
Catastrophic Health Expenditure in Brazil: Regional ... · Regional Differences, Budget Constraints...
23
Catastrophic Health Expenditure in Brazil: Regional Differences, Budget Constraints and Private Health Insurance Maria Dolores Montoya Diaz•, Flavia Mori Sarti♦ Antonio Carlos Coelho Campino♣ Roberto Iunes * •PhD.,University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy - Ribeirao Preto (FEARP/ USP)/Senior Researcher at FIPE (Economic Research Foundation) E-MAIL for all correspondence [email protected] BUSINESS ADDRESS: Faculdade de Economia, Administração e Contabilidade da Universidade de São Paulo em Ribeirão Preto. Av. dos Bandeirantes, 3900 14049-900 – Ribeirão Preto – SP - PHONE: +55 11 3602-3910 FAX: + 55 11 3633-4488 ♦ PhD., University of São Paulo , Vice-Coordinator in Graduate Program in Complex System Modeling (School of Arts and Human Sciences -USP)/ Senior Researcher at FIPE (Economic Research Foundation) ♣ PhD, University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy (FEA/USP)/ Senior Researcher at FIPE (Economic Research Foundation) *Senior Evaluation Officer, Office of Evaluation and Oversight, Inter-American Development Bank
Transcript of Catastrophic Health Expenditure in Brazil: Regional ... · Regional Differences, Budget Constraints...

Catastrophic Health Expenditure in Brazil: Regional Differences, Budget Constraints and
Private Health InsuranceMaria Dolores Montoya Diaz•, Flavia Mori Sarti♦Antonio Carlos Coelho Campino♣ Roberto Iunes *
•PhD.,University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy - Ribeirao Preto (FEARP/USP)/Senior Researcher at FIPE (Economic Research Foundation) E-MAIL for all correspondence [email protected] BUSINESS ADDRESS: Faculdade de Economia, Administração e Contabilidade da Universidade de São Paulo em Ribeirão Preto. Av. dos Bandeirantes, 3900 14049-900 – Ribeirão Preto – SP - PHONE: +55 11 3602-3910 FAX: + 55 11 3633-4488♦ PhD., University of São Paulo , Vice-Coordinator in Graduate Program in Complex System Modeling (School of Arts and Human Sciences -USP)/ Senior Researcher at FIPE (Economic Research Foundation)♣ PhD, University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy (FEA/USP)/ Senior Researcher at FIPE (Economic Research Foundation)*Senior Evaluation Officer, Office of Evaluation and Oversight, Inter- American Development Bank

Catastrophic Health Expenditure in Brazil: Regional Differences, Budget Constraints and
Private Health Insurance
Maria Dolores Montoya Diaz•
Flavia Mori Sarti♦
Antonio Carlos Coelho Campino♣
Roberto Iunes *
• PhD., University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy - Ribeirao Preto (FEARP/USP)/Senior Researcher at FIPE (Economic Research Foundation) E-MAIL for all correspondence [email protected] BUSINESS ADDRESS: Faculdade de Economia, Administração e Contabilidade da Universidade de São Paulo em Ribeirão Preto. Av. dos Bandeirantes, 3900 14049-900 – Ribeirão Preto – SP - PHONE: +55 11 3602-3910 FAX: + 55 11 3633-4488 ♦ PhD., University of São Paulo , Vice-Coordinator in Graduate Program in Complex System Modeling (School of Arts and Human Sciences -USP)/ Senior Researcher at FIPE (Economic Research Foundation) ♣ PhD, University of São Paulo, Department of Economics - School of Economics, Business Administration and Accountancy (FEA/USP)/ Senior Researcher at FIPE (Economic Research Foundation) *Senior Evaluation Officer, Office of Evaluation and Oversight, Inter-‐American Development Bank;

1
Introduction
The analysis of private expenditure in health care is quite traditional in Brazil. Nevertheless,
it is of interest to note the scarcity of studies aimed at the analysis of catastrophic expenditures in
health care in the Brazilian population, exceptions granted to the texts of Xu et al. (2003) and
Diniz et al. (2007).
Xu et al. (2003) based their investigation on the Life Standards Survey (Pesquisa sobre
Padroes de Vida – PPV) performed during 1996-1997 by the Brazilian Institute for Geography
and Statistics (Instituto Brasileiro de Geografia e Estatistica – IBGE, an official institution)
estimating that 10.3% of Brazilian households would be incurring catastrophic expenses in health
care – that is, a commitment superior to 40% of their disbursement capacity.
Diniz et al. (2007) examined the Family Budget Survey (Pesquisa de Orcamentos Familiares
– POF) performed during 2002-2003, also by the Brazilian Institute for Geography and Statistics,
resulting in an estimative that less than 1% of the Brazilian households would have incurred
catastrophic expenses in health care.
According to Diniz et al. (2007), one of the likely causes of such broad divergence between
both results might lie upon the database utilized by Xu et al. (2003), which does not consider
“data concerning expenditure on non-monetary expenses”. Additionally, the authors claim that
the Family Budget Survey is a more adequate data collection for this specific type of analysis,
2
because: (i) it comprises a sample representative for the whole Brazilian territory, (ii) it includes
records of non-monetary expenditures from the households, and, (iii) it is essentially a budget
survey – and not a life-standard research.
