cdn-links.lww.com€¦ · Web viewMicrobiology data of patients with the Middle East Respiratory...
25
Supplementary appendix to Critically Ill Patients with the Middle East Respiratory Syndrome (MERS): A Multicenter Retrospective Cohort Study
Transcript of cdn-links.lww.com€¦ · Web viewMicrobiology data of patients with the Middle East Respiratory...

Supplementary appendix to
Critically Ill Patients with the Middle East Respiratory Syndrome (MERS): A
Multicenter Retrospective Cohort Study

Contents
Author’s Contribution
The MERS Study group
Supplement to Methods
Definitions: Comorbidities: (Guidance for completing Case Record Forms (CRFs) for the World Health Organization (WHO) the International Severe Acute Respiratory and Emerging Infection Consortium (ISARIC))
Rationale for Sensitivity Analyses
Supplement to Results
Table S1: Organizational structure of the 14 participating hospitals in the study.
Table S2: Microbiology data of patients with the Middle East Respiratory Syndrome severe acute respiratory infection (MERS SARI) and non-Middle East Respiratory Syndrome- severe acute respiratory infection (Non-MERS SARI). Pathogens during the hospital stay are shown with the exception for bacterial pathogens in respiratory samples and in blood cultures that are restricted to the first 2 days in the ICU. Numerators refer to the number of patients with identified pathogens and denominators refer to the number of patients tested.
Table S3: Multivariable model to examine whether the Middle East Respiratory Syndrome (MERS) is an independent predictor of 90-day mortality among all patients with severe acute respiratory infection and after restriction to pateints admitted to King Abdulaziz Medical City-Riyadh.
Table S4: Multivariate model to examine the independent predictors of 90-day mortality among all patients and patients excluding Healthcare workers and Healthcare associated with severe acute respiratory infection due to the Middle East Respiratory Syndrome (MERS SARI).
Figure S1: Serial Measurements of A. hemoglobin, B. blood urea nitrogen- BUN, C. alanine amino transferase- ALT, D. bilirubin and and E. partial presuure of carbon diaoxide in arterial blood (PaCO2) in patients with the Middle East Respiratory Syndrome severe acute respiratory infection (MERS SARI) and non-Middle East Respiratory Syndrome severe acute respiratory infection (Non-MERS SARI).
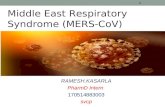
Figure S2: The percentage of patients with SARI who were tested for MERS-CoV. Testing for MERS-CoV among SARI patients was lowest in 2013 and improved with time.

Author’s Contribution
YA: Conception, acquisition of data, design, analytical plan, drafting of the manuscript and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AO: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.YM: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.FH: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AS: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.BR: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.SS: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AM: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be publishedKK: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AM: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.IQ: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AM: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.OS: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AA: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.RR: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AR: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.GM: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.AH: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AK: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.MA: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.MS: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.HM: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.EQ: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.JJ: Statistical analysis and critical revision of the manuscript for important intellectual content, approval of the final version to be published.

MN: Acquisition of data, and critical revision of the manuscript for important intellectual content, approval of the final version to be published.AD: Acquisition of data, critical revision of the manuscript for important intellectual content, approval of the final version to be published.LM: Conception, design, drafting of the manuscript and critical revision of the manuscript for important intellectual content, approval of the final version to be published.RF: Conception, design, drafting of the manuscript and critical revision of the manuscript for important intellectual content, approval of the final version to be published. FH: Conception, design, drafting of the manuscript and critical revision of the manuscript for important intellectual content, approval of the final version to be published. HB: Conception, design, drafting of the manuscript and critical revision of the manuscript for important intellectual content, approval of the final version to be published.

