
Cell-mediated immunity in patients with mycosis fungoides in clinical remission. Effect of thymic...
4
Cell-Mediated Immunity in Patients with Mycosis Fungoides in Clinical Remission Effect of Thymic Humoral Factor on the lmmunocompetence of the Lymphocytes MICHAEL DAVID, MD,* BATYA SHOHAT, PHD,t NATAN TRAININ, MD, PHD,* AND ELEASAR FEUERMAN, MD*§ In 10 patients with mycosis fungoides (MF) who were in clinical remission following local treatment with nitrogen mustard, cell-mediated immunity was investigated by means of tests for lymphocytes, forming rosettes in the peripheral blood, and the graft-vs-host reaction as well as intradermal skin tests. The effect of thymic humoral factor (THF) on T lymphocytes with impaired immunecompetence was also investigated. The results provided evidence of various kinds of damage to the immunologic system in most of the patients. Of the 10 patients, 4 had low percentages of T cells. Eight of the 10 had a graft-vs.- host reaction which was weak or negative, and in 4 of these, the administration of THF to the lymphocytes induced an improvement in immunereactivity. These results together with other recently reported data indicate that the determination of cell-mediated immunity in patients with MF may be of prognostic importance. Those patients whose T lymphocytes respond to treatment with THF are probably the best candidates for immunotherapy . Cancer 46:41-44. 1980. YCOSIS FUNGOIDES (MF) is a cutaneous T-cell M lymphoma which in its advanced stage may develop into systemic l y m p h ~ m a . ~ It is now generally recognized that there is relationship between the pres- ence of malignancy and the competence of the cell- mediated immunity system, a finding which has opened a new therapeutic approach in the treatment of malig- nant diseases. There is every indication that therapy which enhances and stimulates the immunity system benefits the prognosis of patients with certain malig- nancies.g The thymic humoral factor (THF) isolated by Trainin et al. in Israel, has been found to restore im- munoreactivity in animals thymemectomized at birth.I7 Recently, it has also given encouraging results in clini- cal trials performed in I ~ r a e l . ~ ~ ~ ~ " ~ ~ ~ From the *Department of Dermatology and tunit of Cellular Immunology, Beilinson Medical Center, Tel Aviv University Sackler Medical School, Israel. Supported in part by a grant from the Chief Scientist Office, Ministry of Health, Israel. $ Head, Department of Cellular Biology, Weizman Institute, Rehovot. 8 Head and Chairman, Department of Dermatology, Beilinson Medical Center, and Professor Sackler School of Medicine, Tel Aviv University. Address for reprints: Professor E J Feuerman, Department of Dermatology Beilinson Medical Center, Petah Tiqva, Israel. Accepted for publication July 10, 1979. A number of investigators have studied the im- munecompetence of patients with MF, both during treatment and in untreated cases, with conflicting re- In this report, we present the findings of a study in which we investigated the immunocompetence of patients with MF who were in a state of clinical re- mission following topical treatment with nitrogen mustard and the effect of THF on the function of their T lymphocytes. sults .3,7,8,10,16,22.26 Materials and Methods The 10 patients with MF who were studied were all in a state of clinical remission following local treat- ment with only nitrogen mustard (Table 1). At the time of the investigation, Patients 2 and 3 continued to re- ceive treatment. The nitrogen mustard was applied only to the lesions, once a day, three times weekly. The others stopped the treatment at least six months before the tests were performed. Three of the 10 pa- tients reported transient skin irritation during local treatment. No patient had experienced allergic contact dermatitis. Patients 2 and 10 had also received radio- therapy in the past because of tumoral lesions. No patient showed lymphadenopathy or hepatospleno- megaly when examined during the investigation. The 0008-543X/80/0701/0041 $0.70 0 American Cancer Society 41
-
Upload
michael-david -
Category
Documents
-
view
212 -
download
0
Transcript of Cell-mediated immunity in patients with mycosis fungoides in clinical remission. Effect of thymic...