The present chapter aims at contributing to the literature on the characteristics of the
expenditures in health in Brazilian households. Regional differences regarding to the incidence of
catastrophic expenditures in health care in Brazil are analyzed, in order to verify possible links
between the occurrence of such catastrophic expenditures and the characteristics of the Brazilian
health system (presented in the chapter that describes the evolution and structure of the Brazilian
health system).
Moreover, the study seeks to investigate the impact of health items that were not consumed
by household members due to lack of resources on catastrophic health expenditure incidence.
We intend to verify the possibility that Brazilian public health system, although universal and
inclusive, may not represent an adequate financial protection structure for all segments of low
income population.
Finally, the effects of private insurance on the probability of a household incurring
catastrophic health expenditures is analyzed.

3
Data and Methodology
As pointed out by Diniz et al. (2007), it is important to notice that the chosen methodology
have direct implications with regard to the estimates obtained from the percentage of households
which incur catastrophic expenditures in health care.
The methodology herein applied to identify the Brazilian households incurring catastrophic
expenditures in health care consists, essentially, in calculating the proportion of direct and
indirect expenditures in health care – therefore, including household expenses regarding health
plans and health insurance – upon the capacity of disbursement (P) of the households. The
availability of resources or capacity for disbursement was calculated in two different methods:
1. As the difference between the total expenditures registered by the household members
(G) and the sum of all household expenses in food items (A):
P = G – A
2. As the difference between the total expenditures registered by the household members
(G) and the national poverty line (L):
P = G – L

4
In this second method, it is important to note, that were counted only households with
positives health expenditures.
The analysis was performed using three different limits (20%, 30% and 40%) to indicate the
existence of catastrophic expenditure in the household. Thus, if the percentage of expenditure on
health care surpasses the fixed limit, it is established that the household has suffered catastrophic
expenditures on health care.
The variable G corresponds to the total expenditure of the household, calculated from the
addition of all monetary expenses and non-monetary expenses made by the household.
The variable containing the expenditures on health was calculated by adding outpatient
expenses, hospitalization expenses, expenses with medical apparatuses, expenses on health plans
and health insurance, among other items.
The variable representing a household expenditure level equivalent to the national poverty
line was estimated as described by Silveira et al. (2008).
In relation to the choice to incorporate the expenditure on health plans and health insurance,
the justification is found in Diniz et al. (2007):
“Finally, the majority of papers carry out their estimates taking into consideration, as did Xu at al.
(2003), the direct disbursement alone. The subjacent idea to this choice is that the pre-payment of a health
plan or insurance is made to reduce the risk of a family incurring catastrophic expenditure. Nevertheless,
in order to render this effective, the plan or insurance must be comprehensive, that is to say, it must cover
5
all potential expenses of the family on health, inasmuch as, whenever faced with a health problem, the
family will not be forced to make any out of pocket expenditure. If the plan or insurance does not carry
such characteristic, even by making the pre-payment, a family may yet be forced to disburse a far from
negligible sum of money on an uncovered treatment. Thus, some authors make estimates of catastrophic
expenses also considering the total expenditure on health care, that is, including on this expenditure
payment to plans and insurances.” (Translation by the authors of the chapter).
The database utilized was the Family Budget Survey (Pesquisa de Orcamentos Familiares –
POF) performed in 2002-2003 by the Brazilian Institute for Geography and Statistics. The survey
encompasses nationwide coverage, which allows for analyses with geographical disaggregation:
States (also named Federation Units, or Unidades da Federacao – UF), Metropolitan Areas, and
Regions (North, Northeast, Southeast, South and Middle-West) of the country. The database
under analysis contains 48,470 observations, which represents 48,394,067 Brazilian households.
Additionally, an analysis based on the relation between catastrophic expenditures in health
and the national poverty line was performed, in order to indicate the possibility that expenditures
in health may represent a burden for most of the Brazilian population.
The analysis performed was directed towards the estimation of models that seeks to evaluate
whether there are statistically significant differences among the Brazilian regions, relatively to
the incidence of catastrophic expenditures on health.
In order to achieve such goals, Survey Probit models have been estimated, encompassing a
binary variable as explained variable, indicative of the presence of catastrophic expenditures in
health on the household. Among the “explicatives”, a set of dummy variables for Brazilian
regions were included, using the Southeast Region as reference category for comparison.
6
Other socio-economic, geographic and demographic variables were included in the model for
control purposes:
Dummy variable for the presence of pregnant or breast-feeding women in the
household;
Dummy variable for the presence of any household members with a university level
education;
Number of inmates/household members living in the household;
Number of existing bathrooms in the household;
Dummy variable for the presence of water supply and running-water in the house;
Dummy variable for the presence of sewage and rain water piping;
Total monthly income of the household (in Brazilian reais – BRL);
Dummy variable for the presence of at least one member of the household with 5
years old or less;
Dummy variable for the presence of any members of the household with 65 years old
or more;
Dummy variable for the absence of any household members either 5 years old or less
and 65 years old or more;
Dummy variable for the presence of at least one household member owning a private
health care plan or health insurance;
Dummy variable for the area where the household is situated (rural or urban).
7
It should be noted that the percentages of incidence for catastrophic expenditures in health
care in Brazilian households, as well as the models, were estimated with the incorporation of the
sample design of the Family Budget Survey.
Finally, we try to deal with the possible endogeneity of health insurance by estimating an
instrumental variables model (following Greene (2000, pp.852-855)) and the instrument is the
percentage of household inhabitants that are formally employed.
