
Central and peripheral visual field
107
EXAMINATION OF CENTRAL AND PERIPHERAL VISUAL FIELD- AMSLER GRID , CONFRONTRATION TEST, BJERRUM’S SCREEN etc… Presented by : Deepa Dhungel B. Optom 3 rd year Resource person Mr. Gauri Shankar Shrestha
-
Upload
deepa-dhungel -
Category
Health & Medicine
-
view
58 -
download
3
Transcript of Central and peripheral visual field

EXAMINATION OF CENTRAL AND PERIPHERAL VISUAL FIELD- AMSLER GRID , CONFRONTRATION TEST, BJERRUM’S SCREEN etc…
Presented by : Deepa Dhungel B. Optom 3rd year
Resource personMr. Gauri Shankar Shrestha

Presentation layout• Introduction•Central field examination• - Amsler grid• - Tangent screen• - Berkeley central field test•Peripheral field examination• - Confrontation field• - Arc perimetry •Goldmann and automated perimetry-
central and peripheral field examination

INTRODUCTION•Visual field
The portion of space in which objects visible during steady fixation of gaze in one direction

Normal limits
60° (65 ° -70 °)superiorly Inferior retina
60° (60 ° -65 ° )nasally temporal retina
75° (70 ° -75 °)inferiorly superior retina
100°(90 °-110 °)temporally nasal retina

macula central 10 degrees
fovea central 3 degrees
The visual field is limited by size of retina and margins of the orbit

Central field includes an area from fixation point to a circle 30 ̊ away
Contains the Physiological Blind Spot on its temporal side
•Foveal (At 0 0)•Off center(10 or less)•Para foveal (3 0 not less than 1 0)•Para macular (50 not less than 30)

Peripheral field :
rest of the area beyond 30 ̊ to outer extent
of field of vision

Peripheral field :
•Kinetic perimetry- The temporal field constricts with age after the sixth decade of life
•Automated perimetry- decrease sensitivity•Causes
▫partly to age-related miosis ▫Peripheral corticl cataract▫decreased oxygenation of the peripheral retina

I-4 ↓at the rate of 6% per decade
I-3 ↓at the rate of 8%per decade
I-2 ↓at the rate of 10%per decade

Visual field screening
Central PeripheralVisual Acuity – 5 ̍ of arc
Confrontation – 120 ̊
Amsler Grid – 20 ̊ Perimetry -180 ̊
Tangent screen – 30 ̊
Berkeley central VF test- 10 ̊perimetry
Arc perimetry
tangent screen can be used to test peripheral field upto 60 but ̊normal clinical setup can’t accommodate such a large instrumentation

Terms describing visual field defects
•Central: fixation only
•Cecocentral: from fixation temporally to the blind spot
•Paracentral: region next to, but not including, fixation

•Pericentral : region symmetrically
surrounding, but not involving, fixation
•Arcuate: Corresponds to and represents nerve
fibre bundle loss

•Altitudinal: Involves
two quadrants in
either the superior or
inferior field
•Quadrantanopia: One
quadrant of visual
field involved

EXAMINATION OF CENTRAL VISUAL FIELD
AMSLER GRID
•Introduction:
•Dr. Marc Amsler, 1920
•Manual comprises of seven charts
• 100 cm2 (10 cm Х 10cm), square shaped

•When held 33cm from the eye : allow assessment of central 20A VF
•Correlating, area just inside the temporal vascular arcades not including the optic disc
•Important in testing macular function

Indications for Testing
• Reduced BCVA even with pinholes
• Suspected macular disease
• abnormal color vision
• SUSPECIOUS appearance of macular area

Conventional Charts•Chart 1 (Standard Amsler grid)
•Most familiar and widely used
•Grid pattern consisting of 0.5cm white squares, set against a black background
• Each grid corresponds to 1 degree of visual field
• arranged in 20 horizontal & vertical rows making 20 squares each

Chart no.1
•Most versatile ,
• useful in identifying various forms of distortions , relative and absolute scotomas
Chart 2 2:
•Pt. with a central scotoma may respond better to chart 2
•Similar to Standard grid chart except, diagonal lines intersect at the center of the grid to form an ‘X’▫giving the patient a better idea of where the
fixation point is located

