
CD 004073
195
Vitamin supplementation for preventing miscarriage (Review) Rumbold A, Middleton P, Pan N, Crowther CA This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2011, Issue 1 http://www.thecochranelibrary.com Vitamin supplementation for preventing miscarriage (Review) Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
-
Upload
sabrine-dwigint -
Category
Documents
-
view
4 -
download
1
description
rr
Transcript of CD 004073

Vitamin supplementation for preventing miscarriage (Review)
Rumbold A, Middleton P, Pan N, Crowther CA
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 1
http://www.thecochranelibrary.com
Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
5BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
23ADDITIONAL SUMMARY OF FINDINGS . . . . . . . . . . . . . . . . . . . . . . . . . .
29DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
38CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
91DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 1 Total fetal loss (including
miscarriages or combined miscarriages and stillbirths). . . . . . . . . . . . . . . . . . . . . 106
Analysis 1.2. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 2 Early or late miscarriage. 107
Analysis 1.3. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 3 Placental abruption. 109
Analysis 1.5. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 5 Pre-eclampsia. . . 110
Analysis 1.6. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 6 Stillbirth. . . . . 111
Analysis 1.7. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 7 Perinatal death. . . 112
Analysis 1.8. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 8 Neonatal death. . . 113
Analysis 1.9. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 9 Preterm birth. . . 114
Analysis 1.10. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 10 Very preterm birth. 115
Analysis 1.11. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 11 Birthweight. . . 116
Analysis 1.12. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 12 Small-for-gestational
age. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
Analysis 1.13. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 13 Congenital
malformations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
Analysis 1.14. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 14 Multiple pregnancy. 119
Analysis 1.15. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 15 Apgar score less than
seven at five minutes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
Analysis 1.17. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 17 Anaemia (maternal). 120
Analysis 1.18. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 18 Anaemia (infant). 120
Analysis 1.19. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 19 Placental weight. 121
Analysis 1.20. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 20 Method of feeding. 122
Analysis 1.24. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 24 Any adverse effects of
vitamin supplementation sufficient to stop supplementation. . . . . . . . . . . . . . . . . . 123
Analysis 1.26. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 26 Gynaecological hospital
admission. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
Analysis 1.27. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 27 Admission to neonatal
intensive care unit. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124
Analysis 1.29. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 29 Duration of admission
to the neonatal intensive care unit. . . . . . . . . . . . . . . . . . . . . . . . . . . 125
iVitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.30. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 30 Side effects. . . 125
Analysis 2.1. Comparison 2 Any vitamins (by quality), Outcome 1 Total fetal loss (including miscarriage or combined
miscarriages and stillbirths). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126
Analysis 2.2. Comparison 2 Any vitamins (by quality), Outcome 2 Early or late miscarriage. . . . . . . . . . 127
Analysis 2.3. Comparison 2 Any vitamins (by quality), Outcome 3 Stillbirth. . . . . . . . . . . . . . . 128
Analysis 3.1. Comparison 3 Vitamin C, Outcome 1 Total fetal loss. . . . . . . . . . . . . . . . . . 129
Analysis 3.2. Comparison 3 Vitamin C, Outcome 2 Early or late miscarriage. . . . . . . . . . . . . . . 130
Analysis 3.3. Comparison 3 Vitamin C, Outcome 3 Antepartum haemorrhage and placental abruption. . . . . . 131
Analysis 3.4. Comparison 3 Vitamin C, Outcome 4 Pre-eclampsia. . . . . . . . . . . . . . . . . . 132
Analysis 3.5. Comparison 3 Vitamin C, Outcome 5 Stillbirth. . . . . . . . . . . . . . . . . . . . 133
Analysis 3.6. Comparison 3 Vitamin C, Outcome 6 Perinatal death. . . . . . . . . . . . . . . . . . 134
Analysis 3.7. Comparison 3 Vitamin C, Outcome 7 Neonatal death. . . . . . . . . . . . . . . . . . 135
Analysis 3.8. Comparison 3 Vitamin C, Outcome 8 Preterm birth. . . . . . . . . . . . . . . . . . . 136
Analysis 3.9. Comparison 3 Vitamin C, Outcome 9 Very preterm birth. . . . . . . . . . . . . . . . . 137
Analysis 3.10. Comparison 3 Vitamin C, Outcome 10 Small-for-gestational age. . . . . . . . . . . . . . 138
Analysis 3.11. Comparison 3 Vitamin C, Outcome 11 Birthweight. . . . . . . . . . . . . . . . . . 139
Analysis 3.12. Comparison 3 Vitamin C, Outcome 12 Congenital malformations. . . . . . . . . . . . . 139
Analysis 3.13. Comparison 3 Vitamin C, Outcome 13 Apgar score less than seven at five minutes. . . . . . . . 140
Analysis 3.14. Comparison 3 Vitamin C, Outcome 14 Any adverse effects of vitamin supplementation sufficient to stop
supplementation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
Analysis 3.15. Comparison 3 Vitamin C, Outcome 15 Gynaecological hospital admission. . . . . . . . . . 141
Analysis 3.16. Comparison 3 Vitamin C, Outcome 16 Admission to neonatal intensive care unit. . . . . . . . 142
Analysis 3.17. Comparison 3 Vitamin C, Outcome 17 Side effects. . . . . . . . . . . . . . . . . . 143
Analysis 4.1. Comparison 4 Vitamin A, Outcome 1 Total fetal loss (including miscarriages or combined miscarriages and
stillbirths). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 144
Analysis 4.2. Comparison 4 Vitamin A, Outcome 2 Early or late miscarriage. . . . . . . . . . . . . . . 145
Analysis 4.3. Comparison 4 Vitamin A, Outcome 3 Stillbirth. . . . . . . . . . . . . . . . . . . . 146
Analysis 4.4. Comparison 4 Vitamin A, Outcome 4 Neonatal death. . . . . . . . . . . . . . . . . . 147
Analysis 4.5. Comparison 4 Vitamin A, Outcome 5 Preterm birth. . . . . . . . . . . . . . . . . . . 148
Analysis 4.6. Comparison 4 Vitamin A, Outcome 6 Birthweight. . . . . . . . . . . . . . . . . . . 149
Analysis 4.7. Comparison 4 Vitamin A, Outcome 7 Small-for-gestational age. . . . . . . . . . . . . . . 149
Analysis 4.8. Comparison 4 Vitamin A, Outcome 8 Multiple pregnancy. . . . . . . . . . . . . . . . . 150
Analysis 4.9. Comparison 4 Vitamin A, Outcome 9 Very preterm birth. . . . . . . . . . . . . . . . . 151
Analysis 4.10. Comparison 4 Vitamin A, Outcome 10 Maternal anaemia. . . . . . . . . . . . . . . . 151
Analysis 4.11. Comparison 4 Vitamin A, Outcome 11 Infant anaemia. . . . . . . . . . . . . . . . . 152
Analysis 4.12. Comparison 4 Vitamin A, Outcome 12 Poor growth at childhood follow up. . . . . . . . . . 153
Analysis 5.1. Comparison 5 Multivitamin, Outcome 1 Total fetal loss (including miscarriages or combined miscarriages
and stillbirths). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155
Analysis 5.2. Comparison 5 Multivitamin, Outcome 2 Early or late miscarriage. . . . . . . . . . . . . . 157
Analysis 5.3. Comparison 5 Multivitamin, Outcome 3 Placental abruption. . . . . . . . . . . . . . . . 159
Analysis 5.4. Comparison 5 Multivitamin, Outcome 4 Pre-eclampsia. . . . . . . . . . . . . . . . . . 159
Analysis 5.5. Comparison 5 Multivitamin, Outcome 5 Stillbirth. . . . . . . . . . . . . . . . . . . 160
Analysis 5.6. Comparison 5 Multivitamin, Outcome 6 Perinatal death. . . . . . . . . . . . . . . . . 162
Analysis 5.7. Comparison 5 Multivitamin, Outcome 7 Neonatal death. . . . . . . . . . . . . . . . . 163
Analysis 5.8. Comparison 5 Multivitamin, Outcome 8 Preterm birth. . . . . . . . . . . . . . . . . . 164
Analysis 5.9. Comparison 5 Multivitamin, Outcome 9 Very preterm birth. . . . . . . . . . . . . . . . 165
Analysis 5.10. Comparison 5 Multivitamin, Outcome 10 Birthweight. . . . . . . . . . . . . . . . . 166
Analysis 5.11. Comparison 5 Multivitamin, Outcome 11 Small-for-gestational age (birthweight less than the 10th percentile
or < 2500 g. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167
Analysis 5.12. Comparison 5 Multivitamin, Outcome 12 Congenital malformations. . . . . . . . . . . . 168
Analysis 5.13. Comparison 5 Multivitamin, Outcome 13 Multiple pregnancy. . . . . . . . . . . . . . . 169
Analysis 5.14. Comparison 5 Multivitamin, Outcome 14 Maternal anaemia. . . . . . . . . . . . . . . 170
Analysis 5.15. Comparison 5 Multivitamin, Outcome 15 Breastfeeding. . . . . . . . . . . . . . . . . 171
iiVitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.16. Comparison 5 Multivitamin, Outcome 16 Poor growth at childhood follow up: Underweight in childhood
(6-8 years of age). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
Analysis 5.17. Comparison 5 Multivitamin, Outcome 17 Poor growth at childhood follow up: Stunting in childhood (6-8
years of age). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172
Analysis 5.18. Comparison 5 Multivitamin, Outcome 18 Additional outcomes - infant death. . . . . . . . . 173
Analysis 6.1. Comparison 6 Folic acid, Outcome 1 Total fetal loss (including miscarriages or combined miscarriages and
stillbirths). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 174
Analysis 6.2. Comparison 6 Folic acid, Outcome 2 Early or late miscarriage. . . . . . . . . . . . . . . 176
Analysis 6.3. Comparison 6 Folic acid, Outcome 3 Pre-eclampsia. . . . . . . . . . . . . . . . . . . 178
Analysis 6.4. Comparison 6 Folic acid, Outcome 4 Stillbirth. . . . . . . . . . . . . . . . . . . . . 178
Analysis 6.5. Comparison 6 Folic acid, Outcome 5 Perinatal death. . . . . . . . . . . . . . . . . . 180
Analysis 6.6. Comparison 6 Folic acid, Outcome 6 Neonatal death. . . . . . . . . . . . . . . . . . 180
Analysis 6.7. Comparison 6 Folic acid, Outcome 7 Preterm birth. . . . . . . . . . . . . . . . . . . 181
Analysis 6.8. Comparison 6 Folic acid, Outcome 8 Birthweight. . . . . . . . . . . . . . . . . . . 182
Analysis 6.9. Comparison 6 Folic acid, Outcome 9 Small-for-gestational age. . . . . . . . . . . . . . . 183
Analysis 6.10. Comparison 6 Folic acid, Outcome 10 Congenital malformations. . . . . . . . . . . . . . 184
Analysis 6.11. Comparison 6 Folic acid, Outcome 11 Multiple pregnancy. . . . . . . . . . . . . . . . 185
Analysis 6.12. Comparison 6 Folic acid, Outcome 12 Maternal anaemia. . . . . . . . . . . . . . . . 186
Analysis 6.13. Comparison 6 Folic acid, Outcome 13 Poor growth in childhood: Stunting in childhood (6-8 years of
age). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
Analysis 6.14. Comparison 6 Folic acid, Outcome 14 Poor growth in childhood: Underweight in childhood (6-8 years of
age). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
Analysis 6.15. Comparison 6 Folic acid, Outcome 15 Placental weight. . . . . . . . . . . . . . . . . 188
Analysis 6.16. Comparison 6 Folic acid, Outcome 16 Additional outcomes - infant death. . . . . . . . . . . 188
188ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
189APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
190WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
190HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
190CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
190DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
191SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
191DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
191INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiiVitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Vitamin supplementation for preventing miscarriage
Alice Rumbold1 , Philippa Middleton2, Ning Pan2, Caroline A Crowther2
1The Robinson Institute, The University of Adelaide, Adelaide, Australia. 2ARCH: Australian Research Centre for Health of Women
and Babies, Discipline of Obstetrics and Gynaecology, The University of Adelaide, Adelaide, Australia
Contact address: Alice Rumbold, The Robinson Institute, The University of Adelaide, Ground Floor, Norwich Centre, 55 King William
Road, Adelaide, NT, SA 5006, Australia. [email protected].
Editorial group: Cochrane Pregnancy and Childbirth Group.
Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 1, 2011.
Review content assessed as up-to-date: 7 December 2010.
Citation: Rumbold A, Middleton P, Pan N, Crowther CA. Vitamin supplementation for preventing miscarriage. Cochrane Databaseof Systematic Reviews 2011, Issue 1. Art. No.: CD004073. DOI: 10.1002/14651858.CD004073.pub3.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Miscarriage is a common complication of pregnancy that can be caused by a wide range of factors. Poor dietary intake of vitamins
has been associated with an increased risk of miscarriage, therefore supplementing women with vitamins either prior to or in early
pregnancy may help prevent miscarriage.
Objectives
The objectives of this review are to determine the effectiveness and safety of any vitamin supplementation, on the risk of spontaneous
miscarriage, maternal adverse outcomes and fetal and infant adverse outcomes.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group Trials Register (21 June 2010).
Selection criteria
All randomised and quasi-randomised trials comparing one or more vitamins with either placebo, other vitamins, no vitamins or other
interventions, prior to conception, periconceptionally or in early pregnancy (less than 20 weeks’ gestation).
Data collection and analysis
At least two review authors independently assessed trials for inclusion, extracted data and assessed trial quality.
Main results
We identified 28 trials assessing supplementation with any vitamin(s) starting prior to 20 weeks’ gestation and reporting at least one
primary outcome that was eligible for the review. Overall, the included trials involved 96,674 women and 98,267 pregnancies. Three
trials were cluster randomised and combined contributed data for 62,669 women and 64,210 pregnancies in total. No significant
differences were seen between women taking any vitamins compared with controls for total fetal loss (relative risk (RR) 1.04, 95%
confidence interval (CI) 0.95 to 1.14), early or late miscarriage (RR 1.09, 95% CI 0.95 to 1.25) or stillbirth (RR 0.86, 95% CI 0.65 to
1.13) and most of the other primary outcomes, using fixed-effect models. Compared with controls, women given any type of vitamin(s)
pre or peri-conception were more likely to have a multiple pregnancy (RR 1.38, 95% CI 1.12 to 1.70, three trials, 20,986 women).
1Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Authors’ conclusions
Taking any vitamin supplements prior to pregnancy or in early pregnancy does not prevent women experiencing miscarriage or stillbirth.
However, women taking vitamin supplements may be more likely to have a multiple pregnancy. There is insufficient evidence to
examine the effects of different combinations of vitamins on miscarriage, stillbirth or other maternal and infant outcomes.
P L A I N L A N G U A G E S U M M A R Y
Vitamin supplementation for preventing miscarriage
Supplementing women with any vitamins does not reduce the number of women who miscarry or have a stillbirth.
Poor diet, without enough vitamins, has been associated with an increased risk of women losing their baby in early pregnancy. Taking
vitamin supplements prior to pregnancy or in early pregnancy may reduce the risk of miscarriage, but this review did not find this to
be the case. However, women taking vitamin supplements before or at the time of conception may be more likely to have a multiple
pregnancy. More research is needed to determine the impact of different combinations of vitamins. This review included 28 trials
involving 96,674 women (98,267 pregnancies).
2Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
Vitamin A versus placebo for preventing miscarriage
Patient or population: pregnant women
Settings:
Intervention: vitamin A
Comparison: placebo
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
placebo vitamin A
Total fetal loss (in-
cluding miscarriages or
combined miscarriages
and stillbirths)
Follow-up: 24 weeks1
83 per 10002 86 per 1000
(76 to 97)
RR 1.04
(0.92 to 1.17)
11723
(1 study)
⊕⊕⊕⊕
high3
Neonatal death
Follow-up: 28 days
46 per 10002 50 per 1000
(42 to 60)
RR 1.09
(0.92 to 1.3)
10214
(1 study)
⊕⊕⊕⊕
high3
Preterm birth 282 per 10002 293 per 1000
(251 to 341)
RR 1.04
(0.89 to 1.21)
11723
(1 study)
⊕⊕⊕©
moderate3,4
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
3V
itam
insu
pp
lem
en
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

1 Follow-up up to 24 weeks post birth.2 Control group risk extracted from the original trial reference.3 Only one study for this outcome; therefore no point deducted for inconsistency between studies.4 Gestational age may have been underestimated, because women may have mistaken vaginal bleeding early in pregnancy for menses.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
4V
itam
insu
pp
lem
en
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Miscarriage or pregnancy loss within the first 20 weeks of gesta-
tion is a frequent complication of pregnancy, with 12% to 16% of
all clinically recognised pregnancies ending in miscarriage (Everett
1997; Regan 1989). Recurrent miscarriage, defined as the occur-
rence of three or more consecutive spontaneous miscarriages, af-
fects one to two per cent of women of reproductive age (Coulam
1991). Miscarriage is associated with significant maternal mor-
bidity including haemorrhage and infection and, in some cases,
maternal death (NHMRC 2001), with maternal death more com-
mon in countries that are resource-poor (Goyaux 2001). Women
experiencing miscarriage may suffer significant psychological and
emotional stress. Grief experienced by women and their families
can be complicated by feelings of self-blame, anxiety and depres-
sion, and social withdrawal and marital disturbances may result
(Lee 1996). This emotional distress may be further compounded
when women experience recurrent miscarriage.
Care of women suffering miscarriage is complicated by different
definitions, disagreement on its validity as a clinical disorder and
poor quality data on women not requiring hospital or outpatient
treatment. Miscarriage can be caused by a wide range of factors and
determining the aetiology of miscarriage is often difficult, with a
variety of underlying mechanisms being potentially responsible.
Up to two-thirds of early pregnancy losses (miscarriage before 12
weeks’ gestation), are associated with chromosomal abnormalities
(Stern 1996). While early miscarriages are more likely to be associ-
ated with chromosomal abnormalities and defective placental de-
velopment, late miscarriage (miscarriage occurring between 12 and
20 weeks’ gestation) may be more likely due to structural problems
of the uterus and/or cervix, such as cervical incompetence. Women
experiencing recurrent miscarriage may often have an underlying
medical condition such as autoimmune disease, i.e. systemic lupus
erythematosus and antiphospholipid syndrome, or other blood
clotting disorders such as hyperhomocysteinemia (high levels of
homocysteine in the blood) or another thrombophilia (Preston
1996). Recurrent miscarriage is thought to involve an underly-
ing placental vascular pathology seen also in pre-eclampsia, in-
trauterine growth restriction and placental abruption (Ray 1999).
Current therapies being considered for the prevention of miscar-
riage include progesterone and immunotherapy and these topics
are covered in other Cochrane reviews (Haas 2009; Porter 2006).
Vitamins are essential nutrients required for a range of functions
in the body. Vitamins are either water soluble, such as vitamin C
and the B group vitamins (including folate), or fat soluble such
as vitamin A, D, E and K. Vitamins are obtained from the diet
and also from dietary supplements of either individual vitamin
preparations or a multivitamin preparation. Multivitamins con-
tain a range of vitamins and minerals, usually in doses similar to
the recommended dietary intakes. Folate, vitamin B6 and vitamin
B12 have been recommended for women with hyperhomocys-
teinemia, and therefore supplementation may influence the risk
of spontaneous miscarriage in these women. Similarly, oxidative
stress, where there is overproduction of reactive oxygen molecules
leading to decreased levels of antioxidants, has been linked to spon-
taneous and recurrent miscarriage (Jauniaux 2000; Simsek 1998).
Therefore, intake of antioxidant vitamins such as vitamin C and
vitamin E may be an important factor associated with the risk of
miscarriage. One observational study has demonstrated an associa-
tion between the risk of spontaneous early miscarriage and dietary
factors, with a high risk associated with poor intake of green veg-
etables, fruit and dairy products coupled with a high intake of fat
(Di Cintio 2001). Little information is available about the impact
of vitamins on the risk of early versus late miscarriage; however, di-
etary factors could theoretically influence structural abnormalities
such as cervical incompetence. There is a growing body of research
investigating the relationship between nutrition and placental de-
velopment, fetal growth, pregnancy outcomes and adult diseases
(Godfrey 1996; Morris 2001; NRC 1989). Therefore, adequate
maternal nutrition, particularly vitamin intake, may be an impor-
tant factor in preventing spontaneous miscarriage. There is cur-
rently little information about the most appropriate vitamin type
or combination; therefore, this review will cover all vitamin types.
Similarly, many commercially available vitamin preparations con-
tain a range of combinations of vitamins; therefore, this review
will pool all vitamin types together initially to determine overall if
any vitamins and any improvement in maternal nutrition helps to
prevent miscarriage. We will also discuss individual vitamin types
separately.
The use of any vitamin supplements in pregnancy needs to be care-
fully monitored and evaluated for safety and efficacy. This is par-
ticularly true for early pregnancy use, where there is the potential
for teratogenicity. High maternal levels of preformed vitamin A
(retinoic acid) are known to induce spontaneous miscarriage and
malformations involving the central nervous systems and cardiac
development (WHO 1998). Potential teratogenic effects of other
vitamins have not been reported. In contrast, folate supplementa-
tion and multivitamin supplementation have been associated with
a decreased risk of neural tube defects (Lumley 2001b). Pericon-
ceptional folate and multivitamin supplementation for the preven-
tion of neural tube defects has been covered in another Cochrane
review (Lumley 2001b). Concerns have been raised about the im-
pact of folate and multivitamin supplementation on the rate of
multiple births (Lumley 2001a; Lumley 2001b); however, further
research is needed to establish a direct causal relationship. Potential
side effects of vitamins can occur with hypervitaminosis (excessive
ingestion of one or more vitamins). Hypervitaminosis A (vitamin
A poisoning) has been associated with irritability, fatigue, changes
in the skin, hair loss, headache, and abdominal discomfort (Olsen
1999). Similarly hypervitaminosis D (vitamin D poisoning) has
been associated with nausea, vomiting, weakness, disturbed diges-
tion, and elevated blood and tissue calcium levels (Olsen 1999).
For vitamin E, non-randomised controlled clinical trials of vita-
min E supplementation in a variety of doses have failed to demon-
5Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

strate any consistent side effects (Bendich 1993). However, there
has been limited evaluation of the use of these and other vitamins
in pregnancy. While water soluble vitamins such as vitamin C and
the B group vitamins are easily excreted by the body, the fat soluble
vitamins A, D, E and K may accumulate in the body and in the
developing fetus. The safety of using these vitamins needs to be
clearly demonstrated before they can be recommended for routine
antenatal care.
The aims of this review are to identify all published and unpub-
lished randomised controlled trials that investigate vitamins for
the prevention of miscarriage and to assess the benefits and hazards
of women using vitamins for the prevention of miscarriage.
O B J E C T I V E S
The objectives of this review are:
(1) to determine the effectiveness and safety of any vitamin sup-
plementation taken by women prior to conception, periconcep-
tionally and in early pregnancy on the risk of:
• spontaneous miscarriage;
• maternal adverse outcomes;
• fetal and infant adverse outcomes.
(2) If vitamins are effective, to determine which of these agents
are best and to compare vitamins with other interventions.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All randomised trials and quasi-randomised trials comparing one
or more vitamins with either placebo, other vitamins, no vitamins
or other interventions, prior to conception, periconceptionally or
in early to mid-pregnancy.
The review authors deemed it important to include any supple-
mentation trials, where supplementation began prior to 20 weeks’
gestation, and where at least one primary outcome as specified in
the review was reported, even if the intervention was not specifi-
cally for the prevention of miscarriage. We excluded trials where
the onset of supplementation occurred definitely after 20 weeks’
gestation or where it was reported that the majority of women com-
menced supplementation after 20 weeks’ gestation. We included
trials where the onset of supplementation occurred both prior to
and after 20 weeks’ gestation, and when it could not be established
whether the majority of the women started supplementation prior
to 20 weeks’ gestation. As these trials included some women over
20 weeks’ gestation, who do not meet the eligibility criteria for the
review, the main analyses for fetal loss outcomes were subgrouped
according to the duration of vitamin usage, based on the categori-
sation of gestation at trial entry: before pregnancy, <12 weeks’ ges-
tation, between 12-20 weeks’ gestation or ’mixed’ which included
women enrolled before and after 20 weeks’ gestation).
Types of participants
Pregnant women (less than 20 weeks’ gestation) or women in the
reproductive age group planning on becoming pregnant in the
near future, regardless of whether they are at low or high risk of
having a miscarriage.
Types of interventions
Comparisons of any vitamin(s) alone or in combination with other
agents with either placebo, other vitamin(s), no vitamin(s) or other
interventions for the prevention of miscarriage, either in areas
where there is inadequate dietary intake or where there is presumed
adequate intake of that vitamin(s).
Types of outcome measures
Primary outcomes
For the woman
1. Total fetal loss, defined as the combined numbers of early
miscarriage (spontaneous pregnancy loss less than 12 weeks’
gestation), late miscarriage (spontaneous pregnancy loss greater
than or equal to 12 and less than 20 weeks), and stillbirth
(pregnancy loss at greater than or equal to 20 weeks).
2. Early or late miscarriage.
3. Placental abruption.
4. Pre-eclampsia.
5. Psychological effects (anxiety and depression).
For the infant
1. Stillbirth, perinatal or neonatal death.
2. Preterm birth (defined as birth less than 37 weeks’
gestation).
3. Birthweight.
4. Small-for-gestational age (birthweight less than the third
centile or the most extreme centile reported).
5. Congenital malformations.
To overcome wide variation in the definitions of miscarriage and
stillbirth between studies, we included the combined outcome
’total fetal loss’ in the review.
6Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Secondary outcomes
1. Multiple pregnancy (including only trials supplementing
women prior to or around the time of conception).
2. Very preterm birth (defined as less than 34 weeks’
gestation).
3. Apgar score less than seven at five minutes.
4. Use of blood transfusion for the mother.
5. Anaemia (maternal and infant).
6. Placental weight.
7. Methods of feeding: breastfeeding, formula or both.
8. Subsequent fertility (subsequent pregnancy rate per couple
or as defined by the authors).
9. Poor growth at childhood follow-up.
10. Disability at childhood follow-up.
11. Adverse effects of vitamin supplementation sufficient to
stop supplementation, such as manifestations of
hypervitaminosis, headache, nausea, vomiting, diarrhoea.
12. Maternal views of care.
Use of health service resources
1. Gynaecological hospital admission.
2. Admission to neonatal intensive care unit.
3. Healthcare costs.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group Trials
Register by contacting the Trials Search Co-ordinator (21 June
2010).
The Cochrane Pregnancy and Childbirth Group’s Trials Register
is maintained by the Trials Search Co-ordinator and contains trials
identified from:
1. quarterly searches of the Cochrane Central Register of
Controlled Trials (CENTRAL);
2. weekly searches of MEDLINE;
3. handsearches of 30 journals and the proceedings of major
conferences;
4. weekly current awareness alerts for a further 44 journals
plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL and MEDLINE,
the list of handsearched journals and conference proceedings, and
the list of journals reviewed via the current awareness service can
be found in the ‘Specialized Register’ section within the edito-
rial information about the Cochrane Pregnancy and Childbirth
Group.
Trials identified through the searching activities described above
are each assigned to a review topic (or topics). The Trials Search
Co-ordinator searches the register for each review using the topic
list rather than keywords.
We did not apply any language restrictions.
For details of additional searching carried out for the previous
version of the review, see Appendix 1.
Data collection and analysis
Selection of studies
Two review authors independently assessed for inclusion all the
potential studies identified as a result of the search strategy. We
resolved any disagreement through discussion.
Data extraction and management
We designed a form to extract data. For eligible studies, two review
authors extracted the data using the agreed form. We resolved
discrepancies through discussion. We entered data into Review
Manager software (RevMan 2008) and checked for accuracy.
When information regarding any of the above was unclear, we
attempted to contact authors of the original reports to provide
further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each
study using the criteria outlined in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2009). We resolved any
disagreement by discussion or by involving a third review author.
(1) Sequence generation (checking for possible selection
bias)
We describe for each included study the method used to generate
the allocation sequence in sufficient detail to allow an assessment
of whether it should produce comparable groups.
We assessed the method as:
• adequate (any truly random process, e.g. random number
table; computer random number generator),
• inadequate (any non-random process, e.g. odd or even date
of birth; hospital or clinic record number) or,
• unclear.
(2) Allocation concealment (checking for possible selection
bias)
We describe for each included study the method used to conceal
the allocation sequence and determine whether intervention allo-
cation could have been foreseen in advance of, or during recruit-
ment, or changed after assignment.
We assessed the methods as:
7Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

• adequate (e.g. telephone or central randomisation;
consecutively numbered sealed opaque envelopes);
• inadequate (open random allocation; unsealed or non-
opaque envelopes, alternation; date of birth);
• unclear.
(3) Blinding (checking for possible performance bias)
We described for each included study the methods used, if any, to
blind study participants and personnel from knowledge of which
intervention a participant received. We will consider that studies
are at low risk of bias if they were blinded, or if we judge that the
lack of blinding could not have affected the results. We will assess
blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
• adequate, inadequate or unclear for participants;
• adequate, inadequate or unclear for personnel;
• adequate, inadequate or unclear for outcome assessors.
(4) Incomplete outcome data (checking for possible attrition
bias through withdrawals, dropouts, protocol deviations)
We describe for each included study, and for each outcome or class
of outcomes, the completeness of data including attrition and ex-
clusions from the analysis. We state whether attrition and exclu-
sions were reported, the numbers included in the analysis at each
stage (compared with the total randomised participants), reasons
for attrition or exclusion where reported, and whether missing data
were balanced across groups or were related to outcomes. Where
sufficient information was reported, or supplied by the trial au-
thors, we re-included missing data in the analyses which we un-
dertook. We assessed methods as:
• adequate;
• inadequate;
• unclear.
(5) Selective reporting bias
We describe for each included study how we investigated the pos-
sibility of selective outcome reporting bias and what we found.
We assess the methods as:
• adequate (where it is clear that all of the study’s pre-
specified outcomes and all expected outcomes of interest to the
review have been reported);
• inadequate (where not all the study’s pre-specified outcomes
have been reported; one or more reported primary outcomes were
not pre-specified; outcomes of interest are reported incompletely
and so cannot be used; study fails to include results of a key
outcome that would have been expected to have been reported);
• unclear.
Measures of treatment effect
Dichotomous data
For dichotomous data, we present results as summary risk ratio
(RR) with 95% confidence intervals (CI).
Continuous data
For continuous data, we used the mean difference if outcomes
were measured in the same way between trials. We use the stan-
dardised mean difference to combine trials that measured the same
outcome, but used different methods.
Unit of analysis issues
Where trials recruited women prior to becoming pregnant, we re-
ported the denominators for each trial as all women randomised;
or where there was accurate information about the number of
women in each trial who became pregnant, we reported the de-
nominators as the number of women randomised and with a con-
firmed pregnancy.
We included all included trials in the initial analyses which we
performed by any vitamin to include all vitamin combinations
and then by individual vitamin type.
Cluster-randomised trials
We included cluster-randomised trials in the analyses along with
individually randomised trials. We adopted a generic inverse vari-
ance approach for the meta-analyses for dichotomous outcomes
where trials using cluster-randomisation techniques were included
(Alderson 2004).
Dealing with missing data
For included studies, we noted levels of attrition. We explored the
impact of including studies with high levels of missing data in the
overall assessment of treatment effect by using Sensitivity analysis.
For all outcomes, we carried out analyses, as far as possible, on an
intention-to-treat basis, i.e. we attempted to include all partici-
pants randomised to each group in the analyses, and analysed all
participants in the group to which they were allocated, regardless
of whether or not they received the allocated intervention. The
denominator for each outcome in each trial was the number ran-
domised minus any participants whose outcomes were known to
be missing.
Assessment of heterogeneity
We applied tests of heterogeneity between trials to assess the signif-
icance of any differences between trials in the analyses (I2 greater
8Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

than or equal to 30%) and we explored possible causes of hetero-
geneity.
Data synthesis
We carried out statistical analysis using the Review Manager soft-
ware (RevMan 2008). We used fixed-effect meta-analysis for com-
bining data where it is reasonable to assume that studies are es-
timating the same underlying treatment effect: i.e. where trials
are examining the same intervention, and we judged the trials’
populations and methods sufficiently similar. If there is clinical
heterogeneity sufficient to expect that the underlying treatment
effects differ between trials, or if we detect substantial statistical
heterogeneity, we used random-effects meta-analysis to produce
an overall summary if an average treatment effect across trials is
considered clinically meaningful. We treated the random-effects
summary as the average range of possible treatment effects and we
discuss the clinical implications of treatment effects differing be-
tween trials. If the average treatment effect is not clinically mean-
ingful we would not combine trials.
Where we used random-effects analyses, we have presented the
results as the average treatment effect with its 95% confidence
interval.
Subgroup analysis and investigation of heterogeneity
Where included studies had more than two treatment arms or
compared one or more vitamin intervention with another, we have
not included these studies in the main analysis of ’any vitamins
versus no or minimal vitamins’. We used data from these trials
only in the subgroup analyses according to vitamin type.
As some of the trials included women over 20 weeks’ gestation,
who do not meet the eligibility criteria for the review, we have
subgrouped the main analyses for fetal loss outcomes according to
the duration of vitamin usage subgroup.
Where possible, we classified women into subgroups based on:
1. the type of vitamin (vitamin C, vitamin A, multivitamin
and folic acid);
2. the duration of vitamin usage, based on time of trial entry:
before pregnancy, < 12 weeks’ gestation, between 12-20 weeks’
gestation or ’mixed’, which included women enrolled before and
after 20 weeks’ gestation;
3. the dose of vitamin(s) (below or above the recommended
dietary intake);
4. their risk of spontaneous miscarriage (high risk defined as
the presence of medical conditions associated with miscarriage
such as hyperhomocysteinemia, thrombophilia,
antiphospholipid syndrome, systemic lupus erythematosus; low
risk defined as none of the above conditions); their risk of
recurrent miscarriage (high risk defined as two or more previous
consecutive spontaneous miscarriages, and/or the presence of
medical conditions associated with miscarriage such as
hyperhomocysteinemia, thrombophilia, antiphospholipid
syndrome, systemic lupus erythematosus; low risk defined as
none of the above conditions);
5. low or adequate dietary vitamin intake at trial entry (low
intake defined as less than the recommended daily intake for each
vitamin in that setting, as measured by dietary questionnaire).
If we identified substantial heterogeneity, we performed subgroup
analyses for the main fetal loss outcomes (total fetal loss, early or
late miscarriage, stillbirth) by the above subgroups (where possi-
ble). We modelled heterogeneity that was not explained by sub-
group analyses using a random-effects analysis.
For fixed-effect inverse variance meta-analyses we assessed differ-
ences between subgroups by interaction tests. For random-effects
and fixed-effect meta-analyses using methods other than inverse
variance, we assessed differences between subgroups by inspec-
tion of the subgroups’ confidence intervals; non-overlapping con-
fidence intervals indicate a statistically significant difference in
treatment effect between the subgroups.
Sensitivity analysis
We carried out sensitivity analyses to explore the effect of trial
quality on the primary outcomes related to fetal loss (total fetal
loss, early or late miscarriage, stillbirth). This involved restricting
the analyses to trials with an ’adequate’ rating of allocation con-
cealment. We considered these trials high quality.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of
excluded studies; Characteristics of studies awaiting classification;
Characteristics of ongoing studies.
See tables ’Characteristics of included studies’ and ’Characteristics
of excluded studies’ for details of individual studies.
Included studies
We identified 28 trials assessing supplementation with any vita-
min(s) starting prior to 20 weeks’ gestation. The included trials
involved 34,005 women plus a further 62,669 women who were
enrolled in the three cluster randomised trials. Two of the trials
(one cluster and one small trial) included women who were preg-
nant more than once in the study period, resulting in data being
contributed for 64,210 pregnancies from the cluster trials, and
34,057 pregnancies for the individual trials. Many of the trials as-
sessed interventions not specifically for the prevention of miscar-
riage. Four of the included studies were assessing folic acid supple-
mentation for the prevention of neural tube defects (Czeizel 1994;
ICMR 2000; Kirke 1992; MRC 1991). For the purpose of this
9Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

review however, the authors deemed it important to include any
supplementation trials, where supplementation began prior to 20
weeks’ gestation, and where at least one main outcome as specified
in the review was reported.
Participants
The demographic and obstetric characteristics of women varied
widely between the trials (See table ’Characteristics of included
studies’), as did the gestational age at trial entry and the type
of supplements. Some trials enrolled women prior to conception
(Christian 2003; Czeizel 1994; Hemmi 2003; ICMR 2000; Kirke
1992; MRC 1991) and asked women to continue taking the sup-
plements up until the second or third missed menstrual period.
One trial (Katz 2000) supplemented women from before to con-
ception, through pregnancy and up to 3.5 years postpartum. Other
trials enrolled women in the first trimester (Briscoe 1959; Rumiris
2006) or in early to mid pregnancy (Chappell 1999; Correia
1982; Fawzi 1998; Fawzi 2007; Fleming 1968; Fleming 1986;
Kumwenda 2002; Osrin 2005; People’s League 1942; Roberfroid
2008; Rumbold 2006; Rush 1980; Schmidt 2001; Steyn 2003;
Taylor 1982; Van den Broek 2006; Villar 2009). Some of the trials
enrolling women in early to mid pregnancy included women en-
rolled at or after 20 weeks’ gestation (Chappell 1999; Fawzi 1998;
Fawzi 2007; Fleming 1968; Fleming 1986; Kumwenda 2002;
Osrin 2005; People’s League 1942; Roberfroid 2008; Rumbold
2006; Rush 1980; Schmidt 2001; Spinnato 2007; Steyn 2003;
Van den Broek 2006; Villar 2009); however, none of these studies
separately reported data on the proportion of women who met
the eligibility criteria for the review (i.e. less than 20 weeks’ ges-
tation). One trial (The Summit 2008), enrolled 41,839 women
at ’any gestational age’, however more than 70% of women were
enrolled in the first or second trimester. Two trials (Fawzi 1998;
Kumwenda 2002) involved vitamin A supplementation in women
seropositive for the Human Immunodeficiency Virus (HIV).
The trials were conducted in both resource-rich and resource-
poor countries including the United States (Briscoe 1959; Rush
1980), the United Kingdom (Chappell 1999; People’s League
1942; Taylor 1982), Portugal (Correia 1982), Hungary (Czeizel
1994), Tanzania (Fawzi 1998; Fawzi 2007), Nigeria (Fleming
1968; Fleming 1986), Burkino Faso (Roberfroid 2008), Japan
(Hemmi 2003), India (ICMR 2000), Nepal (Christian 2003; Katz
2000; Osrin 2005), the Republic of Ireland (Kirke 1992), Australia
(Rumbold 2006), Brazil (Spinnato 2007), Malawi (Kumwenda
2002; Van den Broek 2006), Indonesia (Rumiris 2006; Schmidt
2001; The Summit 2008) and South Africa (Steyn 2003). One trial
involved 33 international centres (MRC 1991) and another trial
involved India, Peru, South Africa and Viet Nam (Villar 2009).
Interventions
The 28 trials assessed a range of vitamin supplements, alone
or in combination with other supplements. The vitamins in-
cluded vitamin A, alone or with iron, folic acid, zinc or multi-
vitamins (Christian 2003; Fawzi 1998; Katz 2000; Kumwenda
2002; Schmidt 2001; Van den Broek 2006), vitamin C with
or without multivitamins or vitamin E (Briscoe 1959; Chappell
1999; Hemmi 2003; Rumbold 2006; Spinnato 2007; Steyn 2003;
Villar 2009), folic acid with or without multivitamins and/or
iron (Correia 1982; Czeizel 1994; Fleming 1968; Fleming 1986;
ICMR 2000; Kirke 1992; MRC 1991; Taylor 1982), multivita-
mins with iron and folic acid (Fawzi 2007; Osrin 2005; Roberfroid
2008; Rumiris 2006; The Summit 2008) and multivitamins alone
(People’s League 1942; Rush 1980). The doses of vitamins were
similar for the vitamin C supplementation trials (range 400 mg
to 1000 mg). However, they varied widely between trials for the
folic acid (range 0.3 mg to 10 mg), multivitamins and vitamin A
trials (range 5000 international units (IU) to 23,300 IU).
We were unable to include data from 12 trials in the analysis of ’any
vitamins versus no or minimal vitamins’ because the trials either
had more than two treatment arms or compared one or more vita-
min interventions with each other. For example, one trial (Fawzi
1998) using a 2 x 2 factorial design compared vitamin A supple-
ments with or without multivitamins versus multivitamins (ex-
cluding vitamin A) or placebo. However, results were not explicitly
presented for each group. Similarly, three trials (Kumwenda 2002;
Schmidt 2001; Van den Broek 2006) compared vitamin A sup-
plements with iron and folic acid versus iron and folic acid alone,
and one trial with five treatment arms (Christian 2003) compared
multivitamins with iron, folic acid and vitamin A versus iron, folic
acid and vitamin A alone. Other trials compared folic acid alone
with multivitamins plus folic acid or multivitamins excluding folic
acid (Kirke 1992), multivitamins with vitamin E compared with
multivitamins without vitamin E (Rush 1980), or multivitamins
with iron and folic acid versus iron and folic acid (Fawzi 2007;
Osrin 2005; Roberfroid 2008; Rumiris 2006; The Summit 2008).
We used data from these trials only in the sub analyses according
to vitamin type, as none of the treatment arms were comparable to
the control groups used in the trials included in the ’any vitamins
versus no or minimal vitamins’ comparisons.
Outcomes
Main outcomes
Twenty-four trials reported either pregnancy loss as miscarriage or
stillbirth. We included four trials (Christian 2003; Correia 1982;
Taylor 1982; Villar 2009) as they reported main outcomes (peri-
natal death, neonatal death, infant death, preterm birth, birth-
weight, small-for-gestational age); however, information on mis-
carriage or stillbirth was either not reported separately or at all.
The outcome ’total fetal loss’ included both miscarriage or still-
birth, and overcame problems with different definitions of mis-
carriage and stillbirth. For some trials, miscarriage was considered
to occur up until 26 or 28 weeks’ gestation, while other studies
10Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

reported miscarriage as pregnancy loss prior to 20 weeks’ gesta-
tion, and stillbirth as pregnancy loss greater than or equal to 20
weeks’ gestation. Other studies did not specify their definition
of miscarriage or stillbirth. For the other main outcomes for the
mother, five trials reported placental abruption (Chappell 1999;
Rumbold 2006; Rumiris 2006; Spinnato 2007; Villar 2009), and
another trial (Steyn 2003) reported antepartum haemorrhage in-
cluding placental abruption. Eight trials reported pre-eclampsia or
’toxaemia’ (Chappell 1999; Fleming 1968; People’s League 1942;
Rumbold 2006; Rumiris 2006; Spinnato 2007; Steyn 2003; Villar
2009); no trials reported any psychological effects. For the infant,
perinatal death was reported in nine trials (Christian 2003; Fawzi
2007; Osrin 2005; Roberfroid 2008; Rumbold 2006; Spinnato
2007; Steyn 2003; The Summit 2008; Villar 2009), neonatal death
in 12 trials (Christian 2003; Czeizel 1994; Katz 2000; Fawzi 2007;
Osrin 2005; People’s League 1942; Roberfroid 2008; Rumbold
2006; Rush 1980; Spinnato 2007; Steyn 2003; The Summit
2008), preterm birth in sixteen trials (Chappell 1999; Christian
2003; Czeizel 1994; Fawzi 1998; Fawzi 2007; Fleming 1968; Katz
2000; Osrin 2005; Roberfroid 2008; Rumiris 2006; Rumbold
2006; Rush 1980; Spinnato 2007; Steyn 2003; The Summit 2008;
Van den Broek 2006), very preterm birth in six trials (Fawzi
1998; Fawzi 2007; Rumbold 2006; Spinnato 2007; Steyn 2003;
Villar 2009), birthweight in 10 trials (Christian 2003; Correia
1982; Czeizel 1994; Fawzi 2007; Kumwenda 2002; Osrin 2005;
Roberfroid 2008; Rumbold 2006; Spinnato 2007; Taylor 1982),
small-for-gestational age in 13 trials (Chappell 1999; Christian
2003; Czeizel 1994b; Fawzi 1998; Fawzi 2007; Fleming 1968;
ICMR 2000; Roberfroid 2008; Rumbold 2006; Rumiris 2006;
Spinnato 2007; The Summit 2008; Villar 2009) and congenital
malformations in six trials (Czeizel 1994; Kirke 1992; MRC 1991;
Osrin 2005; Spinnato 2007; Villar 2009). In this review, congen-
ital malformations covered malformations excluding neural tube
defects, as these are covered in the Cochrane review ’Periconcep-
tional supplementation with folate and/or multivitamins for pre-
venting neural tube defects’ (Lumley 2001b).
Other outcomes
Five trials reported multiple pregnancy (Czeizel 1994b; Fleming
1968; ICMR 2000; Katz 2000; Kumwenda 2002); one trial re-
ported Apgar score less than seven at five minutes (Spinnato 2007);
six trials reported maternal anaemia (variously defined) (Christian
2003; Fawzi 1998; Fawzi 2007; Fleming 1986; Osrin 2005; Van
den Broek 2006); two trials reported infant anaemia at various ages
(Fawzi 1998; Kumwenda 2002) and one trial reported placental
weight (Correia 1982). Three trials reported various measures of
childhood growth including weight and length at six weeks and
four months (Kumwenda 2002; Schmidt 2001), and stunting and
underweight in children aged 6-8 years (Christian 2003). One trial
reported on mode of feeding as the number of women breastfeed-
ing (People’s League 1942). One trial reported on adverse effects
of vitamin supplementation sufficient to stop supplementation
(Spinnato 2007) and one trial reported on side effects (Rumbold
2006). Three trials reported on measures of use of health service
resources including maternal admission to ICU (Villar 2009), and
admission to the neonatal intensive care unit (Rumbold 2006;
Steyn 2003; Villar 2009). The following outcomes were not re-
ported by any of the trials: use of blood transfusion for the mother,
subsequent fertility, disability at childhood follow up, and mater-
nal views of care.
Additional outcomes
One trial (Steyn 2003) reported birthweight as the median birth-
weight and range; however, these data were not in a format suitable
for inclusion in the birthweight comparisons (see Table 1). One
trial (Christian 2003) reported infant death and we have included
this outcome in the ’other outcomes reported’ for the multivita-
min and folic acid comparisons.
Excluded studies
We excluded 38 trials, of which 12 reported no clinically meaning-
ful data in a format suitable for inclusion (Hibbard 1968; Laurence
1981; Lira 1989; Meirinho 1987; Mock 2002; Moldenhauer
2002; Semba 2001; Suharno 1993; Tanumihardjo 2002; Thauvin
1992; Villamor 2002; Vutyavanich 1995). Six trials did not clearly
report the gestational age when supplementation was started
(Biswas 1984; Fletcher 1971; Hampel 1974; Lumeng 1976;
Schuster 1984; Trigg 1976) and for two trials the majority of
women were enrolled after 20 weeks and did not report outcomes
separately for women starting supplementation prior to 20 weeks
(Ferguson 1955; Giles 1971). Eleven trials (Baumslag 1970; Blot
1981; Chanarin 1968; Colman 1974; Coutsoudis 1999; Dawson
1962; Edelstein 1968; Feyi-Waboso 2005; Hankin 1966; Marya
1981; Metz 1965; Owen 1966) reported supplementation after
20 weeks’ gestation. One trial (Ross 1985) did not specify the
contents of the supplements; in three trials all women were given
a vitamin supplement (Hunt 1984; Huybregts 2009; Shu 2002);
and two were non-randomised (Smithells 1981; Ulrich 1999).
Three other trials (Beazley 2002; Chaudhuri 1969; Rivas 2000)
supplemented women for the prevention of pre-eclampsia, and
did not report any outcomes related to pregnancy loss. These trials
are covered in the Cochrane review ’Antioxidants for preventing
pre-eclampsia’ (Rumbold 2008).
Risk of bias in included studies
Figure 1 and Figure 2 illustrate that the trials were of variable
quality. In the main analysis, only 10% to 20% weight is from
high-quality trials. Two trials (Fleming 1968; People’s League
1942) used quasi-random allocation methods involving alternate
allocation of participants. Similarly, three trials (Christian 2003;
Katz 2000; The Summit 2008) used cluster randomisation. Two
11Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of these (Christian 2003; Katz 2000) allocated subdistricts within
Nepal to each treatment arm and randomised women by “drawing
numbered identical chits from a hat, blocked on subdistrict”; one
trial (The Summit 2008) allocated individual midwives to each
treatment arm. Concealment of allocation was adequate in 13
trials and blinding was adequate in 17 trials. For many of the other
trials there was inadequate reporting of methodological details to
make an assessment about the risk of bias.
Figure 1. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies
12Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study
13Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

In order to examine possible publication bias, we undertook funnel
plots which graph the effect size against sample size for each trial
for outcomes with 10 or more studies. For the comparisons of any
vitamins versus no vitamins, the funnel plots were symmetrical for
the outcomes total fetal loss (Figure 3) and early or late miscarriage
(Figure 4), indicating a low possibility of publication bias. The
graphs for the analysis of multivitamins were less symmetrical for
the outcomes total fetal loss (Figure 5), early or late miscarriage
(Figure 6), indicating the possibility that smaller negative trials
may be missing.
Figure 3. Funnel plot of comparison: 1 Any vitamins versus no vitamins (or minimal vitamins), outcome: 1.1
Total fetal loss (including miscarriages or combined miscarriages and stillbirths)
14Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
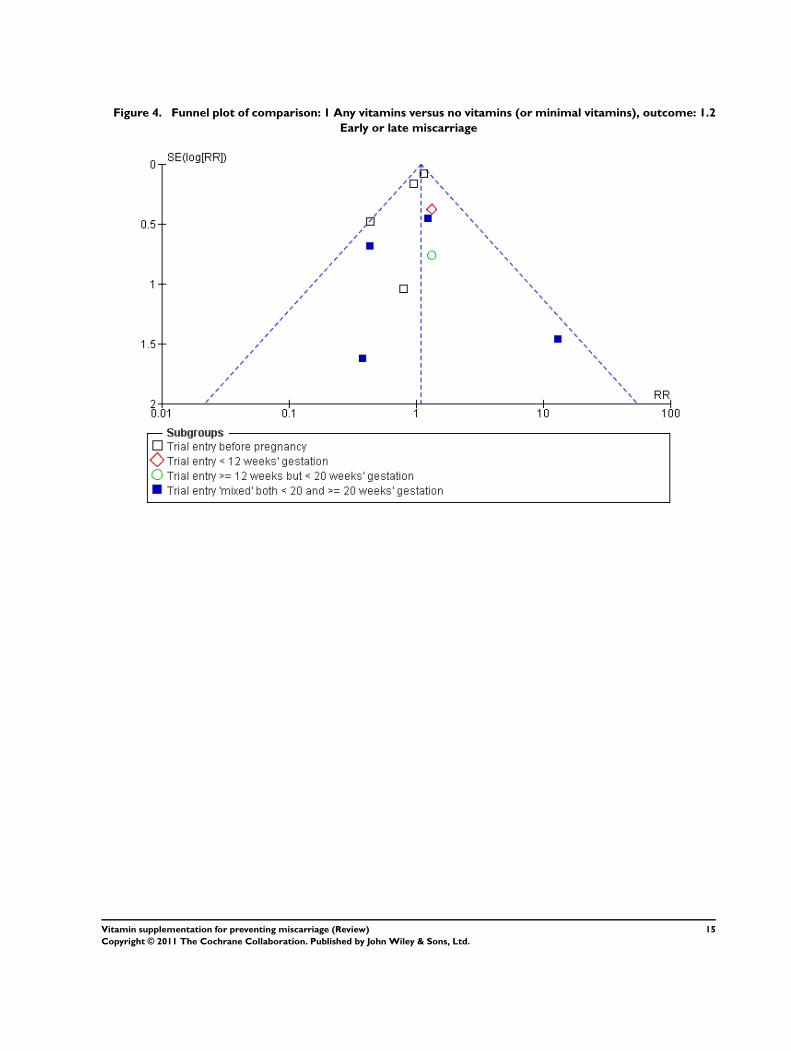
Figure 4. Funnel plot of comparison: 1 Any vitamins versus no vitamins (or minimal vitamins), outcome: 1.2
Early or late miscarriage
15Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 5. Funnel plot of comparison: 5 Multivitamin, outcome: 5.1 Total fetal loss (including miscarriages or
combined miscarriages and stillbirths)
16Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 6. Funnel plot of comparison: 5 Multivitamin, outcome: 5.2 Early or late miscarriage
Effects of interventions
See: Summary of findings for the main comparison Vitamin A
versus placebo for preventing miscarriage; Summary of findings
2 Vitamin A versus B-Carotene for preventing miscarriage;
Summary of findings 3 Vitamin A plus iron plus folate versus
iron plus folate for preventing miscarriage
We have included 28, involving 96,674 women and 98,267 preg-
nancies.
Any vitamins versus no vitamins (or minimal
vitamins)
Primary outcomes
For the woman
For the outcomes of miscarriage and stillbirth, 13 trials contributed
data which included 33,943 pregnancies (Briscoe 1959; Chappell
1999; Czeizel 1994; Fleming 1968; Fleming 1986; Hemmi 2003;
ICMR 2000; Katz 2000; MRC 1991; People’s League 1942;
Rumbold 2006; Spinnato 2007; Steyn 2003). No difference was
seen between women given any type of vitamin(s) compared with
controls for total fetal loss (relative risk 1.04, 95% confidence in-
terval (CI) 0.95 to 1.14, Analysis 1.1) or early or late miscarriage
(risk ratio (RR) 1.09, 95% CI 0.95 to 1.25, Analysis 1.2), using
fixed-effect models. These findings occurred regardless of whether
the trials started supplementation prior to pregnancy, in the first
12 weeks of pregnancy, before 20 weeks’ gestation or both prior to
and after 20 weeks’ gestation. For the other primary maternal out-
comes, no clear difference was seen between women given any type
of vitamin(s) compared with controls for placental abruption (RR
0.66, 95% CI 0.34 to 1.30, four trials, 4264 women (Chappell
1999; Rumbold 2006; Spinnato 2007; Villar 2009), Analysis 1.3),
antepartum haemorrhage including placental abruption (RR 7.00,
95% CI 0.88 to 55.86, one trial, 200 women (Steyn 2003)).
Heterogeneity
We found significant heterogeneity for pre-eclampsia. For pre-
eclampsia, this heterogeneity is likely to be due to the inclu-
sion of People’s League 1942, which was quasi-randomised. Us-
ing a random-effects model, there was no clear difference be-
tween women given any type of vitamin(s) compared with con-
trols for pre-eclampsia (RR 0.88, 95% CI 0.70 to 1.09, 7 trials,
9561 women, Tau2 0.04 (Chappell 1999; Fleming 1968; People’s
17Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