Cell-Mediated Immunity in Patients with Mycosis Fungoides in Clinical Remission
Effect of Thymic Humoral Factor on the lmmunocompetence of the Lymphocytes
MICHAEL DAVID, MD,* BATYA SHOHAT, PHD,t NATAN TRAININ, MD, PHD,* AND ELEASAR FEUERMAN, MD*§
In 10 patients with mycosis fungoides (MF) who were in clinical remission following local treatment with nitrogen mustard, cell-mediated immunity was investigated by means of tests for lymphocytes, forming rosettes in the peripheral blood, and the graft-vs-host reaction as well as intradermal skin tests. The effect of thymic humoral factor (THF) on T lymphocytes with impaired immunecompetence was also investigated. The results provided evidence of various kinds of damage to the immunologic system in most of the patients. Of the 10 patients, 4 had low percentages of T cells. Eight of the 10 had a graft-vs.- host reaction which was weak or negative, and in 4 of these, the administration of THF to the lymphocytes induced an improvement in immunereactivity. These results together with other recently reported data indicate that the determination of cell-mediated immunity in patients with MF may be of prognostic importance. Those patients whose T lymphocytes respond to treatment with THF are probably the best candidates for immunotherapy .
Cancer 46:41-44. 1980.
Y C O S I S FUNGOIDES (MF) is a cutaneous T-cell M lymphoma which in its advanced stage may develop into systemic l y m p h ~ m a . ~ It is now generally recognized that there is relationship between the pres- ence of malignancy and the competence of the cell- mediated immunity system, a finding which has opened a new therapeutic approach in the treatment of malig- nant diseases. There is every indication that therapy which enhances and stimulates the immunity system benefits the prognosis of patients with certain malig- nancies.g
The thymic humoral factor (THF) isolated by Trainin et al. in Israel, has been found to restore im- munoreactivity in animals thymemectomized at birth.I7 Recently, it has also given encouraging results in clini- cal trials performed in I ~ r a e l . ~ ~ ~ ~ " ~ ~ ~
From the *Department of Dermatology and tun i t of Cellular Immunology, Beilinson Medical Center, Tel Aviv University Sackler Medical School, Israel.
Supported in part by a grant from the Chief Scientist Office, Ministry of Health, Israel.
$ Head, Department of Cellular Biology, Weizman Institute, Rehovot.
8 Head and Chairman, Department of Dermatology, Beilinson Medical Center, and Professor Sackler School of Medicine, Tel Aviv University.
Address for reprints: Professor E J Feuerman, Department of Dermatology Beilinson Medical Center, Petah Tiqva, Israel.
Accepted for publication July 10, 1979.
A number of investigators have studied the im- munecompetence of patients with MF, both during treatment and in untreated cases, with conflicting re-
In this report, we present the findings of a study in which we investigated the immunocompetence of patients with MF who were in a state of clinical re- mission following topical treatment with nitrogen mustard and the effect of T H F on the function of their T lymphocytes.
sults .3,7,8,10,16,22.26
Materials and Methods
The 10 patients with MF who were studied were all in a state of clinical remission following local treat- ment with only nitrogen mustard (Table 1). At the time of the investigation, Patients 2 and 3 continued to re- ceive treatment. The nitrogen mustard was applied only to the lesions, once a day, three times weekly. The others stopped the treatment at least six months before the tests were performed. Three of the 10 pa- tients reported transient skin irritation during local treatment. No patient had experienced allergic contact dermatitis. Patients 2 and 10 had also received radio- therapy in the past because of tumoral lesions. No patient showed lymphadenopathy or hepatospleno- megaly when examined during the investigation. The
0008-543X/80/0701/0041 $0.70 0 American Cancer Society
41
42 CANCER July 1 1980 Vol. 46
TABLE 1. Clinical Material
Sex, Clinical stage Duration of Patient age (years) before treatment remission (months)
1 M, 73 I 10 2 M, 63 11-111 18 3 M, 65 I 6 4 M, 44 I 12 5 F, 48 1-11 12 6 M, 73 1-11 7 7 M, 70 I 6 8 M, 37 I 30 9 M, 36 I 20
10 F, 65 11-111 30 ~
The control group composed 24 men and 8 women ranging in age from 32 to 70 years (mean age, 54 years).
