Cases in Transplantation
59
Case Studies of Infectious Case Studies of Infectious Complications in Complications in Hematopoietic Hematopoietic Stem Cell Stem Cell Transplantation Transplantation Deepali Kumar MD Deepali Kumar MD MSc MSc FRCPC FRCPC Infectious Diseases & Multi Infectious Diseases & Multi - - organ Transplantation organ Transplantation University Health Network; University of Toronto University Health Network; University of Toronto
description
Cases in Transplantation
Transcript of Cases in Transplantation

Case Studies of Infectious Case Studies of Infectious
Complications in Complications in
HematopoieticHematopoietic Stem Cell Stem Cell
TransplantationTransplantation
Deepali Kumar MD Deepali Kumar MD MScMSc FRCPCFRCPC
Infectious Diseases & MultiInfectious Diseases & Multi--organ Transplantationorgan Transplantation
University Health Network; University of TorontoUniversity Health Network; University of Toronto

Types of HSCTTypes of HSCT
Lymphoma
Myeloma
Autologous
non-myeloablative myeloablative
Related Matched Unrelated Haploidentical
Allogeneic Syngeneic
Donor Source
Greatest risk of
Infectious complications

AllogeneicAllogeneic TransplantationTransplantation
Recipient DonorConditioning:CyTBI or BuCy or BuFludarabine or
Anti-tumorImmunosuppressiveMyeloablative
Stem Cell InfusionDay 0
G-CSF- mobilized stem cells / marrow
Ex vivo manipulation:
T-cell depletion
CD34 selection
Suicide gene insertion
Adoptive transfer of
antigen-specific T cells

Complications of Complications of AllogeneicAllogeneic
TransplantationTransplantation
INFECTION
GRAFT vs HOST DISEASE
RELAPSE
GVHD prophylaxis and treatments:
Cyclosporin, Tacrolimus, Methotrexate,
Prednisone, MMF, ATG, Alemtuzumab, Sirolimus
Monoclonal antibodies
Pentostatin


SurvivalSurvival

Timeline of InfectionTimeline of Infection
PHASE 1: DAY 0-30 (PRE-
ENGRAFTMENT)
Neutropenia
Damaged mucocutaneous barriers
Febrile Neutropenia
VGS, Staph, GNB
Candida, Early Aspergillus
HSV, HHV6
Idiopathic pneumonitis

PHASE 2: DAY 30-100 (EARLY POST-
ENGRAFTMENT)
Effective phagocytic function
Abnormal CD4/CD8 ratio
IgG2, IgG4, IgA, class switching deficiency
Prolonged immunodeficiency if CMV or
Acute GVHD
VGS, Staph
Moulds (Late Aspergillus)
CMV, Respiratory Viruses,
Toxoplasma

PHASE 3: DAY >100 days (LATE
POST-ENGRAFTMENT)
Macrophage deficiency
Impaired chemotaxis
Ig subclass deficiency
Poor opsonization and RES dysfn
Chronic GVHD
Encapsulated bacteria
Moulds
Pneumocystis
CMV, VZV, Respiratory Viruses

Immune reconstitutionImmune reconstitution
0 6 12
Phagocytic function:
Neutrophil recovery
Impaired function
Humoral immunity:
IgG levels normal
Subclass deficiency
Cellular immunity:
Delayed with GVHD
Months post-transplant

Phase I, preengraftment Phase II, postengraftment PhaseIII
> 30 days 30-100 days > 100 days
Host immune neutropenia, mucositis Impaired cellular immunity Impaired cellularsystem defect acute GvHD acute and chronic GvHD humoral immunity
chronic
Device risk Central line
Respiratory and enteric viruses
Herpes simplexcytomegalovirus
Encapsulated bacteria
Aspergillus
Gram-negative bacilli
Staphylococcal epidermidis
Aspergillus
Candida species
Pneumocystis jiroveci
Herpes simplex
varicella

Case 1Case 1
•• 25 25 y/oy/o man 21 days post MUD man 21 days post MUD
allogeneicallogeneic SCT for ALLSCT for ALL
•• NeutropenicNeutropenic (ANC 0.2), (ANC 0.2), MucositisMucositis
•• CyclosporinCyclosporin, Prednisone 60 mg/d, Prednisone 60 mg/d
•• Fever to 39C with gradual onset Fever to 39C with gradual onset
dyspneadyspnea, increasing O, increasing O22 requirementsrequirements
•• CXR doneCXR done


