Cefazolin Embedded Biodegradable Polypeptide Nanofilms ...
9
Transcript of Cefazolin Embedded Biodegradable Polypeptide Nanofilms ...

Cefazolin Embedded Biodegradable Polypeptide Nanofilms Promising forInfection Prevention: A Preliminary Study on Cell Responses
Hongshuai Li,1 Heather Ogle,1 Bingbing Jiang,1 Michael Hagar,1 Bingyun Li1,2,3
1Biomaterials, Bioengineering & Nanotechnology Laboratory, Department of Orthopaedics, School of Medicine, West Virginia University,Morgantown, West Virginia 26506-9196, 2WVNano Initiative, Morgantown, West Virginia 26506, 3Department of Chemical Engineering, College ofEngineering and Mineral Resources, West Virginia University, Morgantown, West Virginia 26506
Received 15 August 2009; accepted 11 January 2010
Published online 16 February 2010 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jor.21115
ABSTRACT: Implant-associated infection is a serious complication in orthopedic surgery, and endowing implant surfaces with antibacterialproperties could be one of the most promising approaches for preventing such infection. In this study, we developed cefazolin loadedbiodegradable polypeptide multilayer nanofilms on orthopedic implants. We found that the amount of cefazolin released could be tuned. Ahigh local concentration of cefazolin was achieved within the first a few hours and therefore may inhibit bacterial colonization in the criticalpostimplantation period. The developed cefazolin loaded nanofilms showed their in vitro efficacy against Staphylococcus aureus; the moreantibiotics loaded, the longer the nanocoated implant had antibacterial properties. More interestingly, antibiotic-loaded polypeptidemultilayer nanofilms also improved osteoblast bioactivity including cell viability and proliferation. These findings suggested thatbiodegradable polypeptide multilayernanofilms as antibiotic carriers at the implant/tissue interface are compatible with human cells such asosteoblasts and bactericidal to bacteria such as S. aureus. These characteristics could be promising for preventing implant-associatedinfection and potentially improving bone healing. � 2010 Orthopaedic Research Society. Published by Wiley Periodicals, Inc. J Orthop Res
28:992–999, 2010
Keywords: implant-associated infection; local antibiotic delivery; electrostatic layer-by-layer self-assembly; antibiotic; polypeptide
Implant-associated infection is one of the most seriouscomplications in orthopedic surgery. Of the more thantwo million orthopedic implants used in patientsannually in the United States, approximately 4% getinfected.1 The number of implant-associated infectionswill continue to rise as more baby boomers receivebiomedical implants. Bone infections associated withforeign body materials are especially difficult totreat. Removal of the infected implants,2,3 long-termsystemic antibiotic therapy, and multiple revisions withradical debridement are frequently required.1,4,5 Theconsequences of infection can be devastating and maylead to prolonged hospitalization, poor functional out-come, sepsis, and even amputation.6
The most probable reason that implant-associatedinfection is difficult to treat is that pathogens, primarilyStaphylococcus aureus and Staphylococcus epidermidis,colonize on the implant surface and form a bio-film.7–10
Bio-films are resistant to both the immune response andsystemic antibiotic therapies.1 It is, therefore, of greatimportance to prevent the initial bacterial adhesionthereby preventing bio-film formation on implants.Antibiotic coatings on implants could be an effectiveapproach to reduce bacterial colonization in vitro andbio-film formation in vivo.11–13
Many approaches for surface coating, such as dipcoating, spin coating, and plasma spray, have beendeveloped to achieve an antibacterial surface.14–16
Among these techniques, electrostatic layer-by-layer(LBL) self-assembly nanotechnology is one of the mostpromising methods.17 This method is simply based onthe alternative deposition of oppositely charged poly-electrolyte layers. The driving force for film constructionis the alternating charges (positive and negative) thatappear after each layer of polyelectrolyte deposition.This technique offers multiple advantages over otherapproaches. First, the buildup process may be easilyperformed by simple adsorption procedures on anysurfaces of devices used in clinical applications. Second,the formed films may possibly be used as carriers ofproteins and other biologically active molecules that canbe incorporated without losing their bioactivity.18–20
Using this technique, a biodegradable coating maybe developed to deliver ideal drug dosages over adesirable time period leaving no residual materials onimplants.21,22
The objectives of this study were: (i) to developbiodegradable polypeptide multilayer nanofilms poten-tially serving as antibiotic carriers at the implant/tissueinterface; (ii) to evaluate the efficacy of cefazolinloaded poly(L-lysine)/poly(L-glutamic acid) (PLL/PLGA) nanofilms on stainless steel disks (SSDs), inkilling S. aureus; and (iii) to evaluate the effects ofcefazolin loaded nanofilms on osteoblast cell behavior.
MATERIALS AND METHODSLayer-By-Layer Nanocoating and Cefazolin Loading and ReleaseSSDs 10 mm in diameter and 0.25 mm thick were thoroughlycleaned and polypeptide multilayer nanofilms were developedusing the LBL technique. Details of the LBL process werereported earlier.23 The thickness, measured by ellipsometry,24
of 40 layers of PLL and PLGA or PLL/PLGA20 nanofilms wasabout 240 nm.
PLL/PLGA20 nanofilms were loaded with cefazolinby immersing them in a cefazolin solution (pH 7) of 2.5, 5, and
992 JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010
Additional Supporting Information may be found in the onlineversion of this article.Correspondence to: Bingyun Li (Telephone: 1-304-293-1075;Fax: 1-304-293-7070; E-mail: [email protected])
� 2010 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.

