CASE 3 Reyes, Carmen; Reyes, Jenilene; Reyes, Lourdes; Rivera, Laila; Rivere, Djeaune; Robosa, Dean...
62
CASE 3 Reyes, Carmen; Reyes, Jenilene; Reyes, Lourdes; Rivera, Laila; Rivere, Djeaune; Robosa, Dean Antonio; Rodas, Francis; Rodriquez, Reine; Rogelio, Graciella; Roque, Marianne; Ruanto, Maria Theresa
-
Upload
deirdre-hill -
Category
Documents
-
view
216 -
download
1
Transcript of CASE 3 Reyes, Carmen; Reyes, Jenilene; Reyes, Lourdes; Rivera, Laila; Rivere, Djeaune; Robosa, Dean...
CASE 3
Reyes, Carmen; Reyes, Jenilene; Reyes, Lourdes; Rivera, Laila; Rivere, Djeaune; Robosa, Dean Antonio; Rodas, Francis; Rodriquez, Reine; Rogelio, Graciella; Roque, Marianne; Ruanto, Maria Theresa
OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
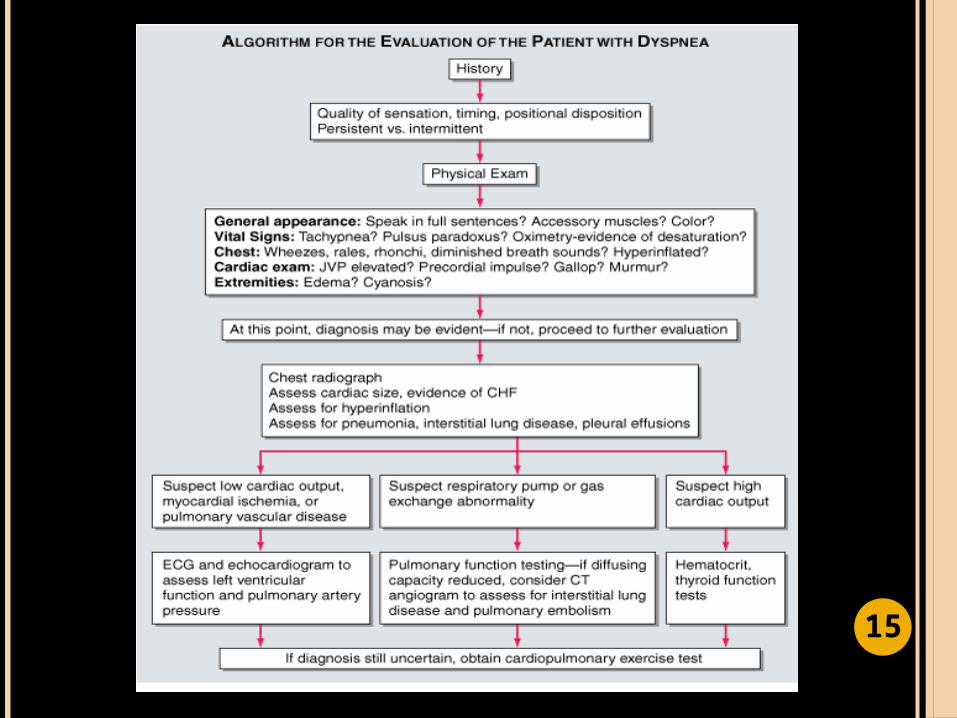
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 2
OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 3
CASE PRESENTATION
R.F. 24 y/o Female
CHIEF COMPLAINT: Shortness of breath
4
HISTORY OF PRESENT ILLNESS
1 month PTA •Patient started having episodes of shortness of breath•No consult was done nor medications taken
2 weeks PTA•Increasing shortness of breath•Difficulty climbing 2 flights of stairs•Consult: given vitamins
1 day PTA •No improvement•Progressive shortness of breath when walking a short distance
ADMISSION5
REVIEW OF SYSTEMS
Poor appetite No headache/blurring of vision No cough/colds Occasional chest pain No abdominal pain/no vomiting No joint pains
6
PAST MEDICAL HISTORY
No previous hospitalizations (+) episodes of sore throat and fever as a
child No hypertension No diabetes No surgeries
7
FAMILY HISTORY
(-) Heart disease (-) Diabetes (-) Asthma/Allergies
8
PERSONAL/SOCIAL HISTORY
Non-smoker Non-alcoholic beverage drinker
9
PHYSICAL EXAMINATION FINDINGS
Conscious, coherent, ambulatory BP: 120/80 HR: 70 bpm RR: 20’s Warm moist skin ,no dermatoses
HEART: apex beat 5th LICS, MCL(+) accentuated S1(+) diastolic murmur
LUNGS: symmetric chest expansionno retractions(+) occasional wheeze
No cyanosis/edema
10

MISSING DATA General Data
Address, occupation, civil status, religion HPI
Type of vitamins taken when consult was done Other possible associated signs and symptoms
PE findings Specific RR Temp BMI JVP
Personal and Social History Type of diet, exercise Occupation (type, workload)
Environmental History Area of residence and associated living conditions
11

SALIENT FEATURES
24 F BP: 120/80 HR: 70 bpm RR: 20s
Progressive shortness of breath
Symmetrical chest expansion
(-) Retractions (+) Wheeze
Apex beat: 5th LICS, MCL
(+) Accentuated S1 (+) Diastolic
murmur
12

OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 1
3
APPROACH TO A PATIENT WITH DYSPNEA
Dyspnea
Pulmonary
14
15
Dyspnea
Pulmonary
APPROACH TO A PATIENT WITH DYSPNEA
16
DYSPNEA
a subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity
derives from interactions among multiple physiological, psychological, social, and environmental factors, and may induce secondary physiological and behavioural responses
17
18
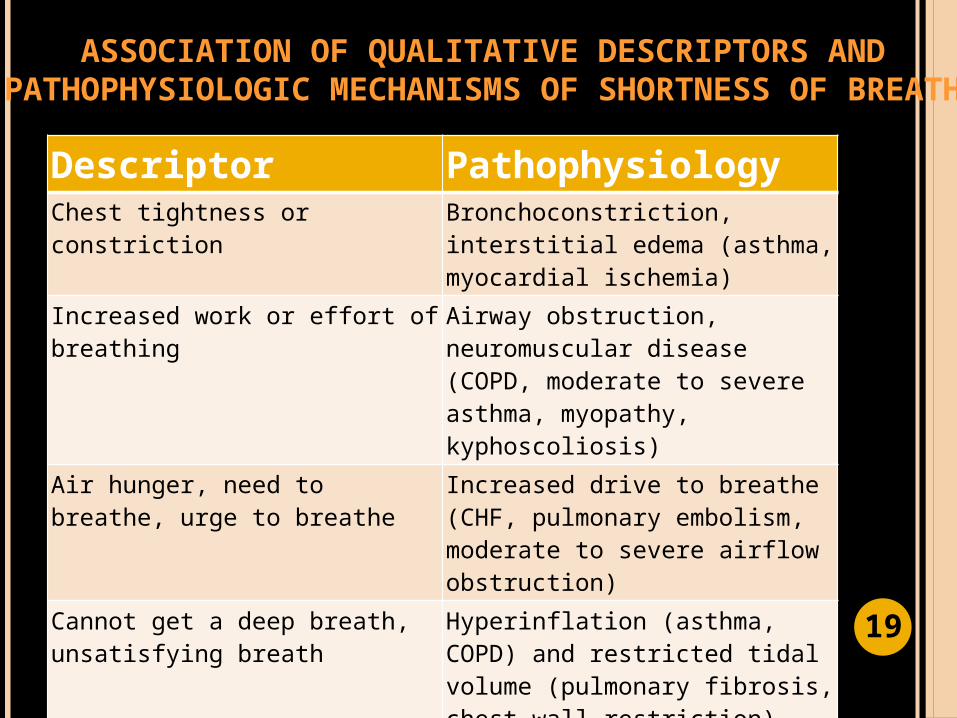
ASSOCIATION OF QUALITATIVE DESCRIPTORS AND PATHOPHYSIOLOGIC MECHANISMS OF SHORTNESS OF
BREATH
Descriptor PathophysiologyChest tightness or constriction Bronchoconstriction, interstitial
edema (asthma, myocardial ischemia)
Increased work or effort of breathing
Airway obstruction, neuromuscular disease (COPD, moderate to severe asthma, myopathy, kyphoscoliosis)
Air hunger, need to breathe, urge to breathe
Increased drive to breathe (CHF, pulmonary embolism, moderate to severe airflow obstruction)
Cannot get a deep breath, unsatisfying breath
Hyperinflation (asthma, COPD) and restricted tidal volume (pulmonary fibrosis, chest wall restriction)
Heavy breathing, rapid breathing, breathing more
Deconditioning 19
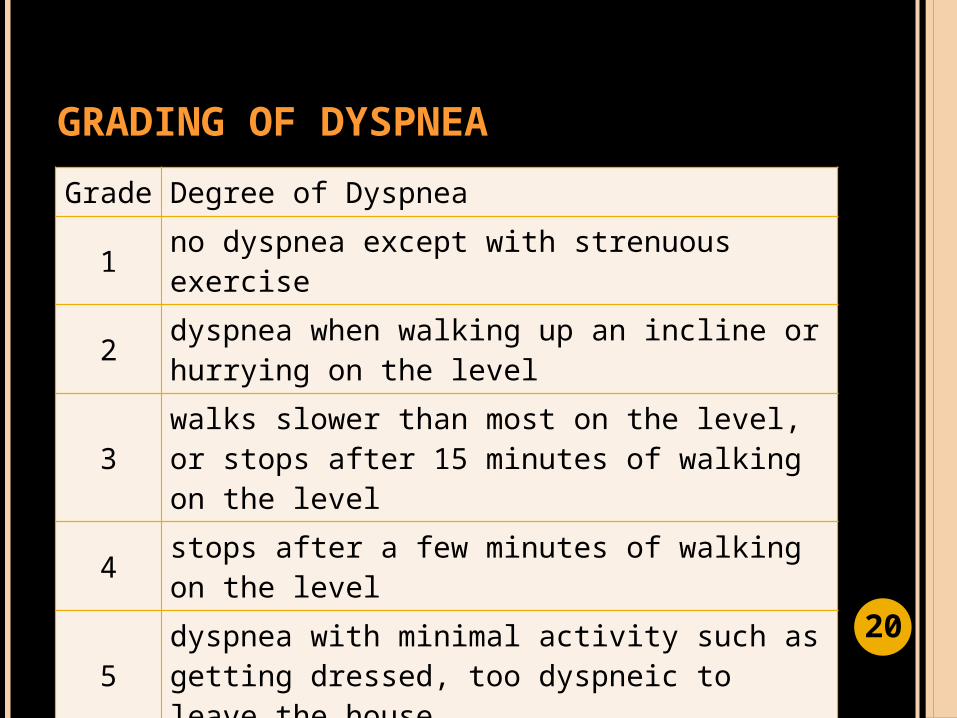
GRADING OF DYSPNEA
Grade Degree of Dyspnea
1 no dyspnea except with strenuous exercise
2 dyspnea when walking up an incline or hurrying on the level
3walks slower than most on the level, or stops after 15 minutes of walking on the level
4 stops after a few minutes of walking on the level
5dyspnea with minimal activity such as getting dressed, too dyspneic to leave the house
20
CHEST PAIN
discomfort or pain anywhere along the front of your body between your neck and upper abdomen
Can be due to cardiopulmonary problems, chest wall problems, GI, psychological
21

Typical Features of Chest Discomfort
Condition Duration Quality Location Associated Features
Angina More than 2 and less than 10 min
Pressure, tightness, squeezing, heaviness, burning
Retrosternal, often with radiation to or isolated discomfort in neck, jaw, shoulders, or arms—frequently on left
Precipitated by exertion, exposure to cold, psychologic stress
S4 gallop or mitral
regurgitation murmur during pain
Aortic stenosis
Recurrent episodes as described for angina
As described for angina
As described for angina
Late-peaking systolic murmur radiating to carotid arteries
Pulmonary hypertension
Variable Pressure Substernal Dyspnea, signs of increased venous pressure including edema and jugular venous distention
Esophageal reflux
10–60 min Burning Substernal, epigastric
Worsened by postprandial recumbency
Relieved by antacids
