celiac disease
37
presented By:Evana AL Youssef Supervisor: Dr.Sana Janakat 14-12-2011 Celiac Disease Jordan University of Science and Technology Faculty of Agriculture Department of Nutrition and Food science
-
Upload
evana-alyoussef -
Category
Health & Medicine
-
view
4.868 -
download
1
description
• Coeliac disease is a genetically-determined chronic inflammatory intestinal disease induced by an environmental precipitant, gluten.• Patients with the disease might have mainly non-gastrointestinal symptoms, and as a result patients present to various medical practitioners.• Epidemiological studies have shown that coeliac disease is very common and affects about one in 250 people.• The disease is associated with an increased rate of osteoporosis, autoimmune diseases, and malignant disease, especially lymphomas.• The mechanism of the intestinal immune-mediated response is not completely clear, but involves an HLA-DQ2 or HLA-DQ8 restricted T-cell immune reaction in the lamina propria as well as an immune reaction in the intestinal epithelium.
Transcript of celiac disease

presented By:Evana AL YoussefSupervisor: Dr.Sana Janakat 14-12-2011
presented By:Evana AL YoussefSupervisor: Dr.Sana Janakat 14-12-2011
Celiac DiseaseCeliac Disease
Jordan University of Science and TechnologyFaculty of AgricultureDepartment of Nutrition and Food science

© 2004, 2002 Elsevier Inc. All rights reserved.
Outline:Outline:
What is Celiac Disease?
What is gluten
Signs and Symptoms
Mechanism Of Action
Risk Factors for Celiac Disease
Diagnosis
Pathology
What is Celiac Disease?
What is gluten
Signs and Symptoms
Mechanism Of Action
Risk Factors for Celiac Disease
Diagnosis
Pathology

© 2004, 2002 Elsevier Inc. All rights reserved.
Outline…..cont:Outline…..cont:
Treatment
Follow-up
Summary
References
Treatment
Follow-up
Summary
References

© 2004, 2002 Elsevier Inc. All rights reserved.
Celiac Disease:Celiac Disease:
Malabsorption damaged small intestine
Inherited Autoimmune Disorder
Intolerance to Gluten Wheat, Ray and Barley
Malabsorption damaged small intestine
Inherited Autoimmune Disorder
Intolerance to Gluten Wheat, Ray and Barley

© 2004, 2002 Elsevier Inc. All rights reserved.
Celiac Disease−CauseCeliac Disease−Cause
Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002.
© 2004, 2002 Elsevier Inc. All rights reserved.
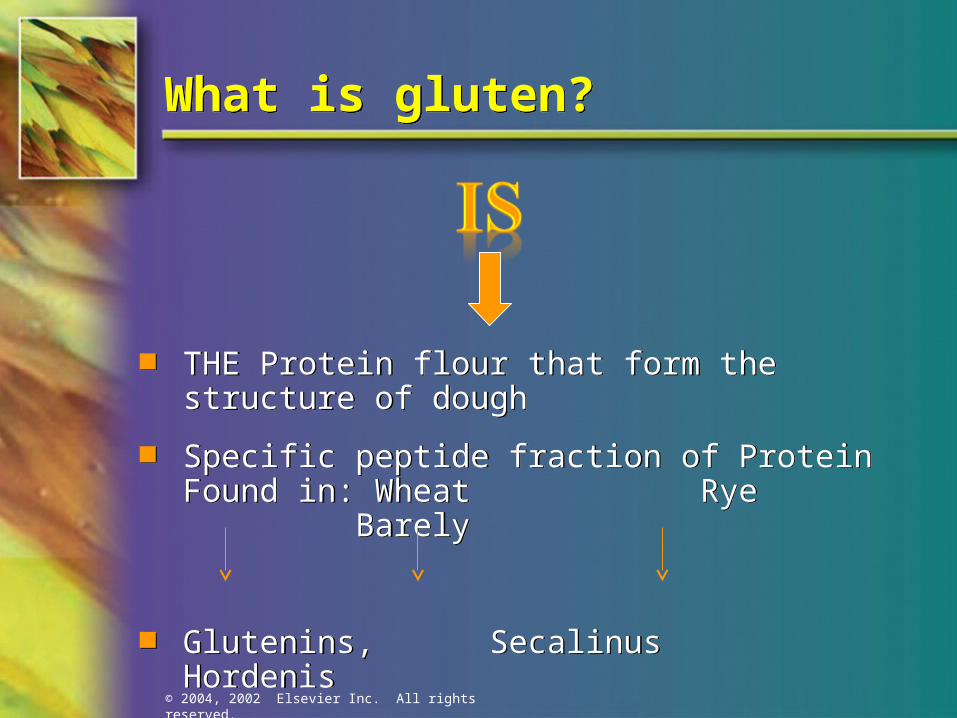
What is gluten?What is gluten?
THE Protein flour that form the structure of dough
Specific peptide fraction of Protein Found in: Wheat Rye Barely
Glutenins, Secalinus Hordenis
Gliadins.
THE Protein flour that form the structure of dough
Specific peptide fraction of Protein Found in: Wheat Rye Barely
Glutenins, Secalinus Hordenis
Gliadins.