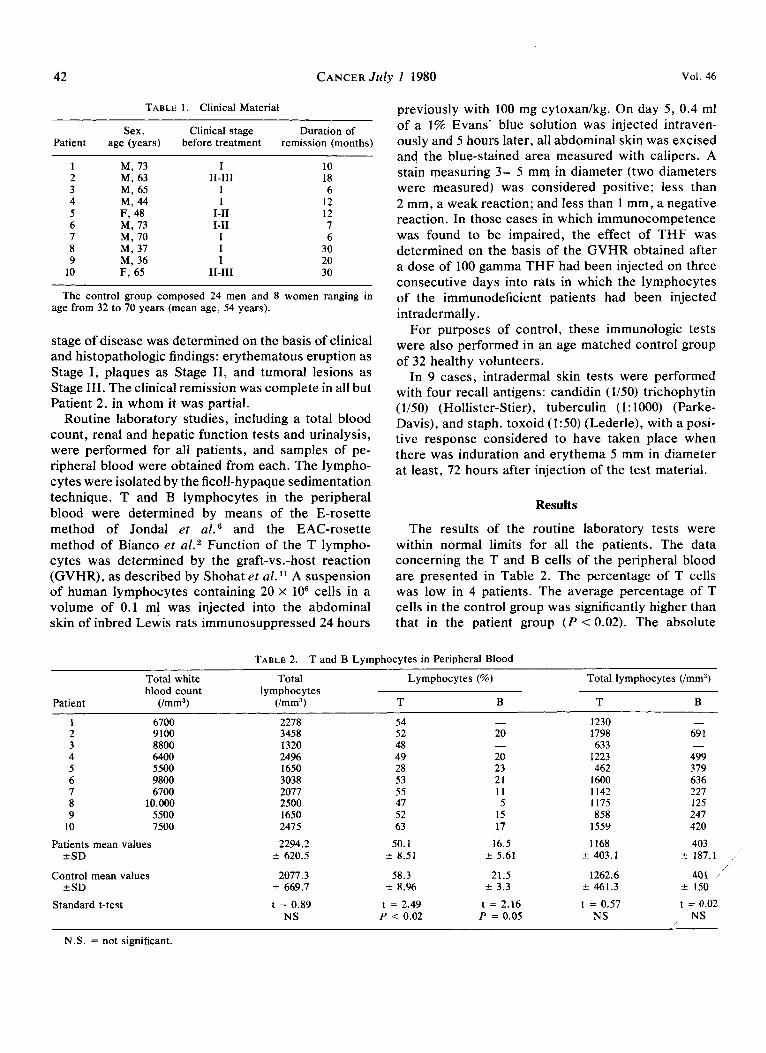
stage of disease was determined on the basis of clinical and histopathologic findings: erythematous eruption as Stage I , plaques as Stage 11, and tumoral lesions as Stage 111. The clinical remission was complete in all but Patient 2, in whom it was partial.
Routine laboratory studies, including a total blood count, renal and hepatic function tests and urinalysis, were performed for all patients, and samples of pe- ripheral blood were obtained from each. The lympho- cytes were isolated by the ficoll-hypaque sedimentation technique. T and B lymphocytes in the peripheral blood were determined by means of the E-rosette method of Jondal et af .6 and the EAC-rosette method of Bianco er af .* Function of the T lympho- cytes was determined by the graft-vs.-host reaction (GVHR), as described by Shohat et al." A suspension of human lymphocytes containing 20 x lo6 cells in a volume of 0.1 ml was injected into the abdominal skin of inbred Lewis rats immunosuppressed 24 hours
previously with 100 mg cytoxadkg. On day 5 , 0.4 ml of a 1% Evans' blue solution was injected intraven- ously and 5 hours later, all abdominal skin was excised and the blue-stained area measured with calipers. A stain measuring 3- 5 mm in diameter (two diameters were measured) was considered positive; less than 2 mm, a weak reaction; and less than 1 mm, a negative reaction. In those cases in which immunocompetence was found to be impaired, the effect of THF was determined on the basis of the GVHR obtained after a dose of 100 gamma THF had been injected on three consecutive days into rats in which the lymphocytes of the immunodeficient patients had been injected intradermally .
For purposes of control, these immunologic tests were also performed in an age matched control group of 32 healthy volunteers.
In 9 cases, intradermal skin tests were performed with four recall antigens: candidin (1/50) trichophytin (1/50) (Hollister-Stier), tuberculin (1: 1000) (Parke- Davis), and staph. toxoid (1:50) (Lederle), with a posi- tive response considered to have taken place when there was induration and erythema 5 mm in diameter at least, 72 hours after injection of the test material.