10 mg/ml for 20 min. In the in vitro release studies, cefazolin-loaded PLL/PLGA20 nanocoated SSDs were incubated in 10 mlphosphate-buffered saline or PBS (pH 7) at 378C. PBS aliquotsolution (0.6 ml) was taken to determine cefazolin concentra-tion at predetermined time points and 0.6 ml fresh PBS wasadded afterwards.
In Vitro Bacterial Inhibition StudyTherapeutic activities of PLL/PLGA20 nanofilms were assessedagainst proliferation of S. aureus, which was isolated froma patient with chronic osteomyelitis. A freshly cultured S.aureus suspension was centrifuged, then washed and dilutedwith PBS to contain �1� 108 colony forming units (CFU)/ml.The suspension was used for two types of bacterial inhibitionassays (see Supplementary Materials): zone of inhibition (ZOI)test and a modified bacterial killing assay.25
In Vitro Bacterial Adhesion StudyA S. aureus suspension, containing �1� 107 CFU/ml of S.aureus was prepared. A highly lipophilic carocyanine dye, thatis, Dio, was used to stain S. aureus before seeding onto SSDs.A 1 ml S. aureus suspension was then added to a 24-well platecontaining bare SSDs or PLL/PLGA20 nanocoated SSDs(without cefazolin) and cultured at 378C for 2 h. After washingwith PBS three times and fixing using 10% formalin, the SSDswere glued onto glass slides and observed under confocalfluorescent microscopy (LSM 510, Carl Zeiss, Thornwood, NY)with excitation/emission wavelengths of 480/505 nm.
Osteoblast Cell Adhesion and VisualizationCRL-11372 human osteoblast cell line (American Type CultureCollection or ATCC, Manassas, VA) was routinely grown inDulbecco’s modified Eagle’s medium/Ham’s nutrient mixtureF-12, 1:1 medium (DMEM: F-12 medium, ATCC) with 10%fetal bovine serum (ATCC), 100 IU/ml penicillin, and 100 mg/mlstreptomycin (ATCC) in a 5% CO2 and 95% air atmosphereincubator at 378C. Cells were also cultured in the absence ofpenicillin and streptomycin, and used to study osteoblastadhesion and viability (see Supplementary Materials). Cellswere seeded on SSD samples in a 24-well plate at 1� 105 cells/well and incubated at 378C in a 5% CO2 humidified incubator.After culturing for 2 and 24 h, the number of adherent cellswere examined using hemocytometry. The SSDs were rinsedthree times with PBS and transferred to a new 24-wellplate. The cells on the SSD samples were then detached with0.25% Trypsin/0.53 mM EDTA solution (ATCC) followed byrinsing with culture medium. The rinsing media was collectedand the number of detached cells was determined using ahemocytometer.
The distribution and morphology of osteoblasts adhered onthe SSDs were examined using scanning electron microscopy(SEM) and confocal fluorescent microscopy. After culturing for2 and 24 h, the cell-seeded SSDs were rinsed with PBS, fixed in2.5% glutaraldehyde, and postfixed in 4% osmium tetroxide.The fixed specimens were dehydrated by immersing them intoincreasing concentrations of ethanol (70%, 85%, 95%, and100%). Then all specimens were dried using a critical pointdryer (CPD030, Bal-Tec, Carlsbad, CA). The specimens wereobserved under SEM (S-4700, Hitachi, Tokyo, Japan). Forconfocal fluorescent microscopy, cells were stained with ahighly lipophilic carocyanine dye Dil before seeding onto theSSDs. Nanocoated and bare SSDs were incubated with thelabeled cells for 2 and 24 h. The adherent osteoblasts wereobserved under confocal fluorescent microscopy with excita-tion/emission wavelengths of 540/560 nm.
Cell ViabilityCell viability was determined by MTT assay using an in vitrotoxicology kit (Sigma-Aldrich, St. Louis, MO). Osteoblastswere seeded on SSDs, incubated at 378C for 4 days, and 200mlof MTT solution was added to each well and incubated for 2 h.Then, 200 ml of MTT solubilization solution was added to eachwell and the dissolved solution was transferred to a 96-wellplate. Absorbance at 570 nm was measured using a micro-plate reader (mQuant, Bio-Tek, Winooski, VT). The backgroundabsorbances of multiwell plates were measured at 690 nm andsubtracted from the 570 nm measurements.
Cell ProliferationCells were seeded on SSDs at a density of 2� 105 cells/well.Sample solutions were collected on days 1, 3, and 5. Briefly,osteoblasts adhered to the surface of SSDs were gently rinsedwith PBS, overlaid with 1 ml Trypsin/EDTA solution per welland incubated at 378C for 5 min. The loosely detached cell layerwas then scraped off the SSD substrate, centrifuged at1,200 rpm for 7 min, and resuspended in 1 ml distilled waterwith 1% Triton X-100. Then the cell suspensions underwentthree freeze–thaw cycles. The triton lysates were stored at�808C until testing for DNA content. A 30 ml aliquot of cellsuspension was used to determine dsDNA content, whichwas measured by a fluorometric quantification method usinga Quant-iT dsDNA high-sensitivity assay kit (Invitrogen,Carlsbad, CA).
