Case Studies in Hospital’s Community Partnerships · All Five Providence Hospitals Discharge...
21
Case Studies in Hospital’s Community Partnerships June Simmons, Partners in Care Foundation Sally Ramirez, RN, MLTCA, IQCI, Providence St. Joseph Health
Transcript of Case Studies in Hospital’s Community Partnerships · All Five Providence Hospitals Discharge...

Case Studies in Hospital’s Community Partnerships
June Simmons, Partners in Care FoundationSally Ramirez, RN, MLTCA, IQCI, Providence St. Joseph Health

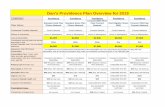
Problem: Inconsistent Transition of Care Programs Across the LA Market
California Tarzana St. Josephs
Holy Cross
LCOM T LCOM SP Saint Johns
Total 30 day All Cause Rate (Q3 2015 –Q3 2016)
18.5% 19.7% 19.7% 22.0% 17.5% 16.6% 14.5%
CY 2013Baseline
19.1% 20.0% 21.6% 19.1% 16.5% 12.6%
2

Build or Buy?
• Interdisciplinary analysis of all programs offering TOC services
• Saint Johns experience with the Innovation Center pilot and PIC
3

4
Our Partnership• Partners collaborate with hospitals, physician groups, health plans, community-based
organizations, and government agencies to deliver services that support adults with complex health and social services needs and their caregivers and families
• Evidence-based programs demonstrated to significantly reduce costly hospital readmissions, ED visits, and nursing home placements
Our Focus on Innovation• We shift the emphasis from illness care to preventive care, reducing costs and
improving quality of life for those with chronic conditions• NCQA accredited for Complex Care Management as defined by CMS www.PICF.org
Partners in Care: Mission-Driven OrganizationOur MissionPartners shape the evolving health system by developing and spreading high-value models of community-based care and self-management

This is an evidence-based program that incorporates a strong component of specific cultural and linguistic coverage both regionally and statewide.• Focuses on managing social determinants to maintain patients in their
community setting• Dedicated coach in each ministry to introduce the program to the
patient and initiate referral to the program• Home visit within 72 hours after discharge from hospital or post-acute
SNF using evidence-based Coleman Care Transitions Intervention (Coaching Model) 5
Partners in Care Program Components

• Complete an in-home inventory of all prescribed and OTC medications in the home. Coach works with the pharmacist
• Follow-up calls over 30-day period, arrange physician appointments and transportation as needed
• Cost per case for 30-day program
Partners is committed to a strong partnership with Providence.
6
Partners in Care Program Components(cont.)

Plan• Follow high readmission risk patients
– Contracted health plans to pay for their members– Ministry to pay for Medicare FFS patients
oPropose patients with high-risk LACE score and have one of the Readmission Penalty diagnosis
• Achieve full ROI in 3-5 years– CMS bases the Readmission Penalty on data that is
years old
7

Home Meds ProgramPartners In Care Coach in coordination with PIC Pharmacist will:• Complete a review for identified potential MRPs and make
recommendations for resolution• Pharmacist contacts provider and/or patient to resolve issues• Inventory all meds being taken and present in the home, including over-the-
counters/supplements and send an electronic report to the pharmacist• Assess for potential adverse effects, e.g., BP/pulse, falls, dizziness, confusion• Document adherence issues and understanding of medication regimen • Medication list provided to patient and prescribers• Partners in Care Algorithm identifies targeted potential medication-related
problems (MRPs) • Partners in Care will coordinate with Providence Pharmacy Clinic
8

Project Timeline
Intervention Design August 2017• Partners in Care, Regional leadership, Director CM
from pilot ministry• Weekly meetings• Workflow development• Agreement on metrics• Establish minimum volumes
9

Data for Minimum Volumes# of Cases MONTHLY Volume
FACILITY Diagnosis Min Max Average
CHC AMI 1 4 2CABG 2 2 2Heart Failure 3 16 9Pneumonia 2 6 4Sepsis 14 28 20Total Hip/Knee 1 3 2
CHC Total 23 59 39CJN AMI 1 5 2
CABG 1 1 1Heart Failure 3 7 4Pneumonia 1 9 5Sepsis 6 20 12Total Hip/Knee 2 8 5
CJN Total 14 50 29CLS AMI 1 1 1
Heart Failure 1 3 1Pneumonia 1 3 2Sepsis 1 11 5Total Hip/Knee 1 2 1
CLS Total 5 20 11CLT AMI 1 5 3
CABG 1 6 2Heart Failure 6 18 10Pneumonia 1 10 5Sepsis 9 22 13Total Hip/Knee 1 4 2
CLT Total 24 43 33CSJ AMI 1 3 2
Heart Failure 3 23 10Pneumonia 1 9 5Sepsis 17 29 23Total Hip/Knee 1 6 3
CSJ Total 36 61 42CTZ AMI 1 6 2
CABG 1 1 1Heart Failure 7 25 16Pneumonia 1 12 5Sepsis 26 42 32Total Hip/Knee 1 10 3
CTZ Total 37 96 5910

September 2017
• Education Design– MD one page – Patient pamphlet
11

12

13

14

Prior to Rollout• Obtain PSJH badges for all coaches• Coaches cleared by Employee Health• Obtain EPIC access for Coaches• Train Coaches on how to document in EPIC• CM Directors
– Participate in daily touch base calls– Make sure Director or Manager on site week 1 of roll out– Arrange for Coach to meet staff prior to go live date– Arrange for Coach to meet key medical staff prior to go live date– Educate nursing leadership– Educate staff on how to submit referrals 15