Collaborators
Center NamesSaudi Critical Care Trial GroupKing Saud bin Abdulaziz University for Health Sciences and King Abdullah International Medical Research Center, Riyadh
Yaseen ArabiAbdulaziz AldawoodHanan BalkhyMashael Al AhmadiMusharaf SadatHanan Al MutairiEman Al QasimAhmed DeebHasan AldorziJesna JoseMaliha NaseemMundekkadan ShihabSheryl Ann AbdukahilAron ToledoLara AfeshMohammed Rafique SohailOmar Al Shankeety
King Fahad Medical City, Riyadh Abdullah Al Motairi
Prince Sultan Cardiac Center, Riyadh Ghaleb A. AlmekhlafiYasser mandourahSahar HassanAbid AlwanRaylin CabalRima E MahamedKhaloud M. HarbiAbdulelah Ala Haidary
King Saud Medical City, Riyadh Abelrahman Al-Harthy Ahmed Fouad Mady Omar Elsayed Ramadan Muhammed Asim RanaBasim Raafat Huwait Mohamed Ali Al-Odat Waleed Tharwat Al-Atreeby
King Faisal Specialist Hospital and Research Centre, Riyadh Othman solaiman
King Khalid University hospital, Riyadh Ahmed Abdul MomminMuhammed faresMazen Barry
Security Forces Hospital, Riyadh Awad Al Omari
King Abdulaziz Medical City, Jeddah Fahad Al-HameedJalal Al Refai
King Fahd Armed Forced Hospital, Jeddah Sarah Shalhoub
King Faisel Hospital Research Center, Jeddah Basem M AlraddadiRashed E AlrehailiSarah Batawi
King Fahad Hospital Group, Jeddah Anees SindiRajaa Al-RaddadiAhmed RajabOmimah ShabouniAbeer Mustafa HousaAmal AbdulallaTurkistaniAbdullatif Ayesh Almarashi

Center NamesAmaal ali SarrajSalwa Awad OwnSara Mohammed AlJeaidWijdan Abdulalkareem Baeshen
AlNoor Specialist Hospital, Makkah Kasim Al KhatibHamdy BadrMajduldeen Azzo
King Abdulaziz Medical city-Alahsa Abdulsalam Alaithan
King Fahad Hospital, Madinah Ayman KharabaNoah Noor
United KingdomInfectious Diseases Data Observatory, Oxford University Laura Merson
CanadaSunnybrook Health Sciences Centre, Canada Robert Fowler
United States of AmericaUniversity of Virginia School of Medicine, USA Frederick Hayden

Supplement to Methods
Definitions 2
Comorbidities
Comorbidities are illnesses/risk factors which were known to exist prior to admission with the current illness and remain active problems.
Chronic cardiac disease (not hypertension)
This may be defined as a disease that progressively causes deterioration of the heart and its functioning. In some cases the direct cause of the disease may not be established. Some causes may include an infection that infiltrates the bloodstream that causes damage to the heart or having a genetic imperfection. These could involve:
Congenital Heart Disease (haemodynamically significant) is defined as any structural or functional cardiac disorder that is present from birth which results in (1) need for medication to control congestive heart failure or (2) moderate to severe pulmonary hypertension, or (3) cyanotic heart disease. Excludes asymptomatic ventricular septal defects and patent ductus arteriosus e.g. those where no medication is required
Congestive heart disease is defined as any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood. It is characterized by specific symptoms, such as dyspnoea and fatigue, and signs, such as fluid retention. There are many ways to assess cardiac function. However, there is no diagnostic test for heart failure, since it is largely a clinical diagnosis that is based upon a careful history and physical examination.
Chronic pulmonary disease (including asthma)
Chronic pulmonary disease (not asthma) This is defined as any pulmonary condition other than asthma that is a disease or disorder of slow progression and long duration which causes continuous or episodic periods of illness and/or incapacity.
Asthma (physician diagnosed)This is defined as clinician diagnosed asthma (a common chronic disorder of the airways that is complex and characterized by variable and recurring symptoms, airflow obstruction, bronchial hyper-responsiveness, and underlying inflammation). Current pharmaceutical intervention - for prevention or treatment of symptoms - is not a pre-requisite for the inclusion of this diagnosis.
Chronic Kidney Disease
This is defined as a clinician-diagnosed chronic kidney disease (CKD, also known as chronic kidney failure). The KDIGO and KDOQI definition of chronic kidney disease is kidney damage for 3 months, as defined by structural or functional abnormalities of the kidney, with or without decreased glomerular filtration rate (GFR), that can lead to decreased GFR, manifest by either:
Pathologic abnormalities; or

Markers of kidney damage, including abnormalities in the composition of the blood or urine, or abnormalities in imaging tests;
GFR <60 mL/min/1.73 m2 for 3 months, with or without kidney damage.
Liver disease
Moderate or severe liver disease
This is defined as cirrhosis with portal hypertension, with or without bleeding or a history of variceal bleeding.
Mild liver disease
This is defined as cirrhosis without portal hypertension or chronic hepatitis
Chronic neurological disease including hemiplegia, paraplegia and dementia
Chronic neurological disease
This is defined as conditions in which respiratory function may be compromised due to neurological disease (e.g. polio syndrome sufferers), including individuals with cerebral palsy, multiple sclerosis and related or similar conditions; or hereditary and degenerative disease of the nervous system or muscles; or severe neurological or severe learning disability, or stroke with deficit affecting safety of swallow.
Hemiplegia is defined as chronic and persistent total paralysis of the arm, leg, and trunk on the same side of the body.
Paraplegia is defined as chronic and persistent complete paralysis of the lower half of the body including both legs.
Dementia
This is defined as:
● Evidence from the history and mental status examination that indicates major impairment in learning and memory as well as at least one of the following:
● Impairment in handling complex tasks● Impairment in reasoning ability● Impaired spatial ability and orientation● Impaired language
The cognitive symptoms must significantly interfere with the individual's work performance, usual social activities, or relationships with other people. This must represent a significant decline from a previous level of functioning. The disturbances are of insidious onset and are progressive, based on evidence from the history or serial mental-status examinations. The disturbances are not occurring exclusively during the course of delirium. The disturbances are not better accounted for by a major psychiatric diagnosis. The disturbances are not better accounted for by a systemic disease or another brain disease. Chronic cognitive deficit is included
Any malignancy including leukemia, lymphoma or solid tumors