8
Results
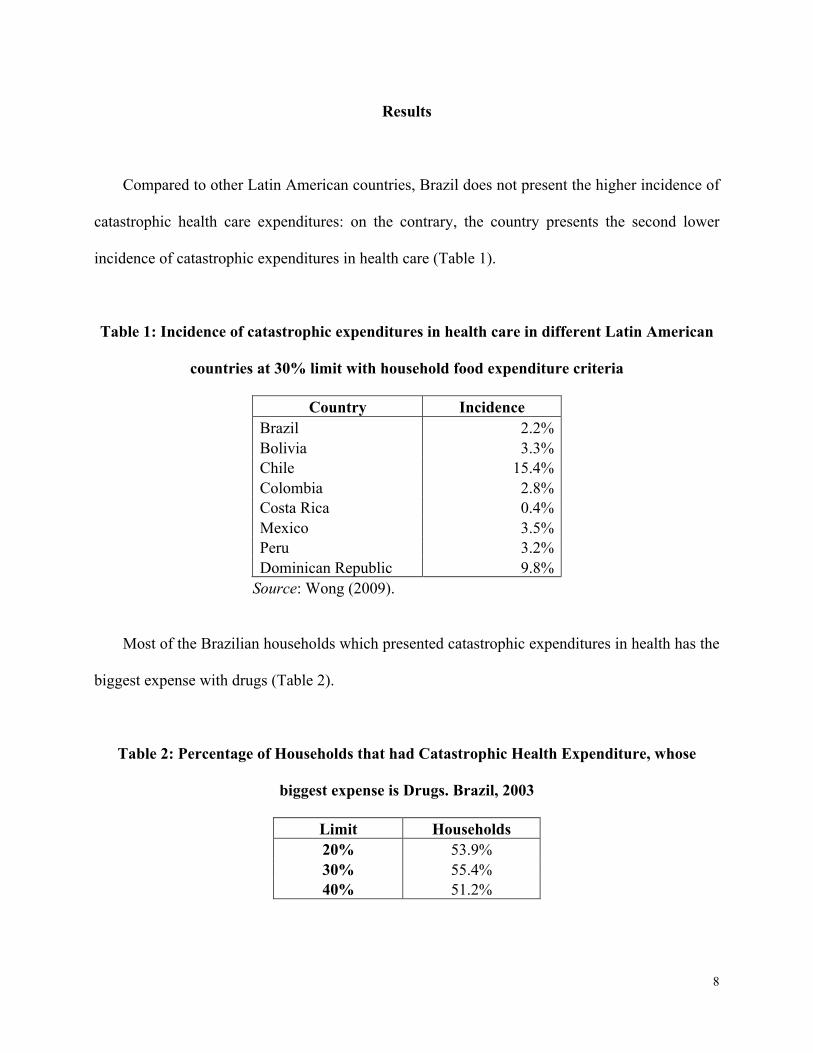
Compared to other Latin American countries, Brazil does not present the higher incidence of
catastrophic health care expenditures: on the contrary, the country presents the second lower
incidence of catastrophic expenditures in health care (Table 1).
Table 1: Incidence of catastrophic expenditures in health care in different Latin American
countries at 30% limit with household food expenditure criteria
Country Incidence Brazil 2.2% Bolivia 3.3% Chile 15.4% Colombia 2.8% Costa Rica 0.4% Mexico 3.5% Peru 3.2% Dominican Republic 9.8%
Source: Wong (2009).
Most of the Brazilian households which presented catastrophic expenditures in health has the
biggest expense with drugs (Table 2).
Table 2: Percentage of Households that had Catastrophic Health Expenditure, whose
biggest expense is Drugs. Brazil, 2003
Limit Households 20% 53.9% 30% 55.4% 40% 51.2%

9
Although the Brazilian public health system presents programs of pharmaceutical assistance,
there are limited sets of therapies and treatments for some types of target diseases available.
Using the criteria of household food expenditures as baseline survival expenditure, the
incidences of catastrophic expenditures in health among Brazilian households are higher in
Middle-West and South regions, presenting a lower incidence in North region for all limits
(Table 3). Regional disaggregation shows that the patterns of incidence of catastrophic
expenditures in health care for the country are very similar to the incidences presented in the
Southeast region.
Table 3: Incidence of catastrophic expenditures in health care with household food
expenditure criteria, disaggregated by regions. Brazil, 2003
Limit Region 20% 30% 40% North 5.0% 1.6% 0.7% Northeast 6.2% 2.1% 0.8% Southeast 6.8% 1.9% 0.8% South 7.5% 2.9% 1.3% Middle-West 7.8% 3.3% 1.4% Brazil 6.7% 2.2% 0.9%
However, considering the highest limit (40%), it is noticeable that the Northeast and
Southeast regions show results closer to the incidences of the North region, whilst the incidences
in the South region are closer to the Middle-West region.
