
Case Presentation Acute Diarrhoea. Mr AB 24 yo man lives interstate Presents with 3 days diarrhoea...
64
Case Presentation Acute Diarrhoea
-
Upload
henry-heathcote -
Category
Documents
-
view
219 -
download
1
Transcript of Case Presentation Acute Diarrhoea. Mr AB 24 yo man lives interstate Presents with 3 days diarrhoea...

Case PresentationAcute Diarrhoea

Mr AB
• 24 yo man lives interstate• Presents with 3 days diarrhoea and 4 days
abdominal pain and feeling generally unwell.• 12-15 episodes of diarrhoea a day
– normal colour– not watery but loose ++– no blood or mucous
• Generalised non-specific crampy abdo pain, right worse than left, radiating to right back.– worst pain ever experienced like ‘stomach in a
vice’
• No vomiting, no fevers/sweats/rigors.• Loss of appetite.
Past Medical History• Gastroenteritis one year ago – 24 hr bug• Gastritis – 18yo – took Somac for a while
Medications• No medications or allergies
Family History
Socially• Parents and sister (25) well
• No infectious contacts,• Just quit smoking 3 pk/wk, w/e ETOH binges• Ate a ‘dodgy’ chicken schnitzel on Friday at shopping centre

Examination
• HR 100, BP 100/70, T 364, RR18, Sats 100%RA
• Looks unwell but not distressed or haemodyn. compromised.
Soft abdo Right sided and bilateral IF tenderness No renal angle tenderness Mild RIF rebound No organomegaly BS increased

Examination II
• Stong Pulses, Dual Heart Sounds, no murmurs
• Chest Clear• MMM, normal turgor, warm to
touch, appears well perfused, thirsty
• FWT – NAD• BSL – 4.6mmol

FBE

Other Bloods

Abdo XR
Questions
• Any other questions or examination points?
• DDx?• Plan?

Progress• Analgesia
– Pain well treated though not completely relived by Panadol and Buscopan
• IV Fluids– HR 75, BP 120/80, T 373
• Admit Surg – Single Room– Observe ?appendicitis DDx gastroenteritis
• Faecal Spec for MCS collected in ED– Loose brown sample, occasional WCC, RBC+
• Overall feeling much better on PM WR.

21/7/2006 – AM WR
• Little change:– few bouts of diarrhoea overnight– crampy abdo pain persists on right side
though not guarding as was yesterday– still no temperature above 373
– feels hungry
• Dilemma:– definitive diagnosis of appendicitis can
really only be made on laparoscopy– What to do now?