Peptic ulcer Prolonged Burning Epigastric, substernal
Relieved with food or antacids
Emotional and psychiatric conditions
Variable; may be fleeting
Variable Variable; may be retrosternal
Situational factors may precipitate symptoms
Anxiety or depression often detectable with careful history
22
APEX BEAT DISPLACEMENT
Patient AB: 5th LICS, MCL Lateral and/or inferior displacement of the
apex beat usually indicates cardiomegaly. May also be displaced by other conditions:
Pleural or pulmonary diseases Deformities of the chest wall or the thoracic
vertebra
23
(+) ACCENTUATED S1
Mitral valve snaps shut more vigorously, producing a louder S1 Blood velocity is increased-> anemia, fever,
hyperthyroidism, anxiety, and during exercise Mitral valve is stenotic
24
(+) DIASTOLIC MURMUR
Early diastolic Begins with S2
Mid diastolic Begins at clear interval after S2
Late diastolic (presystolic)
Begins immediately before S1
25
(+) DIASTOLIC MURMUR
Heard with bell at apex, patient in left lateral decubitus position
Findings on examination Low-frequency diastolic rumble, more intense in
early and late diastole, does not radiate; systole usually quiet; palpable thrill at apex in late diastole common; S1 increased and palpable at left sternal border
Description Narrowed valve restricts forward flow; forceful
ejection into the ventricle Often occurs with mitral regurgitation caused by
rheumatic heart fever or cardiac infection 26
LUNG FINDINGS
Occasional wheeze Musical respiratory sounds thaat may be
audible both to the patient and to others Suggests partial airway obstruction from
secretions, tissue inflammation, or a foreign body.
27
OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 2
8
OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 2
9
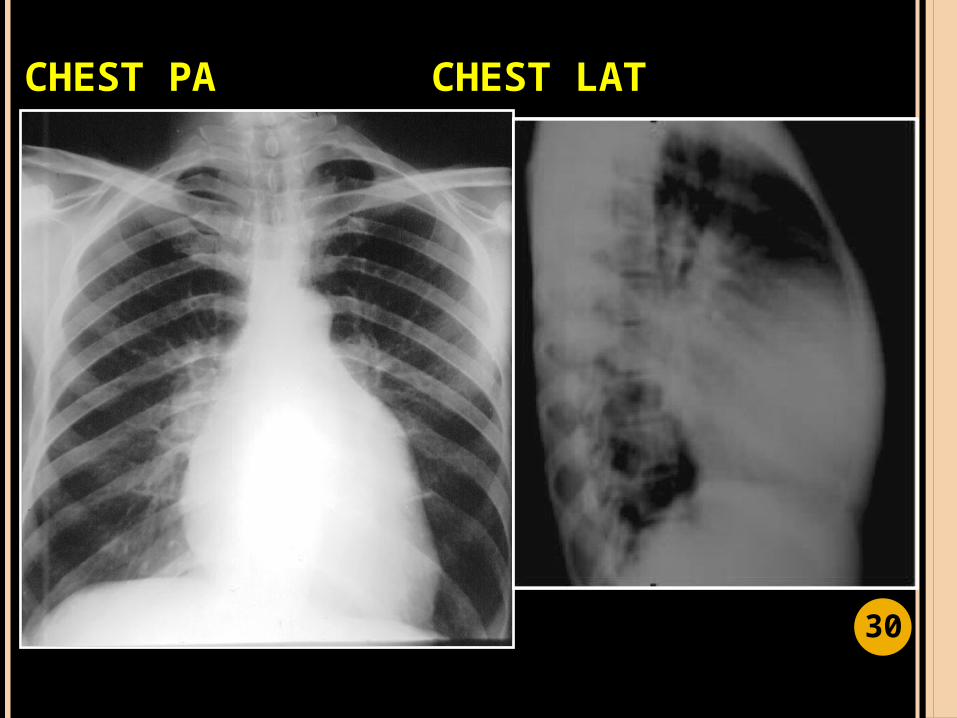
CHEST PA CHEST LAT
30
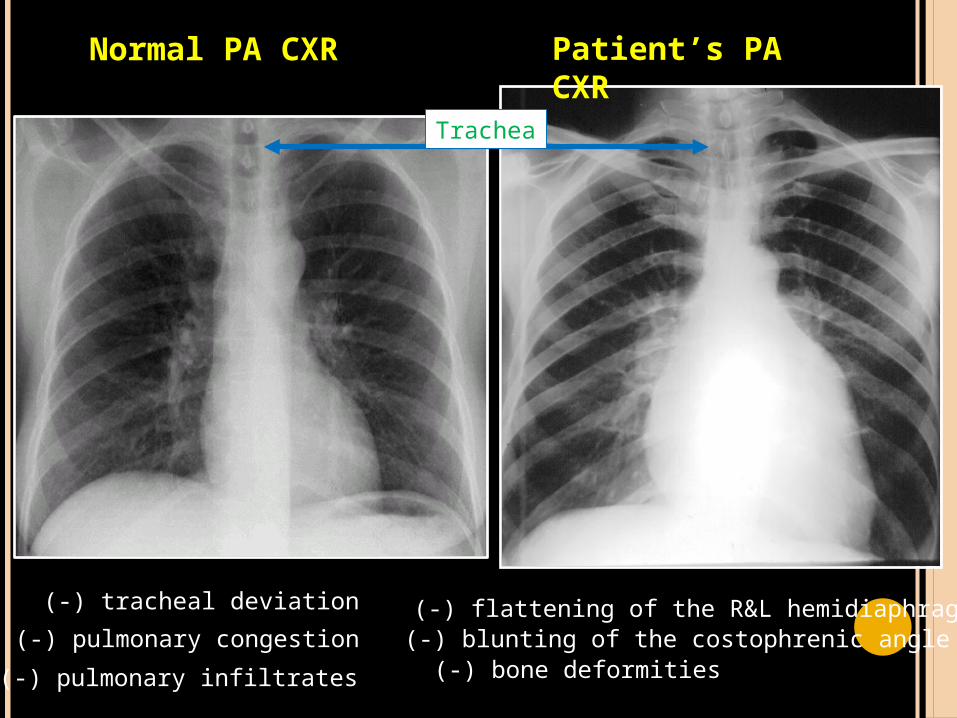
Trachea
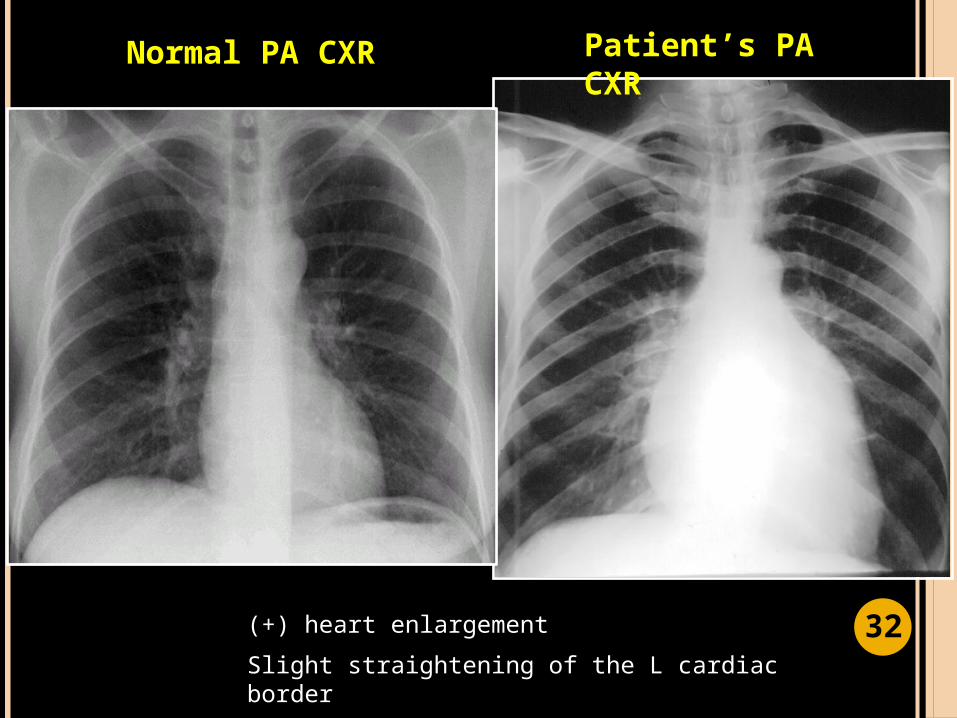
Patient’s PA CXR
Normal PA CXR
(-) blunting of the costophrenic angle(-) pulmonary congestion
(-) pulmonary infiltrates (-) bone deformities
(-) flattening of the R&L hemidiaphragm(-) tracheal deviation
Patient’s PA CXR
Normal PA CXR
(+) heart enlargement
Slight straightening of the L cardiac border
32
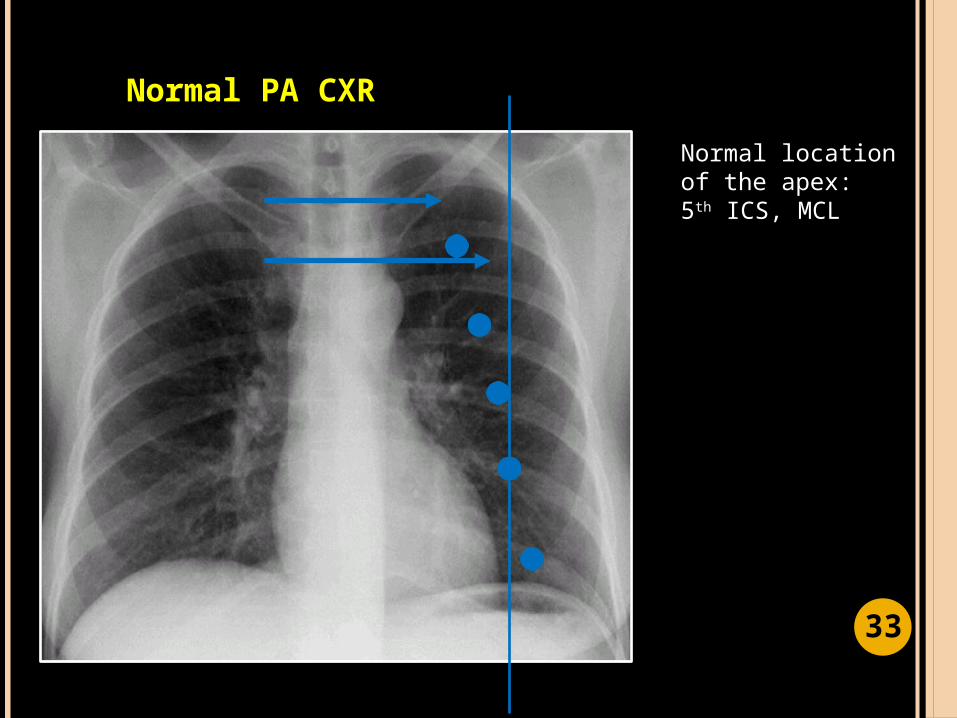
Normal location of the apex: 5th ICS, MCL
Normal PA CXR
33
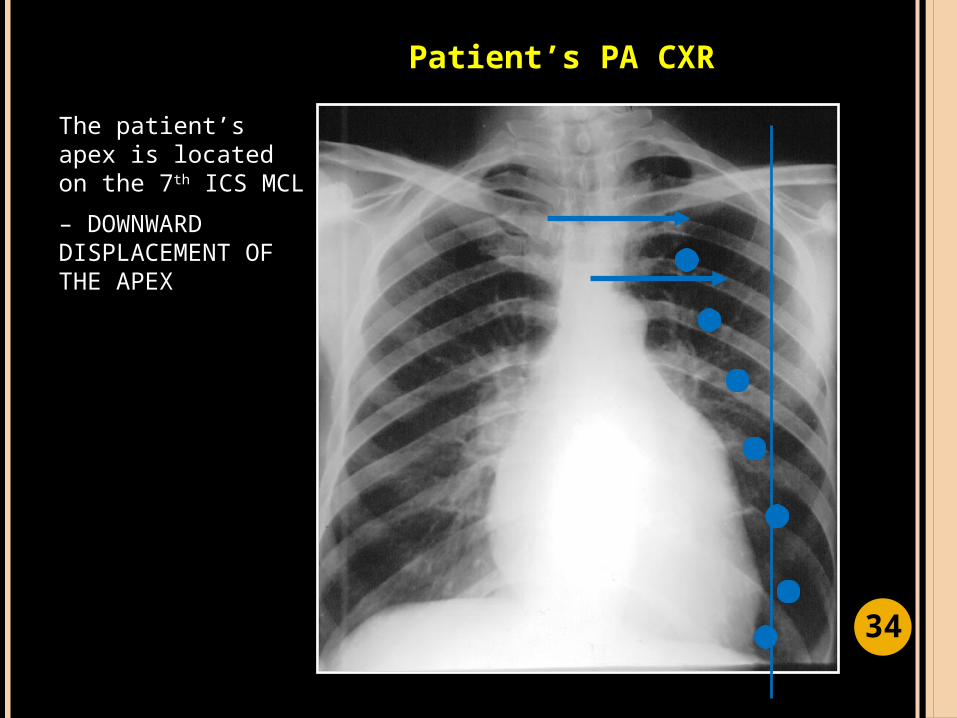
The patient’s apex is located on the 7th ICS MCL
– DOWNWARD DISPLACEMENT OF THE APEX
Patient’s PA CXR
34
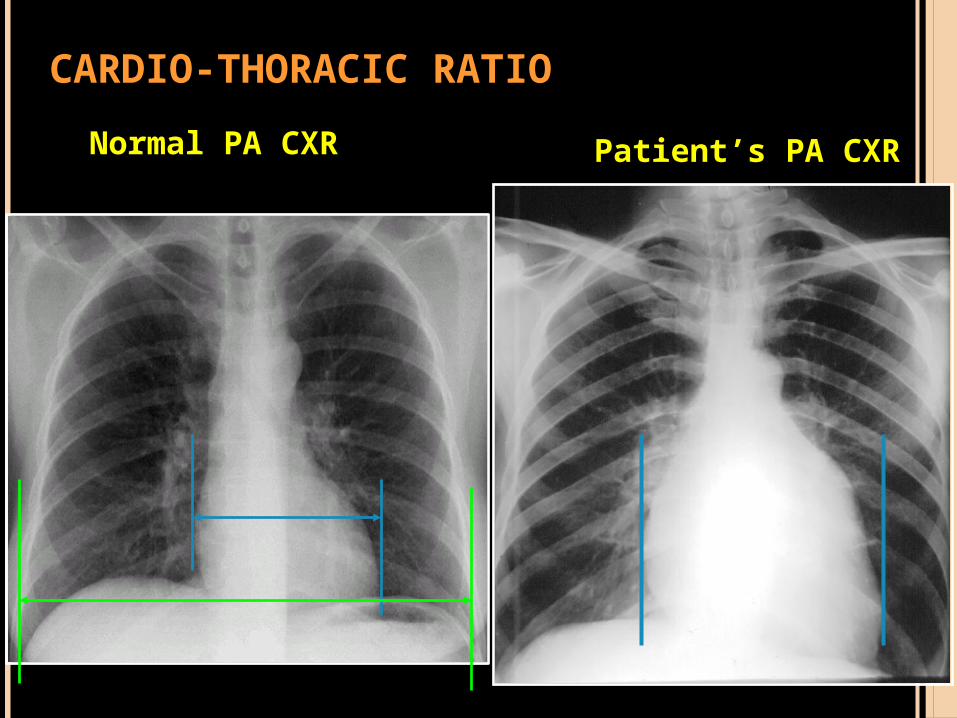
Patient’s PA CXRNormal PA CXR
CARDIO-THORACIC RATIO
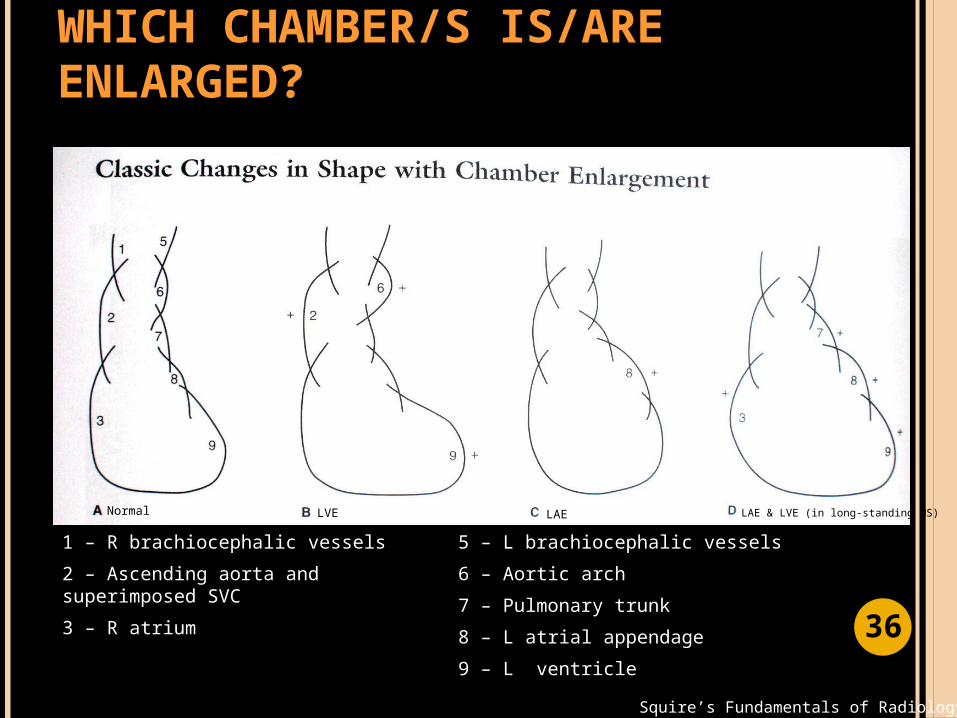
WHICH CHAMBER/S IS/ARE ENLARGED?
