Center for Public Policy Priorities 1 Advocate’s Perspective: Advocate’s Perspective: Texas...
20
Center for Public Policy Priorities www.cppp.org 1 Advocate’s Perspective: Advocate’s Perspective: Texas Medicaid Reforms Health and Human Services Subcommittee, House Committee on Appropriations October 9, 2006 Anne Dunkelberg, Associate Director 900 Lydia Street - Austin, Texas 78702 Phone (512) 320-0222 – fax (512) 320-0227 - www.cppp.org
-
Upload
lambert-sutton -
Category
Documents
-
view
212 -
download
0
Transcript of Center for Public Policy Priorities 1 Advocate’s Perspective: Advocate’s Perspective: Texas...

Center for Public Policy Priorities www.cppp.org
1
Advocate’s Perspective:Advocate’s Perspective:Texas Medicaid Reforms
Health and Human Services Subcommittee,House Committee on Appropriations
October 9, 2006Anne Dunkelberg, Associate Director
900 Lydia Street - Austin, Texas 78702Phone (512) 320-0222 – fax (512) 320-0227 - www.cppp.org

Center for Public Policy Priorities www.cppp.org
2
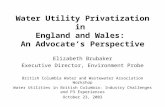
Texas Medicaid: Who it Helps
Children, 1,784,302
Disabled, 360,974
Elderly, 362,953
Poor Parents, 60,445
TANF Parent, 25,411
Maternity, 97,161
August 2006, HHSC data.
Total enrolled 8/1/2006: 2.68 million

Center for Public Policy Priorities www.cppp.org
3
Who Texas Covers Defines Which Reforms are Possible
• VERY few parents on Texas Medicaid• Very few enrollees are “optional”
coverage under federal law• Children, Pregnant Women, the
Elderly, and Persons with Disabilities:– Most of Texas Program– Special Protections in Fed law– Special concerns for their vulnerability

Center for Public Policy Priorities www.cppp.org
4
Enrollees Expenditures
Texas Medicaid Enrollees and Expenditures by Enrollment Group
(2004)
SOURCE: HHSC
Children 30%
Elderly & Disabled59%
Adults 11%Children70%
Elderly & Disabled
21%
Adults 9%
Total = 2.6 million Total = $14.7 billion

Center for Public Policy Priorities www.cppp.org
5
Children Account for Most Medicaid Enrollment Growth (U.S. 2000-2002)
SOURCE: Urban Institute, 2003; estimates of the 2000 MSIS Annual Person Level Summary Files; 2002 data from the CBO March 2003 baseline. *Ever Enrolled
Total Enrollment Growth = 6.6 Million
Children56%
(3.7 million)
Adults35%
(2.3 million)
Blind/Disabled6%
(0.4 million)Aged3%
(0.2 million)

Center for Public Policy Priorities www.cppp.org
6
Elderly & Disabled Account for Most Medicaid Spending Growth
(2000-2002)
DSH 0.7%
*Other 2.5%
Medicare Payments 2.1%
Total = $48.2 Billion.SOURCE: Urban Institute, 2003; estimates based on data from CMS, CMSO, Medicaid Statistical Information System (MSIS) and HCFA/CMS-64 Reports. * Other = Administrative costs and adjustments
Children20.8%
Adults15.4% Disabled
34.3%
Aged24.3%
Aged and Disabled58.6%
Children and Adults
36.2%

Center for Public Policy Priorities www.cppp.org
7What Medicare Does Not Cover: Major Medicaid Cost Driver
(FY2003)Medicare PremiumsPrescribed Drugs
Long-Term Care
Acute Care
Total Spending on Duals $105.4 billion
SOURCE: Urban Institute estimates for KCMU based on an analysis of MSIS and Financial Management reports (CMS Form 64).
Total Medicaid Spending $262.2 billion
Duals 40%
Other Beneficiaries
60%
66%
14%
15%
5%
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured

Center for Public Policy Priorities www.cppp.org
8Challenge: Potential for Savings is Greatest Among
Most Vulnerable• Cautious approach needed in cost containment
aimed at Elderly, Texans with Disabilities.• Savings most likely to take time to manifest –
significant reforms seldom yield immediate results.
• Key areas of Texas Medicaid pay such low rates that ability to reduce costs further is slim.
• HHSC/Texas Medicaid currently tackling enormous number of reforms & program modifications enacted in 2001, 2003, and 2005.

Center for Public Policy Priorities www.cppp.org
9
Medicaid is Growing Slower than Private Health Spending, 2000-
2003
6.9%
9.0%
12.6%
Medicaid Acute CareSpending Per
Enrollee
Health Care SpendingPer Person with
Private Coverage1
Monthly PremiumsFor Employer-
Sponsored Insurance2
1 Strunk and Ginsburg, 2004.2 Kaiser/HRET Survey, 2003.
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured

Center for Public Policy Priorities www.cppp.org
10
What Texas Spends
State "Own Source" Budget, 2006-07: $90 Billion
All Other, $7.0 b, 8%
Business/Econ Devel., $9.2 b, 10%
Criminal Justice, $8.3 b, 9%
Other Health & Human Services,
$5.1 b, 6%
Medicaid, $14.1 b, 16%
Higher Education,
$17.7 b, 20%
K-12 Education, $28.6 b, 31%
"Own Source" = Excludes Federal Funds
Sources: LBB, SB 1

Center for Public Policy Priorities www.cppp.org
11
Medicaid spending HAS grown Quickly over last Decade….
BUT:• Medicaid’s cost-per-client has been growing at
about HALF the rate of Employer-sponsored group insurance.– Texas and the US do need to control health care costs, but
not just in Medicaid. Targeting Medicaid alone will not solve the problems.
• Texas’ STATE DOLLAR Medicaid spending (that’s the money YOU have to raise, NOT the federal tax dollars we bring back home as Medicaid match) is till #3 AFTER K-12 education, and Higher Ed.
• Medicaid is the #1 source of federal dollars in our state budget, far outstripping the next highest area (usually highways).

