
Case #1 - Continuing Medical Education - UCSF Medical ... · Case #1 72 y/o woman with hearing loss...
26
1 Current Issues in Otolaryngology Steven D. Pletcher MD Assistant Professor Department of Otolaryngology – Head and Neck Surgery University of California, San Francisco Otorhinolaryngology – Head and Neck Surgery Formerly known as ENT Early Nights and Tennis Easy, Not Tough Ear, Nose, and Throat Ear Hearing Loss Case #1 72 y/o woman with hearing loss and tinnitus Otologic History No vertigo, otalgia, or otorrhea No history of prior surgery or frequent infections + history of hearing loss in family (father and grandfather) Went to “Rock concerts” in the sixties
Transcript of Case #1 - Continuing Medical Education - UCSF Medical ... · Case #1 72 y/o woman with hearing loss...

1
Current Issues in Otolaryngology
Steven D. Pletcher MDAssistant Professor
Department of Otolaryngology –Head and Neck Surgery
University of California, San Francisco
Otorhinolaryngology – Head and Neck Surgery
Formerly known as ENTEarly Nights and TennisEasy, Not Tough
Ear, Nose, and Throat
Ear
Hearing Loss
Case #172 y/o woman with hearing loss and tinnitusOtologic History
No vertigo, otalgia, or otorrheaNo history of prior surgery or frequent infections
+ history of hearing loss in family (father and grandfather)Went to “Rock concerts” in the sixties

2
Case #1
PMH: noneMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane
Case #1
Tuning fork tests (512 Hz)Weber: MidlineRinne: Air conduction > Bone Conduction Bilaterally
Weber & Rinne Tests Audiogram
3
Diagnosis
PresbycusisTreatment
Consideration of Hearing AidsListening strategies and assistive devicesAvoidance of noise exposure
New Frontiers?Implantable hearing aidsCochlear Implants “partial insertion”
Case #2
Hearing Loss
Case #236 y/o woman with hearing loss and tinnitus
Symptoms worse on right sideOtologic History
No vertigo, otalgia, or otorrheaNo prior ear surgery No history of ear infections+ family history of hearing loss (mother in late 20’s)No history of noise exposure
Case #2
PMH: recently delivered first childMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane

4
Case #2Tuning fork tests (512 Hz)
Weber: To the RightRinne
Bone conduction > Air conduction bilaterally
Audiogram
Most Likely Diagnosis?
Meniere’s diseaseOtosclerosisOtitis Media with EffusionCholesteatomaAcoustic Neuroma
DiagnosisOtosclerosis
Disease of abnormal bone remodeling within the middle/inner earMost patients present with unilateral conductive hearing loss and normal TM examination
More severe cases may be bilateral with associated sensorineural hearing loss
Conductive loss due to fixation of the Stapes footplate within the Oval Window

5
Ear Picture Otosclerosis
Patients often have a family history of hearing lossIn women, symptoms may worsen during pregnancy
Otosclerosis
TreatmentHearing AidSurgery (Stapedectomy/Stapedotomy)
Stapes Surgery
Popularized by Dr. John Shea in the 1956Revolutionized treatment of otosclerosis
Stapes bone partially removedProsthesis inserted and linked to incus

6
Stapes Surgery
Results90% with complete or near complete correction of conductive component of hearing loss9% with no change in hearing1% with complete sensorineural loss
Post-op Audiogram
7
Post-op Audiogram
Case #3
Hearing Loss
Case #360 y/o woman with right-sided hearing loss and tinnitusOtologic History
No vertigo, otalgia, or otorrheaNo history of prior surgery or frequent infectionsNo history of hearing loss in family Went to “Rock concerts” in the sixties
Case #3
PMH: noneMeds: noneExam
Vth and VIIth nerves normalNormal appearance of tympanic membrane