Squire’s Fundamentals of Radiology, 6th ed.
1 – R brachiocephalic vessels
2 – Ascending aorta and superimposed SVC
3 – R atrium
5 – L brachiocephalic vessels
6 – Aortic arch
7 – Pulmonary trunk
8 – L atrial appendage
9 – L ventricle
Normal LVE LAE LAE & LVE (in long-standing MS)
36
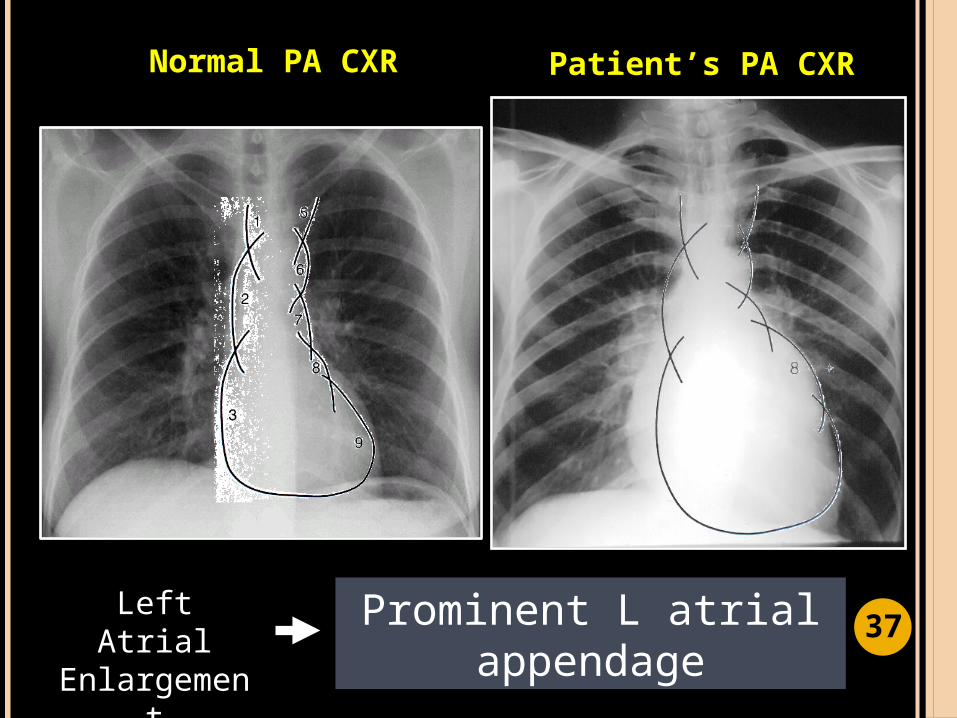
Patient’s PA CXRNormal PA CXR
Prominent L atrial appendage
Left Atrial Enlargement 3
7
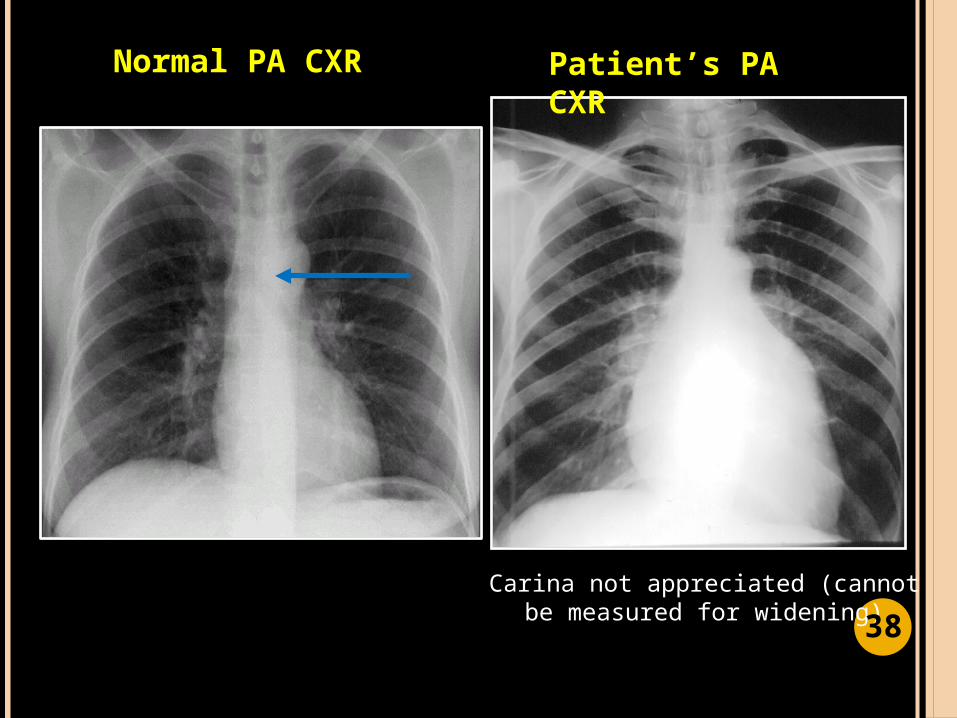
Patient’s PA CXR
Normal PA CXR
Carina not appreciated (cannot be measured for widening) 3
8
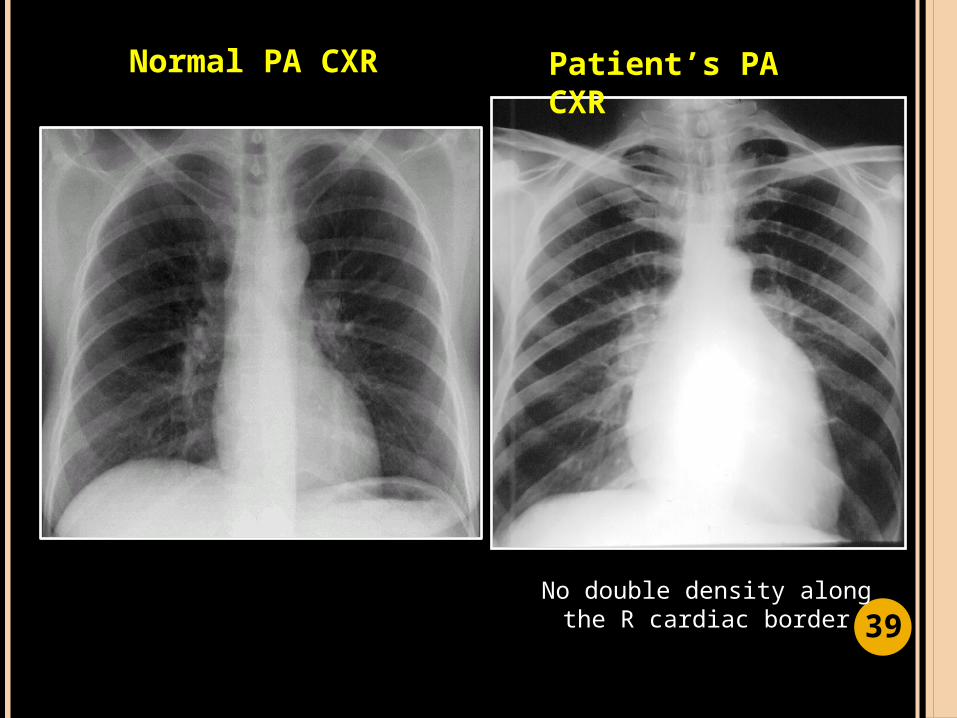
Patient’s PA CXR
Normal PA CXR
No double density along the R cardiac border 3
9
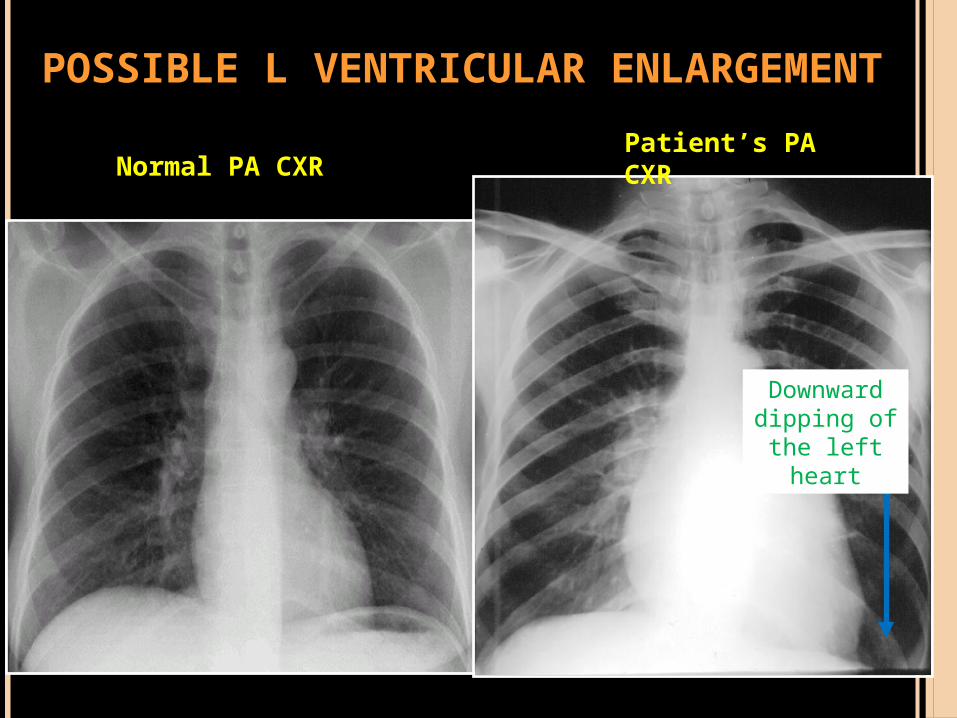
Normal PA CXR
Downward dipping of
the left heart
Patient’s PA CXR
POSSIBLE L VENTRICULAR ENLARGEMENT
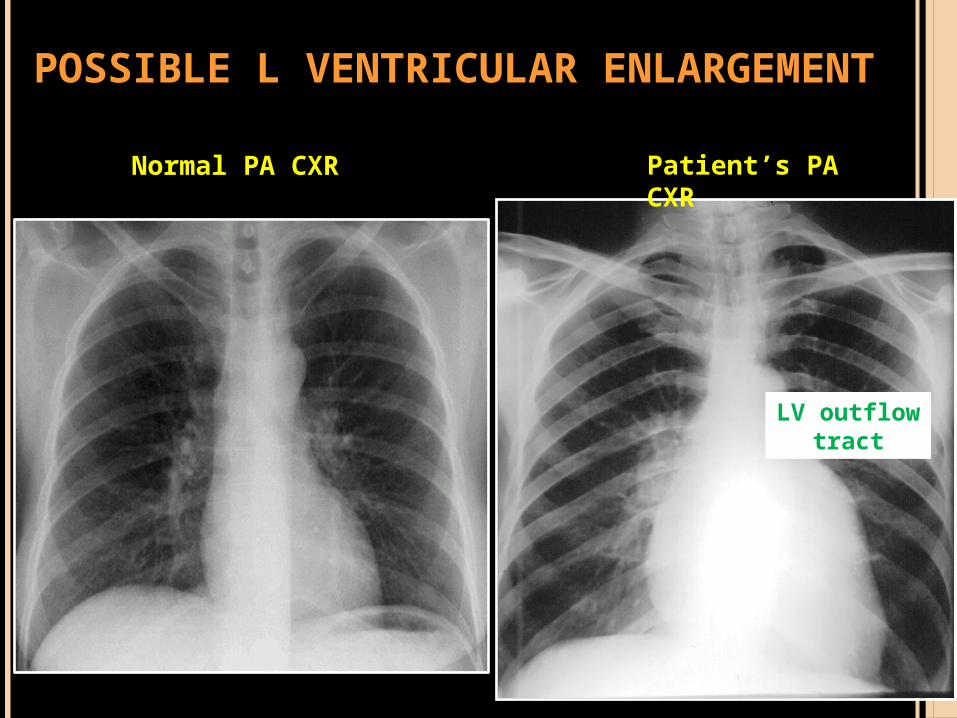
Normal PA CXR
LV outflow tract
Patient’s PA CXR
POSSIBLE L VENTRICULAR ENLARGEMENT
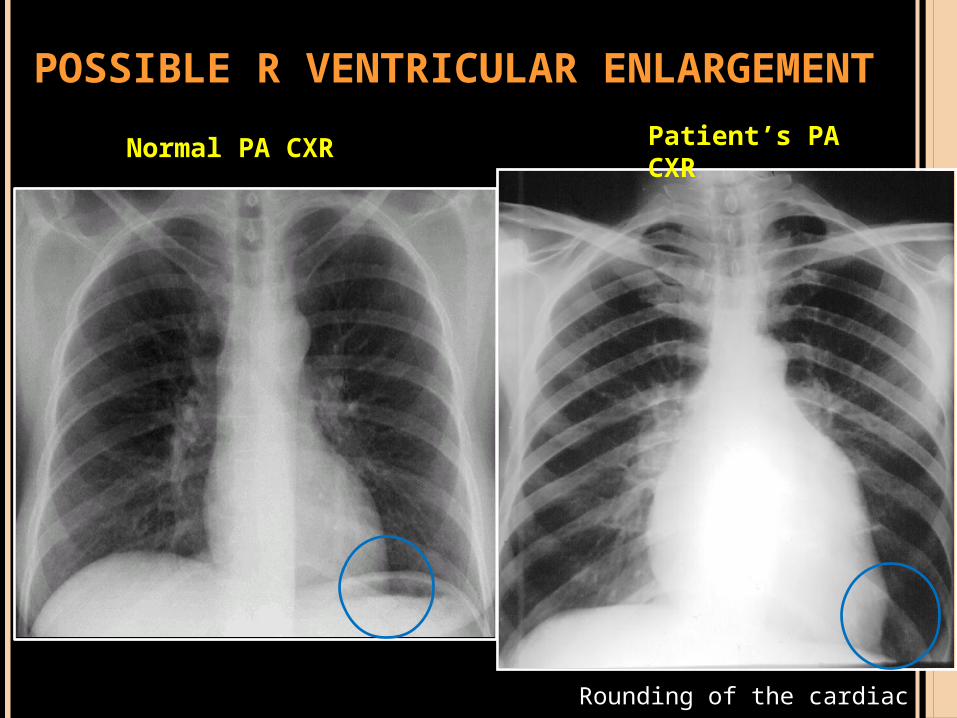