League 1942; Rumbold 2006; Spinnato 2007; Steyn 2003; Villar
2009), Analysis 1.5).
For the infant
No difference was seen between women given any type of vita-
min(s) compared with controls for stillbirth (RR 0.86, 95% CI
0.65 to 1.13, nine trials, 15,980 women (Chappell 1999; Czeizel
1994; Fleming 1968; ICMR 2000; MRC 1991; People’s League
1942; Rumbold 2006; Spinnato 2007; Steyn 2003), Analysis
1.6); perinatal death (RR 0.83, 95% CI 0.62 to 1.11, four trials,
4313 women (Rumbold 2006; Spinnato 2007; Steyn 2003; Villar
2009), Analysis 1.7); neonatal death (relative risk 1.11, 95% CI
0.94 to 1.31, six trials, 27,657 women (Czeizel 1994b; Katz 2000;
People’s League 1942; Rumbold 2006; Spinnato 2007; Steyn
2003), Analysis 1.8); preterm birth (relative risk 1.02 95% CI
0.94 to 1.10, eight trials, 27,657 women (Chappell 1999; Czeizel
1994; Fleming 1968; Katz 2000; Rumbold 2006; Spinnato 2007;
Steyn 2003; Villar 2009), Analysis 1.9); small-for-gestational-
age infants (RR 0.96 95% CI 0.84 to 1.08, seven trials, 9,356
women (Chappell 1999; Czeizel 1994; Fleming 1968; ICMR
2000; Rumbold 2006; Spinnato 2007; Villar 2009), Analysis 1.12)
or congenital malformations (RR 1.47, 95% CI 0.90 to 2.40, four
trials, 8933 women (Czeizel 1994; MRC 1991; Spinnato 2007;
Villar 2009), Analysis 1.13).
Heterogeneity
We found significant heterogeneity for birthweight. This is likely
to be due to the inclusion of Correia 1982, which was at high risk of
bias due to more than 20% of participants being excluded. Using
a random-effects model, there was no clear difference between
women given any type of vitamin(s) compared with controls for
birthweight (mean difference (MD) 16.99 g, 95% CI -37.66 to
71.64, five trials, 7497 women, Tau2 1748.69 (Correia 1982;
Czeizel 1994b; Rumbold 2006; Spinnato 2007; Taylor 1982),
Analysis 1.11). When this trial was excluded from the analysis there
was no heterogeneity present; however the direction of effects did
not change (MD 2.01, 95% CI -21.51-25.52, four trials, 7468
women (Czeizel 1994b; Rumbold 2006; Spinnato 2007; Taylor
1982)).
Secondary outcomes
Women given any type of vitamin(s) compared with controls
were more likely to have a multiple pregnancy (relative risk 1.38,
95% CI 1.12 to 1.70, three trials, 20,986 women (Czeizel 1994b;
ICMR 2000; Katz 2000)) and greater placental weight (MD 96.00
g, 95% CI 30.73 to 161.27, one trial, 29 women (Correia 1982)).
No overall difference was seen between women given any vita-
min(s) compared with controls for the outcomes very preterm
birth (RR 0.93, 95% CI 0.75 to 1.15, four trials, 4181 women
(Rumbold 2006; Spinnato 2007; Steyn 2003; Villar 2009)); Ap-
gar score less than seven at five minutes (RR 0.66, 95% CI 0.27 to
1.60, 1 trial, 700 women (Spinnato 2007)); infant anaemia (RR
1.05, 95% CI 0.98 to 1.12, one trial, 836 infants (Fawzi 1998));
the number of women breastfeeding (RR 0.98, 95% CI 0.96 to
1.01, one trial, 4878 women (People’s League 1942)); any mater-
nal admission to the intensive care unit (RR 0.20, 95% CI 1.69,
one trial, 1365 women (Villar 2009)); any admission to the neona-
tal intensive care unit (RR 0.81, 95% CI 0.59 to 1.11, one trial,
1515 infants (Villar 2009)) or the duration of admission to the
neonatal intensive care unit (MD 1.30 days, 95% CI -0.28 to 2.88,
one trial, 181 women (Steyn 2003)). There was no significant dif-
ference between women given any type of vitamin(s) compared
with controls for adverse effects sufficient to stop supplementation
(RR 1.16, 95% CI 0.39 to 3.41, one trial, 739 women (Spinnato
2007)); however, women given any type of vitamin(s) were more
likely to report abdominal pain compared with controls (RR 1.63,
95% CI 1.12 to 2.36, one trial, 1734 women (Rumbold 2006)).
Heterogeneity
We found significant heterogeneity for maternal anaemia. The
cause of this heterogeneity is unclear, however it may be due to
differences in the participants; for example, one study (Fawzi
1998) included women who were HIV positive. There was no
significant difference between women given any type of vitamin(s)
compared with controls for maternal anaemia (RR 0.90, 95%
CI 0.46 to 1.73, 2 trials, 1190 women, Tau2 0.16 (Fawzi 1998;
Fleming 1986)) using a random-effects model. No other secondary
outcomes were reported.
Sensitivity analyses by quality rating
Five trials had an allocation concealment rating of ’Adequate’
(Chappell 1999; Kirke 1992; Kumwenda 2002; MRC 1991; Steyn
2003); 10 trials had a rating of ’Unclear’ (Briscoe 1959; Christian
2003; Correia 1982; Czeizel 1994; Fawzi 1998; Hemmi 2003;
ICMR 2000; Katz 2000; Rush 1980; Schmidt 2001) and two tri-
als had a rating of ’No’ (Fleming 1968; People’s League 1942). The
sensitivity analyses excluded the trials with an allocation conceal-
ment rating of unclear or ’No’ (inadequate). Amongst the trials
with adequate allocation concealment (high quality studies), there
was no difference in total fetal loss between women supplemented
with any vitamins compared with controls (relative risk 0.97, 95%
CI 0.84 to 1.12, five trials, 4916 women (Chappell 1999; MRC
1991; Rumbold 2006; Spinnato 2007; Steyn 2003)). Similarly,
we found no difference between women supplemented with any
vitamins compared with controls for early or late miscarriage or
stillbirth, when the analyses were restricted to high quality studies
only. These sensitivity analyses indicate that the analyses for the
effects of any vitamins on outcomes related to fetal loss are no
different when only high quality studies are included.
18Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Subgroup analyses by vitamin type
Vitamin C supplementation
The trials involving vitamin C supplementation included the fol-
lowing interventions: vitamin C plus multivitamins versus placebo
plus multivitamins (Briscoe 1959), vitamin C and vitamin E sup-
plementation versus placebo (Chappell 1999; Rumbold 2006;
Spinnato 2007; Villar 2009) and vitamin C alone versus no sup-
plement or placebo (Hemmi 2003; Steyn 2003).
Primary outcomes
For the woman
We found no significant difference in the risk of total fetal loss be-
tween women receiving vitamin C with multivitamins compared
with placebo plus multivitamins (RR 1.32, 95% CI 0.63 to 2.77,
one trial, 406 women (Briscoe 1959)), vitamin C and vitamin E
compared with placebo (RR 0.82, 95% CI 0.48 to 1.42, three
trials, 2899 women (Chappell 1999; Rumbold 2006; Spinnato
2007)) or vitamin C compared with no supplement or placebo
(RR 1.28, 95% CI 0.58 to 2.83, two trials, 224 women (Hemmi
2003; Steyn 2003)) (Analysis 3.1). Similarly, there was no overall
difference seen in early or late miscarriage between women receiv-
ing vitamin C with multivitamins compared with placebo plus
multivitamins (RR 1.32, 95% CI 0.63 to 2.77, one trial, 406
women (Briscoe 1959)), vitamin C and vitamin E compared with
placebo (RR 0.70, 95% CI 0.27 to 1.84, two trials, 2616 women
(Rumbold 2006; Spinnato 2007) or vitamin C compared with no
supplement or placebo (RR 1.17, 95% CI 0.52 to 2.65, two trials,
224 women (Hemmi 2003; Steyn 2003)).
There was no significant difference between women receiving any
combination of vitamin C supplementation compared with con-
trol for other primary outcomes including placental abruption or
antepartum haemorrhage.
Heterogeneity
We found significant heterogeneity for the outcome pre-eclampsia
in the subgroup analyses of vitamin C and E versus placebo. Using
a random-effects analysis, there was no significant difference in
the risk of pre-eclampsia amongst women given vitamin C and
E supplementation compared with a placebo (RR 0.94, 95% CI
0.72 to 1.22, four trials, 4264 women, Tau2 0.04 (Chappell 1999;
Rumbold 2006; Spinnato 2007; Villar 2009)), or women given
vitamin C alone compared with placebo (RR 1.00, 95% CI 0.21
to 4.84, one trial, 200 women (Steyn 2003)). The heterogeneity
appears to be due to the inclusion of Chappell 1999, and may
be due to differences in the risk profile of participants. When we
excluded this study from the analysis there was no heterogeneity,
and the direction of effects moved towards the null (RR 1.03,
95% CI 0.88 to 1.20, three trials, 4081 women (Rumbold 2006;
Spinnato 2007; Villar 2009)).
For the infant
We found no significant difference in the risk of stillbirth be-
tween women receiving vitamin C and vitamin E compared with
placebo (RR 0.89, 95% CI 0.46 to 1.73, three trials, 2899 women
(Chappell 1999; Rumbold 2006; Spinnato 2007)) or vitamin C
compared with placebo (RR 3.00, 95% CI 0.12 to 72.77, one trial,
200 women (Steyn 2003)). There was no significant difference
between women receiving any combination of vitamin C supple-
mentation compared with control for other primary outcomes in-
cluding perinatal death, neonatal death, very preterm birth (less
than 34 weeks), small-for-gestational-age infants, birthweight and
congenital malformations.
Women supplemented with vitamin C compared with placebo
were at increased risk of having a preterm birth (RR 1.43, 95% CI
1.03 to 1.99, one trial, 200 women (Steyn 2003)); however, no
increased risk of preterm birth was seen when women were given
vitamin C in addition to vitamin E compared with placebo (RR
0.97, 95% CI 0.85 to 1.10, four trials, 4264 women (Chappell
1999; Rumbold 2006; Spinnato 2007; Villar 2009)).
Secondary outcomes
There was no significant difference between women receiving any
combination of vitamin C supplementation compared with con-
trol for the secondary outcomes: Apgar score less than seven at five
minutes, maternal hospitalisation or admission to the neonatal
intensive care unit. There was no significant difference between
women given vitamin C and vitamin E compared with placebo for
adverse effects sufficient to stop supplementation (RR 1.16, 95%
CI 0.39 to 3.41, one trial, 739 women (Spinnato 2007)); however,
women given vitamin C and vitamin E were more likely to report
abdominal pain compared with women given a placebo (RR 1.63,
95% CI 1.12 to 2.36, one trial, 1734 women (Rumbold 2006)).
Vitamin A supplementation
The trials involving vitamin A supplementation included the
following interventions: vitamin A and/or beta-carotene versus
placebo (Katz 2000), vitamin A with or without multivitamins ver-
sus multivitamins (excluding vitamin A) or placebo (Fawzi 1998)
and vitamin A plus iron and folic acid versus iron and folic acid
(Kumwenda 2002; Schmidt 2001; Van den Broek 2006).
Primary outcomes
19Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

For the woman
We found no difference in total fetal loss between women given
vitamin A compared with placebo (relative risk 1.04, 95% CI
0.92 to 1.17, one trial, 11,723 women (Katz 2000)), beta-carotene
compared with placebo (RR 1.03, 95% CI 0.91 to 1.16, one
trial, 11,303 women (Katz 2000)), vitamin A compared with beta-
carotene (RR 1.01, 95% CI 0.90 to 1.14, one trial, 11,720 women
(Katz 2000)), vitamin A or beta-carotene compared with placebo
(RR 1.05, 95% CI 0.91 to 1.21, one trial, 17,373 women (Katz
2000)), vitamin A with or without multivitamins compared with
multivitamins or placebo (RR 0.80, 95% CI 0.53 to 1.21, one
trial, 1074 women (Fawzi 1998)) or vitamin A with iron and folic
acid compared with iron and folic acid (RR 1.01, 95% CI 0.61
to 1.66, three trials, 1640 women (Kumwenda 2002; Schmidt
2001; Van den Broek 2006)) (Analysis 4.1). Similarly, we found
no differences in the rate of early or late miscarriage.
For the infant
We found no differences in the rate of stillbirth, neonatal death,
preterm birth or very preterm birth between women given any
type of vitamin A, alone or in combination with beta-carotene,
multivitamin or iron and folic acid, compared with controls. In-
fants of women given vitamin A with iron and folic acid compared
with iron and folic acid alone had higher birthweight (MD 90.00
g, 95% CI 2.68 to 177.32, one trial, 594 women (Kumwenda
2002)). However, we found no difference in the number of infants
born small-for-gestational age between women given vitamin A
with or without multivitamins compared with multivitamins or
placebo (RR 0.84, 95% CI 0.58 to 1.21, one trial, 1075 women
(Fawzi 1998)).
Secondary outcomes
The rate of multiple pregnancy was higher in women given either
vitamin A or beta-carotene compared with placebo (relative risk
1.39, 95% CI 1.05 to 1.84, one trial, 15,845 women (Katz 2000)),
and there were trends towards an increase in the rate of multiple
pregnancy for women given vitamin A versus placebo (relative risk
1.35, 95% CI 0.99 to 1.85, one trial, 10,697 women (Katz 2000))
or beta-carotene versus placebo (relative risk 1.37, 95% CI 1.00
to 1.88, one trial, 10,294 women (Katz 2000)). Fewer infants of
women given vitamin A and iron and folic acid compared with
iron and folic acid alone had anaemia at six weeks of age (RR 0.58,
95% CI 0.45 to 0.75, one trial, 562 infants (Kumwenda 2002));
however, at 12 months, no difference was seen (RR 1.03, 95% CI
0.88 to 1.20, one trial, 478 infants (Kumwenda 2002)). Similarly
there was no difference in infant anaemia amongst women given
other combinations of vitamin A during pregnancy, and no differ-
ences in the rate of maternal anaemia for women given any com-
bination of vitamin A in pregnancy. At six weeks of age, infants
of women given vitamin A and iron and folic acid compared with
iron and folic acid alone had greater weight (MD 169 g, 95% CI
16.55 to 321.45, one trial, 546 infants (Kumwenda 2002)) and
length (MD 0.70 cm, 95% CI 0.15 to 1.25, one trial, 546 infants
(Kumwenda 2002)); however, at four months of age we found no
significant difference in weight (MD -100.00 g, 95% CI -377.14
to 177.14, one trial, 148 infants (Schmidt 2001)) or length (MD
-0.50 cm, 95% CI -1.33 to 0.33, one trial, 148 infants (Schmidt
2001)).
Multivitamin supplementation
The trials involving multivitamin supplementation included the
following interventions: multivitamins with or without folic acid
versus no multivitamins or folic acid (Czeizel 1994; MRC 1991);
multivitamins with or without folic acid versus folic acid (Kirke
1992; MRC 1991); multivitamins with or without vitamin A ver-
sus vitamin A or placebo (Fawzi 1998); multivitamins versus con-
trol (People’s League 1942); multivitamins with vitamin E versus
multivitamins without vitamin E or control (Rush 1980); multi-
vitamins with iron and folic acid versus iron and folic acid (Fawzi
2007; Osrin 2005; Roberfroid 2008; Rumiris 2006; The Summit
2008) and multivitamins with folic acid, iron, zinc and vitamin
A versus no multivitamin and folic acid, iron, zinc, vitamin A
(Christian 2003).
Primary outcomes
For the woman
We found moderate heterogeneity in the subgroup analyses of
total fetal loss, early or late miscarriage and stillbirth amongst
women given multivitamins in various combinations with iron
and folic acid. This heterogeneity may be explained by differences
in study populations, for example the inclusion of Rumiris 2006,
which included women with low antioxidant status at entry and
ICMR 2000, which included women who had previously given
birth to a child with an open neural tube defect. Total fetal loss
was significantly lower in women who were given multivitamins
with or without vitamin A compared with those receiving vitamin
A or placebo (RR 0.60, 95% CI 0.39 to 0.91, one trial, 1074
women (Fawzi 1998)), using a random-effects analysis (Analysis
5.1). However, given that these findings occurred in subgroup
analyses and they include studies where the comparison groups
contain either women receiving either vitamin A or placebo, cau-
tion should be taken in interpretation. Using random-effects anal-
yses, we found no other differences in total fetal loss for women
receiving multivitamins with folic acid versus no multivitamins
or folic acid (RR 1.00, 95% CI 0.75 to 1.34, three trials, 6883
women, Tau2 0.03 (Czeizel 1994; ICMR 2000; MRC 1991));
multivitamins without folic acid versus no multivitamins or folic
acid (RR 0.83, 95% CI 0.56 to 1.25, one trial, 907 women (MRC
20Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1991)); multivitamins with or without folic acid versus no multi-
vitamins or folic acid (RR 0.91, 95% CI 0.65 to 1.27, one trial,
1368 women (MRC 1991)); multivitamins with folic acid ver-
sus folic acid (RR 1.03, 95% CI 0.72 to 1.48, two trials, 1096
women (Kirke 1992; MRC 1991)); multivitamins without folic
acid versus folic acid (RR 0.90, 95% CI 0.62 to 1.30, two trials,
1090 women (Kirke 1992; MRC 1991)); multivitamins with or
without folic acid versus folic acid (RR 0.95, 95% CI 0.69 to 1.30,
two trials, 1644 women (Kirke 1992; MRC 1991)); multivitamins
versus control (RR 0.83, 95% CI 0.58 to 1.17, one trial, 5021
women (People’s League 1942)); multivitamins with vitamin E
versus multivitamins without vitamin E or control (RR 0.92, 95%
CI 0.46 to 1.83, one trial, 823 women (Rush 1980)) and women
given multivitamins with iron and folic acid versus iron and folic
acid (RR 0.90, 95% CI 0.75 to 1.09, five trials, 42,404 women,
Tau2 0.02 (Fawzi 2007; Osrin 2005; Roberfroid 2008; Rumiris
2006; The Summit 2008)). Using random-effects models, there
was no clear difference in the risk of early or late miscarriage be-
tween women supplemented with multivitamins compared with
control, for any of the multivitamin comparisons (Analysis 5.2).
For the other primary outcomes, women receiving multivitamins
compared with control were at lower risk of pre-eclampsia (RR
0.70, 95% CI 0.55 to 0.90, one trial, 5021 women (People’s
League 1942)), and there was a trend to a reduced risk of pre-
eclampsia amongst women receiving multivitamins with iron and
folic acid compared with iron and folic acid (RR 0.24, 95% CI
0.06 to 1.01, one trial, 60 women, (Rumiris 2006)), which was of
borderline statistical significance (P = 0.05).
For the infant
There was no clear difference in the risk of stillbirth for any of the
multivitamin comparisons using random-effects models (Analysis
5.5). Infants of women given multivitamins with iron and folic
acid compared with iron and folic acid had a higher birthweight
(MD 61.61 grams, 95% CI 37.32 to 85.91, three trials, 10241
infants (Fawzi 2007; Osrin 2005; Roberfroid 2008)). There were
no clear differences demonstrated in the risk of neonatal death,
infant death, preterm birth, congenital malformations.
Heterogeneity
In addition to total fetal loss, early or late miscarriage and stillbirth
(all discussed above), we also identified substantial heterogeneity
for perinatal death and small-for-gestational age in the compar-
isons of women given multivitamins with iron and folic acid com-
pared with iron and folic acid alone. The source of this heterogene-
ity is unclear; it may be due to different characteristics of women
in these studies. Using a random-effects model, there were no clear
differences in the risks of perinatal death or small-for-gestational
age between any of the multivitamin combinations compared with
controls, with the exception of women given multivitamins with
folic acid, iron, zinc and vitamin A. In this group there was a trend
towards a reduction in the number of infants with a birthweight
less than 2500 g amongst women given multivitamins with folic
acid, iron, zinc and vitamin A versus no multivitamin and folic
acid, iron, zinc, vitamin A (relative risk 0.95 95% CI 0.90 to 1.00,
one trial, 3325 infants (Christian 2003)).
Secondary outcomes
There was no clear difference in the risk of maternal anaemia or
in the number of women breastfeeding, for any of the multivi-
tamin comparisons. Women given multivitamins with folic acid
compared with no multivitamins or folic acid were more likely to
have a multiple pregnancy (RR 1.36, 95% CI 1.00 to 1.85, two
trials, 5141 women (Czeizel 1994b; ICMR 2000)), although this
result was of borderline statistical significance (P = 0.05). Women
given multivitamins with iron and folic acid had a reduced risk of
anaemia compared with women given iron and folic acid alone (RR
0.88, 95% CI 0.81 to 0.96, two trials, 2278 women (Fawzi 2007;
Osrin 2005)). During childhood follow-up, children of women
given multivitamins with folic acid, iron, zinc and vitamin A versus
no multivitamin and folic acid, iron, zinc, vitamin A were more
likely to be stunted at six to eight years of age (relative risk 1.09,
95% CI 1.00 to 1.19, one trial, 3356 children (Christian 2003)),
although this result was of borderline statistical significance (P =
0.05).
Folic acid supplementation
The trials involving folic acid supplementation included the fol-
lowing interventions: folic acid with or without multivitamins
compared with no folic acid or multivitamins (Czeizel 1994;
ICMR 2000; MRC 1991); folic acid with or without multivi-
tamins compared with multivitamins (Kirke 1992; MRC 1991);
folic acid with iron, zinc, multivitamins and vitamin A compared
with vitamin A alone (Christian 2003); folic acid and iron com-
pared with iron (Fleming 1968); folic acid and iron compared
with no iron or folic acid (Fleming 1986) and folic acid compared
with placebo (Correia 1982).
Primary outcomes
For the woman
We found no significant difference in the risk of total fetal loss
between women receiving folic acid with multivitamins compared
with no folic acid or multivitamins (RR 1.09, 95% CI 0.95 to
1.25, three trials, 6883 women (Czeizel 1994; ICMR 2000; MRC
1991)); folic acid without multivitamins compared with no folic
acid or multivitamins (RR 0.95, 95% CI 0.64 to 1.40, one trial,
903 women (MRC 1991)); folic acid with or without multivi-
tamins compared with no folic acid or multivitamins (RR 0.97,
21Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

95% CI 0.69 to 1.35, one trial, 1364 women (MRC 1991)); folic
acid with multivitamins compared with multivitamins (RR 1.15,
95% CI 0.80 to 1.67, two trials, 1102 women (Kirke 1992; MRC
1991)); folic acid without multivitamins compared with multivi-
tamins (RR 1.12, 95% CI 0.77 to 1.62, two trials, 1090 women
(Kirke 1992; MRC 1991)); folic acid with or without multivita-
mins compared with multivitamins (RR 1.14, 95% CI 0.82 to
1.57, two trials, 1644 women (Kirke 1992; MRC 1991)); folic
acid with iron compared with iron (RR 0.23, 95% CI 0.01 to
4.59, one trial, 75 women (Fleming 1968)) and folic acid and
iron compared no iron or folic acid (RR 13.00, 95% CI 0.74 to
226.98, one trial, 160 women (Fleming 1986)) (Analysis 6.1).
For the other primary outcomes, we found no differences in the
risk of pre-eclampsia between women given folic acid, alone or
with multivitamins or iron, compared with controls.
Heterogeneity
We identified significant heterogeneity in the subgroup analyses
of early or late miscarriage comparing folic acid and multivitamins
versus no folic acid or multivitamins (Tau2 0.04). This is likely to
be due to the inclusion of ICMR 2000, which included women
who had previously given birth to a child with an open neural tube
defect and was at increased risk of bias due to incomplete outcome
data for all participants. There was no clear difference in the risk of
early or late miscarriage between women given folic acid compared
with control, for any of the folic acid combinations (Analysis
6.2). Excluding the ICMR study from the analysis reduced the
heterogeneity, and did not change the overall direction of effects.
For the infant
We found no differences in the risk of stillbirth, perinatal death,
neonatal death, preterm birth, small-for-gestational-age infants
(birthweight less than 10th centile), congenital malformations or
infant death between women given folic acid, alone or with mul-
tivitamins or iron, compared with controls. Women given folic
acid compared with placebo had a greater placental weight (MD
96 g, 95% CI 30.73 to 161.27, one trial, 29 women (Correia
1982)), their infants had greater birthweight (MD 312 g, 95% CI
108.52 to 515.48, one trial, 29 women (Correia 1982)); however,
we found no difference in birthweight between women given folic
acid and multivitamins compared with no folic acid or multivita-
mins (MD 3.00 g, 95% CI -24.15 to 30.15, one trial, 4862 women
(Czeizel 1994)). Women receiving folic acid with iron, zinc, mul-
tivitamins and vitamin A compared with vitamin A alone were less
likely to have an infant with a birthweight less than 2500 g (relative
risk 0.94, 95% CI 0.90 to 0.99, one trial, 3325 women (Christian
2003)); however, we found no differences in birthweight less than
2500 g for women receiving any of the other folic acid compar-
isons.
Secondary outcomes
Women receiving folic acid and multivitamins compared with no
folic acid or multivitamins were more likely to have a multiple
pregnancy (RR 1.36, 95% CI 1.00 to 1.85, two trials, 5141 women
(Czeizel 1994b; ICMR 2000)). Fewer women given folic acid with
iron, zinc, multivitamins and vitamin A compared with vitamin
A alone had anaemia in the third trimester (relative risk 0.83,
95% CI 0.77 to 0.91, one trial, 813 women (Christian 2003));
however, there were no differences seen for any of the other folic
acid comparisons for maternal anaemia overall and severe maternal
anaemia. During childhood follow-up, children of women given
folic acid, iron, zinc, vitamin A compared with multivitamins and
vitamin A were less likely to be stunted at six to eight years of age
(relative risk 0.93, 95% CI 0.86, 1.00, one trial, 3356 children
(Christian 2003)).
Subgroup analyses by women’s risk of spontaneous or
recurrent miscarriage
Information enabling women to be classified at high or low risk of
either spontaneous miscarriage or recurrent miscarriage was not
clearly stated in any of the trials. Based on the inclusion criteria,
one trial (Rumbold 2006) included women at low risk of mis-
carriage. One trial (Briscoe 1959) included women who had ex-
perienced recurrent miscarriage as well as women at high risk of
miscarriage (more than two previous miscarriages and/or bleed-
ing in the pregnancy) and low-risk women (two or less previous
miscarriages and no bleeding in the pregnancy). After classifying
women into these groups, the number of women in the high-risk
group was too small to permit any meaningful comparisons and
we have therefore not performed subgroup analyses.
Subgroup analyses by dose of vitamins and duration
of vitamin usage
Subgroup analyses by dose of vitamin(s) (below or above the rec-
ommended dietary intake) were complicated by the limited num-
ber of studies in each vitamin group, and by the use of multivi-
tamin supplements. For many of the vitamin types and for those
reporting pregnancy loss outcomes, all of the trials supplemented
women with amounts that were above the recommended dietary
intake. Similarly, the duration of vitamin usage was complicated
by the fact that many of the trials had wide recruitment periods,
and one trial (Katz 2000) supplemented women up until three
years postpartum. Nevertheless, subgroups based on time of trial
entry are covered in the main analyses for any vitamins (Analysis
1.1). We have not performed subgroup analyses based on vitamin
dosage.
Subgroup analyses by dietary intake of vitamins
Five trials (Fleming 1968; Kumwenda 2002; People’s League 1942;
Schmidt 2001; Steyn 2003) reported information about women’s
22Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

nutritional status or the percentage of women that were dietary
deficient at trial entry for the vitamin of interest. Other trials re-
ported that they were being undertaken in countries where the
population was at high risk of multiple micronutrient deficiencies
(Osrin 2005; Roberfroid 2008; The Summit 2008; Villar 2009)
or anaemia (Fleming 1986), but provided no specific informa-
tion on nutritional status of participants. Another trial (Rumiris
2006) included women with ’low antioxidant status’. There were
not enough trials within each vitamin group to assess the role of
supplementation in women with dietary deficient intakes of the
individual vitamins and results were not reported separately for
women with a low dietary vitamin intake; therefore, we could not
perform subgroup analyses.
23Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
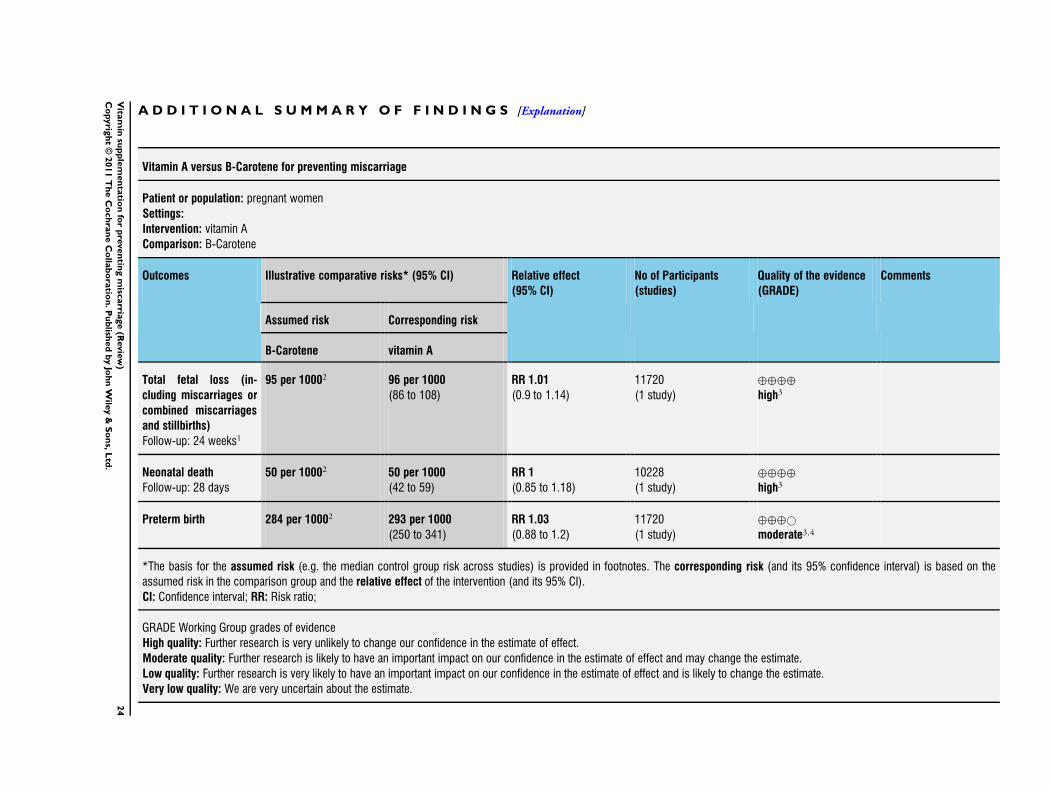
A D D I T I O N A L S U M M A R Y O F F I N D I N G S [Explanation]
Vitamin A versus B-Carotene for preventing miscarriage
Patient or population: pregnant women
Settings:
Intervention: vitamin A
Comparison: B-Carotene
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
B-Carotene vitamin A
Total fetal loss (in-
cluding miscarriages or
combined miscarriages
and stillbirths)
Follow-up: 24 weeks1
95 per 10002 96 per 1000
(86 to 108)
RR 1.01
(0.9 to 1.14)
11720
(1 study)
⊕⊕⊕⊕
high3
Neonatal death
Follow-up: 28 days
50 per 10002 50 per 1000
(42 to 59)
RR 1
(0.85 to 1.18)
10228
(1 study)
⊕⊕⊕⊕
high3
Preterm birth 284 per 10002 293 per 1000
(250 to 341)
RR 1.03
(0.88 to 1.2)
11720
(1 study)
⊕⊕⊕©
moderate3,4
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
24
Vita
min
sup
ple
men
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

1 Follow-up up to 24 weeks post birth.2 Control group risk extracted from the original trial reference.3 Only one study for this outcome; therefore no point deducted for inconsistency between studies.4 Gestational age may have been underestimated, because women may have mistaken vaginal bleeding early in pregnancy for menses.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
25
Vita
min
sup
ple
men
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Vitamin A plus iron plus folate versus iron plus folate for preventing miscarriage
Patient or population: pregnant women
Settings:
Intervention: vitamin A plus iron plus folate
Comparison: iron plus folate
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
iron plus folate vitamin A plus iron plus
folate
Total fetal loss (in-
cluding miscarriages or
combined miscarriages
and stillbirths)
Low risk population RR 1.01
(0.61 to 1.66)
1640
(3 studies)
⊕©©©
very low2,3,4,5
25 per 10001 25 per 1000
(15 to 41)
Medium risk population
31 per 10001 31 per 1000
(19 to 51)
High risk population
52 per 10001 52 per 1000
(32 to 86)
Stillbirth Study population RR 1.29
(0.57 to 2.91)
1640
(3 studies)
⊕©©©
very low2,3,4,5
14 per 1000 18 per 1000
(8 to 41)
Medium risk population
26
Vita
min
sup
ple
men
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

17 per 1000 22 per 1000
(10 to 49)
Preterm birth 56 per 10001 62 per 1000
(33 to 117)
RR 1.11
(0.59 to 2.09)
700
(1 study)
⊕⊕©©
low4,5,6
Birthweight
(grams)
The mean birthweight in
the control groups was
2,805
The mean Birthweight in
the intervention groups
was
90 higher
(2.68 to 177.32 higher)
594
(1 study)
⊕⊕©©
low3,6
Maternal anaemia Study population RR 0.96
(0.82 to 1.12)
700
(1 study)
⊕⊕⊕©
moderate4,6
513 per 1000 492 per 1000
(421 to 575)
Medium risk population
513 per 1000 492 per 1000
(421 to 575)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: Confidence interval; RR: Risk ratio;
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Control group risk extracted from the original trial reference(s).2 One study had incomplete data (of 243 pregnant women initially enrolled, 182 attended the postpartum examination; reasons for all
dropouts not reported); however, this study contributed less than 30% of the weight to this analysis, and a point has not been deducted.3 One study included only women with HIV.4 One study included only women with anaemia.2
7V
itam
insu
pp
lem
en
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

5 Wide 95% CIs.6 Only one study for this outcome; therefore no point deducted for inconsistency between studies.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
28
Vita
min
sup
ple
men
tatio
nfo
rp
reven
ting
misc
arria
ge
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

D I S C U S S I O N
We did not find any evidence to support the use of any vitamins
for preventing either early or late miscarriage or stillbirth. Women
given multivitamins with or without vitamin A compared with
those receiving vitamin A alone or placebo and women given mul-
tivitamins with iron and folic acid compared with those receiv-
ing iron and folic acid alone were at lower risk of ’total fetal loss’.
However, there should be caution interpreting these findings, as
they occurred in additional analyses by type of vitamin; the control
group involved either vitamin A supplementation, iron and folic
acid supplementation or placebo; and findings were no longer sig-
nificant when total fetal loss was examined separately as miscar-
riage or stillbirth.
Women given any vitamins alone or in combination with other
vitamins during the pre- or peri-conceptional period were more
likely to have a multiple pregnancy. These differences persisted in
the additional analyses by type of vitamin, whereby vitamin A,
multivitamins and folic acid were found to be associated with an
increase in multiple pregnancy. These findings are in agreement
with the Cochrane review ’Periconceptional supplementation with
folic acid and/or multivitamins for preventing neural tube defects’
(Lumley 2001b), as well as a re-analysis of individual trial data
(Czeizel 1994b) and several other large cohort studies on the rate
of twinning amongst users of multivitamins and folic acid (Ericson
2001), and after food fortification with folic acid (Waller 2003).
The potential mechanisms of action behind the vitamins and their
impact on multiple pregnancy are not well understood, although
there is some speculation that the vitamins may influence the rate
of twinning rather than improving the survival of multiple fetuses
(Katz 2001). An increase in multiple pregnancy along with in-
creases in perinatal morbidity and mortality is of concern; how-
ever, as direct causality is yet to be established, further monitor-
ing of pre- and peri-conceptional vitamin supplementation is re-
quired. Furthermore, although seven trials in this review enrolled
women prior to conception, only three of these trials reported on
multiple pregnancy, so there is also potential for bias due to selec-
tive reporting of multiple pregnancy.
We detected significant heterogeneity for pre-eclampsia and birth-
weight in the comparisons of ’any vitamin versus no or minimal
vitamins’. This heterogeneity appears to be due to: (a) the inclu-
sion of two studies at high risk of bias due to quasi-random alloca-
tion and large losses to follow-up (Correia 1982; People’s League
1942); and (b) combining all trials regardless of vitamin type in
the analyses. When we conducted subgroup analyses by individ-
ual vitamin type, heterogeneity was no longer apparent for birth-
weight, with the exception of sub-analyses of folic acid supple-
mentation where data were contributed by one trial at high risk
of bias (Correia 1982).
In the analyses by vitamin type, supplementing women with vita-
min A, iron and folic acid or multivitamins combined with miner-
als and folic acid was associated with a significant increase in infant
birthweight, and for multivitamins, a reduced risk of low birth-
weight babies, and maternal anaemia. These findings are consistent
with the Cochrane review ’Multiple-micronutrient supplementa-
tion for women during pregnancy’ (Haider 2006), which found a
decrease in the number of low birthweight babies, small-for-gesta-
tional-age babies and in maternal anaemia amongst women sup-
plemented with multiple micronutrients compared with two or
fewer micronutrients or control. However, as the beneficial effects
seen for maternal anaemia and infant growth measures were not
consistent across all multivitamin combinations, further research
is required to confirm the effects of multivitamins on maternal
and infant health outcomes. Small improvements in infant growth
were also seen with vitamin A and folic acid supplementation.
However, these findings should be interpreted with caution, as in
many instances the data are contributed from single trials.
Vitamin C supplementation was associated with a small increase in
the risk of preterm birth. One trial, involving 200 women at high
risk of giving birth preterm, contributed data for this outcome.
The authors of this trial concluded that the increase in preterm
birth in the vitamin group did not translate into poorer neonatal
outcomes (Steyn 2003). Further studies are required before any
recommendations can be made regarding vitamin C supplemen-
tation. Women supplemented with multivitamins had a reduced
risk of pre-eclampsia. However this finding should be interpreted
with caution as the data come from one quasi-randomised trial
(People’s League 1942). The role of vitamins in the prevention of
pre-eclampsia is explored in the Cochrane review ’Antioxidants
for preventing pre-eclampsia’ (Rumbold 2008).
Our review included trials that randomised women prior to con-
ception; however, in some cases, not all women enrolled in these
trials fell pregnant during the study period. Some of the trials re-
ported outcomes only for women falling pregnant, whereas other
trials did not distinguish between women that were never pregnant
and women that may have been pregnant but were lost to follow-
up. The outcomes in this review relating to pregnancy complica-
tions are not relevant for the women that never became pregnant
during the study period. In this review, where trials provided ac-
curate information about the number of women who joined the
study and became pregnant in the time period, we included this
number in the totals, rather than the number of women that may
have been randomised. Where it was not clear about the exact
number of women with a confirmed pregnancy, we included all
women that had been randomised. This may therefore mean that
women in the denominator were never pregnant during the study
period. By including these women who were never pregnant in
the totals, the review assumes that if these women had become
pregnant, they would not have had a miscarriage, which is unlikely
to be entirely correct. Including these women creates the potential
to underestimate any treatment effects observed.
Similarly, for one large trial (Katz 2000) and one smaller trial
(Roberfroid 2008), some women were pregnant more than once
29Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

during the study period. In these trials, the denominators reported
are the total number of pregnancies during the study period, not
the total number of women randomised, which incorrectly as-
sumes that each data point included is independent from the next.
This has the potential to either underestimate or overestimate the
results, depending on whether the women contributing data for
more than one pregnancy may be more or less susceptible to expe-
riencing miscarriage or stillbirth. One way to overcome this may
be to summarise the data for each woman so that there is only one
set of data points for each woman; however, we were unable to do
this for these particular studies.
Many of the trials included in the review were not of high quality,
either due to poor or unclear allocation concealment or large losses
to follow-up, which increases the risk of bias in the results. The
data were also complicated by differing definitions of miscarriage.
For some trials, miscarriage was considered to occur up until 26
or 28 weeks’ gestation, while other studies reported miscarriage
as pregnancy loss prior to 20 weeks’ gestation, and stillbirth as
pregnancy loss greater or equal to 20 weeks’ gestation. Other stud-
ies did not specify their definition of miscarriage or stillbirth. In
addition to the problems with differing definitions, the timing of
the onset of vitamin supplementation for some of the included
trials occurred in mid-pregnancy, which may limit the impact of
supplementation on the risk of miscarriage. The review attempted
to overcome these issues by using the outcome ’total fetal loss’,
which included either miscarriage or stillbirth.
In order to determine the effect of publication bias, we undertook
funnel plots for comparisons with 10 or more studies. Overall, in
the comparisons of any vitamins versus no vitamins, the funnel
plots were symmetrical, suggesting a low possibility of publication
bias. The graphs for the analysis of multivitamins were less sym-
metrical, indicating the possibility that smaller negative trials may
be missing. However it is also possible that this asymmetry is due
to differences in maternal characteristics between trials.
Women given any vitamins were also more likely to self-report
abdominal pain in late pregnancy, although this outcome was only
reported by one trial assessing vitamin C and E supplementation (
Rumbold 2006). Few studies recorded or reported any information
about side effects of vitamin supplementation. We are unaware of
any other studies reporting an association between vitamins and
abdominal pain; nevertheless, these findings highlight the need to
assess potential side effects and adverse effects in trials.
No trials reported on any potential psychological effects such as
anxiety and depression, for women experiencing miscarriage or
stillbirth.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Any vitamins do not help prevent either early or late miscarriage
or stillbirth. Supplementing women with vitamin A or multivita-
mins, with or without folic acid, may increase the risk of having a
multiple birth, which may confer increases in perinatal morbidity
and mortality. There is insufficient evidence to examine the effect
of different combinations of vitamins on miscarriage, stillbirth and
measures of infant growth.
Implications for research
The impact of different combinations of vitamins (i.e. multivita-
min preparations with or without vitamin A and folic acid) on
miscarriage, stillbirth, birthweight and measures of infant growth
is unclear. Any future studies of vitamin supplementation should
be high quality and focus on women at high risk of miscarriage,
assess the most appropriate vitamin type and dosage, show it is
beneficial without causing any harms to the mother or fetus and
include assessments of any psychological effects and long-term fol-
low-up of mothers and infants.
A C K N O W L E D G E M E N T S
We thank Simon Gates for statistical advice regarding inclusion
of cluster randomised trials, Lelia Duley for helpful comments on
the format of the review and Sonja Henderson for assisting with
review administration.
30Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Briscoe 1959 {published data only}
Briscoe CC. The role of vitamin C-hesperidin in the
prevention of abortion. Obstetrics & Gynecology 1959;14
(3):288–90.
Chappell 1999 {published data only}
Chappell LC, Seed PT, Briely AL, Kelly FJ, Lee R, Hunt
BJ, et al.Effect of antioxidants on the occurrence of pre-
eclampsia in women at increased risk: a randomised trial.
Lancet 1999;354:810–6.
Christian 2003 {published data only}
Christian P, Khatry SK, Katz J, Pradhan EK, LeClerq
SC, Shrestha SR, et al.Effects of alternative maternal
micronutrient supplements on low birth weight in rural
Nepal: double blind randomised community trial. BMJ
2003;326(7389):571.
Christian P, Shrestha J, LeClerq S, Khatry SK, Jiang T,
Wagner T, et al.Supplementation with micronutrients in
addition to iron and folic acid does not further improve
the hematologic status of pregnant women in rural Nepal.
Journal of Nutrition 2003;133:3492–8.
Christian P, Stewart CP, LeClerq SC, Wu L, Katz J, West KP
Jr, et al.Antenatal and postnatal iron supplementation and
childhood mortality in rural Nepal: a prospective follow-
up in a randomized, controlled community trial. American
Journal of Epidemiology 2009;170(9):1127–36.∗ Christian P, West Jr KP, Khatry SK, Leclerq SC,
Pradhan EK, Katz J, et al.Effects of maternal micronutrient
supplementation on fetal loss and infant mortality. American
Journal of Clinical Nutrition 2003;78:1194–202.
Kulkarni B, Christian P, LeClerq SC, Khatry SK.
Determinants of compliance to antenatal micronutrient
supplementation and women’s perceptions of supplement
use in rural Nepal. Public Health Nutrition 2010;13(1):
82–90.
Stewart CP, Christian P, LeClerq SC, West KP Jr, Khatry
SK. Antenatal supplementation with folic acid + iron + zinc
improves linear growth and reduces peripheral adiposity
in school-age children in rural Nepal. American Journal of
Clinical Nutrition 2009;90(1):132–40.
Correia 1982 {published data only}
Correia JM, Silva Cruz A, Silva Meirinho M. The
importance of the contribution of folic acid in gestation
[Importancia del aporte de acido folico en las gestacion].
Progresos de Obstetricia y Ginecologia 1982;25(6):381–6.
Czeizel 1994 {published data only}
Czeizel A, Rode K. Trial to prevent first occurrence of
neural tube defects by periconceptional multivitamin
supplementation [letter]. Lancet 1984;2:40.
Czeizel AE. Controlled studies of multivitamin
supplementation on pregnancy outcomes. Annals of the
New York Academy of Science 1993;678:266–75.
Czeizel AE. Controlled studies of multivitamin
supplementation on pregnancy outcomes. Annals of the
New York Academy of Sciences 1993;678:266–75.
Czeizel AE. Limb reduction defects and folic acid
supplementation [letter]. Lancet 1995;345:932.
Czeizel AE. Nutritional supplementation and prevention of
congenital abnormalities. Current Opinion in Obstetrics andGynecology 1995;7:88–94.
Czeizel AE. Prevention of congenital abnormalities by
periconceptional multivitamin supplementation. BMJ
1993;306:1645–8.
Czeizel AE, Dudás I. Prevention of the first occurrence
of anencephaly and spina bifida with periconceptional
multivitamin supplementation (conclusion). Orvosi Hetilap
1994;135:2313–7.
Czeizel AE, Dudás I. Prevention of the first occurrence
of neural tube defects by periconceptional vitamin
supplementation. New England Journal of Medicine 1992;
327:1832–5.
Czeizel AE, Dudás I, Frotz G, Técsöi, Hanck A, Kunovits
G. The effect of periconceptional multivitamin-mineral
supplementation on vertigo, nausea and vomiting in the
first trimester of pregnancy. Archives of Gynecology andObstetrics 1992;251:181–5.∗ Czeizel AE, Dudás I, Metneki J. Pregnancy outcomes
in a randomised controlled trial of periconceptional
multivitamin supplementation. Final report. Archives ofGynecology and Obstetrics 1994;255:131–9.
Czeizel AE, Fritz G. Randomized trial of periconceptional
vitamins [letter]. JAMA 1989;262:1634.
Czeizel AE, Métneki J, Dudás I. Higher rate of multiple
births after periconceptional vitamin supplementation
[letter]. New England Journal of Medicine 1994;330:
1687–8.
Czeizel AE, Métneki J, Dudás I. The higher rate of multiple
births after periconceptional multivitamin supplementation:
an analysis of causes. Acta Geneticae Medicae et Gemellologiae
(Roma) 1994;43:175–84.
Czeizel AE, Rockenbauer M, Susansky E. No change
in sexual activity during preconceptional multivitamin
supplementation. British Journal of Obstetrics and
Gynaecology 1996;103:569–73.
Czeizel AE, Rockenbauer M, Susánsky E. No change
in sexual activity during preconceptional multivitamin
supplementation. British Journal of Obstetrics & Gynaecology
1996;103:569–73.
Dudás I, Rockenbauer M, Czeizel AE. The effect of
preconceptional multivitamin supplementation on the
menstrual cycle. Archives of Gynecology and Obstetrics 1995;
256:115–23.
Eros E, Geher P, Gomor B, Czeizel AE. Epileptogenic
activity of folic acid after drug induces SLE (folic acid and
epilepsy). European Journal of Obstetrics & Gynecology and
Reproductive Biology 1998;80:75–8.
Métneki J, Dudás I, Czeizel AE. Periconceptional
multivitamin administration may result in higher frequency
of twin pregnancies. Orvosi Hetilap 1996;137:2401–5.
31Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fawzi 1998 {published data only}
Baylin A, Villamor E, Rifai N, Msamanga G, Fawzi
WW. Effect of vitamin supplementation to HIV-infected
pregnant women on the micronutrient status of their
infants. European Journal of Clinical Nutrition 2005;59(8):
960–8.
Fawzi W, Msamanga G, Renjifo B, Spiegelman D, Urassa E,
Hashemi L, et al.Predictors of intrauterine and intrapartum
transmission of HIV-1 among Tanzanian women. AIDS
2001;15(9):1157–65.
Fawzi WW, Msamanga G, Hunter D, Urassa E, Renjifo
B, Mwakagile D, et al.Randomized trial of vitamin
supplements in relation to vertical transmission of HIV-1 in
Tanzania. Journal of Acquired Immune Deficiency Syndromes2000;23(3):246–54.
Fawzi WW, Msamanga GI, Kupka R, Spiegelman D,
Villamor E, Mugusi F, et al.Multivitamin supplementation
improves hematologic status in HIV-infected women and
their children in Tanzania. American Journal of Clinical
Nutrition 2007;85(5):1335–43.∗ Fawzi WW, Msamanga GI, Spielgelman D, Urassa EJN,
McGrath N, Mwakagile D, et al.Randomised trial of effects
of vitamin supplements on pregnancy outcomes and T cell
counts in HIV-1 infected women in Tanzania. Lancet 1998;
351:1477–82.
Villamor E, Msamanga G, Saathoff E, Manji K, Fawzi WW.
Effect of vitamin supplements on the incidence of malaria
among children born to HIV-infected Women. FASEBJournal 2006;20(4 Pt 1):A125.
Fawzi 2007 {published data only}
Fawzi WW, Msamanga GI, Urassa W, Hertzmark E, Petraro
P, Willett WC, et al.Vitamins and perinatal outcomes
among HIV-negative women in Tanzania. New England
Journal of Medicine 2007;356(14):1423–31.
Fleming 1968 {published data only}
Fleming AF, Hendrickse JP, Allan NC. The prevention of
megaloblastic anaemia in pregnancy in Nigeria. Journalof Obstetrics and Gynaecology of the British Commonwealth
1968;75:425–32.
Fleming 1986 {published data only}
Fleming AF, Ghatoura GBS, Harrison KA, Briggs ND,
Dunn DT. The prevention of anaemia in pregnancy in
primigravidae in the guinea savanna of Nigeria. Annals ofTropical Medicine and Parasitology 1986;80:211–33.
Harrison KA, Fleming AF, Briggs ND, Rossiter CE. Growth
during pregnancy in Nigerian teenage primigravidae. British
Journal of Obstetrics and Gynaecology 1985;Suppl 5:32–9.
Hemmi 2003 {published data only}
Hemmi H, Endo T, Kitajima Y, Manase K, Hata H, Kudo
R. Effects of ascorbic acid supplementation on serum
progesterone levels in patients with a luteal phase defects.
Fertility & Sterility 2003;80(2):456–61.
ICMR 2000 {published data only}
ICMR Collaborating Centres and Central Technical
Co-ordinating Unit. Multicentric study of efficacy
of periconceptional folic acid containing vitamin
supplementation in prevention of open neural tube defects
from India. Indian Journal of Medical Research 2000;112:
206–11.
Katz 2000 {published data only}
Christian P, Khatry SK, Yamini S, Stallings R, LeClerq SC,
Shrestha SR, et al.Zinc supplementation might potentiate
the effect of vitamin A in restoring night vision in pregnant
Nepalese women. American Journal of Clinical Nutrition2001;73(6):1045–51.
Christian P, West KP Jr, Khatry SK, Katz J, LeClerq SC,
Kimbrough-Pradhan E, et al.Vitamin A or beta-carotene
supplementation reduces symptoms of illness in pregnant
and lactating Nepali women. Journal of Nutrition 2000;130
(11):2675–82.
Christian P, West KP Jr, Khatry SK, Katz J, Shrestha SR,
Pradhan EK, et al.Night blindness of pregnancy in rural
Nepal--nutritional and health risk. International Journal of
Epidemiology 1998;27(2):231–7.
Christian P, West KP Jr, Khatry SK, Kimbrough-Pradhan
E, LeClerq SC, Shrestha SR, et al.Night blindness
during pregnancy and subsequent mortality among
women in Nepal: effects of vitamin A and beta-carotene
supplementation. American Journal of Epidemiology 2000;
152(6):542–7.∗ Katz J, West Jnr KP, Khatry S, Pradhan EK, LeClerq SC,
Christian P, et al.Maternal low-dose vitamin A or beta-
carotene supplementation has no effect on fetal loss and
early infant mortality: a randomized cluster trial in Nepal.
American Journal of Clinical Nutrition 2000;71:1570–6.
Katz J, West KP Jr, Khatry SK, LeClerq SC, Christian P,
Pradhan EK, et al.Twinning rates and survival of twins in
rural Nepal. International Journal of Epidemiology 2001;30
(4):802–7.
West KP Jr, Katz J, Khatry SK, LeClerq SC, Pradhan EK,
Shrestha SR, et al.Double blind, cluster randomised trial of
low dose supplementation with vitamin A or beta carotene
on mortality related to pregnancy in Nepal. The NNIPS-2
Study Group. BMJ 1999;318:570–5.
Kirke 1992 {published data only}
Kirke PN, Daly LE, Elwood JH for the Irish Vitamin Study
Group. A randomised trial of low dose folic acid to prevent
neural tube defects. Archives of Disease in Childhood 1992;
67:1442–6.
Kumwenda 2002 {published data only}
Kumwenda D, Miotti PG, Taha TE, Broadhead R,
Biggar RJ, Brookes Jackson J, et al.Antenatal vitamin A
supplementation increases birth weight and decreases
anemia among infants born to human immunodeficiency
virus-infected women in Malawi. Clinical Infectious Diseases2002;35:618–74.
MRC 1991 {published data only}
Mathews F, Murphy M, Wald NJ, Hackshaw A. Twinning
and folic acid use. Lancet 1999;353:292–3.∗ MRC Vitamin Study Research Group. Prevention of
neural tube defects: results of the Medical Research Council
vitamin study. Lancet 1991;338:131–7.
32Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Osrin 2005 {published data only}
Osrin D, Vaidya A, Shrestha Y, Baniya RB, Manandhar
DS, Adhikari RK, et al.Effects of antenatal multiple
micronutrient supplementation on birthweight and
gestational duration in Nepal: double-blind, randomised
controlled trial. Lancet 2005;365:955–62.
People’s League 1942 {published data only}
People’s League of Health. Nutrition of expectant and
nursing mothers: interim report. Lancet 1942;2:10–2.∗ People’s League of Health. The nutrition of expectant and
nursing mothers in relation to maternal and infant mortality
and morbidity. Journal of Obstetrics and Gynaecology of theBritish Empire 1946;53:498–509.
Roberfroid 2008 {published data only}
Roberfroid D, Huybregts L, Lanou H, Henry MC,
Meda N, Kolsteren FP, et al.Effect of maternal multiple
micronutrient supplements on cord blood hormones: a
randomized controlled trial. American Journal of Clinical
Nutrition 2010;91(6):1649–58.∗ Roberfroid D, Huybregts L, Lanou H, Henry MC,
Meda N, Menten J, et al.Effects of maternal multiple
micronutrient supplementation on fetal growth: a double-
blind randomized controlled trial in rural Burkina Faso.
American Journal of Clinical Nutrition 2008;88(5):1330–40.
Rumbold 2006 {published data only}
Rumbold AR, Crowther CA, Haslam RR, Dekker GA,
Robinson JS, for the ACTS Study Group. Vitamins C and
E and the risks of preeclampsia and perinatal complications.
New England Journal of Medicine 2006;354(17):1796–806.
Rumiris 2006 {published data only}
Rumiris D, Purwosunu Y, Wibowo N, Farina A,
Sekizawa A. Lower rate of preeclampsia after antioxidant
supplementation in pregnant women with low antioxidant
status. Hypertension in Pregnancy 2006;25(3):241–53.
Rush 1980 {published data only}
Rush D, Kristal A, Navarro C, Chaunhan P, Blanc W,
Naeye R, et al.The effects of dietary supplementation
during pregnancy on placental morphology, pathology and
histomorphometry. American Journal of Clinical Nutrition
1984;39:863–71.∗ Rush D, Stein Z, Susser M. A randomized trial of prenatal
nutritional supplementation in New York City. Pediatrics1980;65(4):683–97.
Schmidt 2001 {published data only}
Muslimatun S, Schmidt MK, Schultink W, West CE,
Hautvast JA, Gross R, et al.Weekly supplementation with
iron and vitamin A during pregnancy increases hemoglobin
concentration but decreases serum ferritin concentration in
Indonesian pregnant women. Journal of Nutrition 2001;
131(1):85–90.
Muslimatun S, Schmidt MK, West CE, Schultink W, Gross
R, Hautvast JG. Determinants of weight and length of
Indonesian neonates. European Journal of Clinical Nutrition
2002;56(10):947–51.
Muslimatun S, Schmidt MK, West CE, Schultink W,
Hautvast JG, Karyadi D. Weekly vitamin A and iron
supplementation during pregnancy increases vitamin
A concentration of breast milk but not iron status in
Indonesian lactating women. Journal of Nutrition 2001;131
(10):2664–9.
Schmidt MK, Muslimatun S, West CE, Schultink W,
Hautvast JG. Randomised double-blind trial of the effect of
vitamin A supplementation of Indonesian pregnant women
on morbidity and growth of their infants during the first
year of life. European Journal of Clinical Nutrition 2002;56:
338–46.∗ Schmidt MK, Muslimatun S, West CE, Schultink W,
Hautvast JG. Vitamin A and iron supplementation of
Indonesian pregnant women benefits vitamin A status of
their infants. British Journal of Nutrition 2001;86:607–15.
Spinnato 2007 {published data only}
Spinnato II JA, Freire S, Silva JL, Cunha Rudge MV,
Martins-Costa S, Koch MA, et al.Antioxidant therapy
to prevent preeclampsia: a randomized controlled trial.
Obstetrics & Gynecology 2007;110(6):1311–8.
Steyn 2003 {published data only}
Schoeman J, Steyn PS, Odendaal HJ, Grove D. Bacterial
vaginosis diagnosed at the first antenatal visit better predicts
preterm labour than diagnosis later in pregnancy. Journal ofObstetrics and Gynaecology 2005;25(8):751–3.∗ Steyn PS, Odendaal HJ, Schoeman J, Stander C, Fanie N,
Grove D. A randomised, double blind placebo-controlled
trial of ascorbic acid supplementation for the prevention of
preterm labour. Journal of Obstetrics and Gynaecology 2003;
23(2):150–5.
Taylor 1982 {published data only}
Taylor DJ, Mallen C, McDougall N, Lind T. Effect of iron
supplementation on serum ferritin levels during and after
pregnancy. British Journal of Obstetrics and Gynaecology1982;89:1011–7.
The Summit 2008 {published data only}
The Supplementation with Multiple Micronutrients
Intervention Trial (SUMMIT) Study Group, Shankar
AH, Jahari AB, Sebayang SK, Aditiawarman, Apriatni
M, et al.Effect of maternal multiple micronutrient
supplementation on fetal loss and infant death in indonesia:
a double-blind cluster-randomised trial. Lancet 2008;371
(9608):215–27.
Van den Broek 2006 {published data only}∗ Van den Broek N. Vitamin A supplementation for
anaemia in pregnancy. Personal communication 1998.
Van den Broek NR, White SA, Flowers C, Cook JD, Letsky
EA, Tanumihardjo SA, et al.Randomised trial of vitamin
A supplementation in pregnant women in rural Malawi
found to be anaemic on screening by HemoCue. BJOG: aninternational journal of obstetrics and gynaecology 2006;113
(5):569–76.
Villar 2009 {published data only}∗ Villar J, Purwar M, Merialdi M, Zavaleta N, Ngoc N,
Anthony J, et al.Effect of vitamin C & E supplementation of
pregnant women at risk of preeclampsia plus low nutritional
33Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