Results
The results of the routine laboratory tests were within normal limits for all the patients. The data concerning the T and B cells of the peripheral blood are presented in Table 2. The percentage of T cells was low in 4 patients. The average percentage of T cells in the control group was significantly higher than that in the patient group ( P < 0.02). The absolute
TABLE 2. T and B Lymphocytes in Peripheral Blood
Total white Total Lymphocytes (%) Total lymphocytes (/mm9) blood count lymphocytes
Patient (/mm3) (/mm3) T B T B
1 6700 2278 54 - 1230 - 2 9100 3458 52 20 1798 69 1 3 8800 1320 48 - 633 - 4 6400 2496 49 20 1223 499 5 5500 1650 28 23 462 379 6 9800 3038 53 21 1600 636 7 6700 2077 55 11 1142 227 8 10.000 2500 47 5 1175 125 9 5500 1650 52 15 858 247
10 7500 2475 63 17 1559 420
Patients mean values 2294.2 50.1 16.5 1168 403 ? SD ? 620.5 2 8.51 ? 5.61 f 403.1 5 187.1
Control mean values 2071.3 58.3 21.5 1262.6 401 +SD ? 669.7 f 8.96 % 3.3 ? 461.3 ? 150
Standard t-test t = 0.89 t = 2.49 t = 2.16 t = 0.57 t = 0.02
/
NS P < 0.02 P = 0.05 NS NS
N.S. = not significant.

No. 1 MYCOSIS FUNGOIDES . David et al. 43
TABLE 3. Immunocompetence of the Lymphocytes and Delayed Hypersensitivity
Patient
Number of lymphocytes
(Imrn')
1 2 3 4 5 6 7 8 9
10
Normal Normal Low Normal Low Normal Normal Normal Low Normal
GVHR
Negative l m m x 2 m m 1 mm x 1.5 mm 5 m m x 4 m m
Negative Negative
5 mm x 5 mm 2 mm x 1.5 mm 1 mm x 1.5 mm
Negative
GVHR + THF
Intradermal skin tests
(positive/total)
3 m m x 4 m m 4 mm x 4.5 rnm
1.5 mm x 2 mm ND
l rnrnx2rnrn Negative
ND 1.5 mm x 1.5 rnm
4 mm x 5 mm Negative
014 014 0/4 214 0/4 014 ND 014 I I4 114
GVHR = graft-vs.-host reaction; THF = thymic humoral factor; ND = not done.
number of T lymphocytes per mm3 was decreased in 3 patients, yet the average of the absolute number of T cells fell within the range of values found in the control group, with no statistically significant dif- ference between the two groups. The average per- centage of B cells in the control group was significantly higher than that in the patient group ( P = 0.05), but the average of the absolute number of B cells fell within the range of values found in the control group without a statistically significant difference.
The data concerning the cell-mediated immunity of the 10 patients, on the basis of the GVHR and skin tests performed, are presented in Table 3. The GVHR was positive in 2 patients, weak in 4, and negative in 4. Of the 32 control subjects, 30 had positive GVHR. The lymphocytes of 4 of the 8 patients whose T lymphocyts had not mounted a positive local xeno- geneic GVHR were found to regain their immuno- competence following treatment with THF. In 6 pa- tients, all of the intradermal skin tests performed were negative, i .e. , more than half of these patients were anergic. Two patients were hypoergic (1/4) and only 1 patient gave a positive response to two of the four of the antigens. These results indicate that there is a correlation between the function of the T lympho- cytes as measured by the local GVHR and the de- layed hypersensitivity skin reaction in these patients.
Discussion
A number of investigators, including Zucker- Franklin et al. ," Braylan et al. ,3 and Tan et al. ,16 have reported normal and even high values of rosette- forming lymphocytes in the peripheral blood of patients with MF. In contrast, Mendes et al.,R Mackie et ~ l . , ~ Zacharia et u L . , ' ~ and Nordqvist'" all reported de- creased levels in patients with MF. The function of the lymphocytes in these patients was found to be normal by some investigators who used a blastic transforma- tion method.' In our study, although in most patients
the levels of T cells were normal, cell-mediated im- munity was found to be impaired in almost all of them. Thus, the level of T lymphocytes in the peripheral blood is not necessarily an indication of the function of the cell-mediated immunity system, a finding which further supports the observations of Shohat et al. in their investigation of the immunologic mechanisms in cases of malignancy.13
The difference between our results and those men- tioned above may be due to the different methods of testing the T lymphocytes function. It is possible that the GVHR test is a more sensitive method of revealing immunedeficiency.