•A larger white central spot may be applied with tape to the center of the grid if the pt is still unable to achieve or maintain central fixation
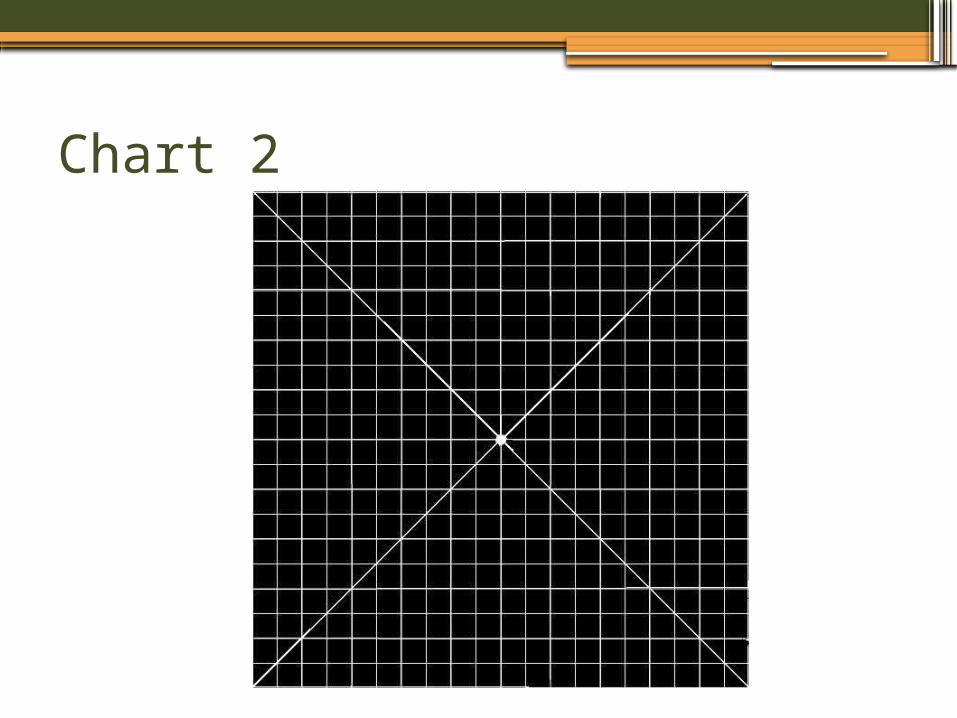
Chart 2
Chart 3:•Configuration identical with that of the
Standard Amsler chart
•but has red squares instead of white ones in black background
•stimulate long wavelength cones found predominantly at the fovea

•Useful in patient suspected of having
• central or cecocentral scotoma a\w nutritional amblyopia, as from alcohol-related thiamine deficiency
• or toxic maculopathy, as from quinine and its derivatives
•evaluation of colour scotomata and desaturation

Chart 4:
•No lines to distort; instead small white dots randomly distributed over black background
• Patient with one or more paracentral scotomas may be able to delineate the area[s] of involvement more easily
• Since the background and scotoma appear same in color for the observer; may result in false results

Chart 4:

Chart 5:
•20 evenly spaced white horizontal lines on a black background
•Possible to rotate the chart to any meridian to check for irregularities in a particular area
•Patient with central or paracentral metamorphopsia d/t various retinal and choroidal disorders; esp sensitive