8
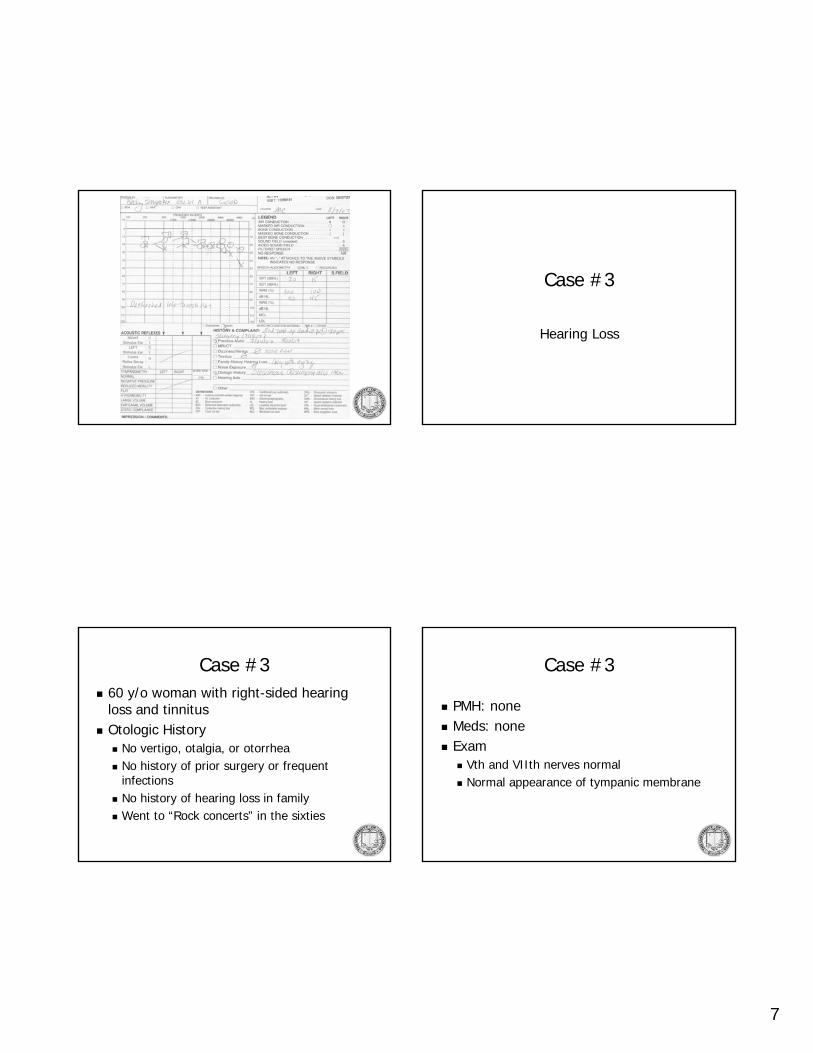
Case #3
Tuning fork tests (512 Hz)Weber MidlineRinne Air conduction > Bone Conduction Bilaterally
Audiogram
Next Step In Evaluation/Treatment?
Hearing Aid evaluation/referralCT scan of the brain/temporal boneCochlear implantationMRI of the brain/temporal bone
Diagnosis
Assymetric Sensorineural Hearing LossPlan: MRI
9
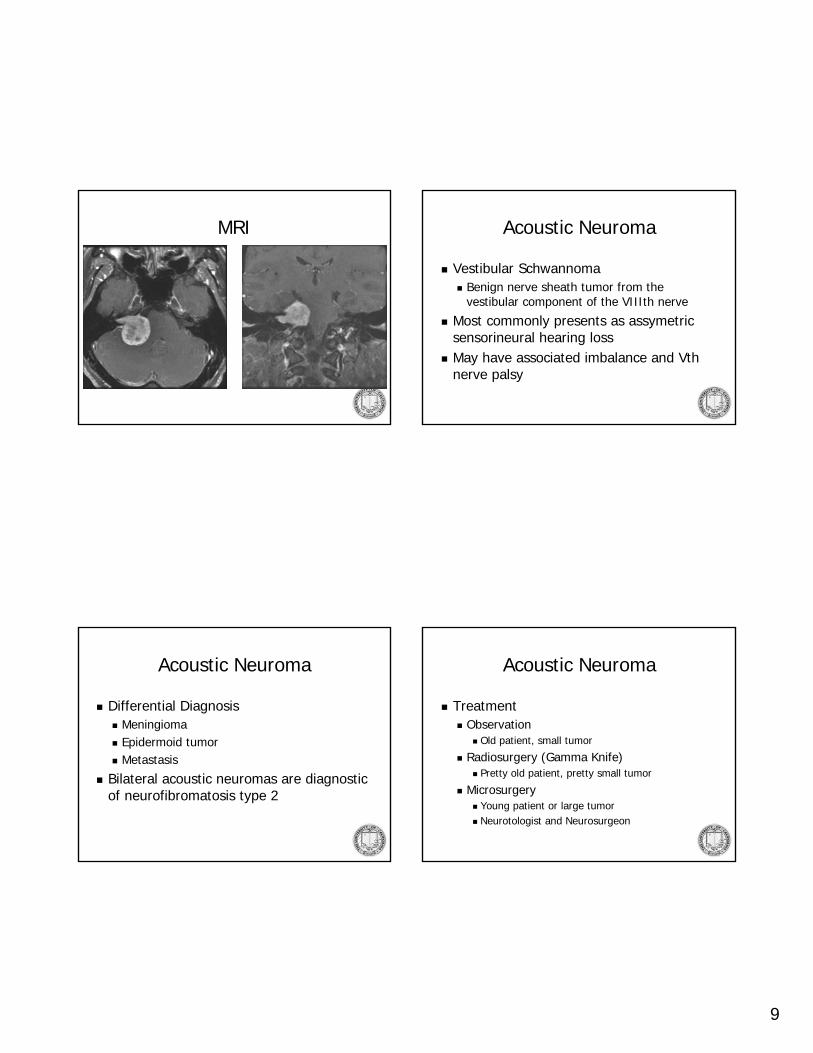
MRI Acoustic Neuroma
Vestibular SchwannomaBenign nerve sheath tumor from the vestibular component of the VIIIth nerve
Most commonly presents as assymetricsensorineural hearing lossMay have associated imbalance and Vthnerve palsy
Acoustic Neuroma
Differential DiagnosisMeningiomaEpidermoid tumorMetastasis
Bilateral acoustic neuromas are diagnostic of neurofibromatosis type 2
Acoustic Neuroma
TreatmentObservation
Old patient, small tumor
Radiosurgery (Gamma Knife)Pretty old patient, pretty small tumor
Microsurgery Young patient or large tumorNeurotologist and Neurosurgeon