status: the WHO trial. Hypertension in Pregnancy 2008;27
(4):501.
Villar J, Purwar M, Merialdi M, Zavaleta N, Thi Nhu Ngoc
N, Anthony J, et al.World Health Organisation multicentre
randomised trial of supplementation with vitamins C and
E among pregnant women at high risk for pre-eclampsia
in populations of low nutritional status from developing
countries. BJOG: an international journal of obstetrics andgynaecology 2009;116(6):780–8.
References to studies excluded from this review
Baumslag 1970 {published data only}
Baumslag N, Edelstein T, Metz J. Reduction of incidence
of prematurity by folic acid supplementation in pregnancy.
British Medical Journal 1970;1:16–7.
Biswas 1984 {published data only}
Biswas MK, Pernoll MJ, Mabie WC. A placebo-controlled
comparative trial of various prenatal vitamin formulations
in pregnant women. Clinical Therapeutics 1984;6(6):763–7.
Blot 1981 {published data only}
Blot I, Papiernik E, Kaltwasser JP, Werner E, Tchernia G.
Influence of routine administration of folic acid and iron
during pregnancy. Gynecologic and Obstetric Investigation
1981;12:294–304.
Chanarin 1968 {published data only}
Chanarin I, Rothman D, Perry J, Stratfull D. Normal
dietary folate, iron and protein intake, with particular
reference to pregnancy. British Medical Journal 1968;2:
394–7.∗ Chanarin I, Rothman D, Ward A, Perry J. Folate status
and requirement in pregnancy. British Medical Journal1968;2:390–4.
Colman 1974 {published data only}∗ Colman N, Barker M, Green R, Metz J. Prevention
of folate deficiency in pregnancy by food fortification.
American Journal of Clinical Nutrition 1974;27:339–44.
Colman N, Larsen JV, Barker M, Barker A, Green R, Metz
J. Prevention of folate deficiency by food fortification. III.
Effect in pregnant subjects of varying amounts of added
folic acid. American Journal of Clinical Nutrition 1975;28:
465–70.
Coutsoudis 1999 {published data only}
Coutsoudis A, Pillay K, Spooner E, Kuhn L, Coovadia
HM. Randomized trial testing the effect of vitamin A
supplementation on pregnancy outcomes and early mother-
to-child HIV-1 transmission in Durban, South Africa.
South African vitamin A study group. AIDS 1999;13(12):
1517–24.
Dawson 1962 {published data only}
Dawson DW, More JR, Aird DC. Prevention of megalo
blastic anaemia in pregnancy by folic acid. Lancet 1962;2:
1015–8.
Edelstein 1968 {published data only}
Edelstein T, Stevens K, Baumslag N, Metz J. Folic acid
and vitamin B12 supplementation during pregnancy in
a population subsisting on a suboptimal diet. Journal of
Obstetrics and Gynaecology of the British Commonwealth
1968;75(2):133–7.
Ferguson 1955 {published data only}
Ferguson JH. Methionine-vitamin B therapy. Obstetrics &
Gynecology 1955;6(2):221–7.
Feyi-Waboso 2005 {published data only}
Feyi-Waboso PA, Chris A, Nwaogu GC, Archibong EI,
Ejikem EC. The role of parenteral multivitamin preparation
(Eldervit-12) in the prevention of anaemia in pregnancy.
Tropical Journal of Obstetrics and Gynaecology 2005;22(2):
159–63.
Fletcher 1971 {published data only}
Fletcher J, Gurr A, Fellingham FR, Prankerd TAJ, Brant
HA, Menzies DN. The value of folic acid supplements
in pregnancy. Journal of Obstetrics and Gynaecology of the
British Commonwealth 1971;78:781–5.
Giles 1971 {published data only}
Giles PFH, Harcourt AG, Whiteside MG. The effect of
prescribing folic acid during pregnancy on birth weight and
duration of pregnancy, a double blind trial. Medical Journalof Australia 1971;5:17–21.
Hampel 1974 {published data only}
Hampel KP, Roetz R. Influence of a long term substitution
with a folate-iron preparation on serum folate, serum iron
and haematological data during pregnancy: result of a
prospective study. Geburtshilfe und Frauenheilkd 1974;34:
409–17.
Hankin 1966 {published data only}
Hankin ME, Cellier KM. Studies of nutrition in pregnancy
V: ascorbic acid levels of blood and milk in pregnancy and
lactation. Australian and New Zealand Journal of Obstetricsand Gynaecology 1966;6:153–60.
Hibbard 1968 {published data only}∗ Hibbard BM, Hibbard ED. The prophylaxis of folate
deficiency in pregnancy. Acta Obstetricia et Gynecologica
Scandinavica 1969;48:339–48.
Hibbard BM, Hibbard ED. The treatment of folate
deficiency in pregnancy. Acta Obstetricia et GynecologicaScandinavica 1969;48:349–56.
Hunt 1984 {published data only}
Hunt IF, Murphy NJ, Cleaver AE, Faraji B, Swendseid ME,
Coulson AH, et al.Zinc supplementation during pregnancy:
effects on selected blood constituents and on progress and
outcome of pregnancy in low-income women of Mexican
descent. American Journal of Clinical Nutrition 1984;40:
508–21.
Huybregts 2009 {published data only}
Huybregts L, Roberfroid D, Lanou H, Menten J, Meda N,
Van Camp J, et al.Prenatal food supplementation fortified
with multiple micronutrients increases birth length: a
randomized controlled trial in rural Burkina Faso. AmericanJournal of Clinical Nutrition 2009;90(6):1593–600.
Laurence 1981 {published data only}
Laurence KM. Prevention of neural tube defects by
improvement in maternal diet and preconceptional folic
34Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
acid supplementation. Progress in Clincial and Biological
Research 1985;163:383–8.∗ Laurence KM, James N, Miller MH, Tennant GB,
Campbell H. Double-blind randomised controlled trial of
folate treatment before conception to prevent recurrence
of neural-tube defects. British Medical Journal (ClinicalResearch Edition) 1981;282:1509–11.
Lira 1989 {published data only}
Lira P, Barrena N, Foradori A, Gormaz G, Grebe G. Folate
deficiency in pregnancy: effect of supplemental folate
[Deficiencia de folatos en el embarazo: Efecto de una
suplementacion con acido folico]. Sangre 1989;34(1):24–7.
Lumeng 1976 {published data only}
Lumeng L, Cleary RE, Wagner R, Pao-Lo Y, Ting-Kai
L. Adequacy of vitamin B6 supplementation during
pregnancy: a prospective study. American Journal of Clinical
Nutrition 1976;29:1379–83.
Marya 1981 {published data only}
Marya RK, Rathee S, Lata V, Mudgil S. Effects of vitamin
D supplementation in pregnancy. Gynecologic and Obstetric
Investigation 1981;12:155–61.
Meirinho 1987 {published data only}
Meirinho M, Correia JM, Silva Cruz A. Administration
of folic acid during pregnancy and trophoblastic disease
[Administracion de acido folico en la gestacion y actividad
trofoblastica]. Progresos de Obstetricia y Ginecologia 1987;30
(2):87–91.
Metz 1965 {published data only}
Metz J, Festenstein H, Welch P. Effect of folic acid and
vitamin B12 supplementation on tests of folate and vitamin
B12 nutrition in pregnancy. American Journal of Clinical
Nutrition 1965;16:472–9.
Mock 2002 {published data only}
Mock DM, Quirk JG, Mock NI. Marginal biotin deficiency
during normal pregnancy. American Journal of Clinical
Nutrition 2002;75:295–9.
Moldenhauer 2002 {published data only}
Moldenhauer J, Guo S, Liang R, Prada J. Dietary intake
levels of the antioxidants vitamin C and vitamin E are
adequately achieved with standard prenatal vitamin
supplementation in high risk pregnancy groups [abstract].
American Journal of Obstetrics and Gynecology 2002;187(6
Pt 2):S99.
Owen 1966 {published data only}
Owen GM, Nelsen CE, Baker GL, Connor WE, Jacobs JP.
Use of vitamin K1 in pregnancy: effect of serum bilirubin
and plasma prothrombin in the newborn. American Journal
of Obstetrics and Gynecology 1967;39(3):368–73.∗ Owen GM, Nelsen CE, Baker GL, Connor WE, Jacobs
JP. Use of vitamin K1 in pregnancy: effect on bilirubin
metabolism and coagulation mechanism in the newborn.
Pediatrics 1966;68(5):850.
Ross 1985 {published data only}
Ross SM, Nel E, Naeye RL. Differing effects of low and
high bulk maternal dietary supplements during pregnancy.
Early Human Development 1985;10:298–302.
Schuster 1984 {published data only}
Schuster K, Bailey LB, Mahan CS. Effect of maternal
pyridoxine-HCl supplementation on the vitamin B-6 status
of mother and infant and on pregnancy outcomes. Journalof Nutrition 1984;114:977–88.
Semba 2001 {published data only}
Semba RD, Kumwenda N, Taha TE, Mtimavalye L,
Broadhead R, Garrett E, et al.Impact of vitamin A
supplementation on anaemia and plasma erthryopoietin
concentrations in pregnant women: a controlled clinical
trial. European Journal of Haematology 2001;66:389–95.
Shu 2002 {published data only}
Shu J, Miao P, Wang RJ. Clinical observation on effect
of Chinese herbal medicine plus human chorionic
gonadotropin and progesterone in treating anticardiolipin
antibody-positive early recurrent spontaneous abortion.
[Chinese]. Zhongguo Zhong Xi Yi Jie He Za Zhi ZhongguoZhongxiyi Jiehe Zazhi/Chinese Journal of Integrated
Traditional & Western Medicine/Zhongguo Zhong Xi Yi Jie HeXue Hui, Zhongguo Zhong Yi Yan Jiu Yuan Zhu Ban 2002;
22(6):414–6.
Smithells 1981 {published data only}
Smithells RW, Sheppard S, Schorah CJ, Sellar MJ, Nevin
NC, Harris R, et al.Apparent prevention of neural tube
defects by periconceptional vitamin supplementation.
Archives of Disease in Childhood 1981;56:911–8.
Suharno 1993 {published data only}
Suharno D, West CE, Muhilal, Karyadi D, Hautvast JG.
Supplementation with vitamin A and iron for nutritional
anaemia in pregnant women in West Java, Indonesia. Lancet1993;342:1325–8.
Tanumihardjo 2002 {published data only}
Tanumihardjo SA. Vitamin A and iron status are improved
by vitamin A and iron supplementation in pregnant
Indonesian women. Journal of Nutrition 2002;132:
1909–12.
Thauvin 1992 {published data only}
Thauvin E, Fusselier M, Arnaud J, Faure H, Favier
H, Coudray C, et al.Effects of a multivitamin mineral
supplement on zinc and copper status during pregnancy.
Biological Trace Elements Research 1992;32:405–14.
Trigg 1976 {published data only}
Trigg KH, Rendall EJC, Johnson A, Fellingham FR,
Prankerd TAJ. Folate supplements during pregnancy.
Journal of the Royal College of General Practitioners 1976;6:
228–30.
Ulrich 1999 {published data only}
Rolschau J, Kristoffersen K, Ulrich M, Grinsted P,
Schaumburg E, Foged N. The influence of folic acid
supplement on the outcome of pregnancies in the county of
Funen in Denmark. Part I. European Journal of Obstetrics &
Gynecology and Reproductive Biology 1999;87(2):105–10.∗ Ulrich M, Kristoffersen K, Rolschau J, Grinsted P,
Schaumburg E, Foged N. The influence of folic acid
supplement on the outcome of pregnancies in the county
of Funen in Denmark. Part II. Congenital anomalies.
35Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A randomised study. European Journal of Obstetrics &
Gynecology and Reproductive Biology 1999;87(2):111–3.
Ulrich M, Kristoffersen K, Rolschau J, Grinsted P,
Schaumburg E, Foged N. The influence of folic acid
supplement on the outcome of pregnancies in the county
of Funen in Denmark. Part III. Congenital anomalies.
An observational study. European Journal of Obstetrics &
Gynecology and Reproductive Biology 1999;87(2):115–8.
Villamor 2002 {published data only}
Villamor E, Msamanga G, Spielgelman D, Antelman G,
Peterson KE, Hunter DJ, et al.Effect of multivitamin and
vitamin A supplements on weight gain during pregnancy
among HIV-1-infected women. American Journal of
Clinical Nutrition 2002;76:1082–90.
Vutyavanich 1995 {published data only}
Vutyavanich T, Wongtra-ngan S, Ruangsri R. Pyroxidone
for nausea and vomiting of pregnancy: a randomized,
double-blind, placebo controlled trial. American Journal ofObstetrics and Gynecology 1995;173(3):881–4.
References to studies awaiting assessment
Chelchowska 2004 {published data only}
Chelchowska M, Laskowska-Klita T, Kubik P, Leibschang
J. The effect of vitamin-mineral supplementation on the
level of MDA and activity of glutathione peroxidase and
superoxide dismutase in blood of matched maternal-cord
pairs [Wplyw suplementacji witaminowo–mineralnej na
poziom MDA oraz aktywnosc peroksydazy glutationowej i
dysmutazy ponadtlenkowej w krwi kobiet ciezarnych i krwi
pepowinowej ich dzieci]. Przeglad Lekarski 2004;61(7):
760–3.
Frenzel 1956 {published data only}
Frenzel KH, Geissler R. The importance of prophylaxis with
multivitamin preparations during pregnancy, childbirth
and nursing period [Die Bedeutung der Prophylaxe
mit Multivitaminpraparaten wahrend Schwangerschaft,
Wochenbett und Stillperiode]. Die Medizinsche Welt 1956;
7(20):767–9.
Kubik 2004 {published data only}
Kubik P, Kowalska B, Laskowska-Klita T, Chelchowska M,
Leibschang J. Effect of vitamin-mineral supplementation
on the status of some microelements in pregnant
women [Wplyw suplementacji preparatem witaminowo–
mineralnym na status wybranych mikroelementow u kobiet
ciezarnych]. Przeglad Lekarski 2004;61(7):764–8.
References to ongoing studies
Fall 2007 {published data only}
Fall C. Mumbai maternal nutrition project. Current
Controlled Trials (www.controlled-trials.com) (accessed 15
February 2007).
Johns 2004 {published data only}
Johns J. The effect of antioxidant supplementation on
women with threatened miscarriage. Current Controlled
Trials (www.controlled-trials.com/mrct) (accessed 6
September 2005) 2004.
Sezikawa 2007 {published data only}
Sezikawa A. Antioxidant supplementation in pregnant
women with low antioxidant status. ClinicalTrials.gov
(http://clinicaltrials.gov/) (accessed 21 June 2007) 2007.
Additional references
Alderson 2004
Alderson P, Green S, Higgins JPT, editors. Cochrane
Reviewers’ Handbook 4.2.2 [updated December 2003]. In:
The Cochrane Library, Issue 1, 2004. Chichester, UK: John
Wiley & Sons, Ltd.
Beazley 2002
Beazley D, Livingston J, Kao L, Sibai B. Vitamin c and e
supplementation in women at high risk for preeclampsia: a
double-blind placebo controlled trial [abstract]. American
Journal of Obstetrics and Gynecology 2002;187(6 Pt 2):S76.
Bendich 1993
Bendich A, Machlin LJ. The safety of oral intake of vitamin
E: data from clinical studies from 1986-1991. In: Packer
L, Fuchs J editor(s). Vitamin E in health and disease. New
York: Marcel Dekker, 1993.
Chaudhuri 1969
Chaudhuri SK. Effect of nutrient supplementation on the
incidence of toxaemia of pregnancy. Journal of Obstetricsand Gynecology of India 1969;19:156–61.
Coulam 1991
Coulam CB. Epidemiology of recurrent spontaneous
abortion. American Journal of Reproductive Immunology1991;26(1):23–7.
Czeizel 1994b
Czeizel AE, Metneki J, Dudas I. The higher rate of multiple
births after periconceptional multivitamin supplementation:
an analysis of causes. Acta Geneticae Medicae et Gemellologiae(Roma) 1994;43:175–84.
Di Cintio 2001
Di Cintio E, Parazzini F, Chatenoud L, Surace M, Benzi G,
Zanconato G, et al.Dietary factors and risk of spontaneous
abortion. European Journal of Obstetrics & Gynecology andReproductive Biology 2001;95:132–6.
Ericson 2001
Ericson A, Kallen B, Aberg A. Use of multivitamins and
folic acid in early pregnancy and multiple births in Sweden.
Twin Research 2001;4(2):63–6.
Everett 1997
Everett C. Incidence and outcome of bleeding before the
20th week of pregnancy: prospective study from general
practice. BMJ 1997;315:32–4.
Godfrey 1996
Godfrey K, Robinson S, Barker DJ, Osmond C, Cox V.
Maternal nutrition in early and late pregnancy in relation to
placental and fetal growth. BMJ 1996;312(7028):410–4.
Goyaux 2001
Goyaux N, Alihonou E, Diadhiou F, Leke R, Thonneau
PF. Complications of induced abortion and miscarriage
in three African countries: a hospital-based study among
36Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

WHO collaborating centres. Acta Obstetricia et Gynecologica
Scandinavica 2001;80:568–73.
Haas 2009
Haas DM, Ramsey PS. Progestogen for preventing
miscarriage. Cochrane Database of Systematic Reviews 2009,
Issue 3. [DOI: 10.1002/14651858.CD003511.pub2]
Haider 2006
Haider BA, Bhutta ZA. Multiple-micronutrient
supplementation for women during pregnancy.. CochraneDatabase of Systematic Reviews 2006, Issue 4. [DOI:
10.1002/14651858]
Higgins 2009
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.2 [updated
September 2009]. The Cochrane Collaboration, 2009.
Available from www.cochrane-handbook.org.
Jauniaux 2000
Jauniaux E, Watson AL, Hempstock J, Bao Y-P, Skepper
JN, Nurton GJ. Onset of maternal arterial blood flow and
placental oxidative stress: a possible factor in human early
pregnancy failure. American Journal of Pathology 2000;157:
2111–22.
Katz 2001
Katz J, West KP Jr, Khatry SK, LeClerq SC, Christian P,
Pradhan EK, et al.Twinning rates and survival of twins in
rural Nepal. International Journal of Epidemiology 2001;30
(4):802–7.
Lee 1996
Lee C, Slade P. Miscarriage as a traumatic event: a review of
the literature and new implications for intervention. Journalof Psychosomatic Research 1996;40(3):235–44.
Lumley 2001a
Lumley J, Watson L, Watson M, Bower C. Modelling
the potential impact of population-wide periconceptional
folate/multivitamin supplementation on multiple births.
BJOG: an international journal of obstetrics and gynaecology
2001;108:937–42.
Lumley 2001b
Lumley J, Watson L, Watson M, Bower C. Periconceptional
supplementation with folate and/or multivitamins for
preventing neural tube defects. Cochrane Databaseof Systematic Reviews 2001, Issue 3. [DOI: 10.1002/
14651858.CD001056]
Morris 2001
Morris CD, Jacobson SL, Anand R, Ewell MG, Hauth JC,
Curet LB, et al.Nutrient intake and hypertensive disorders
of pregnancy: evidence from a large prospective cohort.
American Journal of Obstetrics and Gynecology 2001;184(4):
643–51.
NHMRC 2001
NHMRC. Report on Maternal Deaths in Australia 1994-96.
Canberra: NHMRC, 2001.
NRC 1989
National Research Council Committee on Diet and Health.
Diet and health: implications for reducing chronic disease risk.
Washington DC: National Academy Press, 1989.
Olsen 1999
Olsen RE. Vitamin deficiency, dependency, and toxicity.
In: Beers MH, Berkow R editor(s). The Merck manual of
diagnosis and therapy [electronic resource]. 17th Edition.
Whitehouse Station, NJ: Merck & Co, Inc, 1999.
Porter 2006
Porter TF, LaCoursiere Y, Scott JR. Immunotherapy
for recurrent miscarriage. Cochrane Database ofSystematic Reviews 2006, Issue 2. [DOI: 10.1002/
14651858.CD000112.pub2]
Preston 1996
Preston FE, Rosendaal FR, Walker ID, Briet E, Berntorp E,
Conard J, et al.Increased fetal loss in women with heritable
thrombophilia. Lancet 1996;348:913–6.
Ray 1999
Ray G, Laskin CA. Folic acid and homocyst(e)ine metabolic
defects and the risk of placental abruption, pre-eclampsia
and spontaneous pregnancy loss: a systematic review.
Placenta 1999;20:519–29.
Regan 1989
Regan L, Braude PR, Trembath PL. Influence of past
reproductive performance on risk of spontaneous abortion.
BMJ 1989;299:541–5.
RevMan 2008
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 5.0. Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2008.
Rivas 2000
Rivas-Echeverria CA, Echeverria Y, Molina L, Novoa D.
Synergic use of aspirin, fish oil and vitamins C and E for
the prevention of preeclampsia [abstract]. Hypertension inPregnancy 19;Suppl 1:30.
Rumbold 2008
Rumbold A, Duley L, Crowther C, Haslam RR.
Antioxidants for preventing pre-eclampsia. Cochrane
Database of Systematic Reviews 2008, Issue 1. [DOI:
10.1002/14651858.CD004227.pub3]
Simsek 1998
Simsek M, Naziroglu M, Simsek H, Cay M, Aksakal M,
Kumru S. Blood plasma levels of lipoperoxides, glutathione
peroxidase, beta carotene, vitamin A and E in women with
habitual abortion. Cell Biochemistry and Function 1998;16
(4):277–31.
Stern 1996
Stern JJ, Dorfmann AD, Gutierrez-Najar AJ, Cerrillo M,
Coulam CB. Frequency of abnormal karyotypes among
abortuses from women with and without a history of
recurrent spontaneous abortion. Fertility and Sterility 1996;
65(2):250–3.
37Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Waller 2003
Waller DK, Tita AT, Annegers JF. Rates of twinning before
and after fortification of foods in the US with folic acid,
Texas, 1996 to 1998. Paediatric and Perinatal Epidemiology2003;17(4):378–83.
WHO 1998
WHO. Safe Vitamin A dosage during pregnancy and lactation.Recommendations and report of a consultation (WHO/NUT/
98). Geneva: World Health Organisation, 1998.∗ Indicates the major publication for the study
38Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Briscoe 1959
Methods Randomisation and allocation concealment: unclear, no methodological details given,
dubious as the number of women allocated to the treatment group was more than double
that allocated to the placebo group. “Unselected patients were each given 200 capsules..
. these were given a code, unknown to us and contained either an inert powder or 100
mg each of ascorbic acid and hesperidin.”
Blinding of outcome assessment: women and study investigators did not know the
treatment codes
Documentation of exclusion: none reported.
Use of placebo control: placebo given; however, all women received an additional mul-
tivitamin supplement
Participants 406 women were recruited in the study. Eligible women were “unselected patients” in
private obstetrics care, that were less than or equal to 10 weeks’ pregnant, and were
eligible regardless of whether they were currently bleeding or the number of previous
pregnancies. Women greater than 10 weeks’ gestation were excluded. 406 women were
randomised to either vitamin C (n = 303) or placebo (n = 103), no losses to follow-up
were reported. 77 women in the study had more than 2 previous miscarriages and/or
bleeding in the pregnancy, and 329 had 2 or fewer miscarriages and no bleeding in the
pregnancy
Interventions All women were given 200 tablets, containing either 100 mg each of ascorbic acid and
hesperidin or placebo (an inert powder).
The study lasted for 7 weeks. For the first two weeks, women were asked to take 8 tablets
daily (i.e. daily 800 mg each of vitamin C and hesperidin or placebo). For the following 5
weeks, women took 4 tablets daily (i.e. daily 400 mg each of vitamin C and hesperidin or
placebo). All women received a multiple vitamin supplement containing 50 mg vitamin
C
Outcomes 1. Spontaneous miscarriage.
2. Spontaneous miscarriage in women with 2 or fewer previous miscarriages and no
bleeding in the current pregnancy.
3. Spontaneous miscarriage in women with more than 2 previous miscarriages and/
or bleeding in the current pregnancy.
4. Spontaneous miscarriage in women who experienced recurrent miscarriage.
Notes Women’s risk of spontaneous and recurrent miscarriage is unclear, as there is no infor-
mation about concurrent medical conditions or other risk factors for miscarriage. 9 of
the 406 women were classified as experiencing recurrent miscarriage.
No information is available about women’s nutritional status.
No sample-size calculation reported.
Intention-to-treat analyses performed (no losses to follow-up reported).
Compliance: no compliance information reported.
Location: Philadelphia, USA.
Timeframe: unclear.
39Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Briscoe 1959 (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear No methodological details given.
Allocation concealment? Unclear No methodological details given.
Blinding?
All outcomes
Yes Women and study investigators did not
know the treatment allocation
Incomplete outcome data addressed?
All outcomes
Yes No losses to follow up reported.
Free of selective reporting? Unclear Limited information about selection bias,
stated that ’unselected patients’ were in-
cluded
Free of other bias? Unclear Limited methodological details provided
including patient compliance
Chappell 1999
Methods Randomisation and allocation concealment: a computer-generated randomisation list
using blocks of 10 was given to the hospital pharmacy departments. Researchers allocated
the next available number to participants and women collected the trial tablets from the
pharmacy department
Blinding of outcome assessment: women, caregivers and researchers were blinded to
the treatment allocation until recruitment, data collection and laboratory analyses were
complete
Documentation of exclusion: 123 (43.5%) women were excluded, of which 70 women
were withdrawn because their second Doppler scan was normal. Pregnancy outcome
data were reported for all women randomised
Use of placebo control: placebo control.
Participants 283 women were recruited into the study. Inclusion criteria: abnormal Doppler wave-
form in either uterine artery at 18-22 weeks’ gestation or a history in the preceding
pregnancy of pre-eclampsia necessitating delivery before 37 weeks’ gestation, eclampsia
or the syndrome of HELLP.
Exclusion criteria: heparin or warfarin treatment, abnormal fetal-anomaly scan or mul-
tiple pregnancy.
Women were randomised at 18-22 weeks’ gestation; however, women with a previous
history who were identified at an earlier stage were randomised at 16 weeks’ gestation.
Women with abnormal Doppler waveform analysis returned for a second scan at 24
weeks’ gestation, those with a normal waveform at this time stopped treatment and
were withdrawn from the study. The remaining women who had persistently abnormal
waveforms, and those with a previous history or pre-eclampsia remained in the study and
were seen every 4 weeks through the rest of pregnancy. 1512 women underwent Doppler
40Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chappell 1999 (Continued)
screening, 273 women had abnormal waveforms and of these, 242 women consented to
the study. An additional 41 women who had a history of pre-eclampsia consented. 283
women were randomised to either the vitamin C and E group (n = 141) or the placebo
group (n = 142), 72 women had normal Doppler scans at 24 weeks’ gestation and 24
women did not return for a second scan and were withdrawn. A further 27 women
withdrew from the trial after 24 weeks’ gestation for various reasons. In total, 160 women
completed the trial protocol until delivery, 79 in the vitamin C and E group and 81 in
the placebo group. Pregnancy outcome data were presented for all women randomised
(n = 283) as well as only for those women completing the trial protocol (n = 160)
Interventions Women randomised to the vitamin C and E group received tablets containing 1000 mg
vitamin C daily and capsules containing 400 IU vitamin E daily.
Women randomised to the placebo group received tablets containing microcrystalline
cellulose and soya bean oil, that were identical in appearance to the vitamin C tablets
and vitamin E capsules. After 24 weeks’ gestation women were seen every 4 weeks, and
blood samples were taken at each visit
Outcomes 1. Ratio of PAI-1 to PAI-2.
2. Incidence of pre-eclampsia.
3. Placental abruption.
4. Spontaneous preterm delivery (< 37 weeks).
5. Intrauterine death.
6. Small-for-gestational-age infants (on or below the 10th centile).
7. Mean systolic and diastolic blood pressure before delivery.
8. Gestational age at delivery (median, IQR).
9. Birthweight (median, IQR).
10. Birthweight centile (median, IQR).
Notes Women’s risk of spontaneous and recurrent miscarriage is unclear, women were at high
risk of pre-eclampsia.
No information is available about women’s nutritional status.
Sample-size calculation reported, based on a 30% reduction in PAI-1.
Intention-to-treat analyses performed.
Compliance: “within the treated group, plasma ascorbic acid concentration increased by
32% from baseline values and plasma alpha-tocopherol increased by 54%”.
Location: London, UK.
Timeframe: unclear.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated random number list.
Allocation concealment? Yes Random number list used blocks of 10 and
was held by the pharmacy department
Blinding?
All outcomes
Yes Women, caregivers and researchers were
blinded until the analyses were completed
41Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chappell 1999 (Continued)
Incomplete outcome data addressed?
All outcomes
Yes 123 (43.5%) women were excluded, of
which, 70 women were withdrawn because
their second Doppler scan was normal.
Data were reported for all women ran-
domised
Free of selective reporting? Yes Data reported for all outcomes in methods.
Free of other bias? Yes The study appears to be free of other
sources of bias.
Christian 2003
Methods Randomisation and allocation concealment: cluster randomisation of 30 “village devel-
opment communities” using blocks of 5 within each community, randomisation oc-
curred by “drawing numbered identical chits from a hat”
Blinding of outcome assessment: women, field staff, investigators and statisticians did
not know the treatment codes until the end of the study
Documentation of exclusion: 534 (10.7%) women or infants were excluded and 343 (6.
7%) infants were lost to follow up
Use of placebo control: no placebo given, women in the control group were given vitamin
A only
Participants All women of reproductive age in the 30 village development communities were con-
sidered eligible. Women who were currently pregnant, breastfeeding a baby < 9 months
old, menopausal, sterilised or widowed were excluded.
Within the timeframe, 14,185 women were identified as likely to become pregnant.
Of these, 4998 pregnancies were confirmed with urine testing; however, 4926 women
remained in the trial with 72 women excluded either due to false positive pregnancy
testing, unknown outcomes or induced abortions. Women were allocated to either vita-
min A control (n = 1037), folic acid (n = 929), folic acid-iron (n = 940), folic acid-iron-
zinc (n = 982) or multiple micronutrients (n = 1038). 830 pregnancies (16.8%) ended
in either miscarriage, stillbirth or maternal death. The remaining pregnancies resulted in
4130 livebirths. Of these, 805 (19.5%) were excluded as they were either lost to follow-
up or birthweight was measured after 72 hours after birth. The final analysis involved
3325 infants allocated to control (n = 685), folic acid (n = 628), folic acid-iron (n = 635)
, folic acid-iron-zinc (n = 672) or multiple micronutrients (n = 705)
Interventions Women were allocated to one of five groups:
1. control (1000 mcg vitamin A);
2. folic acid (400 mcg, 1000 mcg vitamin A);
3. folic acid-iron (60 mg ferrous fumarate, 400 mcg folic acid, 1000 mcg vitamin A);
4. folic acid-iron-zinc (30 mg zinc sulphate, 60 mg ferrous fumarate, 400 mcg folic
acid, 1000 mcg vitamin A);
5. multiple micronutrients-folic acid-iron-zinc (60 mg ferrous fumarate, 400 mcg
folic acid, 30 mg zinc sulphate,1000 mcg vitamin A, 10 mcg vitamin D,10 mg vitamin
E, 1.6 mg vitamin B-1, 1.8 mg vitamin B-2, 20 mg niacin, 2.2 mg vitamin B-6, 2.6
mcg vitamin B12, 100 mg vitamin C, 65 mcg vitamin K, 2.0 mg copper, 100 mg
42Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Christian 2003 (Continued)
magnesium).
At enrolment women received 15 caplets and were instructed to take one caplet every
night. Women were then visited by field staff twice a week to monitor compliance and
replenish supplies of the caplets
Outcomes 1. Perinatal death, defined as stillbirths (gestational age >= 28 wk) and deaths among
liveborn infants in the first 7 days of life.
2. Neonatal deaths, defined as deaths from 0 to 28 days of life.
3. Infant death, defined as deaths from 0 to 90 days of life.
4. Birthweight.
5. Length.
6. Chest circumference.
7. Head circumference.
8. Low birthweight (< 2500 g).
9. Small-for-gestational age (below 10th centile for USA national reference for fetal
growth).
10. Preterm birth (< 37 weeks).
“The rate if miscarriage did not differ by treatment group and ranged between 12% and
15% (data not show)”. “Miscarriage was defined as a pregnancy that ended in a fetal loss
before 28 wk of gestation.”
Notes The following information was given about multiple births: “the numbers of twin preg-
nancies (34 pairs of liveborn twins and 8 pairs with one stillborn) was comparable across
treatment groups”.
Women’s risk of spontaneous and recurrent miscarriage is unclear, as there is no infor-
mation about concurrent medical conditions or other risk factors for miscarriage.
Information on women’s diet was recorded; however, no information was reported about
micronutrient intake, including vitamin A.
Sample-size calculation reported, 1000 pregnancies per group allowed for a minimum
detectable difference of 75 g in birthweight, and >= 34% reduction in fetal loss and >=
45% reduction in infant mortality, with 80% power.
Intention-to-treat analyses performed and the relative risks and confidence intervals were
adjusted to account for any cluster design effect.
Compliance: median compliance during pregnancy was 88%.
Location: Salarhi, Nepal.
Timeframe: December 1998 to April 2001.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Unlcear, ’cluster randomisation using
blocks of 5 within each community’
Allocation concealment? Unclear Unlcear, randomisation occurred by ’draw-
ing numbered identical chits from a hat’
Blinding?
All outcomes
Yes Women, field workers and researchers were
blinded until after the analysis
43Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Christian 2003 (Continued)
Incomplete outcome data addressed?
All outcomes
Yes 534 (10.7%) women or infants were ex-
cluded and 343 (6.7%) infants were lost to
follow-up, intention to treat analysis per-
formed
Free of selective reporting? Unclear Information about women’s diet was col-
lected but not reported
Free of other bias? Unclear Unclear due to limited information about
the cluster design including allocation con-
cealment
Correia 1982
Methods Randomisation and allocation concealment: unclear, “randomised” stated in text but no
details given
Blinding of outcome assessment: “double blind clinical test” stated in the text
Documentation of exclusion: 16 women (35%) excluded.
Use of placebo control: placebo control.
Participants 45 women were initially recruited into the study; however, results are presented for 29
women (folic acid group n = 16, placebo group n = 13). Women were excluded if they
had any “pathological data” or if there was “evidence of neglect”. No other details given
Interventions Women were randomised to either daily ingestion of 10 mg folic acid or placebo. Women
were asked to take the tablets from between 12 and 16 weeks until the end of pregnancy
Outcomes 1. Fetal weight (birthweight).
2. Placental weight.
Notes Women risk of spontaneous and recurrent miscarriage is unclear. Women’s nutritional
status is also unclear.
No sample-size calculation reported.
Compliance: unclear, no details given.
Country: Portugal.
Timeframe: unknown.
Published in Portuguese.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear No methodological details given.
Allocation concealment? Unclear No methodological details given.
44Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Correia 1982 (Continued)
Blinding?
All outcomes
Unclear Unclear, “double blind clinical test” stated
in the text.
Incomplete outcome data addressed?
All outcomes
No 16 women (35%) excluded.
Free of selective reporting? No Women were excluded if they had any
“pathological data” or if there was “evidence
of neglect” but not details given
Free of other bias? Unclear Limited methodological details given.
Czeizel 1994
Methods Randomisation and allocation concealment: unclear, “women agreed to their allocation
on the basis of a random table”
Blinding of outcome assessment: unclear, women were aware of the “blind use of one of
two kinds of tablets”, but no other details given
Documentation of exclusion: 49 women (1%) were lost to follow-up and excluded
Use of placebo control: “trace element control” given.
Participants 7765 women were recruited into the study. Women participating in the HOFPP who
volunteered to take part, were not currently pregnant, and who conceived within 12
months of ceasing contraception. In the first two years of the HOFPP, women were also
required to be aged < 35 years, and not to have had a previous pregnancy except a prior
induced abortion. 7905 women were approached, of which 140 refused participation,
7765 were randomised and 5502 women had a confirmed pregnancy and were allocated
to either multivitamins (n = 2819) or control (n = 2683). 49 women of the 5502
confirmed pregnancies were lost to follow-up
Interventions Women were provided with multivitamin or trace element ’control’ from at least 28 days
before conception continuing until at least the second missed menstrual period.
The multivitamin with folic acid contained 6000 IU vitamin A, 1.6 mg vitamin B1, 1.8
mg vitamin B2, 2.6 mg vitamin B6, 4.0 mcg vitamin B12, 100 mg vitamin C, 500 IU
vitamin D, 15 mg vitamin E, 19 mg nicotinamide, 10 mg calcium pantothenate, 0.2 mg
biotin, 0.8 mg folic acid, 125 mg calcium, 125 mg phosphorus, 100 mg magnesium, 60
mg iron, 1 mg copper, 1 mg manganese, 7.5 mg zinc.
The trace element control contained 7.5 mg vitamin C, 1 mg copper, 1 mg manganese
and 7.5 mg zinc
Outcomes 1. Neural tube defects and other birth defects.
2. Miscarriage.
3. Ectopic pregnancy.
4. Termination of pregnancy.
5. Live births.
6. Stillbirths.
7. Multiple gestation.
8. Subgroup data is available on menstrual cycle, first trimester symptoms and sexual
45Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Czeizel 1994 (Continued)
activity.
Notes Women’s risk of spontaneous and recurrent miscarriage is unclear.
Information on their dietary status is unknown.
No sample-size calculation reported.
Partial intention-to-treat analyses performed.
Compliance: compliance was assessed by questioning, checking the tick-off on the basal
temperature chart and counting of unused tablets. 70% of women in the multivitamin
group and 71% in the control group took the full course of the supplements, with an
additional 20% and 21% in the multivitamin and control groups respectively receiving
a partial course of supplementation.
Location: Hungary.
Time frame: 1 February 1984 to 30 April 1992.
The denominators used for this trial are the number of women randomised and with
a confirmed pregnancy (i.e. 2819 for the multivitamin group and 2683 for the control
group)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Methodological details unclear.
Allocation concealment? Unclear Methodological details unclear, ’women
agreed to their allocation on the basis of a
random table’
Blinding?
All outcomes
Unclear Women were aware of the ’blind use of one
of two kinds of tablets’, but no other details
given
Incomplete outcome data addressed?
All outcomes
Yes 49 women (1%) excluded, partial intention
to treat analyses performed
Free of selective reporting? Unclear Denominators vary with serial publica-
tions.
Free of other bias? Unclear Limited methodological details provided.
46Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fawzi 1998
Methods Randomisation and allocation concealment: block randomisation using blocks of 20,
eligible women were “assigned the next numbered bottle of regimen”. The study used
a 2 by 2 factorial design and women were randomised to 1 of 4 groups. Tablets were
indistinguishable and packaged in identically coded bottles
Blinding of outcome assessment: women and study investigators were unaware of the
treatment allocation, no information given about blinding of outcome assessors
Documentation of exclusion: 64 women (6%) were lost to follow-up and excluded
Use of placebo control: placebo given.
Participants 1085 women were recruited into the study. Pregnant women between 12 and 27 weeks’
gestation who were HIV-1 infected, living in Dar es Salaam and intended to stay there
for at least one year were eligible for the study. Women not HIV-1 positive or moving
out of Dar es Salaam were excluded. 13,879 pregnant women consented to be HIV-1
tested, of which 1806 were positive, and 1085 were randomised. Of these, 3 women
were not pregnant and 7 women died before delivery and were excluded from the trial.
Of the remaining 1075 women, 54 women (5%) were lost to follow-up by the time of
delivery, leaving birth outcomes reported for 1021 women. Women were randomised
to 1 of 4 groups: vitamin A (n = 269), multivitamins excluding vitamin A (n = 269);
multivitamins including vitamin A (n = 270) or placebo (n = 267)
Interventions Women were randomised to 1 of 4 groups:
1. vitamin A (30 mg beta-carotene plus 5000 IU preformed vitamin A);
2. multivitamins excluding vitamin A (20 mg vitamin B1, 20 mg vitamin B2, 25 mg
vitamin B6, 100 mg niacin, 50 mcg vitamin B12, 500 mg vitamin C, 30 mg vitamin
E, 0.8 mg folic acid);
3. multivitamins including vitamin A, all formulated in 2 tablets; or
4. placebo.
All women received 400 mg ferrous sulphate and 5 mg folic acid daily, as well as 500 mg
chloroquine phosphate weekly. At delivery, all women taking vitamin A were to receive
an additional oral dose of 200,000 IU vitamin A and the others an extra dose of a placebo.
Pill counts were conducted at each visit and new tablets were given out at each visit
Outcomes 1. Miscarriage, defined as delivery before 28 weeks’ gestation.
2. Stillbirth, defined as delivery of a dead baby at or after 28 weeks’ gestation.
3. Fetal death, defined as either miscarriage or stillbirth.
4. Low birthweight, defined as birthweight less than 2500 g.
5. Very low birthweight, defined as birthweight less than 2000 g.
6. Preterm delivery, defined as delivery before 37 weeks.
7. Severe preterm birth, defined as delivery before 34 weeks.
8. Small-for-gestational age, defined as birthweight less than the 10th percentile for
gestational age.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear, although may be
increased due to their HIV-1 positive status.
Women’s nutritional status is also unclear.
Figures change with serial publications, particularly for secondary outcomes, and results
are not reported separately for the individual 4 groups. Results are reported as: any
multivitamins, multivitamin, any vitamin A or no vitamin A.
Sample-size calculation performed allowing for 20% loss to follow up.
47Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fawzi 1998 (Continued)
Intention-to-treat analyses performed.
Compliance: compliance assessed by the percentage of prescribed tablets absent from
the returned bottles, and in plasma vitamin A concentrations in a subset of 100 women.
Median compliance assessed using pill counts was 90% by the time of delivery.
Location: Tanzania.
Timeframe: April 1995 to July 1997.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Block randomisation using blocks of 20.
Allocation concealment? Unclear Women assigned the ’next numbered bottle
of regimen’.
Blinding?
All outcomes
Yes Women and investigators were blinded.
Incomplete outcome data addressed?
All outcomes
No 64 women (6%) were lost to follow up and
excluded, intention to treat analyses per-
formed
Free of selective reporting? Unclear Figures change with serial publications,
particularly for secondary outcomes, and
results are not reported separately for the
individual 4 groups
Free of other bias? Unclear Limited methodological details provided.
Fawzi 2007
Methods Randomisation: unclear about sequence generation.
Allocation concealment: States a list was prepared according to the randomisation se-
quence in blocks of 20, tablets were bottled in identical coded bottles, eligible women
were given the next numbered bottle
Blinding of outcome assessment: Women and research assistants who assessed the study
outcomes were unaware of the intervention groups
Documentation of exclusion: 49 women lost to follow-up (multivitamin group: 23,
placebo group: 26), no post-randomisation exclusions
Use of placebo control: placebo given.
Participants 8428 women were randomised in the study. Pregnant women between 12 and 27 weeks
who had a negative test for HIV infection and planned to stay in the city until delivery
and for 1 year thereafter recruited through antenatal clinics in Dar es Salaam. 8468
women were enrolled, however 40 women were then found to be ineligible. 8428 women
were randomly assigned to receive either a multivitamin (n = 4214) or placebo (n = 4214)
from the time of enrolment until 6 weeks after delivery. 6 women died before delivery
48Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fawzi 2007 (Continued)
and 43 were lost to follow up by the time of delivery
Interventions The supplements included 20 mg of vitamin B1, 20 mg of vitamin B2, 25 mg of vitamin
B6, 100 mg of niacin, 50 mcg of vitamin B12, 500 mg of vitamin C, 30 mg of vitamin
E, and 0.8 mg of folic acid
The active tablets and placebo were similar in shape, size, and colour
All women, irrespective of the assigned study regimen, were given daily doses of iron (60
mg of elemental iron) and folic acid (0.25 mg). They were also given malaria prophylaxis
in the form of sulfadoxine-pyrimethamine tablets at 20 weeks and 30 weeks of gestation
Outcomes 1. Low birthweight (< 2500 g).
2. Preterm delivery (before 37 weeks’ gestation).
3. Fetal death.
4. Birthweight below 2000 g.
5. Extremely preterm delivery (before 34 weeks).
6. Small-for-gestational age (birthweight below the 10th percentile for gestational
age).
7. Fetal death and death in the first 6 weeks of life.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear.
Intention to treat analyses performed.
Compliance: Average compliance was 88%, no difference in compliances between the
two groups
Location: Tanzania.
Timeframe: August 2001 and July 2004.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Generation of sequence not reported, ex-
cept that there were blocks of 20 in the se-
quence
Allocation concealment? Yes Identical coded bottles prepared according
to the randomisation list, eligible women
were assigned the next numbered bottle
Blinding?
All outcomes
Yes Women and outcome assessors were
blinded to allocation.
Incomplete outcome data addressed?
All outcomes
Yes 49 (1%) women lost to follow-up, balanced
across groups, analyses by intention to treat
Free of selective reporting? Yes All pre-specified outcomes appear to be re-
ported.
49Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fawzi 2007 (Continued)
Free of other bias? Yes The study appears to be free of other
sources of bias.
Fleming 1968
Methods Randomisation and allocation concealment: quasi-randomised, alternate women were
allocated to receive folic acid or placebo according to the order in which they attended
antenatal clinic. No other methodological details were given
Blinding of outcome assessment: women and investigators were blinded to the treatment
allocation, until after the completion of the trial
Documentation of exclusion: 21 women (28%) excluded from the analysis
Use of placebo control: control tablet containing iron given
Participants 75 women were recruited into the trial. Women were eligible if they were primigravida,
less than 26 weeks’ pregnant (range of gestation 10 to 26 weeks’), with haematocrit value
(PCV) 27 per cent or more, and who had not received treatment so far as was known.
Women with Haemoglobin (Hb) SC, Hb.SS, Hb.CC were excluded. Alternate patients
were allocated to group A (placebo) or B (folic acid). 75 women were included (40 in
group A and 35 in group B) initially; however, only 26 in group A and 28 in group B
completed the trial. 16 women (10 in group A and 8 in group B) defaulted from the
trial, 3 (2 in group A and 1 in group B) were anaemic on the second visit warranting folic
acid treatment, 1 in group A self medicated with folic acid and 1 in group A ’aborted’
Interventions All women received antimalarials and iron supplements as per the standard antenatal
care at the hospital.
Women in group B received 5 mg folic acid tablets on each attendance, which was
fortnightly initially and weekly in the last trimester.
Group A received “one tablet of lactose base and colouring matter in the same manner.”
Outcomes 1. PCV and reticulocyte index.
2. Serum folic acid concentration and ’megaloblastic score’.
3. Malarial infection.
4. Maternal morbidity (pyelonephritis, pre-eclamptic toxaemia, septicaemia,
puerperal psychosis).
5. Prematurity.
6. Birthweight (mean birthweight but no standard deviation).
7. Fetal mortality.
Notes Results not reported as intention to treat; however, where possible, the review authors
included data in the review as intention to treat.
Unclear of women’s risk of spontaneous and recurrent miscarriage.
16 women in the trial showed evidence of folic acid deficiency at trial entry.
Sample-size calculation: none reported.
No intention-to-treat analyses performed.
Compliance: no compliance information reported specifically; however, women were
“seen to swallow” the tablets at their fortnightly and weekly visits.
Location: Nigeria.
Time frame: unclear.
50Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fleming 1968 (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No Quasi-randomised, alternate allocation.
Allocation concealment? No Quasi-randomised, alternate allocation.
Blinding?
All outcomes
Yes Women and investigators blinded.
Incomplete outcome data addressed?
All outcomes
No 21 women (28%) excluded from the anal-
ysis.
Free of selective reporting? Unclear Results not reported as intention to treat;
however, where possible, the review authors
included data in the review as intention to
treat
Free of other bias? Unclear Limited methodological details provided.
Fleming 1986
Methods Randomisation and allocation concealment: women were “randomly allocated to one of
five groups using a random number table”, no other details given
Blinding of outcome assessment: Women and investigators were blinded to the treatment
allocation, until after the completion of the trial
Documentation of exclusion: 18 women (9%) were excluded due to anaemia at enrol-
ment, ’defaulting’, or being ’mentally subnormal’, these women were replaced by other
women chosen by an investigator. A further 42 women were excluded before delivery
and another 30 failed to attend the postnatal clinic, birth outcomes were available for
160 women (80%)
Use of placebo control: no placebo control.
Participants 228 women met the eligibility criteria; however 200 pregnant women were recruited
into the study. Women were allocated to one of five groups; 40 women were allocated
to each group
Eligible women included:
1. Hausa women living in Zaria and planning to deliver in Zaria;
2. pregnant for the first time;
3. at less than 24 weeks’ gestation, as estimated by the height of the fundus uteri;
4. the wives of unskilled or semiskilled men.
Women were excluded if they had already taken any antimalarial treatment or haema-
tinics during the pregnancy, or had the following complications: hydatiform mole, hae-
moglobin SC disease, overt anaemia or proteinuria
The mean gestational age of women at enrolment was 18.5 weeks
51Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fleming 1986 (Continued)
Interventions Women were allocated to 1 of 5 groups:
• Group 1: No active treatment (control);
• Group 2: Antimalarials only (600mg chloroquine/day + 100 mg proguanil/day);
• Group 3: Iron + antimalarials (60 mg iron/day + 600mg chloroquine/day + 100
mg proguanil/day);
• Group 4: Folic acid + antimalarials (1 mg folic acid/day + 600mg chloroquine/day
+ 100 mg proguanil/day);
• Group 5: Iron + folic acid + antimalarials (1 mg folic acid/day + 60 mg iron/day +
600mg chloroquine/day + 100 mg proguanil/day).
Outcomes Maternal outcomes
1. Anaemia (severe and mild/moderate) before 28 weeks’, between 28-36 weeks’,
and after 36 weeks’ gestation.
2. Gestation age.
3. Mode of delivery.
4. Complications of pregnancy (abortion, hypertension, pre-eclampsia or eclampsia,
hydramnios, abdominal pain).
Infant outcomes
1. Fetal distress.
2. Birthweight.
3. Apgar score at two minutes.
4. Fetal complications.
Laboratory outcomes
1. Hb concentration, red cell indices and WBC at first attendance, 28 weeks, 36
weeks, at delivery (form mother and infant) and six weeks postpartum.
Not all outcomes were reported for each individual treatment group. Miscarriage was
reported for the combined groups 4 and 5, therefore for the purpose of this review the
groups 4 and 5 are combined (folic acid + iron) and compared with group 2 and group
3 (iron + antimalarials). The authors reported that 8 women had hypertension without
other signs, 21 women had preeclampsia and 6 developed eclampsia, with no association
between these outcomes and treatment group. No other details were provided, including
the breakdown of these outcomes by treatment group
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women were at high risk of anaemia. Information about other nutritional indices was
not provided
Intention to treat analyses not performed, however, where possible, the review authors
included data in the review as intention to treat
Compliance: 72 women (36%) were classed as defaulters.
Location: Nigeria.
Timeframe: Unclear.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear A random number table was used but no
details provided of how it was generated
52Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Fleming 1986 (Continued)
Allocation concealment? Unclear No details provided about the allocation.
Blinding?
All outcomes
Yes Neither the researchers nor the patients
were aware of the treatment allocation un-
til after the completion of the study
Incomplete outcome data addressed?
All outcomes
No 228 women met the entry criteria, but
only 200 were included in the trial. 18
women were excluded and replaced by
other women
Free of selective reporting? No Not all outcomes are reported by treatment
group. In serial publications up to 70% of
the data was excluded
Free of other bias? Unclear Limited methodological details provided.
Hemmi 2003
Methods Randomisation and allocation concealment: unclear, “patients were randomly assigned
to the control group or the study group”. No other methodological details given
Blinding of outcome assessment: unclear, no details given.
Documentation of exclusion: 28 women (19%) in the control group were excluded, no
details given for the exclusion
Use of placebo control: no placebo control.
Participants 150 women were recruited into the study. Women with a luteal phase defect, as described
by a peak serum P level < 120 mg/mL in the mid-luteal phase measured at 3 time points,
were eligible and invited to participate. Luteal phase defects were ascertained in two
consecutive menstrual cycles, and the third cycle was the intervention cycle. Women
receiving IVF-ET treatment were excluded. 313 women were considered for enrolment
in the study, 150 (48%) were randomised. 28 women were withdrawn from the control
group, leaving 122 women in the study, who were allocated to vitamin C (n = 76) or
control (n = 46). 5 women in the control group and 19 women in the vitamin C group
became pregnant during the study period
Interventions Women in the intervention group took 750 mg vitamin C per day from the first day
of the third menstrual cycle until a urinary pregnancy test was positive. Pregnancy rate
was checked up until 6 months after the study cycle was started. Women in the control
group received no supplementation and no treatment was given in the third cycle
Outcomes 1. Serum P concentrations.
2. Serum E2 (oestrogen) concentrations.
3. Pregnancy rate.
4. Miscarriage.
53Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hemmi 2003 (Continued)
Notes Women’s risk of spontaneous or recurrent miscarriage was unclear according to criteria
specified in the review.
Their dietary intake of vitamin C is unknown.
No sample-size calculation was reported.
Analyses were not based on intention to treat.
Compliance: no details of any compliance assessments were given.
Country: Japan.
Time frame: January 1997 to December 2000.
The denominators used for this trials are the number of women randomised and with a
confirmed pregnancy (i.e. 19 for the vitamin group and 5 for the control group)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Methodological details unclear.
Allocation concealment? Unclear Methodological details unclear.
Blinding?
All outcomes
Unclear Methodological details unclear.
Incomplete outcome data addressed?
All outcomes
No 28 women (19%) in the control group ex-
cluded.
Free of selective reporting? Unclear No details of exclusion of women in the
control group given.
Free of other bias? No No placebo control.
ICMR 2000
Methods Randomisation and allocation concealment: unclear, “containers of vitamin or placebo
capsules were given a random number” and “the key to random numbers was kept at
the ICMR Headquarters”. No other methodological details were given
Blinding of outcome assessment: “double blind” mentioned in the text, but no details
given
Documentation of exclusion: 187 women (40%) were excluded from the analysis
Use of placebo control: placebo control.
Participants 466 women were recruited into the study. Women who had previously given birth to a
child with an open NTD, and planned to have another child were eligible and invited to
participate. This was regardless of their parity, number of previous births with an NTD,
age, consanguinity, and socio-economic status. Women who had previously given birth
to a child with closed spina bifida, or with a history of diabetes or abnormal fasting
and post-prandial blood sugar, history of epilepsy, congenital anomalies indicative of a
genetic syndrome in the previous NTD, history of vitamin intake in the 3 months prior
to enrolment, and pregnancy were excluded. 466 women were enrolled and randomised
54Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ICMR 2000 (Continued)
to either vitamin (n = 231) or placebo (n = 235), of these women, 90 were lost to follow-
up immediately and 71 did not conceive until the final follow-up. Of the remaining
305 women who were known to become pregnant (vitamin n = 152, placebo n = 153),
pregnancy outcomes were unknown for 26 women. In the paper, 279 of the initial 466
women were included in the analysis; however, in this review results are presented for
main outcomes on an intention-to-treat basis (i.e. n = 466)
Interventions The folic acid containing multivitamin included 120 mg ferrous sulphate, 240 mg
calcium phosphate, 4000 IU vitamin A, 400 IU vitamin D, 2.5 mg vitamin B1, 2.5 mg
vitamin B2, 2 mg vitamin B6, 15 mg nicotinamide, 40 mg vitamin C, 4 mg folic acid,
10 mg zinc.
The placebo tablets contained the following trace elements: 120 mg ferrous sulphate
and 240 mg calcium phosphate. Both capsules were identical in appearance and women
were provided with the tablets from at least 28 days before conception and continuing
until at least the second missed menstrual period
Outcomes 1. Recurrence of neural tube defects.
2. Live births.
3. Stillbirths.
4. Spontaneous and induced abortion.
5. Multiple birth.
Notes The risk profile of women in the trial for spontaneous and recurrent miscarriage is
unclear, as is the dietary intake of participants.
Sample-size calculation performed, assuming a 20 per cent drop out rate. The trial was
terminated after publication of the MRC trial in 1991.
Compliance: compliance was assessed at 3 monthly visits, by checking a diary card
maintained by the woman and the number of capsules returned. If the total number of
missed days in 3 months did not exceed 10 days, and the total number of missed days at
a stretch did not exceed three, compliance was taken as satisfactory. Women not meeting
the above criteria were excluded if they became pregnant in that particular quarter. No
compliance data are specifically reported.
Analyses not based on intention to treat.
Country: India.
Time frame: 1988 to 1991.
The denominators used for this trial are based on the number of women randomised
(i.e. 231 for the vitamin group and 235 for the placebo group). There was not enough
information to accurately confirm the number of women that did or did not become
pregnant due to the large number of losses to follow up
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Containers ’given a random number’.
Allocation concealment? Unclear ’Key to random numbers were kept at the
ICMR headquarters’ but no other details
given
55Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ICMR 2000 (Continued)
Blinding?
All outcomes
Unclear Double blind mentioned in the text but no
details given.
Incomplete outcome data addressed?
All outcomes
No 187 (40%) women excluded.
Free of selective reporting? Unclear Difficult to assess given the high losses to
follow-up.
Free of other bias? Unclear Limited methodological details provided.
Katz 2000
Methods Randomisation and allocation concealment: cluster randomised. 270 centres in the
Salarhi district, Nepal, were involved which included 30 subdistricts each with 9 wards.
Each ward was assigned to 1 of 3 treatment groups. “Wards were assigned by a random
draw of numbered chits, blocked on subdistrict”
Blinding of outcome assessment: women and study investigators were not aware of
the treatment codes. Maternal mortality was assessed by study investigators blinded to
treatment allocation, no details were given for other outcomes
Documentation of exclusions: 157 (1%) women were lost to follow-up and excluded
Use of placebo: placebo control.
Participants 15,832 women were recruited into the study. All married women of child bearing age in
the Salarhi district, Nepal, were eligible and invited to participate in the study. Women
migrating into the study area, or women that were never pregnant or refused participa-
tion, or women who migrated before being pregnant, were excluded from the analysis.
Eligible women were identified from census data and marriage registers. 44,646 women
were recruited, of which 1136 (2.5%) were excluded as they either emigrated before
becoming pregnant, died or refused consent. During the study period 15,832 women
identified themselves as being pregnant, and 157 women were lost to follow-up in the
postpartum period. Results are reported for 17,373 pregnancies, allocated to the fol-
lowing groups: vitamin A (n = 6070), beta-carotene (n = 5650) or placebo (n = 5653).
Denominators for the treatment groups vary for the measures of early infant mortality,
due to losses to follow-up after birth
Interventions The three treatment groups consisted of a weekly single oral supplement of either:
1. 23,300 IU preformed vitamin A as retinyl palmitate;
2. 42 mg of all trans beta-carotene;
3. placebo.
All capsules contained mg dl-alpha-tocopherol as an antioxidant. Women took the tablets
prior to conception, during pregnancy and postpartum, for a total of 3.5 years
Outcomes 1. Fetal loss, defined as any reported miscarriage, stillbirth or maternal death during
pregnancy. The outcomes were based on self reports, and women who reported to be
pregnant for >= 6 weeks but then no longer reported being pregnant were considered to
have had a miscarriage.
Serial publications also reported neonatal death.
56Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Katz 2000 (Continued)
Notes Women’s risk profile for spontaneous or recurrent miscarriage was unclear, as was their
dietary intake of vitamin A.
Compliance: women were distributed the capsules in their home on a weekly basis,
receipt of capsules was noted only if the distributor observed the woman swallowing the
capsule. Over half of the women who became pregnant during the study received over
80% of their intended supplements, and 75% of pregnant women received at least half
of their eligible doses.
There were serial publications of this study causing the study numerators and denomi-
nators to vary between published versions, and multiple pregnancy figures reported did
not include higher order pregnancies.
Sample-size calculation performed.
Partial intention-to-treat analyses, and the relative risks and confidence intervals were
adjusted to account for any cluster design effect.
Country: Nepal.
Timeframe: April 1994 to September 1997.
The denominators used for this trial are the number of women randomised who identified
themselves as pregnant (i.e. 6070 for the vitamin A group, 5650 for the beta-carotene
group and 5653 for the placebo group)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Cluster randomised, unclear how sequence
was generated.
Allocation concealment? Unclear Each ward was assigned to the treatment
groups based on ’a random draw of num-
bered chits, blocked on subdistrict’
Blinding?
All outcomes
Yes Women and investigators blinded to treat-
ment allocation.
Incomplete outcome data addressed?
All outcomes
Unclear 157 women (1%) were lost to follow-up
and excluded, partial intention to treat
analysis performed
Free of selective reporting? No Denominators vary in serial publications of
this trial.
Free of other bias? No Some women were pregnant more than
once during the study period, however the
denominators reported are the total num-
ber of pregnancies during the study pe-
riod, not the total number of women ran-
domised, which incorrectly assumes that
each data point included is independent
from the next
57Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kirke 1992
Methods Randomisation and allocation concealment: block randomisation, stratified by hospital,
using “consecutively numbered, opaque, sealed envelopes”
Blinding of outcome assessment: women and study investigators were initially blinded to
the treatment allocation, however the tablet preparations were changed after 55 women
were randomised and after this only participants were blinded
Documentation of exclusion: 3 women (1%) were lost to follow-up and excluded
Use of placebo control: 3 treatment regimens were assessed, no placebo control
Participants 354 women were recruited into the study. Women with a previous neural tube defect
defined as anencephalus, iniencephalus, encephalocoele, and spina bifida aperta, who
were not pregnant when contacted but were planning a future pregnancy, were eligible
and invited to participate. Women were identified from case registers at the participat-
ing hospitals. Women with conditions likely to result in impaired absorption from the
gastrointestinal tract were excluded.
435 women were approached, of which 354 (84%) consented and were randomised to
either F (n = 115 ), MV (n = 119) or MF (n = 120). 16 women did not become pregnant,
and 75 women withdrew; however, their pregnancy outcome status was known, and 18
of these women subsequently became pregnant after withdrawing. 3 women were lost
to follow-up. 281 women (93 in the F group, 93 in the MF group and 95 in the MV
group) became pregnant in the study period and their pregnancy outcome was known
Interventions Indistinguishable trial tablets were initially made by Beecham and Glaxo, however
Beecham withdrew their support after 55 women had been randomised. After this time
a commercially available pregnavite Forte F was used (MF tablet) and Antigen Pharma-
ceuticals produced a white multivitamin tablet without folic acid. This was associated
with a loss of blinding. Women were randomised to one of three treatments:
1. folic acid alone (F);
2. multivitamin with folic acid (MF);
3. multivitamin with no folic acid (MV).
The F and MF resulted in a daily dose of 0.3 mg folic acid. The MF and MV resulted in
a daily dose of 4000 IU vitamin A, 400 IU calciferol, 1.5 mg thiamine hydrochloride, 1.
5 mg riboflavine, 1 mg pyridoxine hydrochloride, 15 mg nicotinamide, 40 mg ascorbic
acid, 480 mg calcium phosphate, and 252 mg ferrous sulphate. Women took the tablets
for at least 2 months prior to conception and until the date of the 3rd missed period
Outcomes 1. Recurrence risk of neural tube defects.
2. Spontaneous abortion.
3. Ectopic pregnancy.
4. Livebirth.
5. Stillbirth.
6. Congenital malformations excluding neural tube defects.
Notes The trial was stopped after there were poor recruitment rates and birth rates. A sample-
size calculation required 462 women to show a reduction in neural tube defects from
5% to 1%. Data from 106 women who were already pregnant at time of recruitment
are also included.
The risk profile of women in the trial for spontaneous and recurrent miscarriage is
unclear, as is their dietary intake.
Compliance: compliance was assessed on tablet counts and blood tests; however, the
58Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kirke 1992 (Continued)
results are not presented.
Intention-to-treat analyses were performed.
Country: Republic of Ireland.
Timeframe: December 1981 to January 1988.
The denominators used for this trial are the number of women randomised who became
pregnant in the study period and their pregnancy outcome was known (i.e. 93 in the F
group, 93 in the MF group and 95 in the MV group)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Block randomisation stratified by hospital
site.
Allocation concealment? Yes Consequtively numbered, opaque sealed
envelopes used.
Blinding?
All outcomes
Yes Only participants were blinded.
Incomplete outcome data addressed?
All outcomes
Yes 3 women (1%) lost to follow-up and ex-
cluded. Intention to treat analyses per-
formed
Free of selective reporting? Unclear Compliance data not reported.
Free of other bias? No The trial was stopped after there were poor
recruitment rates and birth rates
Kumwenda 2002
Methods Randomised controlled trial of vitamin A, iron and folic acid supplementation versus
iron and folic acid only, during pregnancy, to improve infant outcomes born to women
infected with HIV in Malawi
Randomisation and allocation concealment: “treatment assignment was determined by
use of a computer’s random-number generator” and “mothers were assigned an original
study identification number at enrolment and were given the next sequentially numbered
opaque bottle with supplements”. “Treatment assignment was concealed by pre pack-
ing study supplements in sequentially numbered series assigned to study identification
numbers.”
Blinding of outcome assessment: unclear, not specifically stated, but participants were
blind to their treatment allocation
Documentation of exclusion: 63 (9%) women were lost to follow-up and 14 (2%) pairs
of twins were excluded
Use of placebo control: control tablets containing iron and folic acid were given
59Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kumwenda 2002 (Continued)
Participants Pregnant women between 18 and 29 weeks’ gestation and infected with HIV. The average
gestation of participants was 23 weeks. 693 women were enrolled and allocated to either
vitamin A (n = 340) or control (n = 357), of which pregnancy outcomes were known for
623 women. 63 women were lost to follow-up and 14 sets of twins were excluded due
to their higher risk of low birthweight and infant mortality
Interventions All women received orally administered daily doses of 30 mg iron and 400 mcg folic
acid during the study. Women in the intervention group received 10,000 IU vitamin
A (3 mg retinol equivalent) orally, in addition to the iron and folic acid supplements.
Women were asked to take the tablets from enrolments until delivery. Tablet counts
were conducted every 4 weeks. All women received 30 mg retinol equivalents at 6 weeks
postpartum, according to standard postpartum care in Malawi
Outcomes 1. Infant haemoglobin level at 6 weeks and 12 months of age.
2. Percentage of infants with anaemia at 6 weeks of age and at 12 months, defined as
a haemoglobin level of < 110 g/L.
3. Birthweight.
4. Percentage of infants < 2500 g at birth.
5. Weight and length at 6 weeks, 14 weeks and 6 months of age.
6. Transmission of HIV to the infant, infant mortality at < 6 weeks of age, at 12
months and at 24 months.
7. Stillbirth and spontaneous abortion (undefined).
Notes Women’s risk of spontaneous and recurrent miscarriage is unclear, although may be
increased due to their HIV status.
50% of women in the vitamin A group and 51% of women in the control group had
deficient levels of vitamin A (defined as plasma vitamin A < 0.70 umol/L) at trial entry.
Sample-size calculation performed.
No intention-to-treat analyses were performed.
Compliance: more than 95% of women in both groups took > 90% of study supplements,
as ascertained by tablet counts.
Location: Malawi.
Timeframe: November 1995 toDecember 1996.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated random number list.
Allocation concealment? Yes Sequentially number opaque bottles used.
Blinding?
All outcomes
Unclear Not specifically stated but women were
blinded.
Incomplete outcome data addressed?
All outcomes
Unclear 63 women (9%) lost to follow-up and 14
pairs of twins (2%) excluded. No intention
to treat analyses performed
60Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kumwenda 2002 (Continued)
Free of selective reporting? Yes All pre-specified outcomes appear to be re-
ported.
Free of other bias? Unclear Insufficient information to assess whether
an important risk of other bias exists
MRC 1991
Methods Randomisation and allocation concealment: third party randomisation, “randomisation
was carried out through the Clinical Trials Service Unit in Oxford”. Randomisation was
stratified by centre
Blinding of outcome assessment: women, caregivers and study investigators were blinded
to the treatment allocation
Documentation of exclusion: 164 women (9%) excluded.
Use of placebo control: placebo control.
Participants 1817 women were recruited into the study. Women who had a previous pregnancy
affected by a neural tube defect, and were planning another pregnancy and not already
taking supplements were eligible for the study. Women whose affected child had Meckel’s
syndrome and those women with epilepsy were excluded. 1817 women were randomised
to either F (n = 449), MV (n = 453), MF (n = 461) or P (n = 454), of which, 1195
were informative pregnancies that is, where the outcome of NTD or not was definitely
known (F n = 298, MV n = 302, MF n = 295, P n = 300). Results for pregnancy loss
are reported for both informative and not informative pregnancies. 164 women were
excluded as they may have been pregnant at the time of randomisation
Interventions Women were randomised into 1 of 4 groups:
1. 4 mg, 240 mg di-calcium phosphate and 120 mg ferrous sulphate (F);
2. 4000 IU vitamin A, 400 IU calciferol, 1.5 mg thiamine hydrochloride, 1.5 mg
riboflavine, 1 mg pyridoxine hydrochloride, 15 mg nicotinamide, 40 mg ascorbic acid,
240 mg di-calcium phosphate and 120 mg ferrous sulphate (MV);
3. folic acid combined with the multivitamins specified above (MF);
4. placebo containing 240 mg di-calcium phosphate and 120 mg ferrous sulphate
only (P).
Women took the tablets prior to conception and attended the site every 3 months to
collect additional supplies and again during the 12th week of pregnancy. No special
dietary advice was given to women
Outcomes 1. Neural tube defect and other birth defects.
2. Spontaneous abortions.
3. Ectopic pregnancy.
4. Termination or pregnancy.
5. Livebirth.
6. Stillbirth.
7. Multiple pregnancy.
8. Subsequent publications report on blood folic acid and zinc concentrations.
61Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