POSSIBLE R VENTRICULAR ENLARGEMENT
Normal PA CXR
Rounding of the cardiac apex
Patient’s PA CXR
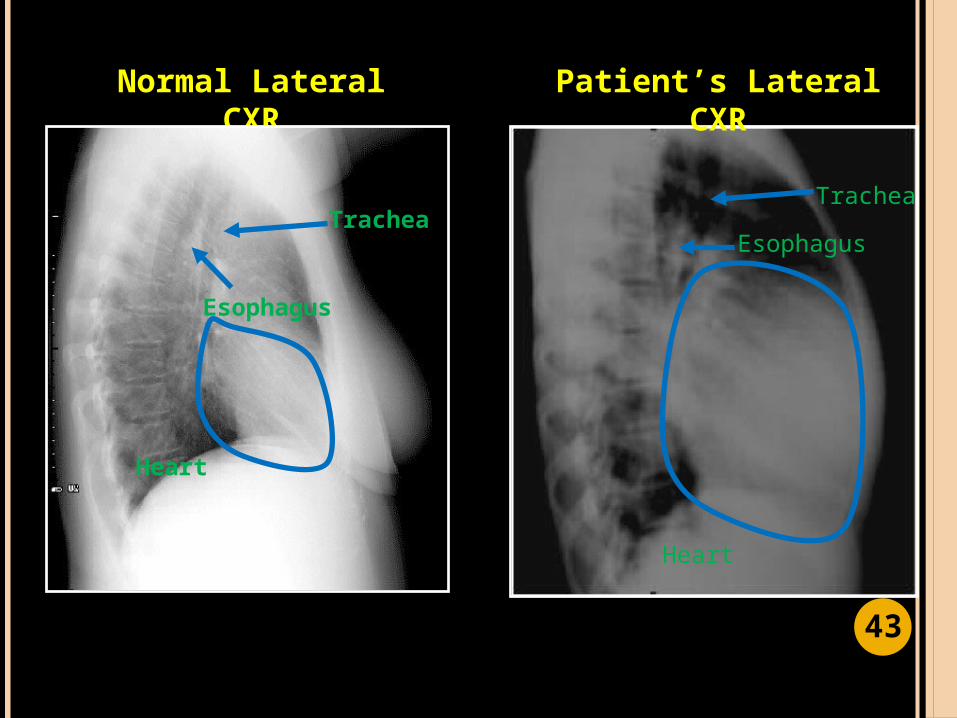
Normal Lateral CXR
Patient’s Lateral CXR
Trachea
EsophagusTrachea
Esophagus
Heart
Heart
43
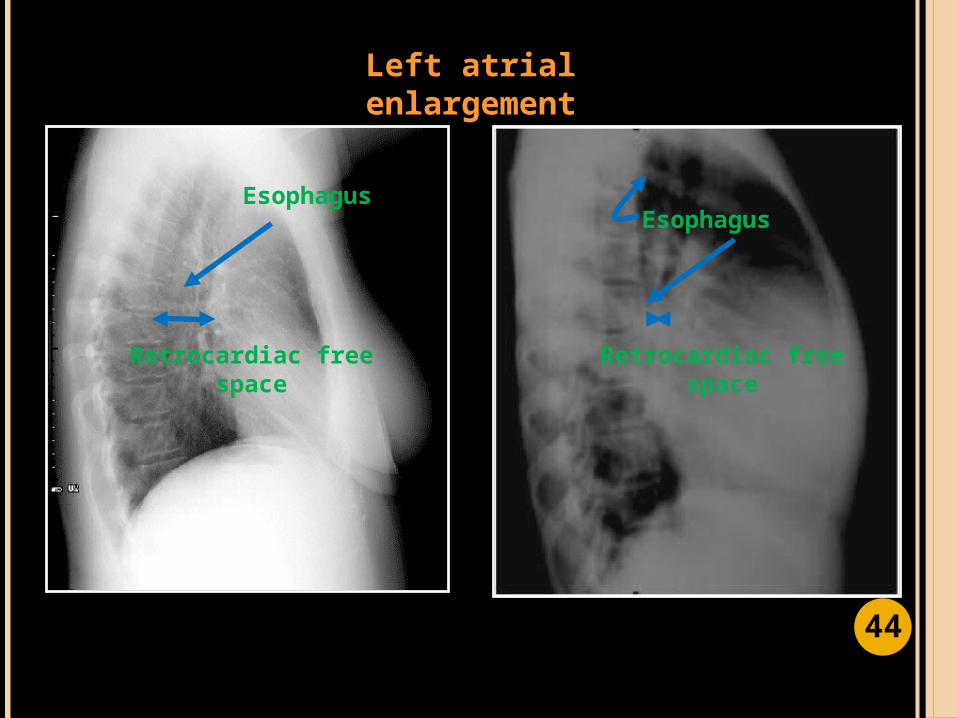
Left atrial enlargement
Esophagus
Retrocardiac free space
Esophagus
Retrocardiac free space
44

LV outflow tract
Left cardiac border
Left cardiac border
LV outflow tract
Left venticular enlargement
45
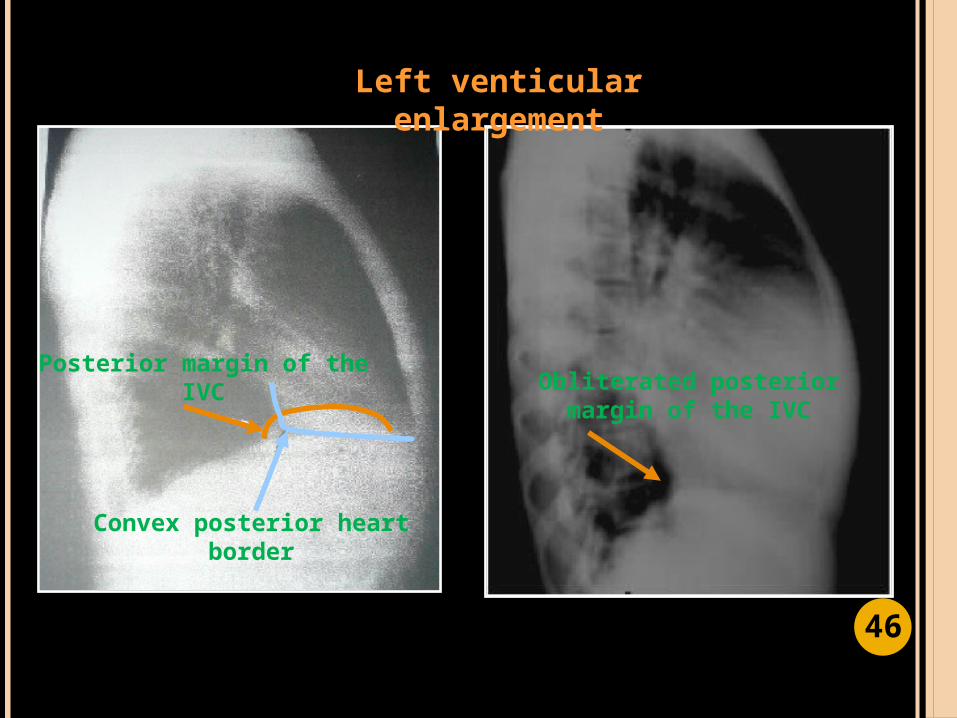
Convex posterior heart border
Posterior margin of the IVC Obliterated posterior
margin of the IVC
Left venticular enlargement
46

Left venticular enlargement
Hoffman Rigler sign
47
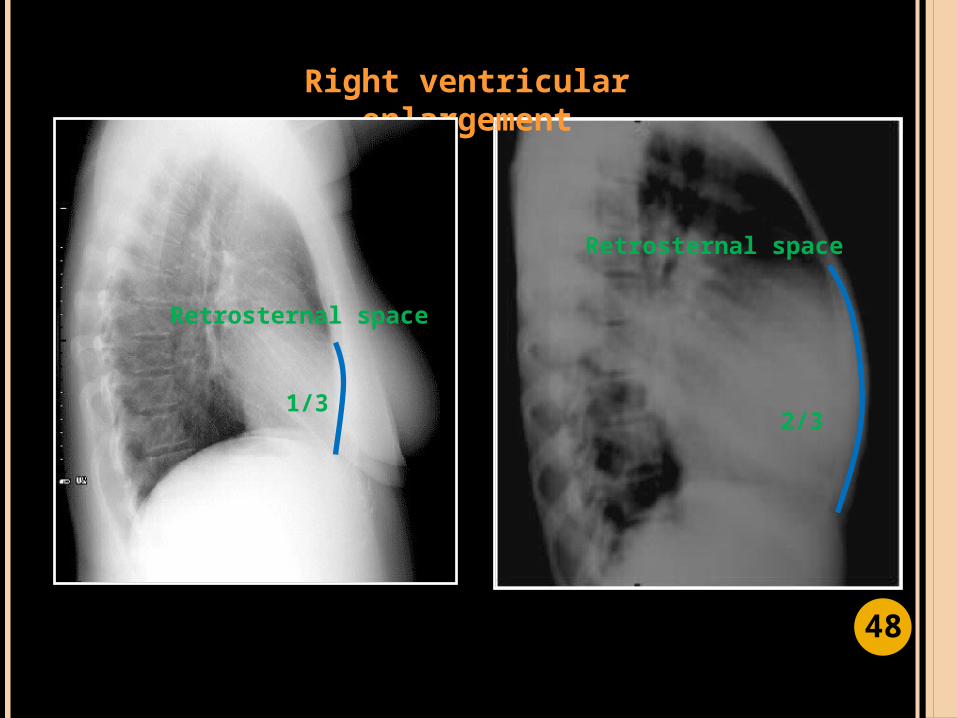
Right ventricular enlargement
Retrosternal space
2/31/3
Retrosternal space
48
OUTLINE OF PRESENTAION
To present a case of a 24F presenting with shortness of breath
To present an approach and an algorithm in the diagnosis of a patient with shortness of breath