The Brazilian Family Budget Survey performed in 2002-2003 also included a survey of
health items that were not consumed by household members due to lack of resources, ie, by
10
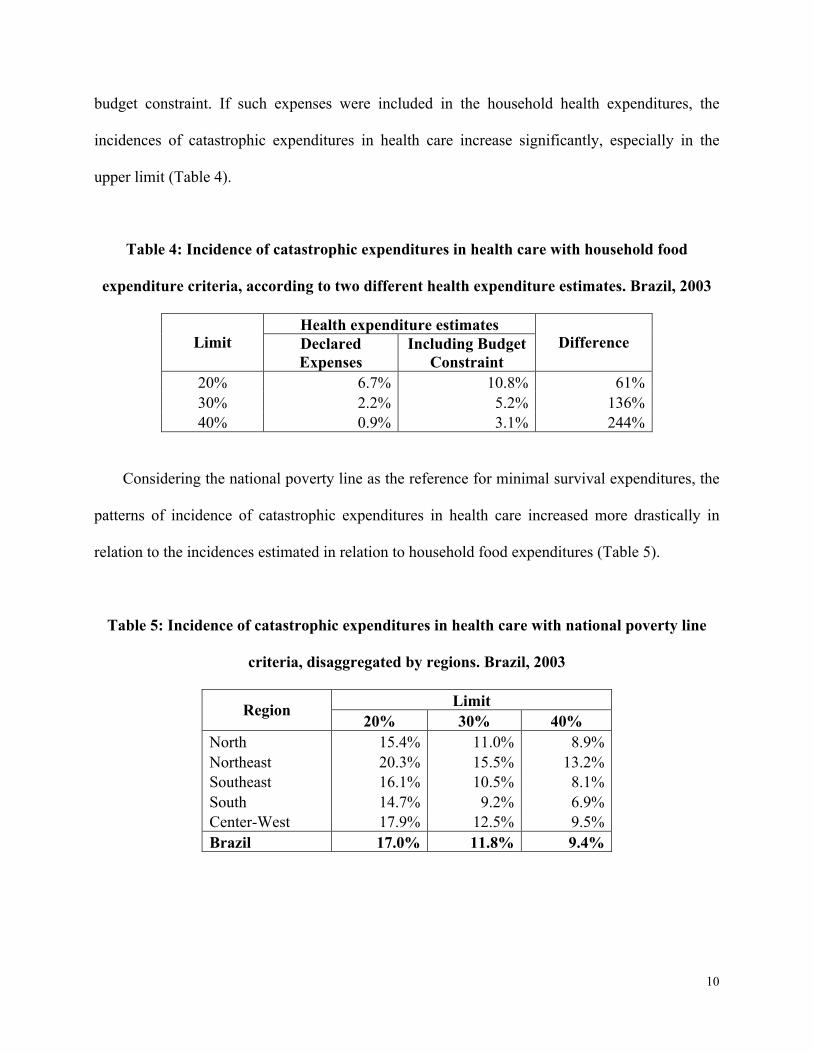
budget constraint. If such expenses were included in the household health expenditures, the
incidences of catastrophic expenditures in health care increase significantly, especially in the
upper limit (Table 4).
Table 4: Incidence of catastrophic expenditures in health care with household food
expenditure criteria, according to two different health expenditure estimates. Brazil, 2003
Health expenditure estimates Limit Declared
Expenses Including Budget
Constraint Difference
20% 6.7% 10.8% 61% 30% 2.2% 5.2% 136% 40% 0.9% 3.1% 244%
Considering the national poverty line as the reference for minimal survival expenditures, the
patterns of incidence of catastrophic expenditures in health care increased more drastically in
relation to the incidences estimated in relation to household food expenditures (Table 5).
Table 5: Incidence of catastrophic expenditures in health care with national poverty line
criteria, disaggregated by regions. Brazil, 2003
Limit Region 20% 30% 40%
North 15.4% 11.0% 8.9% Northeast 20.3% 15.5% 13.2% Southeast 16.1% 10.5% 8.1% South 14.7% 9.2% 6.9% Center-West 17.9% 12.5% 9.5% Brazil 17.0% 11.8% 9.4%

11
Moreover, the incidences of catastrophic expenditures in health care at national level
followed more closely the patterns of incidence described for Center-West region. The incidences
in other Brazilian regions did not hold any similarity among each other.
Once more, adding up the set of budget constraint health expenditures, the incidences of
catastrophic expenditures in health care estimated using the national poverty line criteria increase
notably (Table 6).
Table 6: Incidence of catastrophic expenditures in health care with national poverty line
criteria, according to two different health expenditure estimates. Brazil, 2003
Health Expenditures Estimates Limit Declared
Expenses Including Budget
Constraint Difference
20% 17.0% 21.5% 26% 30% 11.8% 15.3% 30% 40% 9.4% 12.5% 33%
Nevertheless, the differences between the incidence estimates based on declared health
expenses and based on budget constraint expenses – reported under national poverty line criteria
– decreased, in relation to the results reported under household food expenditures criteria
(previously presented in Table 4).