Chart 5:
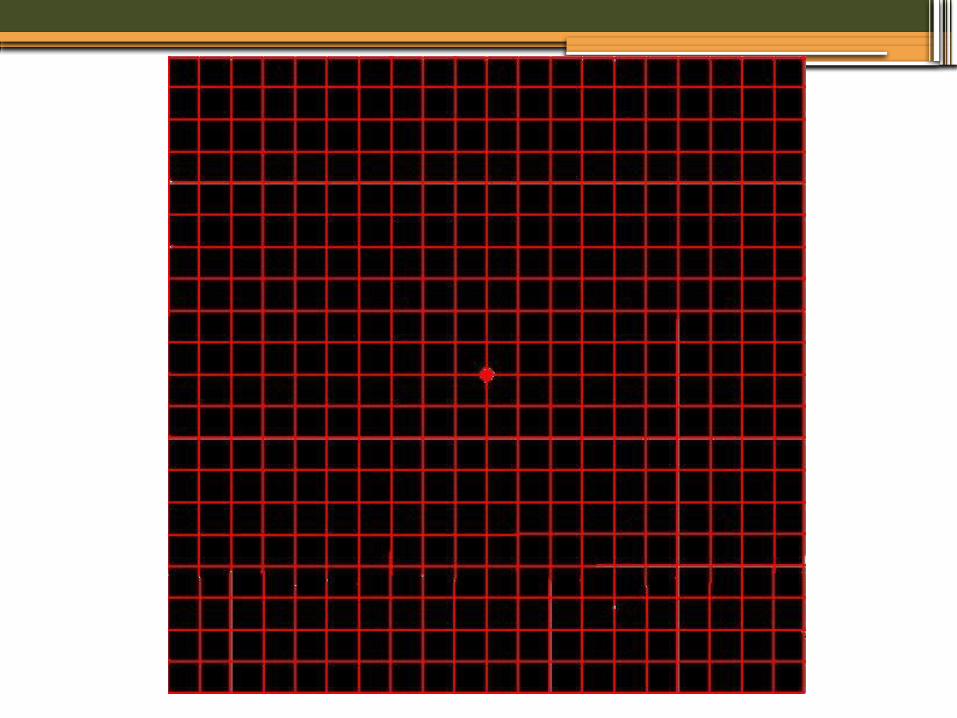
Chart 6:
•Varies slightly from chart no 5
•Contains black lines against a white background and
• the areas 1 degree above and below the fixation dot are bisected by additional horizontal lines.

Metamorphopsia along the reading level may be more easily observed with this chart

Chart 7 NO 7: • This chart breaks the horizontally oriented 6 ̊X
8 ̊central area, corresponding anatomically to the normal macula, into 0.5 degree squares
• Making it a more sensitive detector to insidious macular compromise
• More useful in cases where there is subtle visual disturbance from macular disease, esp early in the course of the disease


Clinical Procedure
•Pt. should be wearing appropriate correction for test distance
•No lights should be shown to the eye right before the test, pupil should not be dilated
•Chart should be uniformly illuminated
Five series of questions
1) Can you see the central white dot?
to rule out a central scotoma

•If ‘Yes’, a central scotoma unlikely unless false positive response d/t poor pt compliance
•If ‘ It looks washed out’ or ‘It seems slightly blurry’, suspect for a relative central scotoma

37
RELATIVE CENTRAL SCOTOMA

If the pt is unable to see the central white dot at all, an absolute central scotoma may be +nt

2. Can you see all the four sides of the large square as well as all four of its corners?
• to rule out arcuate, altitudinal, quandrantic, or hemianopic field defects, as well as overall field constrictions

• If ‘Yes’, may proceed to Question no 3
• If ‘No’ then the pts should be asked to document the missing sides/corners as accurately as possible in the tear-off chart

Arcuate scotoma-As seen by an advanced glaucoma patient

3.Are any of the small squares blurry or missing on any part of the grid?
• to rule out relative or absolute paracentral, cecocentral, or altitudinal scotomas

• If ‘No’ proceed to Question no 4
• If ‘Yes’, initially rule out the false-positive responses
• if the pt is not properly corrected or if media opacities create a blurriness or a doubling of the horizontal/vertical lines (monocular diplopia)

A Positive Or Absolute Para-central Scotoma as a Result Of A Healed Chorioretinal Scar

4.Do any of the horizontal or vertical lines that make up the squares appear wavy or bent?
• to rule out metamorphopsia and other forms distortions
• If ‘No’, may proceed to Question no 5
• If the answer is ‘Yes ’, the clinician must initially rule out false-positive responses
• if the patient is looking through the line
of a multifocal segment he/she is wearing or noticing the peripheral distortions of a progressive addition lens

Gaurav Bhardwaj
Central Metamorphopsia

Macropsia
A space-occupying
pathology (Tumor)
that forces the cones
closer causing the
Grid to Be Seen
distorted
Retinal image will fall
on more cones than
normal