CaseCase
•• Started on broad spectrum antibiotics: Started on broad spectrum antibiotics:
Piperacillin/tazobactamPiperacillin/tazobactam + + azithromycinazithromycin
•• Day 23 postDay 23 post--transplant transplant –– diffuse diffuse
maculopapularmaculopapular rash, fever continuesrash, fever continues
•• Antimicrobials changed to Antimicrobials changed to MeropenemMeropenem
for possible penicillinfor possible penicillin--related rashrelated rash

•• Day 24 Day 24 –– BAL doneBAL done
–– C&S negativeC&S negative
–– Fungal, AFB stains negativeFungal, AFB stains negative
–– Respiratory virus DFA Respiratory virus DFA negneg
–– LegionellaLegionella, PCP , PCP negneg
•• CMV CMV antigenemiaantigenemia –– insufficient cellsinsufficient cells

PneumonitisPneumonitis postpost--SCTSCT
•• InfectiousInfectious–– BacterialBacterial
–– Respiratory viruses, CMV, HHVRespiratory viruses, CMV, HHV--6, HSV6, HSV
–– PCP, PCP, legionellalegionella
–– AFB, fungalAFB, fungal
•• NonNon--infectiousinfectious–– P.edema, Alveolar hemorrhageP.edema, Alveolar hemorrhage
–– Idiopathic interstitial Idiopathic interstitial pneumonitispneumonitis (8(8--17%)17%)
–– Acute GVHDAcute GVHD
–– Chronic GVHD (Chronic GVHD (bronchiolitisbronchiolitis obliteransobliterans))

CaseCase
•• HHVHHV--6 PCR + 30,000 copies/6 PCR + 30,000 copies/mLmL
•• Is this the culprit?Is this the culprit?

HERPESVIRUSESHERPESVIRUSES
Alpha
� HSV 1 and 2
� Varicella
zoster virus
Beta
� CMV
� HHV-6 and HHV-7
Gamma
�EBV ���� PTLD
�KSHV or HHV-8 ����
Kaposi’s Sarcoma

HHVHHV--6 Epidemiology6 Epidemiology
•• Etiology of Etiology of roseolaroseola ((exanthemexanthem subitumsubitum))
•• During infection, primary target cell (as for HIV) is During infection, primary target cell (as for HIV) is CD4+ T lymphocytesCD4+ T lymphocytes
•• LifeLife--long latency in epithelia of bronchial and long latency in epithelia of bronchial and salivary glands, and probably salivary glands, and probably monocytesmonocytes/macrophages/macrophages
•• Two subtypes: HHVTwo subtypes: HHV--6A and HHV6A and HHV--6B6B(6B most commonly reactivates)(6B most commonly reactivates)
•• Adult Adult seroprevalenceseroprevalence is 90%is 90%

HHVHHV--6 in HSCT6 in HSCT
•• An increasingly recognized pathogenAn increasingly recognized pathogen
•• 22--4 weeks post4 weeks post--transplanttransplant
•• Linked to several clinical syndromes Linked to several clinical syndromes (although not conclusive):(although not conclusive):–– Interstitial Interstitial pneumonitispneumonitis
–– Skin rash similar to acute GVHDSkin rash similar to acute GVHD
–– EncephalitisEncephalitis
–– Bone marrow suppression or delayed engraftmentBone marrow suppression or delayed engraftment
–– ThromboticThrombotic microangiopathymicroangiopathy
–– EnteritisEnteritis

Incidence of HHVIncidence of HHV--6 Infection in6 Infection in
Transplant RecipientsTransplant Recipients
0
10
20
30
40
50
60
70
80
90
percent (%
)
over
all
Bon
e m
arro
w
liver
kidn
ey
Hea
rt
Lung

HHV6 DiagnosticsHHV6 Diagnostics
•• Serology Serology –– not useful in HSCT settingnot useful in HSCT setting
•• Viral isolation Viral isolation –– low sensitivitylow sensitivity
•• Quantitative realQuantitative real--time PCR time PCR –– to detect to detect DNAemiaDNAemia
•• ImmunohistochemistryImmunohistochemistry on tissue specimenson tissue specimens
•• AntigenemiaAntigenemia assaysassays

Is therapy useful?Is therapy useful?
•• In vitro, HHV6 is sensitive to GCV, In vitro, HHV6 is sensitive to GCV, FoscarnetFoscarnet, , CidofovirCidofovir, resistant to Acyclovir, resistant to Acyclovir
•• Clinical efficacy is unknownClinical efficacy is unknown
•• Case reports suggest decrease in viral load Case reports suggest decrease in viral load with with GanciclovirGanciclovir, no controlled trials, no controlled trials
•• Decreasing Decreasing immunosuppressionimmunosuppression may helpmay help
•• No evidence to support routine monitoring of No evidence to support routine monitoring of HHV6HHV6