Additionally, the occurrence of catastrophic expenditures in health care may lead the
household to fall under the national poverty line. Thus, it is interesting to verify the incidence of
impoverishment caused by catastrophic expenditures in health care in Brazilian households in
12
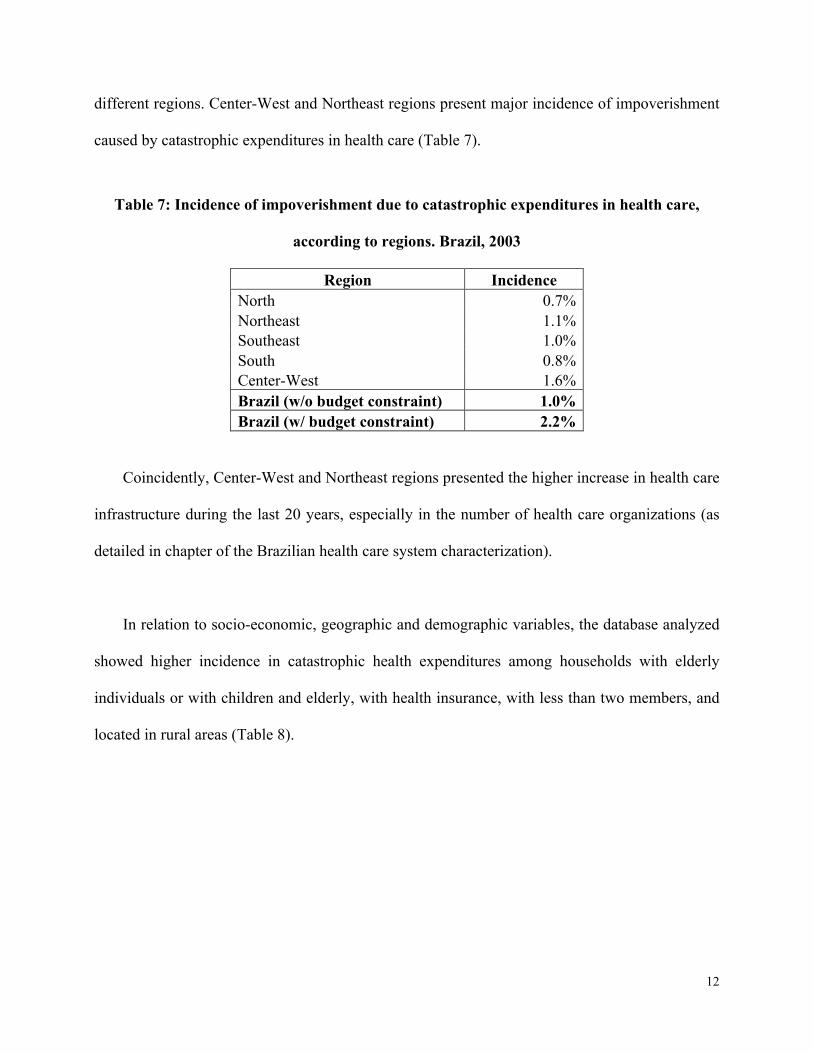
different regions. Center-West and Northeast regions present major incidence of impoverishment
caused by catastrophic expenditures in health care (Table 7).
Table 7: Incidence of impoverishment due to catastrophic expenditures in health care,
according to regions. Brazil, 2003
Region Incidence North 0.7% Northeast 1.1% Southeast 1.0% South 0.8% Center-West 1.6% Brazil (w/o budget constraint) 1.0% Brazil (w/ budget constraint) 2.2%
Coincidently, Center-West and Northeast regions presented the higher increase in health care
infrastructure during the last 20 years, especially in the number of health care organizations (as
detailed in chapter of the Brazilian health care system characterization).
In relation to socio-economic, geographic and demographic variables, the database analyzed
showed higher incidence in catastrophic health expenditures among households with elderly
individuals or with children and elderly, with health insurance, with less than two members, and
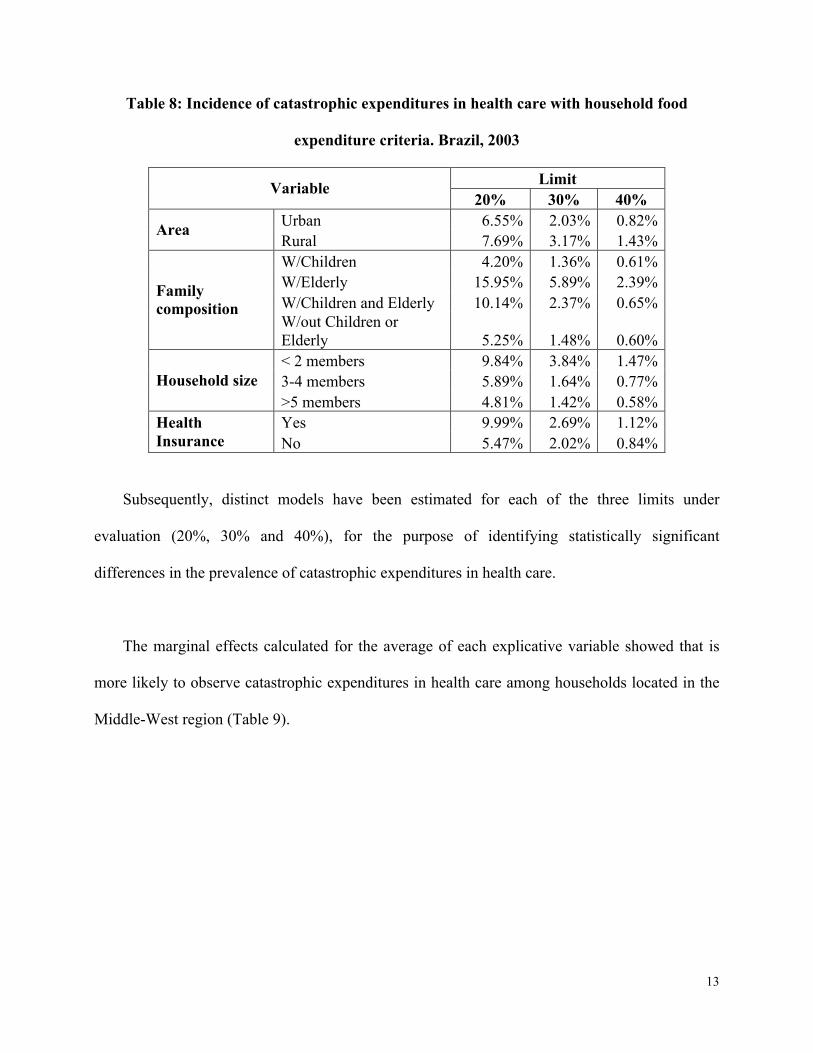
located in rural areas (Table 8).