To present the differential diagnosis and clinical impression of the patient
To discuss the chest x-ray findings and correlate it with the PE examination findings
To discuss the roles of other imaging modalities 4
9
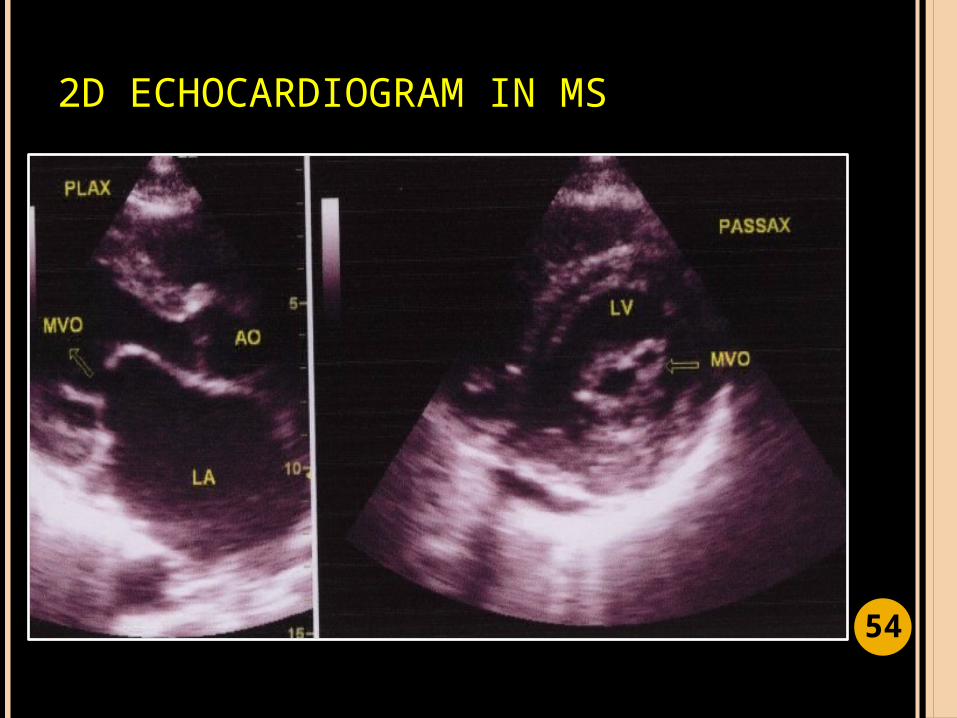
ECHOCARDIOGRAM
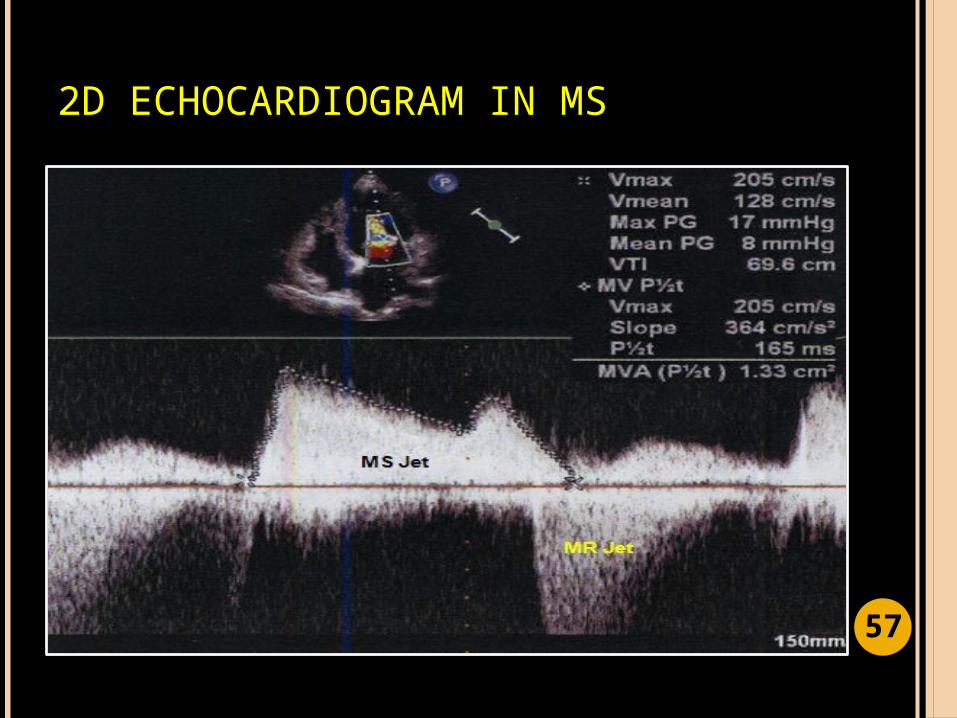
Most specific and sensitive method of diagnosing and quantifying the severity of mitral stenosis
Graphic outline of the heart's movement .
Two- dimensional (2-D) Echo is capable of displaying a cross-sectional "slice" of the beating heart, including the chambers, valves and the major blood vessels that exit from the left and right ventricle
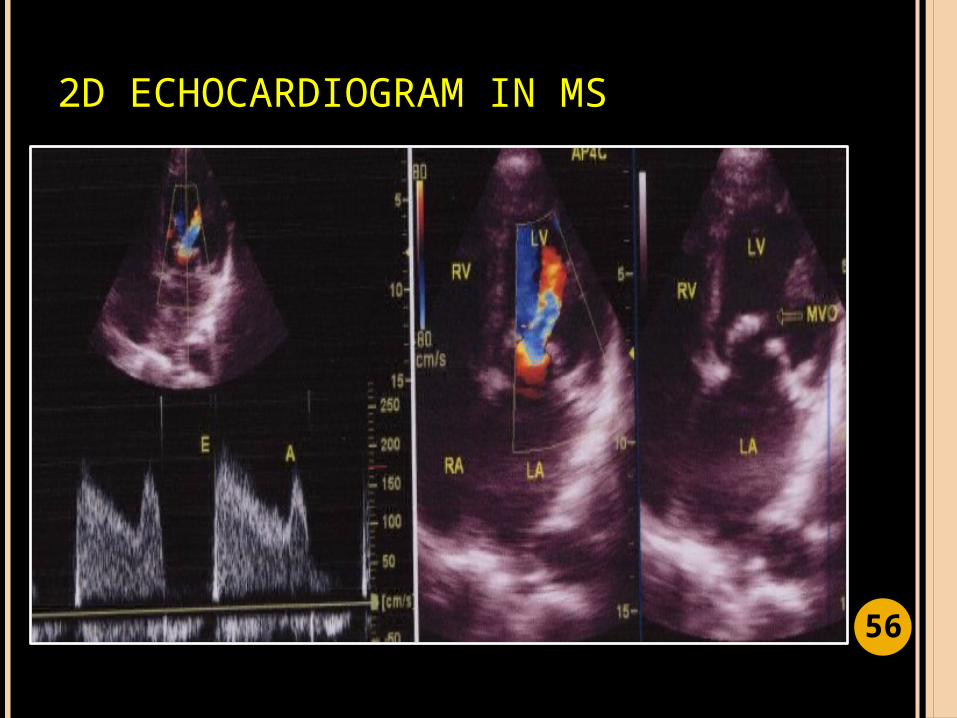
Echo is often combined with Doppler ultrasound and color Doppler to evaluate blood flow across the heart’s valves. 5
0
2D ECG: SIGNIFICANCE
Assess the heart’s function
Determine the presence of disease of the heart muscle, valves and pericardium, heart tumors, and congenital heart disease