A Pt with macular edema Or
Any other pathology that forces the cones apart
Retinal image will stimulate fewer cones than normal
And the lines Of the Amsler grid will be seen as smaller
Micropsia

• to rule out scintillating scotomas
• If ‘No’ the series of questions are complete
- can expect patient to have normal central visual field
Gaurav Bhardwaj
5. Is any part of the grid shimmering, flickering, or colored?
•If ‘Yes’, may herald the onset of a scotoma of retinal origin,
• particularly if early serous or hemorrhagic detachment is disrupting retinal topography

Dispensing Amsler grid
•First category- pt with progressive disease,
•-toxic maculopathy or atypical retinitis pigmentosa [field defect starts from center to periphery]
• -predisposed to developing significant alterations in the functional vision over time

Second category
•- patient with active disease, such as optic neuritis or macular neuroretinopathy
•whose visual acuity may improve or worsen within a relatively short time span

Third category
•- patient with recurrent disease, such as central serous retinopathy or toxoplasmic retinochoroiditis
• who may have already suffered vision loss and at risk of experiencing a reactivation of the disease process

ARMD

Berkeley Central Visual field Test•simple power-point presentation of a 50-
point scoring system
•central 10 degree of the visual field- dark lines on a white background used
•viewing distance-twice the distance b/w the long vertical red lines seen at the edge of each slide

•Test Targets
•subtend approx 30’of arc
•equivalent to 10/1000W or Goldmann-III
•20 targets –positioned superiorly and 30 inferiorly

•Five points are tested along 10 different hemi-meridians at eccentricities of 1°, 3°, 5°, 7° and 9°
•four hemi-meridians in the superior field (at 25°,
•65°, 115° and 165°), and
•six hemi-meridians in the inferior field (at 195°, 225°, 255°, 285°, 315°and 345°)

Technique:
•Pt. instructed to fixate at the central black dot point at the intersection of diagonal lines
•progress forward or backward through the sequence of the MS PowerPoint slides using the ARROW keys
• the subject responds using the MOUSE or giving a verbal response
•Between each of the 50 test slides, there was a blank slide with no test target.

•doesn’t detect metamorphopsia, •phenomenon of filling-in•and scotomas;
• however,does detect the loss of sensitivity and presence of maculopathy
Effectiveness of measuring the central field with the Berkeley field testSanjeeb K Mishra, Gauri S Shrestha, Hiral Korani
compared the efficacy of measuring the central VF field using BCFT and the Amsler grid test
Sensitivity, specificity Amsler grid test were found to be 80%, 100% resp,
• BCFT - 71%, 99%
•Conclusion: The BCFT test was as good as the Amsler grid test at detecting the presence of maculopathy.

Limitations of Amsler Grid
•high level of false-negative reports presence of scotomas was noted in 2% of
control subjects who had no symptoms of scotoma
•use of a preferred retinal locus away from the scotoma boundary
•asymmetry of attentional deployment in the peripheral retina
•phenomenon of filling-in

Tangent screen:
• aka Bjerrum’s screen ; Captimetry•Simplest form of perimetry, uses a white
tangent screen
•evaluates the central 30 ̊field at 1 m
•A black felt background with circular stitching every five degrees

BJE
RR
UM
’S
SC
REEN
.

• Black felt material is intended to absorb light
• The white test object is designed to reflect light
• Thus a light source directed at a tangent screen produces high contrast for a test target
• To calculate the angular position ,distance
from the fixation point is divided by the
fixation distance to obtain the tangent of
the angle
• Meridians of the tangent screen are
usually laid out with black stitching , like
dial of a clock
Tests Not only the light sensitivity of the retina but it also depends on motion detection

67
Technique
• Patient should seat at 1m from a 1m tangent screen and is asked to fixate the central fixation spot
• patient should be wearing their Rx
• non tested eye must be occluded
• Target should be brought from non seeing to seeing part of the field

68
• 1mm target (white) is moved from the central fixation point along the H-meridian to the right
• Central field using target → 1/1000W (central or paracentral scotoma)
• Paracentral scotoma → by presenting target at roughly clock intervals around 150 radius from fixation
• The blind spot should → using a 5/1000W target