10
Hearing Loss
Conductive SensorineuralCerumenImpactionTM Perforation Effusion/OMOtosclerosis
PresbycusisNoise InducedCongenitalAcoustic Neuroma
Nose
Nasal Congestion and Drainage
Case #444y/o man with nasal congestion and clear nasal drainageHPI
Frequent sneezingHeadachesItchy eyes
Case #4
PMH: asthmaMeds: sudafedExam
Bilateral inferior turbinate enlargementClear nasal mucus

11
Next Step In Evaluation/Treatment
Empiric trial of antihistamine/nasal steroidAllergy testingCT scan of the sinusesAntibiotic treatmentAnti-leukotriene medication
Case #4
DiagnosisAllergic Rhinitis
TreatmentTrial of antihistamine/nasal steroid sprayAllergy testingSinus CT scan if refractory symptoms
Allergic Rhinitis
Affects 35-50 million AmericansOften associated with other “atopic”symptoms
Allergic Rhinitis
Treatment OptionsAntihistamines (oral, intranasal)Steroid Nasal SpraysAllergen AvoidanceCromolyn Nasal SprayImmunotherapyAnti-leukotriene agentsDecongestants

12
Case #5
Nasal Congestion and Drainage
Case #544y/o man with nasal congestion and clear nasal drainage for 6 monthsHPI
“I Always have a cold”Facial congestion/pressureIntermittent HeadacheOccasional exacerbations with green/yellow drainageLoss of smell
Case #5
PMH: asthmaMeds: has tried nasonex, claritin, sudafed, and multiple antibiotics without improvementExam
Bilateral inferior turbinate enlargementClear nasal mucus
Sinusitis
Major FactorsFacial Pressure/PainFacial CongestionNasal ObstructionNasal DischargeHyposmia/AnosmiaPurulence on ExamFever (acute sinusitis)
Minor FactorsHeadacheFever (chronic sinusitis)HalitosisFatigueDental PainCoughEar pressure/fullness
13
Case #5
DiagnosisPossible Sinusitis
EvaluationNasal EndoscopyCT scan
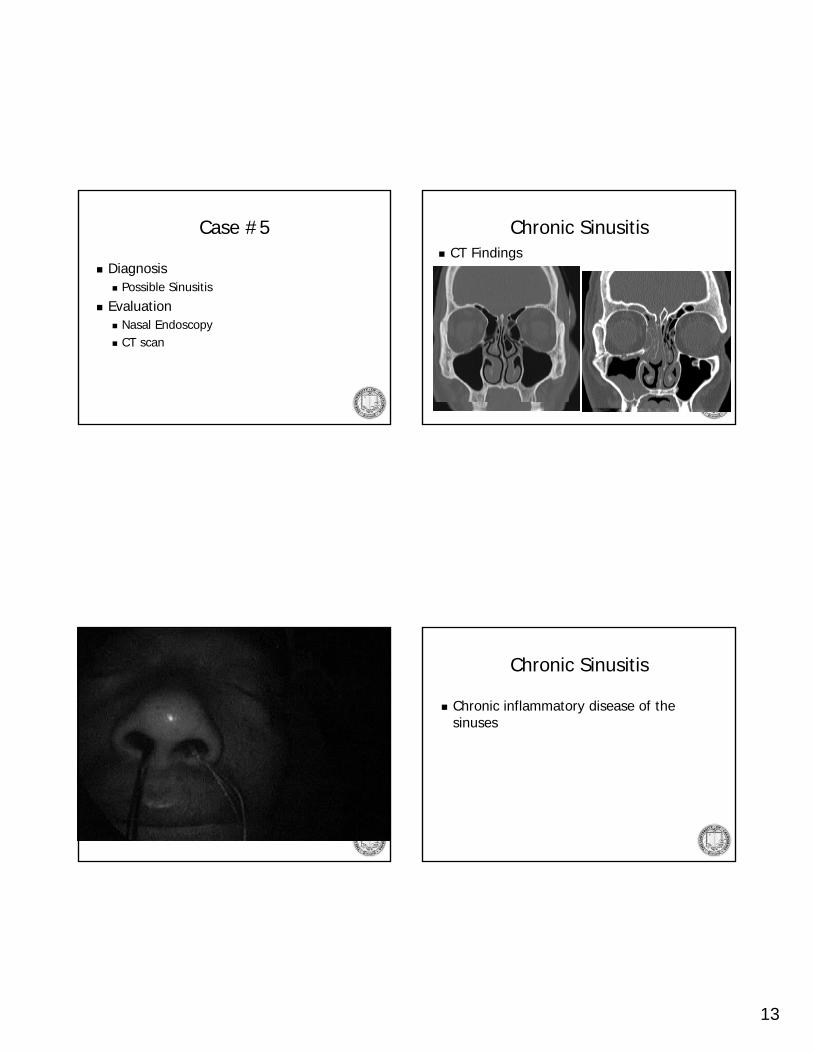
Chronic SinusitisCT Findings
Nasal Endoscopy Video Chronic Sinusitis
Chronic inflammatory disease of the sinuses

14
What Causes Chronic Sinusitis?
Bacterial InfectionFungal InfectionSystemic Immune DysfunctionImpaired Mucociliary Clearance
Chronic Sinusitis
TreatmentAntibiotics & Steroids (Oral vs. Topical)Surgery for patients refractory to medical management
Debridement Video
Case #6
Nasal Drainage

15
Case #644y/o woman with clear nasal drainage for 6 monthsHPI
Always right-sided“Gush of water” when I get up in the morningProfessional “9-ball” player, drips on pool table when she leans over to shootNo nasal congestion or facial pain/pressureRare headache
Case #6
PMH: ObesityMeds: has tried nasonex, claritin, sudafed, and multiple antibiotics without improvementExam
Normal nasal examPatient leans over …
Case #6
DiagnosisRhinorrhea … ? etiology
EvaluationNasal EndoscopyCollect fluid for Beta-2 Transferrin evaluation CT scan