Metastatic solid tumour
This is defined as currently active neoplastic growth or deposit that has spread via lymph or blood to an area of the body that is remote from the primary neoplasm (tumour).
Malignancy neoplasm (including leukaemia and lymphoma)
This refers to any known malignant neoplastic disease, including haematological malignancies, that is considered to be biologically active. A tumor composed of atypical neoplastic, often pleomorphic cells that invade other tissues. Malignant neoplasms often metastasize to distant anatomic sites and may recur after excision. The most common malignant neoplasms are carcinomas (adenocarcinomas or squamous cell carcinomas), Hodgkin and non-Hodgkin lymphomas, leukemias, melanomas, and sarcomas. It specifically does not include malignancies that have been cured or where there is no evidence of on-going disease relating to that malignancy following treatment.
Acquired Immune deficiency syndrome
AIDS/HIV
This refers to laboratory-confirmed HIV-1 or HIV-2 infection (irrespective of the CD4 lymphocyte count/percentage or HIV viral load in blood), or a patient with an AIDS-defining condition.
Obesity (as defined by clinical staff)
This refers to patients for whom an attending clinician has assessed them to be obese - ideally but not necessarily with an objective measurement of obesity, such as calculation of the body mass index (BMI of 30 or more) or measurement of abdominal girth.
Diabetes with complications
This is defined as diabetes mellitus (type I or type II) with evidence of one or more organ or tissue damage due to diabetes mellitus, irrespective of the need for current treatment of diabetes. Examples of chronic complications include: diabetic cardiomyopathy; diabetic nephropathy; diabetic neuropathy; diabetic retinopathy; diabetic myonecrosis; peripheral vascular disease; coronary artery disease; stroke (other examples exist).
Rheumatologic disease
This is defined as an inflammatory and degenerative diseases of connective tissue structures. It includes chronic arthropathies and arthritis, connective tissue disorders and vasculitides.
Rationale for sensitivity analyses:
We carried multiple sensitivity analyses to ensure the robustness of the independent association of MERS and mortality. First, because non-MERS SARI data were from one center (KAMC-R), we carried out a sensitivity analysis by restricting the logistic regression analysis to patients from KAMC-R. Second, because MERS SARI patients included community-acquired and healthcare-associated cases, we performed an additional

sensitivity analysis by restricting the logistic regression analysis to patients with community-acquired infection. Third, because some of non-MERS SARI were not tested for MERS-CoV, we performed a sensitivity analysis including only non-MERS SARI who were tested for MERS-CoV.

Question ResponseTotal bed capacity in the hospital — median (Q1, Q3) 550 (500,
1200)Number of hospitals that underwent a formal hospital accreditation — no.(%) 12 (85.7)Number of hospitlas with infection control departments or committees — no. (%) 14 (100.0)
Number of ICU beds per hospital — median (Q1, Q3) 42 (34, 64)Number of ICUs that run as closed units — no. (%) 11 (78.6)Number of ICU consultants per hospital — median (Q1, Q3) 9 (5, 20)Number of ICU nurses per hospital — median (Q1, Q3) 109 (80, 198)Number of ICUs with nurse to patient ratio 1:1 — no. (%) 12 (85.7)
Number of beds in the ICUs that admit MERS patients — median (Q1, Q3) 29 (20, 35)Number of single rooms in the ICUs that admit MERS SARI patients — median (Q1, Q3) 11 (6, 12)Number of negative pressure rooms in the ICU that admit MERS SARI patients — median (Q1, Q3)
7 (5, 11)
rRT-PCR of MERS-CoV performed in the same hospital (vs. referred) — no. (%) 3 (21.4)Availabilty of Influenza panel— no. (%) 5 (35.7)Availabilty of Viral Multiplex PCR— no. (%) 4 (28.5)Availability of ECMO — no. (%) 7 (50.0)Availability of high frequency oscillation(HFO) — no. (%) 11 (78.6)
Table S1. Organizational features of the 14 participating hospitals in the study.