.
•Initially physiological blind spot (15*
temporal to fixation pt) is charted which
corresponds to optic nerve head
•Blind spot dimensions:
• Horizontally 7-8 A
Vertically 10-11 A

• Blind spot should be plotted 1st so the pt understands everyone has a non seeing area normal
• and have a better understanding of what it is like when the target disappears
• Marking done with the black-headed pin

• Speed of the target is approx 50/sec• The smaller the target size the more
sensitive the test
• Thus isopter can be made to know the extension of the field as well as any type of scotomas

Examination of peripheral visual field

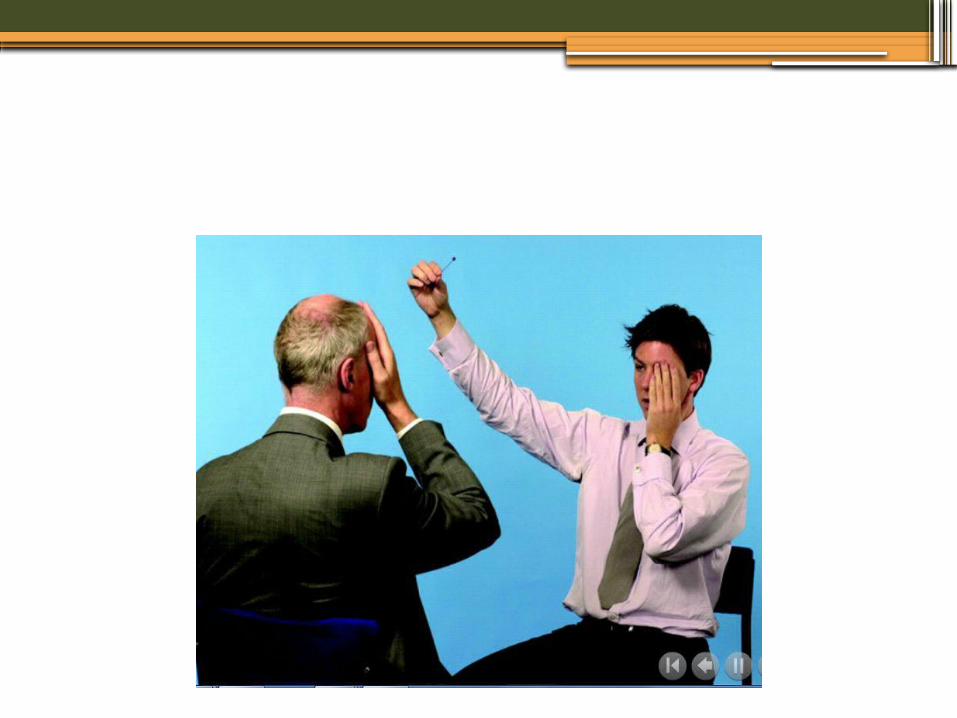
Confrontation visual field testing
•Simple and preliminary test, 120A of VF
•Examiner separated with the pt by a distance of about 60cm,
•will ask the pt to cover one eye and stare at the examiner
•When the patient covers his right eye, the examiner covers their left eye, and vice versa

Testing distance depends upon purpose of the test
To test temp 60 deg field; testing distance of 60cm is needed
The distance y would be equal to d

•Target is moved in a flat plane midway betn the pt and examiner
• from a position as far as possible from the line of sight inward until pt reports seeing it
•The process should be repeated in each of the quadrants for each eye separately

•If a defect is detected, re-examine that area and define it further
•Compares the pt's VF with examiner’s, so it does assume normal examiner VFs!
•Any discrepancies b/w the examiner’s and pt.’s VF should prompt further field examination

Demonstration

Lister’s Perimeter aka Arc Perimetry
•Extent of peripheral field
•Metallic semicircular arc, graded with degrees & white dot in centre for fixation
•Arc can be rotated in different meridians
•Pt seated facing arc, One eye occluded, fixates on the central white dot
•Test object (white, 3-5mm) moved along the arc from periphery towards centre
•Point which is 1st seen is registered on chart
•Arc moved 30 A each time & 12 readings noted
•Perimeter extent of Peripheral field is noted