13
Table 8: Incidence of catastrophic expenditures in health care with household food
expenditure criteria. Brazil, 2003
Limit Variable 20% 30% 40%
Urban 6.55% 2.03% 0.82% Area Rural 7.69% 3.17% 1.43% W/Children 4.20% 1.36% 0.61% W/Elderly 15.95% 5.89% 2.39% W/Children and Elderly 10.14% 2.37% 0.65%
Family composition
W/out Children or Elderly 5.25% 1.48% 0.60% < 2 members 9.84% 3.84% 1.47% 3-4 members 5.89% 1.64% 0.77% Household size >5 members 4.81% 1.42% 0.58% Yes 9.99% 2.69% 1.12% Health
Insurance No 5.47% 2.02% 0.84%
Subsequently, distinct models have been estimated for each of the three limits under
evaluation (20%, 30% and 40%), for the purpose of identifying statistically significant
differences in the prevalence of catastrophic expenditures in health care.
The marginal effects calculated for the average of each explicative variable showed that is
more likely to observe catastrophic expenditures in health care among households located in the
Middle-West region (Table 9).

14
Table 9: Marginal effects of Survey Probit Models with three limits for catastrophic
expenditures in health care. Brazil, 2003
Limit Variable 20% 30% 40%
-0.0062 -0.0008 -0.0001 North region(d) (-0.82) (-0.22) (-0.03)
-0.0014 0.0006 -0.0004 Northeast region(d) (-0.21) -0.2100 (-0.25)
0.0059 0.00736** 0.00392** South region(d) (0.86) (2.09) (1.98)
0.0188** 0.0149*** 0.00655** Middle-West region(d) (2.23) (3.17) (2.39)
-0.0060 -0.0033 -0.0003 Presence of pregnant / breast-feeding women(d) (-1.16) (-1.33) (-0.16)
-0.0140** -0.00700*** -0.00364*** Presence of member with university level education(d) (-2.12) (-3.07) (-2.87)
-0.00484*** -0.00252*** -0.00102*** Number of household members (-4.39) (-3.61) (-3.41)
-0.0032 -0.0017 -0.0004 Number of bathrooms (-0.92) (-1.37) (-0.46)
-0.00810* -0.0019 -0.0014 Presence of water supply and running-water(d) (-1.78) (-0.80) (-0.60)
-0.0038 -0.0026 -0.0014 Presence of sewage and rain water piping(d) (-0.85) (-1.05) (-1.17)
-0.00000411** 0.0000 0.0000 Household income (-2.43) (-0.90) (0.14)
-0.0161 -0.00963*** -0.00600*** Presence of children with less than 5 years old(d) (-0.83) (-2.67) (-3.01)
0.0881** 0.0182*** 0.0024 Presence of elderly more than 65 years old(d) (2.33) (3.01) (0.78)
-0.0075 -0.0124** -0.00929** Absence of children or elderly(d) (-0.31) (-2.26) (-2.47)
0.0657*** 0.0136*** 0.00505*** Presence of health insurance(d) (10.64) (5.11) (3.26)
0.0141** 0.00828** 0.00415* Household in rural area(d) (2.25) (2.49) (1.83) Obs.: Marginal effects. t statistics in parenthesis. (d) for discrete change of dummy variable from 0 to 1 * p<0.10, ** p<0.05, *** p<0.01

15
In relation to regional differences, it was observed that the coefficients from the Southeast
region and the Middle-West region were statistically significant on the models with definition of
catastrophic expenditures in 30% and 40% limit.
The results point to the existence of significant differences among the Southeast, South and
Middle-West regions. It should be observed that the differences between the Southeast and
Middle-West regions were also significant for the model with incidence of catastrophic
expenditure at a lower limit, that is, 20%.
It is interesting to notice that the existence of a household member with university level
education causes the reduction in the probability of occurrence of catastrophic expenditure in
health care. Also, the number of members in the household is inversely related with the
probability of occurrence of catastrophic expenditures in health care. Inversely, there is a higher
probability of occurring catastrophic expenditures in health care within the household if it is
situated in the rural area.
It should be noted, still, that the composition of the household also appears to bear an
influence on the incidence of catastrophic expenditures in health care, depending on the limits
adopted in defining catastrophic expenditures. Thus, households with or without children, as well
as households with no elderly individuals, show a lower probability for the occurrence of a
catastrophic expenditure in health care (models for limits of 30% and 40%), whereas households
with elderly individuals present a higher probability for occurrence of a catastrophic expenditure
(models for limits of 20% and 30%).
