Central Auditory Processing Disorder Files/Central... · What Is Central Auditory Processes? Katz,...
59
Central Auditory Processing Disorder (CAPD)
-
Upload
truongcong -
Category
Documents
-
view
222 -
download
2
Transcript of Central Auditory Processing Disorder Files/Central... · What Is Central Auditory Processes? Katz,...

Central Auditory Processing Disorder(CAPD)
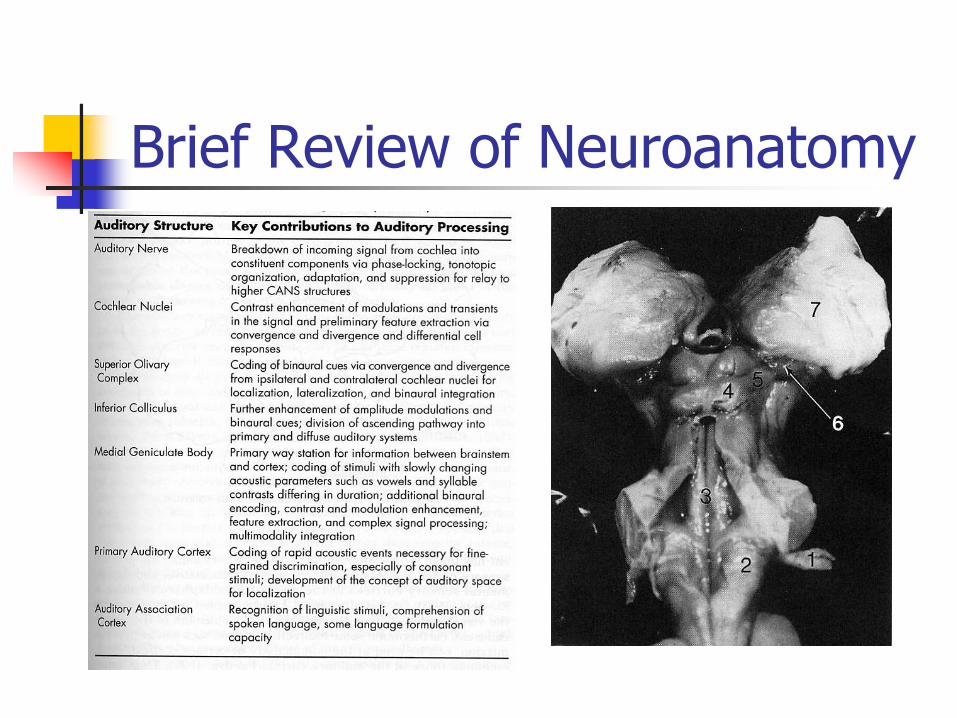
Brief Review of Neuroanatomy