The role of cell-mediated immunity in depressing the proliferation of malignant cells has already been noted. But there is also evidence that malignant dis- eases may damage the immunity system, as indicated by the improvement in immunoreactivity found after operative removal of the malignancy. l 4 , I s
The course of MF is characterized by exacerbations following remission, for which reason some investi- gators advise that treatment be continued even during remission.21 Vonderheid et al . reported that patients who were DNCB-sensitive achieved clinical remission sooner than those who were not.21 Taken together with our finding of varying amounts of damage to the immunologic system, it may be concluded that these patients should be committed to intensive follow up including regular investigation of their immunocom- petence. It is possible that a decrease in immuno- reactivity in a patient who is in a stage of remission may predict a clinical exacerbation of the disease.
Nitrogen mustard is an immunosuppressive agent; therefore, it cannot be excluded for certain that treatment with it is responsible for, or contributes to, the impairment of T cell function. The fact that the majority of patients received local treatment only, and it was stopped many months before the investigation, diminishes this possibility. Furthermore, no potential

44 CANCER July 1 1980 Vol. 46
side-effects of the treatment such as lymphopenia or bone marrow depression were found. Thus, in our opinion, the possibility that the treatment is responsible for the damage of T cells is small.
Only a few attempts at using immunotherapy in MF have been reported. Some investigators have used transfer factor, with varying Recently, Vonderheid reported encouraging results after in- ducing delayed hypersensitivity with DNCB and mechlorethamine.21
In several of our cases, the injection of T H F im- proved the function of previously deficient T cells inoculated into rats. This supports the finding of others that T H F is able to induce maturation of T cells.12 Furthermore, in vitro preincubation of T H F with normal human lymphocytes has been found to increase the GVH reactivity on their intradermal inoculation into rats with suppressed immunity systems.lR Recent clinical trials with T H F in Israel have yielded en- couraging results, with an improvement in immune- competence having been achieved in cases of subacute sclerosing panencephalitis, l9 in cases of lymphopro- liferative neoplasms affected by v a r i ~ e l l a , ~ ~ ~ ~ ~ and in cases of severe disseminated adenovirus infection.20 It is noteworthy that Goldstein et ~ 1 . ~ have treated cancer patients, including 2 with MF, with Thymosin. They found that more than 75% of the patients showed a significant increase in absolute number of E-rosettes.
All of the above should encourage us to use this hor- mone in vivo in patients with MF. It may be presumed that those patients whose T lymphocytes show matura- tion following treatment with T H F in rats are good can- didates for immunotherapy with this hormone.
REFERENCES
1 . Arnold LH, Rees BR. American academy of Dermatology. Cufis 1976; 17:896.
2. Bianco C, Patrick R, Nussenzweig V. A population of lympho- cytes bearing a membrane receptor for antigen-antibody comple- ment complexes. Separation and characterization. J Exp Med 1970; 132:702.
3. Braylan R, Variakojis D, Yachnin S. The Sezary syndrome lymphoid cell-abnormal mitogenic responsiveness and surface prop- erties (Abstr.). Clin Res 1973; 21:870.
4. Goldstein AL, Rosco JL. Thymosin for immunodeficiency diseases and cancer. Comp Ther 1978; 4:49.
5 . Edelson R. NIH conference: cutaneous T-cell lymphoma; the Sezary syndrome, mycosis fungoides and related disorders. Ann Infern Med 1975; 831534.
6. Jondal M, Holm G, Wigzell H. Surface markers on human T and B lymphocytes, a large population of lymphocytes forming non-immune rosettes with sheep red blood cells. J Exp Med 1972; 136:207.
7. Mackie R, Sless FR, Cochran R, De Sousa M. Lymphocyte abnormalities in mycosis fungoides. Br J Derm 1976; 94: 173.
8. Mendes NF, Mussati CC, Tolnai EA. T and B lymphocyte membrane markers in cells from patients with leukemia and lymphoma. Int Arch Allergy Appl Immunol 1974; 46:695.