16
A highlight should be deservedly cast upon the fact that the variables that characterize the
living conditions in the house (water supply and sewage) and the presence of pregnant and breast-
feeding women do not seem to bear any influence whatsoever on the probability of occurrence of
catastrophic expenditures in health care.
The presence of health insurance presents positive marginal effects, which seem to indicate
that the ownership of a health care insurance or health plan would increase the probability of
occurrence of a catastrophic expenditure in health care.
It may seem an illogical statement, since the argument typically employed for the acquisition
of a health plan or health insurance is precisely the reduction of the financial risks associated to
an eventual health problem. However, it is necessary to consider that, the model does not allow
considering the result as evidence that the possession of a health plan or insurance increases the
probability of occurrence of catastrophic expenditures in health care.
Also, it is possible to consider the existence of an endogeneity bias, that is, as health plans
and health insurances, in general, are relatively expensive for most of the Brazilian individuals,
households that acquire health plans or insurances – especially if not granted by the company in
which any family members work – tend to have, at least, one family member with some kind of
chronic disease.
We try to deal with the possible endogeneity of health insurance by estimating an
instrumental variables model (following Greene (2000, pp.852-855)) and the instrument is the
17
percentage of household inhabitants that are formally employed. In these models, we also
incorporate the structure of the complex survey data.
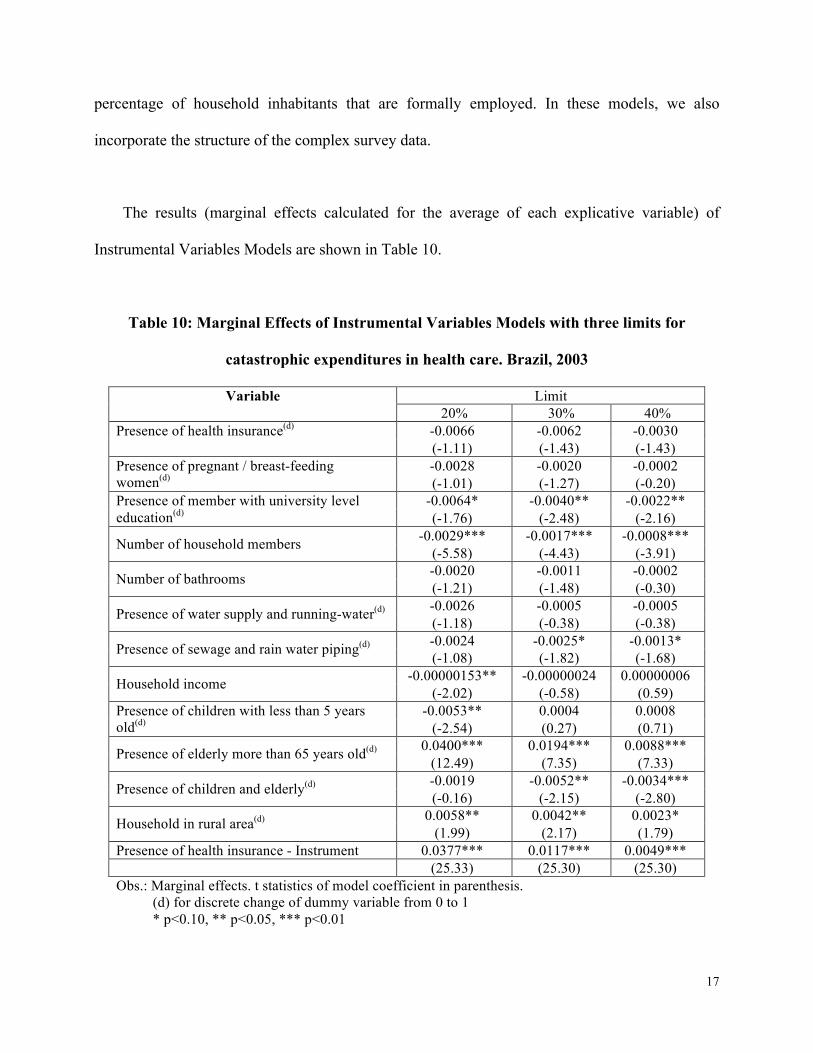
The results (marginal effects calculated for the average of each explicative variable) of
Instrumental Variables Models are shown in Table 10.
Table 10: Marginal Effects of Instrumental Variables Models with three limits for
catastrophic expenditures in health care. Brazil, 2003
Limit Variable 20% 30% 40%
-0.0066 -0.0062 -0.0030 Presence of health insurance(d) (-1.11) (-1.43) (-1.43)
-0.0028 -0.0020 -0.0002 Presence of pregnant / breast-feeding women(d) (-1.01) (-1.27) (-0.20)
-0.0064* -0.0040** -0.0022** Presence of member with university level education(d) (-1.76) (-2.48) (-2.16)
-0.0029*** -0.0017*** -0.0008*** Number of household members (-5.58) (-4.43) (-3.91) -0.0020 -0.0011 -0.0002 Number of bathrooms (-1.21) (-1.48) (-0.30) -0.0026 -0.0005 -0.0005 Presence of water supply and running-water(d) (-1.18) (-0.38) (-0.38) -0.0024 -0.0025* -0.0013* Presence of sewage and rain water piping(d) (-1.08) (-1.82) (-1.68)
-0.00000153** -0.00000024 0.00000006 Household income (-2.02) (-0.58) (0.59) -0.0053** 0.0004 0.0008 Presence of children with less than 5 years
old(d) (-2.54) (0.27) (0.71) 0.0400*** 0.0194*** 0.0088*** Presence of elderly more than 65 years old(d) (12.49) (7.35) (7.33)
-0.0019 -0.0052** -0.0034*** Presence of children and elderly(d) (-0.16) (-2.15) (-2.80) 0.0058** 0.0042** 0.0023* Household in rural area(d) (1.99) (2.17) (1.79)
Presence of health insurance - Instrument 0.0377*** 0.0117*** 0.0049*** (25.33) (25.30) (25.30) Obs.: Marginal effects. t statistics of model coefficient in parenthesis. (d) for discrete change of dummy variable from 0 to 1 * p<0.10, ** p<0.05, *** p<0.01

18
The following variables are statistically significant:
For 20% threshold: Negative impact (reduce the probability of catastrophic health spending)
– if there is someone in the household with higher education, number of household members,
Familiar Income, Presence of children; Positive impact (increase the probability of catastrophic
health spending) – if there is someone in the household 65 years old or more, if the household is
in the rural area.