Repeat Bloods

Repeat Bloods
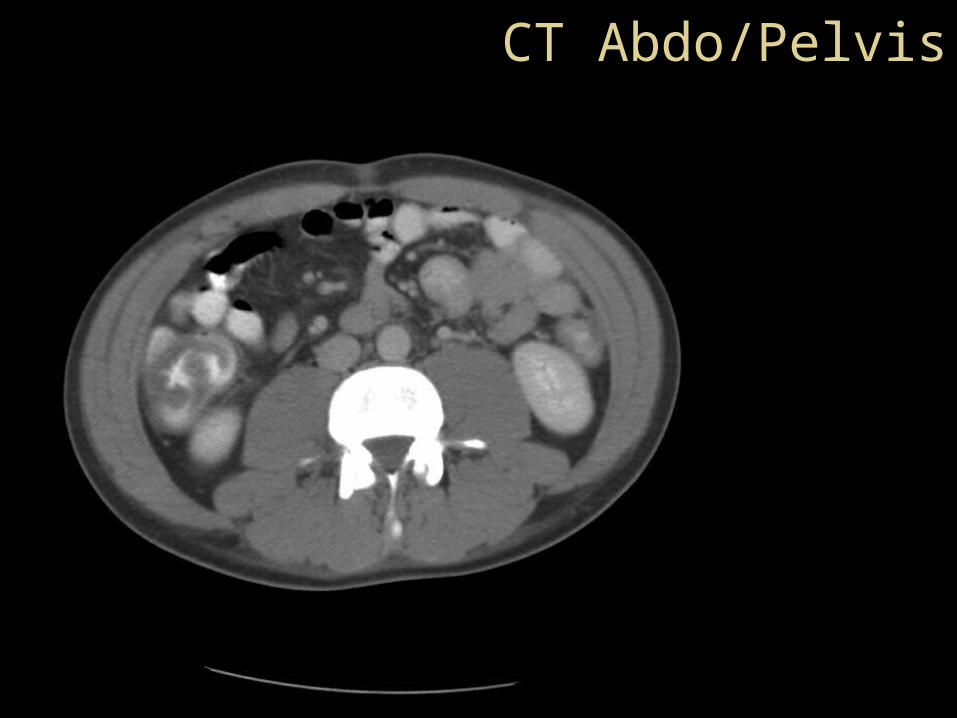
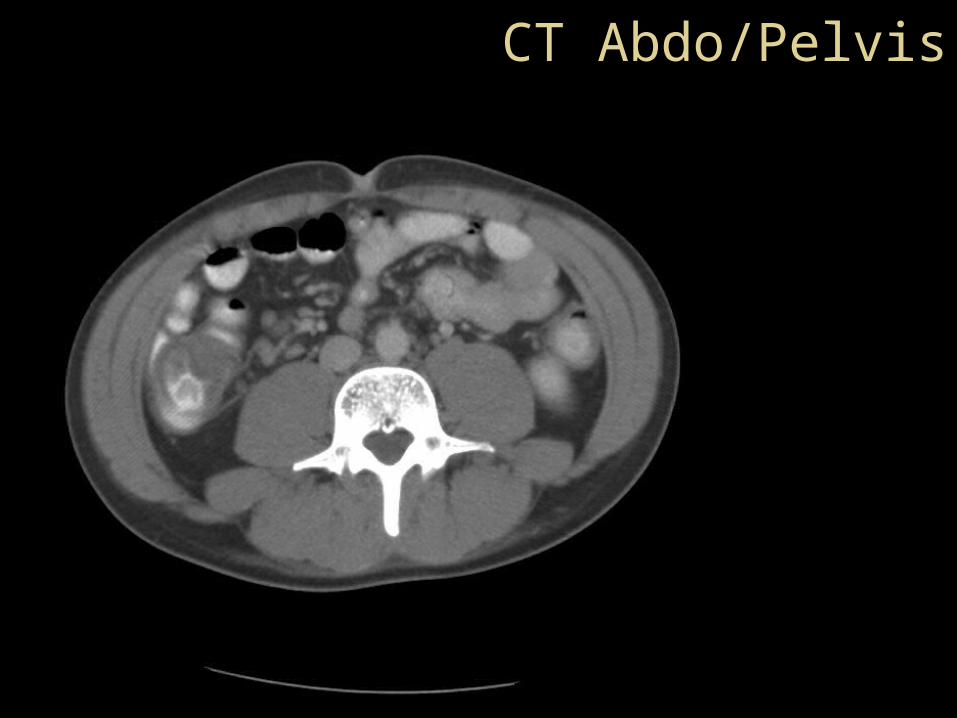