Table S2: Microbiology data of patients with the Middle East Respiratory Syndrome severe acute respiratory infection (MERS SARI) and non- Middle East Respiratory Syndrome severe acute respiratory infection (Non-MERS SARI). Pathogens during the hospital stay are shown with the exception for bacterial pathogens in respiratory samples and in blood cultures that are restricted to the first 2 days in the ICU. Nominators refer to the number of patients with identified pathogens and denominators refer to the number of patients tested.
Variable MERS SARIN=330
Non-MERS SARI
N=222
P value
MERS-CoV rRT-PCR — no. (%) 330 (100) 0 (0) Diagnosed from 1st rRT-PCR* 237/311 0/129 Diagnosed from 2ed rRT-PCR* 51/311 0/129 Diagnosed from 3th rRT-PCR* 17/311 0/129 Diagnosed from 4th rRT-PCR* 2/311 0/129 Diagnosed from 5th or more rRT-PCR* 4/311 0/129
Number of patients with other viruses — no. (%) 17 (5) 52 (24) <0.001** Influenza Influenza A including H1N1 2/163 29/152 Influenza B 0/108 3/152 Rhinovirus 1/48 9/51 Parainfluenza 1/49 1/51 Respiratory syncytial virus (RSV) 1/48 1/51 Adenovirus 1/48 1/51 Bocavirus 1/49 1/51 Enterovirus 1/48 0/51 Humancoronavirus-229E 0/46 1/51 Humancoronavirus-NL63 0/43 1/51 Humancoronavirus-OC43 1/47 3/51 Humancoronavirus-HKU1 4/6 0/1 Human metapneumovirus 0/49 1/51 Norovirus 0/1 1/1 Cytomegalovirus 5/13 7/11
Number of patients with bacterial pathogens in respiratory samples (± 3 days of ICU admission) — no. (%)
60(18.5) 56 (25.2) 0.046**
Gram negative bacilli Acinetobacter Spp 17/150 14/131 Pseudomonas Spp 9/150 14/131 Klebsiella pneumoniae 8/150 6/131 Others 4/150 2/131Gram positive cocci Staphylococcus aureus 15/150 21/131 Streptococcus. pneumoniae 3/150 2/131 Others 5/150 4/131Other pathogens Legionella pneumophila 1/23 0/51 Mycoplasma pneumoniae 3/19 2/12 Chlamydia pneumoniae 1/15 0/5 Mycobacterium tuberculosis 1/30 4/104
Number of patients with bacterial pathogens in blood culture (± 3 days of ICU admission) — no. (%)
26 (8) 29 (13) 0.046**
Gram negative bacilli Enterobacter Spp 3/208 5/181 Klebsiella pneumoniae 4/208 1/181 E. Coli 3/208 0/181 Pseudomonas Spp 1/208 2/181 Others 1/208 4/181Gram positive cocci Staphylococcus aureus 17/208 13/181 Streptococcus pneumoniae 0/208 1/181 Others 0/208 4/181
* Details on negative MERS-CoV rRT-PCR tests are available on only 311 patients. **Chi-square test is used to calculate the P-value.

Table S3. Multivariable model to examine whether the Middle East Respiratory Syndrome (MERS) is an independent predictor of 90-day mortality among all patients with severe acute respiratory infection. Sensitivity analyses were performed by restriction to patients admitted to King Abdulaziz Medical City-Riyadh (KAMC-R) only, community acquired cases only, Influenza A only and non MERS-SARI who have been tested for MERS.Variables Number of
observationsaOR (95% CI) P-value
Group, MERS SARI vs non-MERS SARI, all cohort 551 5.87 (4.02, 8.56) <0.001
Group, MERS SARI vs non-MERS SARI, King Abdulaziz Medical City-Riyadh only 312 4.14 (2.21, 7.76) <0.001
Group, MERS SARI vs non-MERS SARI, Community-acquired cases only 387 5.51 (3.68, 8.25) <0.001
Group, MERS vs non-MERS SARI- with only patients tested for MERS-CoV included 458 4.66 (3.36, 6.47) <0.001
aOR: adjusted Odds Ratio; CI: Confidence Interval;All analyses are adjusted for clustering for sites. Covariates: age, male sex, diabetes with chronic complications, chronic cardiac disease, chronic renal disease, chronic pulmonary disease including asthma, obesity, chronic neurological disease ,immunosuppression use prior to admission and period July 2014-2015 vs before July 2014.Chi-square Test is used to calculate the P-value