Case 2Case 2
•• 35 y/o woman 12 months post 35 y/o woman 12 months post allogeneicallogeneicmatched unrelated stem cell transplant matched unrelated stem cell transplant
•• Underlying disease: AML in remissionUnderlying disease: AML in remission
•• Chronic problems with GVHD of skin, gut Chronic problems with GVHD of skin, gut (diarrhea)(diarrhea)
•• Meds: Prednisone 60 mg daily, MMF 500mg Meds: Prednisone 60 mg daily, MMF 500mg bid, bid, SeptraSeptra qMWFqMWF

•• Presents to clinic in February 2006 with 3 day Presents to clinic in February 2006 with 3 day hxhx of fever 38.6C, dry cough, of fever 38.6C, dry cough, exertionalexertionaldyspneadyspnea
•• Illness in family members? Epidemiologic Illness in family members? Epidemiologic exposures: noneexposures: none
•• P/E: BP 110/70 HR 120 RR 30 O2 sat 85% R/AP/E: BP 110/70 HR 120 RR 30 O2 sat 85% R/A
•• Chest: bibasilar cracklesChest: bibasilar crackles
•• WBC 12.5WBC 12.5


Empiric antibioticsEmpiric antibiotics
•• CeftriaxoneCeftriaxone + + AzithromycinAzithromycin
•• Piperacillin/tazobactamPiperacillin/tazobactam + ciprofloxacin+ ciprofloxacin
•• VoriconazoleVoriconazole + + ImipenemImipenem
•• TMP/SMX + TMP/SMX + Piperacillin/tazobactamPiperacillin/tazobactam + + VoriconazoleVoriconazole + + OseltamivirOseltamivir
•• OtherOther

ResultsResults
•• BAL BAL –– Streptococcus Streptococcus pneumoniaepneumoniae and and
Influenza AInfluenza A
•• Blood culture Blood culture –– S. S. pneumoniaepneumoniae

Key pointsKey points
•• Two vaccineTwo vaccine--preventable diseases: preventable diseases:
pneumococcuspneumococcus & influenza& influenza
•• Vaccine recommendationsVaccine recommendations
•• ImmunogenicityImmunogenicity of of pneumococcalpneumococcal and and
influenza vaccines postinfluenza vaccines post--SCTSCT

Invasive Invasive pneumococcalpneumococcal disease disease
postpost--SCTSCT
•• Incidence of IPI: 8.2 / 1000 transplantsIncidence of IPI: 8.2 / 1000 transplants
•• Chronic GVHD: 20.8 / 1000Chronic GVHD: 20.8 / 1000
•• AutologousAutologous: 3.8 / 1000: 3.8 / 1000
•• General Population: ~10General Population: ~10--15 / 100,00015 / 100,000
•• Most disease appears to occur >100dMost disease appears to occur >100d
•• Risk factors: Risk factors: alloallo transplant; chronic transplant; chronic
GVHDGVHD
Engelhard et al, Br J Hem 2003; Kulkarni et al, Blood 2000

What do we know about What do we know about
PneumococcalPneumococcal vaccine responses?vaccine responses?
•• Antibody responses present 6Antibody responses present 6--12 12 mosmos post post alloallo SCT in patients without GVHDSCT in patients without GVHD
•• No improvement with two doses of vaccineNo improvement with two doses of vaccine
•• No advantage to donor vaccination with No advantage to donor vaccination with polysaccharide vaccinepolysaccharide vaccine
•• No advantage in vaccination of auto SCT pts No advantage in vaccination of auto SCT pts before stem cell harvestbefore stem cell harvest
Guinan Transplantation 1994; Storek BMT 2004

What may work?What may work?
•• Donor vaccination with Donor vaccination with pneumococcalpneumococcalconjugate vaccineconjugate vaccine
•• EBMT recommendation: single dose of EBMT recommendation: single dose of PS vaccine at 12 months, measure PS vaccine at 12 months, measure immunity q 2immunity q 2--3 years3 years
•• CDC recommendation: PS vaccine at CDC recommendation: PS vaccine at 12, 24 months and q5 years12, 24 months and q5 years
Ljungman, BMT 2005; MMWR 2000

Influenza vaccineInfluenza vaccine
•• Influenza can be fatal even several years Influenza can be fatal even several years
postpost--SCTSCT
•• Annual influenza vaccination is Annual influenza vaccination is
recommended but timing postrecommended but timing post--SCT is unclearSCT is unclear
–– < 6 months : no response< 6 months : no response
–– 6 6 mosmos –– 2 yrs: 25% response2 yrs: 25% response
–– > 2 yrs: 60% response> 2 yrs: 60% response
–– Two doses: marginal benefitTwo doses: marginal benefit
Engelhard et al. BMT 1993