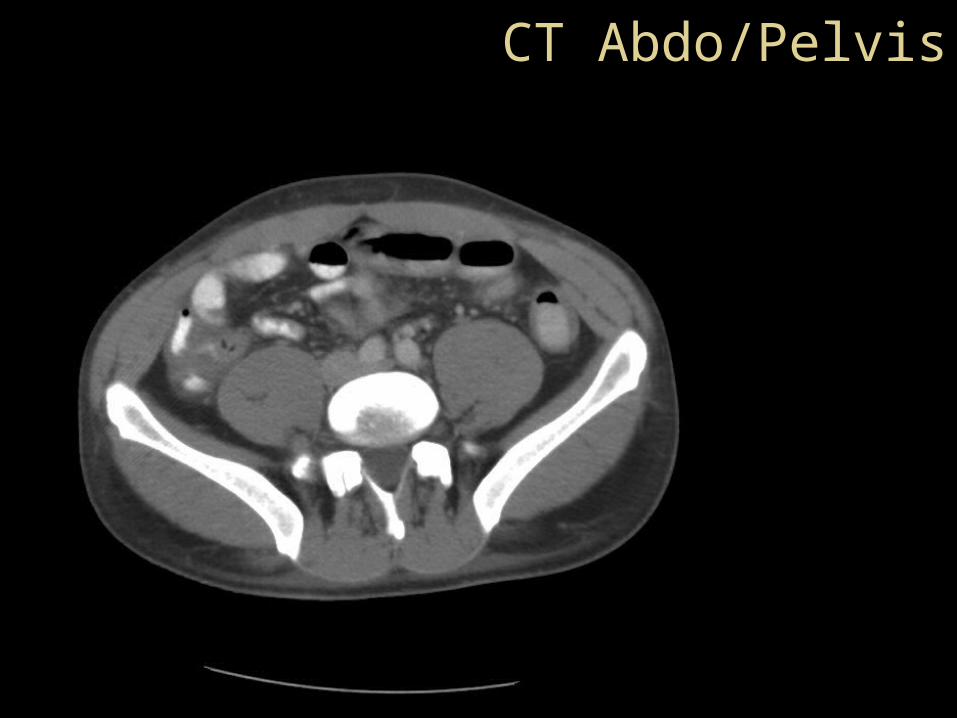
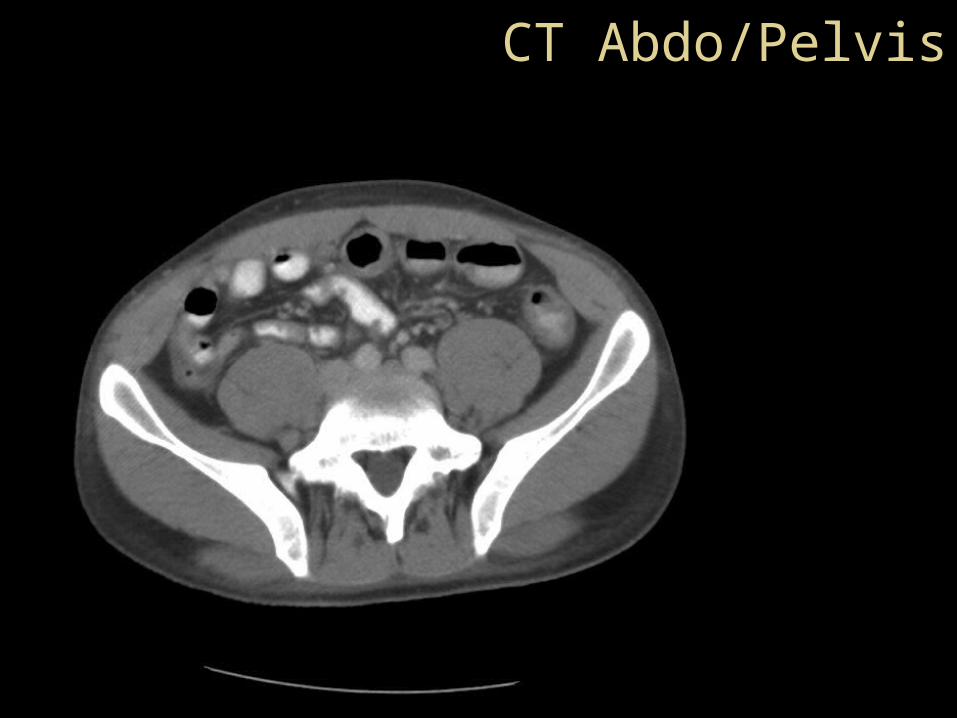
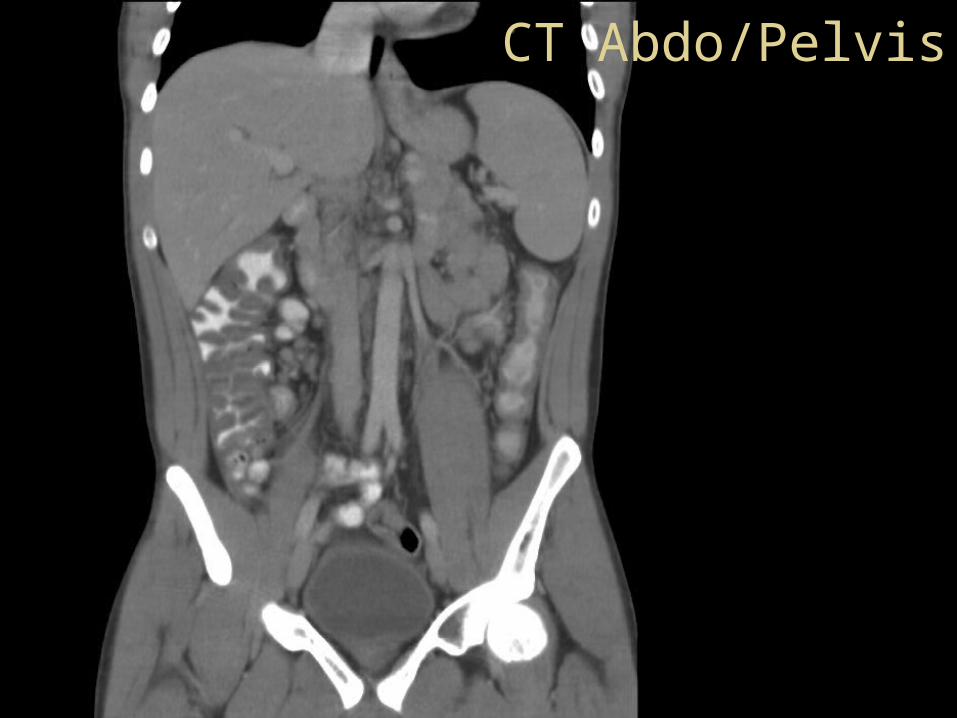
CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis
CT Abdo/Pelvis
CT Abdo/Pelvis