MRC 1991 (Continued)
Notes The trial was stopped early after there were 1195 informative pregnancies, according to
prespecified stopping rules. The aim of the study was to obtain information on at least
2000 informative pregnancies unless a sufficiently clear result emerged sooner.
Women’s risk profile for spontaneous and recurrent miscarriage was unclear, as was their
nutritional status.
Compliance: compliance based on self reports, and data were available for women with
an informative pregnancy only, where 79 (6%) women reported they stopped taking
their capsules before their last scheduled visit.
Intention-to-treat analyses are reported in this review including not informative preg-
nancies (i.e. n = 1817).
Location: multi-national study coordinated from the United Kingdom.
Timeframe: July 1983 to April 1991.
The denominators used for this trial are the number of women randomised i.e. (449 for
the F group, 453 for the MV group, 461 for the MF and 454 for the P group). There was
no information provided about any women randomised that did not become pregnant
in the study period
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Third party randomisation, “randomisa-
tion was carried out through the Clinical
Trials Service Unit in Oxford”
Allocation concealment? Yes Third party randomisation, “randomisa-
tion was carried out through the Clinical
Trials Service Unit in Oxford”
Blinding?
All outcomes
Yes Women, caregivers and investigators
blinded to treatment allocation
Incomplete outcome data addressed?
All outcomes
Yes 164 women (9%) excluded, intention-to-
treat analyses performed
Free of selective reporting? Unclear No information provided about any
women randomised that did not become
pregnant in the study period
Free of other bias? No The trial was stopped early after there were
1195 informative pregnancies, according
to prespecified stopping rules
62Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Osrin 2005
Methods Randomisation and allocation concealment: One of the authors ’randomly allocated
1200 participant numbers by computer into two groups in permuted blocks of 50’. Ev-
ery identification number was allocated a supplement container, which was then packed
by a team member not otherwise involved in the trial. After enrolment, another author
allocated participants sequential identification numbers with the corresponding supple-
ment containers
Blinding of outcome assessment: double blind stated but no other details given
Documentation of exclusion: 61 women (5%) withdrew or were lost to follow-up, how-
ever data on miscarriage were reported for those who withdrew due to miscarriage
Use of placebo control: control of iron and folic acid supplements given which looked
identical to the intervention supplements
Participants 1200 women were recruited into the study. Women were eligible if they were: less than
20 completed weeks, had a singleton pregnancy, no notable fetal abnormality, no existing
maternal illness of a severity that could compromise the outcome of pregnancy, and lived
in an area of Dhanusha or the adjoining district of Mahottari accessible for home visits
Maternal illnesses that led to exclusion were: recently treated recurrent cysticercosis,
need for chlorpromazine or anticoagulant drugs with changing doses, and symptomatic
mitral stenosis or multivalvular heart disease. Fetal exclusions were: twin pregnancies,
anencephaly, occipital meningocele, encephalocele, duodenal atresia and a grossly dilated
pelvicalyceal system
Interventions Intervention group: vitamin A 800 µg, vitamin E 10 mg, vitamin D 5 µg, vitamin B1 1.
4 mg, vitamin B2 1.4 mg, niacin 18 mg, vitamin B6 1.9 mg, vitamin B12 2.6 µg, folic
acid 400µg, vitamin C 70 mg, iron 30 mg, zinc 15 mg, copper 2 mg, selenium 65 µg,
and iodine 150 µg
Control group: iron 60 mg and folic acid 400 µg.
Supplementation began at a minimum of 12 weeks’ gestation and continued until de-
livery
Outcomes 1. Birthweight.
2. Gestational duration.
3. Infant length and head circumference.
4. Miscarriage defined as cessation of confirmed pregnancy before 23 weeks’
gestation.
5. Stillbirth defined as delivery of an infant showing no signs of life (movement,
breathing, or heartbeat) after 23 weeks’ gestation.
6. Early neonatal death defined as death of a live born infant in the first 7 days after
birth.
7. Late neonatal death as death of a live born infant after 7 but within 28 days.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear, however, women are presumable at high risk
of under-nutrition as the paper states that in Nepal ’deficiencies of several micronutrients
have been well described in individual studies and in a national sample’
Intention to treat analyses performed.
Compliance: Median ’adherence’ was 98% in the control group and 97% in the inter-
vention group
Location: Nepal.
63Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Osrin 2005 (Continued)
Timeframe: August 2002 to October 2003.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated in permuted blocks of
50.
Allocation concealment? Unclear One of the authors allocated participants
with sequential identification numbers, but
unclear if this person was involved in the
recruitment of participants
Blinding?
All outcomes
Unclear Double blind stated in the text but no other
details given.
Incomplete outcome data addressed?
All outcomes
Yes 61 women (5%) withdrew or were lost
to follow-up, however data on miscarriage
were reported for those who withdrew due
to miscarriage. Intention-to-treat analyses
performed
Free of selective reporting? Yes All pre-specified outcomes appear to be re-
ported.
Free of other bias? Yes The study appears to be free of other
sources of bias.
People’s League 1942
Methods Randomisation and allocation concealment: “women enrolled at the antenatal clinic
were divided into two main groups by placing them alternatively on separate lists”
Blinding of outcome assessment: unclear, no information given on blinding of partici-
pants, carers or outcome assessors
Documentation of exclusion: 622 (11%) women were excluded.
Use of placebo control: no placebo given.
Participants 5644 women were recruited into the study. All women attending the antenatal clinics
and who were less than or equal to 24 weeks’ gestation and who were in ’good health’
were eligible for the study. Women who were more than 24 weeks’ gestation and women
who suffered from any disease or physical abnormality were excluded from the study.
After enrolment, women who had twin births and who miscarried at an early stage were
also excluded.
5644 women were initially enrolled in the study of which 5022 (89%) remained in the
study. Of the 622 (11%) women withdrawn from the trial, 494 were evacuated from
the London area (due to World War 2), 39 women had twin births and 89 women
miscarried at an early stage. 5022 women remained in the study and were allocated to
64Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

People’s League 1942 (Continued)
either multivitamins (n = 2510) or control (n = 2512). Women were further divided into
primiparae and multiparae, and various age groups
Interventions Women allocated to the treatment group were given daily vitamin C 100 mg, ferrous iron
0.26 g, calcium 0.26 g, minute quantities of iodine, manganese and copper, adsorbate of
vitamin B1 containing all factors of the B complex and halibut liver oil 0.36 g containing
vitamin A (52,000 IU per g) and vitamin D (2500 IU per g).
Women allocated to the control group received no placebo.
Outcomes 1. Toxaemia classified into subgroups based on: hypertension only, albuminuria with
or without hypertension, or hypertension with albuminuria (pre-eclampsia).
2. Maternal sepsis.
3. Length of gestation (categorised as less than 40 weeks, 40 weeks, and greater than
40 weeks).
4. Percentage of women breastfeeding.
5. Stillbirth.
6. Neonatal mortality (defined as death before 8 days).
7. Birthweight (pounds) (only reported for primiparae and multiparae separately).
Notes Women risk status for spontaneous and recurrent miscarriage is unclear.
Dietary intake at trial entry: “vitamin C shortage affected about half the women”.
Intention-to-treat analyses: not performed.
Compliance: unclear, no information provided.
Sample-size calculation: unclear. “It was decided that the investigation should include a
minimum of 5000 pregnant women”. No other details given.
Location: England.
Timeframe: 1938 to 1939.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? No Quasi-randomistion using alternate sepa-
rate lists.
Allocation concealment? No No allocation concealment.
Blinding?
All outcomes
Unclear No information about blinding provided.
Incomplete outcome data addressed?
All outcomes
Unclear 622 women (11%) excluded, intention to
treat analyses not performed
Free of selective reporting? Unclear Limited methodological details provided.
Free of other bias? Unclear Limited methodological details provided.
65Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Roberfroid 2008
Methods Randomisation and allocation concealment: the randomisation scheme was generated
by a computer program in permuted blocks of 4. Randomisation numbers were sealed
in opaque envelopes. At each inclusion, the consulting physician opened the next sealed
envelope and transmitted the randomisation number to a pharmacist managing the
allocation sequence and the packaging of drugs at a central location
Blinding of outcome assessment: the consulting physicians, pharmacist and women were
blinded to allocation
Documentation of exclusions: 107 women were lost to follow-up (however their preg-
nancy outcome was reported). Post randomisation 26 twins were excluded (multivitamin
group: 15; iron/folic acid group: 11 twins (including one set of triplets). Only singleton
pregnancies were included in the analysis because fetal loss and anthropometric measures
at birth in multiple pregnancies are not primarily nutrition related. 3 women died before
delivery and 1 woman underwent a therapeutic abortion
Participants 1374 women were recruited to participate, however 52 women were randomly assigned
twice for consecutive pregnancies, resulting in data for 1426 pregnancies. Women had a
pregnancy confirmed by urine testing and were randomly assigned to receive either IFA
(n = 712) or UNIMMAP (n = 714) daily until 3 months after delivery. Women were
recruited between 5 to 36 weeks’ gestation; 34.6% (n = 493) of the participants were
recruited in the first trimester of pregnancy, mean gestational age at enrolment was 17.
3 weeks (SD 7.8 wk)
Interventions UNIMMAP: vitamin A 800 µg, Vitamin D 200 IU, Vitamin E 10 mg, Vitamin B-1 1.4
mg, Vitamin B-2 1.4 mg, Niacin 18 mg, Folic acid 400 µg, Vitamin B-6 1.9 mg, Vitamin
B-12 2.6 µg, Vitamin C 70 mg, Zinc 15 mg, Iron 30 mg, Copper 2 mg, Selenium 65
µg, Iodine150 µg
IFA (control): folic acid 400 µg, Iron 60 mg.
In a case of maternal illness, appropriate treatments were provided according to national
guidelines. Severely anaemic women (haemoglobin < 70 g/L, without dyspnoea) received
ferrous sulphate (200 mg) + folic acid (0.25 mg) twice daily, for 3 months, regardless of
their allocation group. All participants also received 400 mg albendazole in the second
and third trimesters. If malaria occurred despite chemoprophylaxis, quinine (300 mg, 3
times/day) was given for 5 days. Vitamin A (200,000 IU) was given to all women after
delivery, in accordance with national recommendations
Outcomes 1. Gestational duration.
2. Birthweight, birth length, and Rohrer ponderal index at birth (weight(g)X100/
length3(cm)).
3. Low birthweight (< 2500 g).
4. Small-for-gestational age (birthweight below the 10th percentile).
5. Large-for-gestational age (birthweight above the 90th percentile of the study
population).
6. Thoracic circumference, head circumference, mid upper arm circumference.
7. Haemoglobin concentration in mothers during the third trimester, haemoglobin
and sTfR concentrations in cord blood.
8. Preterm birth (< 37 weeks’ gestation).
9. Stillbirth (delivery of an infant showing no sign of life after a gestational age of 28
weeks).
10. Perinatal death.
66Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Roberfroid 2008 (Continued)
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear. 18% of women in
each group had experienced a previous fetal loss
Women’s nutritional status is unclear, although women are presumable at risk as the
purpose of the trial is to correct multiple micronutrient deficiencies
Intention to treat analyses not performed, however the review included details of losses
to follow-up where the outcome was known
Compliance: unclear, states that there was no difference in compliance between the two
groups
Location: Burkino Faso.
Timeframe: March 2004 to October 2006.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated with permuted blocks
of 4.
Allocation concealment? Yes Randomization numbers were kept in
sealed opaque envelopes.
Blinding?
All outcomes
Yes Consulting physicians, pharmacist and
women were blinded to the intervention
Incomplete outcome data addressed?
All outcomes
No Data were reported for singletons only.
Free of selective reporting? Unclear As above - data only reported for singletons.
Free of other bias? No Some women were pregnant more than
once during the study period, however the
denominators reported are the total num-
ber of pregnancies during the study pe-
riod, not the total number of women ran-
domised, which incorrectly assumes that
each data point included is independent
from the next
67Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rumbold 2006
Methods Randomisation and allocation concealment: computer generated random number list
with balanced variable blocks and stratification for collaborating centre and gestational
age (< 18 weeks vs 18 weeks or more), allocation occurred via a central telephone ran-
domisation service. The treatment packs contained four sealed, opaque, white plastic
bottles of either the antioxidants vitamin C and vitamin E or the placebo and were
prepared by a researcher not involved in recruitment or clinical care
Blinding of outcome assessment: women, caregivers and investigators were blinded to
allocation
Documentation of exclusion: no losses to follow-up.
Use of placebo control: placebo given.
Participants 1877 women were recruited into the study. Eligible women included those: with a
nulliparous singleton pregnancy, between 14 and 22 weeks of gestation and with normal
blood pressure at the first measurement in pregnancy and again at trial entry
Women who had any of the following were excluded: known multiple pregnancy, known
potentially lethal fetal anomaly, known thrombophilia, chronic renal failure, antihy-
pertensive therapy, or specific contraindications to vitamin C or E therapy such as
haemochromatosis or anticoagulant therapy
Women were allocated to the vitamin C and E group (n = 935) or placebo (n = 935)
Interventions Women allocated to the vitamin C and E group took four coated tablets of a combination
of 250 mg of vitamin C (as ascorbic acid) and 100 IU of vitamin E (as d-alpha-tocopherol
succinate) each day from trial entry until delivery (total daily dose of vitamin C: 1000
mg; vitamin E: 400 IU)
Women were advised not to take any other antioxidant supplements, although a multi-
vitamin preparation that provided a daily intake of no more than 200 mg of vitamin C
or 50 IU of vitamin E was permitted
Outcomes 1. Pre-eclampsia.
2. A composite measure of death or serious outcomes in the infant.
3. Small-for-gestational age.
4. Serious infant complications occurring before hospital discharge.
5. For women included a composite of any of the following until six weeks
postpartum: death, pulmonary edema, eclampsia, stroke, thrombocytopenia, renal
insufficiency, respiratory distress syndrome, cardiac arrest, respiratory arrest, placental
abruption, abnormal liver function, preterm pre labor rupture of membranes, major
postpartum haemorrhage, postpartum pyrexia, pneumonia, deep-vein thrombosis, or
pulmonary embolus requiring anticoagulant therapy.
Notes Women were at low risk of spontaneous and recurrent miscarriage based on the review
criteria
The majority of women participating had a baseline dietary intake of vitamin C and E
above the Australian recommended daily amount
Intention to treat analyses performed.
Compliance: There was no difference in compliance between the vitamin group (67%)
and the placebo group (70%)
Location: Australia.
Timeframe: December 2001 and January 2005.
68Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rumbold 2006 (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated random number list.
Allocation concealment? Yes Allocation occurred via a central telephone
randomisation service. Tablets were pro-
vided in sealed opaque bottles
Blinding?
All outcomes
Yes Women, caregivers and investigators were
blinded.
Incomplete outcome data addressed?
All outcomes
Yes No losses to follow-up.
Free of selective reporting? Yes All pre-specified outcomes reported.
Free of other bias? Yes The study appears to be free of other
sources of bias.
Rumiris 2006
Methods Generation of random number sequence: a computer generated random number se-
quence
Randomisation and allocation concealment: central allocation (randomisation by an
independent third party who had no conflict of interest in the study)
Blinding of outcome assessment: treatment allocations were blinded to both the inves-
tigator and the patient until the study was finished
Documentation of exclusion: none reported.
Use of placebo control: no, comparisons were between antioxidants versus iron and folic
acid
Participants 60 women between 8 and 12 weeks gestation were eligible for randomisation (supple-
mentation group: n = 29; folic acid group: n = 31)
Setting: at the antenatal clinic of the Department of Obstetrics and Gynecology, Uni-
versity of Indonesia between March 2003 and June 2004
Eligibility criteria: pregnant women with low antioxidant status
Exclusion criteria:
1. history or current use of anti-hypertensive medication or diuretics;
2. use of vitamins C >150 mg and/or E > 75 IU per day;
3. known placental abnormalities;
4. current pregnancy as a result of in vitro fertilisation;
5. regular use of platelet active drugs or non-steroidal anti-inflammatory drugs
(NSAIDs);
6. known fetal abnormalities;
7. documented uterine bleeding within a week of screening;
8. uterine malformations;
69Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
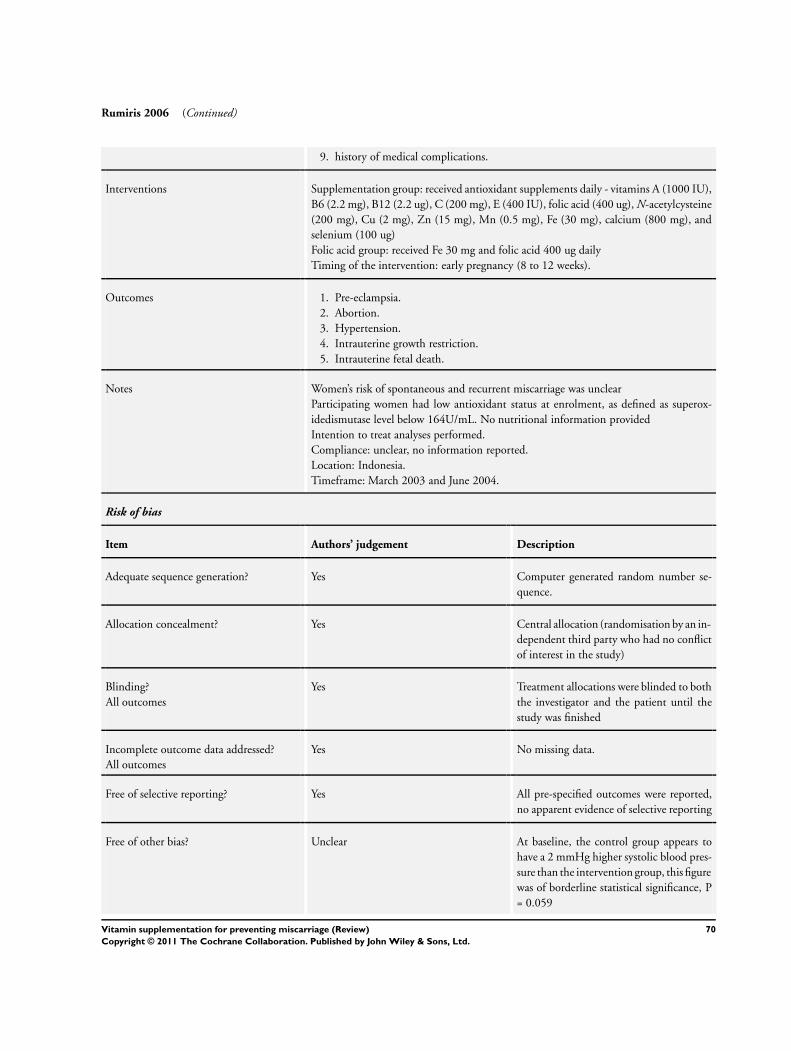
Rumiris 2006 (Continued)
9. history of medical complications.
Interventions Supplementation group: received antioxidant supplements daily - vitamins A (1000 IU),
B6 (2.2 mg), B12 (2.2 ug), C (200 mg), E (400 IU), folic acid (400 ug), N-acetylcysteine
(200 mg), Cu (2 mg), Zn (15 mg), Mn (0.5 mg), Fe (30 mg), calcium (800 mg), and
selenium (100 ug)
Folic acid group: received Fe 30 mg and folic acid 400 ug daily
Timing of the intervention: early pregnancy (8 to 12 weeks).
Outcomes 1. Pre-eclampsia.
2. Abortion.
3. Hypertension.
4. Intrauterine growth restriction.
5. Intrauterine fetal death.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Participating women had low antioxidant status at enrolment, as defined as superox-
idedismutase level below 164U/mL. No nutritional information provided
Intention to treat analyses performed.
Compliance: unclear, no information reported.
Location: Indonesia.
Timeframe: March 2003 and June 2004.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated random number se-
quence.
Allocation concealment? Yes Central allocation (randomisation by an in-
dependent third party who had no conflict
of interest in the study)
Blinding?
All outcomes
Yes Treatment allocations were blinded to both
the investigator and the patient until the
study was finished
Incomplete outcome data addressed?
All outcomes
Yes No missing data.
Free of selective reporting? Yes All pre-specified outcomes were reported,
no apparent evidence of selective reporting
Free of other bias? Unclear At baseline, the control group appears to
have a 2 mmHg higher systolic blood pres-
sure than the intervention group, this figure
was of borderline statistical significance, P
= 0.059
70Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rush 1980
Methods Randomisation and allocation concealment: unclear, women were allocated to groups
based on “random assignment”. Randomisation was stratified on pre-pregnancy weight,
weight gain during pregnancy, previous low birthweight infant and protein intake. No
other methodological details given
Blinding of outcome assessment: unclear, women were allocated to 2 forms of treatment
or control, where both treatments were given as a canned beverage and the control group
were given standard oral multivitamins. No information is given on blinding of outcome
assessors
Documentation of exclusion: 237 women (22%) were excluded.
Use of placebo control: no placebo, the control group received standard prenatal multi-
vitamin supplements
Participants 1051 women were recruited into the study. Women eligible were black, English speaking,
and not greater than 30 weeks’ gestation. They also had one of the following criteria:
low pre-pregnant weight (under 110 pounds at conception); low weight gain at the time
of recruitment; at least 1 previous low birthweight infant; a history of protein intake of
less than 50 g in the 24 hours preceding recruitment. Women were not eligible if they
were known to be seeking a termination, had specific chronic health disorders, if they
admitted to recent use of narcotics or heavy use of alcohol, or weighed >= 140 pounds
at conception.
The mean gestation at enrolment ranged from 16-18 weeks for the treatment groups.
1225 women were invited to join the study, of which 1051 (84%) consented. Of these,
237 (22%) were excluded and 814 women (77%) remained active in the study until
delivery and were allocated to one of three groups: supplement (n = 263), complement
(n = 272) or control (n = 279)
Interventions Women were randomised to 1 of 3 groups:
1. high protein supplement (daily 40 g animal protein, 470 calories, 1000 mg
calcium, 100 mg magnesium, 60 mg iron, 4 mg zinc, 2 mg copper, 150 mcg iodine,
6000 IU vitamin A, 400 IU vitamin D, 30 USPU vitamin E, 60 mg vitamin C, 3 mg
vitamin B1, 15 mg vitamin B2, 15 mg niacin, 2.5 mg vitamin B6, 1 mg pantothenic
acid, 200 mcg biotin, 350 mcg folic acid, 8 mcg vitamin B12);
2. balanced protein-energy complement (6 g animal protein, 250 mg calcium, 12
mg magnesium, 40 mg iron, 0.084 mg zinc, 0.15 mg copper, 100 mcg iodine, 4000 IU
vitamin A, 400 IU vitamin D, 60 mg vitamin C, 3 mg vitamin B1, 15 mg vitamin B2,
10 mg niacin, 3 mg vitamin B6, 1 mg pantothenic acid, 350 mcg folic acid, 3 mcg
vitamin B12);
3. control (250 mg calcium, 0.15 mg magnesium, 117 mg iron, 0.85 mg zinc, 0.15
mg copper, 100 mcg iodine, 4000 IU vitamin A, 400 IU vitamin D, 60 mg vitamin C,
3 mg vitamin B1, 2 mg vitamin B2, 10 mg niacin, 3 mg vitamin B6, 1 mg pantothenic
acid, 350 mcg folic acid, 3 mcg vitamin B12).
Women received the high protein or balanced protein-energy supplements in the format
of a drink. Women in the control group received a standard oral prenatal multivitamin
supplement
Outcomes 1. Total weight gain, average weight gain and early weight gain during pregnancy.
2. Duration of gestation (presented as cumulative rates of delivery from life tables for
each treatment group).
71Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rush 1980 (Continued)
3. Preterm birth < 37 weeks.
4. Fetal death (before < 20 weeks’ gestation and >= 20 weeks’ gestation).
5. Neonatal death (according to gestation at delivery).
6. Birthweight (mean).
7. Somatic measures of infant growth at 1 year of age.
8. Psychological measures at 1 year of age.
Notes Women’s risk of spontaneous and recurrent miscarriage is unclear, as there is no informa-
tion about concurrent medical conditions or other risk factors for miscarriage. Women
in the trial had a low caloric intake at trial entry, and unexpectedly, an adequate protein
intake. No other specific nutritional information is reported.
Sample-size calculation reported: 250 women were required in each treatment group to
show a 125 g difference in birthweight. A 25% loss to follow-up was incorporated into
the sample size.
Intention-to-treat analyses not performed.
There were 9 sets of twins amongst the three treatment groups.
Compliance: “on average, about three quarters of the prescribed amount of beverage was
probably ingested”.
Location: New York City, USA.
Timeframe: 1969 to 1976.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear No methodological details given beyond re-
porting of ’random assignment’
Allocation concealment? Unclear No methodological details given beyond re-
porting of ’random assignment’
Blinding?
All outcomes
Unclear Unlkely as women were given canned bev-
erages or multivitamins
Incomplete outcome data addressed?
All outcomes
Unclear 237 women (22%) excluded, no intention
to treat analysis.
Free of selective reporting? Unclear Unclear if all pre-specified outcomes re-
ported.
Free of other bias? Unclear Limited methodological details provided.
72Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schmidt 2001
Methods Randomisation and allocation concealment: unclear, women were “randomly assigned
on an individual basis, to double-blind, weekly supplementation until delivery”
Blinding of outcome assessment: unclear, double blind stated in text but no details given
Documentation of exclusion: 42 women (17%) were lost to follow-up and excluded
Use of placebo control: control tablets containing iron and folic acid were given
Participants 243 women were recruited into this study. Pregnant women between 16 and 20 weeks’
gestation, aged between 17 and 35 years old, with a parity < 6 and haemoglobin level
between 80-140 g/l, were eligible for this study. Women were randomised to receive
either vitamin A plus iron and folic acid (n = 122) or iron and folic acid only (n = 121).
Of these 22 (18%) and 20 (17%) women in vitamin A plus iron and folic acid and the
iron and folic acid groups respectively, dropped out between enrolment and the follow-
up at 4 months
Interventions Women were randomised to a weekly supplementation with 120 mg ferrous sulfate and
500 mcg folic acid, with or without vitamin A (2400 retinol equivalents). Women were
asked to take the trial tablets from between 16 and 20 weeks’ gestation until birth
Outcomes 1. Stillbirth.
2. Concentrations of haemoglobin, serum ferritin and serum transferrin receptors, at or
near term.
3. Concentrations of iron and vitamin A in breast milk.
4. Haemoglobin and serum vitamin A concentrations in the mother and infant at 4
months postpartum.
5. General health, growth and development measures in the first year of life
Notes Women risk status for spontaneous and recurrent miscarriage is unclear.
At baseline, between 13% and 17% of women had marginal vitamin A deficiency 44%
to 50% of women were anaemic.
Sample-size calculation performed allowing for a 50% drop-out during the study period.
Intention-to-treat analyses were not performed.
Compliance: adherence to the tablet intake was assessed through interview during a
postnatal home visit, which revealed that the median tablet intake was 50 tablets (i.e. 25
weeks), while only 17% of the subjects took more than 90 tablets.
Location: Indonesia.
Serial publications of this data report different denominators.
Time frame: November 1997 to May 1998.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear No information provided about sequence
generation.
Allocation concealment? Unclear Women were ’randomly assigned on an in-
dividual basis’ but no other details given
73Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schmidt 2001 (Continued)
Blinding?
All outcomes
Unclear Double blind used in the text but not de-
tails provided.
Incomplete outcome data addressed?
All outcomes
Unclear 42 women (17%) were lost to follow-up
and excluded, no intention to treat analyses
performed
Free of selective reporting? No Serial publications of this study report dif-
ferent denominators
Free of other bias? Unclear Limited methodological details provided.
Spinnato 2007
Methods Generation of random number sequence: the randomisation sequence was constructed
by the data coordinating centre (DCC) as permuted blocks of random size, stratified
by clinical centre, and implemented via a program residing on the clinical centres study
computer
Randomisation and allocation concealment: central allocation
Blinding of outcome assessment: all clinicians and clinical investigators were blinded to
group assignment
Documentation of exclusion: none reported.
Use of placebo control: placebo control.
Participants 739 eligible women between 120/7 and 196/7 weeks of gestation were enrolled in the
study (treatment: 371; placebo: 368)
Setting: four Brazilian clinical centres: one primary clinical centre (Recife) and 3 addi-
tional clinical sites (Campinas, Botucatu, and Porto Alegre); each site’s major teaching
hospital serves a primarily urban low-income population
Eligibility criteria: women between 120/7 and 196/7 weeks of gestation and diagnosed
with nonproteinuric chronic hypertension or a prior history of pre-eclampsia in their
most recent pregnancy that progressed beyond 20 weeks’ gestation
Exclusion criteria:multifetal gestation, allergy to vitamin C or vitamin E, requirement for
aspirin or anticoagulant medication, 24-hour urinary protein ≥ 300 mg, pre-pregnancy
diabetes mellitus, known fetal anomaly incompatible with life
Loss to follow-up: 32 women (treatment 16; placebo 16).
Interventions Intervention group: daily treatment with both vitamin C (1000 mg) and E (400 IU)
until delivery or until the diagnosis of pre-eclampsia
Control group: daily placebo until delivery or until the diagnosis of pre-eclampsia
Timing of the intervention: between 120/7 and 196/7 weeks of gestation.
Outcomes 1. Pre-eclampsia (women were followed through the 14th day postpartum for the
occurrence of pre-eclampsia).
2. Severity of pre-eclampsia.
3. Gestational hypertension.
4. Abruptio placentae.
5. Premature rupture of membranes.
74Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Spinnato 2007 (Continued)
6. Preterm birth.
7. Small-for-gestational age.
8. Low birthweight infant.
Notes 25 inclusion/exclusion criteria violations (23 enrolled outside 12-19 weeks’ gestation; 2
twin gestations - one lost to spontaneous abortions, one delivered liveborn in treatment
group); all 25 women remained in their assigned study groups
26 women had early treatment terminations (treatment 19; placebo 7), but remained in
follow-up
Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear.
Intention to treat analyses performed.
Compliance: average compliance was 85%, and similar between treatment groups
Location: Brazil.
Timeframe: July 2, 2003 and November 23, 2006.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated sequence number.
Allocation concealment? Yes Central allocation.
Blinding?
All outcomes
Yes All clinicians and clinical investigators were
blinded to group assignment
Incomplete outcome data addressed?
All outcomes
Yes Small numbers of missing data, balanced
across groups (32 women; treatment 16;
placebo 16)
Free of selective reporting? Yes All pre-specified outcomes were reported,
no apparent evidence of selective reporting
Free of other bias? Yes The study appears to be free of other
sources of bias.
75Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Steyn 2003
Methods Randomisation and allocation concealment: “randomisation was undertaken by com-
puter-generated numbers”. Roche Pharmaceutical supplied numbered containers with
either vitamin C or matching placebo, and they retained the study code until completion
of the study. No other methodological details given
Blinding of outcome assessment: “double blind” stated, Roche Pharmaceuticals retained
the code until completion of the study
Documentation of exclusion: none reported.
Use of placebo control: placebo control.
Participants 200 women were recruited into the study. Women with a history of a previous mid-
trimester abortion (defined as spontaneous expulsion of the uterine contents between
13 and 26 weeks’ gestational age), or previous preterm labour, and less than 26 weeks’
gestation were eligible and invited to participate. Women with iatrogenic causes of their
previous preterm labour such as previous induction of labour before term for severe pre-
eclampsia, were excluded. 203 consecutive women were approached, of which 200 (98.
5%) consented and were randomised to either vitamin C (n = 100) or placebo (n = 100)
. No losses to follow-up were reported
Interventions Twice daily tablet of either 250 mg vitamin C or placebo, from trial entry until 34 weeks’
gestation. All women were tested for bacterial vaginosis and all women with positive
cultures for Mycoplasma hominis (and between 22 and 32 weeks’ gestation) were treated
with erythromycin for 7 days
Outcomes 1. Preterm labour, defined as spontaneous onset of labour and delivery before 37
completed weeks.
2. The secondary outcome was perinatal outcome, a composite endpoint including
birthweight, gestational age at delivery, perinatal mortality, duration of admission in
the neonatal intensive care unit and neonatal complications.
The age of fetal viability was considered to be 28 weeks’ gestation
Notes Results are from an interim analysis performed when 100 participants were recruited
into each arm. Recruitment was stopped after the interim analysis revealed few differ-
ences between the two groups. Unclear if there was a sample-size calculation performed.
Women’s risk profile spontaneous and recurrent miscarriage is unclear, although they are
clearly at high risk of preterm birth. It is also unclear if multiple births were included.
6% of women had an inadequate dietary intake of vitamin C, defined as an intake <
67% of the recommended dietary allowance (70 mg per day).
Compliance: women were requested to bring the containers to each visit and the remain-
ing tablets were counted to improve and control compliance; however, no compliance
data were reported.
Country: South Africa.
Timeframe: unclear.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated sequence number.
76Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Steyn 2003 (Continued)
Allocation concealment? Yes Roche pharmaceuticals supplied numbered
study containers and kept the study code
until completion of the study
Blinding?
All outcomes
Unclear Double blind stated in the text but not de-
tails given.
Incomplete outcome data addressed?
All outcomes
Yes No losses to follow-up reported.
Free of selective reporting? Unclear Recruitment stopped after an interim anal-
ysis.
Free of other bias? No Results are from an interim analysis per-
formed when 100 participants were re-
cruited into each arm
Taylor 1982
Methods Generation of random number sequence: not reported.
Randomisation and allocation concealment: women were randomised, no further details
given
Blinding of outcome assessment: not reported.
Documentation of exclusion: no losses to follow-up reported, however three women
were delivered before 37 weeks and were therefore excluded from the study
Use of placebo control: no.
Participants 48 healthy pregnant women at 12 weeks’ gestation (intervention group: 21; control
group: 24)
Eligibility criteria: healthy pregnant women with no adverse medical or obstetric history
Loss to follow-up: no.
Interventions Intervention group: 325 mg of ferrous sulphate and 350 µg of folic acid to be taken daily
throughout the remainder of pregnancy
Control group: the women in non-therapy group were not given any supplements
Timing of the intervention: from 12 weeks’ gestation until delivery
Outcomes 1. Serum ferritin concentration.
2. Mean cell volume.
3. Haemoglobin concentration.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear.
Intention to treat analyses: no, 3 women excluded.
Compliance: unclear, no information reported.
Location: Scotland.
Timeframe: unclear.
77Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Taylor 1982 (Continued)
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not reported.
Allocation concealment? Unclear Women were randomised, no further de-
tails given.
Blinding?
All outcomes
Unclear Not reported.
Incomplete outcome data addressed?
All outcomes
Yes No missing data; three women were deliv-
ered before 37 weeks and were therefore ex-
cluded from the study
Free of selective reporting? Yes All pre-specified outcomes were reported,
no apparent evidence of selective reporting
Free of other bias? Unclear Limited methodological details provided.
The Summit 2008
Methods Generation of random number sequence: computer-generated number; 262 clustered
unit of randomisations (all pregnant women served by the same midwife received sup-
plements with the same midwife identification number)
Randomisation and allocation concealment: central allocation
Blinding of outcome assessment: all study scientists and personnel, government staff,
and enrollees were unaware of the allocation
Documentation of exclusion: 1748 loss to follow-up before delivery (IFA: 853; MMN:
895); 1128 loss to follow-up after delivery (IFA: 553; MMN: 575). 10,549 pregnant
women excluded post-randomisation because of trial termination (IFA group: 5057;
MMN group: 5492)
Use of placebo control: no placebo, comparisons were between multiple micronutrients
and iron and folic acid
Participants 41,839 pregnant women of any gestational age living on Lombok, Nusa Tenggara Barat
Province, Indonesia. Women were allocated to iron and folic acid (n = 20,543) or multiple
micronutrient (n = 21,296)
Interventions MMN group: the MMN was the UNIMMAP formulation containing 30 mg iron
(ferrous fumarate) and 400 ug folic acid along with 800 ug retinol (retinyl acetate),
200 IU vitamin D (ergocalciferol), 10 mg vitamin E (alpha tocopherol acetate), 70 mg
ascorbic acid, 1.4 mg vitamin B1 (thiamine mononitrate), 18 mg niacin (niacinanide)
, 1.9 mg vitamin B6 (pyridoxine), 2.6 ug vitamin B12 (cyanocobalamin), 15 mg zinc
(zinc gluconate), 2 mg copper, 65 ug selenium, and 150 ug iodine - one capsule daily
up to 3 months after birth
IFA group: the IFA contained 30 mg iron (ferrous fumarate) and 400 ug folic acid - one
78Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The Summit 2008 (Continued)
capsule daily up to 3 months after birth
Timing of the intervention: any time during pregnancy.
Outcomes 1. Early infant mortality (deaths until 90 days postpartum).
2. Neonatal mortality.
3. Fetal loss (abortions and stillbirths).
4. Low birthweight.
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear. However, 30% of women in each group had
an mid upper arm circumference < 23.5cm, which was used as an indicator of women
being undernourished
Intention to treat analyses performed.
Compliance: median compliance was 85%, there was no difference between treatment
groups in compliance
Location: Indonesia.
Timeframe: July 1, 2001, and April 1, 2004.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated number.
Allocation concealment? Yes Central allocation.
Blinding?
All outcomes
Yes All study scientists and personnel, govern-
ment staff, and enrollees were unaware of
the allocation
Incomplete outcome data addressed?
All outcomes
No Loss to follow-up: 1748 loss to follow-up
before delivery (IFA: 853; MMN: 895);
1128 loss to follow-up after delivery (IFA:
553; MMN: 575)
Post-randomisation exclusion: 10,
549 pregnant women excluded because of
trial termination (IFA group: 5057; MMN
group: 5492)
Free of selective reporting? Yes All pre-specified outcomes were reported,
no apparent evidence of selective reporting
Free of other bias? Yes The study appears to be free of other
sources of bias.
79Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
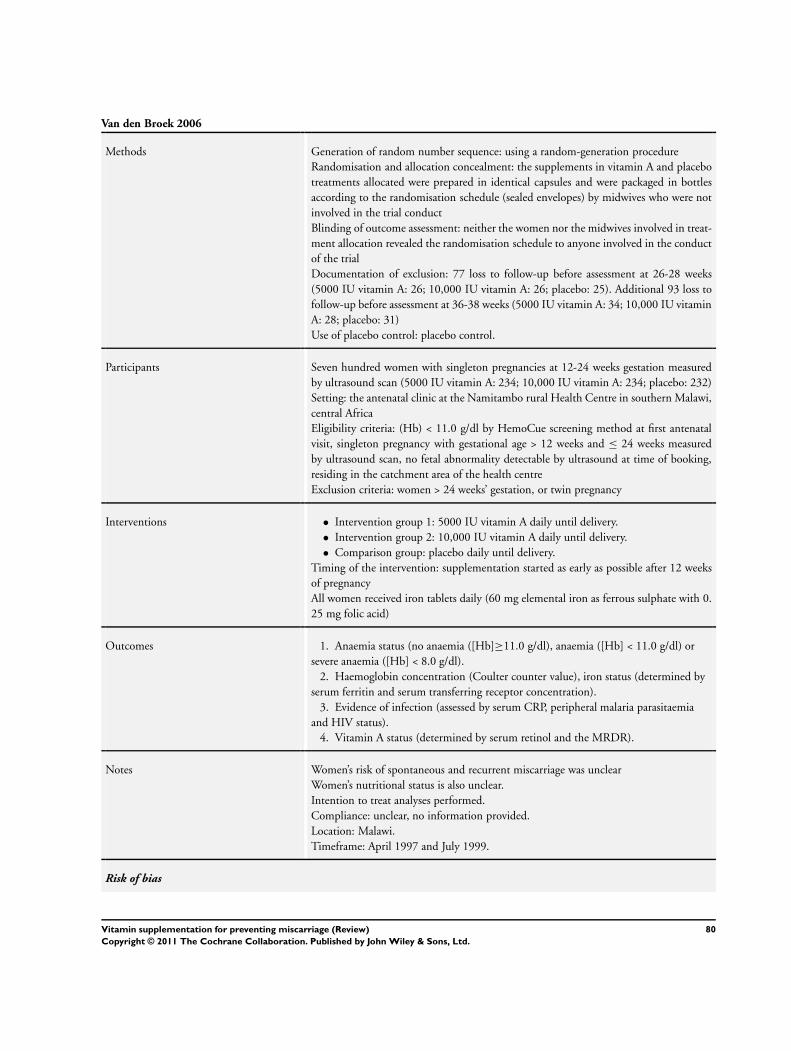
Van den Broek 2006
Methods Generation of random number sequence: using a random-generation procedure
Randomisation and allocation concealment: the supplements in vitamin A and placebo
treatments allocated were prepared in identical capsules and were packaged in bottles
according to the randomisation schedule (sealed envelopes) by midwives who were not
involved in the trial conduct
Blinding of outcome assessment: neither the women nor the midwives involved in treat-
ment allocation revealed the randomisation schedule to anyone involved in the conduct
of the trial
Documentation of exclusion: 77 loss to follow-up before assessment at 26-28 weeks
(5000 IU vitamin A: 26; 10,000 IU vitamin A: 26; placebo: 25). Additional 93 loss to
follow-up before assessment at 36-38 weeks (5000 IU vitamin A: 34; 10,000 IU vitamin
A: 28; placebo: 31)
Use of placebo control: placebo control.
Participants Seven hundred women with singleton pregnancies at 12-24 weeks gestation measured
by ultrasound scan (5000 IU vitamin A: 234; 10,000 IU vitamin A: 234; placebo: 232)
Setting: the antenatal clinic at the Namitambo rural Health Centre in southern Malawi,
central Africa
Eligibility criteria: (Hb) < 11.0 g/dl by HemoCue screening method at first antenatal
visit, singleton pregnancy with gestational age > 12 weeks and ≤ 24 weeks measured
by ultrasound scan, no fetal abnormality detectable by ultrasound at time of booking,
residing in the catchment area of the health centre
Exclusion criteria: women > 24 weeks’ gestation, or twin pregnancy
Interventions • Intervention group 1: 5000 IU vitamin A daily until delivery.
• Intervention group 2: 10,000 IU vitamin A daily until delivery.
• Comparison group: placebo daily until delivery.
Timing of the intervention: supplementation started as early as possible after 12 weeks
of pregnancy
All women received iron tablets daily (60 mg elemental iron as ferrous sulphate with 0.
25 mg folic acid)
Outcomes 1. Anaemia status (no anaemia ([Hb]≥11.0 g/dl), anaemia ([Hb] < 11.0 g/dl) or
severe anaemia ([Hb] < 8.0 g/dl).
2. Haemoglobin concentration (Coulter counter value), iron status (determined by
serum ferritin and serum transferring receptor concentration).
3. Evidence of infection (assessed by serum CRP, peripheral malaria parasitaemia
and HIV status).
4. Vitamin A status (determined by serum retinol and the MRDR).
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear
Women’s nutritional status is also unclear.
Intention to treat analyses performed.
Compliance: unclear, no information provided.
Location: Malawi.
Timeframe: April 1997 and July 1999.
Risk of bias
80Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Van den Broek 2006 (Continued)
Item Authors’ judgement Description
Adequate sequence generation? Yes Random-generation procedure used.
Allocation concealment? Yes The vitamin A and placebo treatments al-
located were prepared in identical capsules
and packaged in bottles according to the
randomisation schedule (sealed envelopes)
by midwives who were not involved in the
trial conduct
Blinding?
All outcomes
Yes Neither the women nor the midwives in-
volved in treatment allocation revealed the
randomisation schedule to anyone involved
in the conduct of the trial
Incomplete outcome data addressed?
All outcomes
No 77 loss to follow-up before assessment at
26-28 weeks (5000 IU vitamin A: 26; 10,
000 IU vitamin A: 26; placebo: 25). Ad-
ditional 93 loss to follow-up before assess-
ment at 36-38 weeks (5000 IU vitamin A:
34; 10,000 IU vitamin A: 28; placebo: 31)
Free of selective reporting? Yes All pre-specified outcomes were reported,
no apparent evidence of selective reporting
Free of other bias? Yes The study appears to be free of other
sources of bias.
Villar 2009
Methods Generation of random number sequence: no sequence generation details available
Randomisation and allocation concealment: central allocation (randomisation was per-
formed by the statisticians of the British VIP Trial)
Blinding of outcome assessment: “double blind” stated.
Documentation of exclusion: 10 women (treatment 6; placebo 4), and 29 infants (treat-
ment 13, placebo 16) were lost to follow-up
Use of placebo control: placebo control.
Participants 1365 women between14-22 gestational age agreed to participate and were randomised
(vitamins group: 687; placebo group: 678)
Setting: antenatal clinics located in Nagpur, India; Lima and Trujillo, Peru; Cape Town,
South Africa; and Ho Chi Minh City, Viet Nam which served populations with low so-
cial-economic status and had evidence of overall low nutritional status, between October
2004 and December 2006
Eligibility criteria: pregnant women considered high risk for pre-eclampsia (chronic
hypertension, renal disease, pre-eclampsia-eclampsia in the pregnancy preceding the
index pregnancy requiring delivery before 37 weeks’ gestation, HELLP syndrome in any
81Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Villar 2009 (Continued)
previous pregnancy, pre-gestational diabetes, primiparous with a body mass index > 30
kg/m2, history of medically indicated preterm delivery, abnormal uterine artery Doppler
waveforms and women with antiphospholipid syndrome), multifetal gestation. Women
ingesting medications with aspirin-like compounds were not excluded
Exclusion criteria: women ingesting vitamin supplements that contained ≥ 200 mg of
vitamin C and/or ≥ 50 IU of vitamin E and women receiving warfarin
Interventions Intervention group: received 1000 mg vitamin C and 400 IU of vitamin E daily until
delivery
Comparison group: received placebo daily until delivery.
Timing of the intervention: between 14 and 22 weeks’ gestation
Outcomes 1. Pre-eclampsia.
2. Eclampsia.
3. Placental abruption.
4. Low birthweight (LBW) (< 2500 g).
5. Small-for-gestational age (< 10th centile of the WHO recommended standard).
6. Intrauterine or neonatal death before hospital discharge.
7. Preterm delivery (< 37 weeks).
8. Early preterm delivery (< 34 weeks).
9. Very LBW (< 1500 g).
10. ≥ 7 days in the neonatal intensive care unit.
11. Congenital malformations.
Pre-eclampsia information was unavailable for 14 women in the vitamins and 9 in the
placebo group
There were data from 81 supplemented (11.8%) and 100 placebo-treated (14.7%)
women with multiple pregnancies, for whom newborn outcomes were considered sepa-
rately
Notes Women’s risk of spontaneous and recurrent miscarriage was unclear. Women at high risk
of pre-eclampsia were included but data on fetal loss was not reported separately for this
group
No specific information on women’s nutritional status is included; however, the paper
states that the trial was conducted in populations with ’documented low nutritional
status’
Intention to treat analyses performed.
Compliance: Median compliance was 87%, and was similar between the treatment
groups
Location: Antenatal clinics in India, Peru, South Africa and Viet Nam
Timeframe: October 2004 and December 2006.
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Randomisation sequence blocked by centre
in groups of 2 to ten10 individuals
82Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
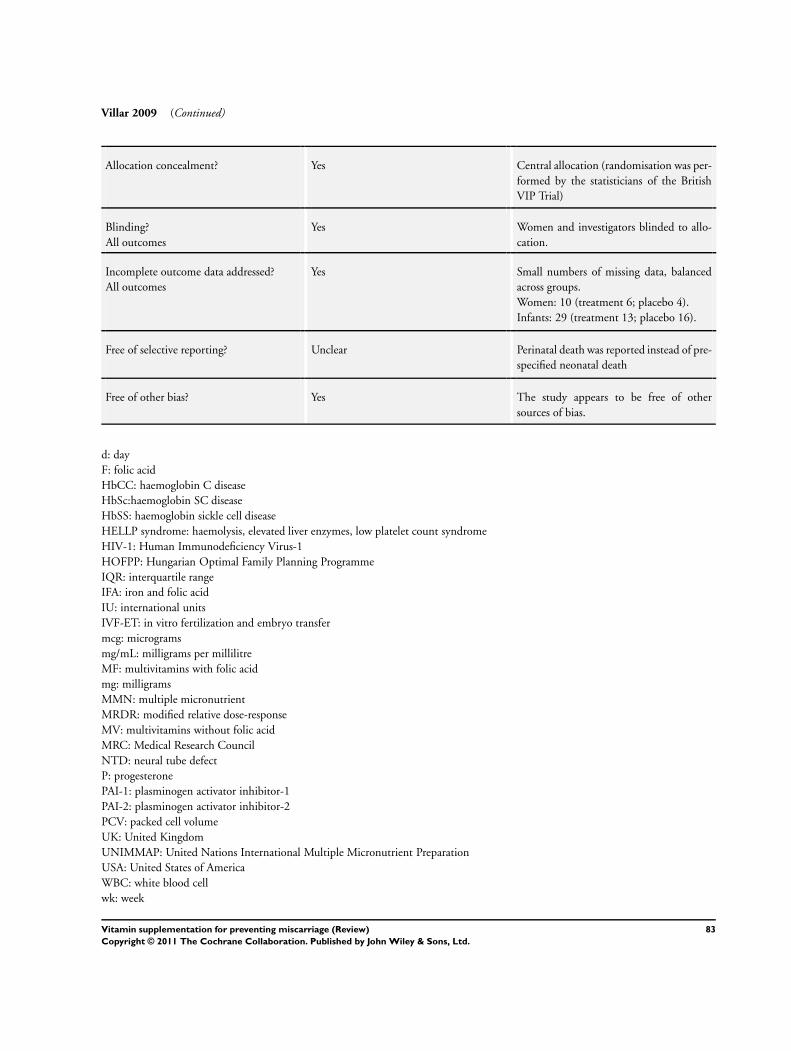
Villar 2009 (Continued)
Allocation concealment? Yes Central allocation (randomisation was per-
formed by the statisticians of the British
VIP Trial)
Blinding?
All outcomes
Yes Women and investigators blinded to allo-
cation.
Incomplete outcome data addressed?
All outcomes
Yes Small numbers of missing data, balanced
across groups.
Women: 10 (treatment 6; placebo 4).
Infants: 29 (treatment 13; placebo 16).
Free of selective reporting? Unclear Perinatal death was reported instead of pre-
specified neonatal death
Free of other bias? Yes The study appears to be free of other
sources of bias.
d: day
F: folic acid
HbCC: haemoglobin C disease
HbSc:haemoglobin SC disease
HbSS: haemoglobin sickle cell disease
HELLP syndrome: haemolysis, elevated liver enzymes, low platelet count syndrome
HIV-1: Human Immunodeficiency Virus-1
HOFPP: Hungarian Optimal Family Planning Programme
IQR: interquartile range
IFA: iron and folic acid
IU: international units
IVF-ET: in vitro fertilization and embryo transfer
mcg: micrograms
mg/mL: milligrams per millilitre
MF: multivitamins with folic acid
mg: milligrams
MMN: multiple micronutrient
MRDR: modified relative dose-response
MV: multivitamins without folic acid
MRC: Medical Research Council
NTD: neural tube defect
P: progesterone
PAI-1: plasminogen activator inhibitor-1
PAI-2: plasminogen activator inhibitor-2
PCV: packed cell volume
UK: United Kingdom
UNIMMAP: United Nations International Multiple Micronutrient Preparation
USA: United States of America
WBC: white blood cell
wk: week
83Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Baumslag 1970 Onset of supplementation was > 20 weeks’ gestation.
Women were supplemented with either iron, iron and folic acid or iron, folic acid and vitamin B12 from
“after the 24th week of pregnancy”
Biswas 1984 Unclear of the gestational age at which women entered the trial
Blot 1981 Onset of supplementation was > 20 weeks’ gestation.
Supplementation with either iron and folic acid or iron alone occurred “at the end of the 6th month of
pregnancy”. Unclear if women were randomised to the treatment groups
Chanarin 1968 Onset of supplementation was > 20 weeks’ gestation.
Women were given a folic acid supplement after the 20th week of pregnancy. Abortion was reported according
to folic acid status at 15 weeks, prior to supplementation
Colman 1974 Onset of supplementation was > 20 weeks’ gestation.
Women were supplemented “during the final month of pregnancy”. Outcomes reported included folic acid
red cell and serum folic acid concentration and haemoglobin concentration
Coutsoudis 1999 Onset of supplementation was > 20 weeks’ gestation.
Women were given vitamin A and beta-carotene “during the third trimester of pregnancy”
Dawson 1962 Onset of supplementation was > 20 weeks’ gestation.
Women were supplemented with folic acid “on or after the 28th week”. Group allocation was not done
randomly. Reported outcomes include incidence of folic acid deficiency and megaloblastic anaemia, and
haemoglobin concentration
Edelstein 1968 Onset of supplementation was > 20 weeks’ gestation.
Supplementation was started at the 28th week of pregnancy. Outcomes reported included serum folate activity
and serum folate, urinary formiminoglutamic acid, serum vitamin B12, mean haemoglobin and haematocrit
values
Ferguson 1955 Only 24 (9%) of the 269 women in the trial began to participate before 15 weeks’ gestation and outcomes
not reported separately according to gestation at enrolment
Feyi-Waboso 2005 Onset of supplementation was 20 or more weeks’ gestation.
Fletcher 1971 No inclusion/exclusion criteria reported, unclear of gestational age at enrolment to the study, reports combined
outcomes for “antepartum and threatened or complete abortion” and “stillbirth or neonatal death or congenital
malformation” (not reported separately)
Giles 1971 Onset of supplementation was > 20 weeks’ gestation for a large proportion of the participants.
4 groups in the study, two of which involved supplementation after 20 weeks’ gestation. Results were not
reported separately between groups
84Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Hampel 1974 Unclear of the gestational age at which women entered the trial
Hankin 1966 No main outcomes reported.
Supplementation was from “approximately 20 weeks”, no clinically relevant outcomes, outcomes relating to
vitamin C status in plasma and breast milk reported
Hibbard 1968 No main outcomes reported.
Biochemical measures of blood folate status reported.
Hunt 1984 All women received a multivitamin in addition to the zinc supplement or placebo
Huybregts 2009 Both groups received a multivitamin supplement (same vitamin content in each group)
Laurence 1981 No main outcomes or pregnancy loss outcomes reported. Miscarriage reported in those women where there
was a neural tube defect, but not in all women according to treatment group
Lira 1989 No main outcomes reported.
Biochemical measures of iron and folate status reported.
Lumeng 1976 Unclear gestational age at enrolment, 5 women were excluded due to abortion, premature labour, inadequate
dietary records or missing more than 3 prenatal visits. Exclusions were not reported by group allocation.
Outcomes related to maternal and fetal plasma levels of pyridoxal 5’-phosphate and coenzyme saturation of
aspartate aminotransferase and alanine aminotransferase in maternal erthrocytes were reported
Marya 1981 Onset of supplementation was > 20 weeks’ gestation.
Women were supplemented with vitamin D “throughout the 3rd trimester”
Meirinho 1987 No clinical outcomes reported.
Maternal plasma concentrations of trophoblastic protein SP1 were reported
Metz 1965 Onset of supplementation was > 20 weeks’ gestation.
Women were supplemented with either iron or iron and folic acid, or iron, folic acid and vitamin B12.
Supplementation was started after the 24th week of pregnancy
Mock 2002 No main outcome reported.
Women were enrolled in either early or late pregnancy. Biochemical measures of biotin status reported
Moldenhauer 2002 No main outcomes reported.
Unclear if this is a cohort study or randomised trial. Women in this study were participating in a randomised
placebo controlled trial of calcium supplementation, and completed a dietary assessment at 12-21 weeks’
gestation and 29-31 weeks’ gestation. Unclear whether all women took a standard prenatal multivitamin or just
women in the placebo group. Results are presented according to “teens”, “twins” and “singleton” pregnancies,
not according to whether women took the supplement or not. Outcomes reported included dietary intakes of
vitamin C and E (with and without the contribution of the prenatal vitamin supplement)
Owen 1966 Onset of supplementation was > 20 weeks’ gestation.
Women supplemented with oral vitamin K1 “several days before delivery”
85Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Ross 1985 Unclear about content of vitamin supplements.
Women were supplemented with high or low ’bulk’ dietary supplements with vitamins added; however, the
vitamin supplements added were not specified
Schuster 1984 Unclear of gestation at enrolment to the trial.
No pregnancy loss outcomes reported.
Semba 2001 No main outcomes reported.
Women enrolled between 18 and 28 weeks’ gestation, no clinical outcomes reported, only haemoglobin and
plasma erythropoietin concentrations
Shu 2002 Both groups received a multivitamin (same vitamin content in both groups)
Smithells 1981 Non-randomised study of periconceptional multivitamin supplementation for the prevention of neural tube
defects
Suharno 1993 No main outcomes reported.
Anaemic pregnant women were enrolled between 16 and 24 weeks’ gestation. The only clinical outcome
reported was the percentage of women with anaemia following treatment with a combination of vitamin A
and iron or placebo
Tanumihardjo 2002 No main outcomes reported.
Mean gestation at enrolment was 17.6 weeks, no clinical outcomes reported, markers of vitamin A and iron
status reported
Thauvin 1992 No main outcomes reported.
Women were supplemented from 3 months’ gestation, data on pregnancy outcomes including spontaneous
abortion were collected but not reported
Trigg 1976 Unclear of gestation at enrolment to the trial.
Ulrich 1999 Non-randomised study.
Observational cohort study of folic acid users, randomised to different doses of folic acid, but no controls
Villamor 2002 No main outcomes reported.
Women enrolled between 12 and 27 weeks’ gestation, no pregnancy loss or main outcomes reported, only
reports measures of weight gain during pregnancy
Vutyavanich 1995 No main outcomes reported.
Women were enrolled in the study if they were less than 17 weeks’ gestation; however, no pregnancy loss or
main outcomes were reported, only measures of nausea and vomiting
86Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of studies awaiting assessment [ordered by study ID]
Chelchowska 2004
Methods Unlcear.
Participants 138 pregnant women recruited from the Mother and Child Institute Hospital, Warsaw, Poland. Inclusion criteria
included: maternal good health, no smoking, normal pregnancy, no vitamin and mineral supplementation prior to
12 weeks’ gestation, and no fetal development defects
Interventions Women took either the VIBOVIT®mama preparation or a placebo from 12 weeks’ gestation until delivery. The
VIBOVIT®mama preparation consisted of: vitamin D (400 IU), vitamin A (2000 IU), beta-carotene (3000 mcg),
vitamin E (18 IU), zinc (15 mg), copper (2 mg) and selenium (20 mcg)
Outcomes Lipid peroxidation and activity of superoxide dismutase and selenium-dependent glutathione peroxidase in blood
samples taken from the mother and the cord blood of the infant
Notes Translated from Polish. Appears to be the same study as the Kubik 2004 paper, but reporting biochemical outcomes
Frenzel 1956
Methods Unclear.
Participants Unclear.
Interventions Unclear.
Outcomes Unclear.
Notes A copy of the paper could not be located.
Kubik 2004
Methods Unclear, described in the abstract as: “healthy pregnant women were divided by a double blinded trial into a test
group taking vitamin and mineral supplementation and a control group taking placebo”
Participants 138 pregnant women recruited from the Mother and Child Institute Hospital, Warsaw, Poland. Inclusion criteria
included: maternal good health, no smoking, normal pregnancy, no vitamin and mineral supplementation prior to
12 weeks’ gestation, and no fetal development defects
Interventions Women took either the VIBOVIT®mama preparation or a placebo from 12 weeks’ gestation until delivery. States
in the abstract that women took a vitamin and mineral supplement (VIBOVIT®mama) which contained zinc (15
mg), copper (2 mg) and selenium (20 mcg)
Outcomes Pregnancy induced hypertension, mode of birth, birthweight, Apgar scores, and other outcomes related to the ’course
of pregnancy and delivery’, biochemical measures of antioxidant status
Notes Translated from Polish. Actual numbers are not presentation, only %, and it is unclear how many women were
allocated to each group at the onset of the study
87Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of ongoing studies [ordered by study ID]
Fall 2007
Trial name or title Mumbai Maternal Diet Study: randomised controlled trial of micronutrient-dense food before and during
pregnancy to prevent low birthweight
Methods Randomised controlled trial.
Participants Inclusion criteria:
1. women living in slum communities in Bandra and Khar districts of Mumbai served by the Women of
India Network (WIN) primary health care clinics;
2. women who wish to join;
3. married;
4. aged 15 to 35 years;
5. not pregnant at recruitment;
6. not using any PERMANENT form of contraception;
7. intending to have more children;
8. planning any future deliveries in Mumbai.
Exclusion criteria:
1. women living outside the study area;
2. non-married women;
3. women outside the age range specified;
4. women currently pregnant (these may become eligible after delivery);
5. women who have undergone sterilisation surgery, or whose husbands have had a vasectomy;
6. women definitely not planning further pregnancies;
7. women definitely planning further deliveries outside Mumbai.
Interventions Women who are not pregnant, but are planning to have further children, will be recruited and randomised to
one of four groups, to receive one of two interventions: a daily food-based supplement made from vegetables,
fruit, and milk, of differing micronutrient content. Supplementation will be supervised. Field staff will record
menstrual dates, in order to detect pregnancy as early as possible. Women who become pregnant will have
investigations during pregnancy, including blood samples and ultrasound scans
Outcomes 1. Birthweight.
2. Infant mortality.
3. Maternal micronutrient status.
4. Maternal infection load and immune status.
5. Fetal losses (miscarriages and stillbirths).
6. Newborn body composition.
7. Newborn immune function.
Starting date 09/01/2006.
Contact information Dr Caroline Fall
MRC Epidemiology Resource Centre
Southampton General Hospital
University of Southampton
Tremona Road
Notes Anticipated end date: 31/03/2010, listed as completed.
88Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Johns 2004
Trial name or title The effect of antioxidant supplementation on women with threatened miscarriage
Methods Randomised controlled trial.
Participants 580 women who present with first trimester bleeding.
Interventions Vitamin C 1000 mg and Vitamin E 400 IU
versus placebo.
Outcomes 1. Incidence of miscarriage.
2. Late miscarriage.
3. Pre-term labour.
4. Pre-term pre-labour rupture of the membranes.
5. Fetal growth restriction.
6. Pre-eclampsia.
Starting date 01/03/2004.
Contact information Dr Jemma Johns
UCLH/UCL Research & Development Governance Committee
Research and Development Directorate
University College London Hospitals NHS Trust
1st Floor, Maple House
149 Tottenham Court Road
Notes Listed as completed.
Sezikawa 2007
Trial name or title Vitamin C and E Supplementation in Pregnant Women With Low Antioxidant Status
Methods Randomised controlled trial.
Participants Pregnant women with low antioxidant status at 10-12 weeks gestation age
Inclusion criteria:
• agree to consent form, and consent to protocol of research;
• Known healthy singleton 6-10 weeks pregnant women.
Exclusion criteria:
• blood pressure > 135/85;
• proteinuria;
• history or current use of anti-hypertensive medication or diuretics;
• use of vitamins C > 150 mg and/or E > 75 IU per day;
• pregestational diabetes;
• known placental abnormalities;
• current pregnancy is a result of in vitro fertilisation;
• regular use of platelet active drugs or non-steroidal anti-inflammatory drugs;
• known fetal abnormalities;
• documented uterine bleeding within a week of screening;
89Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sezikawa 2007 (Continued)
• uterine malformations;
• history of medical complications;
• illicit drug or alcohol abuse during current pregnancy;
• intent to deliver elsewhere;
• known psychologic problems;
• participating in another interventional study.
Interventions Vitamin C 1000 mg and E 400 IU versus placebo.
Outcomes 1. Pre-eclampsia.
2. Other adverse pregnancy outcomes.
Starting date October 2006.
Contact information Akihiko Sekizawa, MD, PhD
Showa University School of Medicine
Notes Listed as completed, last updated February 16th, 2010.
90Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
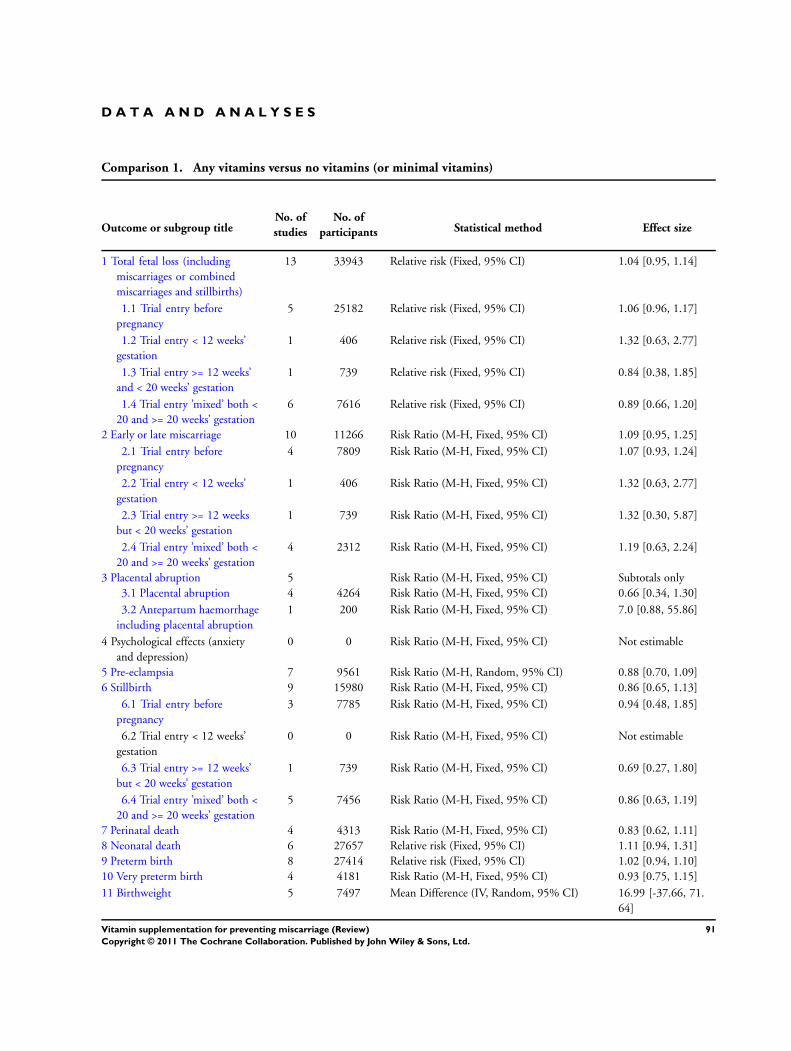
D A T A A N D A N A L Y S E S
Comparison 1. Any vitamins versus no vitamins (or minimal vitamins)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss (including
miscarriages or combined
miscarriages and stillbirths)
13 33943 Relative risk (Fixed, 95% CI) 1.04 [0.95, 1.14]
1.1 Trial entry before
pregnancy
5 25182 Relative risk (Fixed, 95% CI) 1.06 [0.96, 1.17]
1.2 Trial entry < 12 weeks’
gestation
1 406 Relative risk (Fixed, 95% CI) 1.32 [0.63, 2.77]
1.3 Trial entry >= 12 weeks’
and < 20 weeks’ gestation
1 739 Relative risk (Fixed, 95% CI) 0.84 [0.38, 1.85]
1.4 Trial entry ’mixed’ both <
20 and >= 20 weeks’ gestation
6 7616 Relative risk (Fixed, 95% CI) 0.89 [0.66, 1.20]
2 Early or late miscarriage 10 11266 Risk Ratio (M-H, Fixed, 95% CI) 1.09 [0.95, 1.25]
2.1 Trial entry before
pregnancy
4 7809 Risk Ratio (M-H, Fixed, 95% CI) 1.07 [0.93, 1.24]
2.2 Trial entry < 12 weeks’
gestation
1 406 Risk Ratio (M-H, Fixed, 95% CI) 1.32 [0.63, 2.77]
2.3 Trial entry >= 12 weeks
but < 20 weeks’ gestation
1 739 Risk Ratio (M-H, Fixed, 95% CI) 1.32 [0.30, 5.87]
2.4 Trial entry ’mixed’ both <
20 and >= 20 weeks’ gestation
4 2312 Risk Ratio (M-H, Fixed, 95% CI) 1.19 [0.63, 2.24]
3 Placental abruption 5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
3.1 Placental abruption 4 4264 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.34, 1.30]
3.2 Antepartum haemorrhage
including placental abruption
1 200 Risk Ratio (M-H, Fixed, 95% CI) 7.0 [0.88, 55.86]
4 Psychological effects (anxiety
and depression)
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
5 Pre-eclampsia 7 9561 Risk Ratio (M-H, Random, 95% CI) 0.88 [0.70, 1.09]
6 Stillbirth 9 15980 Risk Ratio (M-H, Fixed, 95% CI) 0.86 [0.65, 1.13]
6.1 Trial entry before
pregnancy
3 7785 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.48, 1.85]
6.2 Trial entry < 12 weeks’
gestation
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
6.3 Trial entry >= 12 weeks’
but < 20 weeks’ gestation
1 739 Risk Ratio (M-H, Fixed, 95% CI) 0.69 [0.27, 1.80]
6.4 Trial entry ’mixed’ both <
20 and >= 20 weeks’ gestation
5 7456 Risk Ratio (M-H, Fixed, 95% CI) 0.86 [0.63, 1.19]
7 Perinatal death 4 4313 Risk Ratio (M-H, Fixed, 95% CI) 0.83 [0.62, 1.11]
8 Neonatal death 6 27657 Relative risk (Fixed, 95% CI) 1.11 [0.94, 1.31]
9 Preterm birth 8 27414 Relative risk (Fixed, 95% CI) 1.02 [0.94, 1.10]
10 Very preterm birth 4 4181 Risk Ratio (M-H, Fixed, 95% CI) 0.93 [0.75, 1.15]
11 Birthweight 5 7497 Mean Difference (IV, Random, 95% CI) 16.99 [-37.66, 71.
64]
91Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

