,0%
18,0%
12,0%
15,0%
12,0%
13,4%
12,0%
0%
5%
10%
15%
20%
25%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Avg

Courtesy of Antonio Wolff
HER2 testing (dis)concordance in adjuvant trastuzumab trials
Concordance Central vs. Local Lab
N9831JNCI
2002(total n = 119)
ASCO
2004(total n = 976)
JCO 2006(total n = 2535)
IHC 3+(HercepTest)
74% 79.5% 82%(false pos 18%)
FISH +(PathVysion)
67% 85% 88%(false pos 12%)
Magnitude of false-neg HER2 testing un lear ut real…

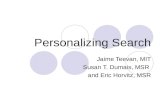
The ALTTO trial
PATIENTS 10829
NO TUMOR 244
DCIS only 297
HER-2 NOT ELIGIBLE
17921329 locally pos (14.6%)
463 locally equivocal
ELIGIBLE 8496
730 locally equivocal (61.2%)
Courtesy G Viale

Patients 3451No tumor 15DCIS only 34Not assessable (core biopsy, etc.) 66
HER-2 Not eligible 338 (9.8%)Eligible 2998
APHINITY Trial

Quality is a multidisciplinary matter

Specimen is viable& biologically
reactive
Molecular composition subject to further alteration/degradation
Factors (examples)
• Antibiotics
• Other drugs
• Type of anesthesia
• Duration of anesthesia
• Arterial clamp time
Factors (examples)
• Time at room temperature
• Temperature of the room
• Type of fixative
• Time in fixative
• Rate of freezing
• Size of aliquots
Time.0
Pre-acquisition Post-acquisition
Biospecimen lifecycle: preanalytical factors
affect molecular composition and integrity

Rapidity of fixation
Invasive ductal carcinoma
Breast cancer
Histopronostical Annotations
Quick procedure quality of RNA but alsoof proteins

A tige ’s degradation
→ degradation of antigens (ER, PR, HER2) after retardated fixation (from1h) and overnight à +4°C in a saline solution

Deleterious effect of
underfixation on breast
biomarkers
Modern Pathol
2009

Key Recommendations: Pathologists• Should ensure that any specimen used for HER2 testing (cytological specimens, needle biopsies, or resection specimens) begins the fixation process quickly (time to fixative within 1 hour) and is fixed in 10% neutral buffered formalin for 6 to72 hours, and that routine processing, as well as staining or probing are done according to standardized analytically validated protocols• Should ensure that the laboratory conforms to standards set for CAP accreditation, or an equivalent accreditation authority, including initial test validation, ongoing internal quality assurance, ongoing external proficiency testing, and routine periodic performance monitoring.
www.asco.org/guidelines/ © American Society of Clinical Oncology®. All rights reserved.
Harmonizationwith CAP guidelines for ER /PR

Multidisciplinary sessions
Treatment initiation Oncologist afterthe multidisciplinary tumor board
Tissue biopsyRadiologist, endoscopist, surgeons
Sampling Fixation IHC testing
Treatment
Realization of IHC tests Technician
Fixation and tissue transportationNurses , OR nurses, courier
Interpretation and pathology reportPathologist
Diagnostic


Possibility of vaccum preservation before fixation (tissue safe system)
Inking of the breast specimen

Her2 testing - Internal control: normal breast

External controls

Overfixation is less harmfull

TAKE HOME MESSAGES

When to question a pathology report• PgR+, ER-• Lobular, tubular carcinoma HER2+• Grade 1, ER+++, PgR+++, HER2+• Grade 3, ER-, ki67 <5%• Grade 3 ER+++, PgR+++• Medulary carcinoma is extremely rare (ask for a second opinion)Redo HER2 on surgical specimen if grade 3, ER- or ER+ If ER and/or PgR is negative on a biopsy redo on surgical specimen

CONCLUSION

TNM
Classical prognosis and predictive factors.• Age• Grade • Histological subtypes• ER/PR and HER2 status• Ki67• Molecular tests• Tumor margins

Patient with
cancer
Biospecimen
tumor « mini-me »
Researcher
Oncologist
Patient cured
Reflects tumor
biology
Personalized medicine

Patient with
cancer
Biospecimen
tumor « mini-me »
Researcher
Induced
molecular
changes
Oncologist
Patient not cured
Reflects tumor
biology
Personalized medicine


MOLECULAR SIGNATURES

TNM
Yes , we have molecular biology !• Age• Grade • Histological subtypes• ER/PR and HER2 status• Vascular invasion• Tumor margins

Centralized tests

MammaPrint (Agendia, NL)
HR+ ET HR - / HER2- , T < 5cm, N ≤ 3
Fresh frozen=> FFPEDNA array70 GENES
CELL CYCLE/ PROLIFERATIONSIGNAL TRANSDUCTION
INVASION, METASTASIS, ANGIOGENESIS
« CENTRALIZED » TEST RECENTLY ADAPTATED TO FFPE
Group of genes (« signatures »)EARLY RECURRENCE (Dg < 5 ans)PROGNOSTIC GOOD SIGNATURE :LOW RISKPOOR SIGNATURE :HIGH RISK
HR+& HR-