CT Abdo/Pelvis
CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis
CT Abdo/Pelvis

CT Abdo/Pelvis
CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis
CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis

CT Abdo/Pelvis
CT Report
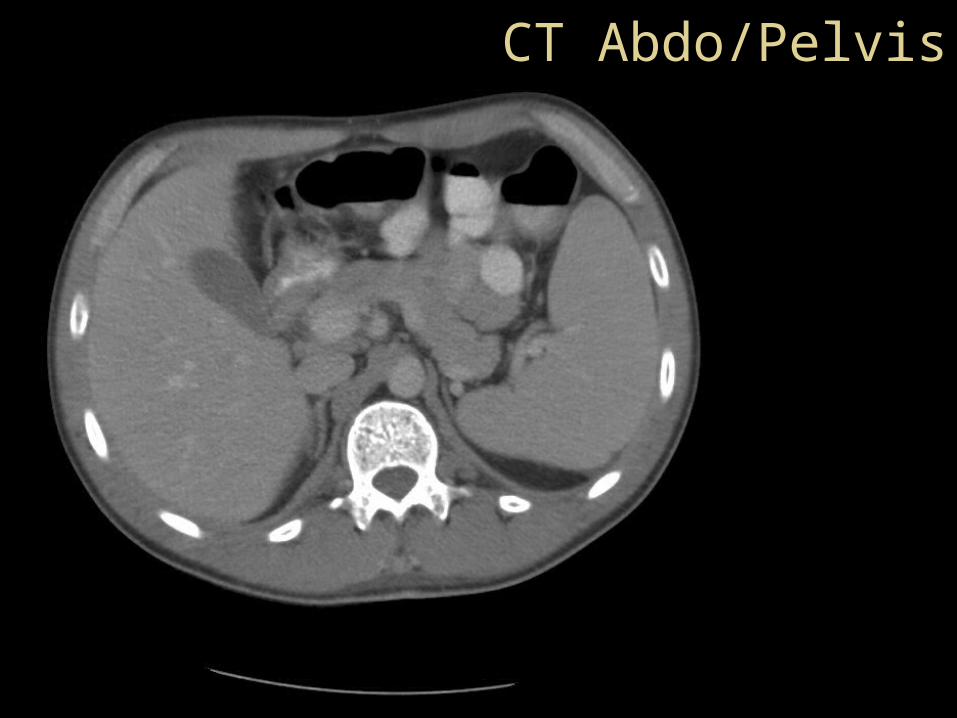
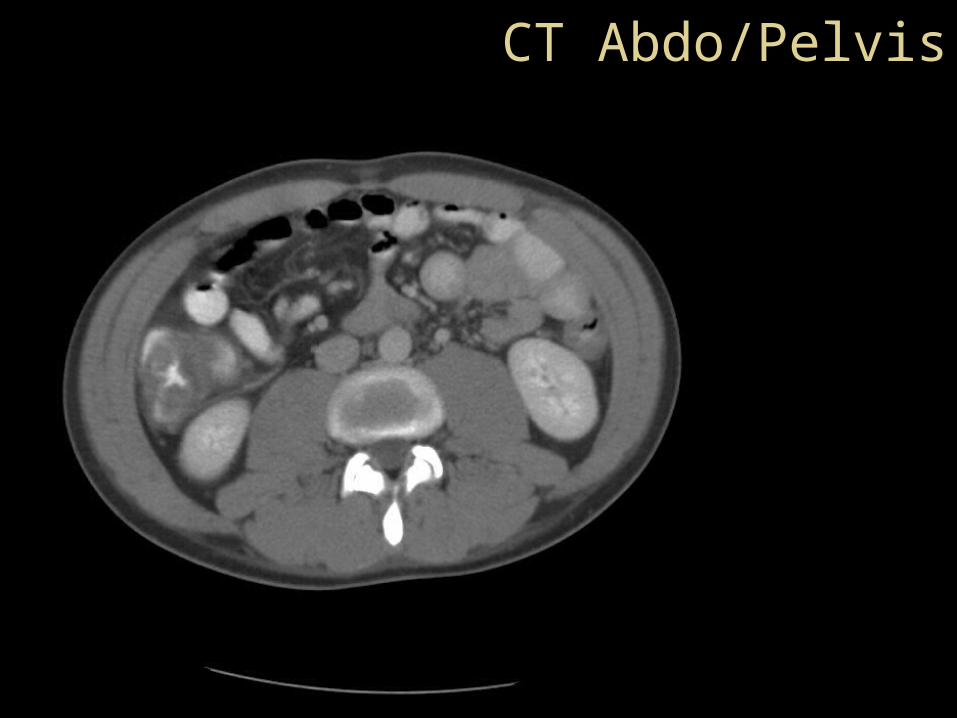
• Severe right sided colitis extending from caecum to hepatic flexure.
• No terminal ileitis.• No skip lesions.• Suggest biopsy!!!!
AXR Report• No soft tissue definition.• Some ‘loss of definition’ within the
right sacroiliac joint.• ? inflammatory arthropathy.

Further History
• Frequently gets sore knees and shoulders from time to time.– blames it on football
• Back pain occasionally– when standing for long periods– doesn’t know if always worse on right
• No chronic diarrhoea.• No history of red eye, skin complaints,
non-axial joint pain, redness or stiffness, no mouth ulcers, no other extra-intestinal manifestations of IBD.

Progress
• Diarrhoea and pain settled and patient tolerating FWD at day two admission.
• Back pain occasional and mild.• Gastro Med Review:
– no active treatment required at this stage if symptoms improving
– requires gastro and rheum f/u– otherwise can go home– will need colonoscopy in 4-6 weeks
• GP in Newcastle was contacted.• D/C three days after admission.


