Statistical MethodsData were expressed as the mean� standard deviation (SD).Statistical differences were analyzed using the one-wayANOVA analysis. p< 0.05 was considered statistically signi-ficant. SPSS software 11.0 was used for statistical analysis.
RESULTSCefazolin Release from Polypeptide NanofilmsDifferent amounts of cefazolin were loaded into PLL/PLGA20 nanofilms; all the nanofilms had similarpharmacokinetics (Fig. 1). All nanofilms had aburst release of cefazolin in the first 2 h followed by arelease of 16% or less afterwards. The PLL/PLGA20
nanofilms loaded with cefazolin at a higher antibiotic
Figure 1. Release profiles of PLL/PLGA20 nanocoated SSDsloaded with cefazolin at three different concentrations. Threesamples were tested at each cefazolin concentration.
CELL RESPONSES TO CEFAZOLIN EMBEDDED NANOFILMS 993
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010
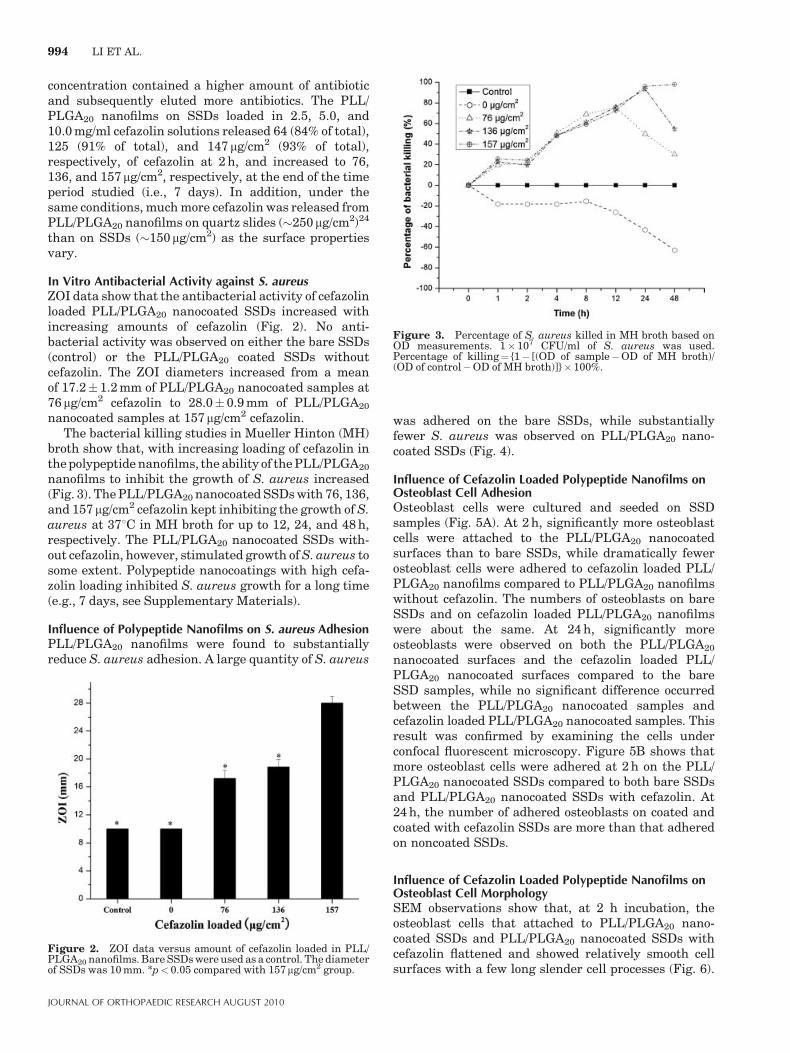
concentration contained a higher amount of antibioticand subsequently eluted more antibiotics. The PLL/PLGA20 nanofilms on SSDs loaded in 2.5, 5.0, and10.0 mg/ml cefazolin solutions released 64 (84% of total),125 (91% of total), and 147 mg/cm2 (93% of total),respectively, of cefazolin at 2 h, and increased to 76,136, and 157mg/cm2, respectively, at the end of the timeperiod studied (i.e., 7 days). In addition, under thesame conditions, much more cefazolin was released fromPLL/PLGA20 nanofilms on quartz slides (�250mg/cm2)24
than on SSDs (�150mg/cm2) as the surface propertiesvary.
In Vitro Antibacterial Activity against S. aureusZOI data show that the antibacterial activity of cefazolinloaded PLL/PLGA20 nanocoated SSDs increased withincreasing amounts of cefazolin (Fig. 2). No anti-bacterial activity was observed on either the bare SSDs(control) or the PLL/PLGA20 coated SSDs withoutcefazolin. The ZOI diameters increased from a meanof 17.2� 1.2 mm of PLL/PLGA20 nanocoated samples at76 mg/cm2 cefazolin to 28.0�0.9 mm of PLL/PLGA20
nanocoated samples at 157mg/cm2 cefazolin.The bacterial killing studies in Mueller Hinton (MH)
broth show that, with increasing loading of cefazolin inthe polypeptide nanofilms, the ability of the PLL/PLGA20
nanofilms to inhibit the growth of S. aureus increased(Fig. 3). The PLL/PLGA20 nanocoated SSDs with 76, 136,and 157mg/cm2 cefazolin kept inhibiting the growth of S.aureus at 378C in MH broth for up to 12, 24, and 48 h,respectively. The PLL/PLGA20 nanocoated SSDs with-out cefazolin, however, stimulated growth of S. aureus tosome extent. Polypeptide nanocoatings with high cefa-zolin loading inhibited S. aureus growth for a long time(e.g., 7 days, see Supplementary Materials).