© 2004, 2002 Elsevier Inc. All rights reserved.

© 2004, 2002 Elsevier Inc. All rights reserved.
What are symptoms of CD:What are symptoms of CD:

© 2004, 2002 Elsevier Inc. All rights reserved.
Small Intestine villi:Small Intestine villi:
Absorption
Normal villiFlattened villi
Malabsorption

© 2004, 2002 Elsevier Inc. All rights reserved.
Celiac Disease−PathophysiologyCeliac Disease−Pathophysiology
(Adapted from Bray GA. Gray DS, Obesity, part 1: Pathogenisis. West J Med 149:429, 1988; and Lew EA, Garfinkle L; Variations in mortality by weight among 750,000 men and women. J Clin Epidemiol 32:563, 1979.)
Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002.

© 2004, 2002 Elsevier Inc. All rights reserved.
Mechanism:Mechanism:
Body attacks normal tissue resulting in damage to lining of small intestinal villi
Villi contain blood vessels which absorb nutrients
Villi increase area for absorption of nutrients
Body attacks normal tissue resulting in damage to lining of small intestinal villi
Villi contain blood vessels which absorb nutrients
Villi increase area for absorption of nutrients

© 2004, 2002 Elsevier Inc. All rights reserved.
Mechanism…..cont.:Mechanism…..cont.:
Digested nutrients are carried away by circulating blood
If villi are damaged, vitamins, minerals, calcium, carbohydrates, protein, and fats are not absorbed well
Digested nutrients are carried away by circulating blood
If villi are damaged, vitamins, minerals, calcium, carbohydrates, protein, and fats are not absorbed well

© 2004, 2002 Elsevier Inc. All rights reserved.
Mechanisms:Mechanisms:

© 2004, 2002 Elsevier Inc. All rights reserved.
Mechanism:Mechanism:

© 2004, 2002 Elsevier Inc. All rights reserved.
Risk Factor of CDRisk Factor of CD
Malignant disease: lymphomas
Deficiencies in folic acid, vitamin B12, fat-soluble & vitamins
Increased mortality due to increased risk of malignancy
Type 1 diabetes mellitus
Arthritis, Osteoporosis
Malignant disease: lymphomas
Deficiencies in folic acid, vitamin B12, fat-soluble & vitamins
Increased mortality due to increased risk of malignancy
Type 1 diabetes mellitus
Arthritis, Osteoporosis

© 2004, 2002 Elsevier Inc. All rights reserved.
Risk Factor….cont:Risk Factor….cont:
endomysial antibody negative
few respond to steroids
Down syndrome
Unexplained iron-deficiency anemia
Dermatitis herpetiformis
endomysial antibody negative
few respond to steroids
Down syndrome
Unexplained iron-deficiency anemia
Dermatitis herpetiformis

© 2004, 2002 Elsevier Inc. All rights reserved.
Dermatitis Herpetiformis:Dermatitis Herpetiformis:

© 2004, 2002 Elsevier Inc. All rights reserved.
Differential Diagnosis of Celiac Disease Differential Diagnosis of Celiac Disease
Anorexia nervosa
Autoimmune enteropathy
Bacterial overgrowth
Collagenous sprue
Crohn's disease
Human immunodeficiencyvirus enteropathy
Infective gastroenteritis
Anorexia nervosa
Autoimmune enteropathy
Bacterial overgrowth
Collagenous sprue
Crohn's disease
Human immunodeficiencyvirus enteropathy
Infective gastroenteritis
Irritable bowel syndrome
Ischemic enteritis
Lactose intolerance
Pancreatic insufficiency
Soy protein intolerance
Intestinal lymphoma
Irritable bowel syndrome
Ischemic enteritis
Lactose intolerance
Pancreatic insufficiency
Soy protein intolerance
Intestinal lymphoma