Table S4. Multivariate model to examine the independent predictors of 90-day mortality among MERS SARI patients adjusted by clustering for sites and after restriction to patients admitted to King Abdulaziz Medical City-Riyadh (KAMC-R) , community acquired cases only.
Variables All MERS patients# Community acquired @ KAMC-R only$
aOR (95% CI) P-value aOR (95% CI) P-value aOR (95% CI) P-valueAge (per one year increase) 1.05 (1.03, 1.07) <.0001 1.10 (1.07, 1.14) <.0001 1.07 (1.03, 1.11) 0.0004Male sex 0.65 ( 0.41, 1.02) 0.06 0.25 (0.10, 0.67) 0.006 0.53 ( 0.16, 1.79) 0.31Diabetes with chronic complications 1.39 ( 0.75, 2.57) 0.30 4.20 ( 1.06,16.60) 0.04 2.07 ( 0.41,10.55) 0.38Chronic cardiac disease 1.19 ( 0.68, 2.05) 0.54 0.73 ( 0.46, 1.14) 0.16 0.77 ( 0.17, 3.50) 0.74Chronic renal disease 2.48 (1.26, 4.89) 0.008 1.44 ( 0.60, 3.43) 0.41 2.57 ( 0.63,10.44) 0.19Chronic pulmonary disease (including asthma) 0.77 ( 0.44, 1.37) 0.38 0.63 ( 0.18, 2.27) 0.48 0.65 ( 0.13, 3.19) 0.60Obesity 0.92 ( 0.29, 2.90) 0.89 0.31 ( 0.10, 1.01) 0.05 4.53 ( 0.32,64.16) 0.26Chronic neurological disease 6.47 ( 0.49, 84.22) 0.16 0.61 ( 0.03,12.66) 0.75Immunosuppressant use prior to admission 1.17 ( 0.33, 4.16) 0.81 20.41 ( 0.73, 567.89) 0.08 0.99 ( 0.15, 6.71) 0.99July 2014-2015 vs before July 2014-2015 0.60 (0.32, 1.12) 0.11 0.22 (0.07, 0.71) 0.012 1.31 (0.22, 7.93) 0.77
aOR: adjusted Odds Ratio ; CI: Confidence Interval; KAMC-R: King Abdulaziz Medical City-Riyadh.Chi-square Test is used to calculate the P-value#Number of Observations=329,@Number of Observations=165,$Number of Observations=90

Figure S1: Serial Measurements of A. hemoglobin, B. blood urea nitrogen (BUN), C. alanine amino transferase (ALT), D. bilirubin and E. partial presuure of carbon diaoxide in arterial blood (PaCO2) in patients with the Middle East Respiratory Syndrome severe acute respiratory infection (MERS SARI) and non- Middle East Respiratory Syndrome severe acute respiratory infection (Non-MERS SARI). Median and 95% confidence intervals are displayed. * denotes statistical significance for the difference between the two groups on each day after Benferoni correction using independent Student’s t-test or Wilcoxon-Mann-Whitney test based on normality assumption. P values for between group differences and for between group differences over time using repeated measures analysis of variance are given for each variable.
P= 0.78 for
between group differencesP= 0.39 for between group differences over time
P= 0.77 for between group differencesP= 0.95 for between group differences over time
P= 0.54 for between group differencesP= 0.97 for between group differences over time
P= 0.43 for between group differencesP= 0.91 for between group differences over time
P= 0.82 for between group differencesP= 0.11 for between group differences over time
D
A B
A
C
C
E


Figure S2: Percentage of SARI patients who were tested for MERS-CoV rRT-PCR at KAMC-R.

01 Sept 2012- 30 June 2014
01 July 2014-31 DEC 2014
01 Jan 2015- 30 June 2015
01 July 2015-31 DEC 2015
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0
20
40
60
80
100
120
140
160
Number of SARI cases
% tested
% te
sted
for M
ERS-
CoV
rRT-
PCR
Num
ber o
f SAR
I cas
es
Refrences:
1. Ministry of Health. Case Definition and Surveillance Guidance http://www.moh.gov.sa/en/CCC/Regulations/Case Definition.pdf. Accessed on March 31, 2016.
2. The International Severe Acute Respiratory and Emerging Infection Consortium (ISARIC) https://isarictghnorg/ Last accessed March 25, 2016.
3. Vincent JL, de Mendonca A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on "sepsis-related problems" of the European Society of Intensive Care Medicine. Crit Care Med 1998; 26(11): 1793-800.