Brief Review of Neuroanatomy
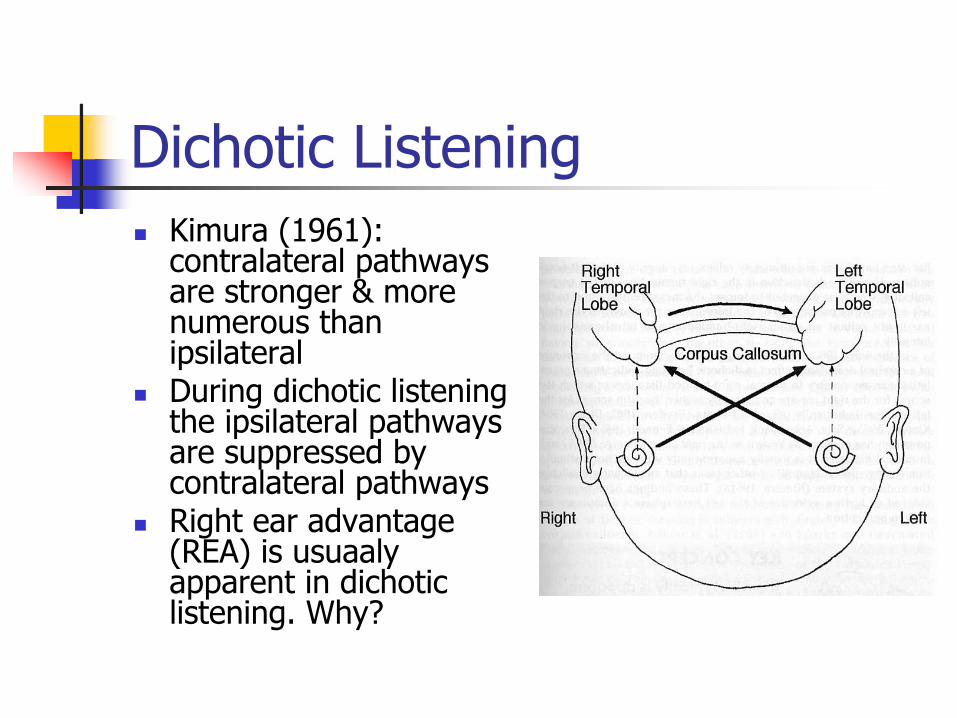
Dichotic ListeningKimura (1961): contralateral pathways are stronger & more numerous than ipsilateralDuring dichotic listening the ipsilateral pathways are suppressed by contralateral pathwaysRight ear advantage (REA) is usuaalyapparent in dichotic listening. Why?
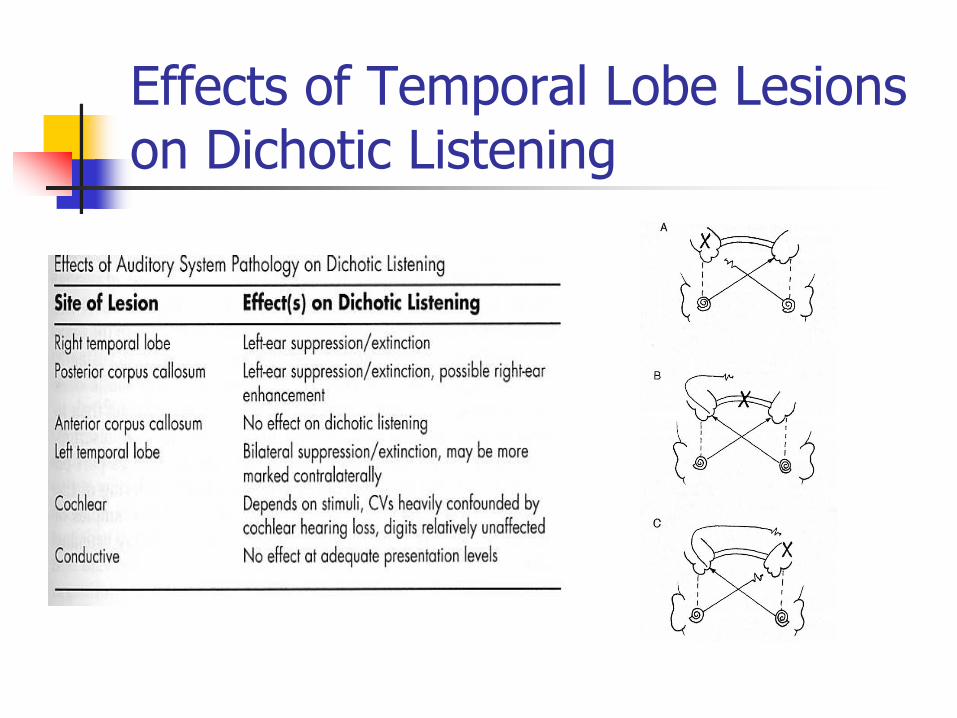
Effects of Temporal Lobe Lesions on Dichotic Listening
What Is Central Auditory Processes?
Katz, Stecker & Henderson (1992) described central auditory processing as "what we do with what we hear." Central auditory processes are the auditory system mechanisms and processes responsible for the following behavioral phenomena (ASHA 1996)
1. Sound localization and lateralization 2. Auditory discrimination 3. Temporal aspects of audition including: temporal
resolution, temporal masking, temporal integration and temporal ordering.
4. Auditory performance with competing acoustic signals 5. Auditory performance with degraded signals
What is CAPD?CAPD is an observed deficiency in one or more of the ASHA (1996) listed behaviors (see previous slide)CAPD can result from dysfunction of the processes that are dedicated to audition, as well from more global deficits (e.g., language deficits, memory deficits, and attention deficits)The prevalence of CAPD in children is estimated to be between 2 and 3% (Chermak & Musiek, 1997), with it being twice as prevalent in males
WHAT ARE SOME OF THE BEHAVIORAL MANIFESTATIONS OF CAPD?
1. Difficulty hearing in noisy situations 2. Difficulty following long conversations 3. Difficulty hearing conversations on the telephone 4. Difficulty learning a foreign language or challenging vocabulary
words 5. Difficulty remembering spoken information (i.e., auditory memory
deficits) 6. Difficulty taking notes 7. Difficulty maintaining focus on an activity if other sounds are present
child is easily distracted by other sounds in the environment 8. Difficulty with organizational skills 9. Difficulty following multi-step directions 10. Difficulty in directing, sustaining, or dividing attention 11. Difficulty with reading and/or spelling 12. Difficulty processing nonverbal information (e.g., lack of music
appreciation) Source: Schminky & Baran (2000)
Diagnostic Problem (Jerger & Musiek, 2000)
Other types of childhood disorders may exhibit similar behaviors, e.g., attention deficit hyperactivity disorder (ADHD), language impairment, reading disability,autistic spectrum disordersSome audiological test battery may fail to distinguish CAPD from children with other problemsOther confounding factors, e.g., lack of motivation, attention, cooperation and understanding

Differentiation Between CAPD & ADHD
Read Chermark et al., 1999.Only 2 (i.e., inattention & distractibility) of the 11 most frequently cited behaviors reported as common to both condition
Screening For CAPDScreening by Questionnaire: observation of suspect behaviors via questionnaires (Jerger & Musiek, 2000)
Fisher's Auditory Problems Checklist (Fisher 1985) for Kdg. to grade 6Screening Instrument for Targeting Educational Risk by Anderson 1989 (S.I.F.T.E.R) for grade 1 & aboveChildren’s Auditory Processing Performance Scale (CHAPPS) by Smoski, 1990
Screening by Test (Jerger & Musiek, 2000).A dichotic digit test (Musiek, 1983)A gap-detection testSCAN-A (Keith, 1986)

Dichotic Digit TestOne of the more commonly used tests in Dichotic Speech Tests is the Dichotic Digits test (Musiek, 1983)Number 1-10 excluding 7 is usedPresentation level: 50 dB re: SRTThe child is asked to listen to four numbers presented to the two ears at comfortable listening levels (50 dB SL re:SRT)In each test item two numbers are presented to one ear and two numbers are presented to the other ear. For example, in this figure, 5 is presented to the right ear at the same time 1 is presented to the left ear.
Then the numbers 9 and 6 are presented simultaneously to the right and left ears