Lister’s perimeter

Bernell Disc Perimeter
•a kinetic perimeter ; uses plastic disc formed in a semicircle
•To mark boundaries of the VF
•White target against black background- high contrast

To test the nasal and temporal boundary – disc oriented horizontally
To test superior and inferior boundary –disc oriented verically
A stimulus is mechanically moved across the arc from non seeing area to seeing area

•patient responses are punched onto recording paper
•Larger targets are used – useful in low vision pt

Quantitative Perimeters- Both central and peripheral
VF examination

Goldmann Perimetry
• 1945
•Can utilize both kinetic and static techniques using the on-off feature of the light stimulus
•Advantage of evaluating the peripheral field(outside 30deg)

• can test out to 180 degrees
• standardizes the background and target illumination
• standardizes most stimulus presentation factors

•However the central fixation region is smaller than tangent screen,
• so minor defects in this region are more difficult to map
•Stimulus could be varied by precise increments of brightness and size
•Stimulus could be easily presented to any area of the retina by use of a projection system

•Typically 2 or 3 isopters are plotted
•because relative defects that might not be plotted using stronger stimuli may be found by using weaker ones

•Scotomas are identified by static testing,
•then delineated by kinetic testing and their severity measured through variation of stimulus size and intensity


Interpretation
• The visual field is considered abnormal if:
▫ the threshold values are significantly brighter (0.5 log units or more) than the expected values
AND / OR
▫ Scotomas or depressions are present

Automated perimetry
•computer assisted examination (and not a fully automatic test)
•Results depend on the patient’s collaboration and the accuracy of the answers
•Field testing strategy mainly static field testing

•Test target is placed at a preselected field position, and is gradually raised until the patient detects it
•output is in the form of grayscale with the darkness of shading corresponding to decreased sensitivity in the field

Programmes in Humphrey for central field examination•Macula
•localized test ; thresholds 16 locations•within the central 5° with 2° spacing
• Each location is tested three times to provide better estimates

•Central 10-2
•provides a high-resolution test of the central 10° with a tight 2° grid, offset 1° from the meridians
• A total of 68 locations are used
• Useful in carefully defining central or paracentral scotomas
•Central 24-1
•Central 24°,40 points are used
•Central 30-1
•Central 30 , ̊ Central 76 point

Central 24-2
•Central 24 degrees; 6 deg spacing
•80 locations

•Central 30-2
•Central 30 deg, 6 deg spacing
•166 locations

For peripheral fields
•Peripheral 60 and 60-4
•Additional exploration of peripheral VF (beyond 30°)
•Peripheral 60 points ; test out to 60° with a uniform grid testing 60 additional locations

•Nasal Step Program
• Patients with possible nasal steps can be further explored
•with the nasal step program, which tests 12 locations up to 50° nasally
Full Field
•Tests out to 120 degrees
•Tests 120 points or 246 points
•Takes longer time

Examination program in OCTOPUS
G1/G2•Central 30 deg, 59 test locations
Program 32
•General threshold examination upto 76 test locations , 6 deg grid

Macula M1/M2
•Covers central 10 deg VF
•M1- 56 test locations in an equidistant grid pattern with a spacing of 2 deg
•M2- 45 test locations in central 4 deg area 0.7 deg spacing

•To conclude ,
•“Always screen the patients and test the suspects”
•So, a simple confrontation test can give valuable information about current status of pt’s visual field and prompt further field examination

References• Clinical procedures in optometry ; J.Boyd Estaridge,
Jimmy D. Barlett and John F. Amos
• Primary care optometry; Theodere Grosvenor
• VISUAL FIELD Examination and Interpretation; Third Edition; Thomas J. Walsh,
• Visual fields via the visual pathway ;Fiona Rowe
• Visual fields; Robbin cubbidge
• Internet

•THANK YOU








![Painting and visual information processing · Human vision comprises central and peripheral vision, organized in a rhombic-like visual field [4]. Peripheral vision is just as important](https://static.fdocuments.us/doc/165x107/5edd5f9aad6a402d66687127/painting-and-visual-information-processing-human-vision-comprises-central-and-peripheral.jpg)