OncotypeDX (Genomic Health, USA)
HR+ / HER2- , T1-3, N-/N+
FFPE specimens
qRT-PCR21 GENES PROLIFERATION, OESTROGENE,
HER2, INVASION (16 GENES) + REFS (5 GENES)« CENTRALIZED » TEST(recurrence score) RSLate recurrence (10 years)Benefit from adjuvant TTPROGNOSTIC AND PREDICTIVELOW RISK :
+ HORMONOTHERAPY / - CHEMOTHERAPYINTERMEDIATE RISK :DISCUSSIONHIGH RISK :
+ HORMONOTHERAPY / + CHEMOTHERAPY


Decentralized tests

EndoPredict (Sividon, GE)
HR+ / HER2- , T1-2, N0
FFPEqRT-PCR8 GENES SIGNATURE
PROLIFERATION, OESTROGENES
« LOCAL » TEST(SPECIAL EQUIPMENT IS REQUIRED)
SCORE OF RECURRENCE EP SCORELATE AND EARLY RECURRENCES(5 & 10 YEARS)PROGNOSISLOW RISK HIGH RISK
UBE2C
BIRC5DHCR7
STC2
AZGP1IL65T
RBBP8MGP

Prosigna (PAM50) (NanoString Technology, USA )
IDENTIFICATION OF « MOLECULAR3 SUBTYPES »(LumA, LumB, HER2-enrichi, Basal)
FFPEDNA ARRAY WITH BARCODES
(1 gene = 1 barcode)50 GENES« LOCAL » TEST (SPECIAL EQUIPMENT IS REQUIRED)LATE AND EARLY RECURRENCES(5 & 10 YEARS)PROGNOSISLOW RISK (ROR)
Intermediate riskHIGH RISK (ROR)


THE FUTURE …

77
• Acquired, frequent Mutations (20-30%)• Recurrent, 4 hotspot
• D538G, Y537S/N/C• 74% des mutations ESR1
• Prognostic and predictive of response AI

PIK3CA
• Recurrent mutations- exon 9: E542K, E545K, Helicase domain- exon 20: H1047R, Kinase domain- Frequent: 30 to 40% of BC• Prognostic role?• Predictive role

79

TNM
Classical prognosis and predictive factors• Age• Grade • Histological subtypes• ER/PR and HER2 status• Ki67 +/- mitotic index• Vascular invasion• Tumor margins
Molecular signatures

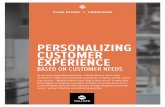
Luminal A Luminal B Triple-negative
ER<10%
PR<10%
HER2-
Ki67 >14%
High grade
ER >10%
Ki67 >14%
PR < 20%
HER2 + possible
ER > 10%
Ki67<14%
PR > 20%
HER2 -
HER2
ER <10%
PR < 10%
HER2 3+
High
Grade
ER+ ER-
AR +
EGFR+/-
HER2 +/-
Molecular
apocrine
TubularCribriform,
IDC grade 1, Mucinous
ILC grade 1
MicropapillaryILC grade 2 & 3IDC grade 2 et3, Mucinous type BNeuroendocrine
ApocrineCCI grade 3
MedullairyMétaplasiqueCCI &CLI grade 3
ProliferationMutations of TP53 or PIK3CA
Genomic instabilityIntratumor heterogeneity
BRCAness
Breast Cancer classification in practice
- Low frequency of mutations- Mutation in numerous genes- Most frequently mutated genes:
PIK3CA, MAP3K1, MAP2K4
CCI grade 2 & 3, Micropapillaire
TILs
Cheang et al CCR 2008, Prat et al JCO 2013, Kennecke et al JCO 2010,
Cheang et al, JNCI 2009, Goldhirsh et al Annals of Oncol 2012 , Cirqueira et al Breast J 2015
Blows et al Plos Medicine 2010
AdenoidcysticSecretoryLow grade metaplasic
ER<10%
PR<10%
HER2-
Low grade
Translocations (ETV6; NTRK3)(MYB; NF1B)
Mutations IDH2

• ER+, HER2- EBC: Luminal A and B subtypes predict 10-
year outcome regardless of previous systemic treatment as
well as residual risk of distant recurrence after 5 years of
endocrine therapy.
• HER2+: the 4 main intrinsic subtypes can be found
• HER2+/HER2-enriched benefit the most from
neoadjuvant trastuzumab, or dual HER2 blockade with
trastuzumab/lapatinib, in combination with CT
• HER2+/Luminal A disease have a relative better
outcome compared to the other subtypes.

• triple-negative breast cancer (TNBC), of 70-80% Basal-like from a biological perspective, should be
considered a cancer-type by itself.
• Distinction between Basal-like versus non-Basal-like within TNBC predict
• survival following (neo)adjvuvant multi-agent
chemotherapy,
• bevacizumab benefit in the neoadjuvant setting
(CALGB40603)
• docetaxel vs. carboplatin benefit in first-line
metastatic disease (TNT study).