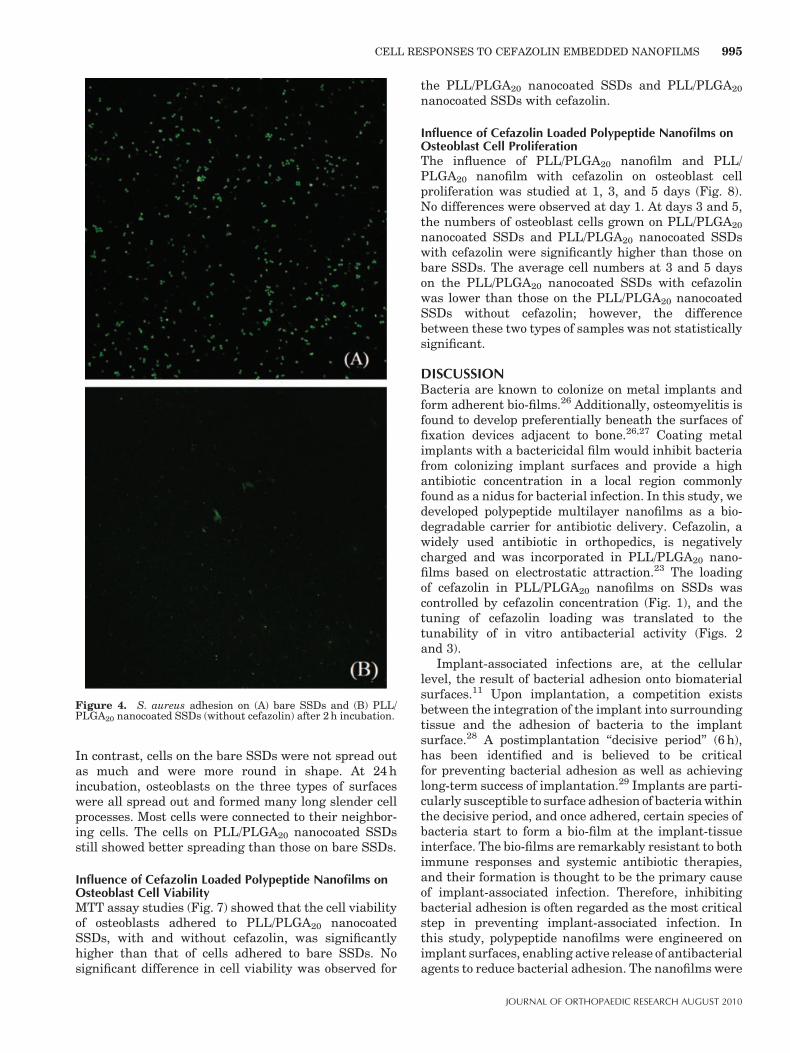
Influence of Polypeptide Nanofilms on S. aureus AdhesionPLL/PLGA20 nanofilms were found to substantiallyreduce S. aureus adhesion. A large quantity of S. aureus
was adhered on the bare SSDs, while substantiallyfewer S. aureus was observed on PLL/PLGA20 nano-coated SSDs (Fig. 4).
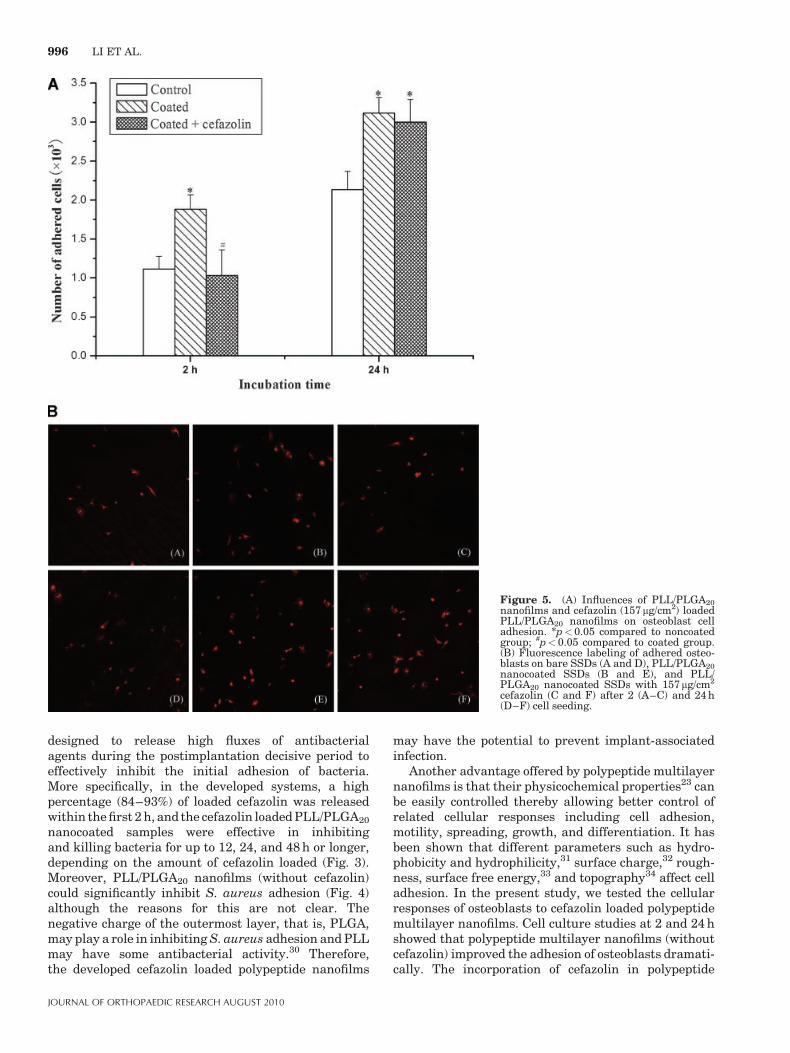
Influence of Cefazolin Loaded Polypeptide Nanofilms onOsteoblast Cell AdhesionOsteoblast cells were cultured and seeded on SSDsamples (Fig. 5A). At 2 h, significantly more osteoblastcells were attached to the PLL/PLGA20 nanocoatedsurfaces than to bare SSDs, while dramatically fewerosteoblast cells were adhered to cefazolin loaded PLL/PLGA20 nanofilms compared to PLL/PLGA20 nanofilmswithout cefazolin. The numbers of osteoblasts on bareSSDs and on cefazolin loaded PLL/PLGA20 nanofilmswere about the same. At 24 h, significantly moreosteoblasts were observed on both the PLL/PLGA20
nanocoated surfaces and the cefazolin loaded PLL/PLGA20 nanocoated surfaces compared to the bareSSD samples, while no significant difference occurredbetween the PLL/PLGA20 nanocoated samples andcefazolin loaded PLL/PLGA20 nanocoated samples. Thisresult was confirmed by examining the cells underconfocal fluorescent microscopy. Figure 5B shows thatmore osteoblast cells were adhered at 2 h on the PLL/PLGA20 nanocoated SSDs compared to both bare SSDsand PLL/PLGA20 nanocoated SSDs with cefazolin. At24 h, the number of adhered osteoblasts on coated andcoated with cefazolin SSDs are more than that adheredon noncoated SSDs.
Influence of Cefazolin Loaded Polypeptide Nanofilms onOsteoblast Cell MorphologySEM observations show that, at 2 h incubation, theosteoblast cells that attached to PLL/PLGA20 nano-coated SSDs and PLL/PLGA20 nanocoated SSDs withcefazolin flattened and showed relatively smooth cellsurfaces with a few long slender cell processes (Fig. 6).
Figure 2. ZOI data versus amount of cefazolin loaded in PLL/PLGA20 nanofilms. Bare SSDs were used as a control. The diameterof SSDs was 10 mm. *p< 0.05 compared with 157mg/cm2 group.
Figure 3. Percentage of S. aureus killed in MH broth based onOD measurements. 1�107 CFU/ml of S. aureus was used.Percentage of killing¼ {1� [(OD of sample�OD of MH broth)/(OD of control�OD of MH broth)]}�100%.
994 LI ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010