Dichotic Digit TestChild is asked to repeat all numbers heard and a percent correct score is determined for each ear and compared to age-appropriate normsThe minimum patient age should be 7 yearsTest administration time: 4-5 minutes minutesAdvantages:
Good validityShort administration timeResistive to effect of peripheral lossLittle linguistic loadDigits are easily transferred to picture-pointing taskModerately high sensitivity to brainstem, cortical, and inter-hemispheric lesions

Dichotic Digit TestInterpretation:
The cut off norm is 90% and lower for 12 years to adult7 years – 7:11; 55% left, 70% right8 years to 8:11; 65% left, 75% right9 years to 9:11; 75% left, 80% right10 years to 10:11; 78% left, 85% right11 years to 11 years, 11 months; 88% left, 90% right
Fairly sensitive to intra-cranial lesionContralateral in right temporal lobe lesionBilateral in left temporal lobe lesion
Sensitive to inter-hemispheric lesion (corpus callosum)Sensitive to brain stem lesionResistant to mild-moderate cochlear lost

The Gap Detection TestGap detection is a hearing test that measures the ability to resolve differences in timeThree noise bursts, with one of them having a silent interval ("gap") in it are presentedThe task is to pick the one with the gapDepending on the response, the gap may become longer or shorter or totally undetectable The computer program may be used to automatically track the responses and calculate the smallest gap that can be detected
The Gap Detection TestInterpretation
A normally-hearing person may detect 1-2 msec gap if the stimuli are presented at a comfortably loud levelperson with CAPD may have a significantly greater gap detection threshold A standard test developed by Keith (2000) can be used; Random Gap Detection Test (RGDT)
Several pairs of tonal or click stimuli are presented to listener, who is required to indicate whether one or two sounds are heardSubtest 1 is a practice consisting of 500 Hz tone pairs with interstimulus interval (ISIs) presented in ascending order from 0-40 msSubtest 2 is the standard test with random ordering of ISI from 500-4000 HZRefer to the manuals provided
SCAN-AScreening Test for auditory Disorders (SCAN, Keith, 1986)For children between 3-11 yearsFour subtests
Filtered wordsAuditory figure ground (speech in noise)Competing words (recall two or more competing words – divided attention) Competing sentences (revised, Keith, 2000)
Administered at MCLTest time: approximately 20 minutes
SCAN-A-B-C
DisadvantagesBellis (1996) found alarming false positives and false negatives for the testThe passing score in all subtests should not be taken as evidence that further evaluation is unnecessary, but rather be viewed in light of other data (Bellis, 1996)
Differential Diagnosis of CAPD(Jerger & Musiek, 2000)
Behavioral Tests
Electrophysiologic & ElectroacousticTests
Neuroimaging Studies
Behavioral Tests (Medwetsky, 2002)Based On The Particular Skill
Span of ApprehensionLexical DecodingPhonologic DecodingTolerance-Fading MemoryAuditory IntegrationSequencingAuditory Attention

Span of ApprehensionTests how much information can be retained in short term/working memory
Test of Auditory-Perceptual Skills (TAPS-R; Gardner, 1996) – Auditory Numbers Forward (ANF)
This test evaluates how much information a child can hold in conscious, short-term/working memory for familiar items such as numbers, familiar words, or everyday directionHas been normed for children ages 4-12Can provide scaled score, percentile, and age-equivalent scores
Lexical Decoding
Ability to process information both accurately and quickly using lexical (word) items
Staggered Spondaic Word Test (SSW, Katz & Ivey, 1994)Competing Sentence Test (CST; Willeford& Burleigh, 1994)