For 30% threshold: Negative impact (reduce the probability of catastrophic health spending)
– if there is someone in the household with higher education, number of household members,
domestic sewage treated, presence of children and elderly. Positive impact (increase the
probability of catastrophic health spending) – if there is someone in the household 65 years old or
more, if the household is in the rural area.
For 40% threshold: Negative impact (reduce the probability of catastrophic health spending)
– if there is someone in the household with higher education, number of inhabitants, domestic
sewage treated, presence of children and elderly; Positive impact (increase the probability of
catastrophic health spending) – presence of elderly more than 65 years old and if the household is
in the rural area.

19
Discussion
The results seem to indicate the existence of regional differences – even between the urban
and rural zones – with regard to the incidence of catastrophic expenditures in health care, a fact in
itself deserves an in depth survey, since such differences may be linked to inefficiency in the
health care services provided publicly by the Unified Health System (Sistema Unico de Saude –
SUS), that could be caused, by lack of infrastructure or services supply, problems regarding
public health system communication in relation to the population; among other aspects.
Also, it should be interesting to analyze more extensively the role of catastrophic health care
expenditures in the impoverishment processes observed in other countries. In Brazil, catastrophic
expenditures in health care, associated to a decentralized public health system marked by deep
scarcity of resources in some regions, showed a certain degree of influence in bringing
households under the national poverty line.
In addition, it may be noticed that the presence of at least one household member with a
university level of education decreases the probability of occurrence of catastrophic expenditures
in health care. Thus, once again, a link between a higher level of education and better health,
already pointed out in other papers or projects, may be observed.
In conclusion, a point that also deserves a special attention is related to the fact that
households with at least one elderly member showed higher probability for the occurrence of
catastrophic expenditures in health care. This result indicates that further evaluations ought to be
20
carried out on the treatment currently applied to elderly individuals within SUS, which may
indicate to faults in the Brazilian public health services, which may end up forcing families to
incur private health care expenditures and compeling the household finances into complete
disarray.
Finally, our results indicate that when we incorporate both the complex structure of the data
and the endogeneity, we find that in Brazil the variable private health insurance is not statistically
significant to explain catastrophic health payments. But, when only the complex structure of the
data is incorporated, ignoring the possible endogeneity of health insurance, we find results
similar to Wagstaff and Lindelow(2008) have found to China. In this case, private health
insurance increases the risk of household incurring catastrophic health expenditures. Essentially,
the results show that, at best, private health insurance in Brazil is not contributing to reduce the
households´ financial risk.

21
Bibliographic References
DINIZ, B. P. C.; SERVO, L. M. S.; EIRADO, M.; PIOLA, S. F. Gasto das Famílias com Saúde
no Brasil: evolução e debate sobre gasto catastrófico. In: Fernando Gaiger Silveira; Luciana
Mendes Santos Servo; Tatiane Menezes; Sérgio Franciso Piola. (Org.). O gasto e consumo das
famílias brasileiras contemporâneas. 1a ed. Brasília: IPEA, 2007.
GREENE, W. Econometric Analysis, 4th edition, Prentice Hall, Upper Saddle River, 2000.
SILVEIRA, F. G.; CARVALHO, A. X. Y.; AZZONI, C. R.; CAMPOLINA, B.; IBARRA, A.
dimensão, magnitude e localização das populações pobres do Brasil. Texto para Discussão 1278.
Brasília: IPEA, maio de 2008.
WAGSTAFF, A. and LINDELOW, M. Journal of Health Economics. Volume 27, Issue 4, Pages
990-1005, 2008.
WAGSTAFF, A.; VAN DOORSLAER, E. Catastrophe and impoverishment in paying for health
care: with applications to Vietnam 1993-1998. Health Economics, v. 12, Issue 11, p. 921-933,
2003.
WONG, R. Gasto catastrófico en salud y grupos vulnerables en América Latina: Análysis
comparativo entre países. Grupo de Trabajo del Proyecto de Protección Financiera em Salud,
patrocinado por IDRC; 2009.
XU, K.; EVANS, D. B.; KAWABATA, K.; ZERAMDINI, R.; KLAVUS, J.; MURRAY, C. J. L.
Household catastrophic health expenditure: a multicountry analysis. The Lancet, v. 362, p. 111-
116, July 2003.


