In contrast, cells on the bare SSDs were not spread outas much and were more round in shape. At 24 hincubation, osteoblasts on the three types of surfaceswere all spread out and formed many long slender cellprocesses. Most cells were connected to their neighbor-ing cells. The cells on PLL/PLGA20 nanocoated SSDsstill showed better spreading than those on bare SSDs.
Influence of Cefazolin Loaded Polypeptide Nanofilms onOsteoblast Cell ViabilityMTT assay studies (Fig. 7) showed that the cell viabilityof osteoblasts adhered to PLL/PLGA20 nanocoatedSSDs, with and without cefazolin, was significantlyhigher than that of cells adhered to bare SSDs. Nosignificant difference in cell viability was observed for
the PLL/PLGA20 nanocoated SSDs and PLL/PLGA20
nanocoated SSDs with cefazolin.
Influence of Cefazolin Loaded Polypeptide Nanofilms onOsteoblast Cell ProliferationThe influence of PLL/PLGA20 nanofilm and PLL/PLGA20 nanofilm with cefazolin on osteoblast cellproliferation was studied at 1, 3, and 5 days (Fig. 8).No differences were observed at day 1. At days 3 and 5,the numbers of osteoblast cells grown on PLL/PLGA20
nanocoated SSDs and PLL/PLGA20 nanocoated SSDswith cefazolin were significantly higher than those onbare SSDs. The average cell numbers at 3 and 5 dayson the PLL/PLGA20 nanocoated SSDs with cefazolinwas lower than those on the PLL/PLGA20 nanocoatedSSDs without cefazolin; however, the differencebetween these two types of samples was not statisticallysignificant.
DISCUSSIONBacteria are known to colonize on metal implants andform adherent bio-films.26 Additionally, osteomyelitis isfound to develop preferentially beneath the surfaces offixation devices adjacent to bone.26,27 Coating metalimplants with a bactericidal film would inhibit bacteriafrom colonizing implant surfaces and provide a highantibiotic concentration in a local region commonlyfound as a nidus for bacterial infection. In this study, wedeveloped polypeptide multilayer nanofilms as a bio-degradable carrier for antibiotic delivery. Cefazolin, awidely used antibiotic in orthopedics, is negativelycharged and was incorporated in PLL/PLGA20 nano-films based on electrostatic attraction.23 The loadingof cefazolin in PLL/PLGA20 nanofilms on SSDs wascontrolled by cefazolin concentration (Fig. 1), and thetuning of cefazolin loading was translated to thetunability of in vitro antibacterial activity (Figs. 2and 3).