SSWIs a dichotic procedureSpondees are presented in an overlapped fashion: the 2nd
word of the 1st spondee occurs at the same time as the first word of the 2nd spondeeThus, one ear (leading ear) is presented with 1st syllable in isolation (non-competing), followed by 2nd syllable in a dichotic mode (competing). The other ear (lagging ear) begins with the 1st syllable presented in the dichotic mode and finished with the 2nd syllable presented in isolationEach ear serves as the leading ear for half of the test presentationsPresentation level: 50 dB SL re: SRT/PTATest time: 8 minutesNormed for ages 5-69 years
SSWTest outcome
Error scores are calculated for each ear in both the competing and non-competing modesCorrections can be applied to account for hearing lossMany error patterns can be identified, interested students can refer to Katz & Ivey (1994) in Handbook of Clinical Audiology. 4th edition (pp.239-255)This test is sensitive to intra-cranial (temporal/cerebral) lesion
Contralateral deficit if primary auditory areas involvedMixed results for brainstem lesions
CST25 pairs of sentences with 6-7 words are simultaneously presented in dichotic mannerAll the sentences have similar duration, word length and semantic contentNormed for ages 5 years through adulthoodPresentation level:
target ear (test ear) 35 dB SL re: SRTNon-test ear receives competing sentences at 50 dB SL re:SRT
10 paired sentences for each test condition
CSTOutcome and interpretation
Sentences are generally scored as correct if the meaning and content of the sentence was identified appropriatelyThe scores are then compared to age norms for the better and poorer earsAbnormal competing sentence tests performance has been reported in patients with temporal lobe lesions (Musiek, 1983), predominantly in the ear contralateral to the lesion
Other Scoring Methods (Musiek)Each of the 10 target sentences is assigned a value of 10 points and is divided into quadrants, each worth 2.5 points or 25% of total sentence scoreThe child’s response is scored in terms of quadrants correct. Each sentence will have maximum score of 10% with possible scores of 7.5, 5. 2.5 and 0% scores. The maximum total score of 100% for 10 sentences
Target: I think we’ll have rain todayCompeting: There was frost on the groundResponses:
I think we’ll have rain today; Score: 10%I think we’ll have frost today; score 7.5%There was rain today; 5%There was frost today; 2.5%There was frost on the ground; o%
Norms Based on Previous Scoring (Bellis, 2002)
7 years – 7:11; 35% left, 80% right8 years to 8:11; 39% left, 82% right9 years to 9:11; 74% left, 90% right10 years to 10:11; 88% left, 90% right11 years to 11 years, 11 months; 90% both ears12 years to adult: 90% both ears
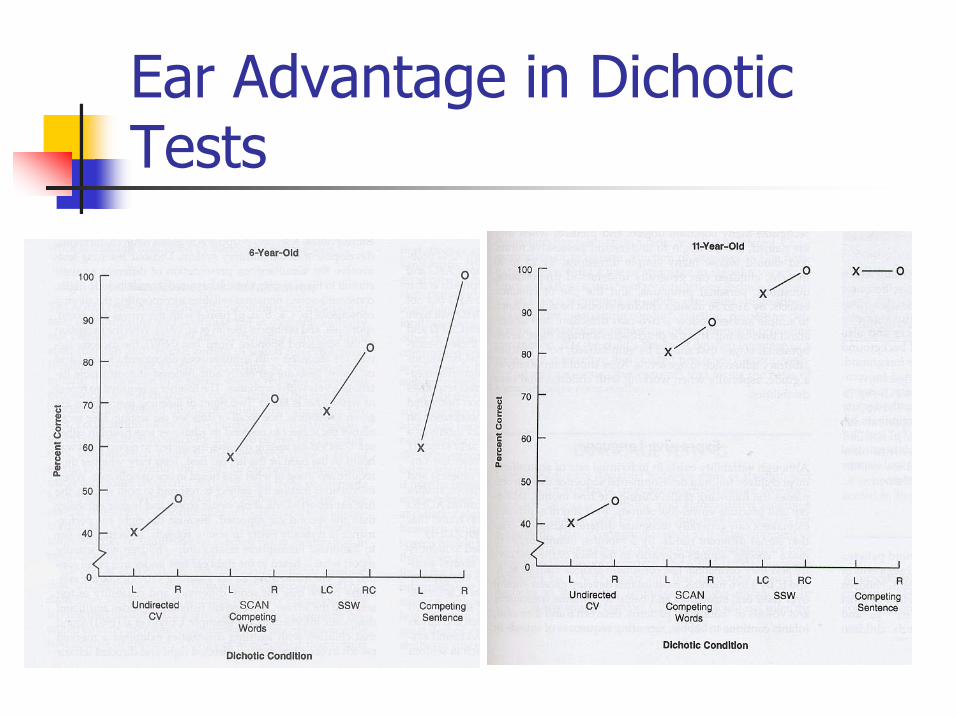
Ear Advantage in Dichotic Tests

Phonologic DecodingEncompasses a broad range of skills that can be divided into two main areas:
Phonological awareness: the ability to think about and manipulate the speech segments of a language (Swank & Catts, 1994)Phonics: the ability to represent individual speech sounds through the use of symbols (e.g., letters)
In this category we only discuss Phonemic Synthesis Test (PST; Katz & Harmon, 1982)

PSTAssesses the ability to blend individual phonemes to form the target wordConsists of 25 test words presented phoneme by phoneme for each word Words are presented one sound at a time to the child, who will then blend the sounds into words It evaluates discriminations, sequencing and/or sound blendingNorms available down to 6 years of age Highly predictive of the ability to read wordsAlso closely associated with articulation, spelling, and receptive language (Katz & Harmon, 1982)Administration time: 15 minutes

PSTThe following outcomes can be determined through careful analysis of the error patterns:
More errors on the initial phoneme: associated with tolerance-fading memory (ability to retain/recall earlier presented information successfully) because of an inability to retain earlier presented informationMore errors on the vowel and final phonemes: associated with phonologic decoding difficulty (an ability to process phonemes accurately and quickly)Reversals: associated with sequencing or organizational difficulty