12 Small-for-gestational age 7 9356 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.84, 1.08]
12.1 Birthweight less than
10th centile or birthweight <
2500 g
7 9356 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.84, 1.08]
13 Congenital malformations 4 8933 Risk Ratio (M-H, Fixed, 95% CI) 1.47 [0.90, 2.40]
14 Multiple pregnancy 3 20986 Relative risk (Fixed, 95% CI) 1.38 [1.12, 1.70]
15 Apgar score less than seven at
five minutes
1 700 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.27, 1.60]
16 Use of blood transfusion for the
mother
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
17 Anaemia (maternal) 2 1190 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.46, 1.73]
18 Anaemia (infant) 1 836 Risk Ratio (M-H, Fixed, 95% CI) 1.05 [0.98, 1.12]
19 Placental weight 1 29 Mean Difference (IV, Fixed, 95% CI) 96.0 [30.73, 161.27]
20 Method of feeding 1 4878 Risk Ratio (M-H, Fixed, 95% CI) 0.98 [0.96, 1.01]
20.1 Breastfeeding 1 4878 Risk Ratio (M-H, Fixed, 95% CI) 0.98 [0.96, 1.01]
20.2 Formula 0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
20.3 Breastfeeding and
formula
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
21 Subsequent fertility 0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
22 Poor growth at childhood
follow-up
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
23 Disability at childhood follow-
up
0 0 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
24 Any adverse effects of vitamin
supplementation sufficient to
stop supplementation
1 739 Risk Ratio (M-H, Fixed, 95% CI) 1.16 [0.39, 3.41]
25 Maternal views of care 0 0 Mean Difference (IV, Fixed, 95% CI) Not estimable
26 Gynaecological hospital
admission
1 1365 Risk Ratio (M-H, Fixed, 95% CI) 0.20 [0.02, 1.69]
26.1 Any maternal admission
to ICU
1 1365 Risk Ratio (M-H, Fixed, 95% CI) 0.20 [0.02, 1.69]
27 Admission to neonatal intensive
care unit
2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
27.1 Any admission to NICU 1 1515 Risk Ratio (M-H, Fixed, 95% CI) 0.81 [0.59, 1.11]
27.2 > 4 days of NICU care 1 1853 Risk Ratio (M-H, Fixed, 95% CI) 0.60 [0.27, 1.37]
27.3 > 7 days in NICU 1 1515 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.54, 1.39]
28 Healthcare costs 0 0 Mean Difference (IV, Fixed, 95% CI) Not estimable
29 Duration of admission to the
neonatal intensive care unit
1 181 Mean Difference (IV, Fixed, 95% CI) 1.30 [-0.28, 2.88]
30 Side effects 1 1734 Risk Ratio (M-H, Fixed, 95% CI) 1.63 [1.12, 2.36]
30.1 Abdominal pain 1 1734 Risk Ratio (M-H, Fixed, 95% CI) 1.63 [1.12, 2.36]
92Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
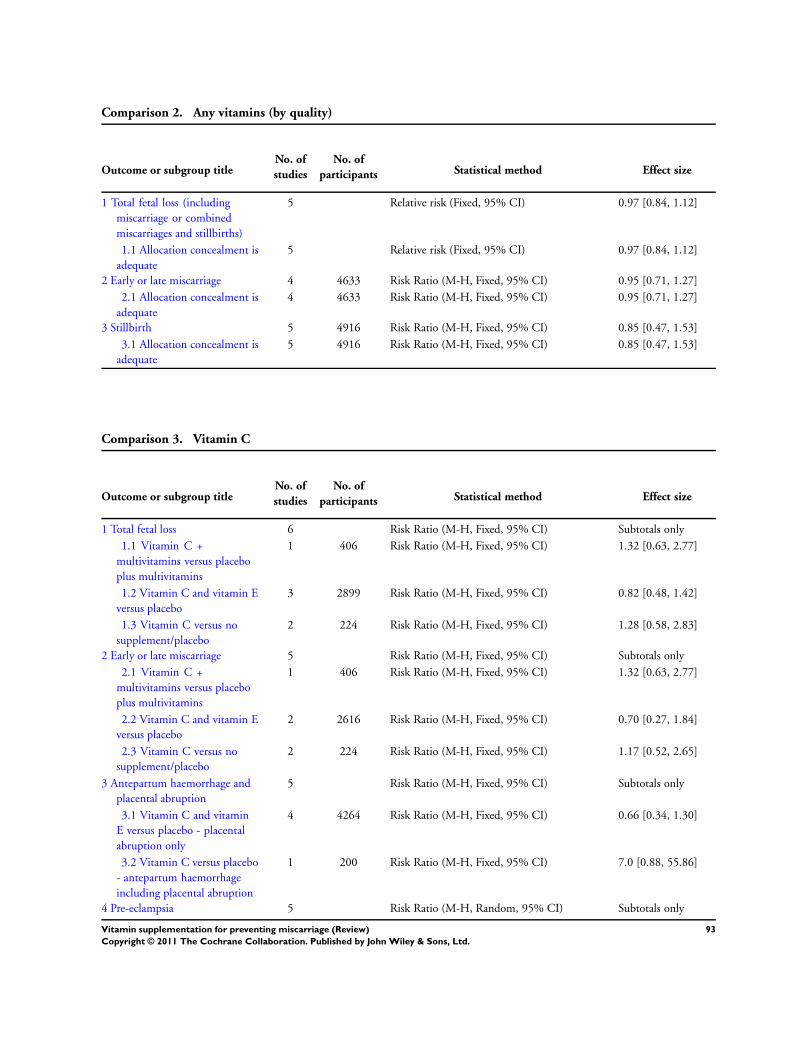
Comparison 2. Any vitamins (by quality)
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss (including
miscarriage or combined
miscarriages and stillbirths)
5 Relative risk (Fixed, 95% CI) 0.97 [0.84, 1.12]
1.1 Allocation concealment is
adequate
5 Relative risk (Fixed, 95% CI) 0.97 [0.84, 1.12]
2 Early or late miscarriage 4 4633 Risk Ratio (M-H, Fixed, 95% CI) 0.95 [0.71, 1.27]
2.1 Allocation concealment is
adequate
4 4633 Risk Ratio (M-H, Fixed, 95% CI) 0.95 [0.71, 1.27]
3 Stillbirth 5 4916 Risk Ratio (M-H, Fixed, 95% CI) 0.85 [0.47, 1.53]
3.1 Allocation concealment is
adequate
5 4916 Risk Ratio (M-H, Fixed, 95% CI) 0.85 [0.47, 1.53]
Comparison 3. Vitamin C
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss 6 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
1.1 Vitamin C +
multivitamins versus placebo
plus multivitamins
1 406 Risk Ratio (M-H, Fixed, 95% CI) 1.32 [0.63, 2.77]
1.2 Vitamin C and vitamin E
versus placebo
3 2899 Risk Ratio (M-H, Fixed, 95% CI) 0.82 [0.48, 1.42]
1.3 Vitamin C versus no
supplement/placebo
2 224 Risk Ratio (M-H, Fixed, 95% CI) 1.28 [0.58, 2.83]
2 Early or late miscarriage 5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
2.1 Vitamin C +
multivitamins versus placebo
plus multivitamins
1 406 Risk Ratio (M-H, Fixed, 95% CI) 1.32 [0.63, 2.77]
2.2 Vitamin C and vitamin E
versus placebo
2 2616 Risk Ratio (M-H, Fixed, 95% CI) 0.70 [0.27, 1.84]
2.3 Vitamin C versus no
supplement/placebo
2 224 Risk Ratio (M-H, Fixed, 95% CI) 1.17 [0.52, 2.65]
3 Antepartum haemorrhage and
placental abruption
5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
3.1 Vitamin C and vitamin
E versus placebo - placental
abruption only
4 4264 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.34, 1.30]
3.2 Vitamin C versus placebo
- antepartum haemorrhage
including placental abruption
1 200 Risk Ratio (M-H, Fixed, 95% CI) 7.0 [0.88, 55.86]
4 Pre-eclampsia 5 Risk Ratio (M-H, Random, 95% CI) Subtotals only
93Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

4.1 Vitamin C and vitamin E
versus placebo
4 4264 Risk Ratio (M-H, Random, 95% CI) 0.94 [0.72, 1.22]
4.2 Vitamin C versus placebo 1 200 Risk Ratio (M-H, Random, 95% CI) 1.0 [0.21, 4.84]
5 Stillbirth 4 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
5.1 Vitamin C and vitamin E
versus placebo
3 2899 Risk Ratio (M-H, Fixed, 95% CI) 0.89 [0.46, 1.73]
5.2 Vitamin C versus placebo 1 200 Risk Ratio (M-H, Fixed, 95% CI) 3.0 [0.12, 72.77]
6 Perinatal death 4 4313 Risk Ratio (M-H, Fixed, 95% CI) 0.83 [0.62, 1.11]
6.1 Vitamin C versus placebo 1 182 Risk Ratio (M-H, Fixed, 95% CI) 0.51 [0.05, 5.54]
6.2 Vitamin C and vitamin E
versus placebo
3 4131 Risk Ratio (M-H, Fixed, 95% CI) 0.84 [0.63, 1.12]
7 Neonatal death 3 2717 Risk Ratio (M-H, Fixed, 95% CI) 0.69 [0.30, 1.61]
7.1 Vitamin C versus placebo 1 181 Risk Ratio (M-H, Fixed, 95% CI) 0.69 [0.12, 4.03]
7.2 Vitamin C and E versus
placebo
2 2536 Risk Ratio (M-H, Fixed, 95% CI) 0.69 [0.27, 1.81]
8 Preterm birth 5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
8.1 Vitamin C and vitamin E
versus placebo
4 4264 Risk Ratio (M-H, Fixed, 95% CI) 0.97 [0.85, 1.10]
8.2 Vitamin C versus placebo 1 200 Risk Ratio (M-H, Fixed, 95% CI) 1.43 [1.03, 1.99]
9 Very preterm birth 4 4181 Risk Ratio (M-H, Fixed, 95% CI) 0.93 [0.75, 1.15]
9.1 Vitamin C versus placebo 1 200 Risk Ratio (M-H, Fixed, 95% CI) 1.3 [0.78, 2.17]
9.2 Vitamin C and vitamin E
versus placebo
3 3981 Risk Ratio (M-H, Fixed, 95% CI) 0.88 [0.70, 1.10]
10 Small-for-gestational age 4 4233 Risk Ratio (M-H, Fixed, 95% CI) 0.90 [0.78, 1.04]
10.1 Vitamin C and vitamin
E versus placebo
4 4233 Risk Ratio (M-H, Fixed, 95% CI) 0.90 [0.78, 1.04]
11 Birthweight 2 2561 Mean Difference (IV, Fixed, 95% CI) 1.25 [-47.45, 49.95]
11.1 Vitamin C and vitamin
E versus placebo
2 2561 Mean Difference (IV, Fixed, 95% CI) 1.25 [-47.45, 49.95]
12 Congenital malformations 2 2254 Risk Ratio (M-H, Fixed, 95% CI) 1.44 [0.73, 2.84]
12.1 Vitamin C and vitamin
E versus placebo
2 2254 Risk Ratio (M-H, Fixed, 95% CI) 1.44 [0.73, 2.84]
13 Apgar score less than seven at
five minutes
1 700 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.27, 1.60]
13.1 Vitamin C and vitamin
E versus placebo
1 700 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.27, 1.60]
14 Any adverse effects of vitamin
supplementation sufficient to
stop supplementation
1 739 Risk Ratio (M-H, Fixed, 95% CI) 1.16 [0.39, 3.41]
14.1 Vitamin C and vitamin
E versus placebo
1 739 Risk Ratio (M-H, Fixed, 95% CI) 1.16 [0.39, 3.41]
15 Gynaecological hospital
admission
1 1365 Risk Ratio (M-H, Fixed, 95% CI) 0.20 [0.02, 1.69]
15.1 Vitamin C and vitamin
E versus placebo: Any maternal
admission to ICU
1 1365 Risk Ratio (M-H, Fixed, 95% CI) 0.20 [0.02, 1.69]
16 Admission to neonatal intensive
care unit
2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
16.1 Vitamin C and vitamin E
versus placebo: Any admission
to NICU
1 1515 Risk Ratio (M-H, Fixed, 95% CI) 0.81 [0.59, 1.11]
94Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

16.2 Vitamin C and vitamin
E versus placebo: > 4 days of
NICU care
1 1853 Risk Ratio (M-H, Fixed, 95% CI) 0.60 [0.27, 1.37]
16.3 Vitamin C and vitamin
E versus placebo: > 7 days of
NICU care
1 1515 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.54, 1.39]
17 Side effects 1 1734 Risk Ratio (M-H, Fixed, 95% CI) 1.63 [1.12, 2.36]
17.1 Vitamin C and vitamin
E versus placebo: Abdominal
pain
1 1734 Risk Ratio (M-H, Fixed, 95% CI) 1.63 [1.12, 2.36]
Comparison 4. Vitamin A
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss (including
miscarriages or combined
miscarriages and stillbirths)
5 Relative risk (Fixed, 95% CI) Subtotals only
1.1 Vitamin A versus placebo 1 11723 Relative risk (Fixed, 95% CI) 1.04 [0.92, 1.17]
1.2 B-carotene versus placebo 1 11303 Relative risk (Fixed, 95% CI) 1.03 [0.91, 1.16]
1.3 Vitamin A versus
B-carotene
1 11720 Relative risk (Fixed, 95% CI) 1.01 [0.90, 1.14]
1.4 Vitamin A or B-carotene
versus placebo
1 17373 Relative risk (Fixed, 95% CI) 1.05 [0.91, 1.21]
1.5 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1074 Relative risk (Fixed, 95% CI) 0.80 [0.53, 1.21]
1.6 Vitamin A + iron + folate
versus iron + folate
3 1640 Relative risk (Fixed, 95% CI) 1.01 [0.61, 1.66]
2 Early or late miscarriage 3 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
2.1 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1075 Risk Ratio (M-H, Fixed, 95% CI) 0.76 [0.37, 1.55]
2.2 Vitamin A + iron + folate
versus iron + folate
2 1397 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.47, 1.63]
3 Stillbirth 4 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
3.1 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1075 Risk Ratio (M-H, Fixed, 95% CI) 1.04 [0.60, 1.79]
3.2 Vitamin A + iron + folate
versus iron + folate
3 1640 Risk Ratio (M-H, Fixed, 95% CI) 1.29 [0.57, 2.91]
4 Neonatal death 1 Relative risk (Fixed, 95% CI) Subtotals only
4.1 Vitamin A versus placebo 1 10214 Relative risk (Fixed, 95% CI) 1.09 [0.92, 1.30]
4.2 B-carotene versus placebo 1 9788 Relative risk (Fixed, 95% CI) 1.09 [0.91, 1.30]
4.3 Vitamin A versus
B-carotene
1 10228 Relative risk (Fixed, 95% CI) 1.0 [0.85, 1.18]
4.4 Vitamin A or B-carotene
versus placebo
1 15115 Relative risk (Fixed, 95% CI) 1.09 [0.91, 1.30]
95Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5 Preterm birth 3 Relative risk (Fixed, 95% CI) Subtotals only
5.1 Vitamin A versus placebo 1 11723 Relative risk (Fixed, 95% CI) 1.04 [0.89, 1.21]
5.2 B-carotene versus placebo 1 11303 Relative risk (Fixed, 95% CI) 1.01 [0.86, 1.18]
5.3 Vitamin A versus
B-carotene
1 11720 Relative risk (Fixed, 95% CI) 1.03 [0.88, 1.20]
5.4 Vitamin A or B-carotene
versus placebo
1 17373 Relative risk (Fixed, 95% CI) 1.02 [0.89, 1.17]
5.5 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1075 Relative risk (Fixed, 95% CI) 1.07 [0.84, 1.37]
5.6 Vitamin A + iron + folate
versus iron + folate
1 700 Relative risk (Fixed, 95% CI) 1.11 [0.59, 2.09]
6 Birthweight 1 594 Mean Difference (IV, Fixed, 95% CI) 90.0 [2.68, 177.32]
6.1 Vitamin A + iron + folate
versus iron + folate
1 594 Mean Difference (IV, Fixed, 95% CI) 90.0 [2.68, 177.32]
7 Small-for-gestational age 1 1075 Risk Ratio (M-H, Fixed, 95% CI) 0.84 [0.58, 1.21]
7.1 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1075 Risk Ratio (M-H, Fixed, 95% CI) 0.84 [0.58, 1.21]
8 Multiple pregnancy 1 Relative risk (Fixed, 95% CI) Subtotals only
8.1 Vitamin A versus placebo 1 10697 Relative risk (Fixed, 95% CI) 1.35 [0.99, 1.85]
8.2 B-carotene versus placebo 1 10294 Relative risk (Fixed, 95% CI) 1.37 [1.00, 1.88]
8.3 Vitamin A versus
B-carotene
1 10699 Relative risk (Fixed, 95% CI) 1.03 [0.77, 1.37]
8.4 Vitamin A or B-carotene
versus placebo
1 15845 Relative risk (Fixed, 95% CI) 1.39 [1.05, 1.84]
9 Very preterm birth 1 1075 Risk Ratio (M-H, Fixed, 95% CI) 1.11 [0.71, 1.74]
9.1 Vitamin A (with/without
multivitamins) versus
multivitamins or placebo
1 1075 Risk Ratio (M-H, Fixed, 95% CI) 1.11 [0.71, 1.74]
10 Maternal anaemia 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
10.1 Vitamin A +
beta-carotene with or without
multivitamin versus placebo
1 807 Risk Ratio (M-H, Fixed, 95% CI) 0.86 [0.60, 1.24]
10.2 Vitamin A +
beta-carotene versus placebo
1 539 Risk Ratio (M-H, Fixed, 95% CI) 0.91 [0.60, 1.38]
10.3 Vitamin A + iron and
folic acid versus iron and folic
acid
1 700 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.82, 1.12]
11 Infant anaemia 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
11.1 Infant anaemia at 6
weeks’ of age - vitamin A + iron
+ folate versus iron + folate
1 562 Risk Ratio (M-H, Fixed, 95% CI) 0.58 [0.45, 0.75]
11.2 Infant anaemia at 12
months - vitamin A + iron +
folate versus iron + folate
1 478 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.88, 1.20]
11.3 Infant anaemia - vitamin
A + beta-carotene with or
without multivitamins versus
placebo
1 625 Risk Ratio (M-H, Fixed, 95% CI) 0.99 [0.92, 1.06]
96Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

11.4 Infant anaemia - vitamin
A + beta-carotene versus
placebo
1 406 Risk Ratio (M-H, Fixed, 95% CI) 0.99 [0.92, 1.08]
12 Poor growth at childhood
follow up
2 Mean Difference (IV, Fixed, 95% CI) Subtotals only
12.1 Weight (g) at 6 weeks:
vitamin A + iron + folate versus
iron + folate
1 546 Mean Difference (IV, Fixed, 95% CI) 169.0 [16.55, 321.
45]
12.2 Length (cm) at 6 weeks:
vitamin A + iron + folate versus
iron + folate
1 546 Mean Difference (IV, Fixed, 95% CI) 0.70 [0.15, 1.25]
12.3 Weight (g) at 4 months:
vitamin A + iron + folate versus
iron + folate
1 148 Mean Difference (IV, Fixed, 95% CI) -100.0 [-377.14,
177.14]
12.4 Length (cm) at 4 months:
vitamin A + iron + folate versus
iron + folate
1 148 Mean Difference (IV, Fixed, 95% CI) -0.5 [-1.33, 0.33]
Comparison 5. Multivitamin
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss (including
miscarriages or combined
miscarriages and stillbirths)
12 Risk Ratio (M-H, Random, 95% CI) Subtotals only
1.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
3 6883 Risk Ratio (M-H, Random, 95% CI) 1.00 [0.75, 1.34]
1.2 Multivitamin without
folic acid versus no
multivitamin/folic acid
1 907 Risk Ratio (M-H, Random, 95% CI) 0.83 [0.56, 1.25]
1.3 Multivitamins
with/without folic acid versus
no multivitamins/folic acid
1 1368 Risk Ratio (M-H, Random, 95% CI) 0.91 [0.65, 1.27]
1.4 Multivitamin + folic acid
versus folic acid
2 1096 Risk Ratio (M-H, Random, 95% CI) 1.03 [0.72, 1.48]
1.5 Multivitamin without
folic acid versus folic acid
2 1090 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.62, 1.30]
1.6 Multivitamin
with/without folic acid versus
folic acid
2 1644 Risk Ratio (M-H, Random, 95% CI) 0.95 [0.69, 1.30]
1.7 Multivitamin
with/without vitamin A versus
vitamin A or placebo
1 1074 Risk Ratio (M-H, Random, 95% CI) 0.60 [0.39, 0.91]
1.8 Multivitamins versus
control
1 5021 Risk Ratio (M-H, Random, 95% CI) 0.83 [0.58, 1.17]
97Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1.9 Multivitamin + vitamin
E versus multivitamin without
vitamin E or controls
1 823 Risk Ratio (M-H, Random, 95% CI) 0.92 [0.46, 1.83]
1.10 Multivitamins + iron +
folic acid versus iron + folic
acid
5 42404 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.75, 1.09]
2 Early or late miscarriage 10 Risk Ratio (M-H, Random, 95% CI) Subtotals only
2.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
3 6883 Risk Ratio (M-H, Random, 95% CI) 0.99 [0.72, 1.38]
2.2 Multivitamin without
folic acid versus no
multivitamin/folic acid
1 907 Risk Ratio (M-H, Random, 95% CI) 0.89 [0.59, 1.34]
2.3 Multivitamin
with/without folic acid versus
no multivitamin/folic acid
1 1368 Risk Ratio (M-H, Random, 95% CI) 0.95 [0.67, 1.34]
2.4 Multivitamin + folic acid
versus folic acid
2 1096 Risk Ratio (M-H, Random, 95% CI) 1.04 [0.72, 1.49]
2.5 Multivitamin without
folic acid versus folic acid
2 1090 Risk Ratio (M-H, Random, 95% CI) 0.89 [0.61, 1.31]
2.6 Multivitamin
with/without folic acid versus
folic acid
2 1644 Risk Ratio (M-H, Random, 95% CI) 0.96 [0.70, 1.33]
2.7 Multivitamin + vitamin
E versus multivitamin without
vitamin E or controls
1 823 Risk Ratio (M-H, Random, 95% CI) 1.04 [0.26, 4.13]
2.8 Multivitamin + iron +
folic acid versus iron + folic
acid
5 42404 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.73, 1.11]
3 Placental abruption 1 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
3.1 Multivitamins + iron +
folic acid versus iron + folic
acid
1 60 Risk Ratio (M-H, Fixed, 95% CI) Not estimable
4 Pre-eclampsia 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
4.1 Multivitamin versus
control
1 5021 Risk Ratio (M-H, Fixed, 95% CI) 0.70 [0.55, 0.90]
4.2 Multivitamin + iron +
folic acid versus iron + folic
acid
1 60 Risk Ratio (M-H, Fixed, 95% CI) 0.24 [0.06, 1.01]
5 Stillbirth 11 Risk Ratio (M-H, Random, 95% CI) Subtotals only
5.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
3 6883 Risk Ratio (M-H, Random, 95% CI) 1.04 [0.51, 2.10]
5.2 Multivitamin without
folic acid versus no
multivitamin/folic acid
1 907 Risk Ratio (M-H, Random, 95% CI) 0.14 [0.01, 2.76]
5.3 Multivitamin
with/without folic acid versus
no multivitamin/folic acid
1 1368 Risk Ratio (M-H, Random, 95% CI) 0.33 [0.06, 1.97]
5.4 Multivitamin + folic acid
versus folic acid
2 1096 Risk Ratio (M-H, Random, 95% CI) 0.97 [0.14, 6.88]
98Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5.5 Multivitamin without
folic acid versus folic acid
2 1090 Risk Ratio (M-H, Random, 95% CI) 0.99 [0.04, 22.88]
5.6 Multivitamin
with/without folic acid versus
folic acid
2 1644 Risk Ratio (M-H, Random, 95% CI) 0.79 [0.15, 4.10]
5.7 Multivitamin versus
control
1 5021 Risk Ratio (M-H, Random, 95% CI) 0.83 [0.58, 1.17]
5.8 Multivitamin + vitamin
E versus multivitamin without
vitamin E or controls
1 823 Risk Ratio (M-H, Random, 95% CI) 0.88 [0.39, 1.98]
5.9 Multivitamin + iron +
folic acid versus iron + folic
acid
5 42404 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.75, 1.07]
6 Perinatal death 5 Relative risk (Random, 95% CI) Subtotals only
6.1 Multivitamin + folic acid
+ iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 4308 Relative risk (Random, 95% CI) 1.11 [0.98, 1.26]
6.2 Multivitamin + iron +
folic acid versus iron + folic
acid
4 42344 Relative risk (Random, 95% CI) 0.99 [0.80, 1.21]
7 Neonatal death 8 Relative risk (Fixed, 95% CI) Subtotals only
7.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
1 4930 Relative risk (Fixed, 95% CI) 1.59 [0.30, 8.30]
7.2 Multivitamin + vitamin
E versus multivitamin without
vitamin E or controls
1 787 Relative risk (Fixed, 95% CI) 1.44 [0.91, 2.27]
7.3 Multivitamin versus
control
1 4895 Relative risk (Fixed, 95% CI) 1.0 [0.75, 1.34]
7.4 Multivitamin + folic acid
+ iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 4122 Relative risk (Fixed, 95% CI) 1.15 [0.97, 1.36]
7.5 Multivitamin + iron +
folic acid versus iron + folic
acid
4 40706 Relative risk (Fixed, 95% CI) 0.91 [0.80, 1.03]
8 Preterm birth 8 Relative risk (Fixed, 95% CI) Subtotals only
8.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
1 5502 Relative risk (Fixed, 95% CI) 1.01 [0.91, 1.12]
8.2 Multivitamin + folic acid
+ iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 3320 Relative risk (Fixed, 95% CI) 0.98 [0.90, 1.07]
8.3 Multivitamin + vitamin
E versus multivitamin without
vitamin E or controls
1 814 Relative risk (Fixed, 95% CI) 0.99 [0.85, 1.15]
8.4 Multivitamin + iron +
folic acid versus iron + folic
acid
5 39540 Relative risk (Fixed, 95% CI) 1.00 [0.96, 1.04]
99Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

9 Very preterm birth 1 8428 Risk Ratio (M-H, Fixed, 95% CI) 0.88 [0.73, 1.06]
9.1 Multivitamin + iron +
folic acid versus iron + folic
acid
1 8428 Risk Ratio (M-H, Fixed, 95% CI) 0.88 [0.73, 1.06]
10 Birthweight 4 Mean Difference (IV, Fixed, 95% CI) Subtotals only
10.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
1 4862 Mean Difference (IV, Fixed, 95% CI) 3.0 [-24.15, 30.15]
10.2 Multivitamin + iron +
folic acid versus iron + folic
acid
3 10241 Mean Difference (IV, Fixed, 95% CI) 61.61 [37.32, 85.91]
11 Small-for-gestational age
(birthweight less than the 10th
percentile or < 2500 g
8 Relative risk (Random, 95% CI) Subtotals only
11.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
1 4862 Relative risk (Random, 95% CI) 1.09 [0.94, 1.26]
11.2 Multivitamin + folic acid
versus no multivitamin/folic
acid (birthweight < 2500 g)
1 186 Relative risk (Random, 95% CI) 0.91 [0.63, 1.32]
11.3 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 3320 Relative risk (Random, 95% CI) 0.98 [0.95, 1.02]
11.4 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A (birthweight < 2500
g)
1 3325 Relative risk (Random, 95% CI) 0.95 [0.90, 1.00]
11.5 Multivitamins + iron +
folic acid versus iron + folic
acid
5 21434 Relative risk (Random, 95% CI) 0.93 [0.77, 1.12]
12 Congenital malformations 4 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
12.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
2 5777 Risk Ratio (M-H, Fixed, 95% CI) 1.69 [0.81, 3.53]
12.2 Multivitamin without
folic acid without versus no
multivitamin/folic acid
1 907 Risk Ratio (M-H, Fixed, 95% CI) 1.60 [0.53, 4.86]
12.3 Multivitamin
with/without folic acid versus
no multivitamin/folic acid
1 1368 Risk Ratio (M-H, Fixed, 95% CI) 1.99 [0.75, 5.26]
12.4 Multivitamin + folic acid
versus folic acid
2 1096 Risk Ratio (M-H, Fixed, 95% CI) 1.71 [0.72, 4.04]
12.5 Multivitamin without
folic acid versus folic acid
2 1090 Risk Ratio (M-H, Fixed, 95% CI) 1.61 [0.67, 3.85]
12.6 Multivitamin
with/without folic acid versus
folic acid
2 1644 Risk Ratio (M-H, Fixed, 95% CI) 1.66 [0.76, 3.63]
100Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

12.7 Multivitamin + iron +
folic acid versus iron + folic
acid
1 1200 Risk Ratio (M-H, Fixed, 95% CI) 1.0 [0.14, 7.08]
13 Multiple pregnancy 2 5141 Risk Ratio (M-H, Fixed, 95% CI) 1.36 [1.00, 1.85]
13.1 Multivitamin + folic acid
versus no multivitamin/folic
acid
2 5141 Risk Ratio (M-H, Fixed, 95% CI) 1.36 [1.00, 1.85]
14 Maternal anaemia 4 Relative risk (Fixed, 95% CI) Subtotals only
14.1 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A (any anaemia)
1 813 Relative risk (Fixed, 95% CI) 0.92 [0.83, 1.03]
14.2 Multivitamin + folic
acid + iron + zinc+vitamin A
versus folic acid + iron + zinc +
vitamin A (severe anaemia)
1 813 Relative risk (Fixed, 95% CI) 0.82 [0.53, 1.27]
14.3 Multivitamins versus
placebo
1 538 Relative risk (Fixed, 95% CI) 0.78 [0.50, 1.22]
14.4 Multivitamins + vitamin
A + beta-carotene versus
placebo
1 535 Relative risk (Fixed, 95% CI) 0.82 [0.53, 1.26]
14.5 Multivitamins + iron +
folic acid versus iron + folic
acid
2 2278 Relative risk (Fixed, 95% CI) 0.88 [0.81, 0.96]
15 Breastfeeding 1 4878 Risk Ratio (M-H, Fixed, 95% CI) 0.98 [0.96, 1.01]
15.1 Multivitamin versus
control
1 4878 Risk Ratio (M-H, Fixed, 95% CI) 0.98 [0.96, 1.01]
16 Poor growth at childhood
follow up: Underweight in
childhood (6-8 years of age)
1 3356 Risk Ratio (Fixed, 95% CI) 1.05 [0.97, 1.13]
16.1 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 3356 Risk Ratio (Fixed, 95% CI) 1.05 [0.97, 1.13]
17 Poor growth at childhood
follow up: Stunting in
childhood (6-8 years of age)
1 3356 Risk Ratio (Fixed, 95% CI) 1.09 [1.00, 1.19]
17.1 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 3356 Risk Ratio (Fixed, 95% CI) 1.09 [1.00, 1.19]
18 Additional outcomes - infant
death
1 4122 Relative risk (Fixed, 95% CI) 1.10 [0.94, 1.29]
18.1 Multivitamin + folic
acid + iron + zinc + vitamin A
versus folic acid + iron + zinc +
vitamin A
1 4122 Relative risk (Fixed, 95% CI) 1.10 [0.94, 1.29]
101Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 6. Folic acid
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Total fetal loss (including
miscarriages or combined
miscarriages and stillbirths)
6 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
1.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
3 6883 Risk Ratio (M-H, Fixed, 95% CI) 1.09 [0.95, 1.25]
1.2 Folic acid without
multivitamin versus no folic
acid/multivitamin
1 903 Risk Ratio (M-H, Fixed, 95% CI) 0.95 [0.64, 1.40]
1.3 Folic acid with/without
multivitamin versus no folic
acid/multivitamin
1 1364 Risk Ratio (M-H, Fixed, 95% CI) 0.97 [0.69, 1.35]
1.4 Folic acid + multivitamin
versus multivitamin
2 1102 Risk Ratio (M-H, Fixed, 95% CI) 1.15 [0.80, 1.67]
1.5 Folic acid without
multivitamin versus
multivitamin
2 1090 Risk Ratio (M-H, Fixed, 95% CI) 1.12 [0.77, 1.62]
1.6 Folic acid with or
without multivitamin versus
multivitamin
2 1644 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [0.82, 1.57]
1.7 Folic acid + iron versus
iron
1 75 Risk Ratio (M-H, Fixed, 95% CI) 0.23 [0.01, 4.59]
1.8 Folic acid + iron +
antimalarials versus iron +
antimalarials
1 160 Risk Ratio (M-H, Fixed, 95% CI) 13.0 [0.74, 226.98]
2 Early or late miscarriage 6 Risk Ratio (M-H, Random, 95% CI) Subtotals only
2.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
3 6883 Risk Ratio (M-H, Random, 95% CI) 0.99 [0.72, 1.38]
2.2 Folic acid without
multivitamins versus no folic
acid/multivitamin
1 903 Risk Ratio (M-H, Random, 95% CI) 0.97 [0.65, 1.44]
2.3 Folic acid with/without
multivitamin versus no folic
acid/multivitamin
1 1364 Risk Ratio (M-H, Random, 95% CI) 0.99 [0.70, 1.39]
2.4 Folic acid + multivitamin
versus multivitamin
2 1102 Risk Ratio (M-H, Random, 95% CI) 1.16 [0.80, 1.69]
2.5 Folic acid without
multivitamin versus
multivitamin
2 1090 Risk Ratio (M-H, Random, 95% CI) 1.12 [0.77, 1.64]
2.6 Folic acid with/without
multivitamin versus
multivitamin
2 1642 Risk Ratio (M-H, Random, 95% CI) 1.09 [0.79, 1.51]
2.7 Folic acid + iron versus
iron
1 75 Risk Ratio (M-H, Random, 95% CI) 0.38 [0.02, 9.03]
102Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.8 Folic acid + iron +
antimalarials versus iron +
antimalarials
1 160 Risk Ratio (M-H, Random, 95% CI) 13.0 [0.74, 226.98]
3 Pre-eclampsia 1 75 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [0.17, 7.69]
3.1 Folic acid + iron versus
iron
1 75 Risk Ratio (M-H, Fixed, 95% CI) 1.14 [0.17, 7.69]
4 Stillbirth 5 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
4.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
3 6883 Risk Ratio (M-H, Fixed, 95% CI) 1.03 [0.51, 2.09]
4.2 Folic acid without
multivitamin versus no folic
acid/multivitamin
1 903 Risk Ratio (M-H, Fixed, 95% CI) 0.67 [0.11, 4.02]
4.3 Folic acid with/without
multivitamin versus no folic
acid/multivitamin
1 1364 Risk Ratio (M-H, Fixed, 95% CI) 0.67 [0.15, 2.96]
4.4 Folic acid + multivitamin
versus multivitamin
2 1102 Risk Ratio (M-H, Fixed, 95% CI) 1.00 [0.20, 4.99]
4.5 Folic acid without
multivitamin versus
multivitamin
2 1090 Risk Ratio (M-H, Fixed, 95% CI) 4.97 [0.58, 42.29]
4.6 Folic acid with/without
multivitamin versus
multivitamin
2 1644 Risk Ratio (M-H, Fixed, 95% CI) 0.84 [0.20, 3.53]
4.7 Folic acid + iron versus
iron
1 75 Risk Ratio (M-H, Fixed, 95% CI) 0.38 [0.02, 9.03]
5 Perinatal death 1 4308 Relative risk (Fixed, 95% CI) 0.97 [0.85, 1.11]
5.1 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A
1 4308 Relative risk (Fixed, 95% CI) 0.97 [0.85, 1.11]
6 Neonatal death 2 Relative risk (Fixed, 95% CI) Subtotals only
6.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
1 4930 Relative risk (Fixed, 95% CI) 1.59 [0.30, 8.28]
6.2 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A
1 4122 Relative risk (Fixed, 95% CI) 0.96 [0.80, 1.14]
7 Preterm birth 3 Relative risk (Fixed, 95% CI) Subtotals only
7.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
1 5502 Relative risk (Fixed, 95% CI) 1.01 [0.91, 1.12]
7.2 Folic acid +
multivitamin versus no folic
acid/multivitamin
1 75 Relative risk (Fixed, 95% CI) 1.01 [0.65, 1.56]
7.3 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A
1 3320 Relative risk (Fixed, 95% CI) 1.02 [0.94, 1.11]
8 Birthweight 3 Mean Difference (IV, Fixed, 95% CI) Subtotals only
8.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
1 4862 Mean Difference (IV, Fixed, 95% CI) 3.0 [-24.15, 30.15]
103Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