Implant-associated infections are, at the cellularlevel, the result of bacterial adhesion onto biomaterialsurfaces.11 Upon implantation, a competition existsbetween the integration of the implant into surroundingtissue and the adhesion of bacteria to the implantsurface.28 A postimplantation ‘‘decisive period’’ (6 h),has been identified and is believed to be criticalfor preventing bacterial adhesion as well as achievinglong-term success of implantation.29 Implants are parti-cularly susceptible to surface adhesion of bacteria withinthe decisive period, and once adhered, certain species ofbacteria start to form a bio-film at the implant-tissueinterface. The bio-films are remarkably resistant to bothimmune responses and systemic antibiotic therapies,and their formation is thought to be the primary causeof implant-associated infection. Therefore, inhibitingbacterial adhesion is often regarded as the most criticalstep in preventing implant-associated infection. Inthis study, polypeptide nanofilms were engineered onimplant surfaces, enabling active release of antibacterialagents to reduce bacterial adhesion. The nanofilms were
Figure 4. S. aureus adhesion on (A) bare SSDs and (B) PLL/PLGA20 nanocoated SSDs (without cefazolin) after 2 h incubation.
CELL RESPONSES TO CEFAZOLIN EMBEDDED NANOFILMS 995
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010
designed to release high fluxes of antibacterialagents during the postimplantation decisive period toeffectively inhibit the initial adhesion of bacteria.More specifically, in the developed systems, a highpercentage (84–93%) of loaded cefazolin was releasedwithin the first 2 h, and the cefazolin loaded PLL/PLGA20
nanocoated samples were effective in inhibitingand killing bacteria for up to 12, 24, and 48 h or longer,depending on the amount of cefazolin loaded (Fig. 3).Moreover, PLL/PLGA20 nanofilms (without cefazolin)could significantly inhibit S. aureus adhesion (Fig. 4)although the reasons for this are not clear. Thenegative charge of the outermost layer, that is, PLGA,may play a role in inhibiting S. aureus adhesion and PLLmay have some antibacterial activity.30 Therefore,the developed cefazolin loaded polypeptide nanofilms
may have the potential to prevent implant-associatedinfection.
Another advantage offered by polypeptide multilayernanofilms is that their physicochemical properties23 canbe easily controlled thereby allowing better control ofrelated cellular responses including cell adhesion,motility, spreading, growth, and differentiation. It hasbeen shown that different parameters such as hydro-phobicity and hydrophilicity,31 surface charge,32 rough-ness, surface free energy,33 and topography34 affect celladhesion. In the present study, we tested the cellularresponses of osteoblasts to cefazolin loaded polypeptidemultilayer nanofilms. Cell culture studies at 2 and 24 hshowed that polypeptide multilayer nanofilms (withoutcefazolin) improved the adhesion of osteoblasts dramati-cally. The incorporation of cefazolin in polypeptide
Figure 5. (A) Influences of PLL/PLGA20nanofilms and cefazolin (157 mg/cm2) loadedPLL/PLGA20 nanofilms on osteoblast celladhesion. *p<0.05 compared to noncoatedgroup; #p< 0.05 compared to coated group.(B) Fluorescence labeling of adhered osteo-blasts on bare SSDs (A and D), PLL/PLGA20nanocoated SSDs (B and E), and PLL/PLGA20 nanocoated SSDs with 157mg/cm2
cefazolin (C and F) after 2 (A–C) and 24 h(D–F) cell seeding.
996 LI ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010
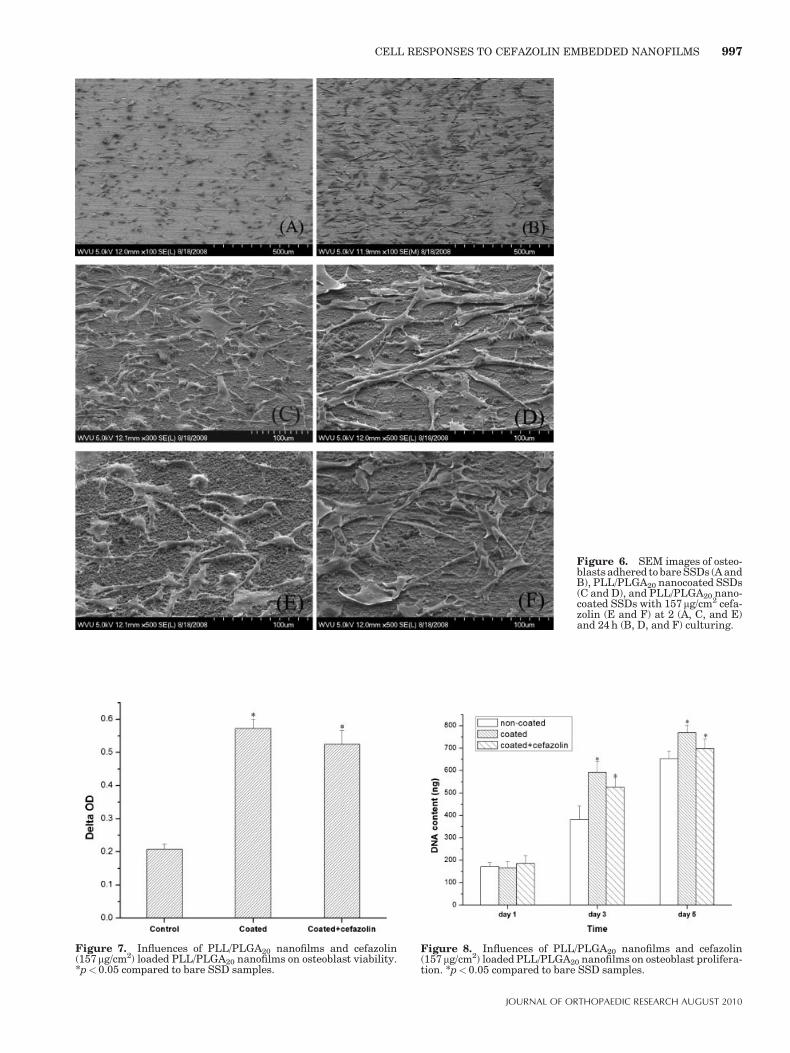
Figure 6. SEM images of osteo-blasts adhered to bare SSDs (A andB), PLL/PLGA20 nanocoated SSDs(C and D), and PLL/PLGA20 nano-coated SSDs with 157mg/cm2 cefa-zolin (E and F) at 2 (A, C, and E)and 24 h (B, D, and F) culturing.