Auditory IntegrationIncludes:
Binaural integration of acoustic stimuli: integrating signals transmitted separately to each earInter-hemispheric transfer of auditory-linguistic information (assessing ear dominance)Integration of auditory-linguistic information across processing regions (segmental and suprasegmental)Integration of information between modalities:i.e., auditory-visual integration
Binaural IntegrationIt is sensitive to brainstem lesions and it is the initial stage of processing. It includes:
Integration of different intensity and temporal information of one signal source from the two ears (e.g., localizing a sound)Integration a portion of one signal presented to one ear and a complementary portion presented to the other ear and to combine the two portions to derive a target stimulus (also called binaural fusion)
Two tests will be discussed in this category:Binaural fusion (BF, Matzker, 1959)Masking Level Difference (MLD, Hirsh, 1948; Licklider, 1948)
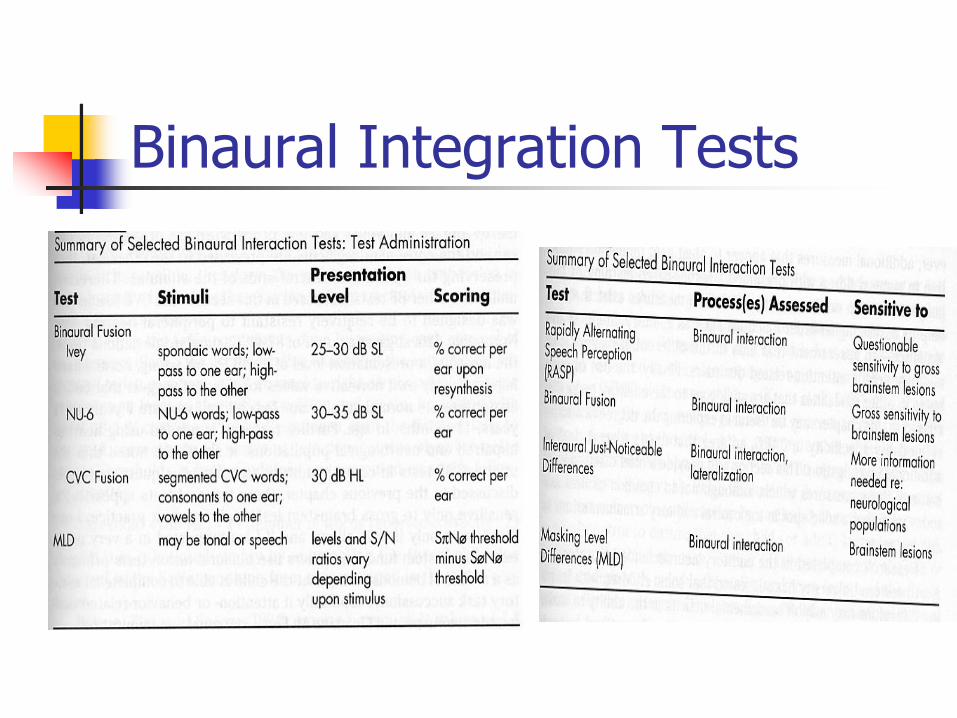
Binaural Integration Tests

BFIs a measure in which words, usually monosyllables, are pass-band filtered into a low-pass band and a high pass bandA low pass band (e.g., from 500-800 Hz) is presented to one ear and the high pass band (e.g., 1815-2500 Hz) to the other earRecognition of either band in isolation is poorNormal listeners are capable of fusing the two pass-bands when they are presented binaurally with a high level of accuracyPatients with brain stem lesions (Palva & Jokinem, 1975; Smith & Resnick, 1972) and some patients with temporal lobe disorder (Lynn & Gilory, 1972) have poor BF scores

BFThere are a number of commercial BF tests available:
The Ivey BF test, which uses spondees and is included in the Willeford central test battery (Willford & Burleigh, 1985)The NU-6 BF test (Wilson & Mueller, 1984): uses monosyllabic words to reduce linguistic redundancy, thereby increasing sensitivityThe CVC-BF task (Wilson, 1994): uses initial consonant-vowel nucleus-final consonant word list. The carrier phrase and vowel segments are presented to one ear, and the consonant segments to the other ear
MLDMany experiments have shown that the threshold for detecting a signal masked by noise is lower when the noise and signal are presented in a particular way to both ears. Before describing the experiments you have to become familiar to different terminology that is used in these types of experiments.
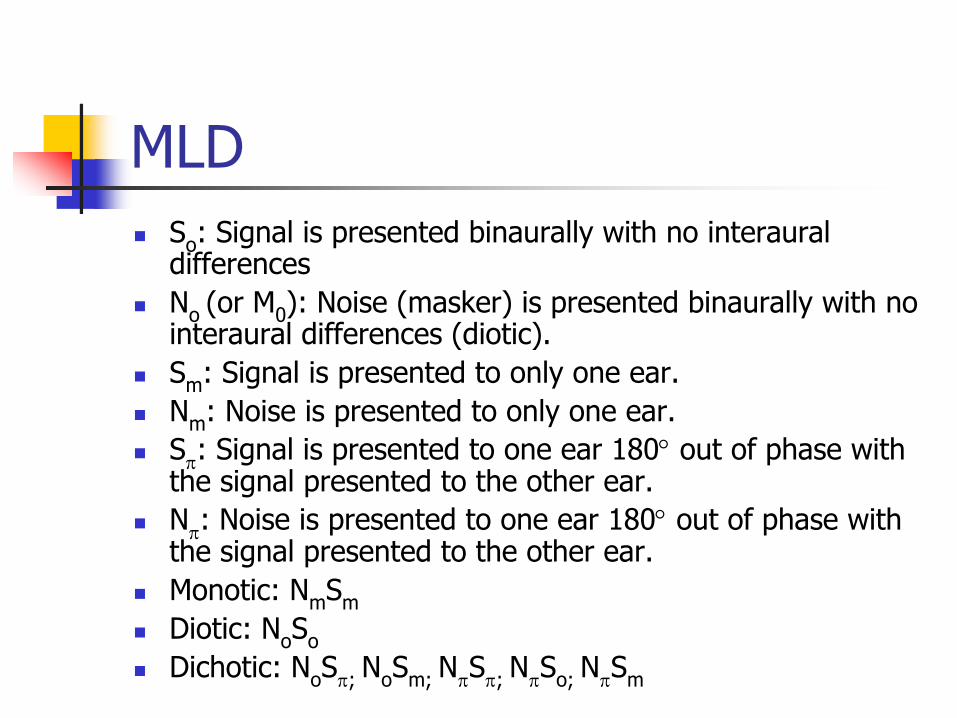
MLDSo: Signal is presented binaurally with no interauraldifferencesNo (or M0): Noise (masker) is presented binaurally with no interaural differences (diotic).Sm: Signal is presented to only one ear.Nm: Noise is presented to only one ear.Sπ: Signal is presented to one ear 180° out of phase with the signal presented to the other ear.Nπ: Noise is presented to one ear 180° out of phase with the signal presented to the other ear.Monotic: NmSmDiotic: NoSoDichotic: NoSπ; NoSm; NπSπ; NπSo; NπSm
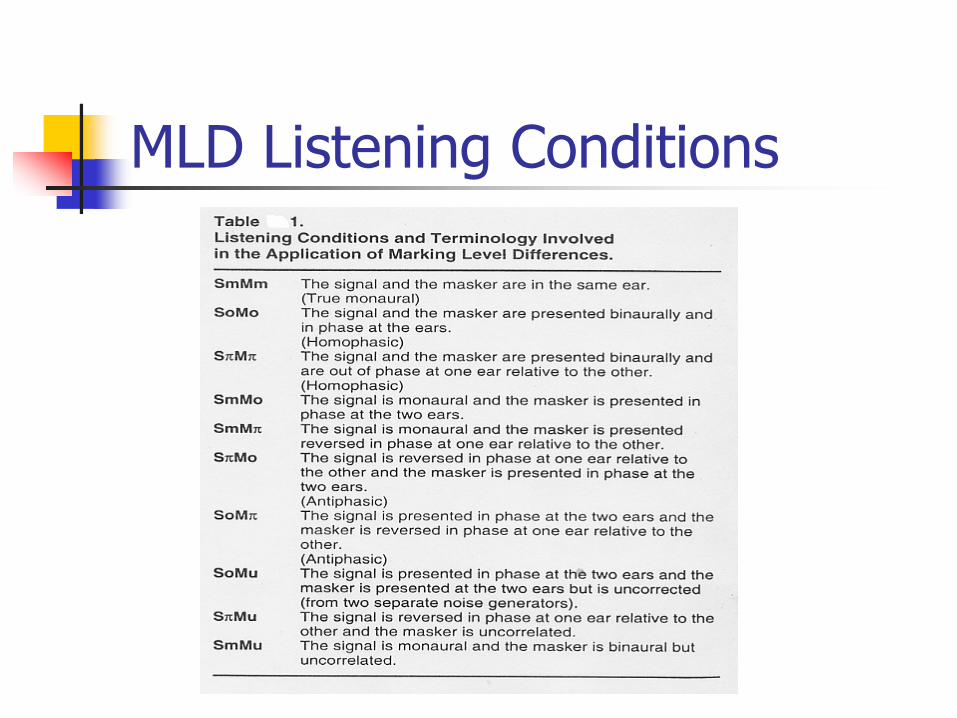
MLD Listening Conditions
MLD