What can be done?What can be done?
•• EBMT: Single dose of inactivated vaccine no EBMT: Single dose of inactivated vaccine no
sooner than 4sooner than 4--6 months post6 months post
•• CDC: vaccine no sooner than 6 CDC: vaccine no sooner than 6 mosmos
•• Yearly vaccination thereafterYearly vaccination thereafter
•• Vaccinate family and transplant unit staffVaccinate family and transplant unit staff
Ljungman, BMT 2005; MMWR 2000

VaccinationsVaccinations
X*MMR
XXXiPV
XXXHepB
XXXTd
X*Varicella
XXXHiB
XXPneumococcal PS
241412
mos
Vaccine
* No immunosuppression or GVHD

Clinical QuestionClinical Question
•• The stem cell transplant clinician calls you to The stem cell transplant clinician calls you to
say that he would like to start using say that he would like to start using CampathCampath
for conditioning prefor conditioning pre--HSCTHSCT
•• He wonders if he should alter his He wonders if he should alter his
antimicrobial prophylaxis or monitoring antimicrobial prophylaxis or monitoring
strategy for infectious complicationsstrategy for infectious complications
•• You sayYou say……

CampathCampath--1H (1H (AlemtuzumabAlemtuzumab))
•• CD52 Monoclonal antibodyCD52 Monoclonal antibody
•• Used in the following settings: Used in the following settings:
–– therapy for therapy for lymphoproliferativelymphoproliferative
malignancy (CLL)malignancy (CLL)
–– low intensity conditioning regimen prelow intensity conditioning regimen pre--
HSCT (with HSCT (with busulfanbusulfan, , fludarabinefludarabine))
–– Induction therapy for solid organ Induction therapy for solid organ
transplantstransplants

CampathCampath ((AlemtuzumabAlemtuzumab))
•• Reduces GVHD but Potent Reduces GVHD but Potent immunosuppressiveimmunosuppressivewith delayed immune reconstitutionwith delayed immune reconstitution
•• Lymphocyte population depleted by Lymphocyte population depleted by cell cell lysislysis (ADCC)(ADCC)
•• Long lasting effects, Long lasting effects, lymphopenialymphopenia up to up to 2 years (median 9 months)2 years (median 9 months)

Infectious ComplicationsInfectious Complications
•• Several case reports and seriesSeveral case reports and series
•• Most common Most common OIsOIs: :
–– HSV reactivation, HSV reactivation, CMVCMV, VZV, PCP and , VZV, PCP and
Invasive Pulmonary Invasive Pulmonary AspergillosisAspergillosis
•• Most common Most common NOIsNOIs::
–– Sepsis/Sepsis/bacteremiabacteremia, pneumonia, pneumonia
Martin et al, CID 2006; Thursky Br J Hem 2006

CMV prophylaxis & CMV prophylaxis & CampathCampath
conditioningconditioning•• Retrospective study: Acyclovir prophylaxis (n=18) vs. preRetrospective study: Acyclovir prophylaxis (n=18) vs. pre--
transplant transplant GanciclovirGanciclovir + post+ post--transplant transplant ValacyclovirValacyclovir (n=67)(n=67)
•• Population: undergoing HSCT with Population: undergoing HSCT with CampathCampath conditioningconditioning
Kline et al, BMT 2006
45 days45 days
29%29%
Gan+ValacyGan+Valacy
0.0080.00820 days20 daysTime to CMVTime to CMV
0.0040.00453%53%CMV CMV viremiaviremia
ppAcyAcy

SummarySummary
•• Recognition of emerging pathogens in Recognition of emerging pathogens in
HSCTHSCT
•• Preventative measures for HSCT Preventative measures for HSCT
patientspatients
•• Newer Newer immunosuppressivesimmunosuppressives with new with new
challenges for the ID physicianchallenges for the ID physician

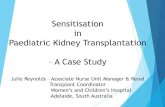
An unusual caseAn unusual case
•• 39 y/o woman presents with vision loss and 39 y/o woman presents with vision loss and pain of left eye in Aprpain of left eye in Apr’’0404
•• Recent Recent hxhx: :
–– Sept Sept ‘‘03, pt had a MUD SCT for AML03, pt had a MUD SCT for AML
–– GVHD of gut, skin, liverGVHD of gut, skin, liver•• Prednisone 100Prednisone 100--125mg/d; 125mg/d; CsACsA 175mg bid175mg bid
–– Recurrent episodes CMV Recurrent episodes CMV viremiaviremia NovNov’’03 03 –– Mar Mar ’’04 04 treated with GCVtreated with GCV
–– PancytopeniaPancytopenia –– JanJan’’04, transfused, 04, transfused, SeptraSeptra d/cd/c’’dd