Figure 7. Influences of PLL/PLGA20 nanofilms and cefazolin(157mg/cm2) loaded PLL/PLGA20 nanofilms on osteoblast viability.*p<0.05 compared to bare SSD samples.
Figure 8. Influences of PLL/PLGA20 nanofilms and cefazolin(157 mg/cm2) loaded PLL/PLGA20 nanofilms on osteoblast prolifera-tion. *p<0.05 compared to bare SSD samples.
CELL RESPONSES TO CEFAZOLIN EMBEDDED NANOFILMS 997
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010

multilayer nanofilms decreased the adhesion of osteo-blasts at 2 h culturing; this effect vanished at 24 h, whichwas probably due to the substantial release of cefazolinwithin the first few hours. As a result, no difference inosteoblast cell adhesion was observed at 24 h betweenPLL/PLGA20 nanocoated samples and PLL/PLGA20
nanocoated samples with cefazolin; cefazolin loadedpolypeptide nanofilms have similar (2 h) or enhanced(24 h) osteoblast cell adhesion compared to the control(Fig. 5A). Our results also showed that PLL/PLGA20
nanofilms, with and without cefazolin, could improvethe viability and proliferation of osteoblasts, and nodifferences at a relatively long time period (a few days)were found in viability and proliferation of osteoblastsbetween the PLL/PLGA20 nanofilms and PLL/PLGA20
nanofilms with cefazolin (Figs. 7 and 8). These resultssuggested, for the first time, that the developed antibioticloaded polypeptide multilayer nanofilms, used as surfacecoatings, are biocompatible with osteoblasts and pro-mote osteoblast proliferation.
In summary, this study showed that biodegradableimplantnanofilmscan be engineered to haveantibacterialactivity against organisms frequently associated withosteomyelitis. Polypeptide multilayer nanofilms, with orwithout cefazolin, were found to be biocompatiblewith osteoblasts. The developed polypeptide nanocoatedimplants could be used prophylactically to reduce theincidence of soft tissue and bone infection that frequentlycomplicate open fractures. Meanwhile, the nanocoatingsmay improve bone healing through improving osteoblastcell adhesion, viability, and proliferation. In the future,the effects of cefazolin loaded polypeptide nanofilms onosseointegration will be studied.
ACKNOWLEDGMENTSThe authors acknowledge financial support from the AOFoundation, National Science Foundation (OISE-0737735),NASA West Virginia Experimental Program to StimulateCompetitive Research, and West Virginia University. ProjectS-07-43L was supported by the AO Research Fund of the AOFoundation. The authors appreciate the use of confocal laserscanning microscope at the Microscopic Imaging Facilities atWest Virginia University Health Sciences Center, supportedin part by the Mary Babb Randolph Cancer Center and NIHgrant p20 RR016440. We acknowledge John G. Thomas, PhD(Department of Pathology) for the contribution of S. aureusand consultation on bacterial culture. We thank Karen Martinfor assisting in confocal imaging, Suzanne Smith for proof-reading, Nina Clovis for laboratory training, and Vincent Kishfor assistance in SEM sample preparation. M. H. also thanksthe E. J. Van Liere fellowship.
REFERENCES1. Darouiche RO. 2004. Treatment of infections associated with
surgical implants. N Engl J Med 350(14):1422–1429.2. Sanderson PJ. 1989. Preventing infection in orthopaedic
implants. J Antimicrob Chemother 24(3):277–280.3. Taylor GJ, Bannister GC, Calder S. 1990. Perioperative
wound infection in elective orthopaedic surgery. J Hosp Infect16(3):241–247.
4. Anderson JM. 2001. Biological responses to materials. AnnRev Mater Res 31:81–110.
5. An YH, Friedman RJ. 1996. Prevention of sepsis in total jointarthroplasty. J Hosp Infect 33(2):93–108.
6. Calhoun JH, Manring MM. 2005. Adult osteomyelitis. InfectDis Clin North Am 19(4):765–786.
7. Barton AJ, Sagers RD, Pitt WG. 1996. Bacterial adhesion toorthopedic implant polymers. J Biomed Mater Res 30(3):403–410.