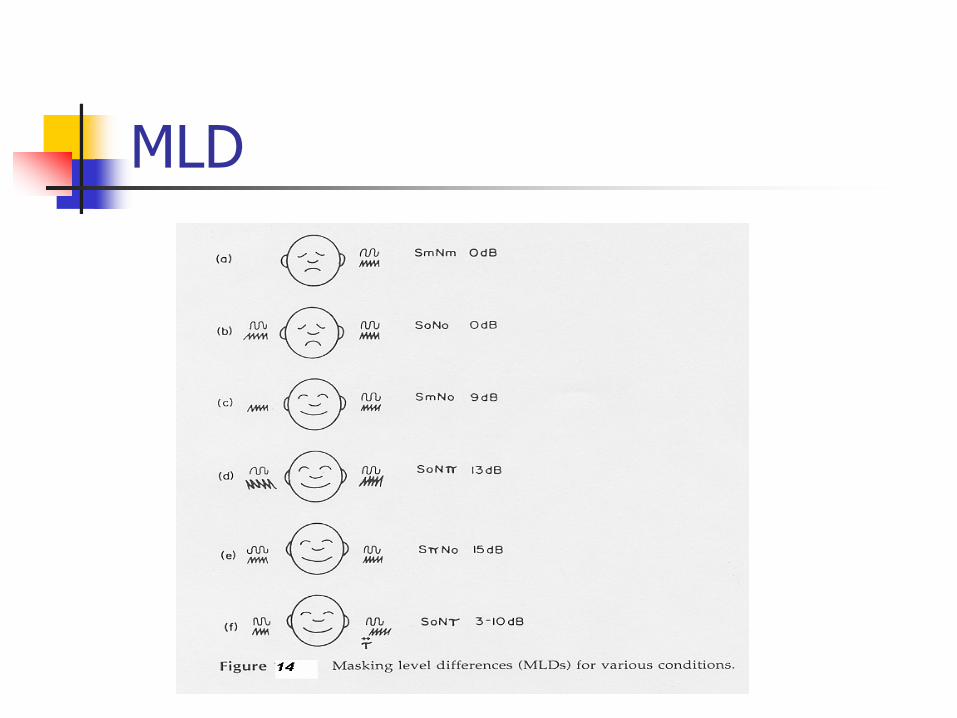
MLDBinaural advantage occurs only when the stimuli are in some way different at the two ears (dichotic)We can define MLD as difference in masked threshold between dichotically presented stimuli and signals that are presented monotically (or diotically). The size of the MLD varies from as large as about 15 dB for NoSπ condition to as little as 0 dB The largest MLDs are obtained when either the signal (SπNo) or the noise (SoNπ) is opposite in phase at the two ears MLD is largest for low frequencies-about 15 dB for 250 Hz- and decreases for higher frequencies until a constant of about 3 dB is maintained about 1500-2000 Hz
MLDIn clinic MLD is performed for 500 Hz and it is defined as the difference in threshold between the in-phase and out-of-phase conditionsFor 500 Hz, the MLD should be greater than 7 dB and is usually around 12 dBAbnormal performance on the MLD is consistent with brainstem disorder (Hannley et al., 1983; Hendler et al., 1990; Lynn et al., 1981)Care must be taken in interpreting MLD results in the presence of hearing loss at 500 Hz
Interhemispheric Transfer of Auditory-Linguistic Information
It test the efficiency of transfer of auditory-linguistic information between the two hemispheres of the brainIt is a dichotic testAcoustic stimuli are transmitted most efficiently to the hemisphere contralateral to the stimulated earLanguage processing center resides in the left hemisphere in most individuals (Bhatnagar & Andy, 1995), therefore, stimuli presented to the left ear must ultimately cross over from right to left via corpus callosumCorpus callusum is one of the last cortical structures to reach physical maturityA right ear advantage is usually observed in children until age 11 (Pinheiro & Musiek, 1985)
Tests for Interhemispheric Transfer of Auditory-Linguistic Information
The dichotic tests that can be used for this category are:
Dichotic Digits Test (DDT; Musiek, 1983)Staggered Spondaic Word (SSW)Competing Sentence Test (CST)