•• AprApr’’0404
–– blurred vision and pain of left eye, blurred vision and pain of left eye, scleralscleral
edema, tearing of eyeedema, tearing of eye
•• Ophthalmology Ophthalmology dxdx: posterior : posterior uveitisuveitis
and and vitritisvitritis, possible , possible endophthalmitisendophthalmitis, ,
hypopyonhypopyon

11stst MRIMRI

Posterior Posterior UveitisUveitis, , KeratitisKeratitis in SCTin SCT
•• InfectiousInfectious
–– ToxoplasmaToxoplasma
–– CMV, HSVCMV, HSV
–– SyphilisSyphilis
–– MycobacterialMycobacterial
+ + EndophthalmitisEndophthalmitis
–– NocardiaNocardia
–– Candida, Crypto, Candida, Crypto, AspergillusAspergillus, , ScedoScedo, , BlastomycesBlastomyces, , CoccidioidesCoccidioides
•• NonNon--infectiousinfectious
–– Intraocular leukemia, autoimmuneIntraocular leukemia, autoimmune

•• VitrectomyVitrectomy 2 weeks later 2 weeks later –– benign infiltration, no benign infiltration, no HSVHSV
•• High dose Prednisone 150mg d/t visual lossHigh dose Prednisone 150mg d/t visual loss
•• May May ’’04 04 –– progression of eye disease, progression of eye disease, proptosisproptosis, , scleralscleral edemaedema
•• New subcutaneous nodulesNew subcutaneous nodules
•• Hospital admission for broad spectrum antibiotics / Hospital admission for broad spectrum antibiotics / antifungalsantifungals

22ndnd MRIMRI

CT abdomen CT abdomen –– subcusubcu nodulesnodules

CutaneousCutaneous / Subcutaneous nodules/ Subcutaneous nodules
•• CandidemiaCandidemia –– tropicalistropicalis
•• CryptococcusCryptococcus
•• FusariumFusarium
•• MycobacterialMycobacterial fortuitumfortuitum / / abscessusabscessus / TB/ TB
•• NocardiaNocardia
•• SporothrixSporothrix
•• NonNon--infectiousinfectious–– LeukemicLeukemic infiltrationinfiltration
–– SweetSweet’’s syndromes syndrome

Case (contCase (cont’’d)d)
•• Skin biopsy x 2Skin biopsy x 2–– chronic inflammation, chronic inflammation,
fungal stain neg.fungal stain neg.
•• ScleralScleral edema beginning to affect right edema beginning to affect right
eye. eye. ScleralScleral biopsy neg.biopsy neg.
•• EnucleationEnucleation of left eyeof left eye
for diagnosis / therapyfor diagnosis / therapy

Enucleation



NocardiaNocardia asteroidesasteroides
•• Disseminated disease reported postDisseminated disease reported post--
SCT in case report and case seriesSCT in case report and case series
–– Incidence 0.3%Incidence 0.3%
–– Time to diagnosis: 210 d post Time to diagnosis: 210 d post txtx
–– AlloAllo SCTSCT
–– Chronic GVHDChronic GVHD
–– 40% pts on TMP/SMX prophylaxis40% pts on TMP/SMX prophylaxis
Van Burik, CID 1997; Daly, TransID 2003

Another unusual caseAnother unusual case
•• 52 y/o woman 6 months post 52 y/o woman 6 months post autologousautologous SCT SCT for multiple for multiple myelomamyeloma, on , on hemodialysishemodialysis
•• Presents with 4 wk Presents with 4 wk hxhx of right leg lesionsof right leg lesions
•• No systemic symptoms, no lesions No systemic symptoms, no lesions elsewhereelsewhere
•• Skin biopsy Skin biopsy –– necrotizing inflammationnecrotizing inflammation
•• No response to 2 weeks of IV No response to 2 weeks of IV CefazolinCefazolin



Skin biopsySkin biopsy
•• Mycobacterium abscessusMycobacterium abscessus
•• Clarithromycin, Rifampin, EthambutolClarithromycin, Rifampin, Ethambutol
•• Unable to tolerate Rif / EthUnable to tolerate Rif / Eth
•• Continued on Clari alone with Continued on Clari alone with
resolutionresolution

Thank you!Thank you!