Evaluate the effectiveness of medical or surgical treatments
Follow the progress of valve disease
51
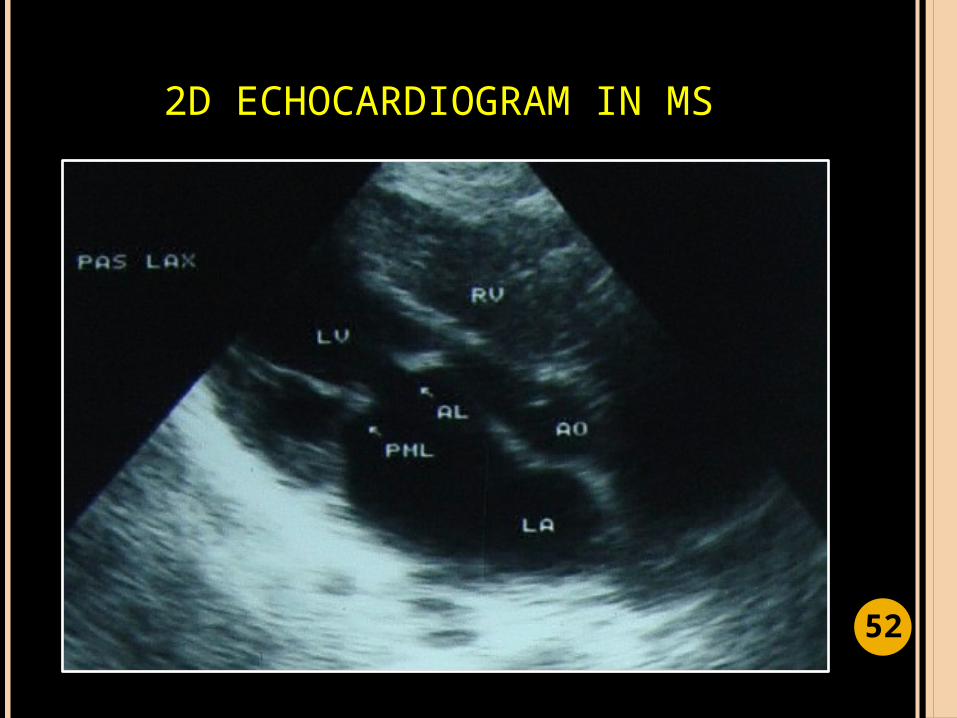
2D ECHOCARDIOGRAM IN MS
52
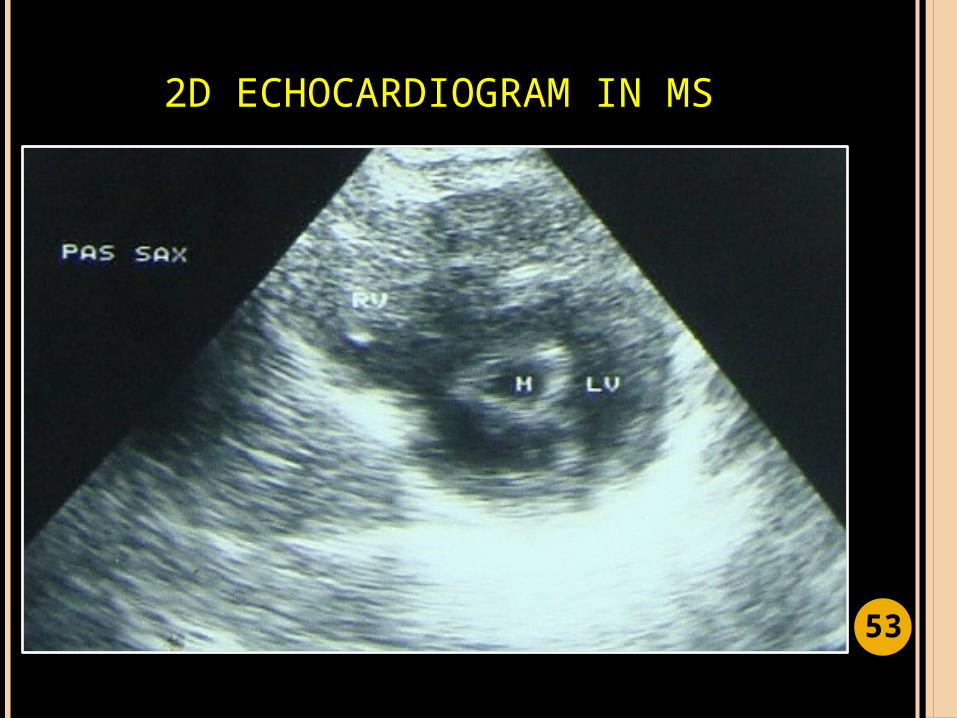
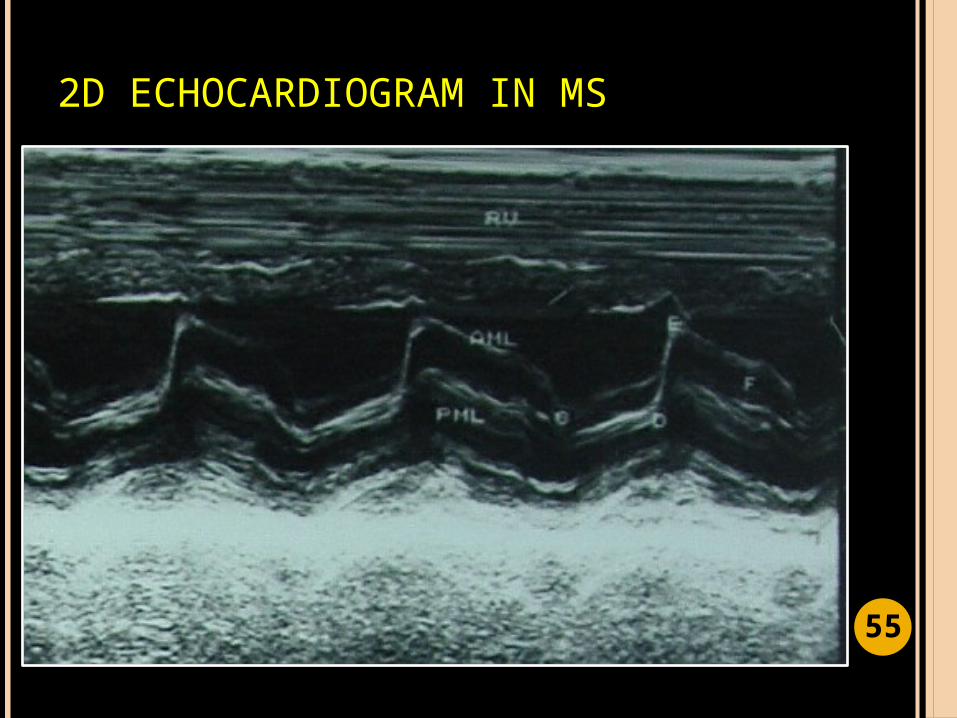
2D ECHOCARDIOGRAM IN MS
53
2D ECHOCARDIOGRAM IN MS
54
2D ECHOCARDIOGRAM IN MS
55
2D ECHOCARDIOGRAM IN MS
56
2D ECHOCARDIOGRAM IN MS
57
SUMMARY
Presented a case of a 24F presenting with shortness of breath
Discussed the approach and the algorithm in the diagnosis of a patient with shortness of breath
Explained the differential diagnosis and clinical impression of the patient
Discussed the chest x-ray findings and correlate it with the PE examination findings
Explained the roles of other imaging modalities 5
8
THANK YOU

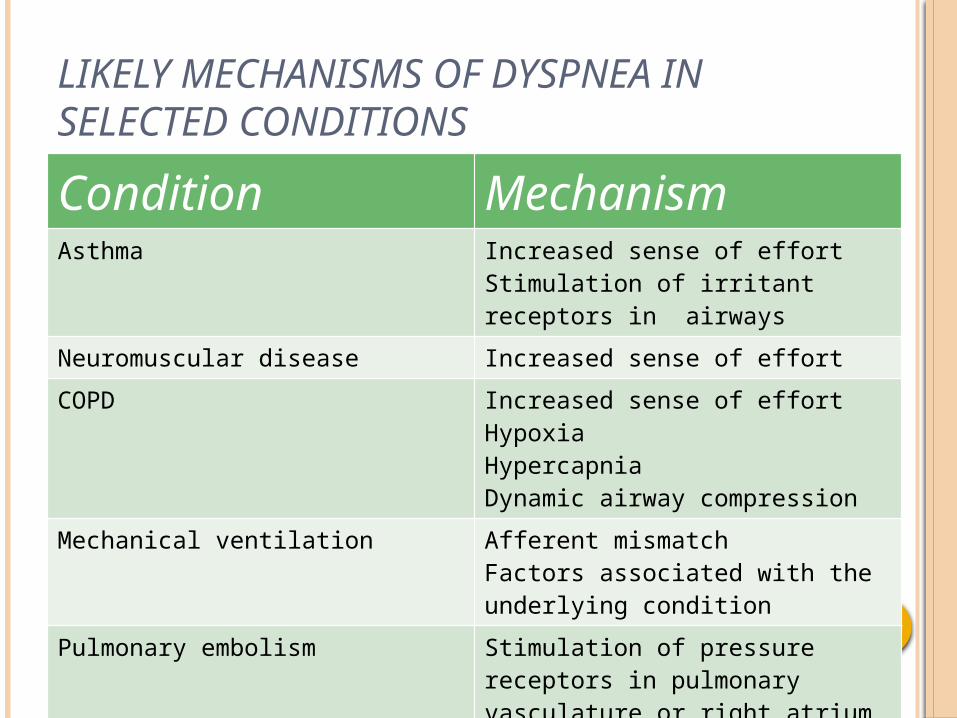
LIKELY MECHANISMS OF DYSPNEA IN SELECTED CONDITIONS
Condition MechanismAsthma Increased sense of effort
Stimulation of irritant receptors in airways