8.2 Folic acid versus placebo 1 29 Mean Difference (IV, Fixed, 95% CI) 312.0 [108.52, 515.
48]
8.3 Folic + iron versus control 1 45 Mean Difference (IV, Fixed, 95% CI) -32.0 [-213.62, 149.
62]
9 Small-for-gestational age 4 Relative risk (Fixed, 95% CI) Subtotals only
9.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
1 4862 Relative risk (Fixed, 95% CI) 1.09 [0.94, 1.26]
9.2 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A
1 3320 Relative risk (Fixed, 95% CI) 0.97 [0.92, 1.03]
9.3 Folic acid + iron versus
iron (birthweight < 2500 g)
1 75 Relative risk (Fixed, 95% CI) 1.06 [0.48, 2.33]
9.4 Folic acid +
multivitamin versus no folic
acid/multivitamin (birthweight
< 2500 g)
1 186 Relative risk (Fixed, 95% CI) 0.91 [0.63, 1.32]
9.5 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A (birthweight
< 2500 g)
1 3325 Relative risk (Fixed, 95% CI) 0.94 [0.90, 0.99]
10 Congenital malformations 3 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
10.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
2 5777 Risk Ratio (M-H, Fixed, 95% CI) 1.69 [0.81, 3.53]
10.2 Folic acid without
multivitamin versus no folic
acid/multivitamin
1 903 Risk Ratio (M-H, Fixed, 95% CI) 1.42 [0.45, 4.43]
10.3 Folic acid with/without
multivitamin versus no folic
acid/multivitamin
1 1364 Risk Ratio (M-H, Fixed, 95% CI) 1.90 [0.71, 5.04]
10.4 Folic acid + multivitamin
versus multivitamin
2 1102 Risk Ratio (M-H, Fixed, 95% CI) 1.07 [0.51, 2.26]
10.5 Folic acid without
multivitamin versus
multivitamin
2 1090 Risk Ratio (M-H, Fixed, 95% CI) 0.62 [0.26, 1.49]
10.6 Folic acid with or
without multvitamin versus
multivitamin
2 1644 Risk Ratio (M-H, Fixed, 95% CI) 0.85 [0.43, 1.67]
11 Multiple pregnancy 2 Risk Ratio (M-H, Fixed, 95% CI) Subtotals only
11.1 Folic acid +
multivitamin versus no folic
acid/multivitamin
2 5141 Risk Ratio (M-H, Fixed, 95% CI) 1.36 [1.00, 1.85]
12 Maternal anaemia 3 Relative risk (Fixed, 95% CI) Subtotals only
12.1 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A (any anaemia)
1 813 Relative risk (Fixed, 95% CI) 0.83 [0.77, 0.91]
12.2 Folic acid + iron + zinc
+ multivitamin + vitamin
A versus vitamin A (severe
anaemia)
1 813 Relative risk (Fixed, 95% CI) 0.82 [0.59, 1.16]
104Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
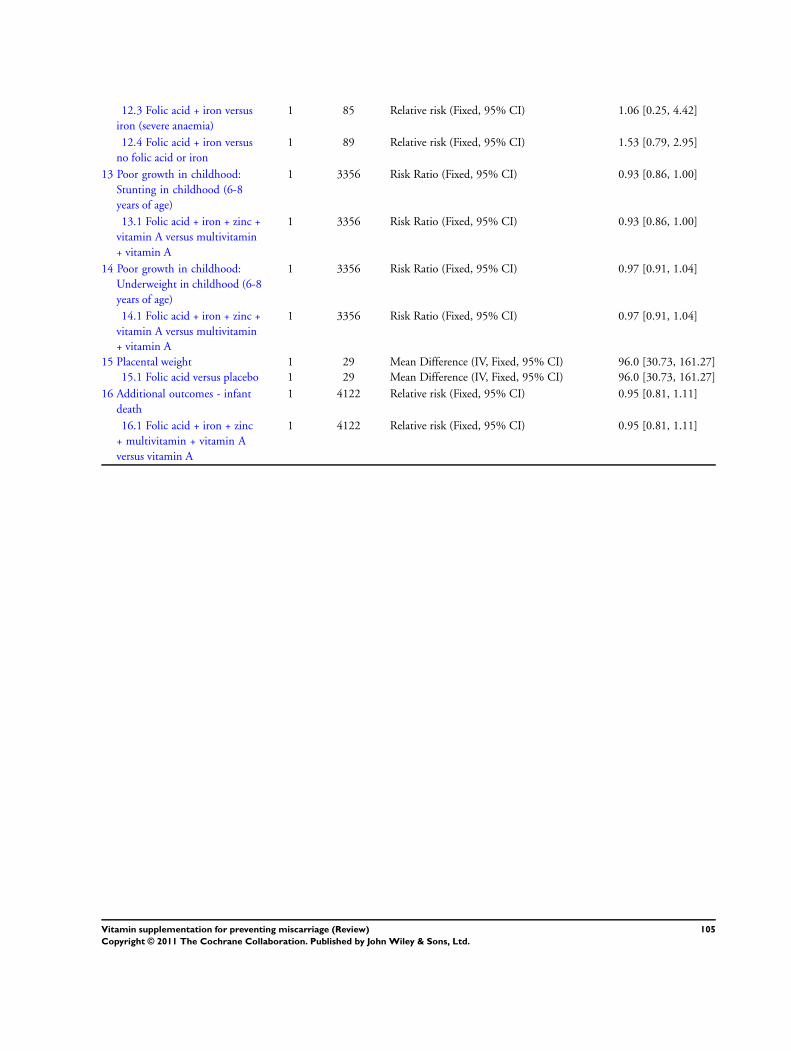
12.3 Folic acid + iron versus
iron (severe anaemia)
1 85 Relative risk (Fixed, 95% CI) 1.06 [0.25, 4.42]
12.4 Folic acid + iron versus
no folic acid or iron
1 89 Relative risk (Fixed, 95% CI) 1.53 [0.79, 2.95]
13 Poor growth in childhood:
Stunting in childhood (6-8
years of age)
1 3356 Risk Ratio (Fixed, 95% CI) 0.93 [0.86, 1.00]
13.1 Folic acid + iron + zinc +
vitamin A versus multivitamin
+ vitamin A
1 3356 Risk Ratio (Fixed, 95% CI) 0.93 [0.86, 1.00]
14 Poor growth in childhood:
Underweight in childhood (6-8
years of age)
1 3356 Risk Ratio (Fixed, 95% CI) 0.97 [0.91, 1.04]
14.1 Folic acid + iron + zinc +
vitamin A versus multivitamin
+ vitamin A
1 3356 Risk Ratio (Fixed, 95% CI) 0.97 [0.91, 1.04]
15 Placental weight 1 29 Mean Difference (IV, Fixed, 95% CI) 96.0 [30.73, 161.27]
15.1 Folic acid versus placebo 1 29 Mean Difference (IV, Fixed, 95% CI) 96.0 [30.73, 161.27]
16 Additional outcomes - infant
death
1 4122 Relative risk (Fixed, 95% CI) 0.95 [0.81, 1.11]
16.1 Folic acid + iron + zinc
+ multivitamin + vitamin A
versus vitamin A
1 4122 Relative risk (Fixed, 95% CI) 0.95 [0.81, 1.11]
105Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.1. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 1 Total fetal
loss (including miscarriages or combined miscarriages and stillbirths).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 1 Total fetal loss (including miscarriages or combined miscarriages and stillbirths)
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Trial entry before pregnancy
Czeizel 1994 2819 2683 0.131 (0.0779) 35.2 % 1.14 [ 0.98, 1.33 ]
Hemmi 2003 19 5 -0.2357 (1.047) 0.2 % 0.79 [ 0.10, 6.15 ]
ICMR 2000 231 235 -0.6162 (0.3959) 1.4 % 0.54 [ 0.25, 1.17 ]
Katz 2000 11720 5653 0.0488 (0.0706) 42.8 % 1.05 [ 0.91, 1.21 ]
MRC 1991 1363 454 -0.0834 (0.1611) 8.2 % 0.92 [ 0.67, 1.26 ]
Subtotal (95% CI) 16152 9030 87.8 % 1.06 [ 0.96, 1.17 ]
Heterogeneity: Chi2 = 4.64, df = 4 (P = 0.33); I2 =14%
Test for overall effect: Z = 1.18 (P = 0.24)
2 Trial entry < 12 weeks’ gestation
Briscoe 1959 303 103 0.2776 (0.3778) 1.5 % 1.32 [ 0.63, 2.77 ]
Subtotal (95% CI) 303 103 1.5 % 1.32 [ 0.63, 2.77 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.73 (P = 0.46)
3 Trial entry >= 12 weeks’ and < 20 weeks’ gestation
Spinnato 2007 371 368 -0.1744 (0.4038) 1.3 % 0.84 [ 0.38, 1.85 ]
Subtotal (95% CI) 371 368 1.3 % 0.84 [ 0.38, 1.85 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.43 (P = 0.67)
4 Trial entry ’mixed’ both < 20 and >= 20 weeks’ gestation
Chappell 1999 141 142 -0.6931 (1.1986) 0.1 % 0.50 [ 0.05, 5.24 ]
Fleming 1968 35 40 -1.4697 (1.5635) 0.1 % 0.23 [ 0.01, 4.93 ]
Fleming 1986 80 80 2.5649 (1.4607) 0.1 % 13.00 [ 0.74, 227.65 ]
People’s League 1942 2510 2511 -0.1863 (0.179) 6.7 % 0.83 [ 0.58, 1.18 ]
Rumbold 2006 935 942 -0.1625 (0.4026) 1.3 % 0.85 [ 0.39, 1.87 ]
Steyn 2003 100 100 0.3221 (0.4412) 1.1 % 1.38 [ 0.58, 3.28 ]
Subtotal (95% CI) 3801 3815 9.4 % 0.89 [ 0.66, 1.20 ]
Heterogeneity: Chi2 = 5.50, df = 5 (P = 0.36); I2 =9%
Test for overall effect: Z = 0.76 (P = 0.45)
0.001 0.01 0.1 1 10 100 1000
Favours vitamins Favours control
(Continued . . . )
106Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
Total (95% CI) 20627 13316 100.0 % 1.04 [ 0.95, 1.14 ]
Heterogeneity: Chi2 = 12.01, df = 12 (P = 0.44); I2 =0%
Test for overall effect: Z = 0.92 (P = 0.36)
Test for subgroup differences: Chi2 = 1.87, df = 3 (P = 0.60), I2 =0.0%
0.001 0.01 0.1 1 10 100 1000
Favours vitamins Favours control
Analysis 1.2. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 2 Early or
late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 2 Early or late miscarriage
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Trial entry before pregnancy
Czeizel 1994 301/2819 251/2683 69.4 % 1.14 [ 0.97, 1.34 ]
Hemmi 2003 3/19 1/5 0.4 % 0.79 [ 0.10, 6.06 ]
ICMR 2000 6/231 14/235 3.7 % 0.44 [ 0.17, 1.11 ]
MRC 1991 126/1363 44/454 17.8 % 0.95 [ 0.69, 1.32 ]
Subtotal (95% CI) 4432 3377 91.4 % 1.07 [ 0.93, 1.24 ]
Total events: 436 (Vitamin(s)), 310 (Control)
Heterogeneity: Chi2 = 4.70, df = 3 (P = 0.20); I2 =36%
Test for overall effect: Z = 1.00 (P = 0.32)
2 Trial entry < 12 weeks’ gestation
Briscoe 1959 31/303 8/103 3.2 % 1.32 [ 0.63, 2.77 ]
Subtotal (95% CI) 303 103 3.2 % 1.32 [ 0.63, 2.77 ]
Total events: 31 (Vitamin(s)), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.73 (P = 0.47)
3 Trial entry >= 12 weeks but < 20 weeks’ gestation
0.01 0.1 1 10 100
Favours vitamins Favours control
(Continued . . . )
107Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Spinnato 2007 4/371 3/368 0.8 % 1.32 [ 0.30, 5.87 ]
Subtotal (95% CI) 371 368 0.8 % 1.32 [ 0.30, 5.87 ]
Total events: 4 (Vitamin(s)), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.37 (P = 0.71)
4 Trial entry ’mixed’ both < 20 and >= 20 weeks’ gestation
Fleming 1968 0/35 1/40 0.4 % 0.38 [ 0.02, 9.03 ]
Fleming 1986 6/80 0/80 0.1 % 13.00 [ 0.74, 226.98 ]
Rumbold 2006 3/935 7/942 1.9 % 0.43 [ 0.11, 1.66 ]
Steyn 2003 10/100 8/100 2.2 % 1.25 [ 0.51, 3.04 ]
Subtotal (95% CI) 1150 1162 4.6 % 1.19 [ 0.63, 2.24 ]
Total events: 19 (Vitamin(s)), 16 (Control)
Heterogeneity: Chi2 = 5.36, df = 3 (P = 0.15); I2 =44%
Test for overall effect: Z = 0.53 (P = 0.59)
Total (95% CI) 6256 5010 100.0 % 1.09 [ 0.95, 1.25 ]
Total events: 490 (Vitamin(s)), 337 (Control)
Heterogeneity: Chi2 = 10.24, df = 9 (P = 0.33); I2 =12%
Test for overall effect: Z = 1.25 (P = 0.21)
0.01 0.1 1 10 100
Favours vitamins Favours control
108Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 3 Placental
abruption.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 3 Placental abruption
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Placental abruption
Chappell 1999 1/141 3/142 14.2 % 0.34 [ 0.04, 3.19 ]
Rumbold 2006 3/935 1/942 4.7 % 3.02 [ 0.31, 29.00 ]
Spinnato 2007 4/371 8/368 38.1 % 0.50 [ 0.15, 1.63 ]
Villar 2009 6/687 9/678 43.0 % 0.66 [ 0.24, 1.84 ]
Subtotal (95% CI) 2134 2130 100.0 % 0.66 [ 0.34, 1.30 ]
Total events: 14 (Vitamin(s)), 21 (Control)
Heterogeneity: Chi2 = 2.31, df = 3 (P = 0.51); I2 =0.0%
Test for overall effect: Z = 1.20 (P = 0.23)
2 Antepartum haemorrhage including placental abruption
Steyn 2003 7/100 1/100 100.0 % 7.00 [ 0.88, 55.86 ]
Subtotal (95% CI) 100 100 100.0 % 7.00 [ 0.88, 55.86 ]
Total events: 7 (Vitamin(s)), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.84 (P = 0.066)
0.01 0.1 1 10 100
Favours vitamins Favours control
109Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 5 Pre-
eclampsia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 5 Pre-eclampsia
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Chappell 1999 11/142 24/142 8.4 % 0.46 [ 0.23, 0.90 ]
Fleming 1968 2/35 2/40 1.3 % 1.14 [ 0.17, 7.69 ]
People’s League 1942 100/2510 143/2511 24.4 % 0.70 [ 0.55, 0.90 ]
Rumbold 2006 56/935 47/942 17.6 % 1.20 [ 0.82, 1.75 ]
Spinnato 2007 49/371 55/368 18.5 % 0.88 [ 0.62, 1.26 ]
Steyn 2003 3/100 3/100 1.9 % 1.00 [ 0.21, 4.84 ]
Villar 2009 164/687 157/678 27.9 % 1.03 [ 0.85, 1.25 ]
Total (95% CI) 4780 4781 100.0 % 0.88 [ 0.70, 1.09 ]
Total events: 385 (Vitamin(s)), 431 (Control)
Heterogeneity: Tau2 = 0.04; Chi2 = 12.07, df = 6 (P = 0.06); I2 =50%
Test for overall effect: Z = 1.17 (P = 0.24)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
110Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
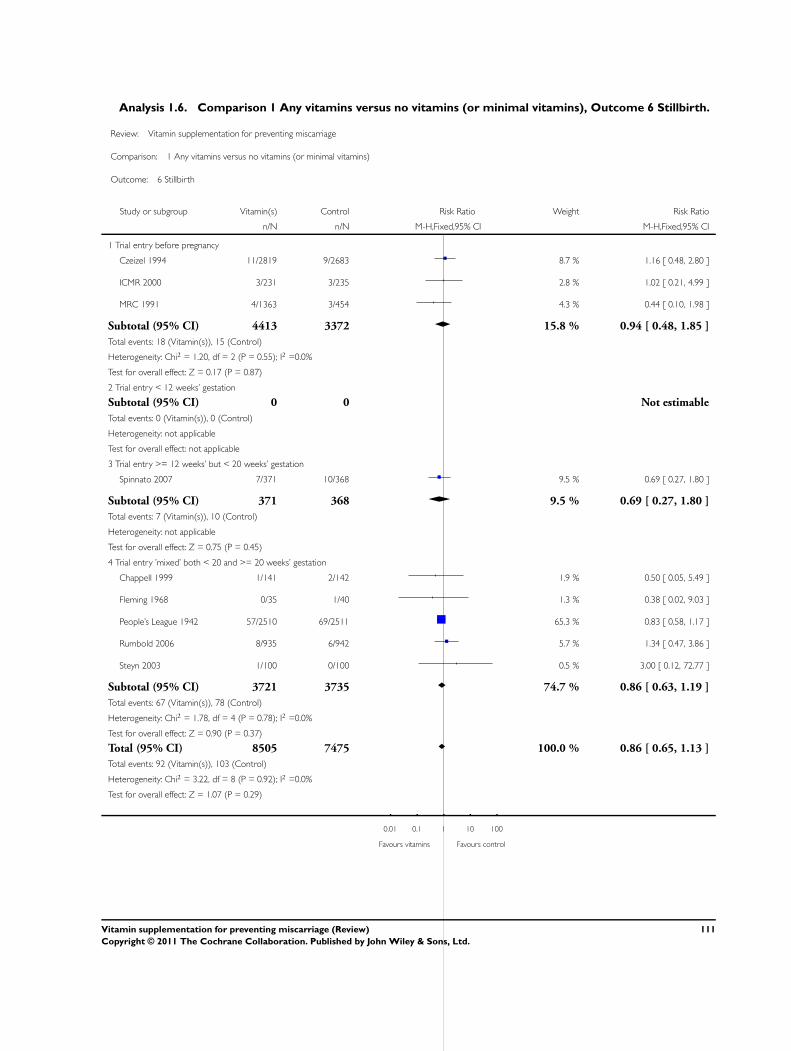
Analysis 1.6. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 6 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 6 Stillbirth
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Trial entry before pregnancy
Czeizel 1994 11/2819 9/2683 8.7 % 1.16 [ 0.48, 2.80 ]
ICMR 2000 3/231 3/235 2.8 % 1.02 [ 0.21, 4.99 ]
MRC 1991 4/1363 3/454 4.3 % 0.44 [ 0.10, 1.98 ]
Subtotal (95% CI) 4413 3372 15.8 % 0.94 [ 0.48, 1.85 ]
Total events: 18 (Vitamin(s)), 15 (Control)
Heterogeneity: Chi2 = 1.20, df = 2 (P = 0.55); I2 =0.0%
Test for overall effect: Z = 0.17 (P = 0.87)
2 Trial entry < 12 weeks’ gestation
Subtotal (95% CI) 0 0 Not estimable
Total events: 0 (Vitamin(s)), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: not applicable
3 Trial entry >= 12 weeks’ but < 20 weeks’ gestation
Spinnato 2007 7/371 10/368 9.5 % 0.69 [ 0.27, 1.80 ]
Subtotal (95% CI) 371 368 9.5 % 0.69 [ 0.27, 1.80 ]
Total events: 7 (Vitamin(s)), 10 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.75 (P = 0.45)
4 Trial entry ’mixed’ both < 20 and >= 20 weeks’ gestation
Chappell 1999 1/141 2/142 1.9 % 0.50 [ 0.05, 5.49 ]
Fleming 1968 0/35 1/40 1.3 % 0.38 [ 0.02, 9.03 ]
People’s League 1942 57/2510 69/2511 65.3 % 0.83 [ 0.58, 1.17 ]
Rumbold 2006 8/935 6/942 5.7 % 1.34 [ 0.47, 3.86 ]
Steyn 2003 1/100 0/100 0.5 % 3.00 [ 0.12, 72.77 ]
Subtotal (95% CI) 3721 3735 74.7 % 0.86 [ 0.63, 1.19 ]
Total events: 67 (Vitamin(s)), 78 (Control)
Heterogeneity: Chi2 = 1.78, df = 4 (P = 0.78); I2 =0.0%
Test for overall effect: Z = 0.90 (P = 0.37)
Total (95% CI) 8505 7475 100.0 % 0.86 [ 0.65, 1.13 ]
Total events: 92 (Vitamin(s)), 103 (Control)
Heterogeneity: Chi2 = 3.22, df = 8 (P = 0.92); I2 =0.0%
Test for overall effect: Z = 1.07 (P = 0.29)
0.01 0.1 1 10 100
Favours vitamins Favours control
111Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.7. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 7 Perinatal
death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 7 Perinatal death
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Rumbold 2006 9/935 10/942 10.4 % 0.91 [ 0.37, 2.22 ]
Spinnato 2007 13/371 16/368 16.8 % 0.81 [ 0.39, 1.65 ]
Steyn 2003 1/90 2/92 2.1 % 0.51 [ 0.05, 5.54 ]
Villar 2009 56/753 68/762 70.7 % 0.83 [ 0.59, 1.17 ]
Total (95% CI) 2149 2164 100.0 % 0.83 [ 0.62, 1.11 ]
Total events: 79 (Vitamin(s)), 96 (Control)
Heterogeneity: Chi2 = 0.20, df = 3 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 1.27 (P = 0.20)
0.01 0.1 1 10 100
Favours vitamins Favours control
112Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.8. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 8 Neonatal
death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 8 Neonatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
Czeizel 1994 2507 2423 1.0647 (1.6288) 0.3 % 2.90 [ 0.12, 70.60 ]
Katz 2000 10228 4887 0.0862 (0.091) 86.3 % 1.09 [ 0.91, 1.30 ]
People’s League 1942 2453 2442 0.3436 (0.2646) 10.2 % 1.41 [ 0.84, 2.37 ]
Rumbold 2006 924 929 -1.3863 (1.1014) 0.6 % 0.25 [ 0.03, 2.16 ]
Spinnato 2007 344 339 -0.0101 (0.6429) 1.7 % 0.99 [ 0.28, 3.49 ]
Steyn 2003 89 92 -0.3711 (0.8964) 0.9 % 0.69 [ 0.12, 4.00 ]
Total (95% CI) 16545 11112 100.0 % 1.11 [ 0.94, 1.31 ]
Heterogeneity: Chi2 = 3.35, df = 5 (P = 0.65); I2 =0.0%
Test for overall effect: Z = 1.19 (P = 0.23)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours vitamins Favours control
113Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
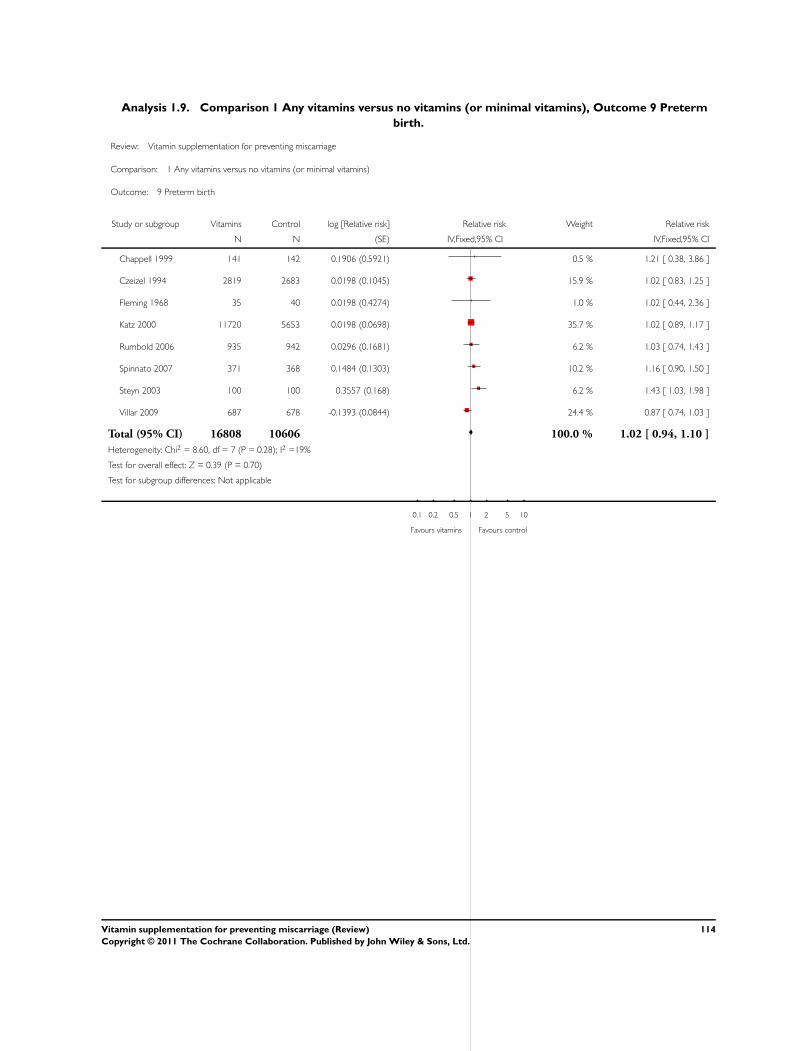
Analysis 1.9. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 9 Preterm
birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 9 Preterm birth
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
Chappell 1999 141 142 0.1906 (0.5921) 0.5 % 1.21 [ 0.38, 3.86 ]
Czeizel 1994 2819 2683 0.0198 (0.1045) 15.9 % 1.02 [ 0.83, 1.25 ]
Fleming 1968 35 40 0.0198 (0.4274) 1.0 % 1.02 [ 0.44, 2.36 ]
Katz 2000 11720 5653 0.0198 (0.0698) 35.7 % 1.02 [ 0.89, 1.17 ]
Rumbold 2006 935 942 0.0296 (0.1681) 6.2 % 1.03 [ 0.74, 1.43 ]
Spinnato 2007 371 368 0.1484 (0.1303) 10.2 % 1.16 [ 0.90, 1.50 ]
Steyn 2003 100 100 0.3557 (0.168) 6.2 % 1.43 [ 1.03, 1.98 ]
Villar 2009 687 678 -0.1393 (0.0844) 24.4 % 0.87 [ 0.74, 1.03 ]
Total (95% CI) 16808 10606 100.0 % 1.02 [ 0.94, 1.10 ]
Heterogeneity: Chi2 = 8.60, df = 7 (P = 0.28); I2 =19%
Test for overall effect: Z = 0.39 (P = 0.70)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
114Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
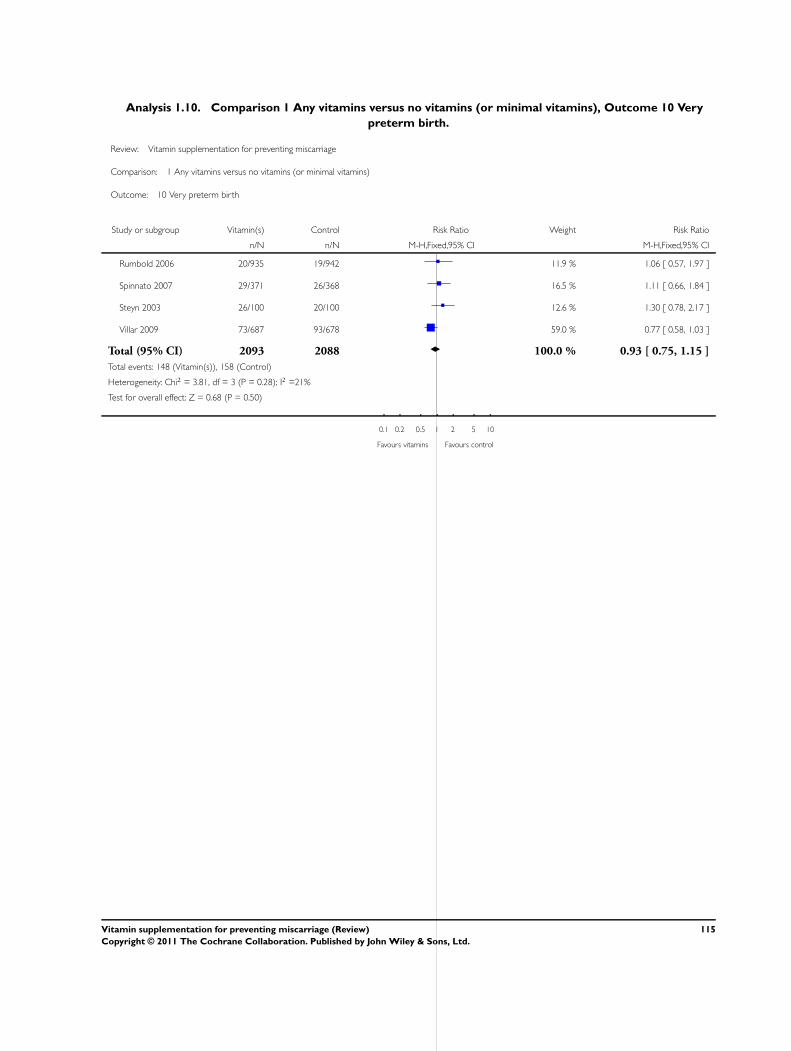
Analysis 1.10. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 10 Very
preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 10 Very preterm birth
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Rumbold 2006 20/935 19/942 11.9 % 1.06 [ 0.57, 1.97 ]
Spinnato 2007 29/371 26/368 16.5 % 1.11 [ 0.66, 1.84 ]
Steyn 2003 26/100 20/100 12.6 % 1.30 [ 0.78, 2.17 ]
Villar 2009 73/687 93/678 59.0 % 0.77 [ 0.58, 1.03 ]
Total (95% CI) 2093 2088 100.0 % 0.93 [ 0.75, 1.15 ]
Total events: 148 (Vitamin(s)), 158 (Control)
Heterogeneity: Chi2 = 3.81, df = 3 (P = 0.28); I2 =21%
Test for overall effect: Z = 0.68 (P = 0.50)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
115Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.11. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 11
Birthweight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 11 Birthweight
Study or subgroup Vitamin(s) ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Correia 1982 16 3440 (304) 13 3128 (255) 6.2 % 312.00 [ 108.52, 515.48 ]
Czeizel 1994 2471 3291 (488) 2391 3288 (478) 40.1 % 3.00 [ -24.15, 30.15 ]
Rumbold 2006 924 3392 (599) 929 3386 (584) 31.0 % 6.00 [ -47.87, 59.87 ]
Spinnato 2007 356 3019.7 (779.3) 352 3039.7 (767.5) 15.2 % -20.00 [ -133.94, 93.94 ]
Taylor 1982 21 3470 (365) 24 3502 (232) 7.5 % -32.00 [ -213.62, 149.62 ]
Total (95% CI) 3788 3709 100.0 % 16.99 [ -37.66, 71.64 ]
Heterogeneity: Tau2 = 1748.69; Chi2 = 9.10, df = 4 (P = 0.06); I2 =56%
Test for overall effect: Z = 0.61 (P = 0.54)
-1000 -500 0 500 1000
Favours control Favours vitamins
116Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.12. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 12 Small-
for-gestational age.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 12 Small-for-gestational age
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Birthweight less than 10th centile or birthweight < 2500 g
Chappell 1999 33/141 45/142 10.3 % 0.74 [ 0.50, 1.08 ]
Czeizel 1994 101/2471 81/2391 18.9 % 1.21 [ 0.91, 1.61 ]
Fleming 1968 3/35 3/40 0.6 % 1.14 [ 0.25, 5.30 ]
ICMR 2000 12/96 14/90 3.3 % 0.80 [ 0.39, 1.64 ]
Rumbold 2006 80/935 92/942 21.1 % 0.88 [ 0.66, 1.17 ]
Spinnato 2007 49/356 49/352 11.3 % 0.99 [ 0.68, 1.43 ]
Villar 2009 141/687 149/678 34.5 % 0.93 [ 0.76, 1.15 ]
Total (95% CI) 4721 4635 100.0 % 0.96 [ 0.84, 1.08 ]
Total events: 419 (Vitamin(s)), 433 (Control)
Heterogeneity: Chi2 = 4.99, df = 6 (P = 0.55); I2 =0.0%
Test for overall effect: Z = 0.70 (P = 0.48)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
117Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.13. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 13
Congenital malformations.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 13 Congenital malformations
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Czeizel 1994 7/2471 6/2391 22.1 % 1.13 [ 0.38, 3.35 ]
MRC 1991 27/1363 5/454 27.2 % 1.80 [ 0.70, 4.64 ]
Spinnato 2007 1/371 2/368 7.3 % 0.50 [ 0.05, 5.45 ]
Villar 2009 19/753 12/762 43.3 % 1.60 [ 0.78, 3.28 ]
Total (95% CI) 4958 3975 100.0 % 1.47 [ 0.90, 2.40 ]
Total events: 54 (Vitamin(s)), 25 (Control)
Heterogeneity: Chi2 = 1.25, df = 3 (P = 0.74); I2 =0.0%
Test for overall effect: Z = 1.54 (P = 0.12)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
118Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.14. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 14 Multiple
pregnancy.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 14 Multiple pregnancy
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
Czeizel 1994 2471 2391 0.3436 (0.1589) 44.4 % 1.41 [ 1.03, 1.93 ]
ICMR 2000 137 142 -1.0498 (1.1242) 0.9 % 0.35 [ 0.04, 3.17 ]
Katz 2000 10699 5146 0.3293 (0.1431) 54.7 % 1.39 [ 1.05, 1.84 ]
Total (95% CI) 13307 7679 100.0 % 1.38 [ 1.12, 1.70 ]
Heterogeneity: Chi2 = 1.51, df = 2 (P = 0.47); I2 =0.0%
Test for overall effect: Z = 3.06 (P = 0.0023)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours vitamins Favours control
Analysis 1.15. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 15 Apgar
score less than seven at five minutes.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 15 Apgar score less than seven at five minutes
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Spinnato 2007 8/351 12/349 100.0 % 0.66 [ 0.27, 1.60 ]
Total (95% CI) 351 349 100.0 % 0.66 [ 0.27, 1.60 ]
Total events: 8 (Vitamin(s)), 12 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.91 (P = 0.36)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
119Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.17. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 17 Anaemia
(maternal).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 17 Anaemia (maternal)
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Fawzi 1998 99/811 39/219 60.8 % 0.69 [ 0.49, 0.96 ]
Fleming 1986 15/80 11/80 39.2 % 1.36 [ 0.67, 2.78 ]
Total (95% CI) 891 299 100.0 % 0.90 [ 0.46, 1.73 ]
Total events: 114 (Vitamin(s)), 50 (Control)
Heterogeneity: Tau2 = 0.16; Chi2 = 2.92, df = 1 (P = 0.09); I2 =66%
Test for overall effect: Z = 0.32 (P = 0.75)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
Analysis 1.18. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 18 Anaemia
(infant).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 18 Anaemia (infant)
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Fawzi 1998 571/639 168/197 100.0 % 1.05 [ 0.98, 1.12 ]
Total (95% CI) 639 197 100.0 % 1.05 [ 0.98, 1.12 ]
Total events: 571 (Vitamin(s)), 168 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.43 (P = 0.15)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
120Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
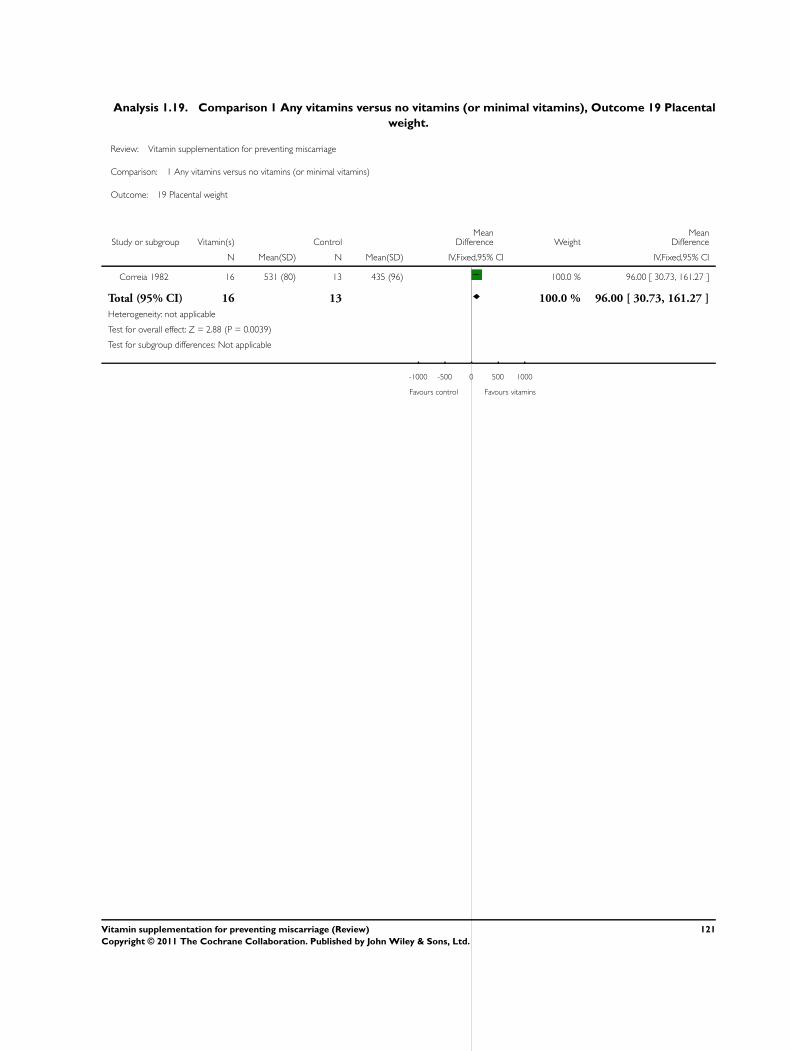
Analysis 1.19. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 19 Placental
weight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 19 Placental weight
Study or subgroup Vitamin(s) ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Correia 1982 16 531 (80) 13 435 (96) 100.0 % 96.00 [ 30.73, 161.27 ]
Total (95% CI) 16 13 100.0 % 96.00 [ 30.73, 161.27 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.88 (P = 0.0039)
Test for subgroup differences: Not applicable
-1000 -500 0 500 1000
Favours control Favours vitamins
121Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.20. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 20 Method
of feeding.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 20 Method of feeding
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Breastfeeding
People’s League 1942 2088/2443 2117/2435 100.0 % 0.98 [ 0.96, 1.01 ]
Subtotal (95% CI) 2443 2435 100.0 % 0.98 [ 0.96, 1.01 ]
Total events: 2088 (Vitamin(s)), 2117 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.49 (P = 0.14)
2 Formula
Subtotal (95% CI) 0 0 Not estimable
Total events: 0 (Vitamin(s)), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: not applicable
3 Breastfeeding and formula
Subtotal (95% CI) 0 0 Not estimable
Total events: 0 (Vitamin(s)), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: not applicable
Total (95% CI) 2443 2435 100.0 % 0.98 [ 0.96, 1.01 ]
Total events: 2088 (Vitamin(s)), 2117 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.49 (P = 0.14)
0.2 0.5 1 2 5
Favours control Favours vitamins
122Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
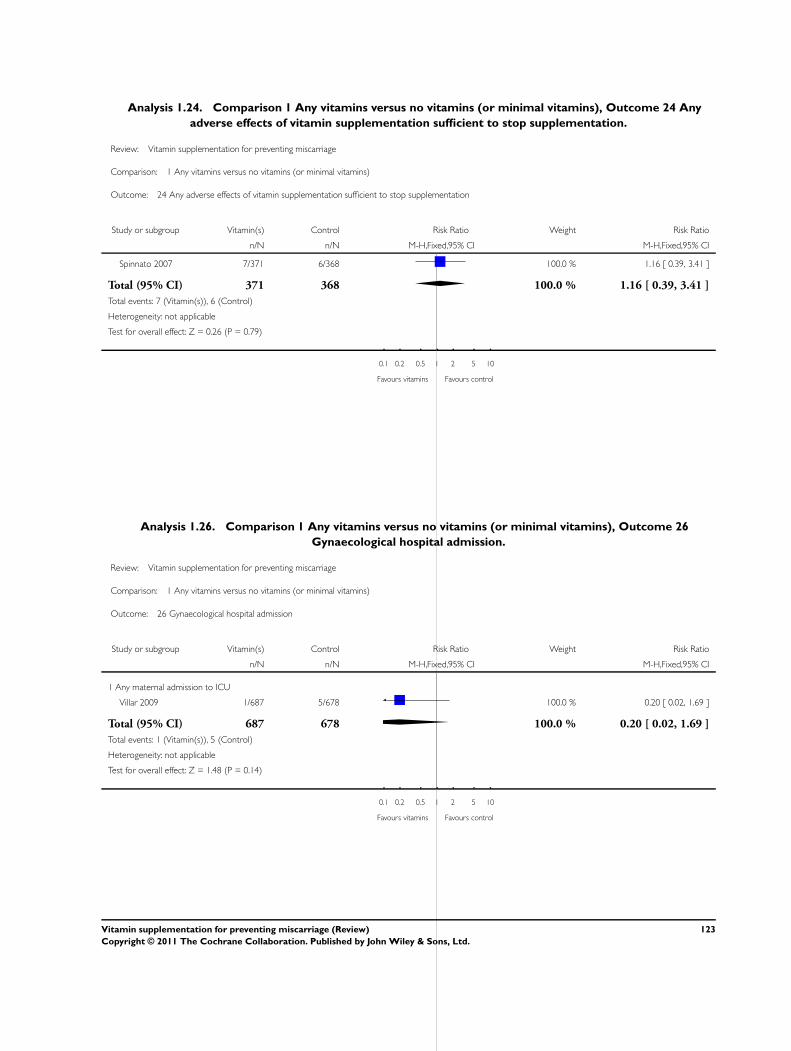
Analysis 1.24. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 24 Any
adverse effects of vitamin supplementation sufficient to stop supplementation.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 24 Any adverse effects of vitamin supplementation sufficient to stop supplementation
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Spinnato 2007 7/371 6/368 100.0 % 1.16 [ 0.39, 3.41 ]
Total (95% CI) 371 368 100.0 % 1.16 [ 0.39, 3.41 ]
Total events: 7 (Vitamin(s)), 6 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.26 (P = 0.79)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
Analysis 1.26. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 26
Gynaecological hospital admission.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 26 Gynaecological hospital admission
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Any maternal admission to ICU
Villar 2009 1/687 5/678 100.0 % 0.20 [ 0.02, 1.69 ]
Total (95% CI) 687 678 100.0 % 0.20 [ 0.02, 1.69 ]
Total events: 1 (Vitamin(s)), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.48 (P = 0.14)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
123Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
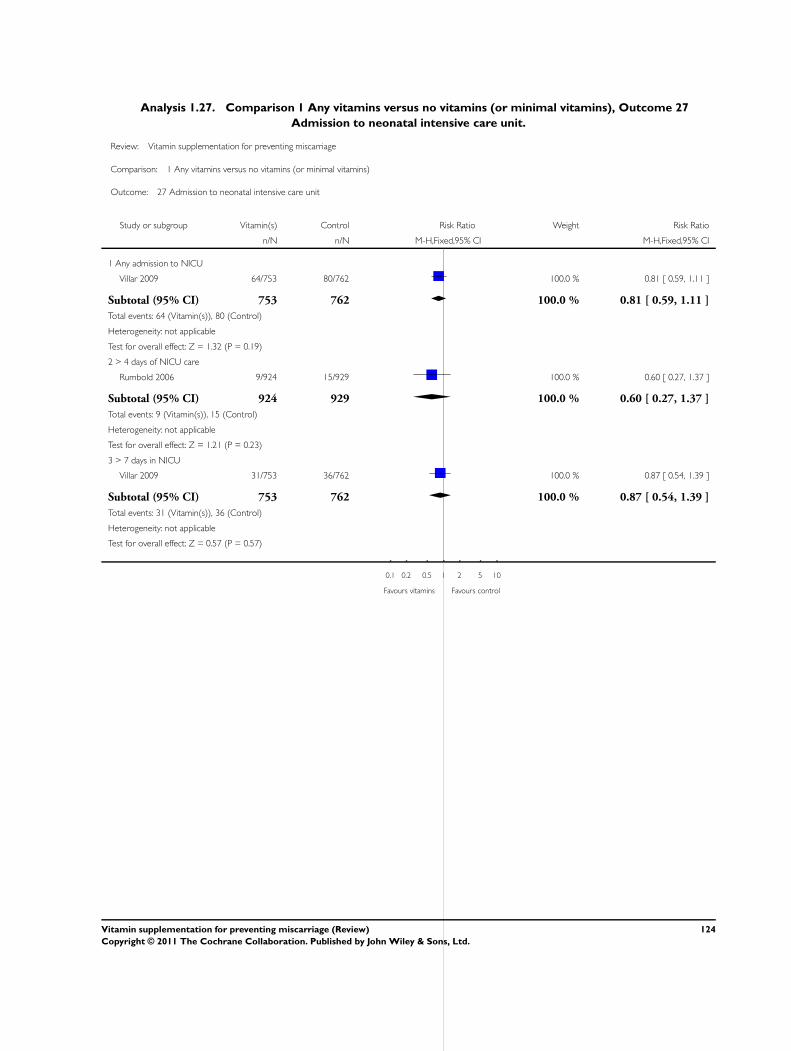
Analysis 1.27. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 27
Admission to neonatal intensive care unit.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 27 Admission to neonatal intensive care unit
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Any admission to NICU
Villar 2009 64/753 80/762 100.0 % 0.81 [ 0.59, 1.11 ]
Subtotal (95% CI) 753 762 100.0 % 0.81 [ 0.59, 1.11 ]
Total events: 64 (Vitamin(s)), 80 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.32 (P = 0.19)
2 > 4 days of NICU care
Rumbold 2006 9/924 15/929 100.0 % 0.60 [ 0.27, 1.37 ]
Subtotal (95% CI) 924 929 100.0 % 0.60 [ 0.27, 1.37 ]
Total events: 9 (Vitamin(s)), 15 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.21 (P = 0.23)
3 > 7 days in NICU
Villar 2009 31/753 36/762 100.0 % 0.87 [ 0.54, 1.39 ]
Subtotal (95% CI) 753 762 100.0 % 0.87 [ 0.54, 1.39 ]
Total events: 31 (Vitamin(s)), 36 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.57 (P = 0.57)
0.1 0.2 0.5 1 2 5 10
Favours vitamins Favours control
124Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.29. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 29 Duration
of admission to the neonatal intensive care unit.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 29 Duration of admission to the neonatal intensive care unit
Study or subgroup Vitamin(s) ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Steyn 2003 89 3.64 (5.6) 92 2.34 (5.2) 100.0 % 1.30 [ -0.28, 2.88 ]
Total (95% CI) 89 92 100.0 % 1.30 [ -0.28, 2.88 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.62 (P = 0.11)
Test for subgroup differences: Not applicable
-10 -5 0 5 10
Favours vitamins Favours control
Analysis 1.30. Comparison 1 Any vitamins versus no vitamins (or minimal vitamins), Outcome 30 Side
effects.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 1 Any vitamins versus no vitamins (or minimal vitamins)
Outcome: 30 Side effects
Study or subgroup Any vitamins Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Abdominal pain
Rumbold 2006 68/865 42/869 100.0 % 1.63 [ 1.12, 2.36 ]
Total (95% CI) 865 869 100.0 % 1.63 [ 1.12, 2.36 ]
Total events: 68 (Any vitamins), 42 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.56 (P = 0.011)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours experimental Favours control
125Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 Any vitamins (by quality), Outcome 1 Total fetal loss (including miscarriage or
combined miscarriages and stillbirths).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 2 Any vitamins (by quality)
Outcome: 1 Total fetal loss (including miscarriage or combined miscarriages and stillbirths)
Study or subgroup log [Relative risk] Relative risk Weight Relative risk
(SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Allocation concealment is adequate
Chappell 1999 -0.301 (0.6202) 1.5 % 0.74 [ 0.22, 2.50 ]
MRC 1991 -0.0362 (0.0834) 80.8 % 0.96 [ 0.82, 1.14 ]
Rumbold 2006 -0.1625 (0.4026) 3.5 % 0.85 [ 0.39, 1.87 ]
Spinnato 2007 -0.1744 (0.4038) 3.4 % 0.84 [ 0.38, 1.85 ]
Steyn 2003 0.1399 (0.2283) 10.8 % 1.15 [ 0.74, 1.80 ]
Total (95% CI) 100.0 % 0.97 [ 0.84, 1.12 ]
Heterogeneity: Chi2 = 0.99, df = 4 (P = 0.91); I2 =0.0%
Test for overall effect: Z = 0.40 (P = 0.69)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours vitamins Favours control
126Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.2. Comparison 2 Any vitamins (by quality), Outcome 2 Early or late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 2 Any vitamins (by quality)
Outcome: 2 Early or late miscarriage
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Allocation concealment is adequate
MRC 1991 126/1363 44/454 78.6 % 0.95 [ 0.69, 1.32 ]
Rumbold 2006 3/935 7/942 8.3 % 0.43 [ 0.11, 1.66 ]
Spinnato 2007 4/371 3/368 3.6 % 1.32 [ 0.30, 5.87 ]
Steyn 2003 10/100 8/100 9.5 % 1.25 [ 0.51, 3.04 ]
Total (95% CI) 2769 1864 100.0 % 0.95 [ 0.71, 1.27 ]
Total events: 143 (Vitamin(s)), 62 (Control)
Heterogeneity: Chi2 = 1.87, df = 3 (P = 0.60); I2 =0.0%
Test for overall effect: Z = 0.33 (P = 0.74)
0.01 0.1 1 10 100
Favours vitamins Favours control
127Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
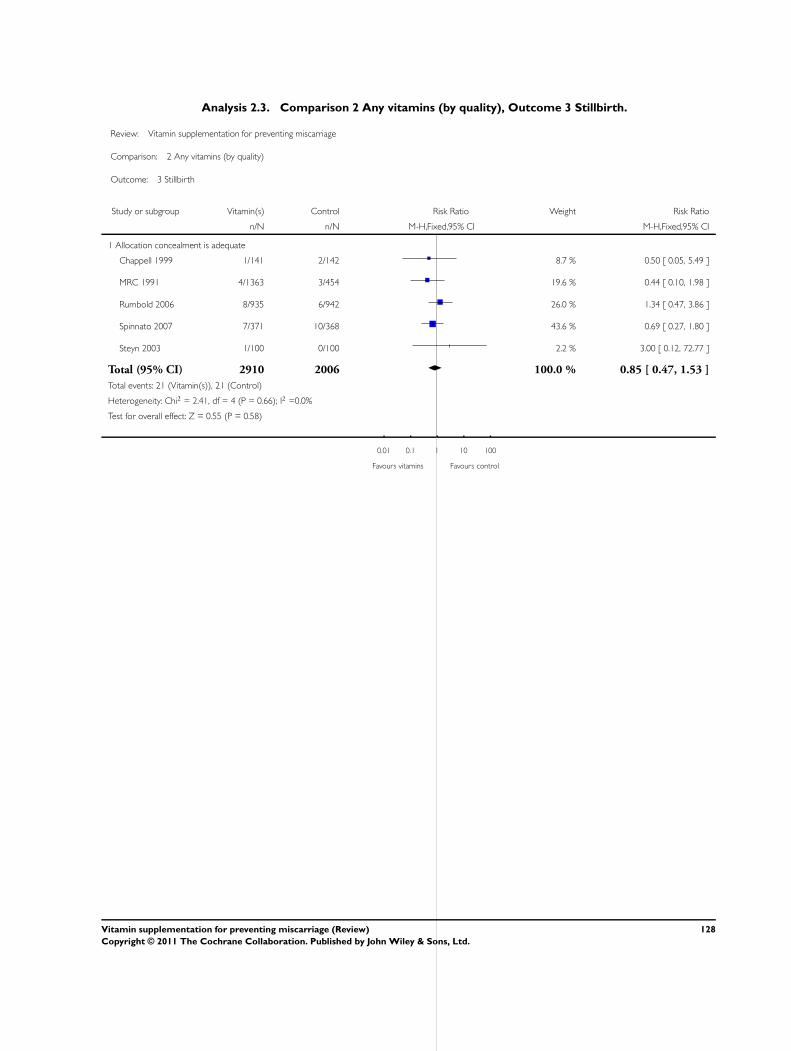
Analysis 2.3. Comparison 2 Any vitamins (by quality), Outcome 3 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 2 Any vitamins (by quality)
Outcome: 3 Stillbirth
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Allocation concealment is adequate
Chappell 1999 1/141 2/142 8.7 % 0.50 [ 0.05, 5.49 ]
MRC 1991 4/1363 3/454 19.6 % 0.44 [ 0.10, 1.98 ]
Rumbold 2006 8/935 6/942 26.0 % 1.34 [ 0.47, 3.86 ]
Spinnato 2007 7/371 10/368 43.6 % 0.69 [ 0.27, 1.80 ]
Steyn 2003 1/100 0/100 2.2 % 3.00 [ 0.12, 72.77 ]
Total (95% CI) 2910 2006 100.0 % 0.85 [ 0.47, 1.53 ]
Total events: 21 (Vitamin(s)), 21 (Control)
Heterogeneity: Chi2 = 2.41, df = 4 (P = 0.66); I2 =0.0%
Test for overall effect: Z = 0.55 (P = 0.58)
0.01 0.1 1 10 100
Favours vitamins Favours control
128Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Vitamin C, Outcome 1 Total fetal loss.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 1 Total fetal loss
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C + multivitamins versus placebo plus multivitamins
Briscoe 1959 31/303 8/103 100.0 % 1.32 [ 0.63, 2.77 ]
Subtotal (95% CI) 303 103 100.0 % 1.32 [ 0.63, 2.77 ]
Total events: 31 (Vitamin C), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.73 (P = 0.47)
2 Vitamin C and vitamin E versus placebo
Chappell 1999 1/141 2/142 7.1 % 0.50 [ 0.05, 5.49 ]
Rumbold 2006 11/935 13/942 46.3 % 0.85 [ 0.38, 1.89 ]
Spinnato 2007 11/371 13/368 46.6 % 0.84 [ 0.38, 1.85 ]
Subtotal (95% CI) 1447 1452 100.0 % 0.82 [ 0.48, 1.42 ]
Total events: 23 (Vitamin C), 28 (Control)
Heterogeneity: Chi2 = 0.17, df = 2 (P = 0.92); I2 =0.0%
Test for overall effect: Z = 0.71 (P = 0.48)
3 Vitamin C versus no supplement/placebo
Hemmi 2003 3/19 1/5 16.5 % 0.79 [ 0.10, 6.06 ]
Steyn 2003 11/100 8/100 83.5 % 1.38 [ 0.58, 3.27 ]
Subtotal (95% CI) 119 105 100.0 % 1.28 [ 0.58, 2.83 ]
Total events: 14 (Vitamin C), 9 (Control)
Heterogeneity: Chi2 = 0.24, df = 1 (P = 0.62); I2 =0.0%
Test for overall effect: Z = 0.60 (P = 0.55)
0.01 0.1 1 10 100
Favours vitamin C Favours control
129Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Vitamin C, Outcome 2 Early or late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 2 Early or late miscarriage
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C + multivitamins versus placebo plus multivitamins
Briscoe 1959 31/303 8/103 100.0 % 1.32 [ 0.63, 2.77 ]
Subtotal (95% CI) 303 103 100.0 % 1.32 [ 0.63, 2.77 ]
Total events: 31 (Vitamin C), 8 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.73 (P = 0.47)
2 Vitamin C and vitamin E versus placebo
Rumbold 2006 3/935 7/942 69.8 % 0.43 [ 0.11, 1.66 ]
Spinnato 2007 4/371 3/368 30.2 % 1.32 [ 0.30, 5.87 ]
Subtotal (95% CI) 1306 1310 100.0 % 0.70 [ 0.27, 1.84 ]
Total events: 7 (Vitamin C), 10 (Control)
Heterogeneity: Chi2 = 1.19, df = 1 (P = 0.27); I2 =16%
Test for overall effect: Z = 0.72 (P = 0.47)
3 Vitamin C versus no supplement/placebo
Hemmi 2003 3/19 1/5 16.5 % 0.79 [ 0.10, 6.06 ]
Steyn 2003 10/100 8/100 83.5 % 1.25 [ 0.51, 3.04 ]
Subtotal (95% CI) 119 105 100.0 % 1.17 [ 0.52, 2.65 ]
Total events: 13 (Vitamin C), 9 (Control)
Heterogeneity: Chi2 = 0.16, df = 1 (P = 0.68); I2 =0.0%
Test for overall effect: Z = 0.39 (P = 0.70)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
130Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
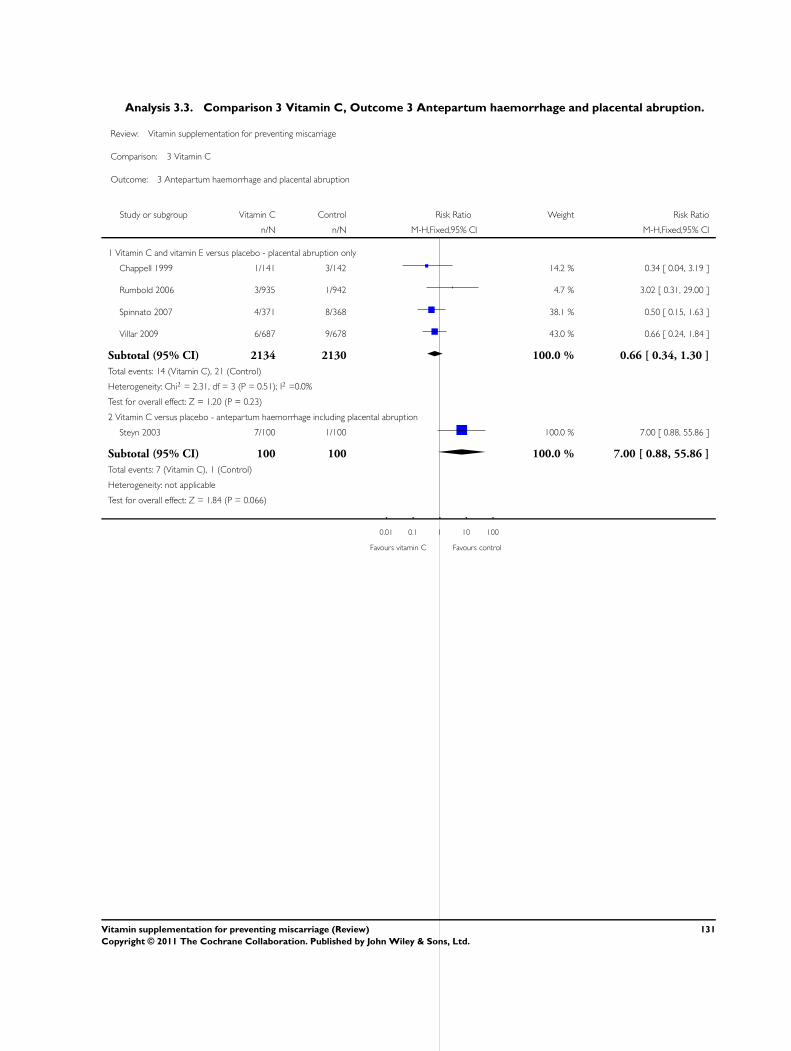
Analysis 3.3. Comparison 3 Vitamin C, Outcome 3 Antepartum haemorrhage and placental abruption.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 3 Antepartum haemorrhage and placental abruption
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo - placental abruption only
Chappell 1999 1/141 3/142 14.2 % 0.34 [ 0.04, 3.19 ]
Rumbold 2006 3/935 1/942 4.7 % 3.02 [ 0.31, 29.00 ]
Spinnato 2007 4/371 8/368 38.1 % 0.50 [ 0.15, 1.63 ]
Villar 2009 6/687 9/678 43.0 % 0.66 [ 0.24, 1.84 ]
Subtotal (95% CI) 2134 2130 100.0 % 0.66 [ 0.34, 1.30 ]
Total events: 14 (Vitamin C), 21 (Control)
Heterogeneity: Chi2 = 2.31, df = 3 (P = 0.51); I2 =0.0%
Test for overall effect: Z = 1.20 (P = 0.23)
2 Vitamin C versus placebo - antepartum haemorrhage including placental abruption
Steyn 2003 7/100 1/100 100.0 % 7.00 [ 0.88, 55.86 ]
Subtotal (95% CI) 100 100 100.0 % 7.00 [ 0.88, 55.86 ]
Total events: 7 (Vitamin C), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.84 (P = 0.066)
0.01 0.1 1 10 100
Favours vitamin C Favours control
131Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.4. Comparison 3 Vitamin C, Outcome 4 Pre-eclampsia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 4 Pre-eclampsia
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Vitamin C and vitamin E versus placebo
Chappell 1999 11/141 24/142 11.5 % 0.46 [ 0.24, 0.91 ]
Rumbold 2006 56/935 47/942 24.2 % 1.20 [ 0.82, 1.75 ]
Spinnato 2007 49/371 55/368 25.6 % 0.88 [ 0.62, 1.26 ]
Villar 2009 164/687 157/678 38.7 % 1.03 [ 0.85, 1.25 ]
Subtotal (95% CI) 2134 2130 100.0 % 0.94 [ 0.72, 1.22 ]
Total events: 280 (Vitamin C), 283 (Control)
Heterogeneity: Tau2 = 0.04; Chi2 = 6.48, df = 3 (P = 0.09); I2 =54%
Test for overall effect: Z = 0.48 (P = 0.63)
2 Vitamin C versus placebo
Steyn 2003 3/100 3/100 100.0 % 1.00 [ 0.21, 4.84 ]
Subtotal (95% CI) 100 100 100.0 % 1.00 [ 0.21, 4.84 ]
Total events: 3 (Vitamin C), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
0.01 0.1 1 10 100
Favours vitamin C Favours control
132Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
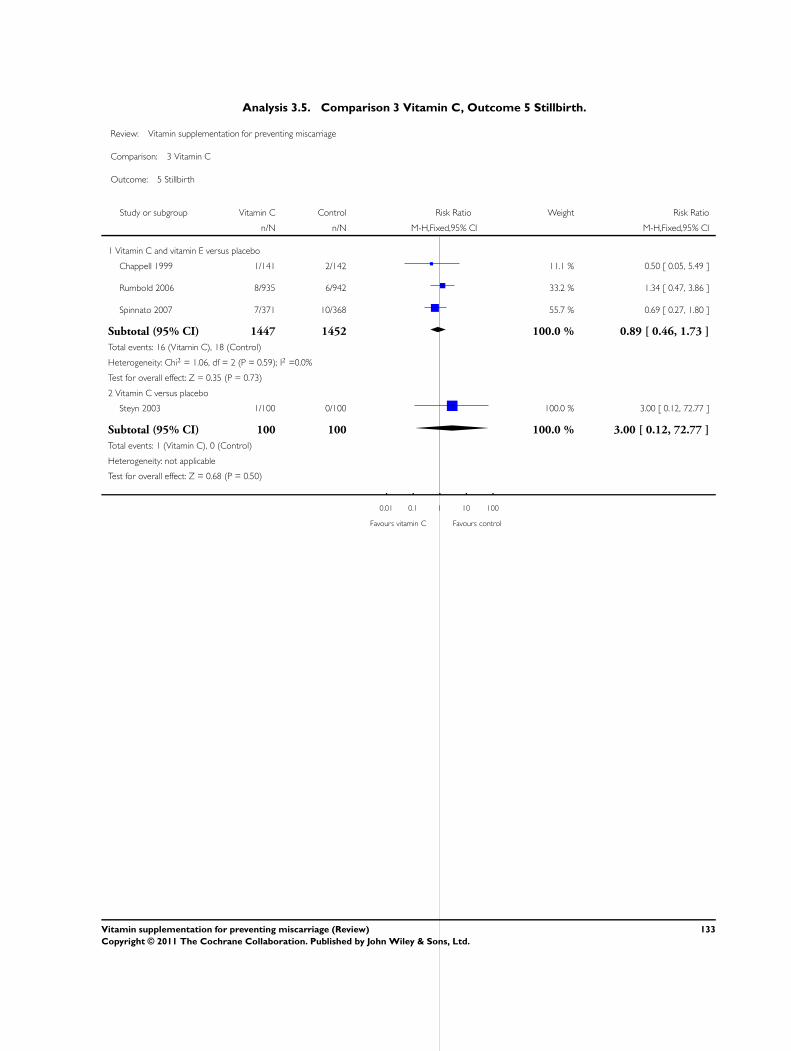
Analysis 3.5. Comparison 3 Vitamin C, Outcome 5 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 5 Stillbirth
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Chappell 1999 1/141 2/142 11.1 % 0.50 [ 0.05, 5.49 ]
Rumbold 2006 8/935 6/942 33.2 % 1.34 [ 0.47, 3.86 ]
Spinnato 2007 7/371 10/368 55.7 % 0.69 [ 0.27, 1.80 ]
Subtotal (95% CI) 1447 1452 100.0 % 0.89 [ 0.46, 1.73 ]
Total events: 16 (Vitamin C), 18 (Control)
Heterogeneity: Chi2 = 1.06, df = 2 (P = 0.59); I2 =0.0%
Test for overall effect: Z = 0.35 (P = 0.73)
2 Vitamin C versus placebo
Steyn 2003 1/100 0/100 100.0 % 3.00 [ 0.12, 72.77 ]
Subtotal (95% CI) 100 100 100.0 % 3.00 [ 0.12, 72.77 ]
Total events: 1 (Vitamin C), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
0.01 0.1 1 10 100
Favours vitamin C Favours control
133Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.6. Comparison 3 Vitamin C, Outcome 6 Perinatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 6 Perinatal death
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C versus placebo
Steyn 2003 1/90 2/92 2.1 % 0.51 [ 0.05, 5.54 ]
Subtotal (95% CI) 90 92 2.1 % 0.51 [ 0.05, 5.54 ]
Total events: 1 (Vitamin C), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
2 Vitamin C and vitamin E versus placebo
Rumbold 2006 9/935 10/942 10.4 % 0.91 [ 0.37, 2.22 ]
Spinnato 2007 13/371 16/368 16.8 % 0.81 [ 0.39, 1.65 ]
Villar 2009 56/753 68/762 70.7 % 0.83 [ 0.59, 1.17 ]
Subtotal (95% CI) 2059 2072 97.9 % 0.84 [ 0.63, 1.12 ]
Total events: 78 (Vitamin C), 94 (Control)
Heterogeneity: Chi2 = 0.04, df = 2 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 1.21 (P = 0.23)
Total (95% CI) 2149 2164 100.0 % 0.83 [ 0.62, 1.11 ]
Total events: 79 (Vitamin C), 96 (Control)
Heterogeneity: Chi2 = 0.20, df = 3 (P = 0.98); I2 =0.0%
Test for overall effect: Z = 1.27 (P = 0.20)
0.01 0.1 1 10 100
Favours vitamin C Favours control
134Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.7. Comparison 3 Vitamin C, Outcome 7 Neonatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 7 Neonatal death
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C versus placebo
Steyn 2003 2/89 3/92 22.7 % 0.69 [ 0.12, 4.03 ]
Subtotal (95% CI) 89 92 22.7 % 0.69 [ 0.12, 4.03 ]
Total events: 2 (Vitamin C), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.41 (P = 0.68)
2 Vitamin C and E versus placebo
Rumbold 2006 1/924 4/929 30.7 % 0.25 [ 0.03, 2.24 ]
Spinnato 2007 6/344 6/339 46.6 % 0.99 [ 0.32, 3.03 ]
Subtotal (95% CI) 1268 1268 77.3 % 0.69 [ 0.27, 1.81 ]
Total events: 7 (Vitamin C), 10 (Control)
Heterogeneity: Chi2 = 1.20, df = 1 (P = 0.27); I2 =17%
Test for overall effect: Z = 0.75 (P = 0.46)
Total (95% CI) 1357 1360 100.0 % 0.69 [ 0.30, 1.61 ]
Total events: 9 (Vitamin C), 13 (Control)
Heterogeneity: Chi2 = 1.20, df = 2 (P = 0.55); I2 =0.0%
Test for overall effect: Z = 0.85 (P = 0.39)
0.01 0.1 1 10 100
Favours vitamin C Favours control
135Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.8. Comparison 3 Vitamin C, Outcome 8 Preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 8 Preterm birth
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Chappell 1999 6/141 5/142 1.4 % 1.21 [ 0.38, 3.87 ]
Rumbold 2006 64/935 63/942 17.2 % 1.02 [ 0.73, 1.43 ]
Spinnato 2007 96/371 82/368 22.6 % 1.16 [ 0.90, 1.50 ]
Villar 2009 188/687 213/678 58.8 % 0.87 [ 0.74, 1.03 ]
Subtotal (95% CI) 2134 2130 100.0 % 0.97 [ 0.85, 1.10 ]
Total events: 354 (Vitamin C), 363 (Control)
Heterogeneity: Chi2 = 3.74, df = 3 (P = 0.29); I2 =20%
Test for overall effect: Z = 0.51 (P = 0.61)
2 Vitamin C versus placebo
Steyn 2003 50/100 35/100 100.0 % 1.43 [ 1.03, 1.99 ]
Subtotal (95% CI) 100 100 100.0 % 1.43 [ 1.03, 1.99 ]
Total events: 50 (Vitamin C), 35 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.11 (P = 0.035)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
136Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.9. Comparison 3 Vitamin C, Outcome 9 Very preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 9 Very preterm birth
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C versus placebo
Steyn 2003 26/100 20/100 12.6 % 1.30 [ 0.78, 2.17 ]
Subtotal (95% CI) 100 100 12.6 % 1.30 [ 0.78, 2.17 ]
Total events: 26 (Vitamin C), 20 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.00 (P = 0.32)
2 Vitamin C and vitamin E versus placebo
Rumbold 2006 20/935 19/942 11.9 % 1.06 [ 0.57, 1.97 ]
Spinnato 2007 29/371 26/368 16.5 % 1.11 [ 0.66, 1.84 ]
Villar 2009 73/687 93/678 59.0 % 0.77 [ 0.58, 1.03 ]
Subtotal (95% CI) 1993 1988 87.4 % 0.88 [ 0.70, 1.10 ]
Total events: 122 (Vitamin C), 138 (Control)
Heterogeneity: Chi2 = 1.87, df = 2 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 1.12 (P = 0.26)
Total (95% CI) 2093 2088 100.0 % 0.93 [ 0.75, 1.15 ]
Total events: 148 (Vitamin C), 158 (Control)
Heterogeneity: Chi2 = 3.81, df = 3 (P = 0.28); I2 =21%
Test for overall effect: Z = 0.68 (P = 0.50)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
137Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.10. Comparison 3 Vitamin C, Outcome 10 Small-for-gestational age.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 10 Small-for-gestational age
Study or subgroup Vitamin C Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Chappell 1999 33/141 45/142 13.4 % 0.74 [ 0.50, 1.08 ]
Rumbold 2006 80/935 92/942 27.3 % 0.88 [ 0.66, 1.17 ]
Spinnato 2007 49/356 49/352 14.7 % 0.99 [ 0.68, 1.43 ]
Villar 2009 141/687 149/678 44.7 % 0.93 [ 0.76, 1.15 ]
Total (95% CI) 2119 2114 100.0 % 0.90 [ 0.78, 1.04 ]
Total events: 303 (Vitamin C), 335 (Control)
Heterogeneity: Chi2 = 1.43, df = 3 (P = 0.70); I2 =0.0%
Test for overall effect: Z = 1.46 (P = 0.14)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
138Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.11. Comparison 3 Vitamin C, Outcome 11 Birthweight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 11 Birthweight
Study or subgroup Vitamin C ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Rumbold 2006 924 3392 (599) 929 3386 (584) 81.7 % 6.00 [ -47.87, 59.87 ]
Spinnato 2007 356 3019.7 (779.3) 352 3039.7 (767.5) 18.3 % -20.00 [ -133.94, 93.94 ]
Total (95% CI) 1280 1281 100.0 % 1.25 [ -47.45, 49.95 ]
Heterogeneity: Chi2 = 0.16, df = 1 (P = 0.69); I2 =0.0%
Test for overall effect: Z = 0.05 (P = 0.96)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours experimental Favours control
Analysis 3.12. Comparison 3 Vitamin C, Outcome 12 Congenital malformations.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 12 Congenital malformations
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Spinnato 2007 1/371 2/368 14.4 % 0.50 [ 0.05, 5.45 ]
Villar 2009 19/753 12/762 85.6 % 1.60 [ 0.78, 3.28 ]
Total (95% CI) 1124 1130 100.0 % 1.44 [ 0.73, 2.84 ]
Total events: 20 (Vitamin(s)), 14 (Control)
Heterogeneity: Chi2 = 0.85, df = 1 (P = 0.36); I2 =0.0%
Test for overall effect: Z = 1.06 (P = 0.29)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
139Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.13. Comparison 3 Vitamin C, Outcome 13 Apgar score less than seven at five minutes.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 13 Apgar score less than seven at five minutes
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Spinnato 2007 8/351 12/349 100.0 % 0.66 [ 0.27, 1.60 ]
Total (95% CI) 351 349 100.0 % 0.66 [ 0.27, 1.60 ]
Total events: 8 (Vitamin(s)), 12 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.91 (P = 0.36)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
140Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.14. Comparison 3 Vitamin C, Outcome 14 Any adverse effects of vitamin supplementation
sufficient to stop supplementation.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 14 Any adverse effects of vitamin supplementation sufficient to stop supplementation
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo
Spinnato 2007 7/371 6/368 100.0 % 1.16 [ 0.39, 3.41 ]
Total (95% CI) 371 368 100.0 % 1.16 [ 0.39, 3.41 ]
Total events: 7 (Vitamin(s)), 6 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.26 (P = 0.79)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
Analysis 3.15. Comparison 3 Vitamin C, Outcome 15 Gynaecological hospital admission.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 15 Gynaecological hospital admission
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo: Any maternal admission to ICU
Villar 2009 1/687 5/678 100.0 % 0.20 [ 0.02, 1.69 ]
Total (95% CI) 687 678 100.0 % 0.20 [ 0.02, 1.69 ]
Total events: 1 (Vitamin(s)), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.48 (P = 0.14)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
141Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.16. Comparison 3 Vitamin C, Outcome 16 Admission to neonatal intensive care unit.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 16 Admission to neonatal intensive care unit
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo: Any admission to NICU
Villar 2009 64/753 80/762 100.0 % 0.81 [ 0.59, 1.11 ]
Subtotal (95% CI) 753 762 100.0 % 0.81 [ 0.59, 1.11 ]
Total events: 64 (Vitamin(s)), 80 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.32 (P = 0.19)
2 Vitamin C and vitamin E versus placebo: > 4 days of NICU care
Rumbold 2006 9/924 15/929 100.0 % 0.60 [ 0.27, 1.37 ]
Subtotal (95% CI) 924 929 100.0 % 0.60 [ 0.27, 1.37 ]
Total events: 9 (Vitamin(s)), 15 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.21 (P = 0.23)
3 Vitamin C and vitamin E versus placebo: > 7 days of NICU care
Villar 2009 31/753 36/762 100.0 % 0.87 [ 0.54, 1.39 ]
Subtotal (95% CI) 753 762 100.0 % 0.87 [ 0.54, 1.39 ]
Total events: 31 (Vitamin(s)), 36 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.57 (P = 0.57)
0.1 0.2 0.5 1 2 5 10
Favours vitamin C Favours control
142Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
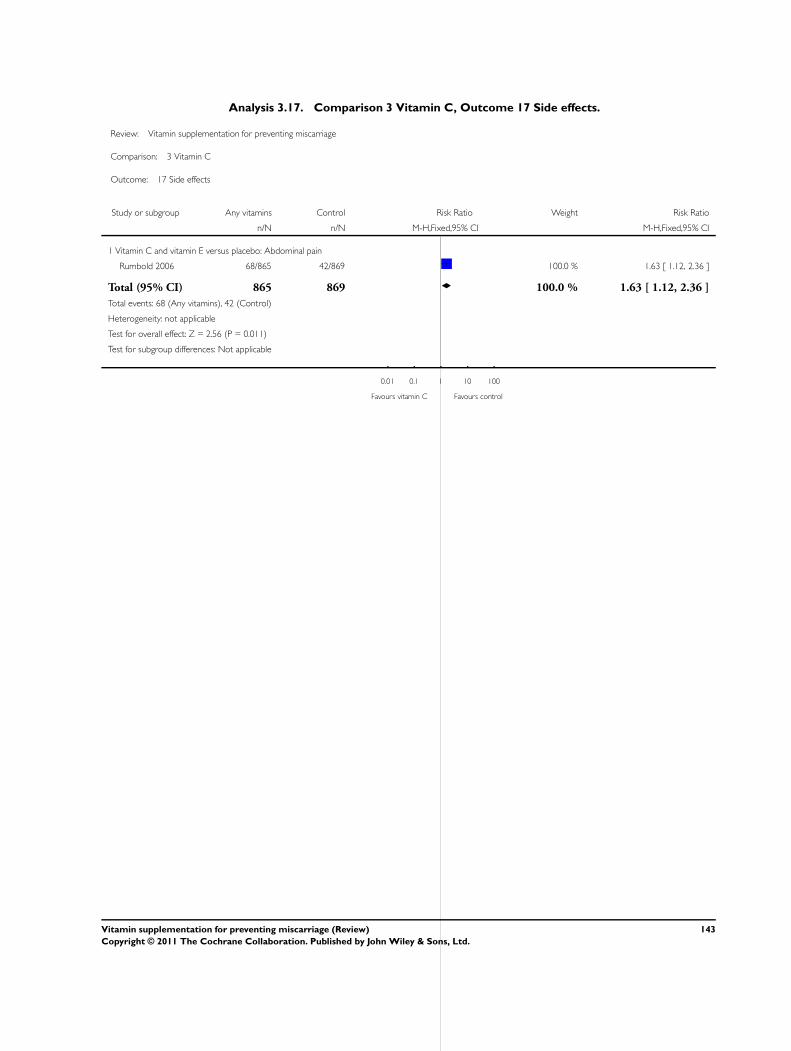
Analysis 3.17. Comparison 3 Vitamin C, Outcome 17 Side effects.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 3 Vitamin C
Outcome: 17 Side effects
Study or subgroup Any vitamins Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin C and vitamin E versus placebo: Abdominal pain
Rumbold 2006 68/865 42/869 100.0 % 1.63 [ 1.12, 2.36 ]
Total (95% CI) 865 869 100.0 % 1.63 [ 1.12, 2.36 ]
Total events: 68 (Any vitamins), 42 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.56 (P = 0.011)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours vitamin C Favours control
143Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Vitamin A, Outcome 1 Total fetal loss (including miscarriages or combined
miscarriages and stillbirths).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 1 Total fetal loss (including miscarriages or combined miscarriages and stillbirths)
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin A versus placebo
Katz 2000 6070 5653 0.0392 (0.0613) 100.0 % 1.04 [ 0.92, 1.17 ]
Subtotal (95% CI) 6070 5653 100.0 % 1.04 [ 0.92, 1.17 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.64 (P = 0.52)
2 B-carotene versus placebo
Katz 2000 5650 5653 0.0296 (0.0613) 100.0 % 1.03 [ 0.91, 1.16 ]
Subtotal (95% CI) 5650 5653 100.0 % 1.03 [ 0.91, 1.16 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.48 (P = 0.63)
3 Vitamin A versus B-carotene
Katz 2000 6070 5650 0.01 (0.0609) 100.0 % 1.01 [ 0.90, 1.14 ]
Subtotal (95% CI) 6070 5650 100.0 % 1.01 [ 0.90, 1.14 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.16 (P = 0.87)
4 Vitamin A or B-carotene versus placebo
Katz 2000 11720 5653 0.0488 (0.0706) 100.0 % 1.05 [ 0.91, 1.21 ]
Subtotal (95% CI) 11720 5653 100.0 % 1.05 [ 0.91, 1.21 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.69 (P = 0.49)
5 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 538 536 -0.2231 (0.2106) 100.0 % 0.80 [ 0.53, 1.21 ]
Subtotal (95% CI) 538 536 100.0 % 0.80 [ 0.53, 1.21 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
6 Vitamin A + iron + folate versus iron + folate
Kumwenda 2002 340 357 0.3577 (0.3883) 42.6 % 1.43 [ 0.67, 3.06 ]
Schmidt 2001 122 121 -0.0101 (0.8118) 9.8 % 0.99 [ 0.20, 4.86 ]
Van den Broek 2006 468 232 -0.3011 (0.3674) 47.6 % 0.74 [ 0.36, 1.52 ]
Subtotal (95% CI) 930 710 100.0 % 1.01 [ 0.61, 1.66 ]
Heterogeneity: Chi2 = 1.52, df = 2 (P = 0.47); I2 =0.0%
Test for overall effect: Z = 0.03 (P = 0.97)
Test for subgroup differences: Chi2 = 1.63, df = 5 (P = 0.90), I2 =0.0%
0.01 0.1 1 10 100
Favours vitamin A Favours control
144Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.2. Comparison 4 Vitamin A, Outcome 2 Early or late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 2 Early or late miscarriage
Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 13/539 17/536 100.0 % 0.76 [ 0.37, 1.55 ]
Subtotal (95% CI) 539 536 100.0 % 0.76 [ 0.37, 1.55 ]
Total events: 13 (Vitamin A), 17 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.75 (P = 0.45)
2 Vitamin A + iron + folate versus iron + folate
Kumwenda 2002 7/340 5/357 24.9 % 1.47 [ 0.47, 4.59 ]
Van den Broek 2006 15/468 11/232 75.1 % 0.68 [ 0.32, 1.45 ]
Subtotal (95% CI) 808 589 100.0 % 0.87 [ 0.47, 1.63 ]
Total events: 22 (Vitamin A), 16 (Control)
Heterogeneity: Chi2 = 1.24, df = 1 (P = 0.27); I2 =19%
Test for overall effect: Z = 0.42 (P = 0.67)
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
145Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.3. Comparison 4 Vitamin A, Outcome 3 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 3 Stillbirth
Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 25/539 24/536 100.0 % 1.04 [ 0.60, 1.79 ]
Subtotal (95% CI) 539 536 100.0 % 1.04 [ 0.60, 1.79 ]
Total events: 25 (Vitamin A), 24 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.13 (P = 0.90)
2 Vitamin A + iron + folate versus iron + folate
Kumwenda 2002 8/340 6/357 57.4 % 1.40 [ 0.49, 3.99 ]
Schmidt 2001 3/122 3/121 29.5 % 0.99 [ 0.20, 4.82 ]
Van den Broek 2006 3/468 1/232 13.1 % 1.49 [ 0.16, 14.22 ]
Subtotal (95% CI) 930 710 100.0 % 1.29 [ 0.57, 2.91 ]
Total events: 14 (Vitamin A), 10 (Control)
Heterogeneity: Chi2 = 0.14, df = 2 (P = 0.93); I2 =0.0%
Test for overall effect: Z = 0.62 (P = 0.54)
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
146Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.4. Comparison 4 Vitamin A, Outcome 4 Neonatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 4 Neonatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin A versus placebo
Katz 2000 5327 4887 0.0862 (0.0882) 100.0 % 1.09 [ 0.92, 1.30 ]
Subtotal (95% CI) 5327 4887 100.0 % 1.09 [ 0.92, 1.30 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.98 (P = 0.33)
2 B-carotene versus placebo
Katz 2000 4901 4887 0.0862 (0.091) 100.0 % 1.09 [ 0.91, 1.30 ]
Subtotal (95% CI) 4901 4887 100.0 % 1.09 [ 0.91, 1.30 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
3 Vitamin A versus B-carotene
Katz 2000 5327 4901 0 (0.0858) 100.0 % 1.00 [ 0.85, 1.18 ]
Subtotal (95% CI) 5327 4901 100.0 % 1.00 [ 0.85, 1.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
4 Vitamin A or B-carotene versus placebo
Katz 2000 10228 4887 0.0862 (0.091) 100.0 % 1.09 [ 0.91, 1.30 ]
Subtotal (95% CI) 10228 4887 100.0 % 1.09 [ 0.91, 1.30 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
Test for subgroup differences: Chi2 = 0.74, df = 3 (P = 0.86), I2 =0.0%
0.001 0.01 0.1 1 10 100 1000
Favours vitamin A Favours control
147Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.5. Comparison 4 Vitamin A, Outcome 5 Preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 5 Preterm birth
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin A versus placebo
Katz 2000 6070 5653 0.0392 (0.0784) 100.0 % 1.04 [ 0.89, 1.21 ]
Subtotal (95% CI) 6070 5653 100.0 % 1.04 [ 0.89, 1.21 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.50 (P = 0.62)
2 B-carotene versus placebo
Katz 2000 5650 5653 0.01 (0.0807) 100.0 % 1.01 [ 0.86, 1.18 ]
Subtotal (95% CI) 5650 5653 100.0 % 1.01 [ 0.86, 1.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.12 (P = 0.90)
3 Vitamin A versus B-carotene
Katz 2000 6070 5650 0.0296 (0.0791) 100.0 % 1.03 [ 0.88, 1.20 ]
Subtotal (95% CI) 6070 5650 100.0 % 1.03 [ 0.88, 1.20 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.37 (P = 0.71)
4 Vitamin A or B-carotene versus placebo
Katz 2000 11720 5653 0.0198 (0.0698) 100.0 % 1.02 [ 0.89, 1.17 ]
Subtotal (95% CI) 11720 5653 100.0 % 1.02 [ 0.89, 1.17 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
5 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 539 536 0.07 (0.1266) 100.0 % 1.07 [ 0.84, 1.37 ]
Subtotal (95% CI) 539 536 100.0 % 1.07 [ 0.84, 1.37 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
6 Vitamin A + iron + folate versus iron + folate
Van den Broek 2006 468 232 0.1044 (0.3227) 100.0 % 1.11 [ 0.59, 2.09 ]
Subtotal (95% CI) 468 232 100.0 % 1.11 [ 0.59, 2.09 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.32 (P = 0.75)
Test for subgroup differences: Chi2 = 0.25, df = 5 (P = 1.00), I2 =0.0%
0.001 0.01 0.1 1 10 100 1000
Favours vitamin A Favours control
148Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
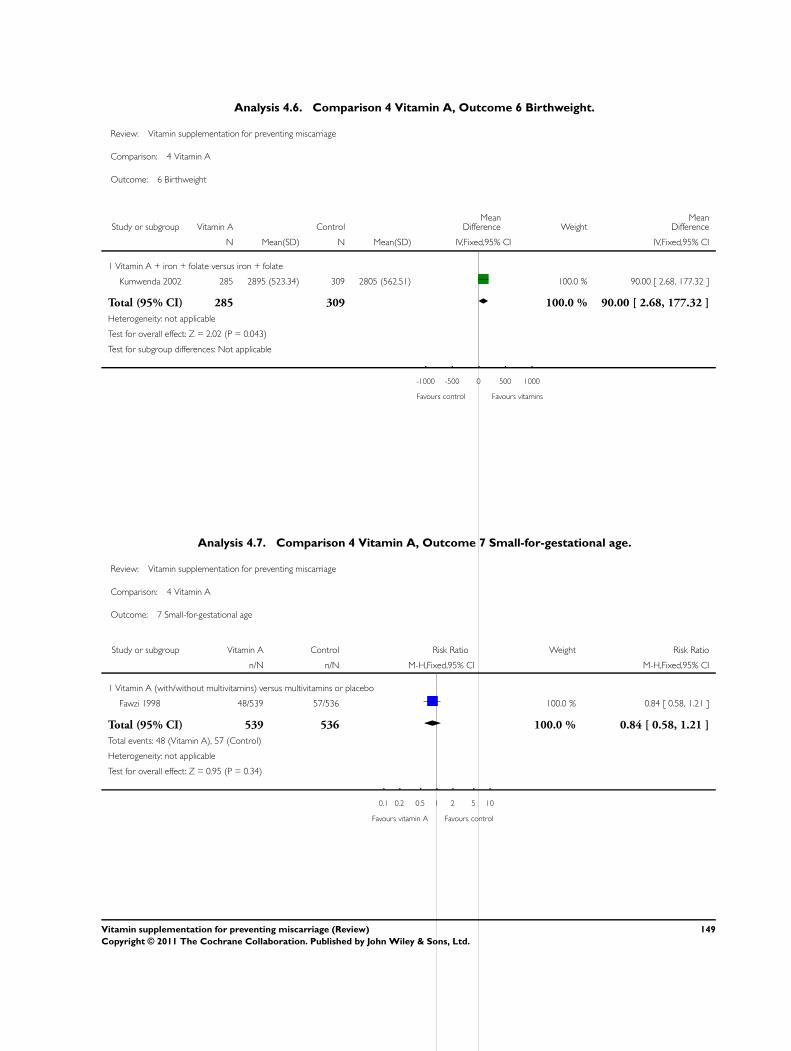
Analysis 4.6. Comparison 4 Vitamin A, Outcome 6 Birthweight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 6 Birthweight
Study or subgroup Vitamin A ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin A + iron + folate versus iron + folate
Kumwenda 2002 285 2895 (523.34) 309 2805 (562.51) 100.0 % 90.00 [ 2.68, 177.32 ]
Total (95% CI) 285 309 100.0 % 90.00 [ 2.68, 177.32 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.02 (P = 0.043)
Test for subgroup differences: Not applicable
-1000 -500 0 500 1000
Favours control Favours vitamins
Analysis 4.7. Comparison 4 Vitamin A, Outcome 7 Small-for-gestational age.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 7 Small-for-gestational age
Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 48/539 57/536 100.0 % 0.84 [ 0.58, 1.21 ]
Total (95% CI) 539 536 100.0 % 0.84 [ 0.58, 1.21 ]
Total events: 48 (Vitamin A), 57 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
149Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
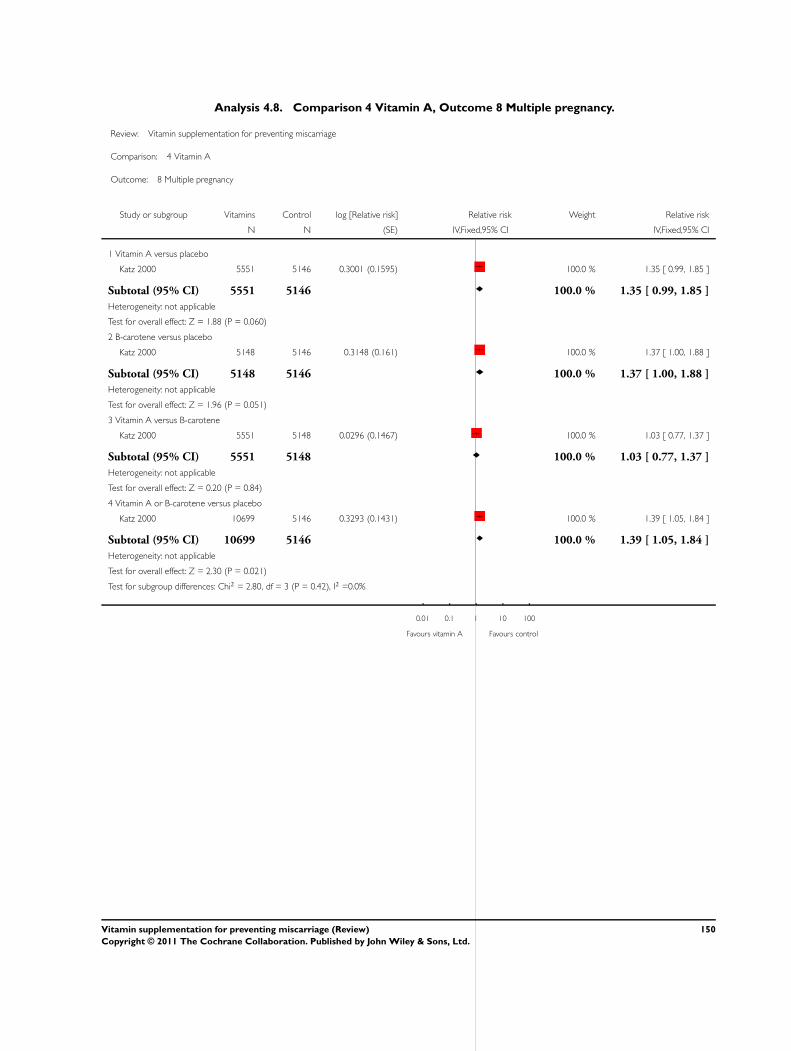
Analysis 4.8. Comparison 4 Vitamin A, Outcome 8 Multiple pregnancy.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 8 Multiple pregnancy
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Vitamin A versus placebo
Katz 2000 5551 5146 0.3001 (0.1595) 100.0 % 1.35 [ 0.99, 1.85 ]
Subtotal (95% CI) 5551 5146 100.0 % 1.35 [ 0.99, 1.85 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.88 (P = 0.060)
2 B-carotene versus placebo
Katz 2000 5148 5146 0.3148 (0.161) 100.0 % 1.37 [ 1.00, 1.88 ]
Subtotal (95% CI) 5148 5146 100.0 % 1.37 [ 1.00, 1.88 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.96 (P = 0.051)
3 Vitamin A versus B-carotene
Katz 2000 5551 5148 0.0296 (0.1467) 100.0 % 1.03 [ 0.77, 1.37 ]
Subtotal (95% CI) 5551 5148 100.0 % 1.03 [ 0.77, 1.37 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.20 (P = 0.84)
4 Vitamin A or B-carotene versus placebo
Katz 2000 10699 5146 0.3293 (0.1431) 100.0 % 1.39 [ 1.05, 1.84 ]
Subtotal (95% CI) 10699 5146 100.0 % 1.39 [ 1.05, 1.84 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.30 (P = 0.021)
Test for subgroup differences: Chi2 = 2.80, df = 3 (P = 0.42), I2 =0.0%
0.01 0.1 1 10 100
Favours vitamin A Favours control
150Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.9. Comparison 4 Vitamin A, Outcome 9 Very preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 9 Very preterm birth
Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin A (with/without multivitamins) versus multivitamins or placebo
Fawzi 1998 38/539 34/536 100.0 % 1.11 [ 0.71, 1.74 ]
Total (95% CI) 539 536 100.0 % 1.11 [ 0.71, 1.74 ]
Total events: 38 (Vitamin A), 34 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.46 (P = 0.64)
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
Analysis 4.10. Comparison 4 Vitamin A, Outcome 10 Maternal anaemia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 10 Maternal anaemia
Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Vitamin A + beta-carotene with or without multivitamin versus placebo
Fawzi 1998 68/540 39/267 100.0 % 0.86 [ 0.60, 1.24 ]
Subtotal (95% CI) 540 267 100.0 % 0.86 [ 0.60, 1.24 ]
Total events: 68 (Experimental), 39 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.80 (P = 0.43)
2 Vitamin A + beta-carotene versus placebo
Fawzi 1998 36/272 39/267 100.0 % 0.91 [ 0.60, 1.38 ]
Subtotal (95% CI) 272 267 100.0 % 0.91 [ 0.60, 1.38 ]
Total events: 36 (Experimental), 39 (Control)
0.01 0.1 1 10 100
Favours experimental Favours control
(Continued . . . )
151Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Experimental Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Heterogeneity: not applicable
Test for overall effect: Z = 0.46 (P = 0.65)
3 Vitamin A + iron and folic acid versus iron and folic acid
Van den Broek 2006 231/468 119/232 100.0 % 0.96 [ 0.82, 1.12 ]
Subtotal (95% CI) 468 232 100.0 % 0.96 [ 0.82, 1.12 ]
Total events: 231 (Experimental), 119 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.48 (P = 0.63)
0.01 0.1 1 10 100
Favours experimental Favours control