9. Morton DZ, Eilber RR, Holmes EC, et al. BCG immuno- therapy of malignant melanoma. Summary of a seven year ex- perience. Ann Surg 1974; 180:635.
10. Nordqvist CB, Kinney PJ. T and B cells and cell-mediated immunity in mycosis fungoides. Cancer 1976; 37:714.
11. Shohat B, Joshua H. Assessment of the functional activity of human lymphocytes in malignant disease by the local graft- versus-host reaction in rats and T-rosettes forming cell test. Clin Exp Immunol 1976; 24534.
12. Shohat B, Spitzer S, Topilsky M, Trainin N. Immunological profile in sarcoidosis patients. The in vifro and in vivo effect of thymic humoral factor. Biomedicine 1978; 29:92.
13. Shohat B, Joshua H, Kott A, Urca I. Cellular immuno- competence in patients with malignant tumors of the gastrointestinal tract. Isr J Med Sci 1976; 12:1463.
14. Shohat B, Kott A, Joshua H, Urca I . Cellular immuno- competence in adenocarcinoma of the breast. Harefuah 1975; 89549.
15. Shohat B, Perry H, Servadio C. Cellular immune competence in patients with transitional cell carcinoma of the bladder. J CIin Immunopathol Immunol 1978; 10:79.
16. Tan HRS, Betterworth MC, McLanghlin H, Malka S, Samman DP. Mycosis fungoides, a disease of antigen persistence. Br J Dermatol 1974; 91:607.
17. Training N, Small M, Zipori D, Umiel T, Kook AI, Rotter V. Characteristics of THF, a thymic hormone. In: Van Bekkum D, ed. Biological Activity of Thymic Hormones. Rotterdam: Kooyker Scientific Publication, 1975: 117.
18. Trainin N, Rotter V, Yakir Y, Handzel Z, Shohat B, Zaizov R. Biochemical and biological properties of T H F in animal and human models (Abstr.). Conference on subcellular factors in im- munity, New York City 1979.
19. Varsano I, Danon Y, Gaber L, Livni E , Shohat B, Yakir, Y, Shneour A, Trainin N. Reconstitution of T-cell function in patients with subacute sclerosing panencephalitis treated with thymus humoral factor. Isr J Med Sci 1976; 12:1168.
20. Varsano J, Schonfeld TM, Matoth B, et al. Severe dis- seminated adenovirus infection successfully treated with a thymic humoral factor, THF. Acta Paediaf Scand 1977; 66:329.
21. Vonderheid CE, Van Scott JE, Johnson CW, Grekin AD, Asbell 0s. Topical chemotherapy and Immunotherapy of mycosis fungoides. Arch Dermafol 1977; 113:454.
22. Zachariae H, Ellegaard J, Grunnet E , Sogaard H, Thulin H. T and B cells and IgE in mycosis fungoides. Acta Dermatov 1975; 55:466.
23. Zachariae H, Grunnet G, Ellegaard J, Thestrup-Pederson K. Transfer factor as additional therapeutic agent in mycosis fungoides. Acta AIlergol 1975; 30:272.
24. Zaizov R, Vogel R, Cohen J, et al. Thymic hormone therapy in immunosuppressed children with lympho-proliferative neoplasm and generalized varicella. Biomedicine 1977; 27: 105.
25. Zaizov R, Vogel R, Walach B, et al. The effect of T H F in lympho and myelo proliferative diseases in children. (Abstr.). Conference on Subcellular Factors in Immunity, New York City, 199.
26. Zucker-Franklin D, Melton WJ, Quagliata F. Ultrastructural, immunologic and functional studies on Sezary cells-a neoplastic variant thymus derived (T) lymphocytes. Proc Nut Acad Sci USA 1974; 71:1887.











![Significance of CD30 Expression by Epidermotropic T Cells ... · diagnosis included LyP, lymphomatoid pityriasis lichenoides and “pityriasis lichenoides-like” mycosis fungoides.[7,8]](https://static.fdocuments.us/doc/165x107/60223092b9e61714693c3a28/significance-of-cd30-expression-by-epidermotropic-t-cells-diagnosis-included.jpg)