© 2004, 2002 Elsevier Inc. All rights reserved.
Haw is celiac disease diagnosed:Haw is celiac disease diagnosed:
Initial Blood Tests
Historical evaluated
Serology tests
Biopsy of small intestine
Initial Blood Tests
Historical evaluated
Serology tests
Biopsy of small intestine
© 2004, 2002 Elsevier Inc. All rights reserved.
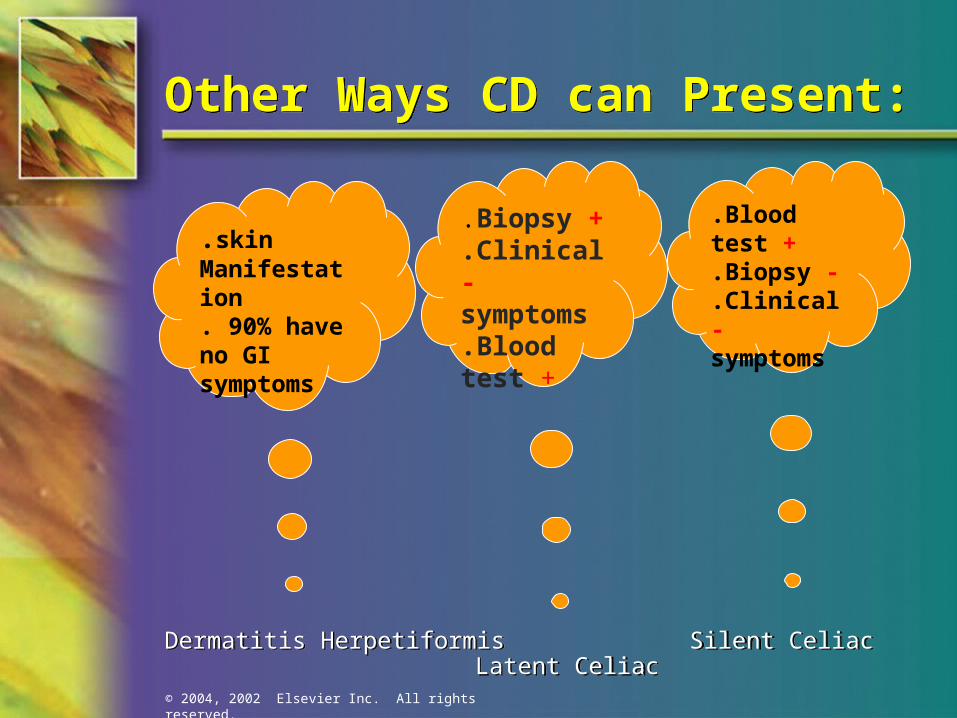
Other Ways CD can Present:Other Ways CD can Present:
Dermatitis Herpetiformis Silent Celiac Latent Celiac
Dermatitis Herpetiformis Silent Celiac Latent Celiac
.Blood test +
.Biopsy -
.Clinical - symptoms
.Biopsy +
.Clinical -symptoms.Blood test +
.skinManifestation . 90% have no GI symptoms

© 2004, 2002 Elsevier Inc. All rights reserved.
Serology TestsSerology Tests
Kind subscription
Anti-tissue transglutaminase antibody (tTG – IgA and IgG)
most sensitive
Anti-endomysial antibody (EMA-IgA
highly specific marker
Anti-deaminated gliadin peptide (DGP – IgA and IgG)
(-) tTG or EMA OR IgA deficient
Anti-gliadin antibody (AgA – IgG and IgA)
used for children < 2 yr

© 2004, 2002 Elsevier Inc. All rights reserved.
Endoscopic and biopsy findings in patients with and without celiac diseaseEndoscopic and biopsy findings in patients with and without celiac disease
Normal small intestine
Celiac Disease
Normal villi
Villous atrophy

© 2004, 2002 Elsevier Inc. All rights reserved.
Normal Human Duodenal Mucosa (A) and Peroral Small Bowel Biopsy Specimen (B) from a Patient with Gluten Enteropathy
Normal Human Duodenal Mucosa (A) and Peroral Small Bowel Biopsy Specimen (B) from a Patient with Gluten Enteropathy
(From Floch MH. Nutrition and Diet Therapy in Gastrointestinal Disease. New York: Menum Medical Book Co., 1981)