Neuromuscular disease Increased sense of effort
COPD Increased sense of effortHypoxiaHypercapniaDynamic airway compression
Mechanical ventilation Afferent mismatchFactors associated with the underlying condition
Pulmonary embolism Stimulation of pressure receptors in pulmonary vasculature or right atrium(possible)
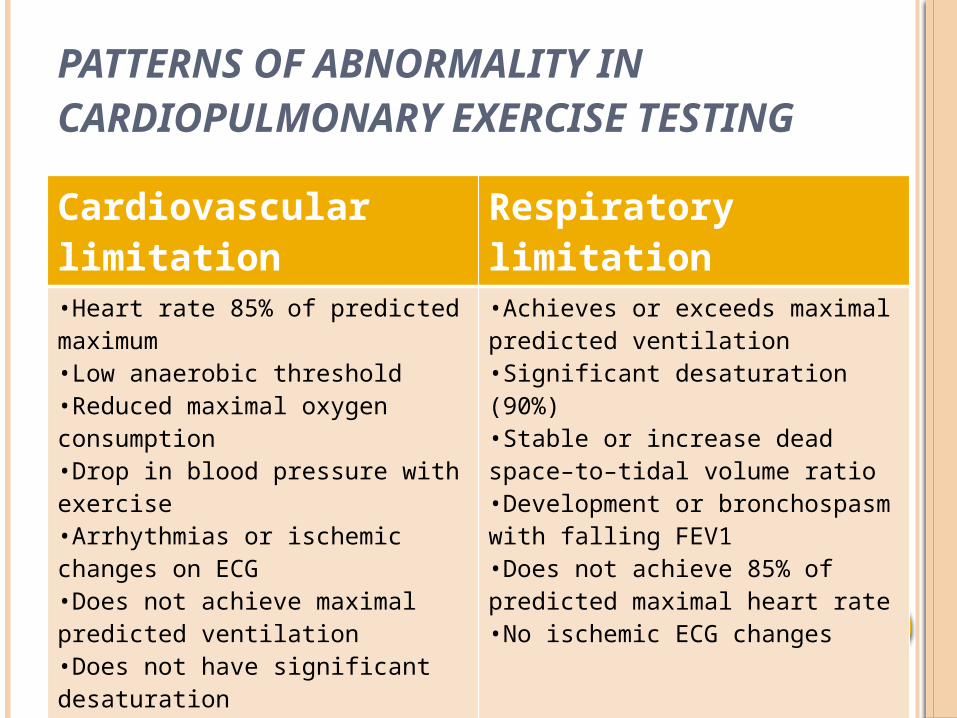
PATTERNS OF ABNORMALITY IN CARDIOPULMONARY EXERCISE TESTING
Cardiovascular limitation
Respiratory limitation
•Heart rate 85% of predicted maximum•Low anaerobic threshold•Reduced maximal oxygen consumption•Drop in blood pressure with exercise•Arrhythmias or ischemic changes on ECG•Does not achieve maximal predicted ventilation•Does not have significant desaturation
•Achieves or exceeds maximal predicted ventilation•Significant desaturation (90%)•Stable or increase dead space–to–tidal volume ratio•Development or bronchospasm with falling FEV1•Does not achieve 85% of predicted maximal heart rate•No ischemic ECG changes