Analysis 4.11. Comparison 4 Vitamin A, Outcome 11 Infant anaemia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 11 Infant anaemia
Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Infant anaemia at 6 weeks’ of age - vitamin A + iron + folate versus iron + folate
Kumwenda 2002 64/273 117/289 100.0 % 0.58 [ 0.45, 0.75 ]
Subtotal (95% CI) 273 289 100.0 % 0.58 [ 0.45, 0.75 ]
Total events: 64 (Vitamin A), 117 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 4.18 (P = 0.000029)
2 Infant anaemia at 12 months - vitamin A + iron + folate versus iron + folate
Kumwenda 2002 129/227 139/251 100.0 % 1.03 [ 0.88, 1.20 ]
Subtotal (95% CI) 227 251 100.0 % 1.03 [ 0.88, 1.20 ]
Total events: 129 (Vitamin A), 139 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.32 (P = 0.75)
3 Infant anaemia - vitamin A + beta-carotene with or without multivitamins versus placebo
Fawzi 1998 362/428 168/197 100.0 % 0.99 [ 0.92, 1.06 ]
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
(Continued . . . )
152Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Vitamin A Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Subtotal (95% CI) 428 197 100.0 % 0.99 [ 0.92, 1.06 ]
Total events: 362 (Vitamin A), 168 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.23 (P = 0.82)
4 Infant anaemia - vitamin A + beta-carotene versus placebo
Fawzi 1998 177/209 168/197 100.0 % 0.99 [ 0.92, 1.08 ]
Subtotal (95% CI) 209 197 100.0 % 0.99 [ 0.92, 1.08 ]
Total events: 177 (Vitamin A), 168 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.17 (P = 0.87)
0.1 0.2 0.5 1 2 5 10
Favours vitamin A Favours control
Analysis 4.12. Comparison 4 Vitamin A, Outcome 12 Poor growth at childhood follow up.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 4 Vitamin A
Outcome: 12 Poor growth at childhood follow up
Study or subgroup Vitamin A ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Weight (g) at 6 weeks: vitamin A + iron + folate versus iron + folate
Kumwenda 2002 273 4627 (908.75) 273 4458 (908.75) 100.0 % 169.00 [ 16.55, 321.45 ]
Subtotal (95% CI) 273 273 100.0 % 169.00 [ 16.55, 321.45 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.17 (P = 0.030)
2 Length (cm) at 6 weeks: vitamin A + iron + folate versus iron + folate
Kumwenda 2002 273 53.7 (3.3) 273 53 (3.3) 100.0 % 0.70 [ 0.15, 1.25 ]
Subtotal (95% CI) 273 273 100.0 % 0.70 [ 0.15, 1.25 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.48 (P = 0.013)
3 Weight (g) at 4 months: vitamin A + iron + folate versus iron + folate
-1000 -500 0 500 1000
Favours control Favours vitamin A
(Continued . . . )
153Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)
Study or subgroup Vitamin A ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Schmidt 2001 72 6100 (850) 76 6200 (870) 100.0 % -100.00 [ -377.14, 177.14 ]
Subtotal (95% CI) 72 76 100.0 % -100.00 [ -377.14, 177.14 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.71 (P = 0.48)
4 Length (cm) at 4 months: vitamin A + iron + folate versus iron + folate
Schmidt 2001 72 60.7 (2.55) 76 61.2 (2.62) 100.0 % -0.50 [ -1.33, 0.33 ]
Subtotal (95% CI) 72 76 100.0 % -0.50 [ -1.33, 0.33 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.18 (P = 0.24)
Test for subgroup differences: Chi2 = 10.74, df = 3 (P = 0.01), I2 =72%
-1000 -500 0 500 1000
Favours control Favours vitamin A
154Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.1. Comparison 5 Multivitamin, Outcome 1 Total fetal loss (including miscarriages or combined
miscarriages and stillbirths).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 1 Total fetal loss (including miscarriages or combined miscarriages and stillbirths)
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 312/2819 260/2683 57.8 % 1.14 [ 0.98, 1.33 ]
ICMR 2000 9/231 17/235 11.1 % 0.54 [ 0.25, 1.18 ]
MRC 1991 47/461 47/454 31.0 % 0.98 [ 0.67, 1.44 ]
Subtotal (95% CI) 3511 3372 100.0 % 1.00 [ 0.75, 1.34 ]
Total events: 368 (Multivitamin), 324 (Control)
Heterogeneity: Tau2 = 0.03; Chi2 = 3.70, df = 2 (P = 0.16); I2 =46%
Test for overall effect: Z = 0.02 (P = 0.98)
2 Multivitamin without folic acid versus no multivitamin/folic acid
MRC 1991 39/453 47/454 100.0 % 0.83 [ 0.56, 1.25 ]
Subtotal (95% CI) 453 454 100.0 % 0.83 [ 0.56, 1.25 ]
Total events: 39 (Multivitamin), 47 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.89 (P = 0.37)
3 Multivitamins with/without folic acid versus no multivitamins/folic acid
MRC 1991 86/914 47/454 100.0 % 0.91 [ 0.65, 1.27 ]
Subtotal (95% CI) 914 454 100.0 % 0.91 [ 0.65, 1.27 ]
Total events: 86 (Multivitamin), 47 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.56 (P = 0.58)
4 Multivitamin + folic acid versus folic acid
Kirke 1992 9/93 9/93 16.5 % 1.00 [ 0.42, 2.41 ]
MRC 1991 47/461 44/449 83.5 % 1.04 [ 0.70, 1.54 ]
Subtotal (95% CI) 554 542 100.0 % 1.03 [ 0.72, 1.48 ]
Total events: 56 (Multivitamin), 53 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.01, df = 1 (P = 0.94); I2 =0.0%
Test for overall effect: Z = 0.18 (P = 0.86)
5 Multivitamin without folic acid versus folic acid
Kirke 1992 9/95 9/93 17.9 % 0.98 [ 0.41, 2.36 ]
MRC 1991 39/453 44/449 82.1 % 0.88 [ 0.58, 1.32 ]
0.5 0.7 1 1.5 2
Favours multivitamin Favours control
(Continued . . . )
155Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Subtotal (95% CI) 548 542 100.0 % 0.90 [ 0.62, 1.30 ]
Total events: 48 (Multivitamin), 53 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.05, df = 1 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 0.58 (P = 0.56)
6 Multivitamin with/without folic acid versus folic acid
Kirke 1992 16/188 9/93 16.5 % 0.88 [ 0.40, 1.91 ]
MRC 1991 86/914 44/449 83.5 % 0.96 [ 0.68, 1.36 ]
Subtotal (95% CI) 1102 542 100.0 % 0.95 [ 0.69, 1.30 ]
Total events: 102 (Multivitamin), 53 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.04, df = 1 (P = 0.84); I2 =0.0%
Test for overall effect: Z = 0.34 (P = 0.73)
7 Multivitamin with/without vitamin A versus vitamin A or placebo
Fawzi 1998 31/537 52/537 100.0 % 0.60 [ 0.39, 0.91 ]
Subtotal (95% CI) 537 537 100.0 % 0.60 [ 0.39, 0.91 ]
Total events: 31 (Multivitamin), 52 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.37 (P = 0.018)
8 Multivitamins versus control
People’s League 1942 57/2510 69/2511 100.0 % 0.83 [ 0.58, 1.17 ]
Subtotal (95% CI) 2510 2511 100.0 % 0.83 [ 0.58, 1.17 ]
Total events: 57 (Multivitamin), 69 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.08 (P = 0.28)
9 Multivitamin + vitamin E versus multivitamin without vitamin E or controls
Rush 1980 11/267 25/556 100.0 % 0.92 [ 0.46, 1.83 ]
Subtotal (95% CI) 267 556 100.0 % 0.92 [ 0.46, 1.83 ]
Total events: 11 (Multivitamin), 25 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
10 Multivitamins + iron + folic acid versus iron + folic acid
Fawzi 2007 184/4214 215/4214 34.7 % 0.86 [ 0.71, 1.04 ]
Osrin 2005 17/600 23/600 7.9 % 0.74 [ 0.40, 1.37 ]
Roberfroid 2008 37/714 27/712 11.8 % 1.37 [ 0.84, 2.22 ]
Rumiris 2006 0/29 9/31 0.4 % 0.06 [ 0.00, 0.92 ]
The Summit 2008 531/15804 579/15486 45.1 % 0.90 [ 0.80, 1.01 ]
Subtotal (95% CI) 21361 21043 100.0 % 0.90 [ 0.75, 1.09 ]
Total events: 769 (Multivitamin), 853 (Control)
Heterogeneity: Tau2 = 0.02; Chi2 = 7.28, df = 4 (P = 0.12); I2 =45%
Test for overall effect: Z = 1.07 (P = 0.29)
0.5 0.7 1 1.5 2
Favours multivitamin Favours control
156Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.2. Comparison 5 Multivitamin, Outcome 2 Early or late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 2 Early or late miscarriage
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 301/2819 251/2683 56.4 % 1.14 [ 0.97, 1.34 ]
ICMR 2000 6/231 14/235 10.2 % 0.44 [ 0.17, 1.11 ]
MRC 1991 45/461 44/454 33.4 % 1.01 [ 0.68, 1.49 ]
Subtotal (95% CI) 3511 3372 100.0 % 0.99 [ 0.72, 1.38 ]
Total events: 352 (Multivitamin), 309 (Control)
Heterogeneity: Tau2 = 0.04; Chi2 = 4.13, df = 2 (P = 0.13); I2 =52%
Test for overall effect: Z = 0.05 (P = 0.96)
2 Multivitamin without folic acid versus no multivitamin/folic acid
MRC 1991 39/453 44/454 100.0 % 0.89 [ 0.59, 1.34 ]
Subtotal (95% CI) 453 454 100.0 % 0.89 [ 0.59, 1.34 ]
Total events: 39 (Multivitamin), 44 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.56 (P = 0.57)
3 Multivitamin with/without folic acid versus no multivitamin/folic acid
MRC 1991 84/914 44/454 100.0 % 0.95 [ 0.67, 1.34 ]
Subtotal (95% CI) 914 454 100.0 % 0.95 [ 0.67, 1.34 ]
Total events: 84 (Multivitamin), 44 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.30 (P = 0.76)
4 Multivitamin + folic acid versus folic acid
Kirke 1992 9/93 9/93 17.2 % 1.00 [ 0.42, 2.41 ]
MRC 1991 45/461 42/449 82.8 % 1.04 [ 0.70, 1.56 ]
Subtotal (95% CI) 554 542 100.0 % 1.04 [ 0.72, 1.49 ]
Total events: 54 (Multivitamin), 51 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.01, df = 1 (P = 0.93); I2 =0.0%
Test for overall effect: Z = 0.19 (P = 0.85)
5 Multivitamin without folic acid versus folic acid
Kirke 1992 7/95 9/93 16.2 % 0.76 [ 0.30, 1.96 ]
0.1 0.2 0.5 1 2 5 10
Favours multivitamin Favours control
(Continued . . . )
157Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
MRC 1991 39/453 42/449 83.8 % 0.92 [ 0.61, 1.39 ]
Subtotal (95% CI) 548 542 100.0 % 0.89 [ 0.61, 1.31 ]
Total events: 46 (Multivitamin), 51 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.13, df = 1 (P = 0.72); I2 =0.0%
Test for overall effect: Z = 0.59 (P = 0.56)
6 Multivitamin with/without folic acid versus folic acid
Kirke 1992 16/188 9/93 17.1 % 0.88 [ 0.40, 1.91 ]
MRC 1991 84/914 42/449 82.9 % 0.98 [ 0.69, 1.40 ]
Subtotal (95% CI) 1102 542 100.0 % 0.96 [ 0.70, 1.33 ]
Total events: 100 (Multivitamin), 51 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.06, df = 1 (P = 0.80); I2 =0.0%
Test for overall effect: Z = 0.22 (P = 0.82)
7 Multivitamin + vitamin E versus multivitamin without vitamin E or controls
Rush 1980 3/267 6/556 100.0 % 1.04 [ 0.26, 4.13 ]
Subtotal (95% CI) 267 556 100.0 % 1.04 [ 0.26, 4.13 ]
Total events: 3 (Multivitamin), 6 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.06 (P = 0.95)
8 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 50/4214 52/4214 23.1 % 0.96 [ 0.65, 1.41 ]
Osrin 2005 2/600 5/600 1.6 % 0.40 [ 0.08, 2.05 ]
Roberfroid 2008 15/714 15/712 8.0 % 1.00 [ 0.49, 2.02 ]
Rumiris 2006 0/29 8/31 0.5 % 0.06 [ 0.00, 1.04 ]
The Summit 2008 286/15804 311/15486 66.7 % 0.90 [ 0.77, 1.06 ]
Subtotal (95% CI) 21361 21043 100.0 % 0.90 [ 0.73, 1.11 ]
Total events: 353 (Multivitamin), 391 (Control)
Heterogeneity: Tau2 = 0.01; Chi2 = 4.63, df = 4 (P = 0.33); I2 =14%
Test for overall effect: Z = 1.02 (P = 0.31)
0.1 0.2 0.5 1 2 5 10
Favours multivitamin Favours control
158Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
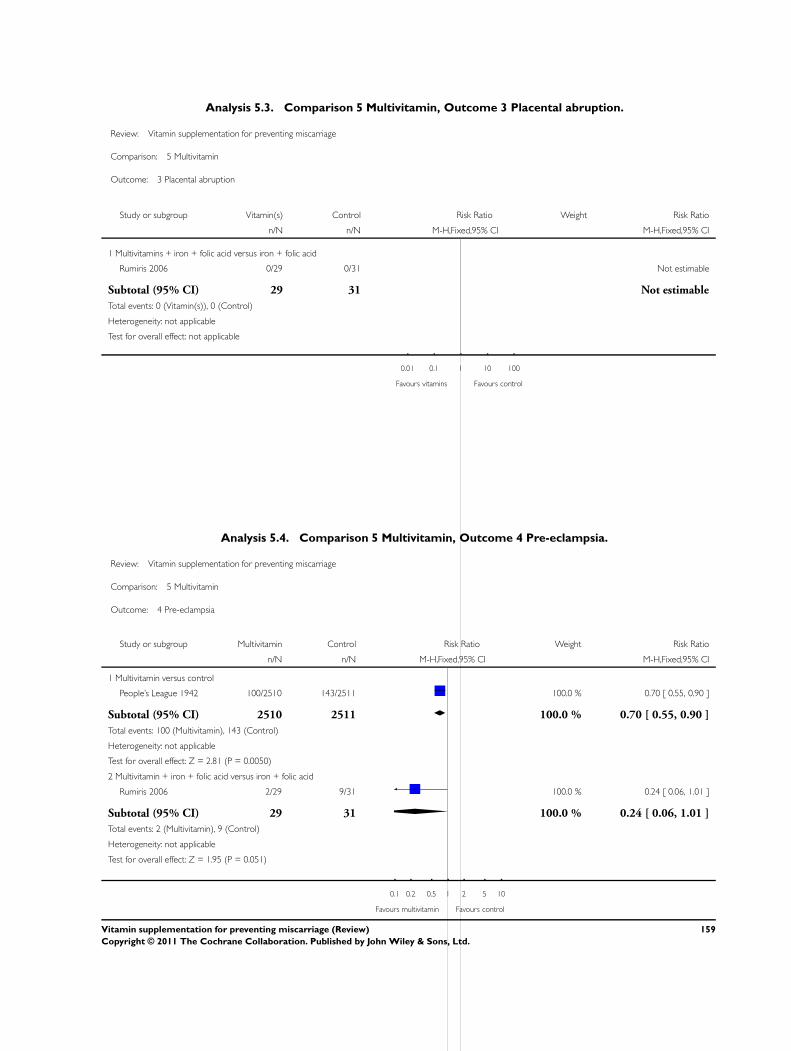
Analysis 5.3. Comparison 5 Multivitamin, Outcome 3 Placental abruption.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 3 Placental abruption
Study or subgroup Vitamin(s) Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamins + iron + folic acid versus iron + folic acid
Rumiris 2006 0/29 0/31 Not estimable
Subtotal (95% CI) 29 31 Not estimable
Total events: 0 (Vitamin(s)), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: not applicable
0.01 0.1 1 10 100
Favours vitamins Favours control
Analysis 5.4. Comparison 5 Multivitamin, Outcome 4 Pre-eclampsia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 4 Pre-eclampsia
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamin versus control
People’s League 1942 100/2510 143/2511 100.0 % 0.70 [ 0.55, 0.90 ]
Subtotal (95% CI) 2510 2511 100.0 % 0.70 [ 0.55, 0.90 ]
Total events: 100 (Multivitamin), 143 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.81 (P = 0.0050)
2 Multivitamin + iron + folic acid versus iron + folic acid
Rumiris 2006 2/29 9/31 100.0 % 0.24 [ 0.06, 1.01 ]
Subtotal (95% CI) 29 31 100.0 % 0.24 [ 0.06, 1.01 ]
Total events: 2 (Multivitamin), 9 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.95 (P = 0.051)
0.1 0.2 0.5 1 2 5 10
Favours multivitamin Favours control
159Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.5. Comparison 5 Multivitamin, Outcome 5 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 5 Stillbirth
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 11/2819 9/2683 64.6 % 1.16 [ 0.48, 2.80 ]
ICMR 2000 3/231 3/235 19.8 % 1.02 [ 0.21, 4.99 ]
MRC 1991 2/461 3/454 15.7 % 0.66 [ 0.11, 3.91 ]
Subtotal (95% CI) 3511 3372 100.0 % 1.04 [ 0.51, 2.10 ]
Total events: 16 (Multivitamin), 15 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.32, df = 2 (P = 0.85); I2 =0.0%
Test for overall effect: Z = 0.10 (P = 0.92)
2 Multivitamin without folic acid versus no multivitamin/folic acid
MRC 1991 0/453 3/454 100.0 % 0.14 [ 0.01, 2.76 ]
Subtotal (95% CI) 453 454 100.0 % 0.14 [ 0.01, 2.76 ]
Total events: 0 (Multivitamin), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.29 (P = 0.20)
3 Multivitamin with/without folic acid versus no multivitamin/folic acid
MRC 1991 2/914 3/454 100.0 % 0.33 [ 0.06, 1.97 ]
Subtotal (95% CI) 914 454 100.0 % 0.33 [ 0.06, 1.97 ]
Total events: 2 (Multivitamin), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.21 (P = 0.23)
4 Multivitamin + folic acid versus folic acid
Kirke 1992 0/93 0/93 Not estimable
MRC 1991 2/461 2/449 100.0 % 0.97 [ 0.14, 6.88 ]
Subtotal (95% CI) 554 542 100.0 % 0.97 [ 0.14, 6.88 ]
Total events: 2 (Multivitamin), 2 (Control)
Heterogeneity: not applicable
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
(Continued . . . )
160Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
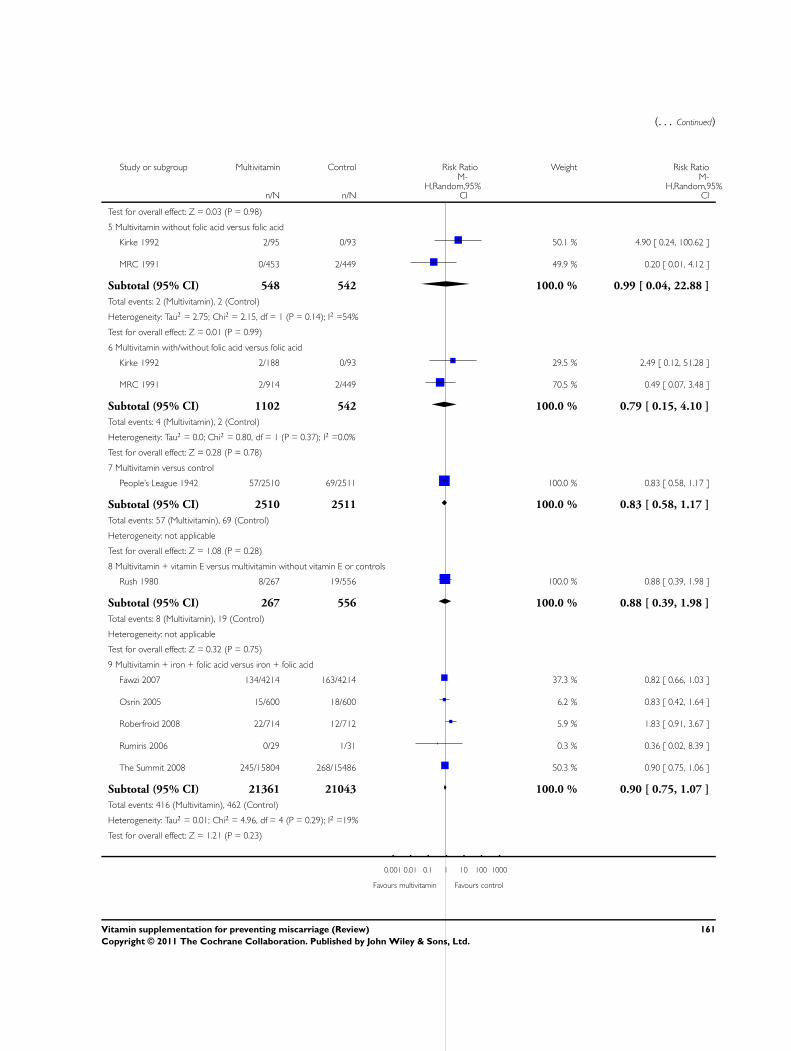
(. . . Continued)
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Test for overall effect: Z = 0.03 (P = 0.98)
5 Multivitamin without folic acid versus folic acid
Kirke 1992 2/95 0/93 50.1 % 4.90 [ 0.24, 100.62 ]
MRC 1991 0/453 2/449 49.9 % 0.20 [ 0.01, 4.12 ]
Subtotal (95% CI) 548 542 100.0 % 0.99 [ 0.04, 22.88 ]
Total events: 2 (Multivitamin), 2 (Control)
Heterogeneity: Tau2 = 2.75; Chi2 = 2.15, df = 1 (P = 0.14); I2 =54%
Test for overall effect: Z = 0.01 (P = 0.99)
6 Multivitamin with/without folic acid versus folic acid
Kirke 1992 2/188 0/93 29.5 % 2.49 [ 0.12, 51.28 ]
MRC 1991 2/914 2/449 70.5 % 0.49 [ 0.07, 3.48 ]
Subtotal (95% CI) 1102 542 100.0 % 0.79 [ 0.15, 4.10 ]
Total events: 4 (Multivitamin), 2 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.80, df = 1 (P = 0.37); I2 =0.0%
Test for overall effect: Z = 0.28 (P = 0.78)
7 Multivitamin versus control
People’s League 1942 57/2510 69/2511 100.0 % 0.83 [ 0.58, 1.17 ]
Subtotal (95% CI) 2510 2511 100.0 % 0.83 [ 0.58, 1.17 ]
Total events: 57 (Multivitamin), 69 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.08 (P = 0.28)
8 Multivitamin + vitamin E versus multivitamin without vitamin E or controls
Rush 1980 8/267 19/556 100.0 % 0.88 [ 0.39, 1.98 ]
Subtotal (95% CI) 267 556 100.0 % 0.88 [ 0.39, 1.98 ]
Total events: 8 (Multivitamin), 19 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.32 (P = 0.75)
9 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 134/4214 163/4214 37.3 % 0.82 [ 0.66, 1.03 ]
Osrin 2005 15/600 18/600 6.2 % 0.83 [ 0.42, 1.64 ]
Roberfroid 2008 22/714 12/712 5.9 % 1.83 [ 0.91, 3.67 ]
Rumiris 2006 0/29 1/31 0.3 % 0.36 [ 0.02, 8.39 ]
The Summit 2008 245/15804 268/15486 50.3 % 0.90 [ 0.75, 1.06 ]
Subtotal (95% CI) 21361 21043 100.0 % 0.90 [ 0.75, 1.07 ]
Total events: 416 (Multivitamin), 462 (Control)
Heterogeneity: Tau2 = 0.01; Chi2 = 4.96, df = 4 (P = 0.29); I2 =19%
Test for overall effect: Z = 1.21 (P = 0.23)
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
161Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.6. Comparison 5 Multivitamin, Outcome 6 Perinatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 6 Perinatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Random,95% CI IV,Random,95% CI
1 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 919 3389 0.1072 (0.0645) 100.0 % 1.11 [ 0.98, 1.26 ]
Subtotal (95% CI) 919 3389 100.0 % 1.11 [ 0.98, 1.26 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.66 (P = 0.097)
2 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 4214 4214 -0.1625 (0.0899) 35.6 % 0.85 [ 0.71, 1.01 ]
Osrin 2005 600 600 0.1989 (0.2754) 11.1 % 1.22 [ 0.71, 2.09 ]
Roberfroid 2008 714 712 0.5653 (0.2677) 11.6 % 1.76 [ 1.04, 2.97 ]
The Summit 2008 15804 15486 -0.1054 (0.0595) 41.8 % 0.90 [ 0.80, 1.01 ]
Subtotal (95% CI) 21332 21012 100.0 % 0.99 [ 0.80, 1.21 ]
Heterogeneity: Tau2 = 0.02; Chi2 = 7.81, df = 3 (P = 0.05); I2 =62%
Test for overall effect: Z = 0.14 (P = 0.89)
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
162Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.7. Comparison 5 Multivitamin, Outcome 7 Neonatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 7 Neonatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 2507 2423 0.4639 (0.8428) 100.0 % 1.59 [ 0.30, 8.30 ]
Subtotal (95% CI) 2507 2423 100.0 % 1.59 [ 0.30, 8.30 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
2 Multivitamin + vitamin E versus multivitamin without vitamin E or controls
Rush 1980 256 531 0.3617 (0.2342) 100.0 % 1.44 [ 0.91, 2.27 ]
Subtotal (95% CI) 256 531 100.0 % 1.44 [ 0.91, 2.27 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.54 (P = 0.12)
3 Multivitamin versus control
People’s League 1942 2453 2442 0 (0.1481) 100.0 % 1.00 [ 0.75, 1.34 ]
Subtotal (95% CI) 2453 2442 100.0 % 1.00 [ 0.75, 1.34 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
4 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 870 3252 0.1399 (0.0861) 100.0 % 1.15 [ 0.97, 1.36 ]
Subtotal (95% CI) 870 3252 100.0 % 1.15 [ 0.97, 1.36 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.62 (P = 0.10)
5 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 4079 4058 -0.1985 (0.1351) 23.1 % 0.82 [ 0.63, 1.07 ]
Osrin 2005 556 550 0.4253 (0.3829) 2.9 % 1.53 [ 0.72, 3.24 ]
Roberfroid 2008 641 642 0.5128 (0.4167) 2.4 % 1.67 [ 0.74, 3.78 ]
The Summit 2008 15273 14907 -0.1054 (0.0767) 71.6 % 0.90 [ 0.77, 1.05 ]
Subtotal (95% CI) 20549 20157 100.0 % 0.91 [ 0.80, 1.03 ]
Heterogeneity: Chi2 = 4.58, df = 3 (P = 0.21); I2 =34%
Test for overall effect: Z = 1.49 (P = 0.14)
Test for subgroup differences: Chi2 = 7.52, df = 4 (P = 0.11), I2 =47%
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
163Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.8. Comparison 5 Multivitamin, Outcome 8 Preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 8 Preterm birth
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 2819 2683 0.0086 (0.0541) 100.0 % 1.01 [ 0.91, 1.12 ]
Subtotal (95% CI) 2819 2683 100.0 % 1.01 [ 0.91, 1.12 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.16 (P = 0.87)
2 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 704 2616 -0.0177 (0.0423) 100.0 % 0.98 [ 0.90, 1.07 ]
Subtotal (95% CI) 704 2616 100.0 % 0.98 [ 0.90, 1.07 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.42 (P = 0.68)
3 Multivitamin + vitamin E versus multivitamin without vitamin E or controls
Rush 1980 263 551 -0.0132 (0.079) 100.0 % 0.99 [ 0.85, 1.15 ]
Subtotal (95% CI) 263 551 100.0 % 0.99 [ 0.85, 1.15 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.17 (P = 0.87)
4 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 4214 4214 0.01 (0.0507) 13.6 % 1.01 [ 0.91, 1.12 ]
Osrin 2005 600 600 -0.1393 (0.1913) 1.0 % 0.87 [ 0.60, 1.27 ]
Roberfroid 2008 714 712 0.0583 (0.1446) 1.7 % 1.06 [ 0.80, 1.41 ]
Rumiris 2006 29 31 -1.0217 (1.1202) 0.0 % 0.36 [ 0.04, 3.23 ]
The Summit 2008 14053 14373 0 (0.0204) 83.8 % 1.00 [ 0.96, 1.04 ]
Subtotal (95% CI) 19610 19930 100.0 % 1.00 [ 0.96, 1.04 ]
Heterogeneity: Chi2 = 1.56, df = 4 (P = 0.82); I2 =0.0%
Test for overall effect: Z = 0.04 (P = 0.97)
Test for subgroup differences: Chi2 = 0.22, df = 3 (P = 0.97), I2 =0.0%
0.002 0.1 1 10 500
Favours multivitamin Favours control
164Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
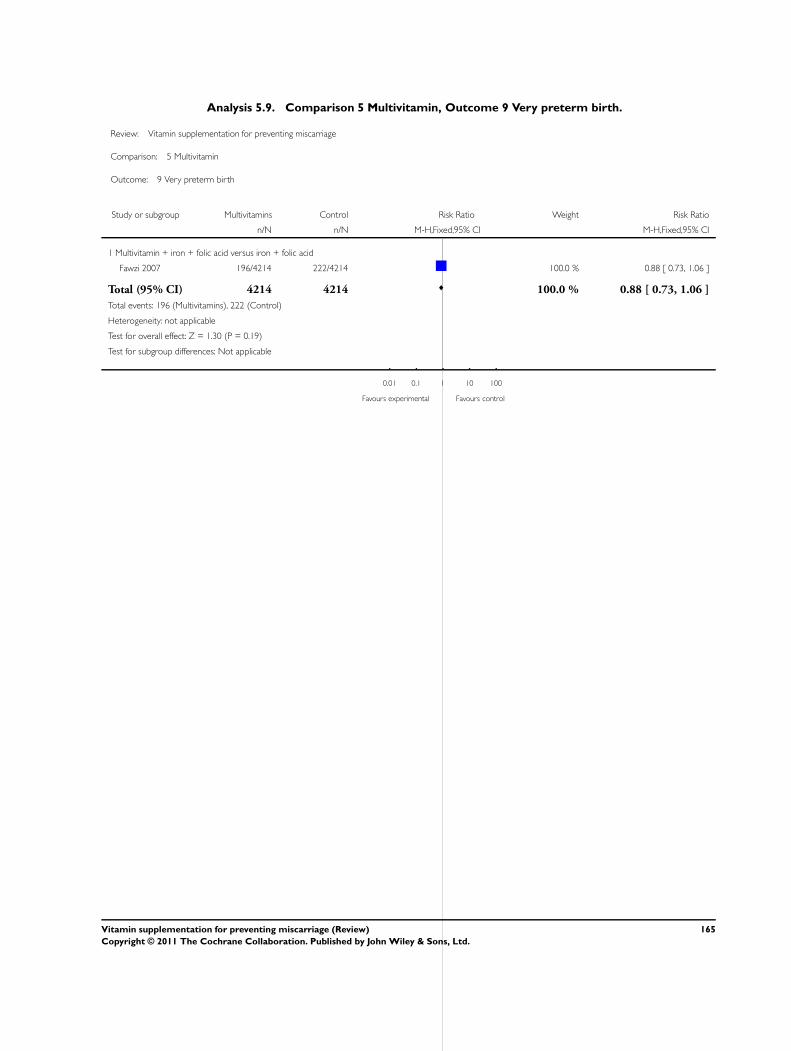
Analysis 5.9. Comparison 5 Multivitamin, Outcome 9 Very preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 9 Very preterm birth
Study or subgroup Multivitamins Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 196/4214 222/4214 100.0 % 0.88 [ 0.73, 1.06 ]
Total (95% CI) 4214 4214 100.0 % 0.88 [ 0.73, 1.06 ]
Total events: 196 (Multivitamins), 222 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.30 (P = 0.19)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours experimental Favours control
165Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.10. Comparison 5 Multivitamin, Outcome 10 Birthweight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 10 Birthweight
Study or subgroup Multivitamin ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 2471 3291 (488) 2391 3288 (478) 100.0 % 3.00 [ -24.15, 30.15 ]
Subtotal (95% CI) 2471 2391 100.0 % 3.00 [ -24.15, 30.15 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.22 (P = 0.83)
2 Multivitamin + iron + folic acid versus iron + folic acid
Fawzi 2007 4079 3148 (747) 4058 3083 (724) 57.8 % 65.00 [ 33.04, 96.96 ]
Osrin 2005 529 2810 (453) 523 2733 (422) 21.1 % 77.00 [ 24.10, 129.90 ]
Roberfroid 2008 526 2914 (450) 526 2877 (424) 21.1 % 37.00 [ -15.84, 89.84 ]
Subtotal (95% CI) 5134 5107 100.0 % 61.61 [ 37.32, 85.91 ]
Heterogeneity: Chi2 = 1.20, df = 2 (P = 0.55); I2 =0.0%
Test for overall effect: Z = 4.97 (P < 0.00001)
-1000 -500 0 500 1000
Favours control Favours multivitamin
166Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.11. Comparison 5 Multivitamin, Outcome 11 Small-for-gestational age (birthweight less than the
10th percentile or < 2500 g.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 11 Small-for-gestational age (birthweight less than the 10th percentile or < 2500 g
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Random,95% CI IV,Random,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 2471 2391 0.0828 (0.0753) 100.0 % 1.09 [ 0.94, 1.26 ]
Subtotal (95% CI) 2471 2391 100.0 % 1.09 [ 0.94, 1.26 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.10 (P = 0.27)
2 Multivitamin + folic acid versus no multivitamin/folic acid (birthweight < 2500 g)
ICMR 2000 96 90 -0.0969 (0.1896) 100.0 % 0.91 [ 0.63, 1.32 ]
Subtotal (95% CI) 96 90 100.0 % 0.91 [ 0.63, 1.32 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.51 (P = 0.61)
3 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 704 2616 -0.0177 (0.0193) 100.0 % 0.98 [ 0.95, 1.02 ]
Subtotal (95% CI) 704 2616 100.0 % 0.98 [ 0.95, 1.02 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.92 (P = 0.36)
4 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A (birthweight < 2500 g)
Christian 2003 705 2620 -0.0506 (0.0281) 100.0 % 0.95 [ 0.90, 1.00 ]
Subtotal (95% CI) 705 2620 100.0 % 0.95 [ 0.90, 1.00 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.80 (P = 0.072)
5 Multivitamins + iron + folic acid versus iron + folic acid
Fawzi 2007 4079 4058 -0.2614 (0.0629) 25.5 % 0.77 [ 0.68, 0.87 ]
Osrin 2005 550 556 -0.1054 (0.0761) 24.3 % 0.90 [ 0.78, 1.04 ]
Roberfroid 2008 518 512 -0.1054 (0.0791) 24.0 % 0.90 [ 0.77, 1.05 ]
Rumiris 2006 29 31 0.0677 (1.3906) 0.5 % 1.07 [ 0.07, 16.33 ]
The Summit 2008 5695 5406 0.1625 (0.0596) 25.8 % 1.18 [ 1.05, 1.32 ]
Subtotal (95% CI) 10871 10563 100.0 % 0.93 [ 0.77, 1.12 ]
Heterogeneity: Tau2 = 0.03; Chi2 = 24.87, df = 4 (P = 0.00005); I2 =84%
Test for overall effect: Z = 0.78 (P = 0.44)
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
167Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.12. Comparison 5 Multivitamin, Outcome 12 Congenital malformations.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 12 Congenital malformations
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 7/2471 6/2391 54.8 % 1.13 [ 0.38, 3.35 ]
MRC 1991 12/461 5/454 45.2 % 2.36 [ 0.84, 6.65 ]
Subtotal (95% CI) 2932 2845 100.0 % 1.69 [ 0.81, 3.53 ]
Total events: 19 (Multivitamin), 11 (Control)
Heterogeneity: Chi2 = 0.93, df = 1 (P = 0.33); I2 =0.0%
Test for overall effect: Z = 1.39 (P = 0.16)
2 Multivitamin without folic acid without versus no multivitamin/folic acid
MRC 1991 8/453 5/454 100.0 % 1.60 [ 0.53, 4.86 ]
Subtotal (95% CI) 453 454 100.0 % 1.60 [ 0.53, 4.86 ]
Total events: 8 (Multivitamin), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.83 (P = 0.40)
3 Multivitamin with/without folic acid versus no multivitamin/folic acid
MRC 1991 20/914 5/454 100.0 % 1.99 [ 0.75, 5.26 ]
Subtotal (95% CI) 914 454 100.0 % 1.99 [ 0.75, 5.26 ]
Total events: 20 (Multivitamin), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.38 (P = 0.17)
4 Multivitamin + folic acid versus folic acid
Kirke 1992 2/93 1/93 12.4 % 2.00 [ 0.18, 21.68 ]
MRC 1991 12/461 7/449 87.6 % 1.67 [ 0.66, 4.20 ]
Subtotal (95% CI) 554 542 100.0 % 1.71 [ 0.72, 4.04 ]
Total events: 14 (Multivitamin), 8 (Control)
Heterogeneity: Chi2 = 0.02, df = 1 (P = 0.89); I2 =0.0%
Test for overall effect: Z = 1.22 (P = 0.22)
5 Multivitamin without folic acid versus folic acid
Kirke 1992 5/95 1/93 12.6 % 4.89 [ 0.58, 41.10 ]
MRC 1991 8/453 7/449 87.4 % 1.13 [ 0.41, 3.10 ]
Subtotal (95% CI) 548 542 100.0 % 1.61 [ 0.67, 3.85 ]
Total events: 13 (Multivitamin), 8 (Control)
Heterogeneity: Chi2 = 1.52, df = 1 (P = 0.22); I2 =34%
Test for overall effect: Z = 1.06 (P = 0.29)
0.01 0.1 1 10 100
Favours multivitamin Favours control
(Continued . . . )
168Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
6 Multivitamin with/without folic acid versus folic acid
Kirke 1992 7/188 1/93 12.5 % 3.46 [ 0.43, 27.73 ]
MRC 1991 20/914 7/449 87.5 % 1.40 [ 0.60, 3.29 ]
Subtotal (95% CI) 1102 542 100.0 % 1.66 [ 0.76, 3.63 ]
Total events: 27 (Multivitamin), 8 (Control)
Heterogeneity: Chi2 = 0.63, df = 1 (P = 0.43); I2 =0.0%
Test for overall effect: Z = 1.27 (P = 0.20)
7 Multivitamin + iron + folic acid versus iron + folic acid
Osrin 2005 2/600 2/600 100.0 % 1.00 [ 0.14, 7.08 ]
Subtotal (95% CI) 600 600 100.0 % 1.00 [ 0.14, 7.08 ]
Total events: 2 (Multivitamin), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
0.01 0.1 1 10 100
Favours multivitamin Favours control
Analysis 5.13. Comparison 5 Multivitamin, Outcome 13 Multiple pregnancy.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 13 Multiple pregnancy
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamin + folic acid versus no multivitamin/folic acid
Czeizel 1994 93/2471 64/2391 95.7 % 1.41 [ 1.03, 1.92 ]
ICMR 2000 1/137 3/142 4.3 % 0.35 [ 0.04, 3.28 ]
Total (95% CI) 2608 2533 100.0 % 1.36 [ 1.00, 1.85 ]
Total events: 94 (Multivitamin), 67 (Control)
Heterogeneity: Chi2 = 1.47, df = 1 (P = 0.23); I2 =32%
Test for overall effect: Z = 1.95 (P = 0.051)
0.01 0.1 1 10 100
Favours multivitamin Favours control
169Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.14. Comparison 5 Multivitamin, Outcome 14 Maternal anaemia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 14 Maternal anaemia
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A (any anaemia)
Christian 2003 183 630 -0.0809 (0.0555) 100.0 % 0.92 [ 0.83, 1.03 ]
Subtotal (95% CI) 183 630 100.0 % 0.92 [ 0.83, 1.03 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.46 (P = 0.14)
2 Multivitamin + folic acid + iron + zinc+vitamin A versus folic acid + iron + zinc + vitamin A (severe anaemia)
Christian 2003 183 630 -0.2007 (0.2237) 100.0 % 0.82 [ 0.53, 1.27 ]
Subtotal (95% CI) 183 630 100.0 % 0.82 [ 0.53, 1.27 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.90 (P = 0.37)
3 Multivitamins versus placebo
Fawzi 1998 271 267 -0.2485 (0.2276) 100.0 % 0.78 [ 0.50, 1.22 ]
Subtotal (95% CI) 271 267 100.0 % 0.78 [ 0.50, 1.22 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.09 (P = 0.27)
4 Multivitamins + vitamin A + beta-carotene versus placebo
Fawzi 1998 268 267 -0.1985 (0.2209) 100.0 % 0.82 [ 0.53, 1.26 ]
Subtotal (95% CI) 268 267 100.0 % 0.82 [ 0.53, 1.26 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.90 (P = 0.37)
5 Multivitamins + iron + folic acid versus iron + folic acid
Fawzi 2007 811 267 -0.1278 (0.0492) 81.9 % 0.88 [ 0.80, 0.97 ]
Osrin 2005 600 600 -0.1054 (0.1046) 18.1 % 0.90 [ 0.73, 1.10 ]
Subtotal (95% CI) 1411 867 100.0 % 0.88 [ 0.81, 0.96 ]
Heterogeneity: Chi2 = 0.04, df = 1 (P = 0.85); I2 =0.0%
Test for overall effect: Z = 2.78 (P = 0.0054)
Test for subgroup differences: Chi2 = 1.05, df = 4 (P = 0.90), I2 =0.0%
0.001 0.01 0.1 1 10 100 1000
Favours multivitamin Favours control
170Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
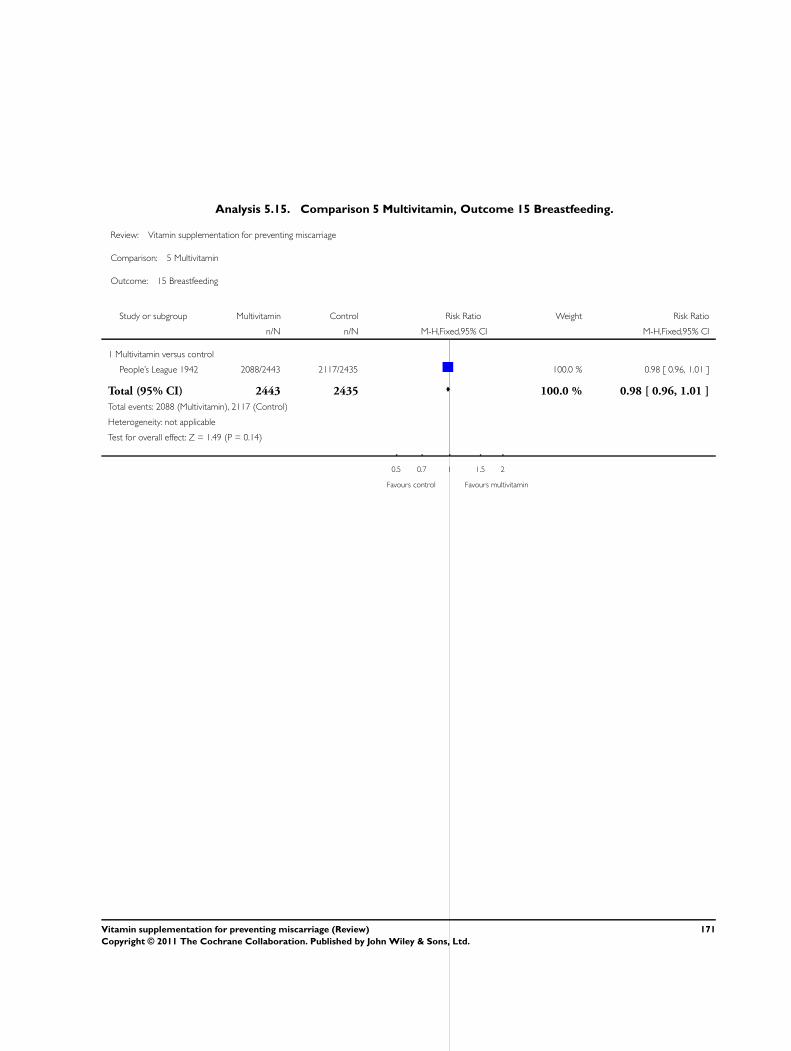
Analysis 5.15. Comparison 5 Multivitamin, Outcome 15 Breastfeeding.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 15 Breastfeeding
Study or subgroup Multivitamin Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Multivitamin versus control
People’s League 1942 2088/2443 2117/2435 100.0 % 0.98 [ 0.96, 1.01 ]
Total (95% CI) 2443 2435 100.0 % 0.98 [ 0.96, 1.01 ]
Total events: 2088 (Multivitamin), 2117 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.49 (P = 0.14)
0.5 0.7 1 1.5 2
Favours control Favours multivitamin
171Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.16. Comparison 5 Multivitamin, Outcome 16 Poor growth at childhood follow up: Underweight
in childhood (6-8 years of age).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 16 Poor growth at childhood follow up: Underweight in childhood (6-8 years of age)
Study or subgroup Multivitamins Control log [Risk Ratio] Risk Ratio Weight Risk Ratio
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 721 2635 0.0488 (0.0389) 100.0 % 1.05 [ 0.97, 1.13 ]
Total (95% CI) 721 2635 100.0 % 1.05 [ 0.97, 1.13 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.25 (P = 0.21)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours multivitamins Favours control
Analysis 5.17. Comparison 5 Multivitamin, Outcome 17 Poor growth at childhood follow up: Stunting in
childhood (6-8 years of age).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 17 Poor growth at childhood follow up: Stunting in childhood (6-8 years of age)
Study or subgroup Multivitamins Control log [Risk Ratio] Risk Ratio Weight Risk Ratio
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 721 2635 0.0862 (0.0444) 100.0 % 1.09 [ 1.00, 1.19 ]
Total (95% CI) 721 2635 100.0 % 1.09 [ 1.00, 1.19 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.94 (P = 0.052)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours multivitamins Favours control
172Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.18. Comparison 5 Multivitamin, Outcome 18 Additional outcomes - infant death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 5 Multivitamin
Outcome: 18 Additional outcomes - infant death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Multivitamin + folic acid + iron + zinc + vitamin A versus folic acid + iron + zinc + vitamin A
Christian 2003 870 3252 0.0934 (0.0809) 100.0 % 1.10 [ 0.94, 1.29 ]
Total (95% CI) 870 3252 100.0 % 1.10 [ 0.94, 1.29 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.15 (P = 0.25)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours multivitamin Favours control
173Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.1. Comparison 6 Folic acid, Outcome 1 Total fetal loss (including miscarriages or combined
miscarriages and stillbirths).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 1 Total fetal loss (including miscarriages or combined miscarriages and stillbirths)
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 312/2819 260/2683 80.6 % 1.14 [ 0.98, 1.33 ]
ICMR 2000 9/231 17/235 5.1 % 0.54 [ 0.25, 1.18 ]
MRC 1991 47/461 47/454 14.3 % 0.98 [ 0.67, 1.44 ]
Subtotal (95% CI) 3511 3372 100.0 % 1.09 [ 0.95, 1.25 ]
Total events: 368 (Folic acid), 324 (Control)
Heterogeneity: Chi2 = 3.70, df = 2 (P = 0.16); I2 =46%
Test for overall effect: Z = 1.18 (P = 0.24)
2 Folic acid without multivitamin versus no folic acid/multivitamin
MRC 1991 44/449 47/454 100.0 % 0.95 [ 0.64, 1.40 ]
Subtotal (95% CI) 449 454 100.0 % 0.95 [ 0.64, 1.40 ]
Total events: 44 (Folic acid), 47 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
3 Folic acid with/without multivitamin versus no folic acid/multivitamin
MRC 1991 91/910 47/454 100.0 % 0.97 [ 0.69, 1.35 ]
Subtotal (95% CI) 910 454 100.0 % 0.97 [ 0.69, 1.35 ]
Total events: 91 (Folic acid), 47 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.20 (P = 0.84)
4 Folic acid + multivitamin versus multivitamin
Kirke 1992 9/93 9/95 18.5 % 1.02 [ 0.42, 2.46 ]
MRC 1991 47/461 39/453 81.5 % 1.18 [ 0.79, 1.77 ]
Subtotal (95% CI) 554 548 100.0 % 1.15 [ 0.80, 1.67 ]
Total events: 56 (Folic acid), 48 (Control)
Heterogeneity: Chi2 = 0.09, df = 1 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 0.77 (P = 0.44)
5 Folic acid without multivitamin versus multivitamin
Kirke 1992 9/93 9/95 18.7 % 1.02 [ 0.42, 2.46 ]
MRC 1991 44/449 39/453 81.3 % 1.14 [ 0.75, 1.72 ]
Subtotal (95% CI) 542 548 100.0 % 1.12 [ 0.77, 1.62 ]
0.01 0.1 1 10 100
Favours folic acid Favours control
(Continued . . . )
174Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Total events: 53 (Folic acid), 48 (Control)
Heterogeneity: Chi2 = 0.05, df = 1 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 0.58 (P = 0.56)
6 Folic acid with or without multivitamin versus multivitamin
Kirke 1992 18/186 9/95 18.6 % 1.02 [ 0.48, 2.19 ]
MRC 1991 91/910 39/453 81.4 % 1.16 [ 0.81, 1.66 ]
Subtotal (95% CI) 1096 548 100.0 % 1.14 [ 0.82, 1.57 ]
Total events: 109 (Folic acid), 48 (Control)
Heterogeneity: Chi2 = 0.09, df = 1 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 0.77 (P = 0.44)
7 Folic acid + iron versus iron
Fleming 1968 0/35 2/40 100.0 % 0.23 [ 0.01, 4.59 ]
Subtotal (95% CI) 35 40 100.0 % 0.23 [ 0.01, 4.59 ]
Total events: 0 (Folic acid), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.97 (P = 0.33)
8 Folic acid + iron + antimalarials versus iron + antimalarials
Fleming 1986 6/80 0/80 100.0 % 13.00 [ 0.74, 226.98 ]
Subtotal (95% CI) 80 80 100.0 % 13.00 [ 0.74, 226.98 ]
Total events: 6 (Folic acid), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.76 (P = 0.079)
0.01 0.1 1 10 100
Favours folic acid Favours control
175Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.2. Comparison 6 Folic acid, Outcome 2 Early or late miscarriage.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 2 Early or late miscarriage
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 301/2819 251/2683 56.4 % 1.14 [ 0.97, 1.34 ]
ICMR 2000 6/231 14/235 10.2 % 0.44 [ 0.17, 1.11 ]
MRC 1991 45/461 44/454 33.4 % 1.01 [ 0.68, 1.49 ]
Subtotal (95% CI) 3511 3372 100.0 % 0.99 [ 0.72, 1.38 ]
Total events: 352 (Folic acid), 309 (Control)
Heterogeneity: Tau2 = 0.04; Chi2 = 4.13, df = 2 (P = 0.13); I2 =52%
Test for overall effect: Z = 0.05 (P = 0.96)
2 Folic acid without multivitamins versus no folic acid/multivitamin
MRC 1991 42/449 44/454 100.0 % 0.97 [ 0.65, 1.44 ]
Subtotal (95% CI) 449 454 100.0 % 0.97 [ 0.65, 1.44 ]
Total events: 42 (Folic acid), 44 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.17 (P = 0.86)
3 Folic acid with/without multivitamin versus no folic acid/multivitamin
MRC 1991 87/910 44/454 100.0 % 0.99 [ 0.70, 1.39 ]
Subtotal (95% CI) 910 454 100.0 % 0.99 [ 0.70, 1.39 ]
Total events: 87 (Folic acid), 44 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.08 (P = 0.94)
4 Folic acid + multivitamin versus multivitamin
Kirke 1992 9/93 7/95 15.7 % 1.31 [ 0.51, 3.38 ]
MRC 1991 45/461 39/453 84.3 % 1.13 [ 0.75, 1.71 ]
Subtotal (95% CI) 554 548 100.0 % 1.16 [ 0.80, 1.69 ]
Total events: 54 (Folic acid), 46 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.08, df = 1 (P = 0.78); I2 =0.0%
Test for overall effect: Z = 0.78 (P = 0.44)
5 Folic acid without multivitamin versus multivitamin
Kirke 1992 9/93 7/95 16.2 % 1.31 [ 0.51, 3.38 ]
MRC 1991 42/449 39/453 83.8 % 1.09 [ 0.72, 1.65 ]
Subtotal (95% CI) 542 548 100.0 % 1.12 [ 0.77, 1.64 ]
0.01 0.1 1 10 100
Favours folic acid Favours control
(Continued . . . )
176Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Total events: 51 (Folic acid), 46 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.13, df = 1 (P = 0.72); I2 =0.0%
Test for overall effect: Z = 0.59 (P = 0.56)
6 Folic acid with/without multivitamin versus multivitamin
Kirke 1992 18/186 9/93 18.3 % 1.00 [ 0.47, 2.14 ]
MRC 1991 87/910 39/453 81.7 % 1.11 [ 0.77, 1.59 ]
Subtotal (95% CI) 1096 546 100.0 % 1.09 [ 0.79, 1.51 ]
Total events: 105 (Folic acid), 48 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.06, df = 1 (P = 0.81); I2 =0.0%
Test for overall effect: Z = 0.51 (P = 0.61)
7 Folic acid + iron versus iron
Fleming 1968 0/35 1/40 100.0 % 0.38 [ 0.02, 9.03 ]
Subtotal (95% CI) 35 40 100.0 % 0.38 [ 0.02, 9.03 ]
Total events: 0 (Folic acid), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.60 (P = 0.55)
8 Folic acid + iron + antimalarials versus iron + antimalarials
Fleming 1986 6/80 0/80 100.0 % 13.00 [ 0.74, 226.98 ]
Subtotal (95% CI) 80 80 100.0 % 13.00 [ 0.74, 226.98 ]
Total events: 6 (Folic acid), 0 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.76 (P = 0.079)
0.01 0.1 1 10 100
Favours folic acid Favours control
177Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.3. Comparison 6 Folic acid, Outcome 3 Pre-eclampsia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 3 Pre-eclampsia
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Folic acid + iron versus iron
Fleming 1968 2/35 2/40 100.0 % 1.14 [ 0.17, 7.69 ]
Total (95% CI) 35 40 100.0 % 1.14 [ 0.17, 7.69 ]
Total events: 2 (Folic acid), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
0.01 0.1 1 10 100
Favours folic acid Favours control
Analysis 6.4. Comparison 6 Folic acid, Outcome 4 Stillbirth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 4 Stillbirth
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 11/2819 9/2683 60.6 % 1.16 [ 0.48, 2.80 ]
ICMR 2000 3/231 3/235 19.5 % 1.02 [ 0.21, 4.99 ]
MRC 1991 2/461 3/454 19.9 % 0.66 [ 0.11, 3.91 ]
Subtotal (95% CI) 3511 3372 100.0 % 1.03 [ 0.51, 2.09 ]
Total events: 16 (Folic acid), 15 (Control)
Heterogeneity: Chi2 = 0.32, df = 2 (P = 0.85); I2 =0.0%
Test for overall effect: Z = 0.09 (P = 0.93)
2 Folic acid without multivitamin versus no folic acid/multivitamin
0.001 0.01 0.1 1 10 100 1000
Favours folic acid Favours control
(Continued . . . )
178Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
MRC 1991 2/449 3/454 100.0 % 0.67 [ 0.11, 4.02 ]
Subtotal (95% CI) 449 454 100.0 % 0.67 [ 0.11, 4.02 ]
Total events: 2 (Folic acid), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.43 (P = 0.66)
3 Folic acid with/without multivitamin versus no folic acid/multivitamin
MRC 1991 4/910 3/454 100.0 % 0.67 [ 0.15, 2.96 ]
Subtotal (95% CI) 910 454 100.0 % 0.67 [ 0.15, 2.96 ]
Total events: 4 (Folic acid), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.54 (P = 0.59)
4 Folic acid + multivitamin versus multivitamin
Kirke 1992 0/93 2/95 83.1 % 0.20 [ 0.01, 4.20 ]
MRC 1991 2/461 0/453 16.9 % 4.91 [ 0.24, 102.06 ]
Subtotal (95% CI) 554 548 100.0 % 1.00 [ 0.20, 4.99 ]
Total events: 2 (Folic acid), 2 (Control)
Heterogeneity: Chi2 = 2.12, df = 1 (P = 0.15); I2 =53%
Test for overall effect: Z = 0.00 (P = 1.0)
5 Folic acid without multivitamin versus multivitamin
Kirke 1992 2/95 0/93 50.4 % 4.90 [ 0.24, 100.62 ]
MRC 1991 2/449 0/453 49.6 % 5.04 [ 0.24, 104.78 ]
Subtotal (95% CI) 544 546 100.0 % 4.97 [ 0.58, 42.29 ]
Total events: 4 (Folic acid), 0 (Control)
Heterogeneity: Chi2 = 0.00, df = 1 (P = 0.99); I2 =0.0%
Test for overall effect: Z = 1.47 (P = 0.14)
6 Folic acid with/without multivitamin versus multivitamin
Kirke 1992 0/186 2/95 83.2 % 0.10 [ 0.00, 2.12 ]
MRC 1991 4/910 0/453 16.8 % 4.49 [ 0.24, 83.13 ]
Subtotal (95% CI) 1096 548 100.0 % 0.84 [ 0.20, 3.53 ]
Total events: 4 (Folic acid), 2 (Control)
Heterogeneity: Chi2 = 3.12, df = 1 (P = 0.08); I2 =68%
Test for overall effect: Z = 0.24 (P = 0.81)
7 Folic acid + iron versus iron
Fleming 1968 0/35 1/40 100.0 % 0.38 [ 0.02, 9.03 ]
Subtotal (95% CI) 35 40 100.0 % 0.38 [ 0.02, 9.03 ]
Total events: 0 (Folic acid), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.60 (P = 0.55)
0.001 0.01 0.1 1 10 100 1000
Favours folic acid Favours control
179Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
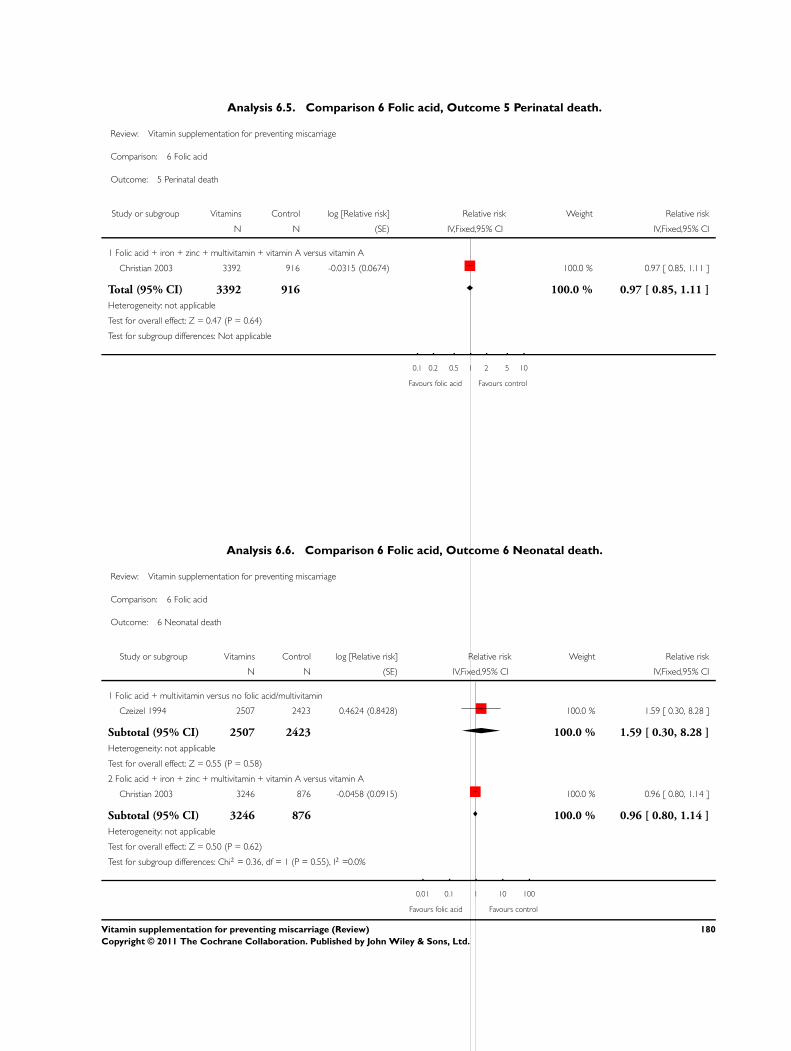
Analysis 6.5. Comparison 6 Folic acid, Outcome 5 Perinatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 5 Perinatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A
Christian 2003 3392 916 -0.0315 (0.0674) 100.0 % 0.97 [ 0.85, 1.11 ]
Total (95% CI) 3392 916 100.0 % 0.97 [ 0.85, 1.11 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.47 (P = 0.64)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours folic acid Favours control
Analysis 6.6. Comparison 6 Folic acid, Outcome 6 Neonatal death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 6 Neonatal death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 2507 2423 0.4624 (0.8428) 100.0 % 1.59 [ 0.30, 8.28 ]
Subtotal (95% CI) 2507 2423 100.0 % 1.59 [ 0.30, 8.28 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
2 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A
Christian 2003 3246 876 -0.0458 (0.0915) 100.0 % 0.96 [ 0.80, 1.14 ]
Subtotal (95% CI) 3246 876 100.0 % 0.96 [ 0.80, 1.14 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.50 (P = 0.62)
Test for subgroup differences: Chi2 = 0.36, df = 1 (P = 0.55), I2 =0.0%
0.01 0.1 1 10 100
Favours folic acid Favours control
180Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.7. Comparison 6 Folic acid, Outcome 7 Preterm birth.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 7 Preterm birth
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 2819 2683 0.0086 (0.0541) 100.0 % 1.01 [ 0.91, 1.12 ]
Subtotal (95% CI) 2819 2683 100.0 % 1.01 [ 0.91, 1.12 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.16 (P = 0.87)
2 Folic acid + multivitamin versus no folic acid/multivitamin
Fleming 1968 35 40 0.0086 (0.2212) 100.0 % 1.01 [ 0.65, 1.56 ]
Subtotal (95% CI) 35 40 100.0 % 1.01 [ 0.65, 1.56 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.04 (P = 0.97)
3 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A
Christian 2003 2635 685 0.0212 (0.0438) 100.0 % 1.02 [ 0.94, 1.11 ]
Subtotal (95% CI) 2635 685 100.0 % 1.02 [ 0.94, 1.11 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.48 (P = 0.63)
Test for subgroup differences: Chi2 = 0.03, df = 2 (P = 0.98), I2 =0.0%
0.1 0.2 0.5 1 2 5 10
Favours folic acid Favours control
181Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.8. Comparison 6 Folic acid, Outcome 8 Birthweight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 8 Birthweight
Study or subgroup Folic acid ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 2471 3291 (488) 2391 3288 (478) 100.0 % 3.00 [ -24.15, 30.15 ]
Subtotal (95% CI) 2471 2391 100.0 % 3.00 [ -24.15, 30.15 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.22 (P = 0.83)
2 Folic acid versus placebo
Correia 1982 16 3440 (304) 13 3128 (255) 100.0 % 312.00 [ 108.52, 515.48 ]
Subtotal (95% CI) 16 13 100.0 % 312.00 [ 108.52, 515.48 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.01 (P = 0.0027)
3 Folic + iron versus control
Taylor 1982 21 3470 (365) 24 3502 (232) 100.0 % -32.00 [ -213.62, 149.62 ]
Subtotal (95% CI) 21 24 100.0 % -32.00 [ -213.62, 149.62 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.35 (P = 0.73)
Test for subgroup differences: Chi2 = 8.89, df = 2 (P = 0.01), I2 =78%
-1000 -500 0 500 1000
Favours control Favours folic acid
182Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.9. Comparison 6 Folic acid, Outcome 9 Small-for-gestational age.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 9 Small-for-gestational age
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 2471 2391 0.0828 (0.0753) 100.0 % 1.09 [ 0.94, 1.26 ]
Subtotal (95% CI) 2471 2391 100.0 % 1.09 [ 0.94, 1.26 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.10 (P = 0.27)
2 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A
Christian 2003 2635 685 -0.0269 (0.0291) 100.0 % 0.97 [ 0.92, 1.03 ]
Subtotal (95% CI) 2635 685 100.0 % 0.97 [ 0.92, 1.03 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.92 (P = 0.36)
3 Folic acid + iron versus iron (birthweight < 2500 g)
Fleming 1968 35 40 0.0569 (0.4031) 100.0 % 1.06 [ 0.48, 2.33 ]
Subtotal (95% CI) 35 40 100.0 % 1.06 [ 0.48, 2.33 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
4 Folic acid + multivitamin versus no folic acid/multivitamin (birthweight < 2500 g)
ICMR 2000 96 90 -0.0969 (0.1896) 100.0 % 0.91 [ 0.63, 1.32 ]
Subtotal (95% CI) 96 90 100.0 % 0.91 [ 0.63, 1.32 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.51 (P = 0.61)
5 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A (birthweight < 2500 g)
Christian 2003 2640 685 -0.0605 (0.0257) 100.0 % 0.94 [ 0.90, 0.99 ]
Subtotal (95% CI) 2640 685 100.0 % 0.94 [ 0.90, 0.99 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.35 (P = 0.019)
Test for subgroup differences: Chi2 = 3.64, df = 4 (P = 0.46), I2 =0.0%
0.1 0.2 0.5 1 2 5 10
Favours folic acid Favours control
183Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
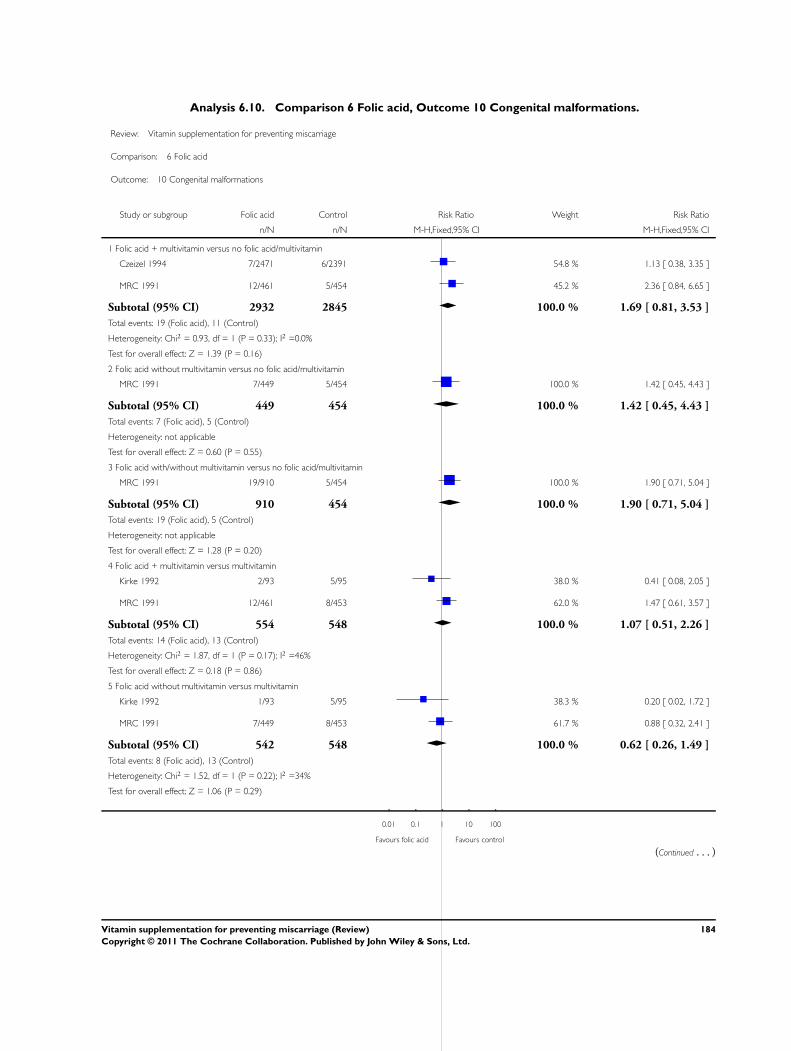
Analysis 6.10. Comparison 6 Folic acid, Outcome 10 Congenital malformations.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 10 Congenital malformations
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 7/2471 6/2391 54.8 % 1.13 [ 0.38, 3.35 ]
MRC 1991 12/461 5/454 45.2 % 2.36 [ 0.84, 6.65 ]
Subtotal (95% CI) 2932 2845 100.0 % 1.69 [ 0.81, 3.53 ]
Total events: 19 (Folic acid), 11 (Control)
Heterogeneity: Chi2 = 0.93, df = 1 (P = 0.33); I2 =0.0%
Test for overall effect: Z = 1.39 (P = 0.16)
2 Folic acid without multivitamin versus no folic acid/multivitamin
MRC 1991 7/449 5/454 100.0 % 1.42 [ 0.45, 4.43 ]
Subtotal (95% CI) 449 454 100.0 % 1.42 [ 0.45, 4.43 ]
Total events: 7 (Folic acid), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.60 (P = 0.55)
3 Folic acid with/without multivitamin versus no folic acid/multivitamin
MRC 1991 19/910 5/454 100.0 % 1.90 [ 0.71, 5.04 ]
Subtotal (95% CI) 910 454 100.0 % 1.90 [ 0.71, 5.04 ]
Total events: 19 (Folic acid), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.28 (P = 0.20)
4 Folic acid + multivitamin versus multivitamin
Kirke 1992 2/93 5/95 38.0 % 0.41 [ 0.08, 2.05 ]
MRC 1991 12/461 8/453 62.0 % 1.47 [ 0.61, 3.57 ]
Subtotal (95% CI) 554 548 100.0 % 1.07 [ 0.51, 2.26 ]
Total events: 14 (Folic acid), 13 (Control)
Heterogeneity: Chi2 = 1.87, df = 1 (P = 0.17); I2 =46%
Test for overall effect: Z = 0.18 (P = 0.86)
5 Folic acid without multivitamin versus multivitamin
Kirke 1992 1/93 5/95 38.3 % 0.20 [ 0.02, 1.72 ]
MRC 1991 7/449 8/453 61.7 % 0.88 [ 0.32, 2.41 ]
Subtotal (95% CI) 542 548 100.0 % 0.62 [ 0.26, 1.49 ]
Total events: 8 (Folic acid), 13 (Control)
Heterogeneity: Chi2 = 1.52, df = 1 (P = 0.22); I2 =34%
Test for overall effect: Z = 1.06 (P = 0.29)
0.01 0.1 1 10 100
Favours folic acid Favours control
(Continued . . . )
184Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
6 Folic acid with or without multvitamin versus multivitamin
Kirke 1992 3/186 5/95 38.3 % 0.31 [ 0.07, 1.26 ]
MRC 1991 19/910 8/453 61.7 % 1.18 [ 0.52, 2.68 ]
Subtotal (95% CI) 1096 548 100.0 % 0.85 [ 0.43, 1.67 ]
Total events: 22 (Folic acid), 13 (Control)
Heterogeneity: Chi2 = 2.64, df = 1 (P = 0.10); I2 =62%
Test for overall effect: Z = 0.48 (P = 0.63)
0.01 0.1 1 10 100
Favours folic acid Favours control
Analysis 6.11. Comparison 6 Folic acid, Outcome 11 Multiple pregnancy.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 11 Multiple pregnancy
Study or subgroup Folic acid Control Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Folic acid + multivitamin versus no folic acid/multivitamin
Czeizel 1994 93/2471 64/2391 95.7 % 1.41 [ 1.03, 1.92 ]
ICMR 2000 1/137 3/142 4.3 % 0.35 [ 0.04, 3.28 ]
Subtotal (95% CI) 2608 2533 100.0 % 1.36 [ 1.00, 1.85 ]
Total events: 94 (Folic acid), 67 (Control)
Heterogeneity: Chi2 = 1.47, df = 1 (P = 0.23); I2 =32%
Test for overall effect: Z = 1.95 (P = 0.051)
0.01 0.1 1 10 100
Favours folic acid Favours control
185Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.12. Comparison 6 Folic acid, Outcome 12 Maternal anaemia.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 12 Maternal anaemia
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A (any anaemia)
Christian 2003 634 179 -0.1805 (0.042) 100.0 % 0.83 [ 0.77, 0.91 ]
Subtotal (95% CI) 634 179 100.0 % 0.83 [ 0.77, 0.91 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.30 (P = 0.000017)
2 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A (severe anaemia)
Christian 2003 634 179 -0.1938 (0.1737) 100.0 % 0.82 [ 0.59, 1.16 ]
Subtotal (95% CI) 634 179 100.0 % 0.82 [ 0.59, 1.16 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.12 (P = 0.26)
3 Folic acid + iron versus iron (severe anaemia)
Fleming 1968 35 50 0.0569 (0.7296) 100.0 % 1.06 [ 0.25, 4.42 ]
Subtotal (95% CI) 35 50 100.0 % 1.06 [ 0.25, 4.42 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.08 (P = 0.94)
4 Folic acid + iron versus no folic acid or iron
Fleming 1986 42 47 0.4253 (0.3352) 100.0 % 1.53 [ 0.79, 2.95 ]
Subtotal (95% CI) 42 47 100.0 % 1.53 [ 0.79, 2.95 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.27 (P = 0.20)
Test for subgroup differences: Chi2 = 3.33, df = 3 (P = 0.34), I2 =10%
0.1 0.2 0.5 1 2 5 10
Favours folic acid Favours control
186Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.13. Comparison 6 Folic acid, Outcome 13 Poor growth in childhood: Stunting in childhood (6-8
years of age).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 13 Poor growth in childhood: Stunting in childhood (6-8 years of age)
Study or subgroup Multivitamins Control log [Risk Ratio] Risk Ratio Weight Risk Ratio
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + iron + zinc + vitamin A versus multivitamin + vitamin A
Christian 2003 1934 1422 -0.0726 (0.0381) 100.0 % 0.93 [ 0.86, 1.00 ]
Total (95% CI) 1934 1422 100.0 % 0.93 [ 0.86, 1.00 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.91 (P = 0.057)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours folic acid Favours control
Analysis 6.14. Comparison 6 Folic acid, Outcome 14 Poor growth in childhood: Underweight in childhood
(6-8 years of age).
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 14 Poor growth in childhood: Underweight in childhood (6-8 years of age)
Study or subgroup Multivitamins Control log [Risk Ratio] Risk Ratio Weight Risk Ratio
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + iron + zinc + vitamin A versus multivitamin + vitamin A
Christian 2003 1934 1422 -0.0305 (0.0341) 100.0 % 0.97 [ 0.91, 1.04 ]
Total (95% CI) 1934 1422 100.0 % 0.97 [ 0.91, 1.04 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.89 (P = 0.37)
Test for subgroup differences: Not applicable
0.01 0.1 1 10 100
Favours folic acid Favours control
187Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
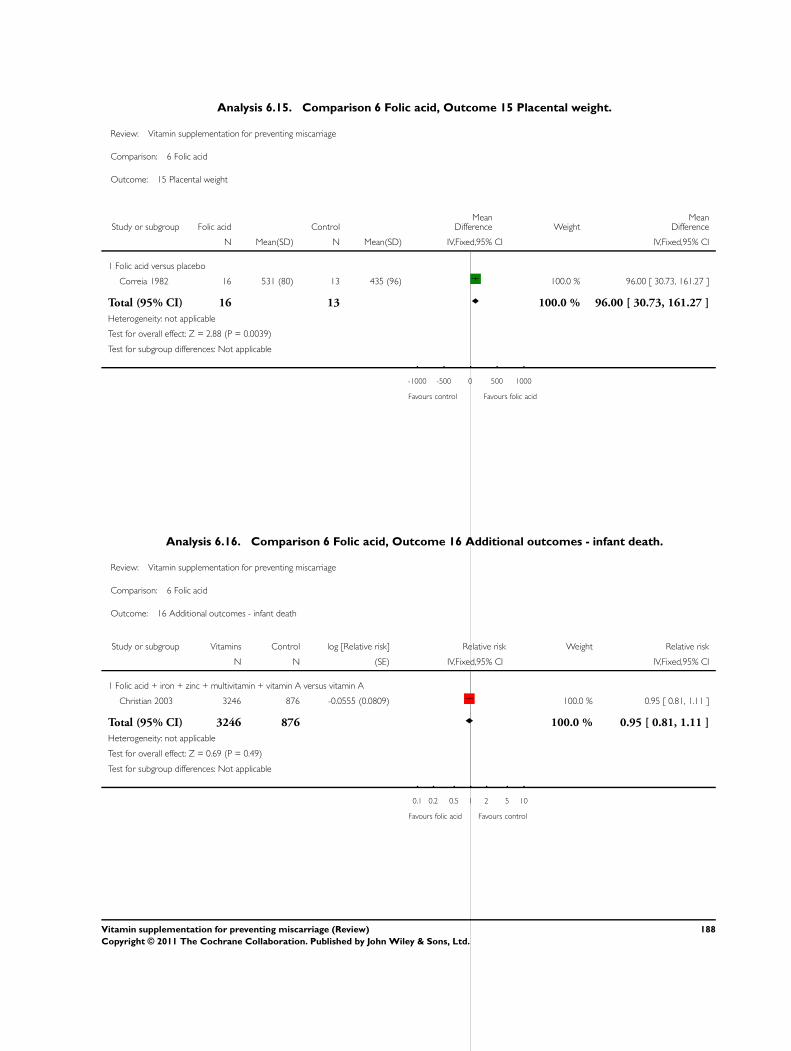
Analysis 6.15. Comparison 6 Folic acid, Outcome 15 Placental weight.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 15 Placental weight
Study or subgroup Folic acid ControlMean
Difference WeightMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid versus placebo
Correia 1982 16 531 (80) 13 435 (96) 100.0 % 96.00 [ 30.73, 161.27 ]
Total (95% CI) 16 13 100.0 % 96.00 [ 30.73, 161.27 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.88 (P = 0.0039)
Test for subgroup differences: Not applicable
-1000 -500 0 500 1000
Favours control Favours folic acid
Analysis 6.16. Comparison 6 Folic acid, Outcome 16 Additional outcomes - infant death.
Review: Vitamin supplementation for preventing miscarriage
Comparison: 6 Folic acid
Outcome: 16 Additional outcomes - infant death
Study or subgroup Vitamins Control log [Relative risk] Relative risk Weight Relative risk
N N (SE) IV,Fixed,95% CI IV,Fixed,95% CI
1 Folic acid + iron + zinc + multivitamin + vitamin A versus vitamin A
Christian 2003 3246 876 -0.0555 (0.0809) 100.0 % 0.95 [ 0.81, 1.11 ]
Total (95% CI) 3246 876 100.0 % 0.95 [ 0.81, 1.11 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.69 (P = 0.49)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours folic acid Favours control
188Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A D D I T I O N A L T A B L E S
Table 1. Additional outcomes
Study ID Outcome Vitamin - N Vitamin - Me-
dian
Vitamin -
Range
Placebo - N Placebo - Me-
dian
Placebo -
Range
Steyn 2003 Median birth-
weight
100 2491 240-3834 100 2664 334-4680
A P P E N D I C E S
Appendix 1. Additional searching carried out for the initial version of the review
For the initial version of the review, authors carried out a separate search of CENTRAL (The Cochrane Library, 2003, Issue 2) for the
following terms: miscarriage*, spontaneous abortion, recurrent abortion, spontaneous pregnancy loss, recurrent pregnancy loss, fetal
death, vitamin*, folate, folic acid; and also MEDLINE (1966 to May 2003), Current Contents (1998 to May 2003) and EMBASE
(1980 to May 2003) using the search strategy given below:
1. miscarriage*
2. spontaneous abortion
3. recurrent abortion
4. habitual abortion
5. spontaneous pregnancy loss
6. recurrent pregnancy loss
7. early pregnancy loss
8. early pregnancy bleeding
9. fetal death
10. #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9
11. vitamin*
12. retinol*
13. carotenoid*
14. thiamin*
15. riboflavin
16. niacin or nicotinamide or nicotinic acid
17. pantothenic acid or pantothenate
18. pyridox*
19. cyanocobalamin or cobalamin
20. ascorb*
21. calciferol
22. tocopherol* or alpha-tocopherol
23. folate*
24. folic acid
25. phylloquinone
26. menaquinone
27. #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #11 or #12
28. #10 and #27
29. random*
30. controlled-clinical-trial
189Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