Center for Public Policy Priorities www.cppp.org
12HHSC/Texas Medicaid:A VERY Full Plate
As HHSC has laid out:• Integrated Eligibility and Enrollment/TAA take-over of CHIP
Eligibility• Managed care Expansion: HMO, PCCM• Preferred Drug List/Prior Authorization/Pharmacy Benefits
Manager• Disease Management• Integrated Care Management/STAR+PLUS• 87 (!) SB 1188-related projects, including ER Utilization, Case
Management Optimization• Women’s Health Waiver• CHIP Perinatal• Medicaid Buy-In (workers with disabilities)• CHIP remiums assistance and 3-Share Waiver• 5 approved and 3 proposed UPL programs• Hospital Reimbursement Studies• Implementing MANDATORY DRA provisions: Long Term Care
Asset restrictions (will yield some savings); US Citizenship Documentation

Center for Public Policy Priorities www.cppp.org
13HHSC/Texas Medicaid:A VERY Full Plate
Many programs are underway which are likely to yield real efficiencies and savings,
But MOST have not yet had sufficient time to reach their full potential.
No “pig in a poke”: Independent Monitoring and Evaluation of all reforms should be required before new programs are continued and/or expanded statewide.
Beware the “Weekend Chore List” Syndrome:
Just because I ask my husband to re-paint all the trim on our house over the Columbus Day weekend does NOT mean he can really accomplish it in that short time.
Overloading the agency with too many simultaneous assignments for change risks undermining the promise and ultimate success of policies enacted in last 5 years.
Rx for near term: Slow Down, Fix, Perfect, Study what we are already doing. Be very selective & cautious in adding to the list we just read.

Center for Public Policy Priorities www.cppp.org
14
Texas’ Limited DRA Options
Cost Sharing options (very limited)Non-Preferred Rx: • DOCTORS, not patients, prescribe non-preferred
drugs. Make sure Dr.s Know when they prescribe something that will require a co-pay, and ask if family can afford.
• Monthly out-of pocket limits are needed to protect sick children, elders, persons with disabilities.
• Denial of Rx to those who cannot pay is OPTION, not mandate. Prescriber should be notified if patient cannot afford co-pay.
Numbers for whom other cost share allowed so small that not cost-effective to implement.

Center for Public Policy Priorities www.cppp.org
15
Texas’ Limited DRA OptionsBenchmark Benefits• Great majority of kids in Texas Medicaid already
in HMO care, which already uses a benchmark package, and state “wraps around” to provide comprehensive EPSDT services.
• Unclear what, if any additional advantage this DRA option offers Texas.
• Children on Texas Medicaid not getting enough preventive care or care management (Frew Lawsuit).
• Could entail significant administrative costs to change from this existing model without strong argument for doing so.

Center for Public Policy Priorities www.cppp.org
16
Texas’ Limited DRA Options
Great Opportunities to Better Serve Texans with Disabilities, the Elderly
• Medicaid Buy-In for Children with Disabilities• Money Follows Person Grants• LTC Partnerships (may only reach limited group,
but still would yield savings if so)• HCBS for mental health care

Center for Public Policy Priorities www.cppp.org
17
Texas’ Limited DRA Options
Health Opportunity Accounts: Caveats!
• Remember, HOAs were a COST, NOT savings to DRA
• MUST fully fund Account • A real pilot: limited area, STUDY results, and make
changes • RIGOROUS oversight of complete information for
clients about what can and cant be counted toward deductible, paid from account is CRITICAL.
• MUST be voluntary.

Center for Public Policy Priorities www.cppp.org
18
Advocates Concerns: DRA, plus other Options under 1115 Waivers
Beware comparing “Perfect Fantasy” to Imperfect Reality. – In 1993, we thought HMOs would solve
all our Medicaid cost problems.– Good ideas can be tough to implement:
IE&E sounded GREAT on paper!– MOST waivers and DRA options have
NOT been implemented yet: still fall in the Perfect Fantasy category.

Center for Public Policy Priorities www.cppp.org
19
Advocates Concerns: DRA, plus other Options under 1115 Waivers • WV:
– Children should not be punished for parents’ shortcomings (e.g., parent, not child chooses ER; child should not lose benefits for parental actions).
– Must doctors be “Enforcers”?• KY:
– Too many different ESI products could be impossible for state to monitor and guarantee kids get FULL EPSDT benefits
– Concerns about being assigned to “wrong” benefits package, and ease/speed of transition to “right” one
– Speed of transition back to standard package if ESI benefits are too limited
• Concerns about Florida Waiver are similar; again, these initiatives have no real track record yet: Perfect fantasy….

Center for Public Policy Priorities www.cppp.org
20
The Center for Public Policy Priorities encourages you to reproduce and distribute these slides, which were developed
for use in making public presentations.
If you reproduce these slides, please give appropriate credit to CPPP.
The data presented here may become outdated. For the most recent information, or to sign up for our free
e-mail updates, visit www.cppp.org
© CPPP