Integration Across Processing Regions
Perception of speech entails processing of both linguistic content (lexicon, semantic, syntax and suprasegmental information (stress, intonation, duration pattern)The linguistic contents are mostly processed in the left hemisphere and suprasegmentalinformation are mostly processed in the right hemisphere (Musiek & Lamb, 1994)Two tests will be discussed here:
Pitch Pattern Sequence (PPS, Pinheiro, 1977)Duration Pattern Sequence (DPS; Musiek et al., 1990)
PPSHas a high sensitivity Administration time: 10 minutesChildren & adult version (not good for children ≤ 8 yrs)It is composed of 120 test sequencesEach sequence containing three tone burstsIn each sequence two of the tone bursts are of the same frequency, whereas the third is of a different frequencyThe tone bursts include
A low frequency tone (880 Hz)A high frequency tone (1122 Hz)
An interstimulus interval of 200 msec.

PPSSix different sequences can be generated (i.e., high-high-low, high-low-high, high-low-low, …)The sequence are typically presented at 50 dB Sl re: SRTThe patient is asked to verbally describe each sequence heard (can also hum in case of children)Percent correct identification scores are derived for each ear
PPS OutcomePatients with compromise of the auditory areas of either hemisphere or of the interhemisphericpathways (i.e, corpus callosum) have difficulty describing the monaurally presented test sequence (Musiek et al, 1994)If the patients can not describe the sequence verbally but can hum the sequence, it is most likely corpus callosum lesion (observed in confirmed cases of posterior commissurotomies, Musiek et al., 1984)Therefore, in a verbal response some processing of stimuli occurs in both hemispheres A cut off score of 78% for young , normal hearing adult (Musiek, 1994)
DPSSimilar to PPSThe patient is asked to verbally describe the sequences heard; long-short-longThe frequency of the tones is maintained at 1000 Hz and the duration of the tones is varied (250 msec and 500 msec)In each sequence two of the three tones have the same duration and the third one if of a different durationThe presentation level: 50 dB re:SRTPercent correct identification scores are derived for each ear

DPS Outcome
The test is highly sensitive to cerebral lesion (86%, Musiek et al., 1990) with most of the cochlear hearing loss (92%) showing normal performanceA cut off score of 73% for young , normal hearing adult (Musiek, 1994)Not appropriate <9 years of age

Auditory-Visual (AV) Integration
AV integration will help hearing impaired individuals to integrate both visual (lip reading) and auditory cues to perceive the speech. It also helps to associate sounds and symbols (phonics) which is essential when learning to read and spellTests:
Lindamood Auditory Conceptualization Test (Lindamood-Charles-H; Lindamood-Patricia-C, 19790SSW

