Case Study Meniscus Tears And Osteochondral Fractures
23
Case Studies of the Knee: Meniscus Tears and Osteochondral Fractures Jennifer Ho (Injury A) Joshua Honrado (Injury B) Claire DeBolt (Injury C)
-
Upload
clairedebolt -
Category
Documents
-
view
1.652 -
download
4
description
Case Study presentation given to UCLA Sports Medicine Internship Program; Co-Presenters: Josh Honrado and Jennifer Ho
Transcript of Case Study Meniscus Tears And Osteochondral Fractures

Case Studies of the Knee:Meniscus Tears
and Osteochondral Fractures
Jennifer Ho (Injury A)Joshua Honrado (Injury
B)Claire DeBolt (Injury C)

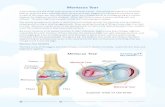
Knee aNATOMY

KNEE ANATOMY

Injury a
• 20 year old male track athlete• 5k and 10k distance events
• 3 years prior, consistent discomfort and pain along L medial joint line
• 4 weeks prior, escalated to extreme pain
• Spoke with ATC and consulted physicians• Preoperative exam and MRI revealed a medial
meniscus tear
• Did not respond well to conservative treatments
• Surgery on Jan 21, 2011

Injury B
• 20 year old male track athlete• High jump, triple jump
• Athlete c/o pain x1wk and swelling in R knee after playing basketball, unable to run/ jump w/o pain (pain similar to initial surgery)
• Spoke with ATC and consulted physicians• Preoperative exam and MRI revealed
possible medial meniscus tear
• Did not respond well to conservative treatment and Celebrex
• Surgery on October 21, 2010

INJURY C
• Previous knee injuries
• Pain and effusion in the right knee; no specific mechanism
• MRI results: anterolateral meniscal abnormality
• Pain over the lateral joint line; negative for special tests
• Diagnosis: Lateral meniscal tear
• Arthroscopic menisectomy

MenisCectomy

MENISCECTOMY IMAGING

Surgery a, b oUTCOMEs
• Partial meniscectomy of the L medial meniscus
• Arthroscopy revealed complex degenerative tear of the posterior horn of the medial meniscus in the white-white zone • Horizontal and vertical tears
• Partial meniscectomy of R medial meniscus
• Arthroscopy revealed mild superficial fraying of posterior horn of medial meniscus in the white-white zone • Same area where original meniscectomy was performed• Originally resected only the torn unstable parts of the
medial meniscus

SURGERY A, B

cHONDRAL FRACTUREs

Screw Fixation and Microfracture Basis

CHONDRAL FRACTURES

General rehabilitation plan
• Decrease Pain and Reduce Swelling; RICE
• Knee Joint Mobilizations• Reduces arthrofibrosis
• Flexibility/ ROM
• Muscular Strength • Quads, hamstrings, abd, add, gastroc
• Neuromuscular Control; Proprioception
• Cardiorespiratory Fitness • Non-weight bearing
• Functional Progression • Sport-specific skills

Rehab a
• Week 1-2: Control pain and swelling, core, ankle and hip passive ROM and strength, balance• Modalities: russian stim, micromassage, cryopress, soft tissue massage
• Gentle stretching, clamshells, calf raises, SL airex balance
• Week 3-8: strengthening and balance, cardiovascular fitness, effusion reduction• Cycling, swimEx, elliptical, decreased activity due to persistent effusion
• Prone hangs (knee extension), 4 way ankle TB exercises, DL squats, russian twists, monster walks, forward/backward walks
• Jump rope, DL/SL squats, lunges, increased time on cardio workouts
• Modalities: graston, microflush, soft tissue massage
• Week 9-11: reduce posterior capsule tightness, proprioceptive + dynamic stability, cardiovascular fitness• DL/SL squats, airex lunge, tennis balance, step-ups, walking supermans, knee grabs, ABC skips,
slide board, AlterG progression
• Modalities: graston
• Week 12-Present: functional progression, return-to-sport• FMS (21), cleared to begin running
• Currently running on the track every other day, slowly adding mileage

REHAB B
• Rehabilitation was a lot faster than initial surgery• Swelling reduced and full ROM by 5th week
• Winter break slowed progression
• Focused on proprioception (SL balance), box jumps, progression of short step approaches
• 4 months after surgery cleared PT eval with FMS screening for in-door high jump• Later cleared for outdoor long-jump

REHAB C
• Weeks 1-3: Decreasing pain and swelling, achieving full extension, slowly increasing ROM, increasing quad control and VMO tone, maintaining glute, hip• Modalities (Russian, microcurrent); Soft tissue mobilization;
Cryotherapy• Ankle pumps; Quad and HS sets; Adductor sets, supine hip flexion,
prone glute activation; Bike (ROM)
• Week 3: PWB (50%), ROM 0-30; Goals: effusion control, maintain extension, gait activity• Extension exercises
• Week 4-7: Passive ROM 1-110; Goals: effusion control, soft tissue and joint mobilization, maintain full extension, FOCUS: VMO• Wall slides • Heel slides, Double leg bridges with squeeze, weight shifts, calf raises,
balance

REHAB C
• Week 7; X-Ray 2: Screw and fragment intact; FWB permitted• Swim-Ex• Balance Exercises• SL exercises
• Week 8; X- Ray 3:No evidence of hardware complication; etc. No pain, little swelling observed.
• Weeks 9-12: Maintained rehab program• 3-way hip, clamsheels (TB), DL bridged (med ball), SL
bridges, SLR, TB side steps, calf raises• Swim Ex: 4 way hip, flutter and bike kicks, jogging

REHAB c
• SURGERY 2: Hardware removal
• Lower extremity strengthening; proprioception
• 3 way hip, clam shells, squatting, side stepping, wall sits, bridging, calf raises, balance exercises
• Lunges, bridge walk-outs, power-ups, monster walks, slide-board, squatting

aTHLETE a: cURRENT STATUS
• As of 11.5 week post-op he was discharged from PT and began to slowly increase mileage
• Currently progressed to 3 miles every other day
• Occasionally feels discomfort from the site of partial meniscectomy when speeding up

Athlete b:current status
• Full participation in outdoor track and field• Does high-jump, long jump, but no longer does
triple jump
• Recently had a case of shin-splints
• Occasionally feels pain discomfort from site of meniscectomy

Athlete C: Current Status
• ~5 weeks post surgery
• Progressing smoothly• Alter G: 50% 60%
• Expected to return to full play by summer ball

THE END