© 2004, 2002 Elsevier Inc. All rights reserved.
Diagnostic:Diagnostic:

© 2004, 2002 Elsevier Inc. All rights reserved.
COROLLARY: ALWAYS TEST FOR TOTAL SERUM IGA WHEN LOOKING FOR CELIAC DISEASECOROLLARY: ALWAYS TEST FOR TOTAL SERUM IGA WHEN LOOKING FOR CELIAC DISEASE
In this subset of patients, research shows that IgG-EMA and IgG-TTG can be detected and are as sensitive and as specific for the diagnosis of celiac disease.
In this subset of patients, research shows that IgG-EMA and IgG-TTG can be detected and are as sensitive and as specific for the diagnosis of celiac disease.

© 2004, 2002 Elsevier Inc. All rights reserved.
Pathology:Pathology:
many mucosal enzymes are altered due to the damage to the absorptive cells
decrease in disaccharides, peptidases, alkaline phosphatase, ATPase, and esterase Length of small intestine varies from patient to patient
correlates with severity of clinical symptoms
usually proximal small intestine more severely involved
many mucosal enzymes are altered due to the damage to the absorptive cells
decrease in disaccharides, peptidases, alkaline phosphatase, ATPase, and esterase Length of small intestine varies from patient to patient
correlates with severity of clinical symptoms
usually proximal small intestine more severely involved

© 2004, 2002 Elsevier Inc. All rights reserved.
Pathology:Pathology:
Loss of normal villous structure
increase in the number of intraepithelial lymphocytes and gamma/delta T cells
These changes decrease the amount of epithelial surface available for digestion and absorption in the involved bowel
Loss of normal villous structure
increase in the number of intraepithelial lymphocytes and gamma/delta T cells
These changes decrease the amount of epithelial surface available for digestion and absorption in the involved bowel

© 2004, 2002 Elsevier Inc. All rights reserved.
Treatment: Treatment:
THE GLUTEN FREE DIET CAN BE LOW IN:
High protein
High calorie
High Iron , folic acid, vit B12 , A, K, and D as water soluble B vitamins (thiamine, riboflavin, niacin, folate)
Calcium
Zinc
Magnesium
Fiber
THE GLUTEN FREE DIET CAN BE LOW IN:
High protein
High calorie
High Iron , folic acid, vit B12 , A, K, and D as water soluble B vitamins (thiamine, riboflavin, niacin, folate)
Calcium
Zinc
Magnesium
Fiber
© 2004, 2002 Elsevier Inc. All rights reserved.
Treatment:Treatment:
The only treatment is the lifelong adherence to the gluten-free diet.
Gluten small intestine start to heal
overall health improves
The only treatment is the lifelong adherence to the gluten-free diet.
Gluten small intestine start to heal
overall health improves
© 2004, 2002 Elsevier Inc. All rights reserved.
Fallow Up:Fallow Up:
Serologic markers (serum IgA tTG) used to monitor compliance with a gluten-free diet
Antibody levels return to normal within three to 12 months of starting a gluten-free diet.
A repeat small bowel biopsy three to four months after initiation of a gluten-free diet is not necessary if the patient responds appropriately to therapy.
If the patient does not respond as expected despite adherence to a gluten-free diet, the physician should consider diseases that may mimic celiac disease.
Serologic markers (serum IgA tTG) used to monitor compliance with a gluten-free diet
Antibody levels return to normal within three to 12 months of starting a gluten-free diet.
A repeat small bowel biopsy three to four months after initiation of a gluten-free diet is not necessary if the patient responds appropriately to therapy.
If the patient does not respond as expected despite adherence to a gluten-free diet, the physician should consider diseases that may mimic celiac disease.

© 2004, 2002 Elsevier Inc. All rights reserved.
Celiac Disease−Medical and Nutritional ManagementCeliac Disease−Medical and Nutritional Management
Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002.