8. Gotz F. 2002. Staphylococcus and biofilms. Mol Microbiol43(6):1367–1378.
9. Gristina AG. 1994. Implant failure and the immuno-incom-petent fibro-inflammatory zone. Clin Orthop Relat Res 298:106–118.
10. Khardori N, Yassien M. 1995. Biofilms in device-relatedinfections. J Ind Microbiol 15(3):141–147.
11. Hetrick EM, Schoenfisch MH. 2006. Reducing implant-relatedinfections: active release strategies. Chem Soc Rev 35(9):780–789.
12. Price JS, Tencer AF, Arm DM, et al. 1996. Controlled releaseof antibiotics from coated orthopedic implants. J BiomedMater Res 30(3):281–286.
13. Lucke M, Schmidmaier G, Sadoni S, et al. 2003. Gentamicincoating of metallic implants reduces implant-related osteo-myelitis in rats. Bone 32(5):521–531.
14. Stigter M, Bezemer J, de Groot K, et al. 2004. Incorporation ofdifferent antibiotics into carbonated hydroxyapatite coatingson titanium implants, release and antibiotic efficacy.J Control Release 99(1):127–137.
15. Humphrey JS, Mehta S, Seaber AV, et al. 1998. Pharmaco-kinetics of a degradable drug delivery system in bone. ClinOrthop Relat Res 349:218–224.
16. Nablo BJ, Schoenfisch MH. 2004. Poly(vinyl chloride)-coatedsol-gels for studying the effects of nitric oxide release onbacterial adhesion. Biomacromolecules 5(5):2034–2041.
17. Decher G. 1997. Fuzzy nanoassemblies: toward layeredpolymeric multicomposites. Science 277(5330):1232–1237.
18. Lvov Y, Ariga K, Ichinose I, et al. 1995. Assembly ofmulticomponent protein films by means of electrostaticlayer-by-layer adsorption. J Am Chem Soc 117(22):6117–6123.
19. Kong W, Wang LP, Gao ML, et al. 1994. Immobilized bilayerglucose-isomerase in porous trimethylamine polystyrene-based on molecular deposition. Chem Commun 1994(11):1297–1298.
20. Ladam G, Schaaf P, Cuisinier FJG, et al. 2001. Proteinadsorption onto auto-assembled polyelectrolyte films. Lang-muir 17:878–882.
21. Ladam G, Schaad P, Voegel JC, et al. 2000. In situdetermination of the structural properties of initially depo-sited polyelectrolyte multilayers. Langmuir 16:1249–1255.
22. Li B, Jiang B, Boyce B, et al. 2009. Multilayer polypeptidenanoscale coatings for the prevention of biomedical deviceassociated infections. Biomaterials 30:2552–2558.
23. Jiang B, Li B. 2009. Polypeptide nanocoatings for preventingdental and orthopaedic device-associated infection: pH-induced antibiotic capture, release, and antibiotic efficacy.J Biomed Mater Res B 88(2):332–338.
24. Jiang B, Li B. 2009. Tunable drug loading and releasefrom polypeptide multilayer nanofilms. Int J Nanomed 4(1):37–53.
25. Helmerhorst EJ, Van’t Hof W, Veerman EC, et al. 1997.Synthetic histatin analogues with broad-spectrum antimicro-bial activity. Biochem J 326(Pt 1):39–45.
26. Webb LX, Holman J, de Araujo B, et al. 1994. Antibioticresistance in staphylococci adherent to cortical bone. J OrthopTrauma 8:28–33.
998 LI ET AL.
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010

27. Chang CC, Merritt K. 1994. Infection at the site of implantedmaterials with and without preadhered bacteria. J Orthop Res12(4):526–531.
28. Gristina AG. 1987. Biomaterial-centered infection: microbialadhesion versus tissue integration. Science 237(4822):1588–1595.
29. Poelstra KA, Barekzi NA, Rediske AM, et al. 2002. Prophy-lactic treatment of gram-positive and gram-negative abdomi-nal implant infections using locally delivered polyclonalantibodies. J Biomed Mater Res 60:206–215.
30. Nishikawa M, Ogawa K. 2006. Inhibition of epsilon-poly-L-lysine biosynthesis in Streptomycetaceae bacteriaby short-chain polyols. Appl Environ Microbiol 72:2306–2312.
31. Grinnell F, Feld MK. 1982. Fibronectin adsorption on hydro-philic and hydrophobic surfaces detected by antibody bindingand analyzed during cell adhesion in serum-containingmedium. J Biol Chem 257(9):4888–4893.
32. Qiu Q, Sayer M, Kawaja M, et al. 1998. Attachment,morphology, and protein expression of rat marrow stromalcells cultured on charged substrate surfaces. J Biomed MaterRes 42:117–127.
33. Kapur R, Rudolph AS. 1998. Cellular and cytoskeletonmorphology and strength of adhesion of cells on self-assembled monolayers of organosilanes. Exp Cell Res 244(1):275–285.
34. Curtis AS, Varde M. 1964. Control of cell behavior: topologicalfactors. J Natl Cancer Inst 33:15–26.
CELL RESPONSES TO CEFAZOLIN EMBEDDED NANOFILMS 999
JOURNAL OF ORTHOPAEDIC RESEARCH AUGUST 2010