Lindamood Auditory Conceptualization Test
Designed to measure a student's level of auditory functioning.Skills measured parallel those basic to spelling and readingSubject manipulates wooden blocks of various colors to indicate his or her conceptualization of speech sound patterns delivered by examinerAge Range: AGE 2-17, AdultsTesting Time: 10 minutes
Summary of Behavioral Tests
If you want to be less affected by the influence of language and cognitive processes (e.g., memory, attention) then you have to select those test battery that have little linguistic load, e.g., nonsense syllables or digitsAlways adhere to a test battery concept
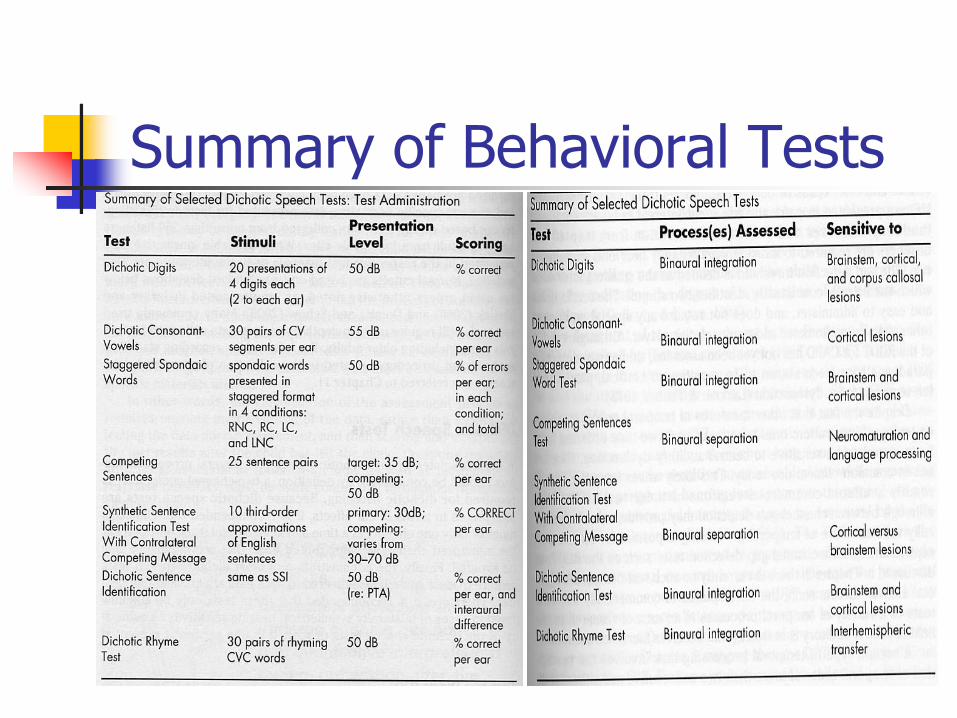
Summary of Behavioral Tests
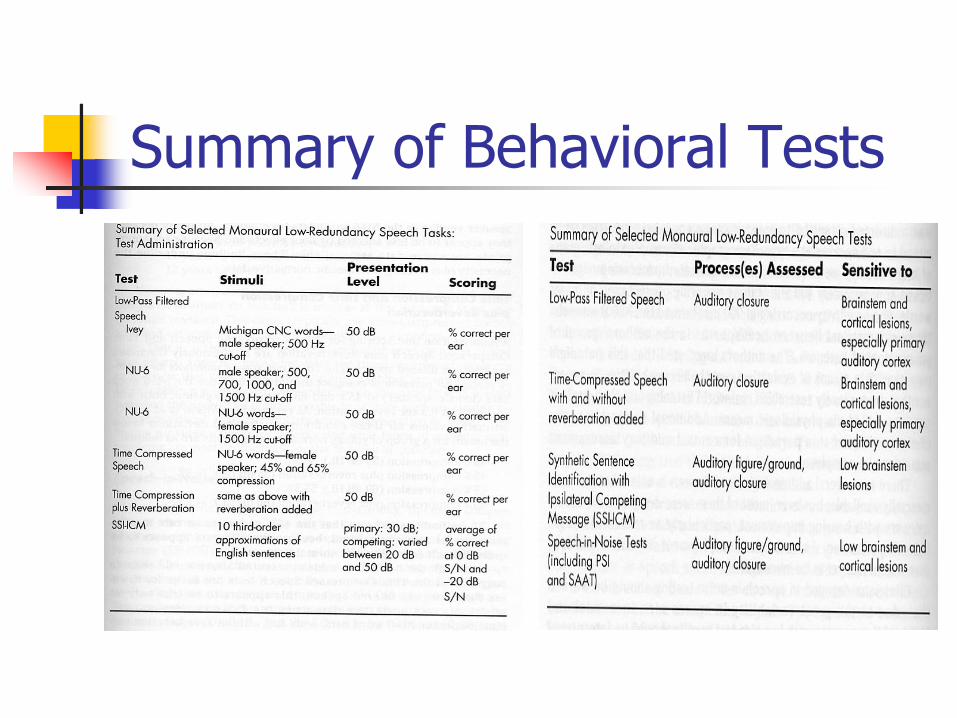
Summary of Behavioral Tests
SSI-CCM SSI-ICMSSI-CCM:
Ten-3rd-order approximations of English SentencesCompeting message consists of continuous discourse (Davy Crockett)Message @ 30 dB HL (pure tone should be normal @500-2000 Hz)The competing varies from 30 dB HL (o S/N) to 70 dB HL (-40 dB S/N)Sntences have to be identify by number on the sentence lists in front of the patientScore is in percent correct for each ear. CCM score is considered to be either the core obtained in most difficult condition (-40 S/N) or the average of the S/N Degree of asymmetry between ears are better indicator of central auditory dysfunctionAdults with normal hearing tends to perform around 100% in all conditions as do most listeners with brainstem lesionPeople with temporal problem tend to do worse in ear contralateral to the lesion

Electrophysiologic Tests (Jerger & Musiek, 2000)
Immittance audiometryOtoacoustic emissionsAuditory brainstem responseAuditory middle latency response (AMLR)Auditory late response (ALR)Mismatched negativity response (MMNR)Event-related response (ERP
Auditory NeuropathyCan exhibit symptomatology similar to CAPD (Read Linda Hood paper)Auditory neuropathy affects the normal synchronous activity in the auditory nerve, without affecting the amplification function in the inner earPatients with auditory neuropathy often complain that they can hear sounds, but cannot understand speechPsychophysical tests indicating that these patients' poor speech recognition is due to a severe impairment in their temporal processing abilitiesThese characteristics are observed on clinical audiologic tests as normal otoacoustic emissions (OAEs) in the presence of an absent or severely abnormal auditory brainstem response (ABR)