31. #29 or #30
32. #28 and #31
W H A T ’ S N E W
Last assessed as up-to-date: 7 December 2010.
Date Event Description
27 August 2010 New search has been performed Search updated. 11 new studied included (Fawzi 2007;
Fleming 1986; Osrin 2005; Roberfroid 2008; Rumbold
2006; Rumiris 2006; Spinnato 2007; Taylor 1982; The
Summit 2008; Van den Broek 2006; Villar 2009), 3
studies excluded (Feyi-Waboso 2005; Huybregts 2009;
Shu 2002). Two new studies are awaiting classification
(Chelchowska 2004; Kubik 2004) and two new ongoing
trials were identified (Fall 2007; Johns 2004; Sezikawa
2007).
27 August 2010 New citation required but conclusions have not changed Substantive amendment and addition of a new author.
H I S T O R Y
Protocol first published: Issue 1, 2003
Review first published: Issue 2, 2005
Date Event Description
20 September 2008 Amended Converted to new review format.
C O N T R I B U T I O N S O F A U T H O R S
Alice Rumbold developed and wrote the protocol, extracted data and prepared the review. Ning Pan and Philippa Middleton extracted
data and were involved in the analysis and writing of the review. Caroline Crowther commented on and revised the various drafts of
the protocol and review during its development.
190Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
Alice Rumbold and Caroline Crowther are investigators on the Australian Collaborative Trial of Supplements with vitamin C and
vitamin E for the prevention of pre-eclampsia (Rumbold 2006). This trial is included in this review but its eligibility for inclusion, trial
quality assessments and data extraction were carried out independently by two of the review authors not involved in the original trial.
S O U R C E S O F S U P P O R T
Internal sources
• Department of Obstetrics and Gynaecology, The University of Adelaide, Australia.
• The University of Adelaide Medical Endowment Fund, Australia.
Dr Rumbold is supported by the Jean B Reid Fellowship
External sources
• Department of Health and Ageing, Australia.
• Department of Nutrition for Health and Development, World Health Organization, Switzerland.
Provided funding for the preparation of this updated review.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
We now include trials where supplementation occurred in mid-pregnancy. This was not specified in the original protocol for this review,
but this was amended to be in line with other miscarriage reviews such as ’Progestogen for preventing miscarriage’ (Haas 2009). We
included trials where the onset of supplementation occurred both prior to and after 20 weeks’ gestation, and when it could not be
established whether the majority of the women started supplementation prior to 20 weeks’ gestation. To overcome differences in the
definition of miscarriage and stillbirth, we have used a combined outcome of total fetal loss (early or late miscarriage or stillbirth). We
have still reported early or late miscarriage and stillbirth separately in addition to this combined outcome. Similarly, we specified in the
original protocol that we would exclude studies reporting greater than 20% losses to follow-up. In this review we have included studies
that reported more than 20% losses to follow-up and undertaken further analyses based on trial quality.
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Dietary Supplements [adverse effects]; Abortion, Habitual [prevention & control]; Abortion, Spontaneous [∗prevention & control];
Ascorbic Acid [administration & dosage]; Pre-Eclampsia [prevention & control]; Pregnancy Outcome; Pregnancy, Multiple; Random-
ized Controlled Trials as Topic; Vitamin A [administration & dosage]; Vitamins [∗administration & dosage; adverse effects]
MeSH check words
Female; Humans; Pregnancy
191Vitamin supplementation for preventing miscarriage (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.


