16
CSF Leak
Post-surgicalEndoscopic Sinus SurgeryNeurosurgery (Pituitary and other skull base tumors)
Post-traumaticSpontaneous
CSF Leak
SpontaneousCommonly in obese, middle aged womenOften delay in diagnosisRisk of meningitis approximately 5%/year
May present with meningitis
Spontaneous CSF Leak
Endoscopic RepairIntrathecal flouresceinSkull base defect identified and cleaned Two-layer repair

17
SKULL BASE
MUCOSAL OVERLAY GRAFT
INTRACRANIALCAVITY
NASAL CAVITY
Two Layer RepairCARTILAGE UNDERLAY GRAFT

18
Throat
Hoarseness
Case #744y/o man with worsening hoarseness over the past 6 monthsHPI
Mild intermittent throat painDescribes voice as “gravely”Symptoms worse in morning and eveningGlobus sensation when swallowing, but no dysphagiaNon-smoker, drinks 2-3 glasses of wine/night
Case #7
PMH: HTNMeds: atenolol, ASA, occasional pepcidExam
Oral cavity WNLNo nasal abnormalitiesNo cervical adenopathy

19
Case #7
Laryngoscopy
Laryngopharyngeal Reflux
Laryngeal manifestations of GERDMay occur without symptoms of heartburn
Typical presentations include hoarseness, globus sensation, chronic sore throatVariable findings on laryngoscopy
20
Laryngopharyngeal Reflux
Gold-standard for diagnosis is 24 hour double pH probeOften treated empirically with PPIArea of controversy
Case #8
Hoarseness
Case #867y/o man with hoarseness for the past monthHPI
No painIncreased effort of speaking“Breathy” voiceVoice worsens throughout dayOccasional coughing with thin liquidsNon-smoker, drinks 2-3 glasses of wine/week
Case #8
PMH: HTNMeds: atenololExam
Oral cavity WNLNo nasal abnormalitiesNo cervical adenopathy

21
Case #8
Laryngoscopy
Unilateral Vocal Fold Paralysis
Compromise of the vagus or recurrent laryngeal nerve
Vagal injuries with associated sensory deficit and increased incidence of aspiration
Unilateral Vocal Fold Paralysis
PresentationHoarseness “Breathy voice”Vocal Fatigue? AspirationSymptoms worse with acute onset of injuryNOT associated with stridor/airway compromise

22
Unilateral Vocal Fold Paralysis
IatrogenicNeoplasticIdiopathic
Unilateral Vocal Fold Paralysis
Iatrogenics/p thyroidectomyAnterior approach C-spine surgeryCardiac SurgeryPosterior Fossa Neurosurgery
May be “stretch injury” with return of function up to 6 months following surgery
Unilateral Vocal Fold Paralysis
NeoplasticLaryngeal cancerThyroid malignanciesPulmonary malignancies Mediastinal metastasis or primary tumorsSkull base neoplasms
Unilateral Vocal Fold Paralysis
Idiopathic? ViralMay recover function 6-12 months following initial insult
23
Unilateral Vocal Fold Paralysis
Work-upImage the course of the recurrent laryngeal nerveLaryngeal EMG?
Unilateral Vocal Fold Paralysis
TreatmentTemporary
Vocal cord injection/medializationVarious materials, most last approx 4 months
PermanentLaryngeal framework surgery (Thyroplasty)Arytenoid adductionReinnervation surgeryTeflon (?Hydroxyapetite) injection
Case #9
Hoarseness

24
Case #954y/o man with worsening hoarseness over the past 6 monthsHPI
Mild intermittent throat painGlobus sensation when swallowing, but no dysphagia25 pack/year smoking history, drinks 6-pack of beer/night
Case #9
PMH: HTNMeds: atenolol, ASA, occasional pepcidExam
Oral cavity WNLNo nasal abnormalitiesNo cervical adenopathyHalitosis
Case #9
Laryngoscopy
25
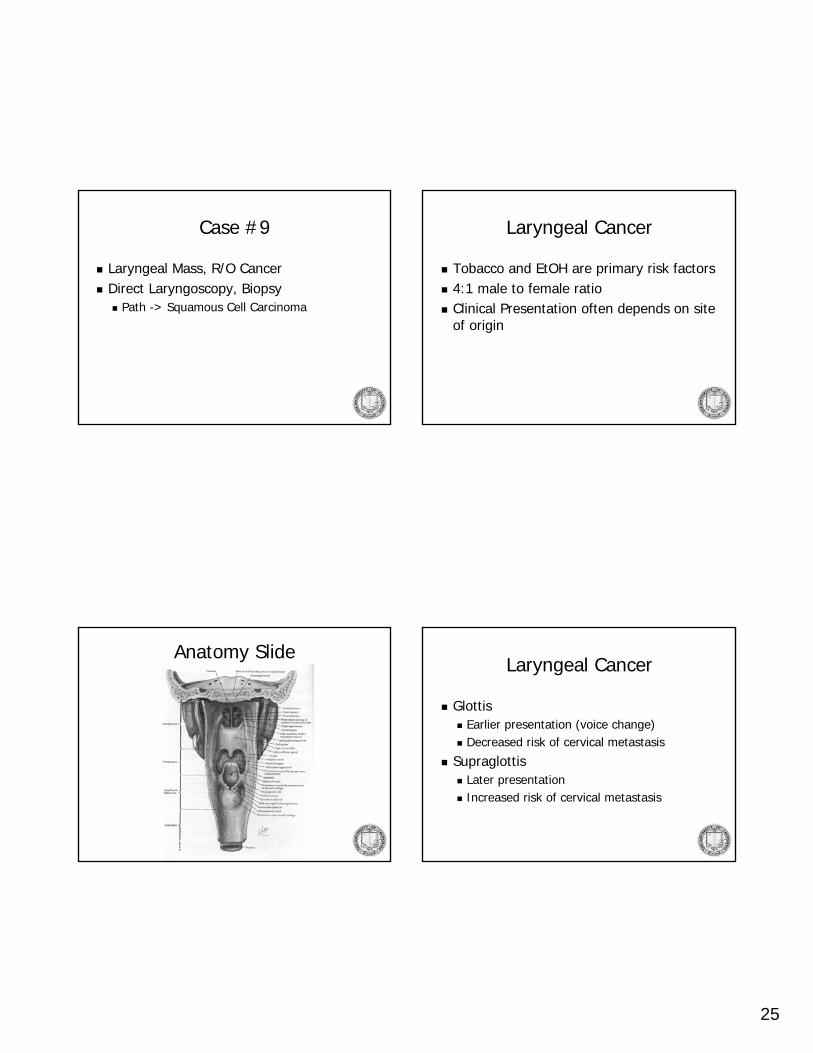
Case #9
Laryngeal Mass, R/O CancerDirect Laryngoscopy, Biopsy
Path -> Squamous Cell Carcinoma
Laryngeal Cancer
Tobacco and EtOH are primary risk factors4:1 male to female ratioClinical Presentation often depends on site of origin
Anatomy SlideLaryngeal Cancer
GlottisEarlier presentation (voice change)Decreased risk of cervical metastasis
SupraglottisLater presentationIncreased risk of cervical metastasis

26
Laryngeal Cancer
TreatmentSurgery, Radiation, and Chemotherapy are three treatment modalitiesStage of cancer and local expertise determines treatment approachOverall trend towards increased use of radiation/chemotherapy and “laryngeal conservation” surgery
Acknowledgements
Mark Courey and Jaime Chang UCSF Laryngology
Lawrence Lustig Otology/Neurotology









![Case Report - Hindawi Publishing Corporationdownloads.hindawi.com/journals/crim/2010/845671.pdf · in complete obstruction, dacryocystitis, otorrhea [4], foetor, anosmia, palatal](https://static.fdocuments.us/doc/165x107/5e55e030b0cf5f34b67fa0b7/case-report-hindawi-publishing-in-complete-obstruction-dacryocystitis-otorrhea.jpg)