October 2018
• Rollout Design• Started with one patient at pilot ministry
– Reviewed the single patient experience and mademodifications at each part of the rollout
– Then rolled out to one unit– Then rolled out entire ministry
16

All Five Providence Hospitals
Discharge Month # of Readmits
# that Received Intervention Readmit Percent # of Readmits
# that DID NOT Receive
InterventionReadmit Percent
Total # of Readmits
Total # of Discharges
Readmit Percent
Oct-17 2 25 8.00% 2 14 14.29% 4 39 10.26%Nov-17 27 152 17.76% 39 108 36.11% 66 260 25.38%Dec-17 14 145 9.66% 41 127 32.28% 55 272 20.22%Jan-18 22 204 10.78% 43 177 24.29% 65 381 17.06%Feb-18 11 98 11.22% 25 110 22.73% 36 208 17.31%
Mar-18 17 137 12.41% 40 165 24.24% 57 302 18.87%Apr-18 22 164 13.41% 67 252 26.59% 89 416 21.39%
May-18 21 134 15.67% 56 225 24.89% 77 359 21.45%Jun-18 19 126 15.08% 51 218 23.39% 70 344 20.35%
TOTAL 155 1185 13.08% 364 1396 26.07% 519 2581 20.11%
Average # of Patients Receiving Intervention Per Month: 131.7
Discharge Month
Intervention Group Control Group
Oct-17 8.00% 14.29%Nov-17 17.76% 36.11%Dec-17 9.66% 32.28%Jan-18 10.78% 24.29%Feb-18 11.22% 22.73%Mar-18 12.41% 24.24%Apr-18 13.41% 26.59%
May-18 15.67% 24.89%Jun-18 15.08% 23.39%
INTERVENTION GROUP CONTROL GROUP TOTAL
Readmission Rate
8.00%
17.76%
9.66%10.78% 11.22%
12.41%13.41%
15.67% 15.08%14.29%
36.11%
32.28%
24.29%22.73%
24.24%26.59%
24.89%23.39%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18
Readmission Rate--Intervention vs. Control Group
Intervention Group Control Group
17

Discharge Month
# that Received Intervention
# that DID NOT Receive
InterventionOct-17 25 14
Nov-17 152 108Dec-17 145 127Jan-18 204 177Feb-18 98 110Mar-18 137 165Apr-18 164 252
May-18 134 225Jun-18 126 218
Discharge Month
Cumulative # of Patients that
Received Intervention
Oct-17 25Nov-17 177Dec-17 322Jan-18 526Feb-18 624Mar-18 761Apr-18 925
May-18 1059Jun-18 1185
Discharge Month
# that Received Intervention
# that DID NOT Receive
InterventionTotal # of
Discharges
Percent Received
Intervention
Percent Who Did Not Receive
InterventionOct-17 25 14 39 64.10% 35.90%
Nov-17 152 108 260 58.46% 41.54%Dec-17 145 127 272 53.31% 46.69%Jan-18 204 177 381 53.54% 46.46%Feb-18 98 110 208 47.12% 52.88%Mar-18 137 165 302 45.36% 54.64%Apr-18 164 252 416 39.42% 60.58%
May-18 134 225 359 37.33% 62.67%Jun-18 126 218 344 36.63% 63.37%
Discharge Month
Percent of Patients that Received Intervention
Percent of Patients that Did Not Receive Intervention
Oct-17 64.10% 35.90%Nov-17 58.46% 41.54%Dec-17 53.31% 46.69%Jan-18 53.54% 46.46%Feb-18 47.12% 52.88%Mar-18 45.36% 54.64%Apr-18 39.42% 60.58%
May-18 37.33% 62.67%Jun-18 36.63% 63.37%
25
152 145
204
98
137164
134126
14
108127
177
110
165
252225 218
0
50
100
150
200
250
300
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18
Number of Patients by Month-Intervention vs. Control Group
# that Received Intervention # that DID NOT Receive Intervention
25177
322
526624
761
9251059
1185
0
200
400
600
800
1000
1200
1400
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18
Cumulative Number of Patient Served Over Time
64.10% 58.46% 53.31% 53.54%47.12% 45.36%
39.42% 37.33% 36.63%35.90%41.54% 46.69% 46.46%
52.88% 54.64%60.58% 62.67% 63.37%
0.00%
20.00%
40.00%
60.00%
80.00%
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18
Percent of Patients by Month--Intervention vs. Control Group
Percent of Patients that Received Intervention
Percent of Patients that Did Not Receive Intervention
18

Current State• Partners in Care has cared for over 3,000 of
our high-risk Medicare FFS patients• We have seen only 48 readmissions for a < 2%
readmission rate (anecdotal data captured byPartners in Care coaches)
• Expansion of program to St. Mary’s Medical Center in Apple Valley
19

Questions?
Raise your hand or submit a question at www.menti.com and enter code 80 39 38

Thank You
June Simmons, President and CEO, Partners in Care Foundation, [email protected]
Sally Ramirez, RN, MLTCA, IQCI, Regional Director, Utilization, Denial and Clinical Training, Providence St. Joseph Health, [email protected]