© 2004, 2002 Elsevier Inc. All rights reserved.
Summary:Summary:
People with celiac disease cannot tolerate gluten, a protein in wheat, rye, and barley.
Untreated celiac disease damages the small intestine and interferes with nutrient absorption.
Without treatment, people with celiac disease can develop complications such as osteoporosis, anemia, and cancer.
A person with celiac disease may or may not have symptoms.
People with celiac disease cannot tolerate gluten, a protein in wheat, rye, and barley.
Untreated celiac disease damages the small intestine and interferes with nutrient absorption.
Without treatment, people with celiac disease can develop complications such as osteoporosis, anemia, and cancer.
A person with celiac disease may or may not have symptoms.
© 2004, 2002 Elsevier Inc. All rights reserved.
Summary:Summary:
Celiac disease is treated by eliminating all gluten from the diet. The gluten-free diet is a lifetime requirement.
A dietitian can teach a person with celiac disease about food selection, label reading, and other strategies to help manage the disease.
If villi are damaged, vitamins, minerals, calcium, carbohydrates, protein, and fats are not absorbed well
Diagnosis involves blood tests and, in most cases, a biopsy of the small intestine.
Celiac disease is treated by eliminating all gluten from the diet. The gluten-free diet is a lifetime requirement.
A dietitian can teach a person with celiac disease about food selection, label reading, and other strategies to help manage the disease.
If villi are damaged, vitamins, minerals, calcium, carbohydrates, protein, and fats are not absorbed well
Diagnosis involves blood tests and, in most cases, a biopsy of the small intestine.

© 2004, 2002 Elsevier Inc. All rights reserved.
References:References:
Celiac Disease: Diagnostic clues to Unmaskan Imposter Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244
Presutti J,Cangemi J, Cassidy H, Hill D, Celiac Disease. American Family Physician. December 15, 2007: 1795-1802
Lancet. 2003 Aug 2;362(9381):383-91.Celiac disease. Green PH, Jabri B.
Department of Medicine, Columbia University College of Physicians and Surgeons, New York 10032, USA [email protected]
Celiac Disease: Diagnostic clues to Unmaskan Imposter
Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244
Krause's book 2008. 681-684 (1352)-Disease of the small intestine-celiac disease
Celiac Disease: Diagnostic clues to Unmaskan Imposter Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244
Presutti J,Cangemi J, Cassidy H, Hill D, Celiac Disease. American Family Physician. December 15, 2007: 1795-1802
Lancet. 2003 Aug 2;362(9381):383-91.Celiac disease. Green PH, Jabri B.
Department of Medicine, Columbia University College of Physicians and Surgeons, New York 10032, USA [email protected]
Celiac Disease: Diagnostic clues to Unmaskan Imposter
Malnick, Stephen, MD. Postgraduate Medicine 1997; 101: 239-244
Krause's book 2008. 681-684 (1352)-Disease of the small intestine-celiac disease

© 2004, 2002 Elsevier Inc. All rights reserved.
Reference: Reference:
Presutti J,Cangemi J, Cassidy H, Hill D, Celiac Disease. American Family Physician. December 15, 2007: 1795-1802. 5. 1981.)
Celiac disease: http://www.nature.com/mi/journal/v2/n1/fig_tab/mi200875f1.html#figure-title.
INSERM U793, University Paris Descartes, Paris, France Correspondence: N Cerf-Bensussan, ([email protected]) Received 8 October 2008; Accepted 8 October 2008; Published online 29 October 2008.
From Floch MH. Nutrition and Diet Therapy in Gastrointestinal Disease. New York: Menum Medical Book Co.,
Presutti J,Cangemi J, Cassidy H, Hill D, Celiac Disease. American Family Physician. December 15, 2007: 1795-1802. 5. 1981.)
Celiac disease: http://www.nature.com/mi/journal/v2/n1/fig_tab/mi200875f1.html#figure-title.
INSERM U793, University Paris Descartes, Paris, France Correspondence: N Cerf-Bensussan, ([email protected]) Received 8 October 2008; Accepted 8 October 2008; Published online 29 October 2008.
From Floch MH. Nutrition and Diet Therapy in Gastrointestinal Disease. New York: Menum Medical Book Co.,

© 2004, 2002 Elsevier Inc. All rights reserved.
Reference:Reference:
www.CeliacHealth.org
www.Celiac.org
www.glutenfree.com
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health NIH Publication No. 08–4269 September 2008
1Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States. Archives of Internal Medicine. 2003;163(3):268–292. 2Ibid.
www.CeliacHealth.org
www.Celiac.org
www.glutenfree.com
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health NIH Publication No. 08–4269 September 2008
1Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States. Archives of Internal Medicine. 2003;163(3):268–292. 2Ibid.

© 2004, 2002 Elsevier Inc. All rights reserved.
Thanks For listening:Thanks For listening: